-
Start Preamble
Start Printed Page 16202
AGENCY:
Environmental Protection Agency (EPA).
ACTION:
Final rule.
SUMMARY:
Based on the Environmental Protection Agency's (EPA's) reconsideration of the air quality criteria and the national ambient air quality standards (NAAQS) for particulate matter (PM), the EPA is revising the primary annual PM2.5 standard by lowering the level from 12.0 µg/m3 to 9.0 µg/m3 . The Agency is retaining the current primary 24-hour PM2.5 standard and the primary 24-hour PM10 standard. The Agency also is not changing the secondary 24-hour PM2.5 standard, secondary annual PM2.5 standard, and secondary 24-hour PM10 standard at this time. The EPA is also finalizing revisions to other key aspects related to the PM NAAQS, including revisions to the Air Quality Index (AQI) and monitoring requirements for the PM NAAQS.
DATES:
This final rule is effective May 6, 2024.
ADDRESSES:
The EPA has established a docket for this action under Docket ID No. EPA–HQ–OAR–2015–0072. All documents in the docket are listed on the https://www.regulations.gov website. Although listed in the index, some information is not publicly available, e.g., CBI or other information whose disclosure is restricted by statute. Certain other material, such as copyrighted material, is not placed on the internet and will be publicly available only in hard copy form. Publicly available docket materials are available electronically through https://www.regulations.gov.
Start Further InfoFOR FURTHER INFORMATION CONTACT:
Dr. Lars Perlmutt, Health and Environmental Impacts Division, Office of Air Quality Planning and Standards, U.S. Environmental Protection Agency, Mail Code C539–04, Research Triangle Park, NC 27711; telephone: (919) 541–3037; fax: (919) 541–5315; email: perlmutt.lars@epa.gov.
End Further Info End Preamble Start Supplemental InformationSUPPLEMENTARY INFORMATION:
Table of Contents
The following topics are discussed in this preamble:
Executive Summary
I. Background
A. Legislative Requirements
B. Related PM Control Programs
C. Review of the Air Quality Criteria and Standards for Particulate Matter
1. Reviews Completed in 1971 and 1987
2. Review Completed in 1997
3. Review Completed in 2006
4. Review Completed in 2012
5. Review Initiated in 2014
a. 2020 Proposed and Final Decisions
b. Reconsideration of the 2020 PM NAAQS Final Action
D. Air Quality Information
1. Distribution of Particle Size in Ambient Air
2. Sources and Emissions Contributing to PM in the Ambient Air
3. Monitoring of Ambient PM
4. Ambient Concentrations and Trends
a. PM2.5 Mass
b. PM2.5 Components
c. PM10
d. PM10–2.5
e. UFP
5. Characterizing Ambient PM2.5 Concentrations for Exposure
a. Predicted Ambient PM2.5 and Exposure Based on Monitored Data
b. Comparison of PM2.5 Fields in Estimating Exposure and Relative to Design Values
6. Background PM
II. Rationale for Decisions on the Primary PM2.5 Standards
A. Introduction
1. Background on the Current Standards
2. Overview of the Health Effects Evidence
a. Nature of Effects
i. Mortality
ii. Cardiovascular Effects
iii. Respiratory Effects
iv. Cancer
v. Nervous System Effects
vi. Other Effects
b. Public Health Implications and At-Risk Populations
c. PM2.5 Concentrations in Key Studies Reporting Health Effects
i. PM2.5 Exposure Concentrations Evaluated in Experimental Studies
ii. Ambient PM2.5 Concentrations in Locations of Epidemiologic Studies
d. Uncertainties in the Health Effects Evidence
3. Summary of Exposure and Risk Estimates
a. Key Design Aspects
b. Key Limitations and Uncertainties
c. Summary of Risk Estimates
B. Conclusions on the Primary PM2.5 Standards
1. CASAC Advice
2. Basis for the Proposed Decision
3. Comments on the Proposed Decision
4. Administrator's Conclusions
C. Decisions on the Primary PM2.5 Standards
III. Rationale for Decisions on the Primary PM10 Standard
A. Introduction
1. Background on the Current Standard
2. Overview of Health Effects Evidence
a. Nature of Effects
i. Mortality
ii. Cardiovascular Effects
iii. Respiratory Effects
iv. Cancer
v. Metabolic Effects
vi. Nervous System Effects
B. Conclusions on the Primary PM10 Standard
1. CASAC Advice
2. Basis for the Proposed Decision
3. Comments on the Proposed Decision
4. Administrator's Conclusions
C. Decisions on the Primary PM10 Standard
IV. Communication of Public Health
A. Air Quality Index Overview
B. Air Quality Index Category Breakpoints for PM2.5
1. Summary of Proposed Revisions
a. Air Quality Index Values of 50, 100, and 150
b. Air Quality Index Values of 200 and Above
2. Summary of Significant Comments on Proposed Revisions
a. Air Quality Index Values of 50, 100, and 150
b. Air Quality Index Values of 200 and Above
c. Other Comments
3. Summary of Final Revisions
C. Air Quality Index Category Breakpoints for PM10
D. Air Quality Index Reporting
1. Summary of Proposed Revisions
2. Summary of Significant Comments on Proposed Revisions
3. Summary of Final Revisions
V. Rationale for Decisions on the Secondary PM Standards
A. Introduction
1. Background on the Current Standards
a. Non-Visibility Effects
b. Visibility Effects
2. Overview of Welfare Effects Evidence
a. Nature of Effects
i. Visibility
ii. Climate
iii. Materials
3. Summary of Air Quality and Quantitative Information
a. Visibility Effects
i. Target Level of Protection in Terms of a PM2.5 Visibility Index
ii. Relationship Between the PM2.5 Visibility Index and the Current Secondary 24-Hour PM2.5 Standard
b. Non-Visibility Effects
B. Conclusions on the Secondary PM Standards
1. CASAC Advice
2. Basis for the Proposed Decision
3. Comments on the Proposed Decision
4. Administrator's Conclusions
C. Decisions on the Secondary PM Standards
VI. Interpretation of the NAAQS for PM
A. Amendments to Appendix K: Interpretation of the NAAQS for Particulate Matter
B. Amendments to Appendix N: Interpretation of the NAAQS for PM2.5
VII. Amendments to Ambient Monitoring and Quality Assurance Requirements Start Printed Page 16203
A. Amendment to 40 CFR Part 50 (Appendix L): Reference Method for the Determination of Fine Particulate Matter as PM2.5 in the Atmosphere—Addition of the Tisch Cyclone as an Approved Second Stage Separator
B. Issues Related to 40 CFR Part 53 (Reference and Equivalent Methods)
C. Changes to 40 CFR Part 58 (Ambient Air Quality Surveillance)
D. Incorporating Data From Next-Generation Technologies
VIII. Clean Air Act Implementation Requirements for the Revised Primary Annual PM2.5 NAAQS
A. Designation of Areas
B. Section 110(a)(1) and (2) Infrastructure SIP Requirements
C. Implementing the Revised Primary Annual PM2.5 NAAQS in Nonattainment Areas
D. Implementing the Primary and Secondary PM10 NAAQS
E. Prevention of Significant Deterioration and Nonattainment New Source Review Programs for the Revised Primary Annual PM2.5 NAAQS
F. Transportation Conformity Program
G. General Conformity Program
IX. Statutory and Executive Order Reviews
A. Executive Order 12866: Regulatory Planning and Review and Executive Order 14094: Modernizing Regulatory Review
B. Paperwork Reduction Act (PRA)
C. Regulatory Flexibility Act (RFA)
D. Unfunded Mandates Reform Act (UMRA)
E. Executive Order 13132: Federalism
F. Executive Order 13175: Consultation and Coordination With Indian Tribal Governments
G. Executive Order 13045: Protection of Children From Environmental Health and Safety Risks
H. Executive Order 13211: Actions Concerning Regulations That Significantly Affect Energy Supply, Distribution or Use
I. National Technology Transfer and Advancement Act (NTTAA)
J. Executive Order 12898: Federal Actions To Address Environmental Justice in Minority Populations and Low-Income Populations and Executive Order 14096: Revitalizing Our Nation's Commitment to Environmental Justice for All
K. Congressional Review Act (CRA)
References
Executive Summary
This document presents the Administrator's final decisions for the reconsideration of the 2020 final decision on the primary (health-based) and secondary (welfare-based) National Ambient Air Quality Standards (NAAQS) for Particulate Matter (PM). More specifically, this document summarizes the background and rationale for the Administrator's final decisions to revise the primary annual PM2.5 standard by lowering the level from 12.0 µg/m3 to 9.0 µg/m3 ; to retain the current primary 24-hour PM2.5 standard (at a level of 35 µg/m3 ); to retain the primary 24-hour PM10 standard; and, not to change the secondary PM standards at this time. In reaching his final decisions, the Administrator considered the currently available scientific evidence in the 2019 Integrated Science Assessment (2019 ISA) and the Supplement to the 2019 ISA (ISA Supplement), quantitative and policy analyses presented in the 2022 Policy Assessment (2022 PA), advice from the Clean Air Scientific Advisory Committee (CASAC), and public comments on the proposal. The EPA has established primary and secondary standards for PM2.5, which includes particles with diameters generally less than or equal to 2.5 µm, and PM10, which includes particles with diameters generally less than or equal to 10 µm. The standards include two primary PM2.5 standards: an annual average standard, averaged over three years, with a level of 12.0 µg/m3 , and a 24-hour standard with a 98th percentile form, averaged over three years, and a level of 35 µg/m3 . It also includes a primary PM10 standard with a 24-hour averaging time, and a level of 150 µg/m3 , not to be exceeded more than once per year on average over three years. Secondary PM standards are set equal to the primary standards, except that the level of the secondary annual PM2.5 standard is 15.0 µg/m3 .
The most recent of the PM NAAQS was completed in December 2020. In that review, the EPA retained the primary and secondary NAAQS, without revision (85 FR 82684, December 18, 2020). Following publication of the 2020 final action, several parties filed petitions for review and petitions for reconsideration of the EPA's final decision.
In June 2021, the Agency announced its decision to reconsider the 2020 PM NAAQS final action.[1] The EPA decided to reconsider the December 2020 decision because the available scientific evidence and technical information indicated that the current standards may not be adequate to protect public health and welfare, as required by the Clean Air Act. The EPA noted that the 2020 PA concluded that the scientific evidence and information called into question the adequacy of the primary PM2.5 standards and supported consideration of revising the level of the primary annual PM2.5 standard to below the current level of 12.0 µg/m3 while retaining the primary 24-hour PM2.5 standard (U.S. EPA, 2020b). The EPA also noted that the 2020 PA concluded that the available scientific evidence and information did not call into question the adequacy of the primary PM10 or secondary PM standards and supported consideration of retaining the primary PM10 standard and secondary PM standards without revision (U.S. EPA, 2020b).
The final decisions presented in this document on the primary PM2.5 standards have been informed by key aspects of the available health effects evidence and conclusions contained in the 2019 ISA and ISA Supplement, quantitative exposure/risk analyses and policy evaluations presented in the 2022 PA, advice from the CASAC [2] and public comment received as part of this reconsideration.[3] The health effects evidence newly available in this reconsideration, in conjunction with the full body of evidence critically evaluated in the 2019 ISA, supports a causal relationship between long- and short-term exposures and mortality and cardiovascular effects, and the evidence supports a likely to be a causal relationship between long-term exposures and respiratory effects, nervous system effects, and cancer. The longstanding evidence base, including animal toxicological studies, controlled human exposure studies, and epidemiologic studies, reaffirms, and in some cases strengthens, the conclusions from past reviews regarding the health effects of PM2.5 exposures. Epidemiologic studies available in this reconsideration demonstrate generally positive, and often statistically significant, PM2.5 health effect associations. Such studies report associations between estimated PM2.5 exposures and non-accidental, cardiovascular, or respiratory mortality; cardiovascular or respiratory hospitalizations or emergency room visits; and other mortality/morbidity outcomes ( e.g., lung cancer mortality or incidence, asthma development). The scientific evidence available in this reconsideration, as evaluated in the 2019 ISA and ISA Supplement, includes Start Printed Page 16204 a number of epidemiologic studies that use various methods to characterize exposure to PM2.5 ( e.g., ground-based monitors and hybrid modeling approaches) and to evaluate associations between health effects and lower ambient PM2.5 concentrations. There are a number of recent epidemiologic studies that use varying study designs that reduce uncertainties related to confounding and exposure measurement error. The results of these analyses provide further support for the robustness of associations between PM2.5 exposures and mortality and morbidity. Moreover, the Administrator notes that recent epidemiologic studies strengthen support for health effect associations at lower PM2.5 concentrations, with these new studies finding positive and significant associations when assessing exposure in locations and time periods with lower annual mean and 25th percentile concentrations than those evaluated in epidemiologic studies available at the time of previous reviews. Additionally, the experimental evidence ( i.e., animal toxicological and controlled human exposure studies) strengthens the coherence of effects across scientific disciplines and provides additional support for potential biological pathways through which PM2.5 exposures could lead to the overt population-level outcomes reported in epidemiologic studies for the health effect categories for which a causal relationship ( i.e., short- and long-term PM2.5 exposure and mortality and cardiovascular effects) or likely to be causal relationship ( i.e., short- and long-term PM2.5 exposure and respiratory effects; and long-term PM2.5 exposure and nervous system effects and cancer) was concluded.
The available evidence in the 2019 ISA continues to provide support for factors that may contribute to increased risk of PM2.5 -related health effects including lifestage (children and older adults), pre-existing diseases (cardiovascular disease and respiratory disease), race/ethnicity, and socioeconomic status. For example, the 2019 ISA and ISA Supplement conclude that there is strong evidence that Black and Hispanic populations, on average, experience higher PM2.5 exposures and PM2.5 -related health risks than non-Hispanic White populations. In addition, studies evaluated in the 2019 ISA and ISA Supplement also provide evidence indicating that communities with lower socioeconomic status (SES), as assessed in epidemiologic studies using indicators of SES including income and educational attainment are, on average, exposed to higher concentrations of PM2.5 compared to higher SES communities.
The quantitative risk assessment, as well as policy considerations in the 2022 PA, also inform the final decisions on the primary PM2.5 standards. The risk assessment in this reconsideration focuses on all-cause or nonaccidental mortality associated with long- and short-term PM2.5 exposures. The primary analyses focus on exposure and risk associated with air quality that might occur in an area under air quality conditions that just meet the current and potential alternative standards. The risk assessment estimates that the current primary PM2.5 standards could allow a substantial number of PM2.5 -associated premature deaths in the United States, and that public health improvements would be associated with just meeting all of the alternative (more stringent) annual and 24-hour standard levels modeled. Additionally, the results of the risk assessment suggest that for most of the U.S., the annual standard is the controlling standard and that revision to that standard has the most potential to reduce PM2.5 exposure-related risk. The analyses are summarized in this document and in the proposal and are described in detail in the 2022 PA.
In its advice to the Administrator, in its review of the 2021 draft PA, the CASAC concurred that the currently available health effects evidence calls into question the adequacy of the primary annual PM2.5 standard. With regard to the primary annual PM2.5 standard, the majority of the CASAC concluded that the level of the standard should be revised within the range of 8.0 to 10.0 µg/m3 , while the minority of the CASAC concluded that the primary annual PM2.5 standard should be revised to a level of 10.0 to 11.0 µg/m3 . With regard to the primary 24-hour PM2.5 standard, the CASAC did not reach consensus on the adequacy of the current standard. The majority of the CASAC concluded that the primary 24-hour PM2.5 was not adequate and that the level of the standard should be revised to within the range of 25 to 30 µg/m3 , while the minority of the CASAC concluded that the standard was adequate and should be retained, without revision. Additionally, in their review of the 2019 draft PA, the CASAC did not reach consensus on the adequacy of the primary annual PM2.5 standard, with the minority recommending revision and the majority recommending the standard be retained. In their review of the 2019 draft PA, the CASAC reached consensus regarding the adequacy of the primary 24-hour PM2.5 standard, concluding that the standard should be retained.
In considering how to revise the suite of primary PM2.5 standards to provide the requisite degree of protection, the Administrator recognizes that the current annual standard and 24-hour standard, together, are intended to provide public health protection against the full distribution of short- and long-term PM2.5 exposures. Further, he recognizes that changes in PM2.5 air quality designed to meet either the annual or the 24-hour standard would likely result in changes to both long-term average and short-term peak PM2.5 concentrations.
As in 2012, the Administrator concludes that the most effective way to reduce total population risk associated with both long- and short-term PM2.5 exposures is to set a generally controlling annual standard, and to provide supplemental protection against the occurrence of peak 24-hour PM2.5 concentrations by means of a 24-hour standard set at the appropriate level. Based on the current evidence and quantitative information, as well as consideration of CASAC advice and public comments, the Administrator concludes that the current primary annual PM2.5 standard is not adequate to protect public health with an adequate margin of safety. The Administrator notes that the CASAC was unanimous in its advice on the 2021 draft PA regarding the need to revise the annual standard. In considering the appropriate level for a revised annual standard, the Administrator concludes that a standard set at a level of 9.0 µg/m3 reflects his judgment about placing the most weight on the strongest available evidence while appropriately weighing the uncertainties.
With regard to the primary 24-hour PM2.5 standard, the Administrator finds the available scientific evidence and quantitative information to be insufficient to call into question the adequacy of the public health protection afforded by the current 24-hour standard. He further notes that a more stringent annual standard set at a level of 9.0 µg/m3 is expected to reduce both average (annual) concentrations and peak (daily) concentrations. The Administrator also notes that, in their review of the 2021 draft PA, the CASAC did not reach consensus on whether revisions to the primary 24-hour PM2.5 standard are warranted at this time. He also notes that, in their review of the 2019 draft PA, the CASAC did reach consensus that the primary 24-hour PM2.5 standard should be retained. The Administrator concludes that the 24-hour standard should be retained to Start Printed Page 16205 continue to provide requisite protection against short-term peak PM2.5 concentrations, particularly when considered in conjunction with the protection provided by the suite of standards and the decision to revise the annual standard to a level of 9.0 µg/m3 .
The primary PM10 standard is intended to provide public health protection against health effects related to exposures to PM10–2.5, which are particles with a diameter between 10 µm and 2.5 µm. The final decision to retain the current 24-hour PM10 standard has been informed by key aspects of the available health effects evidence and conclusions contained in the 2019 ISA, the policy evaluations presented in the 2022 PA, advice from the CASAC and public comments. Specifically, the health effects evidence for PM10–2.5 exposures is somewhat strengthened since past reviews, although the strongest evidence still only provides support for a suggestive of, but not sufficient to infer, causal relationship with long- and short-term exposures and mortality and cardiovascular effects, short-term exposures and respiratory effects, and long-term exposures and cancer, nervous system effects, and metabolic effects. In reaching his final decision on the primary PM10 standard, the Administrator recognizes that, while the available health effects evidence has expanded, recent studies are subject to the same types of uncertainties that were judged to be important in previous reviews. He also recognizes that, in their review of the 2019 draft PA and the 2021 draft PA, the CASAC generally agreed that it was reasonable to retain the primary 24-hour PM10 standard given the available scientific evidence, including retaining PM10 as the indicator. He concludes that the newly available evidence does not call into question the adequacy of the current primary PM10 standard, and retains that standard, without revision.
With respect to the secondary PM standards, this reconsideration focuses on visibility, climate, and materials effects.[4] The Administrator's final decision to not change the current secondary standards at this time has been informed by key aspects of the currently available welfare effects evidence as well as the conclusions contained in the 2019 ISA and ISA Supplement; quantitative analyses of visibility impairment; policy evaluations presented in the 2022 PA; advice from the CASAC; and public comments. Specifically, the welfare effects evidence available in this reconsideration is consistent with the evidence available in previous reviews and supports a causal relationship between PM and visibility, climate, and materials effects. With regard to visibility effects, the Administrator notes that he judges that the evidence supports a target level of protection of 27 dv. He further notes that the results of quantitative analyses of visibility impairment suggest that in areas that meet the current secondary 24-hour PM2.5 standard that estimated light extinction in terms of a 3-year visibility metric would be at or well below the target level of protection. With regard to climate and materials effects, while the evidence has expanded since previous reviews, significant limitations and uncertainties remain in the evidence. While the evidence has expanded since previous reviews, the available scientific evidence remains insufficient to allow the Administrator to make a reasoned judgment about what specific standard(s) would be requisite to protect against known or anticipated adverse effects to public welfare from PM's effects on materials damage or climate.-In their review of the 2019 draft PA and the 2021 draft PA, the CASAC did not recommend revising the secondary PM standards. In considering the available evidence and quantitative information, with its inherent uncertainties and limitations, the Administrator judges that it is appropriate not to change the secondary PM standards at this time.
The final revisions to the primary annual PM2.5 NAAQS trigger a process under which States (and Tribes, if they choose) make recommendations to the Administrator regarding designations, identifying areas of the country that either meet or do not meet the new or revised PM NAAQS. Those areas that do not meet the revised PM NAAQS will need to develop plans that demonstrate how they will meet the standards. As part of these plans, states have the opportunity to advance environmental justice, in this case for overburdened communities in areas with high PM concentrations above the NAAQS, by using the tools described in the current PM NAAQS implementation guidance (80 FR 58010, 58136, August 25, 2016). The EPA is not making changes to any of the current PM NAAQS implementation programs in this final rulemaking.
On other topics, the EPA is finalizing two sets of changes to the PM2.5 sub-index of the Air Quality Index (AQI). First, the EPA is continuing to use the approach used in the revisions to the AQI in 2012 (77 FR 38890, June 29, 2012) of setting the lower breakpoints (50, 100 and 150) based on the levels of the primary annual and 24-hour PM2.5 standards. In so doing, the EPA is revising the AQI value of 50 to 9.0 µg/m3 and is retaining the AQI values of 100 and 150 at 35.4 µg/m3 and 55.4 µg/m3 , respectively. Second, the EPA is revising the upper AQI breakpoints (200 and above), and replacing the linear-relationship approach used in 1999 (64 FR 42530, August 4, 1999) to set these breakpoints, with an approach that more fully considers the PM2.5 health effects evidence from controlled human exposure and epidemiologic studies that has become available in the last 20 years. The EPA is also revising the AQI values of 200, 300 and 500 to 125.4 µg/m3 , 225.4 µg/m3 , and 325.4 µg/m3 , respectively. In addition, this final rule revises the daily reporting requirement from 5 days per week to 7 days per week, while also reformatting appendix G and providing clarifications.
With regard to monitoring-related activities, the EPA finalizes revisions to data calculations and ambient air monitoring requirements for PM to improve the usefulness and appropriateness of data used in regulatory decision making and to better characterize air quality in communities that are at increased risk of PM2.5 exposure and health risk. These changes are found in 40 CFR part 50 (appendices K, L, and N), part 53, and part 58 with associated appendices (A, B, C, D, and E). These changes include addressing updates in data calculations, approval of reference and equivalent methods, updates in quality assurance statistical calculations to account for lower concentration measurements, updates to support improvements in PM methods, a revision to the PM2.5 network design to account for at-risk populations, and updates to the Probe and Monitoring Path Siting Criteria for NAAQS pollutants.
In setting the NAAQS, the EPA may not consider the costs of implementing the standards. This was confirmed by the Supreme Court in Whitman v. American Trucking Associations, 531 U.S. 457, 465–472, 475–76 (2001), as discussed in section II.A of this document. As has traditionally been Start Printed Page 16206 done in NAAQS rulemaking, the EPA prepared a Regulatory Impact Analysis (RIA) to provide the public with information on the potential costs and benefits of attaining several alternative PM2.5 standard levels. In NAAQS rulemaking, the RIA is done for informational purposes only, and the final decisions on the NAAQS in this rulemaking are not based on consideration of the information or analyses in the RIA. The RIA fulfills the requirements of Executive Orders 14094, 13563, and 12866. The RIA estimates the costs and monetized human health benefits of attaining the revised and two alternative annual PM2.5 standard levels and one alternative 24-hour PM2.5 standard level. Specifically, the RIA examines the revised annual standard level of 9.0 µg/m3 in combination with the current 24-hour standard of 35 µg/m3 ( i.e., 9.0/35 µg/m3 ), as well as the following less and more stringent alternative standard levels: (1) An alternative annual standard level of 10.0 µg/m3 in combination with the current 24-hour standard ( i.e., 10.0/35 µg/m3 ), (2) an alternative annual standard level of 8.0 µg/m3 in combination with the current 24-hour standard ( i.e., 8.0/35 µg/m3 ), and (3) an alternative 24-hour standard level of 30 µg/m3 in combination with an alternative annual standard level of 10 µg/m3 ( i.e., 10.0/30 µg/m3 ). The RIA presents estimates of the costs and benefits of applying illustrative national control strategies in 2032 after implementing existing and expected regulations and assessing emissions reductions to meet the current annual and 24-hour particulate matter NAAQS (12.0/35 µg/m3 ).
I. Background
A. Legislative Requirements
Two sections of the Clean Air Act (CAA) govern the establishment and revision of the NAAQS. Section 108 (42 U.S.C. 7408) directs the Administrator to identify and list certain air pollutants and then to issue air quality criteria for those pollutants. The Administrator is to list those pollutants “emissions of which, in his judgment, cause or contribute to air pollution which may reasonably be anticipated to endanger public health or welfare”; “the presence of which in the ambient air results from numerous or diverse mobile or stationary sources”; and for which he “plans to issue air quality criteria. . . .” (42 U.S.C. 7408(a)(1)). Air quality criteria are intended to “accurately reflect the latest scientific knowledge useful in indicating the kind and extent of all identifiable effects on public health or welfare which may be expected from the presence of [a] pollutant in the ambient air. . . .” (42 U.S.C. 7408(a)(2)).
Section 109 [42 U.S.C. 7409] directs the Administrator to propose and promulgate “primary” and “secondary” NAAQS for pollutants for which air quality criteria are issued [42 U.S.C. 7409(a)]. Section 109(b)(1) defines primary standards as ones “the attainment and maintenance of which in the judgment of the Administrator, based on such criteria and allowing an adequate margin of safety, are requisite to protect the public health.” [5] Under section 109(b)(2), a secondary standard must “specify a level of air quality the attainment and maintenance of which, in the judgment of the Administrator, based on such criteria, is requisite to protect the public welfare from any known or anticipated adverse effects associated with the presence of [the] pollutant in the ambient air.” [6]
In setting primary and secondary standards that are “requisite” to protect public health and welfare, respectively, as provided in section 109(b), the EPA's task is to establish standards that are neither more nor less stringent than necessary. In so doing, the EPA may not consider the costs of implementing the standards. See generally Whitman v. American Trucking Associations, 531 U.S. 457, 465–472, 475–76 (2001). Likewise, “[a]ttainability and technological feasibility are not relevant considerations in the promulgation of national ambient air quality standards.” American Petroleum Institute v. Costle, 665 F.2d 1176, 1185 (D.C. Cir. 1981); accord Murray Energy Corporation v. EPA, 936 F.3d 597, 623–24 (D.C. Cir. 2019).
The requirement that primary standards provide an adequate margin of safety was intended to address uncertainties associated with inconclusive scientific and technical information available at the time of standard setting. It was also intended to provide a reasonable degree of protection against hazards that research has not yet identified. See Lead Industries Association v. EPA, 647 F.2d 1130, 1154 (D.C. Cir. 1980); American Petroleum Institute v. Costle, 665 F.2d at 1186; Coalition of Battery Recyclers Ass'n v. EPA, 604 F.3d 613, 617–18 (D.C. Cir. 2010); Mississippi v. EPA, 744 F.3d 1334, 1353 (D.C. Cir. 2013). Both kinds of uncertainties are components of the risk associated with pollution at levels below those at which human health effects can be said to occur with reasonable scientific certainty. Thus, in selecting primary standards that include an adequate margin of safety, the Administrator is seeking not only to prevent pollution levels that have been demonstrated to be harmful but also to prevent lower pollutant levels that may pose an unacceptable risk of harm, even if the risk is not precisely identified as to nature or degree. The CAA does not require the Administrator to establish a primary NAAQS at a zero-risk level or at background concentration levels, see Lead Industries Ass'n v. EPA, 647 F.2d at 1156 n.51, Mississippi v. EPA, 744 F.3d at 1351, but rather at a level that reduces risk sufficiently so as to protect public health with an adequate margin of safety.
In addressing the requirement for an adequate margin of safety, the EPA considers such factors as the nature and severity of the health effects involved, the size of the sensitive population(s), and the kind and degree of uncertainties. The selection of any particular approach to providing an adequate margin of safety is a policy choice left specifically to the Administrator's judgment. See Lead Industries Ass'n v. EPA, 647 F.2d at 1161–62; Mississippi v. EPA, 744 F.3d at 1353.
Section 109(d)(1) of the Act requires the review every five years of existing air quality criteria and, if appropriate, the revision of those criteria to reflect advances in scientific knowledge on the effects of the pollutant on public health and welfare. Under the same provision, the EPA is also to review every five years and, if appropriate, revise the NAAQS, based on the revised air quality criteria. Section 109(d)(1) also provides that the Administrator may review and revise criteria or promulgate new standards earlier or more frequently.
Section 109(d)(2) addresses the appointment and advisory functions of an independent scientific review committee. Section 109(d)(2)(A) requires the Administrator to appoint this committee, which is to be composed of “seven members including at least one member of the National Academy of Sciences, one physician, and one person representing State air Start Printed Page 16207 pollution control agencies.” Section 109(d)(2)(B) provides that the independent scientific review committee “shall complete a review of the criteria . . . and the national primary and secondary ambient air quality standards . . . and shall recommend to the Administrator any new . . . standards and revisions of existing criteria and standards as may be appropriate. . . .” Since the early 1980s, this independent review function has been performed by the Clean Air Scientific Advisory Committee (CASAC) of the EPA's Science Advisory Board.
As previously noted, the Supreme Court has held that section 109(b) “unambiguously bars cost considerations from the NAAQS-setting process.” Whitman v. Am. Trucking Associations, 531 U.S. 457, 471 (2001). Accordingly, while some of these issues regarding which Congress has directed the CASAC to advise the Administrator are ones that are relevant to the standard setting process, others are not. Issues that are not relevant to standard setting may be relevant to implementation of the NAAQS once they are established.
B. Related PM Control Programs
States are primarily responsible for ensuring attainment and maintenance of ambient air quality standards once the EPA has established them. Under section 110, Part C, and Part D, Subparts 1 and 4 of the CAA, and related provisions and regulations, States are to submit, for the EPA's approval, State implementation plans (SIPs) that provide for the attainment and maintenance of the NAAQS for PM through control programs directed to sources of the pollutants involved. The States, in conjunction with the EPA, also administer the prevention of significant deterioration of air quality program that covers these pollutants (see 42 U.S.C. 7470–7479). In addition, Federal programs provide for or result in nationwide reductions in emissions of PM and its precursors under Title II of the Act, 42 U.S.C. 7521–7574, which involves controls for motor vehicles and nonroad engines and equipment; the new source performance standards under section 111 of the Act, 42 U.S.C. 7411; and the national emissions standards for hazardous pollutants under section 112 of the Act, 42 U.S.C. 7412.
C. Review of the Air Quality Criteria and Standards for Particulate Matter
1. Reviews Completed in 1971 and 1987
The EPA first established NAAQS for PM in 1971 (36 FR 8186, April 30, 1971), based on the original Air Quality Criteria Document (AQCD) (DHEW, 1969).[7] The Federal reference method (FRM) specified for determining attainment of the original standards was the high-volume sampler, which collects PM up to a nominal size of 25 to 45 µm (referred to as total suspended particulates or TSP). The primary standards were set at 260 µg/m3 , 24-hour average, not to be exceeded more than once per year, and 75 µg/m3 , annual geometric mean. The secondary standards were set at 150 µg/m3 , 24-hour average, not to be exceeded more than once per year, and 60 µg/m3 , annual geometric mean.
In October 1979 (44 FR 56730, October 2, 1979), the EPA announced the first periodic review of the air quality criteria and NAAQS for PM. Revised primary and secondary standards were promulgated in 1987 (52 FR 24634, July 1, 1987). In the 1987 decision, the EPA changed the indicator for particles from TSP to PM10 , in order to focus on the subset of inhalable particles small enough to penetrate to the thoracic region of the respiratory tract (including the tracheobronchial and alveolar regions), referred to as thoracic particles.[8] The level of the 24-hour standards (primary and secondary) was set at 150 µg/m3 , and the form was one expected exceedance per year, on average over three years. The level of the annual standards (primary and secondary) was set at 50 µg/m3 , and the form was the annual arithmetic mean, averaged over three years.
2. Review Completed in 1997
In April 1994, the EPA announced its plans for the second periodic review of the air quality criteria and NAAQS for PM, and in 1997 the EPA promulgated revisions to the NAAQS (62 FR 38652, July 18, 1997). In the 1997 decision, the EPA determined that the fine and coarse fractions of PM10 should be considered separately. This determination was based on evidence that serious health effects were associated with short- and long-term exposures to fine particles in areas that met the existing PM10 standards. The EPA added new standards, using PM2.5 as the indicator for fine particles (with PM2.5 referring to particles with a nominal mean aerodynamic diameter less than or equal to 2.5 µm). The new primary standards were as follows: (1) An annual standard with a level of 15.0 µg/m[3] , based on the 3-year average of annual arithmetic mean PM2.5 concentrations from single or multiple community-oriented monitors; [9] and (2) a 24-hour standard with a level of 65 µg/m3 , based on the 3-year average of the 98th percentile of 24-hour PM2.5 concentrations at each monitor within an area. Also, the EPA established a new reference method for the measurement of PM2.5 in the ambient air and adopted rules for determining attainment of the new standards. To continue to address the health effects of the coarse fraction of PM10 (referred to as thoracic coarse particles or PM10–2.5, generally including particles with a nominal mean aerodynamic diameter greater than 2.5 µm and less than or equal to 10 µm), the EPA retained the primary annual PM10 standard and revised the form of the primary 24-hour PM10 standard to be based on the 99th percentile of 24-hour PM10 concentrations at each monitor in an area. The EPA revised the secondary standards by setting them equal in all respects to the primary standards.
Following promulgation of the 1997 PM NAAQS, petitions for review were filed by several parties, addressing a broad range of issues. In May 1999, the U.S. Court of Appeals for the District of Columbia Circuit (D.C. Circuit) upheld the EPA's decision to establish fine particle standards and to regulate coarse particle pollution, but vacated the 1997 PM10 standards, concluding that the EPA had not provided a reasonable explanation justifying use of PM10 as an indicator for coarse particles. American Trucking Associations, Inc. v. EPA, 175 F. 3d 1027 (D.C. Cir. 1999). Pursuant to the D.C. Circuit's decision, the EPA removed the vacated 1997 PM10 standards, and the pre-existing 1987 PM10 standards remained in place (65 FR 80776, December 22, 2000). The D.C. Circuit also upheld the EPA's determination not to establish more stringent secondary standards for fine particles to address effects on visibility. American Trucking Associations v. EPA, 175 F. 3d at 1027. Start Printed Page 16208
The D.C. Circuit also addressed more general issues related to the NAAQS, including issues related to the consideration of costs in setting NAAQS and the EPA's approach to establishing the levels of NAAQS. Regarding the cost issue, the court reaffirmed prior rulings holding that in setting NAAQS the EPA is “not permitted to consider the cost of implementing those standards.” American Trucking Associations v. EPA, 175 F. 3d at 1040–41. Regarding the levels of NAAQS, the court held that the EPA's approach to establishing the level of the standards in 1997 ( i.e., both for PM and for the ozone NAAQS promulgated on the same day) effected “an unconstitutional delegation of legislative authority.” American Trucking Associations v. EPA, 175 F. 3d at 1034–40. Although the court stated that “the factors EPA uses in determining the degree of public health concern associated with different levels of ozone and PM are reasonable,” it remanded the rule to the EPA, stating that when the EPA considers these factors for potential non-threshold pollutants “what EPA lacks is any determinate criterion for drawing lines” to determine where the standards should be set.
The D.C. Circuit's holding on the cost and constitutional issues were appealed to the United States Supreme Court. In February 2001, the Supreme Court issued a unanimous decision upholding the EPA's position on both the cost and constitutional issues. Whitman v. American Trucking Associations, 531 U.S. 457, 464, 475–76. On the constitutional issue, the Court held that the statutory requirement that NAAQS be “requisite” to protect public health with an adequate margin of safety sufficiently guided the EPA's discretion, affirming the EPA's approach of setting standards that are neither more nor less stringent than necessary.
The Supreme Court remanded the case to the D.C. Circuit for resolution of any remaining issues that had not been addressed in that court's earlier rulings. Id. at 475–76. In a March 2002 decision, the D.C. Circuit rejected all remaining challenges to the standards, holding that the EPA's PM2.5 standards were reasonably supported by the administrative record and were not “arbitrary and capricious.” American Trucking Associations v. EPA, 283 F. 3d 355, 369–72 (D.C. Cir. 2002).
3. Review Completed in 2006
In October 1997, the EPA published its plans for the third periodic review of the air quality criteria and NAAQS for PM (62 FR 55201, October 23, 1997). After the CASAC and public review of several drafts, the EPA's National Center for Environmental Assessment (NCEA) finalized the AQCD in October 2004 (U.S. EPA, 2004a). The EPA's Office of Air Quality Planning and Standards (OAQPS) finalized a Risk Assessment and Staff Paper in December 2005 (Abt Associates, 2005; U.S. EPA, 2005).[10] On December 20, 2005, the EPA announced its proposed decision to revise the NAAQS for PM and solicited public comment on a broad range of options (71 FR 2620, January 17, 2006). On September 21, 2006, the EPA announced its final decisions to revise the primary and secondary NAAQS for PM to provide increased protection of public health and welfare, respectively (71 FR 61144, October 17, 2006). With regard to the primary and secondary standards for fine particles, the EPA revised the level of the 24-hour PM2.5 standards to 35 µg/m3 , retained the level of the annual PM2.5 standards at 15.0 µg/m3 , and revised the form of the annual PM2.5 standards by narrowing the constraints on the optional use of spatial averaging. With regard to the primary and secondary standards for PM10 , the EPA retained the 24-hour standards, with levels at 150 µg/m3 , and revoked the annual standards. The then-Administrator judged that the available evidence generally did not suggest a link between long-term exposure to existing ambient levels of coarse particles and health or welfare effects. In addition, a new reference method was added for the measurement of PM10–2.5 in the ambient air in order to provide a basis for approving Federal Equivalent Methods (FEMs) and to promote the gathering of scientific data to support future reviews of the PM NAAQS.
Several parties filed petitions for review following promulgation of the revised PM NAAQS in 2006. On February 24, 2009, the D.C. Circuit issued its opinion in the case American Farm Bureau Federation v. EPA, 559 F. 3d 512 (D.C. Cir. 2009). The court remanded the primary annual PM2.5 NAAQS to the EPA because the Agency had failed to adequately explain why the standards provided the requisite protection from both short- and long-term exposures to fine particles, including protection for at-risk populations. Id. at 520–27. With regard to the standards for PM10, the court upheld the EPA's decisions to retain the 24-hour PM10 standard to provide protection from thoracic coarse particle exposures and to revoke the annual PM10 standard. Id. at 533–38. With regard to the secondary PM2.5 standards, the court remanded the standards to the EPA because the Agency failed to adequately explain why setting the secondary PM standards identical to the primary standards provided the required protection for public welfare, including protection from visibility impairment. Id. at 528–32. The EPA responded to the court's remands as part of the next review of the PM NAAQS, which was initiated in 2007 (discussed below).
4. Review Completed in 2012
In June 2007, the EPA initiated the fourth periodic review of the air quality criteria and the PM NAAQS by issuing a call for information (72 FR 35462, June 28, 2007). Based on the NAAQS review process, as revised in 2008 and again in 2009,[11] the EPA held science/policy issue workshops on the primary and secondary PM NAAQS (72 FR 34003, June 20, 2007; 72 FR 34005, June 20, 2007), and prepared and released the planning and assessment documents that comprise the review process ( i.e., Integrated Review Plan, (IRP; U.S. EPA, 2008), Integrated Science Assessment (ISA; U.S. EPA, 2009a), Risk and Exposure Assessment (REA) planning documents for health and welfare (U.S. EPA, 2009b, U.S. EPA, 2009c), a quantitative health risk assessment (U.S. EPA, 2010a) and an urban-focused visibility assessment (U.S. EPA, 2010b), and a Policy Assessment (PA; U.S. EPA, 2011). In June 2012, the EPA announced its proposed decision to revise the NAAQS for PM (77 FR 38890, June 29, 2012).
In December 2012, the EPA announced its final decisions to revise the primary NAAQS for PM to provide increased protection of public health (78 FR 3086, January 15, 2013). With regard to primary standards for PM2.5, the EPA revised the level of the annual PM2.5 standard [12] to 12.0 µg/m[3] and retained the 24-hour PM2.5 standard, with its level of 35 µg/m[3] . For the primary PM10 standard, the EPA retained the 24-hour standard to continue to provide protection against effects associated with short-term exposure to thoracic coarse particles ( i.e., PM10–2.5). With regard to the secondary PM standards, the EPA generally retained the 24-hour Start Printed Page 16209 and annual PM2.5 standards [13] and the 24-hour PM10 standard to address visibility and non-visibility welfare effects.
As with previous reviews, petitioners challenged the EPA's final rule. Petitioners argued that the EPA acted unreasonably in revising the level and form of the annual standard and in amending the monitoring network provisions. On judicial review, the revised standards and monitoring requirements were upheld in all respects. NAM v. EPA, 750 F.3d 921 (D.C. Cir. 2014).
5. Review Initiated in 2014
In December 2014, the EPA announced the initiation of the current periodic review of the air quality criteria for PM and of the PM2.5 and PM10 NAAQS and issued a call for information (79 FR 71764, December 3, 2014). On February 9 to 11, 2015, the EPA's NCEA and OAQPS held a public workshop to inform the planning for the review of the PM NAAQS (announced in 79 FR 71764, December 3, 2014). Workshop participants, including a wide range of external experts as well as the EPA staff representing a variety of areas of expertise ( e.g., epidemiology, human and animal toxicology, risk/exposure analysis, atmospheric science, visibility impairment, climate effects), were asked to highlight significant new and emerging PM research, and to make recommendations to the Agency regarding the design and scope of the review. This workshop provided for a public discussion of the key science and policy-relevant issues around which the EPA structured the review of the PM NAAQS and of the most meaningful new scientific information that would be available in the review to inform understanding of these issues.
The input received at the workshop guided the EPA staff in developing a draft IRP, which was reviewed by the CASAC Particulate Matter Panel and discussed on public teleconferences held in May 2016 (81 FR 13362, March 14, 2016) and August 2016 (81 FR 39043, June 15, 2016). Advice from the CASAC, supplemented by the Particulate Matter Panel, and input from the public were considered in developing the final IRP (U.S. EPA, 2016). The final IRP discusses the approaches to be taken in developing key scientific, technical, and policy documents in the review and the key policy-relevant issues that frame the EPA's consideration of whether the primary and/or secondary NAAQS for PM should be retained or revised.
In May 2018, the then-Administrator issued a memorandum announcing the Agency's intention to conduct the review of the PM NAAQS in such a manner as to ensure that any necessary revisions were finalized by December 2020 (Pruitt, 2018). Following this memo, on October 10, 2018, the then-Administrator additionally announced that the role of reviewing the key assessments developed as part of the ongoing review of the PM NAAQS ( i.e., drafts of the ISA and PA) would be performed by the seven-member chartered CASAC ( i.e., rather than the CASAC Particulate Matter Panel that reviewed the draft IRP).[14]
The EPA released the draft ISA in October 2018 (83 FR 53471, October 23, 2018). The draft ISA was reviewed by the chartered CASAC at a public meeting held in Arlington, VA in December 2018 (83 FR 55529, November 6, 2018) and was discussed on a public teleconference in March 2019 (84 FR 8523, March 8, 2019). The CASAC provided its advice on the draft ISA in a letter to the then-Administrator dated April 11, 2019 (Cox, 2019a). The EPA addressed these comments in the final ISA, which was released in December 2019 (U.S. EPA, 2019a).
The EPA released the draft PA in September 2019 (84 FR 47944, September 11, 2019). The draft PA was reviewed by the chartered CASAC and discussed in October 2019 at a public meeting held in Cary, NC. Public comments were received via a separate public teleconference (84 FR 51555, September 30, 2019). A public meeting to discuss the chartered CASAC letter and response to charge questions on the draft PA was held in Cary, NC, in October 2019 (84 FR 51555, September 30, 2019), and the CASAC provided its advice on the draft PA, including its advice on the current primary and secondary PM standards, in a letter to the then-Administrator dated December 16, 2019 (Cox, 2019b). With regard to the primary standards, the CASAC recommended retaining the current 24-hour PM2.5 and PM10 standards but did not reach consensus on the adequacy of the current annual PM2.5 standard. Some CASAC members expressed support for retaining the current primary annual PM2.5 standard while other members expressed support for revising that standard in order to increase public health protection (Cox, 2019b, p. 1 of letter). These views are described in greater detail in the letter to the then-Administrator (Cox, 2019b) and in the notice of final rulemaking (85 FR 82706–82707, December 18, 2020), as well as below. With regard to the secondary standards, the CASAC recommended retaining the current standards. In response to the CASAC's comments, the 2020 final PA incorporated a number of changes (Cox, 2019b, U.S. EPA, 2020b), as described in detail in section I.C.5 of the 2020 proposal document (85 FR 24100, April 30, 2020).
a. 2020 Proposed and Final Actions
On April 14, 2020, the EPA proposed to retain all of the primary and secondary PM standards, without revision. These proposed decisions were published in the Federal Register on April 30, 2020 (85 FR 24094, April 30, 2020). The EPA's final decision on the PM NAAQS was published in the Federal Register on December 18, 2020 (85 FR 82684, December 18, 2020). In the 2020 rulemaking, the EPA retained the primary and secondary PM2.5 and PM10 standards, without revision. The then-Administrator's rationale for his decisions is described in more detail in section II, III, and V below, and is briefly summarized here.
In reaching his final decision to retain the primary annual and 24-hour PM2.5 standards, the then-Administrator considered the available scientific evidence, quantitative information, CASAC advice, and public comments in his supporting rationale in the 2020 final action (85 FR 82714, December 18, 2020). In so doing, he concluded that the available controlled human exposure studies did not provide support for additional public health protection against exposures to peak PM2.5 concentrations, beyond the protection provided by the combination of the current primary annual and 24-hour PM2.5 standards. He also noted that the available epidemiologic studies did not indicate that associations in those studies are strongly influenced by exposures to peak concentrations in the air quality distribution and thus did not indicate the need for additional protection against short-term exposures to peak PM2.5 concentrations. Accordingly, and taking into account consensus CASAC advice to retain the current primary 24-hour PM2.5 standard, the then-Administrator concluded the primary 24-hour PM2.5 standard should be retained.
With respect to the annual PM2.5 standard, the then-Administrator recognized that important uncertainties and limitations that were present in epidemiologic studies in previous Start Printed Page 16210 reviews remained in the evidence assessed in the 2019 ISA. In considering the epidemiologic evidence, the then-Administrator noted that: (1) The reported mean concentration in the majority of the key U.S. epidemiologic studies using ground-based monitoring data are above the level of the current annual standard; (2) the mean of the reported study means (or medians) ( i.e., 13.5 µg/m3 ) is above the level of the current primary annual PM2.5 standard of 12 µg/m3 ; (3) air quality analyses show the study means to be lower than their corresponding design by 10–20%; and (4) that these analyses must be considered in light of uncertainties inherent in the epidemiologic evidence. The then-Administrator further considered other available information, including the risk assessment, accountability studies, and controlled human exposure studies, and found that, in considering all of the evidence together along with advice from the CASAC, the suite of primary PM2.5 standards were requisite to protect public health with an adequate margin of safety, and should be retained, without revision.
With regard to the primary PM10 standard, the then-Administrator noted that the expanded body of evidence has broadened the range of effects that have been linked with PM10–2.5 exposures. In light of that information, as well as continued uncertainties in the evidence and advice from the CASAC to retain the standard, the then-Administrator judged it appropriate to retain the primary PM10 standard to provide the requisite degree of public health protection against PM10–2.5 exposures, regardless of location, source of origin, or particle composition (85 FR 82725, December 18, 2020).
With regard to the secondary PM standards, the then-Administrator concluded that there was insufficient information available to establish any distinct secondary PM standards to address climate and materials effects of PM. For visibility effects, he found that in the absence of a monitoring network for direct measurement of light extinction, a calculated light extinction indicator that utilizes the IMPROVE algorithms continued to provide a reasonable basis for defining a target level of protection against PM-related visibility impairment. He further found that a visibility index with a 24-hour averaging time was reasonable based on its stability and suitability for representing subdaily periods, and a form based on the 3-year average of annual 90th percentile values was reasonable based on its stability and that it represents the median of the 20 percent worst visibility days which are targeted under the Regional Haze program. With regard to the level of a visibility index, the then-Administrator judged it appropriate to establish a target level of protection of 30 dv, reflecting the upper end of the range of visibility impairment judged to be acceptable by at least 50% of study participants in the available public preference studies, taking into consideration the variability, limitations and uncertainties of the public preference studies. The then-Administrator judged that the secondary 24-hour PM2.5 standard with its level of 35 µg/m3 would provide at least the target level of protection for visual air quality of 30 dv which he judged appropriate. Accordingly, taking into consideration the advice of the CASAC to retain the current secondary PM standards, the then-Administrator found the current secondary standards provide the requisite degree of protection and that they should be retained (85 FR 82742, December 18, 2020).
Following publication of the 2020 final action, several parties filed petitions for review and petitions for reconsideration of the EPA's final decision. The petitions for review were filed in the D.C. Circuit and the Court consolidated the cases.[15] Following EPA's decision to reconsider the 2020 final decision, the Court ordered the consolidated cases to be held in abeyance.
b. Reconsideration of the 2020 PM NAAQS Final Action
Executive Order 13990 directed review of certain agency actions (86 FR 7037, January 25, 2021).[16] An accompanying fact sheet provided a non-exclusive list of agency actions that agency heads should review in accordance with that order, including the 2020 Particulate Matter NAAQS Decision.[17]
On June 10, 2021, the Agency announced its decision to reconsider the 2020 PM NAAQS final action because the available scientific evidence and technical information indicate that the current standards may not be adequate to protect public health and welfare, as required by the Clean Air Act.[18] The Administrator reached this decision in part based on the fact that the EPA noted that the 2020 PA concluded that the scientific evidence and information called into question the adequacy of the primary annual PM2.5 standard and supported revising the level to below the current level of 12.0 µg/m3 while retaining the primary 24-hour PM2.5 standard (U.S. EPA, 2020b). The EPA also noted that the 2020 PA concluded that the available scientific evidence and information supported retaining the primary PM10 standard and secondary PM standards without revision (U.S. EPA, 2020b).
The EPA staff conclusions detailed in the 2020 PA in combination with the CASAC advice that informed the Administrator's decisions regarding the 2020 final action, studies highlighted by public comments on the 2020 proposal, and the numerous studies published since the literature cutoff date of the 2019 ISA all informed the scope of the reconsideration.
In its review of the 2019 draft PA, some members of the CASAC had recommended that greater attention should be given to accountability studies and epidemiologic studies that employ alternative methods for confounder control (also referred to as causal inference or causal modeling studies) in order to “more fully account for effects of confounding, measurement and estimation errors, model uncertainty, and heterogeneity” in epidemiologic studies (Cox, 2019b, p. 8 of consensus responses). In addition, public commenters submitted a number of recent studies published after the literature cutoff date for the 2019 ISA that would have been considered within the scope of the 2019 ISA. While the EPA provisionally considered these studies in responding to public comments,[19] it was determined that, at the time of the 2020 final action, these studies were generally consistent with the evidence assessed in the 2019 ISA (85 FR 82690, December 18, 2020; U.S. EPA, 2020a). As such, and consistent with previous NAAQS reviews, the EPA concluded that the new studies did not materially change any of the broad scientific conclusions regarding the health and welfare effects of PM in ambient air made in the air quality criteria, and therefore, reopening of the air quality criteria was not warranted (85 FR 82691, December 18, 2020). However, at that time, the EPA Start Printed Page 16211 recognized that its “provisional consideration of these studies did not and could not provide the kind of in-depth critical review” (85 FR 82690, December 18, 2020) that studies undergo in the development of an ISA.
In preparing to reconsider the 2020 final decision for the PM NAAQS, the Agency revisited the need to reopen the air quality criteria, given the amount of time that had passed since the literature cutoff date of the 2019 ISA ( i.e., approximately January 2018) and the volume of literature that had become available, including those studies provisionally considered in responding to comments in 2020. In so doing, the EPA preliminarily concluded that at least some of these studies were likely to be relevant to its reconsideration of the air quality criteria and the PM NAAQS and that, in considering public comments on any proposed decisions for the reconsideration, these studies were likely to be raised by public commenters and would potentially warrant a reopening of the air quality criteria. For example, on February 16, 2021, the EPA received two petitions to reconsider the PM NAAQS. One petition objected to the EPA's provisional consideration of studies submitted in public comments on the 2020 proposal and suggested that the provisional consideration was inadequate because the studies could be important in determining whether the existing standards are adequately protective. See, Petition for Reconsideration of National Ambient Air Quality Standards for Particulate Matter, submitted by American Lung Association, et al, dated Feb. 16, 2020. The other petition identified a number of new studies, including one epidemiologic study that was published after the provisional consideration was completed that could further inform the concern expressed by the CASAC that associations reported in epidemiologic studies do not adequately account for “uncontrolled confounding and other potential sources of error and bias.” See Petition for Reconsideration of “Review of the National Ambient Air Quality Standards for Particulate Matter,” submitted by the State of California, dated Feb. 16, 2020. This was also an uncertainty noted by the then-Administrator in the 2020 decision, who also recognized “that methodological study designs to address confounding, such as causal inference methods, are an emerging field of study.” Thus, the Agency concluded it was appropriate to reconsider not only the standards but also the air quality criteria, in light of public comments during the 2020 PM NAAQS proposal and recent studies published since the cutoff date of the 2019 ISA, as reflected in petitions. In deciding to reopen the air quality criteria, the Agency concluded it was reasonable to focus on studies that were most likely to inform decisions on the appropriate standard, but not to reassess areas which, based on the assessment of available science published since the cutoff date of the 2019 ISA and through 2021, were judged unlikely to have new information that would be useful for the Administrator's decision making. The Agency accordingly announced that, in support of the reconsideration, it would develop a supplement to the 2019 ISA and a revised PA.
The EPA also explained that the draft ISA Supplement and draft PA would be reviewed at a public meeting by the CASAC, and the public would have opportunities to comment on these documents during the CASAC review process, as well as to provide input during the rulemaking through the public comment process and public hearings on the proposed rulemaking.
On March 31, 2021, the Administrator announced his decision to reestablish the membership of the CASAC to “ensure the agency received the best possible scientific insight to support our work to protect human health and the environment.” [20] Consistent with this memorandum, a call for nominations of candidates to the EPA's chartered CASAC was published in the Federal Register (86 FR 17146, April 1, 2021). On June 17, 2021, the Administrator announced his selection of the seven members to serve on the chartered CASAC.[21 22] Additionally, a call for nominations of candidates to a PM-specific panel was published in the Federal Register (86 FR 33703, June 25, 2021). The members of the PM CASAC panel were announced on August 30, 2021.[23]
The draft ISA Supplement was released in September 2021 (U.S. EPA, 2021a; 86 FR 54186, September 30, 2021), and included a discussion of the rationale and scope of the Supplement. As explained therein, the ISA Supplement focuses on a thorough evaluation of some studies that became available after the literature cutoff date of the 2019 ISA that could either further inform the adequacy of the current PM NAAQS or address key scientific topics that have evolved since the literature cutoff date for the 2019 ISA. In selecting the health effects to evaluate within the ISA Supplement, the EPA focused on health effects for which the evidence supported a “causal relationship” because those were the health effects that were most useful in informing conclusions in the 2020 PA (U.S. EPA, 2022a, section 1.2.1).[24] Consistent with the rationale for the focus on certain health effects, in selecting the non-ecological welfare effects to evaluate within the ISA Supplement, the EPA focused on the non-ecological welfare effects for which the evidence supported a “causal relationship” and for which quantitative analyses could be supported by the evidence because those were the welfare effects that were most useful in informing conclusions in the 2020 PA.[25] Specifically, for non-ecological welfare effects, the focus within the ISA Supplement is on visibility effects. The ISA Supplement also considers recent health effects evidence that addresses key scientific topics where the literature has evolved since the 2020 review was completed, Start Printed Page 16212 specifically since the literature cutoff date for the 2019 ISA.[26]
Building on the rationale presented in section 1.2.1, the ISA Supplement considers peer-reviewed studies published from approximately January 2018 through March 2021 that meet the following criteria:
• Health Effects
○ U.S. and Canadian epidemiologic studies for health effect categories where the 2019 ISA concluded a “ causal relationship ” ( i.e., short- and long-term PM2.5 exposure and cardiovascular effects and mortality).
U.S. and Canadian epidemiologic studies that employed alternative methods for confounder control or conducted accountability analyses ( i.e., examined the effect of a policy on reducing PM2.5 concentrations).
• Welfare Effects
○ U.S. and Canadian studies that provide new information on public preferences for visibility impairment and/or developed methodologies or conducted quantitative analyses of light extinction.
• Key Scientific Topics
○ Experimental studies ( i.e., controlled human exposure and animal toxicological) conducted at near-ambient PM2.5 concentrations experienced in the U.S.
○ U.S.- and Canadian-based epidemiologic studies that examined the relationship between PM2.5 exposures and severe acute respiratory syndrome coronavirus 2 (SARS–CoV–2) infection and coronavirus disease 2019 (COVID–19) death.
○ At-Risk Populations.
U.S.- and Canadian-based epidemiologic or exposure studies examining potential disparities in either PM2.5 exposures or the risk of health effects by race/ethnicity or socioeconomic status (SES).
Given the narrow scope of the ISA Supplement, it is important to recognize that the evaluation does not encompass the full multidisciplinary evaluation presented within the 2019 ISA that would result in weight-of-evidence conclusions on causality ( i.e., causality determinations). The ISA Supplement critically evaluates and provides key study-specific information for those recent studies deemed to be of greatest significance for informing preliminary conclusions on the PM NAAQS in the context of the body of evidence and scientific conclusions presented in the 2019 ISA.
In developing a revised PA to support the reconsideration, the EPA considered the available scientific evidence, including the evidence presented in the 2019 ISA and ISA Supplement. The 2022 PA considered the quantitative and technical information presented in the 2020 PA, in addition to new and updated analyses conducted since the 2020 final decision. For those health and welfare effects for which the ISA Supplement evaluated recently available studies ( i.e., PM2.5 -related health effects and visibility effects), new updated quantitative analyses were conducted as a part of the development of the 2022 PA. The newly available scientific and technical information presented in the 2022 PA were considered in reaching conclusions regarding the adequacy of the current standards and any potential alternative standards. For those health and welfare effects for which newly available scientific and technical information were not evaluated ( i.e., PM10–2.5 -related health effects and non-visibility welfare effects), the conclusions presented in the 2022 PA rely heavily on the information that supported the conclusions in the 2020 PA.
The CASAC PM panel met at a virtual public meeting in November 2021 to review the draft ISA Supplement (86 FR 52673, September 22, 2021). A virtual public meeting was then held in February 2022, and during this meeting the chartered CASAC considered the CASAC PM panel's draft letter to the Administrator on the draft ISA Supplement (87 FR 958, January 7, 2022).
The chartered CASAC provided its advice on the draft ISA Supplement in a letter to the EPA Administrator dated March 18, 2022 (Sheppard, 2022b). In its review of the draft ISA Supplement, the CASAC noted that they found “the Draft ISA Supplement to be a well-written, comprehensive evaluation of the new scientific information published since the 2019 PM ISA” (Sheppard, 2022b, p. 2 of letter). Furthermore, the CASAC stated that “the final Integrated Science Assessment (ISA) Supplement . . . deserve[s] the Administrator's full consideration and [is] adequate for rulemaking” (Sheppard, 2022b, p. 2 of letter). The CASAC generally endorsed EPA's decisions regarding the limited scope of the draft ISA Supplement, stating that “this limitation [on scope] is appropriate for the targeted purpose of the Draft ISA Supplement” although the CASAC noted it would not be appropriate for ISAs generally, and recommended that the EPA provide additional acknowledgment and explanation for the limited scope (Sheppard, 2022b, p. 2 of letter; see also pp. 2–3 of consensus responses). The EPA specifically noted in the final ISA Supplement, which was released in May 2022 (U.S. EPA, 2022a; hereafter referred to as the ISA Supplement throughout this document) that the “targeted approach to developing the Supplement to the 2019 PM ISA for the purpose of reconsidering the 2020 PM NAAQS decision does not reflect a change to EPA's approach for developing ISAs for NAAQS reviews.” Thus, the evidence presented within the 2019 ISA, along with the targeted identification and evaluation of new scientific information in the ISA Supplement, provides the scientific basis for the reconsideration of the 2020 PM NAAQS final decision.
The draft PA was released in October 2021 (86 FR 56263, October 8, 2021). The CASAC PM panel met at a virtual public meeting in December 2021 to review the draft PA (86 FR 52673, September 22, 2021). A virtual public meeting was then held in February 2022 and March 2022, and during this meeting the chartered CASAC considered the CASAC PM panel's draft letter to the Administrator on the draft PA (87 FR 958, January 7, 2022). The chartered CASAC provided its advice on the draft PA in a letter to the EPA Administrator dated March 18, 2022 (Sheppard, 2022a). The EPA took steps to address these comments in revising and finalizing the PA. The 2022 PA considers the scientific evidence presented in the 2019 ISA and ISA Supplement and considers the quantitative and technical information presented in the 2020 PA, along with updated and newly available analyses since the completion of the 2020 review. For those health and welfare effects for which the ISA Supplement evaluated recently available evidence and for which updated quantitative analyses were supported ( i.e., PM2.5 -related health effects and visibility effects), the 2022 PA includes consideration of this newly available scientific and technical information in reaching preliminary conclusions. For those health and welfare effects for which newly available scientific and technical Start Printed Page 16213 information were not evaluated ( i.e., PM10–2.5 -related health effects and non-visibility effects), the conclusions presented in the 2022 PA rely heavily on the information that supported the conclusions in the 2020 PA. The final PA was released in May 2022 (U.S. EPA, 2022b; hereafter referred to as the 2022 PA throughout this document).
Drawing from his consideration of the scientific evidence assessed in the 2019 ISA and ISA Supplement and the analyses in the 2022 PA, including the uncertainties in the evidence and analyses, and from his consideration of advice from the CASAC, on January 5, 2023, the Administrator proposed to revise the level of the primary annual PM2.5 standard and to retain the primary 24-hour PM2.5 standard, the primary 24-hour PM10 standard, and the secondary PM standards. These proposed decisions were published in the Federal Register on January 27, 2023 (88 FR 5558, January 27, 2023). The EPA held a multi-day virtual public hearing on February 21–23, 2023 (88 FR 6215, January 31, 2023). In total, the EPA received nearly 700,000 comments on the proposal from members of the public by the close of the public comment period on March 28, 2023. Major issues raised in the public comments are discussed throughout the preamble of this final action. A more detailed summary of all significant comments, along with the EPA's responses (henceforth “Response to Comments” document), can be found in the docket for this rulemaking (Docket No. EPA–HQ–OAR–2015–0072).
As in prior reviews, the EPA is basing its decision in this reconsideration on studies and related information in the air quality criteria, which have undergone CASAC and public review. These studies assessed in the 2019 ISA [27] and ISA Supplement [28] and the 2022 PA, and the integration of the scientific evidence presented in them, have undergone extensive critical review by the EPA, the CASAC, and the public. Decisions on the NAAQS should be based on studies that have been rigorously assessed in an integrative manner not only by the EPA but also by the statutorily mandated independent scientific advisory committee, as well as the public review that accompanies this process. It is for this reason that the EPA preliminarily concluded that the scientific evidence available since the completion of the 2019 ISA, including those raised in public comments on the proposal in 2020, warranted a partial reopening of the air quality criteria and prepared an ISA Supplement to enable the EPA, the CASAC, and the public to consider them further. Some commenters have referred to and discussed additional individual scientific studies on the health effects of PM that were not included in the 2019 ISA or ISA Supplement (“new studies”) and that have not gone through this comprehensive review process. In considering and responding to comments for which such “new” studies were cited in support, the EPA has provisionally considered the cited studies in the context of the findings of the 2019 ISA and ISA Supplement. The EPA's provisional consideration of these studies did not and could not provide the kind of in-depth critical review described above, but rather was focused on determining whether they warranted further reopening the review of the air quality criteria to enable the EPA, the CASAC, and the public to consider them further.
This approach, and the decision to rely on the studies and related information in the air quality criteria, which have undergone CASAC and public review, is consistent with the EPA's practice in prior NAAQS reviews and its interpretation of the requirements of the CAA. Since the 1970 amendments, the EPA has taken the view that NAAQS decisions are to be based on scientific studies and related information that have been assessed as a part of the pertinent air quality criteria, and the EPA has consistently followed this approach. This longstanding interpretation was strengthened by new legislative requirements enacted in 1977, which added section 109(d)(2) of the Act concerning CASAC review of air quality criteria. See 71 FR 6114, 61148 (October 17, 2006, final decision on review of NAAQS for particulate matter) for a detailed discussion of this issue and the EPA's past practice.
As discussed in the EPA's 1993 decision not to review the O3 NAAQS, “new” studies may sometimes be of such significance that it is appropriate to delay a decision in a NAAQS review and to supplement the pertinent air quality criteria so the studies can be taken into account (58 FR 13013–13014, March 9, 1993). In the present case, the EPA decided to partially reopen the air quality criteria and prepared an ISA Supplement as a part of the reconsideration to facilitate evaluation of these studies by the EPA, the CASAC, and the public. The narrow scope of the ISA Supplement is supported by EPA's provisional consideration of “new” studies submitted in response to public comments on the 2020 proposal which concluded that, taken in context, the “new” information and findings do not materially change any of the broad scientific conclusions regarding the health and welfare effects of PM in ambient air made in the air quality criteria. Therefore, a full reopening of the air quality criteria was not warranted to assess the health and welfare effects of PM for purposes of the review.
Accordingly, the EPA is basing the final decisions in this reconsideration on the studies and related information included in the PM air quality criteria (including the 2019 PM ISA and ISA Supplement) that have undergone rigorous review by the EPA, the CASAC, and the public. The EPA will consider these “new” studies for inclusion in the air quality criteria for the next PM NAAQS review, which the EPA expects to begin soon after the conclusion of this reconsideration and which will provide the opportunity to fully assess these studies through a more rigorous review process involving the EPA, the CASAC, and the public.
D. Air Quality Information
This section provides a summary of basic information related to PM ambient air quality. It summarizes information on the distribution of particle size in ambient air (section I.D.1), sources and emissions contributing to PM in the ambient air (section I.D.2), monitoring ambient PM in the U.S. (section I.D.3), ambient PM concentrations and trends in the U.S. (I.D.4), characterizing ambient PM2.5 concentrations for exposure (section I.D.5), and background PM (section I.D.6). Additional detail on PM air quality can be found in Chapter 2 of the 2022 PA (U.S. EPA, 2022b).
1. Distribution of Particle Size in Ambient Air
In ambient air, PM is a mixture of substances suspended as small liquid and/or solid particles (U.S. EPA, 2019a, section 2.2) and distinct health and welfare effects have been linked with exposures to particles of different sizes. Particles in the atmosphere range in size from less than 0.01 to more than 10 μm Start Printed Page 16214 in diameter (U.S. EPA, 2019a, section 2.2). The EPA defines PM2.5, also referred to as fine particles, as particles with aerodynamic diameters generally less than or equal to 2.5 μm. The size range for PM10–2.5, also called coarse or thoracic coarse particles, includes those particles with aerodynamic diameters generally greater than 2.5 μm and less than or equal to 10 μm. PM10, which is comprised of both fine and coarse fractions, includes those particles with aerodynamic diameters generally less than or equal to 10 μm. In addition, ultrafine particles (UFP) are often defined as particles with a diameter of less than 0.1 μm based on physical size, thermal diffusivity or electrical mobility (U.S. EPA, 2019a, section 2.2). Atmospheric lifetimes are generally longest for PM2.5, which often remains in the atmosphere for days to weeks (U.S. EPA, 2019a, Table 2–1) before being removed by wet or dry deposition, while atmospheric lifetimes for UFP and PM10–2.5 are shorter and are generally removed from the atmosphere within hours, through wet or dry deposition (U.S. EPA, 2019a, Table 2–1; U.S. EPA, 2022b, section 2.1).
2. Sources and Emissions Contributing to PM in the Ambient Air
PM is composed of both primary (directly emitted particles) and secondary particles. Primary PM is derived from direct particle emissions from specific PM sources while secondary PM originates from gas-phase precursor chemical compounds present in the atmosphere that have participated in new particle formation or condensed onto existing particles (U.S. EPA, 2019a, section 2.3). As discussed further in the 2019 ISA (U.S. EPA, 2019a, section 2.3.2.1), secondary PM is formed in the atmosphere by photochemical oxidation reactions of both inorganic and organic gas-phase precursors. Precursor gases include sulfur dioxide (SO2), nitrogen oxides (NOX), and volatile organic compounds (VOC) (U.S. EPA, 2019a, section 2.3.2.1). Ammonia also plays an important role in the formation of nitrate PM by neutralizing sulfuric acid and nitric acid. Sources and emissions of PM are discussed in more detail the 2022 PA (U.S. EPA, 2022b, section 2.1.1). Briefly, anthropogenic sources of PM include both stationary ( e.g., fuel combustion for electricity production and other purposes, industrial processes, agricultural activities) and mobile ( e.g., diesel- and gasoline-powered highway vehicles and other engine-driven sources) sources. Natural sources of PM include dust from the wind erosion of natural surfaces, sea salt, wildfires, primary biological aerosol particles (PBAP) such as bacteria and pollen, oxidation of biogenic hydrocarbons, such as isoprene and terpenes to produce secondary organic aerosol (SOA), and geogenic sources, such as sulfate formed from volcanic production of SO2 . Wildland fire, which encompass both wildfire and prescribed fire, accounts for 44% of emissions of primary PM2.5 emissions (U.S. EPA, 2021b). Emissions from wildfire comprises 29% of primary PM2.5 emissions.
In recent years, the frequency and magnitude of wildfires have increased (U.S. EPA, 2019a). The magnitude of the public health impact of wildfires is substantial both because of the increase in PM2.5 concentrations as well as the duration of the wildfire smoke season, which is considered to range from May to November. Wildfire can make a large contribution to air pollution (including PM2.5), and wildfire events can threaten public safety and life. The impacts of wildfire events can be mitigated through management of wildland vegetation, including through prescribed fire. Prescribed fire (and some wildfires) can mimic the natural processes necessary to maintain fire-dependent ecosystems, minimizing catastrophic wildfires and the risks they pose to safety, property and air quality (see, e.g.,81 FR 58010, 58038, August 24, 2016). The EPA views the strategic use of prescribed fire as an important tool for reducing wildfire risk and the severity of wildfires and wildfire smoke (88 FR, 54118, 54126, August 9, 2023).[29] As noted in the PM NAAQS proposal, agencies have efforts in place to reduce the frequency and severity of human-caused wildfires (88 FR 5570, January 27, 2023).
Wildfire events produce high PM emissions that may impact the PM concentrations in ambient air to the extent that the concentrations result in an exceedance or violation which may affect the design value in a given area. The EPA's Exceptional Events Rule (81 FR 68216, October 3, 2016) describes the process by which air agencies may request to exclude `event-influenced' data caused by exceptional events, which can include wildfires and prescribed fires on wildland. The EPA has issued guidance specifically addressing exceptional events demonstrations for both wildfires and prescribed fires on wildland. These documents are available on EPA's Exceptional Events Program website.[30] The EPA will develop fire-related exceptional events implementation tools, including updates as needed to existing guidance to facilitate more efficient processing of PM2.5 -related exceptional events demonstrations for both the 24-hour and annual standards.
3. Monitoring of Ambient PM
To promote uniform application of the air quality standards set forth under the CAA and to achieve the degree of public health and welfare protection intended for the NAAQS, the EPA establishes PM Federal Reference Methods (FRMs) for both PM10 and PM2.5 in appendices J and L to 40 CFR part 50, both of which were amended following the 2006 and 2012 PM NAAQS reviews. The current PM monitoring network relies on FRMs and automated continuous Federal Equivalent Methods (FEMs) approved pursuant to 40 CFR part 53, in part to support changes necessary for implementation of the revised PM standards. Additionally, 40 CFR part 58, appendices A through E, detail the requirements to measure ambient air quality and report ambient air quality data and related information. More information on PM ambient monitoring networks is available in section 2.2 of the 2022 PA (U.S. EPA, 2022b).
The PM2.5 monitoring program is one of the major ambient air monitoring programs with a robust, nationally consistent network of ambient air monitoring sites providing mass and/or chemical speciation measurements. 40 CFR part 58, appendix D, section 4.7 provides the applicable PM2.5 network design criteria. For most urban locations, PM2.5 monitors are sited at the neighborhood scale,[31] where PM2.5 concentrations are reasonably homogeneous throughout an entire urban sub-region. In each CBSA with a monitoring requirement, at least one PM2.5 monitoring station representing Start Printed Page 16215 area-wide air quality is sited in an area of expected maximum concentration.[32] By ensuring the area of expected maximum concentration in a CBSA has a site compared to both the annual and 24-hour NAAQS, all other similar locations are thus protected. Sites that represent relatively unique microscale, localized hot-spot, or unique middle scale impact sites are only eligible for comparison to the 24-hour PM2.5 NAAQS.
Under 40 CFR part 50, appendix L, and 40 CFR part 53, and 40 CFR part 58 appendix D there are three main methods components of the PM2.5 monitoring program: filter-based FRMs measuring PM2.5 mass, FEMs measuring PM2.5 mass, and other samplers used to collect the aerosol used in subsequent laboratory analysis for measuring PM2.5 chemical speciation. The FRMs are primarily used for comparison to the NAAQS, but also serve other important purposes, such as developing trends and evaluating the performance of FEMs. PM2.5 FEMs are typically continuous methods used to support forecasting and reporting of the Air Quality Index (AQI) but are also used for comparison to the NAAQS. Samplers that are part of the Chemical Speciation Network (CSN) and Interagency Monitoring of Protected Visual Environments (IMPROVE) network are used to provide chemical composition of the aerosol and serve a variety of objectives. More detail on of each of these components of the PM2.5 monitoring program and of recent changes to PM2.5 monitoring requirements are described in detail in the 2022 PA (U.S. EPA, 2022b, section 2.2.3).
4. Ambient Concentrations and Trends
This section summarizes available information on recent ambient PM concentrations in the U.S. and on trends in PM air quality. Sections I.D.4.a and I.D.4.b summarize information on PM2.5 mass and components, respectively. Section I.D.4.c summarizes information on PM10 . Sections I.D.4.d and I.D.4.e summarize the more limited information on PM10–2.5 and UFP, respectively. Additional detail on PM air quality and trends can be found in the 2022 PA (U.S. EPA, 2022b, section 2.3).
a. PM2.5 mass
At monitoring sites in the U.S., annual PM2.5 concentrations from 2017 to 2019 averaged 8.0 μg/m3 (with the 10th and 90th percentiles at 5.9 and 10.0 μg/m3 , respectively) and the 98th percentiles of 24-hour concentrations averaged 21.3 μg/m3 (with the 10th and 90th percentiles at 14.0 and 29.7 μg/m3 , respectively) (U.S. EPA, 2022b, section 2.3.2.1). The highest ambient PM2.5 concentrations occur in the western U.S., particularly in California and the Pacific Northwest (U.S. EPA, 2022b, Figure 2–15). Much of the eastern U.S. has lower ambient concentrations, with annual average concentrations generally at or below 12.0 μg/m3 and 98th percentiles of 24-hour concentrations generally at or below 30 μg/m3 (U.S. EPA, 2022b, section 2.3.2.1).
Recent ambient PM2.5 concentrations reflect the substantial reductions that have occurred across much of the U.S. (U.S. EPA, 2022b, section 2.3.2.1). From 2000 to 2019, national annual average PM2.5 concentrations declined from 13.5 μg/m[3] to 7.6 μg/m[3] , a 43% decrease (U.S. EPA, 2022b, section 2.3.2.1).[33] These declines have occurred at urban and rural monitoring sites, although urban PM2.5 concentrations remain consistently higher than those in rural areas (Chan et al., 2018) due to the impact of local sources in urban areas. Analyses at individual monitoring sites indicate that declines in ambient PM2.5 concentrations have been most consistent across the eastern U.S. and in parts of coastal California, where both annual average and 98th percentiles of 24-hour concentrations declined significantly (U.S. EPA, 2022b, section 2.3.2.1). In contrast, trends in ambient PM2.5 concentrations have been less consistent over much of the western U.S., with no significant changes since 2000 observed at some sites in the Pacific Northwest, the northern Rockies and plains, and the Southwest, particularly for 98th percentiles of 24-hour concentrations (U.S. EPA, 2022b, section 2.3.2.1). As noted below, some sites in the northwestern U.S. and California, where wildfire have been relatively common in recent years, have experienced high concentrations over shorter periods ( i.e., 2-hour averages).
The recent deployment of PM2.5 monitors near major roads in large urban areas provides information on PM2.5 concentrations near an important emissions source. For 2016–2018, Gantt et al. (2021) reported that 52% and 24% of the time near-road sites reported the highest annual and 24-hour PM2.5 design value [34] in the CBSA, respectively. Of the CBSAs with the highest annual design values at near-road sites reported by Gantt et al. (2021), those design values were, on average, 0.8 µg/m[3] higher than at the highest measuring non-near-road sites (range is 0.1 to 2.1 µg/m[3] higher at near-road sites). Although most near-road monitoring sites do not have sufficient data to evaluate long-term trends in near-road PM2.5 concentrations, analyses of the data at one near-road-like site in Elizabeth, NJ,[35] show that the annual average near-road increment has generally decreased between 1999 and 2017 from about 2.0 μg/m3 to about 1.3 μg/m3 (U.S. EPA, 2022b, section 2.3.2.1).
Ambient PM2.5 concentrations can exhibit a diurnal cycle that varies due to impacts from intermittent emission sources, meteorology, and atmospheric chemistry. The PM2.5 monitoring network in the U.S. has an increasing number of continuous FEM monitors reporting hourly PM2.5 mass concentrations that reflect this diurnal variation. The 2019 ISA describes a two-peaked diurnal pattern in urban areas, with morning peaks attributed to rush-hour traffic and afternoon peaks attributed to a combination of rush hour traffic, decreasing atmospheric dilution, and nucleation (U.S. EPA, 2019a, section 2.5.2.3, Figure 2–32). Because a focus on annual average and 24-hour average PM2.5 concentrations could mask subdaily patterns, and because some health studies examine PM exposure durations shorter than 24-hours, it is useful to understand the broader distribution of subdaily PM2.5 concentrations across the U.S. The 2022 PA presents information on the frequency distribution of 2-hour average PM2.5 mass concentrations from all FEM PM2.5 monitors in the U.S. for 2017–2019. At sites meeting the current primary PM2.5 standards, these 2-hour concentrations generally remain below 10 μg/m3 , and rarely exceed 30 μg/m3 . Two-hour concentrations are higher at sites violating the current standards, generally remaining below 16 μg/m3 and rarely exceeding 80 μg/m3 (U.S. EPA, 2022b, section 2.3.2.2.3). The extreme upper end of the distribution of 2-hour PM2.5 concentrations is shifted higher during the warmer months, generally corresponding to the period of peak wildfire frequency (April to September) in the U.S. At sites meeting the current primary standards, the highest 2-hour concentrations measured rarely occur outside of the period of peak wildfire frequency. Most of the sites measuring Start Printed Page 16216 these very high concentrations are in the northwestern U.S. and California, where wildfires have been relatively common in recent years (see U.S. EPA, 2022b, Appendix A, Figure A–1). When the period of peak wildfire frequency is excluded from the analysis, the extreme upper end of the distribution is reduced (U.S. EPA, 2022b, section 2.3.2.2.3).
b. PM2.5 Components
Based on recent air quality data, the major chemical components of PM2.5 have distinct spatial distributions. Sulfate concentrations tend to be highest in the eastern U.S., while in the Ohio Valley, Salt Lake Valley, and California nitrate concentrations are highest, and relatively high concentrations of organic carbon are widespread across most of the continental U.S. (U.S. EPA, 2022b, section 2.3.2.3). Elemental carbon, crustal material, and sea salt are found to have the highest concentrations in the northeast U.S., southwest U.S., and coastal areas, respectively.
An examination of PM2.5 composition trends can provide insight into the factors contributing to overall reductions in ambient PM2.5 concentrations. The biggest change in PM2.5 composition that has occurred in recent years is the reduction in sulfate concentrations due to reductions in SO2 emissions. Between 2000 and 2015, the nationwide annual average sulfate concentration decreased by 17% at urban sites and 20% at rural sites. This change in sulfate concentrations is most evident in the eastern U.S. and has resulted in organic matter or nitrate now being the greatest contributor to PM2.5 mass in many locations (U.S. EPA, 2019a, Figure 2–19). The overall reduction in sulfate concentrations has contributed substantially to the decrease in national average PM2.5 concentrations as well as the decline in the fraction of PM10 mass accounted for by PM2.5 (U.S. EPA, 2019a, section 2.5.1.1.6; U.S. EPA, 2022b, section 2.3.1).
c. PM10
At long-term monitoring sites in the U.S., the 2017–2019 average of 2nd highest 24-hour PM10 concentration was 68 μg/m[3] (with 10th and 90th percentiles at 28 and 124 μg/m[3] , respectively) (U.S. EPA, 2022b, section 2.3.2.4).[36] The highest PM10 concentrations tend to occur in the western U.S. Seasonal analyses indicate that ambient PM10 concentrations are generally higher in the summer months than at other times of year, though the most extreme high concentration events are more likely in the spring (U.S. EPA, 2019a, Table 2–5). This is due to fact that the major PM10 emission sources, dust and agriculture, are more active during the warmer and drier periods of the year.
Recent ambient PM10 concentrations reflect reductions that have occurred across much of the U.S. (U.S. EPA, 2022b, section 2.3.2.4). From 2000 to 2019, 2nd highest 24-hour PM10 concentrations have declined by about 46% (U.S. EPA, 2022b, section 2.3.2.4).[37] Analyses at individual monitoring sites indicate that annual average PM10 concentrations have generally declined at most sites across the U.S., with much of the decrease in the eastern U.S. associated with reductions in PM2.5 concentrations (U.S. EPA, 2022b, section 2.3.2.4). Annual 2nd highest 24-hour PM10 concentrations have generally declined in the eastern U.S., while concentrations in much of the midwest and western U.S. have remained unchanged or increased since 2000 (U.S. EPA, 2022b, section 2.3.2.4).
Compared to previous reviews, data available from the NCore monitoring network in the current reconsideration allows a more comprehensive analysis of the relative contributions of PM2.5 and PM10–2.5 to PM10 mass. PM2.5 generally contributes more to annual average PM10 mass in the eastern U.S. than the western U.S. (U.S. EPA, 2022b, Figure 2–23). At most sites in the eastern U.S., the majority of PM10 mass is comprised of PM2.5 . As ambient PM2.5 concentrations have declined in the eastern U.S. (U.S. EPA, 2022b, section 2.3.2.2), the ratios of PM2.5 to PM10 have also declined. For sites with days having concurrently very high PM2.5 and PM10 concentrations (U.S. EPA, 2022b, Figure 2–24), the PM2.5 /PM10 ratios are typically higher than the annual average ratios. This is particularly true in the northwestern U.S. where the high PM10 concentrations can occur during wildfires with high PM2.5 (U.S. EPA, 2022b, section 2.3.2.4).
d. PM10–2.5
Since the 2012 review, the availability of PM10–2.5 ambient concentration data has greatly increased because of additions to the PM10–2.5 monitoring capabilities to the national monitoring network. As illustrated in the 2022 PA (U.S. EPA, 2022b, section 2.3.2.5), annual average and 98th percentile PM10–2.5 concentrations exhibit less distinct differences between the eastern and western U.S. than for either PM2.5 or PM10.
Due to the short atmospheric lifetime of PM10–2.5 relative to PM2.5, many of the high concentration sites are isolated and likely near emission sources associated with wind-blown and fugitive dust. The spatial distributions of annual average and 98th percentile concentrations of PM10–2.5 are more similar than that of PM2.5, suggesting that the same dust-related emission sources are affecting both long-term and episodic concentrations (U.S. EPA, 2022b, Figure 2–25). The highest concentrations of PM10–2.5 are in the southwest U.S. where widespread dry and windy conditions contribute to wind-blown dust emissions. Additionally, compared to PM2.5 and PM10, changes in PM10–2.5 concentrations have been small in magnitude and inconsistent in direction (U.S. EPA, 2022b, Figure 2–25). The majority of PM10–2.5 sites in the U.S. do not have a concentration trend from 2000–2019, reflecting the relatively consistent level of dust emissions across the U.S. during the same time period (U.S. EPA, 2022b, section 2.3.2.5).[38]
e. UFP
Compared to PM2.5 mass, there is relatively little data on U.S. particle number concentrations, which are dominated by UFP. In the published literature, annual average particle number concentrations reaching about 20,000 to 30,000 cm3 have been reported in U.S. cities (U.S. EPA, 2019a). In addition, based on UFP measurements in two urban areas (New York City, Buffalo) and at a background site (Steuben County) in New York, there is a pronounced difference in particle number concentration between different types of locations (U.S. EPA, 2022b, Figure 2–26; U.S. EPA, 2019a, Figure 2–18). Urban particle number counts were several times higher than at the background site, and the highest particle number counts in an urban area with multiple sites (Buffalo) were observed at a near-road location (U.S. EPA, 2022b, section 2.3.2.6).
Long-term trends in UFP are not routinely available at U.S. monitoring Start Printed Page 16217 sites. At one background site in Illinois with long-term data available, the annual average particle number concentration declined between 2000 and 2019, closely matching the reductions in annual PM2.5 mass over that same period (U.S. EPA, 2022b, section 2.3.2.6). In addition, a small number of published studies have examined UFP trends over time. While limited, these studies also suggest that UFP number concentrations have declined over time along with decreases in PM2.5 (U.S. EPA, 2022b, section 2.3.2.6). However, the relationship between changes in ambient PM2.5 and UFPs cannot be comprehensively characterized due to the high variability and limited monitoring of UFPs (U.S. EPA, 2022b, section 2.3.2.6).
5. Characterizing Ambient PM2.5 Concentrations for Exposure
Epidemiologic studies use various methods to characterize exposure to ambient PM2.5 . The methods used to estimate PM2.5 concentrations can vary from traditional methods using monitoring data from ground-based monitors to newer methods using more complex hybrid modeling approaches. Studies using hybrid modeling approaches aim to broaden the spatial coverage, as well as estimate more spatially-resolved ambient PM2.5 concentrations, by expanding beyond just those areas with monitors and providing estimates in areas that do not have ground-based monitors ( i.e., areas that are generally less densely populated and tend to have lower PM2.5 concentrations) and at finer spatial resolutions ( e.g., 1 km x 1 km grid cells). Ground-based PM2.5 monitors are generally sited in areas of expected maximum concentration. As such, the hybrid modeling approaches tend to broaden the areas captured in the exposure assessment, and in doing so, the studies that utilize these methods tend to report lower mean PM2.5 concentrations than monitor-based approaches. Further, other aspects of the approaches applied in the various epidemiologic studies to estimate PM2.5 exposure and/or to calculate the related study-reported mean concentration ( i.e., population weighting, trim mean approaches) can affect those data values. More detail related to hybrid modeling methods, performance of the methods, and how the reported mean concentrations compare across approaches is provided in section 2.3.3.2 of the 2022 PA (U.S. EPA, 2022b). The subsections below discuss the characterization of PM2.5 concentrations based on monitoring data (I.D.5.a) and using hybrid modeling approaches (I.D.5.b).
a. Predicted Ambient PM2.5 and Exposure Based on Monitored Data
Ambient concentrations of PM2.5 are often characterized using measurements from national monitoring networks due to the accuracy and precision of the measurements and the public availability of data. For applications requiring PM2.5 characterizations across large areas or provide complete coverage from the site measurements, data interpolation and averaging techniques (such as Average Nearest Neighbor tools, and area-wide or population-weighted averaging of monitors) are sometimes used (U.S. EPA, 2019a, chapter 3).
For an area to meet the NAAQS, all valid design values [39] in that area, including the highest annual and 24-hour design values, must be at or below the levels of the standards. Because the monitoring network siting requirements are specified to capture the high PM2.5 concentrations (U.S. EPA, 2022b, section 2.2.3), areas meeting an annual PM2.5 standard with a particular level would be expected to have long-term average monitored PM2.5 concentrations ( i.e., averaged across space and over time in the area) somewhat below that standard level. This means that the PM2.5 design value in an area is associated with a distribution of PM2.5 concentrations in that area, and, based on monitoring siting requirements, should represent the highest concentration location applicable to be monitored under the PM2.5 NAAQS. Analyses in the 2022 PA indicate that, based on recent air quality in U.S. CBSAs, maximum annual PM2.5 design values are often 10% to 20% higher than annual average concentrations ( i.e., averaged across multiple monitors in the same CBSA) (U.S. EPA, 2022b, section 2.3.3.1, Figures 2–28 and 2–29). This difference between the maximum annual design value and the average concentration in an area can vary, depending on factors such as the number of monitors, monitor siting characteristics, and the distribution of ambient PM2.5 concentrations. Given that higher PM2.5 concentrations have been reported at some near-road monitoring sites relative to the surrounding area (U.S. EPA, 2022b, section 2.3.2.2.2), recent requirements for PM2.5 monitoring at near-road locations in large urban areas (U.S. EPA, 2022b, section 2.2.3.3) may increase the ratios of maximum design values to average annual design values in some areas. Such ratios may also depend on how the averages are calculated ( i.e., averaged across monitors versus across modeled grid cells, as described below in section I.5.b). Compared to annual design values, the analysis in the 2022 PA indicates a more variable relationship between maximum 24-hour PM2.5 design values and annual average concentrations (U.S. EPA, 2022b, section 2.3.3.1, Figure 2–29).
b. Comparison of PM2.5 Hybrid Modeling Approaches in Estimating Exposure and Relative to Design Values
Two types of hybrid approaches that have been utilized in several key PM2.5 epidemiologic studies in the 2019 ISA and ISA Supplement include neural network approaches and a satellite-based method with regression of residual PM2.5 with land-use and other variables to improve estimates of PM2.5 concentration in the U.S. As such, the 2022 PA further compares these two types of approaches across various scales ( e.g., CBSA versus nationwide), taking into account population weighting approaches utilized in epidemiologic studies when estimating PM2.5 exposure (U.S. EPA, 2022b, section 2.3.3.2.4). Additionally, the 2022 PA assesses how average PM2.5 concentrations computed in epidemiologic studies using these hybrid surfaces compare to the maximum design values measured at ground-based monitors. For this assessment, the 2022 PA evaluates the DI2019 [40] and HA2020 [41] hybrid surfaces, surfaces that are used in several of the key epidemiologic studies in the 2022 PA. This analysis is intended to help inform how the magnitude of the overall study-reported mean PM2.5 concentrations in epidemiologic studies may be Start Printed Page 16218 influenced by the approach used to compute that mean and how that value might compare to monitor reported concentrations. The PM2.5 standards are expected to achieve a pattern of air quality through the attainment of a specific design value at each monitor in the monitoring network. As a result, it is important to be able to assess the relationship between monitor concentrations and patterns of air quality evaluated in the epidemiologic studies.
In estimating exposure, some studies focus on estimating concentrations in urban areas, while others examine the entire U.S. or large portions of the country. In general, the areas that are not included in the CBSA-only analysis tend to be more rural or less densely populated areas, tend to have lower PM2.5 concentrations, and likely correspond to those locations where monitoring data availability is limited or nonexistent (U.S. EPA, 2022b, section 2.3.3.2.4, Figure 2–37). To evaluate the differences in mean PM2.5 concentrations across different spatial scales, the 2022 PA analysis compares the DI2019 and HA2020 surfaces. At the national scale, the two surfaces generally produce similar average annual PM2.5 concentrations, with the DI2019 surface being slightly higher compared to the HA2020 surface. The average annual PM2.5 concentrations are also slightly higher using the DI2019 surface compared to the HA2020 surface when the analyses are conducted for CBSAs. Also, regardless of which surface is used, the average annual and 3-year average of the average annual PM2.5 concentrations for the CBSA-only analyses are somewhat higher than for the nationwide analyses (4–8% higher) (U.S. EPA, 2022b, section 2.3.3.2.4, Table 2–5).[42] Overall, these analyses suggest that there are only slight differences in the average PM2.5 concentrations depending on the hybrid modeling method employed, though including other hybrid modeling methods in this comparison could result in larger differences.
The 2022 PA next evaluates how the averages of the hybrid model surfaces compare to regulatory design values using both the DI2019 and HA2020 surfaces and how population weighting influences the mean PM2.5 concentration.[43] As presented in the 2022 PA, the results using the DI2019 and HA2020 surfaces are similar for the average annual PM2.5 concentrations, for each 3-year period. When population weighting is not applied, the average annual PM2.5 concentrations generally range from 7.0 to 8.6 µg/m3 . When population weighting is applied, the average annual PM2.5 concentrations are slightly higher, ranging from 8.2 to 10.2 µg/m3 . As with CBSAs versus the national comparison above, population weighting results in a higher average PM2.5 concentration than when population weighting is not applied (U.S. EPA, 2022b, section 2.3.3.2.4, Table 2–7). For the CBSAs included in the population weighted analyses, the average maximum annual design values generally range from 9.5 to 11.7 µg/m3 . The results are similar for both the DI2019 and HA2020 surfaces and the maximum annual PM2.5 design values measured at the monitors are often 40% to 50% higher than average annual PM2.5 concentrations predicted by hybrid modeling methods when population weighting is not applied. However, when population weighting is applied, the ratio of the maximum annual PM2.5 design values to the predicted average annual PM2.5 concentrations are lower than when population weighting is not applied, with monitored design values generally 15% to 18% higher than population-weighted hybrid modeling average annual PM2.5 concentrations (U.S. EPA, 2022b, section 2.3.3.2.4, Table 2–7).
6. Background PM
In this reconsideration, background PM is defined as all particles that are formed by sources or processes that cannot be influenced by actions within the jurisdiction of concern. U.S. background PM is defined as any PM formed from emissions other than U.S. anthropogenic ( i.e., manmade) emissions. Potential sources of U.S. background PM include both natural sources ( i.e., PM that would exist in the absence of any anthropogenic emissions of PM or PM precursors) and transboundary sources originating outside U.S. borders. Background PM is discussed in more detail in the 2022 PA (U.S. EPA, 2022b, section 2.4). At annual and national scales, estimated background PM concentrations in the U.S. are small compared to contributions from domestic anthropogenic sources.[44] For example, based on zero-out modeling in the last review of the PM NAAQS, annual background PM2.5 concentrations were estimated to range from 0.5–3 µg/m3 across the sites examined. In addition, speciated monitoring data from IMPROVE sites can provide some insights into how contributions from different sources, including sources of background PM, may have changed over time. Such data suggests the estimates of background concentrations using speciated monitoring data from IMPROVE monitors are around 1–3 µg/m3 and have not changed significantly since the 2012 review. Contributions to background PM in the U.S. result mainly from sources within North America. Contributions from intercontinental events have also been documented ( e.g., transport from dust storms occurring in deserts in North Africa and Asia), but these events are less frequent and represent a relatively small fraction of background PM in most of the U.S. (U.S. EPA, 2022b, section 2.4).
II. Rationale for Decisions on the Primary PM 2.5 Standards
This section presents the rationale for the Administrator's decision to revise the primary annual PM2.5 standard down to a level of 9 µg/m[3] and retain the primary 24-hour PM2.5 standard. This rationale is based on a thorough review of the scientific evidence generally published through January 2018,[45] as evaluated in the 2019 ISA (U.S. EPA, 2019a), on the human health effects of PM2.5 associated with long- and short-term exposures [46] to PM2.5 in Start Printed Page 16219 the ambient air. Additionally, this rationale is based on a thorough evaluation of some studies that became available after the literature cutoff date of the 2019 ISA, as evaluated in the ISA Supplement, that could either further inform the adequacy of the current PM NAAQS or address key scientific topics that have evolved since the literature cutoff date for the 2019 ISA, generally through March 2021 (U.S. EPA, 2022a).[47] The Administrator's rationale also takes into account: (1) The 2022 PA evaluation of the policy-relevant information in the 2019 ISA and ISA Supplement and presentation of quantitative analyses of air quality and health risks; (2) CASAC advice and recommendations; and (3) public comments received during the development of these documents.
In presenting the rationale for the Administrator's decisions and its foundations, section II.A provides background on the general approach for this reconsideration and the basis for the existing standard, and also presents brief summaries of key aspects of the currently available health effects and risk information. Section II.B summarizes the CASAC advice and the basis for the proposed conclusions, addresses public comments received on the proposal and presents the Administrator's conclusions on the adequacy of the current standards, drawing on consideration of the scientific evidence and quantitative risk information, advice from the CASAC, and comments from the public. Section II.C summarizes the Administrator's decision on the primary PM2.5 standards.
A. Introduction
The general approach for this reconsideration of the 2020 final decision on the primary PM2.5 standards is fundamentally based on using the EPA's assessment of the current scientific evidence and associated quantitative analyses to inform the Administrator's judgment regarding primary PM2.5 standards that protect public health with an adequate margin of safety. The EPA's assessments are primarily documented in the 2019 ISA, ISA Supplement, and 2022 PA, all of which have received CASAC review and public comment (83 FR 53471, October 23, 2018; 83 FR 55529, November 6, 2018; 85 FR 4655, January 27, 2020; 86 FR 52673, September 22, 2021; 86 FR 54186, September 30, 2021; 86 FR 56263, October 8, 2021; 87 FR 958, January 7, 2022; 87 FR 22207, April 14, 2022; 87 FR 31965, May 26, 2022). In bridging the gap between the scientific assessments of the 2019 ISA and ISA Supplement and the judgments required of the Administrator in determining whether the current standards provide the requisite public health protection, the 2022 PA evaluates policy implications of the evaluation of the current evidence in the 2019 ISA and ISA Supplement, and the risk information documented in the 2022 PA. In evaluating the public health protection afforded by the current standards, the four basic elements of the NAAQS ( i.e., indicator, averaging time, level, and form) are considered collectively.
The final decision on the adequacy of the current primary PM2.5 standards is a public health policy judgment to be made by the Administrator. In reaching conclusions with regard to the standards, the decision will draw on the scientific information and analyses about health effects and population risks, as well as judgments about how to consider the range and magnitude of uncertainties that are inherent in the scientific evidence and analyses. This approach is based on the recognition that the available health effects evidence generally reflects a continuum, consisting of levels at which scientists generally agree that health effects are likely to occur, through lower levels at which the likelihood and magnitude of the response become increasingly uncertain. This approach is consistent with the requirements of the NAAQS provisions of the Clean Air Act and with how the EPA and the courts have historically interpreted the Act (summarized in section I.A above). These provisions require the Administrator to establish primary standards that, in the judgment of the Administrator, are requisite to protect public health with an adequate margin of safety. In so doing, the Administrator seeks to establish standards that are neither more nor less stringent than necessary for this purpose. The Act does not require that primary standards be set at a zero-risk level, but rather at a level that avoids unacceptable risks to public health, including the health of sensitive (also referred to as “at-risk”) groups.[48]
1. Background on the Current Standards
The current primary PM2.5 standards were retained in 2020 based on the scientific evidence and quantitative risk information available at that time, as well as the then-Administrator's judgments regarding the available health effects evidence and the appropriate degree of public health protection afforded by the existing standards (85 FR 82718, December 18, 2020). With the 2020 decision, the then-Administrator retained the primary annual PM2.5 standard with its level of 12.0 μg/m3 and retained the primary 24-hour PM2.5 standard with its level of 35 μg/m3 . The key considerations and the then-Administrator's conclusions regarding the primary PM2.5 standards in the 2020 review are summarized below.
The health effects evidence base available in the 2020 review included extensive evidence from previous reviews as well as the evidence that had emerged since the prior review had been completed in 2012. This evidence base, spanning several decades, documents the relationship between short- and long-term PM2.5 exposure and mortality or serious morbidity effects. The evidence available in the 2019 ISA reaffirmed, and in some cases strengthened, the conclusions from the 2009 ISA regarding the health effects of PM2.5 exposures (U.S. EPA, 2019a). Much of the evidence came from epidemiologic studies conducted in North America, Europe, or Asia examining short-term and long-term exposures that demonstrated generally positive, and often statistically significant, PM2.5 health effect associations with a range of outcomes including non- accidental, cardiovascular, or respiratory mortality; cardiovascular- or respiratory-related hospitalizations or emergency department visits; and other mortality/morbidity outcomes ( e.g., lung cancer mortality or incidence, asthma development). Experimental evidence, as well as evidence from panel studies, strengthened support for potential biological pathways through which PM2.5 exposures could lead to health effects reported in many population-based epidemiologic studies, including support for pathways that could lead to cardiovascular, respiratory, nervous system, and cancer-related effects. Start Printed Page 16220 Based on this evidence, the 2019 ISA concluded there to be a causal relationship between long- and short-term PM2.5 exposure and mortality and cardiovascular effects, as well as likely to be causal relationships between long- and short-term PM2.5 exposure and respiratory effects, and between long-term PM2.5 exposure and cancer and nervous system effects (U.S. EPA, 2019a, section 1.7).
Epidemiologic studies reported PM2.5 health effect associations with mortality and/or morbidity across multiple U.S. cities and in diverse populations, including in studies examining populations and lifestages that may be at increased risk of experiencing a PM2.5 -related health effect ( e.g., older adults, children). The 2019 ISA cited extensive evidence indicating that “both the general population as well as specific populations and lifestages are at risk for PM2.5 -related health effects” (U.S. EPA, 2019a, p. 12–1), including children and older adults, people with pre-existing respiratory or cardiovascular disease, minority populations, and low socioeconomic status (SES) populations.
The risk information available in the 2020 review included risk estimates for air quality conditions just meeting the existing primary PM2.5 standards, and also for air quality conditions just meeting potential alternative standards. The general approach to estimating PM2.5 -associated health risks combined concentration-response (C–R) functions from epidemiologic studies with model-based PM2.5 air quality surfaces, baseline health incidence data, and population demographics for 47 urban areas (U.S. EPA, 2020b, section 3.3, Figure 3–10, Appendix C). The risk assessment estimated that the existing primary PM2.5 standards could allow a substantial number of PM2.5 -associated deaths in the U.S. Uncertainty in risk estimates ( e.g., in the size of risk estimates) can result from a number of factors, including assumptions about the shape of the C–R relationship with mortality at low ambient PM2.5 concentrations, the potential for confounding and/or exposure measurement error, and the methods used to adjust PM2.5 air quality.
Consistent with the general approach routinely employed in NAAQS reviews, the initial consideration in the 2020 review of the primary PM2.5 standards was with regard to the adequacy of the protection provided by the existing standards.
As an initial matter, the then-Administrator considered the range of scientific evidence evaluating these effects, including studies of at-risk populations, to inform his review of the primary PM2.5 standards, placing the greatest weight on evidence of effects for which the 2019 ISA determined there to be a causal or likely to be causal relationship with long- and short-term PM2.5 exposures (85 FR 82714–82715, December 18, 2020).
With regard to indicator, the then-Administrator recognized that, consistent with the evidence available in prior reviews, the scientific evidence continued to provide strong support for health effects following short- and long-term PM2.5 exposures. He noted the 2020 PA conclusions that the information continued to support the PM2.5 mass-based indicator and remained too limited to support a distinct standard for any specific PM2.5 component or group of components, and too limited to support a distinct standard for the ultrafine fraction. Thus, the then-Administrator concluded that it was appropriate to retain PM2.5 as the indicator for the primary standards for fine particles (85 FR 82715, December 18, 2020).
With respect to averaging time and form, the then-Administrator noted that the scientific evidence continued to provide strong support for health effects associations with both long-term ( e.g., annual or multi-year) and short-term ( e.g., mostly 24-hour) exposures to PM2.5, consistent with the conclusions in the 2020 PA. In the 2019 ISA, epidemiologic and controlled human exposure studies examined a variety of PM2.5 exposure durations. Epidemiologic studies continued to provide strong support for health effects associated with short-term PM2.5 exposures based on 24-hour PM2.5 averaging periods, and the EPA noted that associations with subdaily estimates are less consistent and, in some cases, smaller in magnitude (U.S. EPA, 2019a, section 1.5.2.1; U.S. EPA, 2020b, section 3.5.2.2). In addition, controlled human exposure and panel-based studies of subdaily exposures typically examined subclinical effects, rather than the more serious population-level effects that have been reported to be associated with 24-hour exposures ( e.g., mortality, hospitalizations). Taken together, the 2019 ISA concluded that epidemiologic studies did not indicate that subdaily averaging periods were more closely associated with health effects than the 24-hour average exposure metric (U.S. EPA, 2019a, section 1.5.2.1). Additionally, while controlled human exposure studies provided consistent evidence for cardiovascular effects following PM2.5 exposures for less than 24 hours ( i.e., <30 minutes to 5 hours), exposure concentrations in the studies were well-above the ambient concentrations typically measured in locations meeting the existing standards (U.S. EPA, 2020b, section 3.2.3.1). Thus, these studies also did not suggest the need for additional protection against subdaily PM2.5 exposures (U.S. EPA, 2020b, section 3.5.2.2). Therefore, the then-Administrator judged that the 24-hour averaging time remained appropriate (85 FR 82715, December 18, 2020).
With regard to the form of the 24-hour standard (98th percentile, averaged over three years), the then-Administrator noted that epidemiologic studies continued to provide strong support for health effect associations with short-term ( e.g., mostly 24-hour) PM2.5 exposures (U.S. EPA, 2020b, section 3.5.2.3) and that controlled human exposure studies provided evidence for health effects following single short-term “peak” PM2.5 exposures. Thus, the evidence supported retaining a standard focused on providing supplemental protection against short-term peak exposures and supported a 98th percentile form for a 24-hour standard. The then-Administrator further noted that this form also provided an appropriate balance between limiting the occurrence of peak 24-hour PM2.5 concentrations and identifying a stable target for risk management programs (U.S. EPA, 2020b, section 3.5.2.3). As such, the then-Administrator concluded that the available information supported retaining the form and averaging time of the current 24-hour standard (98th percentile, averaged over three years) and annual standard (annual average, averaged over three years) (85 FR 82715, December 18, 2020).
With regard to the level of the standards, in reaching his final decision, the then-Administrator considered the large body of evidence presented and assessed in the 2019 ISA (U.S. EPA, 2019a), the policy-relevant and risk-based conclusions and rationales as presented in the 2020 PA (U.S. EPA, 2020b), advice from the CASAC, and public comments. In particular, in considering the 2019 ISA and 2020 PA, he considered key epidemiologic studies that evaluated associations between PM2.5 air quality distributions and mortality and morbidity, including key accountability studies; the availability of experimental studies to support biological plausibility; controlled human exposure studies examining effects following short-term PM2.5 exposures; air quality analyses; and the important uncertainties and limitations associated with the information (85 FR 82715, December 18, 2020). Start Printed Page 16221
As an initial matter, the then-Administrator considered the protection afforded by both the annual and 24-hour standards together against long- and short-term PM2.5 exposures and health effects. The Administrator recognized that the annual standard was most effective in controlling “typical” PM2.5 concentrations near the middle of the air quality distribution ( i.e., around the mean of the distribution), but also provided some control over short-term peak PM2.5 concentrations. On the other hand, the 24-hour standard, with its 98th percentile form, was most effective at limiting peak 24-hour PM2.5 concentrations, but in doing so also had an effect on annual average PM2.5 concentrations. Thus, while either standard could be viewed as providing some measure of protection against both average exposures and peak exposures, the 24-hour and annual standards were not expected to be equally effective at limiting both types of exposures. Thus, consistent with previous reviews, the then-Administrator's consideration of the public health protection provided by the existing primary PM2.5 standards was based on his consideration of the combination of the annual and 24-hour standards. Specifically, he recognized that the annual standard was more likely to appropriately limit the “typical” daily and annual exposures that are most strongly associated with the health effects observed in epidemiologic studies. The then-Administrator concluded that an annual standard (as the arithmetic mean, averaged over three years) remained appropriate for targeting protection against the annual and daily PM2.5 exposures around the middle portion of the PM2.5 air quality distribution. Further, recognizing that the 24-hour standard (with its 98th percentile form) was more directly tied to short-term peak PM2.5 concentrations, and more likely to appropriately limit exposures to such concentrations, the then-Administrator concluded that the current 24-hour standard (with its 98th percentile form, averaged over three years) remained appropriate to provide a balance between limiting the occurrence of peak 24-hour PM2.5 concentrations and identifying a stable target for risk management programs. However, the then-Administrator recognized that changes in PM2.5 air quality to meet an annual standard would likely result not only in lower short- and long-term PM2.5 concentrations near the middle of the air quality distribution, but also in fewer and lower short-term peak PM2.5 concentrations. The then-Administrator further recognized that changes in air quality to meet a 24-hour standard, with a 98th percentile form, would result not only in fewer and lower peak 24-hour PM2.5 concentrations, but also in lower annual average PM2.5 concentrations (85 FR 82715–82716, December 18, 2020).
Thus, in considering the adequacy of the 24-hour standard, the then-Administrator noted the importance of considering whether additional protection was needed against short-term exposures to peak PM2.5 concentrations. In examining the scientific evidence, he noted the limited utility of the animal toxicological studies in directly informing conclusions on the appropriate level of the standard given the uncertainty in extrapolating from effects in animals to those in human populations. The then-Administrator noted that controlled human exposure studies provided evidence for health effects following single, short-term PM2.5 exposures that corresponded best to exposures that might be experienced in the upper end of the PM2.5 air quality distribution in the U.S. ( i.e., “peak” concentrations). However, most of these studies examined exposure concentrations considerably higher than are typically measured in areas meeting the standards (U.S. EPA, 2020b, section 3.2.3.1). In particular, controlled human exposure studies often reported statistically significant effects on one or more indicators of cardiovascular function following 2-hour exposures to PM2.5 concentrations at and above 120 μg/m3 (at and above 149 μg/m3 for vascular impairment, the effect shown to be most consistent across studies). To provide insight into what these studies may indicate regarding the primary PM2.5 standards, the 2020 PA (U.S. EPA, 2020b, p. 3–49) noted that 2-hour ambient concentrations of PM2.5 at monitoring sites meeting the current standards almost never exceeded 32 μg/m3 . In fact, even the extreme upper end of the distribution of 2-hour PM2.5 concentrations at sites meeting the primary PM2.5 standards remained well-below the PM2.5 exposure concentrations consistently shown in controlled human exposure studies to elicit effects ( i.e., 99.9th percentile of 2-hour concentrations at these sites is 68 μg/m3 during the warm season). Thus, the experimental evidence did not indicate the need for additional protection against exposures to peak PM2.5 concentrations, beyond the protection provided by the combination of the 24-hour and the annual standards (U.S. EPA, 2020b, section 3.2.3.1; 85 FR 82716, December 18, 2020).
With respect to the epidemiologic evidence, the then-Administrator noted that the studies did not indicate that associations in those studies were strongly influenced by exposures to peak concentrations in the air quality distribution and thus did not indicate the need for additional protection against short-term exposures to peak PM2.5 concentrations (U.S. EPA, 2020b, section 3.5.1). The then-Administrator noted that this was consistent with CASAC consensus support for retaining the current 24-hour standard. Thus, the then-Administrator concluded that the 24-hour standard with its level of 35 µg/m3 was adequate to provide supplemental protection ( i.e., beyond that provided by the annual standard alone) against short-term exposures to peak PM2.5 concentrations (85 FR 82716, December 18, 2020).
With regard to the level of the annual standard, the then-Administrator recognized that the annual standard, with its form based on the arithmetic mean concentration, was most appropriately meant to limit the “typical” daily and annual exposures that were most strongly associated with the health effects observed in epidemiologic studies. However, the then-Administrator also noted that while epidemiologic studies examined associations between distributions of PM2.5 air quality and health outcomes, they did not identify particular PM2.5 exposures that cause effects and thus, they could not alone identify a specific level at which the standard should be set, as such a determination necessarily required the then-Administrator's judgment. Thus, consistent with the approaches in previous NAAQS reviews, the then-Administrator recognized that any approach that used epidemiologic information in reaching decisions on what standards are appropriate necessarily required judgments about how to translate the information from the epidemiologic studies into a basis for appropriate standards. This approach included consideration of the uncertainties in the reported associations between daily or annual average PM2.5 exposures and mortality or morbidity in the epidemiologic studies. Such an approach is consistent with setting standards that are neither more nor less stringent than necessary, recognizing that a zero-risk standard is not required by the Clean Air Act (CAA) (85 FR 82716, December 18, 2020).
The then-Administrator emphasized uncertainties and limitations that were present in epidemiologic studies in previous reviews and persisted in the 2020 review. These uncertainties Start Printed Page 16222 included exposure measurement error, potential confounding by copollutants, increasing uncertainty of associations at lower PM2.5 concentrations, and heterogeneity of effects across different cities or regions (85 FR 82716, December 18, 2020). The then-Administrator also noted the advice given by the CASAC on this matter. As described in section I.C.5 above, the CASAC did not reach consensus on the adequacy of the primary annual PM2.5 standard. “Some CASAC members” expressed support for retaining the primary annual PM2.5 standard while “other members” expressed support for revising that standard in order to increase public health protection (Cox, 2019b, p. 1 of consensus letter). The CASAC members who supported retaining the annual standard expressed their concerns with the epidemiologic studies, asserting that these studies did not provide a sufficient basis for revising the existing standards. They also identified several key concerns regarding the associations reported in epidemiologic studies and concluded that “while the data on associations should certainly be carefully considered, this data should not be interpreted more strongly than warranted based on its methodological limitations” (Cox, 2019b, p. 8 consensus responses).
Taking into consideration the views expressed by the CASAC members who supported retaining the annual standard, the then-Administrator recognized that epidemiologic studies examined associations between distributions of PM2.5 air quality and health outcomes, and they did not identify particular PM2.5 exposures that cause effects (U.S. EPA, 2020b, section 3.1.2). While the Administrator remained concerned about placing too much weight on epidemiologic studies to inform conclusions on the adequacy of the primary standards, he noted the approach to considering such studies in the 2012 review. In the 2012 review, it was noted that the evidence of an association in any epidemiologic study was “strongest at and around the long-term average where the data in the study are most concentrated” (78 FR 3140, January 15, 2013). In considering the characterization of epidemiologic studies, the then-Administrator viewed that when assessing the mean concentrations of the key short-term and long-term epidemiologic studies in the U.S. that used ground-based monitoring ( i.e., those studies where the mean is most directly comparable to the current annual standard), the majority of studies had mean concentrations at or above the level of the existing annual standard, with the mean of the study-reported means or medians equal to 13.5 µg/m[3] , a concentration level above the existing level of the primary annual standard of 12 µg/m[3] . The then-Administrator further noted his caution in directly comparing the reported study mean values to the standard level given that study-reported mean concentrations, by design, are generally lower than the design value of the highest monitor in an area, which determines compliance. In the 2020 PA, analyses of recent air quality in U.S. CBSAs indicated that maximum annual PM2.5 design values for a given three-year period were often 10% to 20% higher than average monitored concentrations ( i.e., averaged across multiple monitors in the same CBSA) (U.S. EPA, 2020b, Appendix B, section B.7). He further noted his concern in placing too much weight on any one epidemiologic study but instead judged that it was more appropriate to focus on the body of studies together and therefore noted the calculation of the mean of study-reported means (or medians). Thus, while the then-Administrator was cautious in placing too much weight on the epidemiologic evidence alone, he noted that: (1) The reported mean concentration in the majority of the key U.S. epidemiologic studies using ground-based monitoring data were above the level of the existing annual standard; (2) the mean of the reported study means (or medians) ( i.e., 13.5 µg/m[3] ) was above the level of the current standard; [49] (3) air quality analyses showed the study means to be lower than their corresponding design values by 10–20%; and (4) these analyses must be considered in light of uncertainties inherent in the epidemiologic evidence. When taken together, the then-Administrator judged that, even if it were appropriate to place more weight on the epidemiologic evidence, this information did not call into question the adequacy of the current standards (85 FR 82716–17, December 18, 2020).
In addition to the evidence, the then-Administrator also considered the potential implications of the risk assessment. He noted that all risk assessments have limitations and that he remained concerned about the uncertainties in the underlying epidemiologic data used in the risk assessment. The then-Administrator also noted that in previous reviews, these uncertainties and limitations have often resulted in less weight being placed on quantitative estimates of risk than on the underlying scientific evidence itself ( e.g.,78 FR 3086, 3098–99, January 15, 2013). These uncertainties and limitations included uncertainty in the shapes of C–R functions, particularly at low concentrations; uncertainties in the methods used to adjust air quality; and uncertainty in estimating risks for populations, locations and air quality distributions different from those examined in the underlying epidemiologic study (U.S. EPA, 2020b, section 3.3.2.4). Additionally, the then-Administrator noted similar concern expressed by some members of the CASAC who support retaining the existing standards; they highlighted similar uncertainties and limitations in the risk assessment (Cox, 2019b). In light of all of this, the then-Administrator judged it appropriate to place little weight on quantitative estimates of PM2.5 -associated mortality risk in reaching conclusions about the level of the primary PM2.5 standards (85 FR 82717, December 18, 2020).
The then-Administrator additionally considered an emerging body of evidence from accountability studies that examined past reductions in ambient PM2.5 and the degree to which those reductions resulted in public health improvements. While the then-Administrator agreed with public commenters that well-designed and conducted accountability studies can be informative, he viewed the interpretation of such studies in the context of the primary PM2.5 standards as complicated by the fact that some of the available studies had not evaluated PM2.5 specifically ( e.g., as opposed to PM10 or total suspended particulates), did not show changes in PM2.5 air quality, or had not been able to disentangle health impacts of the interventions from background trends in health (U.S. EPA, 2020b, section 3.5.1). He further recognized that the small number of available studies that did report public health improvements following past declines in ambient PM2.5 had not examined air quality meeting the existing standards (U.S. EPA, 2020b, Table 3–3). This included U.S. studies that reported increased life expectancy, decreased mortality, and decreased respiratory effects following past declines in ambient PM2.5 concentrations. Such studies examined “starting” annual average PM2.5 concentrations ( i.e., prior to the reductions being evaluated) ranging from about 13.2 to >20µg/m3 ( i.e., U.S. EPA, 2020b, Table 3–3). Given the lack of available accountability studies Start Printed Page 16223 reporting public health improvements attributable to reductions in ambient PM2.5 in locations meeting the existing standards, together with his broader concerns regarding the lack of experimental studies examining PM2.5 exposures typical of areas meeting the existing standards, the then-Administrator judged that there was considerable uncertainty in the potential for increased public health protection from further reductions in ambient PM2.5 concentrations beyond those achieved under the existing primary PM2.5 standards (85 FR 82717, December 18, 2020).
When the above considerations were taken together, the then-Administrator concluded that the scientific evidence assessed in the 2019 ISA, together with the analyses in the 2020 PA based on that evidence and consideration of CASAC advice and public comments, did not call into question the adequacy of the public health protection provided by the existing annual and 24-hour PM2.5 standards. In particular, the then-Administrator judged that there was considerable uncertainty in the potential for additional public health improvements from reducing ambient PM2.5 concentrations below the concentrations achieved under the existing primary standards and that, therefore, standards more stringent than the existing standards ( e.g., with lower levels) were not supported. That is, he judged that more stringent standards would be more than requisite to protect the public health with an adequate margin of safety. This judgment reflected the Administrator's consideration of the uncertainties in the potential implications of the lower end of the air quality distributions from the epidemiologic studies due in part to the lack of supporting evidence from experimental studies and retrospective accountability studies conducted at PM2.5 concentrations meeting the existing standards (85 FR 82717, December 18, 2020).
In reaching this conclusion in the 2020 review, the then-Administrator judged that the existing standards provided an adequate margin of safety. With respect to the annual standard, the level of 12 µg/m3 was below the lowest “starting” concentration ( i.e., 13.2 µg/m3 ) in the available accountability studies that showed public health improvements attributable to reductions in ambient PM2.5. In addition, while the then-Administrator placed less weight on the epidemiologic evidence for selecting a standard, he noted that the level of the annual standard was below the reported mean (and median) concentrations in the majority of the key U.S. epidemiologic studies using ground-based monitoring data (noting that these means tend to be 10–20% lower than their corresponding area design values which is the more relevant metric when considering the level of the standard) and below the mean of the reported means (or medians) of these studies ( i.e., 13.5 µg/m3 ). In addition, the then-Administrator recognized that concentrations in areas meeting the existing 24-hour and annual standards remained well-below the PM2.5 exposure concentrations consistently shown to elicit effects in human exposure studies (85 FR 82717–82718, December 18, 2020).
In addition, based on the then-Administrator's review of the science in the 2020 review, including controlled human exposure studies examining effects following short-term PM2.5 exposures, the epidemiologic studies, and accountability studies conducted at levels just above the existing annual standard, he judged that the degree of public health protection provided by the existing annual standard is not greater than warranted. This judgment, together with the fact that no CASAC member expressed support for a less stringent standard, led the then- Administrator to conclude that standards less stringent than the existing standards ( e.g., with higher levels) were also not supported (85 FR 82718, December 18, 2020).
In reaching his final decision in the 2020 review, the then-Administrator concluded that the scientific evidence and technical information continued to support the existing annual and 24-hour PM2.5 standards. This conclusion reflected the then-Administrator's view that there were important limitations and uncertainties that remained in the evidence. The then-Administrator concluded that these limitations contributed to considerable uncertainty regarding the potential public health implications of revising the existing primary PM2.5 standards. Given this uncertainty, and noting the advice from some CASAC members, he concluded that the primary PM2.5 standards, including the indicators (PM2.5 ), averaging times (annual and 24-hour), forms (arithmetic mean and 98th percentile, averaged over three years) and levels (12.0 µg/m3 , 35 µg/m3 ), when taken together, remained requisite to protect the public health. Therefore, in the 2020 review, the Administrator reached the conclusion that the primary 24-hour and annual PM2.5 standards, together, were requisite to protect public health from fine particles with an adequate margin of safety, including the health of at-risk populations, and retained the standards, without revision (85 FR 82718, December 18, 2020).
2. Overview of the Health Effects Evidence
The information summarized here and further detailed in section II.B of the proposal (88 FR 5580, January 27, 2023), is an overview of the policy-relevant aspects of the health effects evidence available in this reconsideration; the assessment of this evidence is documented in the 2019 ISA (U.S. EPA, 2019a) and ISA Supplement (U.S. EPA, 2022a) and its policy implications are further discussed in the 2022 PA (U.S. EPA, 2022b). While the 2019 ISA provides the broad scientific foundation for this reconsideration, additional literature has become available since the cutoff date of the 2019 ISA that expands the body of evidence related to mortality and cardiovascular effects for both short- and long-term PM2.5 exposure, which can inform the Administrator's judgment on the adequacy of the current primary PM2.5 standards. As such, the ISA Supplement builds on the information presented within the 2019 ISA with a targeted identification and evaluation of new scientific information (U.S. EPA, 2022a, section 1.2). The ISA Supplement focuses on PM2.5 health effects evidence where the 2019 ISA concludes a “causal relationship,” because such health effects are given the most weight in an Administrator's decisions in a NAAQS review. As such, in selecting the health effects to evaluate within the ISA Supplement ( i.e., newly available evidence related to short- and long-term PM2.5 exposure and mortality and cardiovascular effects), the primary rationale is based on the causality determinations for health effect categories presented in the 2019 PM ISA, and the subsequent use of the health effects evidence in the 2020 PM PA. Specifically, U.S. and Canadian epidemiologic studies for mortality and cardiovascular effects, along with controlled human exposure studies associated with cardiovascular effects at near ambient concentrations, were considered to be of greatest utility in informing the Administrator's conclusions on the adequacy of the current primary PM2.5 standards. Additionally, studies examining associations outside the U.S. or Canada reflect air quality and exposure patterns that may be less typical of the U.S., and thus less likely to be informative for purposes of reviewing the NAAQS (U.S. EPA, 2022b, p.1–3). While the ISA Supplement does not include information for health effects other than mortality and cardiovascular effects, the Start Printed Page 16224 scientific evidence for other health effect categories is evaluated in the 2019 ISA, which in combination with the ISA Supplement represents the complete scientific record for the reconsideration of the 2020 final decision.
The ISA Supplement also assessed accountability studies because these types of epidemiologic studies were part of the body of evidence that was a focus of the 2020 review. Accountability studies inform our understanding of the potential for public health improvements as ambient PM2.5 concentrations have declined over time. Further, the ISA Supplement considered studies that employed statistical approaches that attempt to more extensively account for confounders and are more robust to model misspecification ( i.e., used alternative methods for confounder control),[50] given that such studies were highlighted by the CASAC and identified in public comments in the 2020 review. Since the literature cutoff date for the 2019 ISA, multiple accountability studies and studies that employ alternative methods for confounder control have become available for consideration in the ISA Supplement and, subsequently, in this reconsideration.
The ISA Supplement also considered recent health effects evidence that addresses key scientific issues where the literature has expanded since the completion of the 2019 ISA.[51] The 2019 ISA evaluated a couple of controlled human exposure studies that investigated the effect of exposure to near-ambient concentrations of PM2.5 (U.S. EPA, 2019a, section 6.1.10 and 6.1.13). The ISA Supplement adds to this limited evidence, including a recent study conducted in young healthy individuals exposed to near-ambient PM2.5 concentrations (U.S. EPA, 2022a, section 3.3.1). Given the importance of identifying populations at increased risk of PM2.5 -related effects, the ISA Supplement also included epidemiologic or exposure studies that examined whether there is evidence of exposure or risk disparities by race/ethnicity or SES. These types of studies provide additional information related to factors that may increase risk of PM2.5 -related health effects and provide additional evidence for consideration by the Administrator in reaching conclusions regarding the adequacy of the current standards. In addition, the ISA Supplement evaluated studies that examined the relationship between short- and long-term PM2.5 exposures and SARS-CoV–2 infection and/or COVID–19 death, as these studies are a new area of research and were raised by a number of public commenters in the 2020 review.
The evidence presented within the 2019 ISA, along with the targeted identification and evaluation of new scientific information in the ISA Supplement, provides the scientific basis for the reconsideration of the 2020 final decision on the primary PM2.5 standards. The subsections below briefly summarize the nature of PM2.5 -related health effects (II.A.2.a), with a focus on those health effects for which the 2019 ISA concluded a “causal” or “likely to be causal” relationship, the potential public health implications and populations at risk (II.A.2.b), and PM2.5 concentrations in key studies reporting health effects (II.A.2.c).
a. Nature of Effects
The evidence base available in the reconsideration includes decades of research on PM2.5 -related health effects (U.S. EPA, 2004b; U.S. EPA, 2009a; U.S. EPA, 2019a), including the full body of evidence evaluated in the 2019 ISA (U.S. EPA, 2019a), along with the targeted evaluation of recent evidence in the ISA Supplement (U.S. EPA, 2022a). In considering the available scientific evidence, the sections below, and in more detail in section II.B.1 of the proposal (88 FR 5580, January 27, 2023), summarize the relationships between long-and short-term PM2.5 exposures and mortality (II.A.2.a.i), cardiovascular effects (II.A.2.a.ii), respiratory effects (II.A.2.a.iii), cancer (II.A.2.a.iv), nervous system effects (II.A.2.a.v) and other effects (II.A.2.a.vi). For these outcomes, the 2019 ISA concluded that the evidence supports either a “causal” or a “likely to be causal” relationship.[52]
i. Mortality
Long-Term PM2.5 Exposures
In the 2012 review, the 2009 ISA reported that the evidence was “sufficient to conclude that the relationship between long-term PM2.5 exposures and mortality is causal” (U.S. EPA, 2009a, p. 7–96). The strongest evidence supporting this conclusion was provided by epidemiologic studies, particularly those examining two seminal cohorts, the American Cancer Society (ACS) cohort and the Harvard Six Cities cohort. Analyses of the Harvard Six Cities cohort included evidence indicating that reductions in ambient PM2.5 concentrations are associated with reduced mortality risk (Laden et al., 2006) and increases in life expectancy (Pope et al., 2009). Further support was provided by other cohort studies conducted in North America and Europe that reported positive associations between long-term PM2.5 exposure and mortality (U.S. EPA, 2019a).
Cohort studies, which have become available since the completion of the 2009 ISA and evaluated in the 2019 ISA, continue to provide consistent evidence of positive associations between long-term PM2.5 exposures and mortality. These studies add support for associations with all-cause and total (non-accidental) mortality,[53] as well as with specific causes of mortality, including cardiovascular disease and respiratory disease (U.S. EPA, 2019a, section 11.2.2). Several of these studies conducted analyses over longer study durations and periods of follow-up than examined in the original ACS and Harvard Six Cities cohort studies and continue to report positive associations between long-term exposure to PM2.5 and mortality (U.S. EPA, 2019a, section 11.2.2.1; Figures 11–18 and 11–19). In addition to studies focusing on the ACS and Harvard Six Cities cohorts, additional studies examining other cohorts also provide evidence of consistent, positive associations between long-term PM2.5 exposure and mortality across a wide range of demographic groups ( e.g., age, sex, occupation), spatial and temporal extents, exposure assessment metrics, and statistical techniques (U.S. EPA, 2019a, sections 11.2.2.1, 11.2.5; U.S. EPA, 2022a, Table 11–8). This includes some of the largest cohort studies conducted to date, such as analyses of the U.S. Medicare cohort that includes Start Printed Page 16225 nearly 61 million enrollees and studies that control for a range of individual and ecological covariates, including race, age, SES, smoking status, body mass index, and annual weather variables ( e.g., temperature, humidity) (U.S. EPA, 2019a).
In addition to those cohort studies evaluated in the 2019 ISA, recent North American cohort studies evaluated in the ISA Supplement continue to examine the relationship between long-term PM2.5 exposure and mortality and report consistent, positive, and statistically significant associations. These recent studies also utilize large and demographically diverse cohorts that are generally representative of the national populations in both the U.S. and Canada. These “studies published since the 2019 ISA support and extend the evidence base that contributed to the conclusion of a causal relationship between long-term PM2.5 exposure and mortality” (U.S. EPA, 2022a, section 3.2.2.2.1, Figure 3–19, Figure 3–20).
Furthermore, studies evaluated in the 2019 ISA and the ISA Supplement that examined cause-specific mortality expand upon previous research that found consistent, positive associations between PM2.5 exposure and specific mortality outcomes, which include cardiovascular and respiratory mortality, as well as other mortality outcomes. For cardiovascular-related mortality, the evidence evaluated in the ISA Supplement is consistent with the evidence evaluated in the 2019 ISA with recent studies reporting positive associations with long-term PM2.5 exposure. When evaluating cause-specific cardiovascular mortality, recent studies reported positive associations for a number of outcomes, such as ischemic heart disease (IHD) and stroke mortality (U.S. EPA, 2022a, Figure 3–23). Moreover, recent studies also provide some initial evidence that individuals with pre-existing health conditions, such as heart failure and diabetes, are at an increased risk of PM2.5 -related health effects (U.S. EPA, 2022a, section 3.2.2.4) and that these individuals have a higher risk of mortality overall, which was previously only examined in studies that used stratified analyses rather than a cohort of people with an underlying health condition (U.S. EPA, 2022a, section 3.2.2.4). With regard to respiratory mortality, epidemiologic studies evaluated in the 2019 ISA and ISA Supplement continue to provide support for associations between long-term PM2.5 exposure and respiratory mortality (U.S. EPA, 2019a, section 5.2.10; U.S. EPA, 2022a, Table 3–2).
A series of epidemiologic studies evaluated in the 2019 ISA tested the hypothesis that past reductions in ambient PM2.5 concentrations are associated with increased life expectancy or a decreased mortality rate and report that reductions in ambient PM2.5 are associated with improvements in longevity (U.S. EPA, 2022a, section 11.2.2.5). Pope et al. (2009) conducted a cross-sectional analysis using air quality data from 51 metropolitan areas across the U.S., beginning in the 1970s through the early 2000s, and found that a 10 µg/m3 decrease in long-term PM2.5 concentration was associated with a 0.61-year increase in life expectancy. In a subsequent analysis, the authors extended the period of analysis to include 2000 to 2007, a time period with lower ambient PM2.5 concentrations and found a decrease in long-term PM2.5 concentration continued to be associated with an increase in life expectancy, though the magnitude of the increase was smaller than during the earlier time period ( i.e., a 10 µg/m3 decrease in long-term PM2.5 concentration was associated with a 0.35-year increase in life expectancy) (Correia et al., 2013). Additional studies conducted in the U.S. or Europe similarly report that reductions in ambient PM2.5 are associated with improvements in longevity (U.S. EPA, 2022a, section 11.2.2.5).
Since the literature cutoff date for the 2019 ISA, a few epidemiologic studies were published that examined the relationship between long-term PM2.5 exposure and life-expectancy (U.S. EPA, 2022a, section 3.2.1.3) and report results that are consistent with and expand upon the body of evidence from the 2019 ISA. For example, Bennett et al. (2019) reported that PM2.5 concentrations above the lowest observed concentration (2.8 µg/m3 ) were associated with a 0.15 year decrease in national life expectancy for women and 0.13 year decrease in national life expectancy for men (U.S. EPA, 2022a, section 3.2.2.2.4, Figure 3–25). Another study compared participants living in areas with PM2.5 concentrations >12 µg/m3 to participants living in areas with PM2.5 concentrations <12 µg/m3 and reported that the number of years of life lost due to living in areas with higher PM2.5 concentrations was 0.84 years over a 5-year period (Ward-Caviness et al., 2020; U.S. EPA, 2022a, section 3.2.2.2.4).
Additionally, a number of accountability studies, which are epidemiologic studies that evaluate whether an environmental policy or air quality intervention resulted in reductions in ambient air pollution concentrations and subsequent reductions in mortality or morbidity, have emerged and were evaluated in the ISA Supplement (U.S. EPA, 2022a, section 3.2.2.3). For example, Sanders et al. (2020a) examined whether policy actions ( i.e., the first annual PM2.5 NAAQS implementation rule in 2005 for the 1997 annual PM2.5 standard with a 3-year annual average of 15.0 μg/m3 ) reduced PM2.5 concentrations and mortality rates in Medicare beneficiaries between 2000–2013, and found that following implementation of the annual PM2.5 NAAQS, annual PM2.5 concentrations decreased by 1.59 μg/m3 (95% CI: 1.39, 1.80) which corresponded to a 0.93% reduction in mortality rates among individuals 65 years and older ([95% CI: 0.10%, 1.77%) in non-attainment counties relative to attainment counties.
The 2019 ISA also evaluated a small number of studies that used alternative methods for confounder control to further assess relationship between long-term PM2.5 exposure and mortality (U.S. EPA, 2019a, section 11.2.2.4). In addition, multiple epidemiologic studies that implemented alternative methods for confounder control and were published since the literature cutoff date of the 2019 ISA were evaluated in the ISA Supplement (U.S. EPA, 2022a, section 3.2.2.3). These studies used a variety of statistical methods including generalized propensity score (GPS), inverse probability weighting (IPW), and difference-in-difference (DID) to reduce uncertainties related to confounding bias in the association between long-term PM2.5 exposure and mortality. These studies reported consistent positive associations between long-term PM2.5 exposure and total mortality (U.S. EPA, 2022a, section 3.2.2.3), and provided further support for the associations reported in the cohort studies referenced above.
The 2019 ISA and ISA Supplement also evaluated the degree to which recent studies examining the relationship between long-term PM2.5 exposure and mortality addressed key policy-relevant issues and/or previously identified data gaps in the scientific evidence, including methods to estimate exposure, methods to control for confounding ( e.g., co-pollutant confounding), the shape of the C–R relationship, as well as examining whether a threshold exists below which mortality effects do not occur. With respect to exposure assessment, based on its evaluation of the evidence, the 2019 ISA concludes that positive associations between long-term PM2.5 exposures and mortality are robust Start Printed Page 16226 across recent analyses using various approaches to estimate PM2.5 exposures ( e.g., based on monitors, models, satellite-based methods, or hybrid methods that combine information from multiple sources) (U.S. EPA, 2019a, section 11.2.5.1). Hart et al. (2015) report that correction for bias due to exposure measurement error increases the magnitude of the hazard ratios (confidence intervals widen but the association remains statistically significant), suggesting that failure to correct for exposure measurement error could result in attenuation or underestimation of risk estimates.
The 2019 ISA additionally concludes that positive associations between long-term PM2.5 exposures and mortality are robust across statistical models that use different approaches to control for confounders or different sets of confounders (U.S. EPA, 2019a, sections 11.2.3 and 11.2.5), across diverse geographic regions and populations, and across a range of temporal periods including periods of declining PM concentrations (U.S. EPA, 2019a, sections 11.2.2.5 and 11.2.5.3). Additional evidence further demonstrates that associations with mortality remain robust in copollutants analyses (U.S. EPA, 2019a, section 11.2.3), and that associations persist in analyses restricted to long-term exposures (annual average PM2.5 concentrations) below 12 μg/m3 (Di et al., 2017b) or 10 μg/m3 (Shi et al., 2016), indicating that risks are not disproportionately driven by the upper portions of the air quality distribution. Recent studies evaluated in the ISA Supplement further assess potential copollutant confounding and indicate that while there is some evidence of potential confounding of the PM2.5 -mortality association by copollutants in some of the studies ( i.e., those studies of the Mortality Air Pollution Associations in Low Exposure Environments (MAPLE) cohort), this result is inconsistent with other recent studies evaluated in the 2019 ISA that were conducted in the U.S. and Canada that found associations in both single and copollutant models (U.S. EPA, 2019a; U.S. EPA, 2022a, section 3.2.2.4)
Additionally, a few studies use statistical techniques to reduce uncertainties related to potential confounding to further inform conclusions on causality for long-term PM2.5 exposure and mortality, as further detailed in section II.B.1.a.i of the proposal (88 FR 5582, January 27, 2023), studies by Greven et al. (2011), Pun et al. (2017), and Eum et al. (2018) completed sensitivity analyses as part of their Medicare cohort study in which they decompose ambient PM2.5 into “spatial” and “spatiotemporal” components in order to evaluate the potential for bias due to unmeasured spatial confounding. Pun et al. (2017) observed positive associations for the “temporal” variation model and approximately null associations for the “spatiotemporal” variation model for all causes of death except for COPD mortality. The difference in the results of these two models for most causes of death suggests the presence of unmeasured confounding, though the authors do not indicate anything about the direction or magnitude of this bias. It is important to note that the “temporal” and “spatiotemporal” coefficients are not directly comparable to the results of other epidemiologic studies when examined individually and can only be used in comparison with one another to evaluate the potential for unmeasured confounding bias. Eum et al. (2018) and Wu et al. (2020) also attempted to address long-term trends and meteorological variables as potential confounders and found that not adjusting for temporal trends could overestimate the association, while effect estimates in analyses that excluded meteorological variables remained unchanged compared to the main analyses. While results of these analyses suggest the presence of some unmeasured confounding, they do not indicate the direction or magnitude of the bias.[54]
An additional important consideration in characterizing the public health impacts associated with PM2.5 exposure is whether C–R relationships are linear across the range of concentrations or if nonlinear relationships exist along any part of this range. Studies evaluated in the 2019 ISA and the ISA Supplement examine this issue, and continue to provide evidence of linear, no-threshold relationships between long-term PM2.5 exposures and all-cause and cause-specific mortality (U.S. EPA, 2019a, section 11.2.4; U.S. EPA, 2022a, section 3.2.2.2.7, Table 3–6). Across the studies evaluated in the 2019 ISA and the ISA Supplement, a variety of statistical methods have been used to assess whether there is evidence of deviations in linearity (U.S. EPA, 2019a, Table 11–7; U.S. EPA, 2022a, section 2.2.3.2). Studies have also conducted cut-point analyses that focus on examining risk at specific ambient PM2.5 concentrations. Generally, the evidence remains consistent in supporting a no-threshold relationship, and in supporting a linear relationship for PM2.5 concentrations >8 μg/m3 . However, uncertainties remain about the shape of the C–R curve at PM2.5 concentrations <8 μg/m3 , with some recent studies providing evidence for either a sublinear, linear, or supralinear relationship at these lower concentrations (U.S. EPA, 2019a, section 11.2.4; U.S. EPA, 2022a, section 2.2.3.2). There was also some limited evidence indicating that the slope of the C–R function may be steeper (supralinear) at lower concentrations for cardiovascular mortality (U.S. EPA, 2022a, section 3.1.1.2.6).
The biological plausibility of PM2.5 -attributable mortality is supported by the coherence of effects across scientific disciplines ( i.e., animal toxicological, controlled human exposure studies, and epidemiologic) when evaluating respiratory and cardiovascular morbidity effects, which are some of the largest contributors to total (nonaccidental) mortality. The 2019 ISA outlines the available evidence for biologically plausible pathways by which inhalation exposure to PM2.5 could progress from initial events ( e.g., pulmonary inflammation, autonomic nervous system activation) to endpoints relevant to population outcomes, particularly those related to cardiovascular diseases such as ischemic heart disease, stroke and atherosclerosis (U.S. EPA, 2019a, section 6.2.1), and to metabolic effects, including diabetes (U.S. EPA, 2019a, section 7.3.1). The 2019 ISA notes “more limited evidence from respiratory morbidity” (U.S. EPA, 2019a, p. 11–101) such as development of chronic obstructive pulmonary disease (COPD) (U.S. EPA, 2019a, section 5.2.1) to support the biological plausibility of mortality due to long-term PM2.5 exposures (U.S. EPA, 2019a, section 11.2.1).
Taken together, epidemiologic studies, including those evaluated in the 2019 ISA and more recent studies evaluated in the ISA Supplement, consistently report positive associations between long-term PM2.5 exposure and mortality across different geographic locations, populations, and analytic approaches (U.S. EPA, 2019a; U.S. EPA, 2022a, section 3.2.2.4). As such, these studies reduce key uncertainties identified in previous reviews, including those related to potential Start Printed Page 16227 copollutant confounding, and provide additional information on the shape of the C–R curve. As evaluated in the 2019 ISA, experimental and epidemiologic evidence for cardiovascular effects, and respiratory effects to a more limited degree, supports the plausibility of mortality due to long-term PM2.5 exposures. Overall, studies evaluated in the 2019 ISA support the conclusion of a causal relationship between long-term PM2.5 exposure and mortality, which is supported and extended by evidence from recent epidemiologic studies evaluated in the ISA Supplement (U.S. EPA, 2022a, section 3.2.2.4).
Short-Term PM2.5 Exposures
The 2009 ISA concluded that “a causal relationship exists between short-term exposure to PM2.5 and mortality” (U.S. EPA, 2009a). This conclusion was based on the evaluation of both multi- and single-city epidemiologic studies that consistently reported positive associations between short-term PM2.5 exposure and non-accidental mortality. These associations were strongest, in terms of magnitude and precision, primarily at lags of 0 to 1 days. Examination of the potential confounding effects of gaseous copollutants was limited, though evidence from single-city studies indicated that gaseous copollutants have minimal effect on the PM2.5 -mortality relationship ( i.e., associations remain robust to inclusion of other pollutants in copollutant models). The evaluation of cause-specific mortality found that effect estimates were larger in magnitude, but also had larger confidence intervals, for respiratory mortality compared to cardiovascular mortality. Although the largest mortality risk estimates were for respiratory mortality, the interpretation of the results was complicated by the limited coherence from studies of respiratory morbidity. However, the evidence from studies of cardiovascular morbidity provided both coherence and biological plausibility for the relationship between short-term PM2.5 exposure and cardiovascular mortality.
Multicity studies evaluated in the 2019 ISA and the ISA Supplement provide evidence of primarily positive associations between daily PM2.5 exposures and mortality, with percent increases in total mortality ranging from 0.19% (Lippmann et al., 2013) to 2.80% (Kloog et al., 2013) [55] at lags of 0 to 1 days in single-pollutant models. Whereas many studies assign exposures using data from ambient monitors, other studies employ hybrid modeling approaches, which estimate PM2.5 concentrations using data from a variety of sources ( i.e., from satellites, land use information, and modeling, in addition to monitors) and enable the inclusion of less urban and more rural locations in analyses ( e.g., Kloog et al., 2013, Lee et al., 2015, Shi et al., 2016).
Some studies have expanded the examination of potential confounders including long-term temporal trends, weather, and co-occurring pollutants. Mortality associations were found to remain positive, although in some cases were attenuated, when using different approaches to account for temporal trends or weather covariates ( e.g., U.S. EPA, 2019a, section 11.1.5.1). For example, Sacks et al. (2012) examined the influence of model specification using the approaches for confounder adjustment from models employed in several multicity studies within the context of a common data set (U.S. EPA, 2019a, section 11.1.5.1). These models use different approaches to control for long-term temporal trends and the potential confounding effects of weather. The authors report that associations between daily PM2.5 and cardiovascular mortality were similar across models, with the percent increase in mortality ranging from 1.5–2.0% (U.S. EPA, 2019a, Figure 11–4). Thus, alternative approaches to controlling for long-term temporal trends and for the potential confounding effects of weather may influence the magnitude of the association between PM2.5 exposures and mortality but have not been found to influence the direction of the observed association (U.S. EPA, 2019a, section 11.1.5.1). Taken together, the 2019 ISA and the ISA Supplement conclude that recent multicity studies conducted in the U.S., Canada, Europe, and Asia continue to provide consistent evidence of positive associations between short-term PM2.5 exposures and total mortality across studies that use different approaches to control for the potential confounding effects of weather ( e.g., temperature) (U.S. EPA, 2019a, section 1.4.1.5.1; U.S. EPA, 2022a, section 3.2.1.2).
With regard to copollutants, studies evaluated in the 2019 ISA provide additional evidence that associations between short-term PM2.5 exposures and mortality remain positive and relatively unchanged in copollutant models with both gaseous pollutants and PM10–2.5 (U.S. EPA, 2019a, section 11.1.4). Additionally, the low (r < 0.4) to moderate correlations (r = 0.4–0.7) between PM2.5 and gaseous pollutants and PM10–2.5 increase the confidence in PM2.5 having an independent effect on mortality (U.S. EPA, 2019a, section 11.1.4). Consistent with the studies evaluated in the 2019 ISA, studies evaluated in the ISA Supplement that used data from more recent years also indicate that associations between short-term PM2.5 exposure and mortality remain unchanged in copollutant models. However, the evidence indicates that the association could be larger in magnitude in the presence of some copollutants such as oxidant gases (Lavigne et al., 2018; Shin et al., 2021).
The generally positive associations reported with mortality are supported by a small group of studies employing alternative methods for confounder control or quasi-experimental statistical approaches (U.S. EPA, 2019a, section 11.1.2.1). For example, two studies by Schwartz et al. report associations between PM2.5 instrumental variables and mortality (U.S. EPA, 2019a, Table 11–2), including in an analysis limited to days with 24-hour average PM2.5 concentrations <30 μg/m3 (Schwartz et al., 2015; Schwartz et al., 2017). In addition to the main analyses, these studies conducted Granger-like causality tests as sensitivity analyses to examine whether there was evidence of an association between mortality and PM2.5 after the day of death, which would support the possibility that unmeasured confounders were not accounted for in the statistical model. Neither study reports evidence of an association with PM2.5 after death ( i.e., they do not indicate unmeasured confounding). Yorifuji et al. (2016) conducted a quasi-experimental study to examine whether a specific regulatory action in Tokyo, Japan ( i.e., a diesel emission control ordinance) resulted in a subsequent reduction in daily mortality (Yorifuji et al., 2016). The authors reported a reduction in mortality in Tokyo due to the ordinance, compared to Osaka, which did not have a similar diesel emission control ordinance in place. In another study, Schwartz et al. (2018) utilized three statistical methods including instrumental variable analysis, a negative exposure control, and marginal structural models to estimate the association between PM2.5 and daily mortality (Schwartz et al., 2018). Results from this study continue to support a relationship between short-term PM2.5 exposure and mortality. Additional epidemiologic studies evaluated in the ISA Supplement that employed alternative methods for confounder control to examine the association between short-term PM2.5 exposure and Start Printed Page 16228 mortality also report consistent positive associations in studies that examine effects across multiple cities in the U.S. (U.S. EPA, 2022a).
The positive associations for total mortality reported across the majority of studies evaluated are further supported by cause-specific mortality analyses, which generally report consistent, positive associations with both cardiovascular and respiratory mortality (U.S. EPA, 2019a, section 11.1.3). Recent multicity studies evaluated in the ISA Supplement add to the body of evidence indicating a relationship between short-term PM2.5 exposure and cause-specific mortality, with more variability in the magnitude and precision of associations for respiratory mortality (U.S. EPA, 2022a; Figure 3–14). For both cardiovascular and respiratory mortality, there has been a limited assessment of potential copollutant confounding, though initial evidence indicates that associations remain positive and relatively unchanged in models with gaseous pollutants and PM10–2.5, which further supports the copollutant analyses conducted for total mortality. The strong evidence for ischemic events and heart failure, as detailed in the assessment of cardiovascular morbidity (U.S. EPA, 2019a, Chapter 6), provides biological plausibility for PM2.5 -related cardiovascular mortality, which comprises the largest percentage of total mortality ( i.e., ~33%) (NHLBI, 2017). Although there is evidence for exacerbations of COPD and asthma, the collective body of respiratory morbidity evidence provides limited biological plausibility for PM2.5 -related respiratory mortality (U.S. EPA, 2019a, Chapter 5).
In the 2009 ISA, one of the main uncertainties identified was the regional and city-to-city heterogeneity in PM2.5 -mortality associations. Studies evaluated in the 2019 ISA examine both city-specific as well as regional characteristics to identify the underlying contextual factors that could contribute to this heterogeneity (U.S. EPA, 2019a, section 11.1.6.3). Analyses focusing on effect modification of the PM2.5 mortality relationship by PM2.5 components, regional patterns in PM2.5 components and city specific differences in composition and sources indicate some differences in the PM2.5 composition and sources across cities and regions, but these differences do not fully explain the observed heterogeneity. Additional studies find that factors related to potential exposure differences, such as housing stock and commuting, as well as city specific factors ( e.g., land use, port volume, and traffic information), may also explain some of the observed heterogeneity (U.S. EPA, 2019a, section 11.1.6.3). Collectively, studies evaluated in the 2019 ISA and the ISA Supplement indicate that the heterogeneity in PM2.5 mortality risk estimates cannot be attributed to one factor, but instead a combination of factors including, but not limited to, PM composition and sources as well as community characteristics that could influence exposures (U.S. EPA, 2019a, section 11.1.12; U.S. EPA, 2022a, section 3.2.1.2.1).
A number of studies evaluated in the 2019 ISA and ISA Supplement conducted systematic evaluations of the lag structure of associations for the PM2.5 -mortality relationship by examining either a series of single day or multiday lags and these studies continue to support an immediate effect ( i.e., lag 0 to 1 days) of short-term PM2.5 exposures on mortality (U.S. EPA, 2019a, section 11.1.8.1; U.S. EPA, 2022a, section 3.2.1.1). Recent studies also conducted analyses comparing the traditional 24-hour average exposure metric with a subdaily metric ( i.e., 1-hour max) and provide evidence of a similar pattern of associations for both the 24-hour average and 1-hour max metric, with the association larger in magnitude for the 24-hour average metric.
Multicity studies indicate that positive and statistically significant associations with mortality persist in analyses restricted to short-term (24-hour average PM2.5 concentrations) PM2.5 exposures below 35 μg/m[3] (Lee et al., 2015),[56] below 30 μg/m3 (Shi et al., 2016), and below 25 μg/m3 (Di et al., 2017a), indicating that risks associated with short-term PM2.5 exposures are not disproportionately driven by the peaks of the air quality distribution. Additional studies examined the shape of the C–R relationship for short-term PM2.5 exposure and mortality and whether a threshold exists below which mortality effects do not occur (U.S. EPA, 2019a, section 11.1.10). These studies used various statistical approaches and consistently demonstrate linear C–R relationships with no evidence of a threshold.
Moreover, recent studies evaluated in the ISA Supplement provide additional support for a linear, no-threshold C–R relationship between short-term PM2.5 exposure and mortality, with confidence in the shape decreasing at concentrations below 5 µg/m3 (Shi et al., 2016; Lavigne et al., 2018). Recent analyses provide initial evidence indicating that PM2.5 -mortality associations persist and may be stronger ( i.e., a steeper slope) at lower concentrations ( e.g., Di et al., 2017a; Figure 11–12 in U.S. EPA, 2019). However, given the limited data available at the lower end of the distribution of ambient PM2.5 concentrations, the shape of the C–R curve remains uncertain at these low concentrations. Although difficulties remain in assessing the shape of the short-term PM2.5 -mortality C–R relationship, to date, studies have not conducted systematic evaluations of alternatives to linearity and recent studies evaluated in the ISA Supplement continue to provide evidence of a no-threshold linear relationship, with less confidence at concentrations lower than 5 µg/m3 .
Overall, epidemiologic studies evaluated in the 2019 ISA and the ISA Supplement build upon and extend the conclusions of the 2009 ISA for the relationship between short-term PM2.5 exposures and total mortality. Supporting evidence for PM2.5 -related cardiovascular morbidity, and more limited evidence from respiratory morbidity, provide biological plausibility for mortality due to short-term PM2.5 exposures. The primarily positive associations observed across studies conducted in diverse geographic locations is further supported by the results from copollutant analyses indicating robust associations, along with evidence from analyses examining the C–R relationship. Overall, studies evaluated in the 2019 ISA support the conclusion of a causal relationship between short-term PM2.5 exposure and mortality, which is further supported by evidence from recent epidemiologic studies evaluated in the ISA Supplement (U.S. EPA, 2022a, section 3.2.1.4, p. 3–69).
ii. Cardiovascular Effects
Long-Term PM2.5 Exposures
The scientific evidence reviewed in the 2009 ISA was “sufficient to infer a causal relationship between long-term PM2.5 exposure and cardiovascular effects” (U.S. EPA, 2009a). The strongest line of evidence comprised findings from several large epidemiologic studies of U.S. and Canadian cohorts that reported consistent positive associations between long-term PM2.5 exposure and cardiovascular mortality (Pope et al., 2004; Krewski et al., 2009; Miller et al., Start Printed Page 16229 2007; Laden et al., 2006). Studies of long-term PM2.5 exposure and cardiovascular morbidity were limited in number. Biological plausibility and coherence with the epidemiologic findings were provided by studies using genetic mouse models of atherosclerosis demonstrating enhanced atherosclerotic plaque development and inflammation, as well as changes in measures of impaired heart function, following 4- to 6-month exposures to PM2.5 concentrated ambient particles (CAPs), and by a limited number of studies reporting CAPs-induced effects on coagulation factors, vascular reactivity, and worsening of experimentally induced hypertension in mice (U.S. EPA, 2009a).
Consistent with the evidence assessed in the 2009 ISA, the 2019 ISA concludes that recent studies, together with the evidence available in previous reviews, support a causal relationship between long-term exposure to PM2.5 and cardiovascular effects. Additionally, recent epidemiologic studies published since the completion of the 2019 ISA and evaluated in the ISA Supplement expands the body of evidence and further supports such a conclusion (U.S. EPA, 2022a). As discussed above (section II.A.2.a.i), results from U.S. and Canadian cohort studies evaluated in the 2019 ISA conducted at varying spatial and temporal scales and employing a variety of exposure assessment and statistical methods consistently report positive associations between long-term PM2.5 exposure and cardiovascular mortality (U.S. EPA, 2019, Figure 6–19, section 6.2.10). Positive associations between long-term PM2.5 exposures and cardiovascular mortality are generally robust in copollutant models adjusted for ozone, NO2, PM10–2.5, or SO2 . In addition, most of the results from analyses examining the shape of the C–R relationship between long-term PM2.5 exposures and cardiovascular mortality support a linear relationship and do not identify a threshold below which mortality effects do not occur (U.S. EPA, 2019a, section 6.2.16, Table 6–52).
The body of literature examining the relationship between long-term PM2.5 exposure and cardiovascular morbidity has greatly expanded since the 2009 ISA, with positive associations reported in several cohorts evaluated in the 2019 ISA (U.S. EPA, 2019a, section 6.2). Though results for cardiovascular morbidity are less consistent than those for cardiovascular mortality (U.S. EPA, 2019a, section 6.2), studies in the 2019 ISA and the ISA Supplement provide some evidence for associations between long-term PM2.5 exposures and the progression of cardiovascular disease. Positive associations with cardiovascular morbidity ( e.g., coronary heart disease, stroke, arrhythmias, myocardial infarction (MI), atherosclerosis progression) are observed in several epidemiologic studies (U.S. EPA, 2019a, sections 6.2.2 to 6.2.9; U.S. EPA, 2022a, section 3.1.2.2). Additionally, studies evaluated in the ISA Supplement report positive associations among those with pre-existing conditions, among patients followed after a cardiac event procedure, and among those with a first hospital admission for heart attacks among older adults enrolled in Medicare (U.S. EPA, 2022a, sections 3.1.1 and 3.1.2).
Recent studies published since the literature cutoff date of the 2019 ISA and evaluated in the ISA Supplement further assessed the relationship between long-term PM2.5 exposure and cardiovascular effects by conducting accountability analyses or by using alternative methods for confounder control in evaluating the association between long-term PM2.5 exposure and cardiovascular hospital admissions (U.S. EPA, 2022a, section 3.1.2.3). Studies that apply alternative methods for confounder control increase confidence in the relationship between long-term PM2.5 exposure and cardiovascular effects by using methods that reduce uncertainties related to potential confounding through statistical and/or study design approaches. For example, to control for potential confounding Wei et al. (2021) used a doubly robust additive model (DRAM) and found an association between long-term exposure to PM2.5 and cardiovascular effects, including MI, stoke, and atrial fibrillation, among the Medicare population. For example, an accountability study by Henneman et al. (2019) utilized a difference-in-difference (DID) approach to determine the relationship between coal-fueled power plant emissions and cardiovascular effects and found that reductions in PM2.5 concentrations resulted in reductions of cardiovascular-related hospital admissions. Furthermore, several recent epidemiologic studies evaluated in the ISA Supplement reported that the association between long-term PM2.5 exposure with stroke persisted after adjustment for NO2 but was attenuated in the model with O3 and oxidant gases represented by the redox weighted average of NO2 and O3 (U.S. EPA, 2022a, section 3.1.2.2.8). Overall, these studies report consistent findings that long-term PM2.5 exposure is related to increased hospital admissions for a variety of cardiovascular disease outcomes among large nationally representative cohorts and provide additional support for a relationship between long-term PM2.5 exposure and cardiovascular effects.
Positive associations reported in epidemiologic studies are supported by toxicological evidence evaluated in the 2019 ISA. The positive associations reported in epidemiologic studies are supported by toxicological evidence for increased plaque progression in mice following long-term exposure to PM2.5 collected from multiple locations across the U.S. (U.S. EPA, 2019a, section 6.2.4.2). A small number of epidemiologic studies also report positive associations between long-term PM2.5 exposure and heart failure, changes in blood pressure, and hypertension (U.S. EPA, 2019a, sections 6.2.5 and 6.2.7). Associations with heart failure are supported by animal toxicological studies demonstrating decreased cardiac contractility and function, and increased coronary artery wall thickness following long-term PM2.5 exposure (U.S. EPA, 2019a, section 6.2.5.2). Similarly, a limited number of animal toxicological studies demonstrating a relationship between long-term PM2.5 exposure and consistent increases in blood pressure in rats and mice are coherent with epidemiologic studies reporting positive associations between long-term exposure to PM2.5 and hypertension.
Additionally, a number of studies evaluated in the ISA Supplement focusing on morbidity outcomes, including those that focused on incidence of MI, atrial fibrillation (AF), stroke, and congestive heart failure (CHF), expand the evidence pertaining to the shape of the C–R relationship between long-term PM2.5 exposure and cardiovascular effects. These studies use statistical techniques that allow for departures from linearity (U.S. EPA, 2022a, Table 3–3), and generally support the evidence characterized in the 2019 ISA showing linear, no-threshold C–R relationship for most cardiovascular disease (CVD) outcomes. However, there is evidence for a sublinear or supralinear C–R relationship for some outcomes (U.S. EPA, 2022a, section 3.1.2.2.9).[57]
Longitudinal epidemiologic analyses also report positive associations with markers of systemic inflammation (U.S. EPA, 2019a, section 6.2.11), coagulation (U.S. EPA, 2019a, section 6.2.12), and Start Printed Page 16230 endothelial dysfunction (U.S. EPA, 2019a, section 6.2.13). These results are coherent with animal toxicological studies generally reporting increased markers of systemic inflammation, oxidative stress, and endothelial dysfunction (U.S. EPA, 2019a, section 6.2.12.2 and 6.2.14).
In summary, the 2019 ISA concludes that there is consistent evidence from multiple epidemiologic studies illustrating that long-term exposure to PM2.5 is associated with mortality from cardiovascular causes. Epidemiologic studies evaluated in the ISA Supplement provide additional evidence of positive associations between long-term PM2.5 exposure and cardiovascular morbidity (U.S. EPA, 2022a, section 3.1.2.2). Associations with coronary heart disease (CHD), stroke and atherosclerosis progression were observed in several additional epidemiologic studies, providing coherence with the mortality findings. Results from copollutant models generally support an independent effect of PM2.5 exposure on mortality. Additional evidence of the independent effect of PM2.5 on the cardiovascular system is provided by experimental studies in animals, which support the biological plausibility of pathways by which long-term exposure to PM2.5 could potentially result in outcomes such as CHD, stroke, CHF, and cardiovascular mortality. Overall, studies evaluated in the 2019 ISA support the conclusion of a causal relationship between long-term PM2.5 exposure and cardiovascular effects, which is supported and extended by evidence from recent epidemiologic studies evaluated in the ISA Supplement (U.S. EPA, 2022a, section 3.1.2.2).
Short-Term PM2.5 Exposures
The 2009 ISA concluded that “a causal relationship exists between short-term exposure to PM2.5 and cardiovascular effects” (U.S. EPA, 2009a). The strongest evidence in the 2009 ISA was from epidemiologic studies of emergency department (ED) visits and hospital admissions for IHD and heart failure (HF), with supporting evidence from epidemiologic studies of cardiovascular mortality (U.S. EPA, 2009a). Animal toxicological studies provided coherence and biological plausibility for the positive associations reported with MI, ED visits, and hospital admissions. These included studies reporting reduced myocardial blood flow during ischemia and studies indicating altered vascular reactivity. In addition, effects of PM2.5 exposure on a potential indicator of ischemia ( i.e., ST segment depression on an electrocardiogram) were reported in both animal toxicological and epidemiologic panel studies.[58] Key uncertainties from the last review resulted from inconsistent results across disciplines with respect to the relationship between short-term exposure to PM2.5 and changes in blood pressure, blood coagulation markers, and markers of systemic inflammation. In addition, while the 2009 ISA identified a growing body of evidence from controlled human exposure and animal toxicological studies, uncertainties remained with respect to biological plausibility.
Studies evaluated in the 2019 ISA provide additional support for a causal relationship between short-term PM2.5 exposure and cardiovascular effects. This includes generally positive associations observed in multicity epidemiologic studies of emergency department visits and hospital admissions for IHD, heart failure (HF), and combined cardiovascular-related endpoints. In particular, nationwide studies of older adults (65 years and older) using Medicare records report positive associations between PM2.5 exposures and hospital admissions for HF (U.S. EPA, 2019a, section 6.1.3.1). Moreover, recent multicity studies, published after the literature cutoff date of the 2019 ISA and evaluated in the ISA Supplement, are consistent with studies evaluated in the 2019 ISA that report positive association between short-term PM2.5 exposure and ED visits and hospital admission for IHD, heart attacks, and HF (U.S. EPA, 2022a, section 3.1). Epidemiologic studies conducted in single cities contribute some support to the causality determination, though associations reported in single-city studies are less consistently positive than in multicity studies, and include a number of studies reporting null associations (U.S. EPA, 2019a, sections 6.1.2 and 6.1.3). As a whole, though, the recent body of IHD and HF epidemiologic evidence supports the evidence from previous ISAs reporting mainly positive associations between short-term PM2.5 concentrations and emergency department visits and hospital admissions.
Consistent with the evidence assessed in the 2019 ISA, some studies evaluated in the ISA Supplement report no evidence of an association with stroke, regardless of stroke subtype. Additionally, as in the 2019 ISA, evidence evaluated in the ISA Supplement continues to indicate an immediate effect of PM2.5 on cardiovascular-related outcomes primarily within the first few days after exposure, and that associations generally persisted in models adjusted for copollutants (U.S. EPA, 2022a, section 3.1.1.2).
The ISA Supplement includes additional epidemiologic studies, published since the literature cutoff date for the 2019 ISA, including accountability analyses and epidemiologic studies that employ alternative methods for confounder control to evaluate the association between short-term PM2.5 exposure and cardiovascular-related effects (U.S. EPA, 2022a, section 3.1.1.3). These studies employ a number of statistical approaches and report positive associations, providing additional support for a relationship between short-term PM2.5 exposure and cardiovascular effects, while also reducing uncertainties related to potential confounder bias.
A number of controlled human exposure, animal toxicological, and epidemiologic panel studies provide evidence that PM2.5 exposure could plausibly result in IHD or HF through pathways that include endothelial dysfunction, arterial thrombosis, and arrhythmia (U.S. EPA, 2019a, section 6.1.1). The most consistent evidence from recent controlled human exposure studies is for endothelial dysfunction, as measured by changes in brachial artery diameter or flow mediated dilation. Multiple controlled human exposure studies that examined the potential for endothelial dysfunction report an effect of PM2.5 exposure on measures of blood flow (U.S. EPA, 2019a, section 6.1.13.2). However, these studies report variable results regarding the timing of the effect and the mechanism by which reduced blood flow occurs ( i.e., availability vs sensitivity to nitric oxide). In addition, some controlled human exposure studies using CAPs report evidence for small increases in blood pressure (U.S. EPA, 2019a, section 6.1.6.3). Although not entirely consistent, there is also some evidence across controlled human exposure studies for conduction abnormalities/arrhythmia (U.S. EPA, 2019a, section 6.1.4.3), changes in heart rate variability (HRV) (U.S. EPA, 2019a, section 6.1.10.2), changes in hemostasis that could promote clot formation (U.S. EPA, 2019a, section 6.1.12.2), and increases in inflammatory cells and markers (U.S. EPA, 2019a, section 6.1.11.2). A recent study by Wyatt et al. Start Printed Page 16231 (2020), evaluated in the ISA Supplement, adds to the limited evidence base of controlled human exposure studies conducted at near ambient PM2.5 concentrations. The study, completed in healthy young adults subject to intermittent exercise, found some significant cardiovascular effects ( e.g., systematic inflammation markers, including C-reactive protein (CRP), and cardiac repolarization). Thus, when taken as a whole, controlled human exposure studies are coherent with epidemiologic studies in that they demonstrate that short-term exposures to PM2.5 may result in the types of cardiovascular endpoints that could lead to emergency department visits and hospital admissions for IHD or HF, as well as mortality in some people.
Animal toxicological studies published since the 2009 ISA and evaluated in the 2019 ISA also support a relationship between short-term PM2.5 exposure and cardiovascular effects. A study demonstrating decreased cardiac contractility and left ventricular pressure in mice is coherent with the results of epidemiologic studies that report associations between short-term PM2.5 exposure and heart failure (U.S. EPA, 2019a, section 6.1.3.3). In addition, and as with controlled human exposure studies, there is generally consistent evidence in animal toxicological studies for indicators of endothelial dysfunction (U.S. EPA, 2019a, section 6.1.13.3). Some studies in animals also provide evidence for changes in a number of other cardiovascular endpoints following short-term PM2.5 exposure including conduction abnormalities and arrhythmia (U.S. EPA, 2019a, section 6.1.4.4), changes in HRV (U.S. EPA, 2019a, section 6.1.10.3), changes in blood pressure (U.S. EPA, 2019a, section 6.1.6.4), and evidence for systemic inflammation and oxidative stress (U.S. EPA, 2019a, section 6.1.11.3).
In summary, evidence evaluated in the 2019 ISA extends the consistency and coherence of the evidence base evaluated in the 2009 ISA and prior assessments. Epidemiologic studies reporting robust associations in copollutant models are supported by direct evidence from controlled human exposure and animal toxicologic studies reporting independent effects of PM2.5 exposures on endothelial dysfunction as well as endpoints indicating impaired cardiac function, increased risk of arrhythmia, changes in HRV, increases in BP, and increases in indicators of systemic inflammation, oxidative stress, and coagulation (U.S. EPA, 2019, section 6.1.16). For some cardiovascular effects, there are inconsistencies in results across some animal toxicological, controlled human exposure, and epidemiologic panel studies, though this may be due to substantial differences in study design and/or study populations. Overall, the results from epidemiologic panel, controlled human exposure, and animal toxicological studies, in particular those related to endothelial dysfunction, impaired cardiac function, ST segment depression, thrombosis, conduction abnormalities, and changes in blood pressure provide coherence and biological plausibility for the consistent results from epidemiologic studies observing positive associations between short-term PM2.5 exposures and IHD and HF, and ultimately cardiovascular mortality. Overall, studies evaluated in the 2019 ISA support the conclusion of a causal relationship between short-term PM2.5 exposure and cardiovascular effects, which is supported and extended by evidence from recent epidemiologic studies evaluated in the ISA Supplement (U.S. EPA, 2022a, section 3.1.1.4).
iii. Respiratory Effects
Long-Term PM2.5 Exposures
The 2009 ISA concluded that “a causal relationship is likely to exist between long-term PM2.5 exposure and respiratory effects” (U.S. EPA, 2009a). This conclusion was based mainly on epidemiologic evidence demonstrating associations between long-term PM2.5 exposure and changes in lung function or lung function growth in children. Biological plausibility was provided by a single animal toxicological study examining pre- and post-natal exposure to PM2.5 CAPs, which found impaired lung development. Epidemiologic evidence for associations between long-term PM2.5 exposure and other respiratory outcomes, such as the development of asthma, allergic disease, and COPD; respiratory infection; and the severity of disease was limited, both in the number of studies available and the consistency of the results. Experimental evidence for other outcomes was also limited, with one animal toxicological study reporting that long-term exposure to PM2.5 CAPs results in morphological changes in nasal airways of healthy animals. Other animal studies examined exposure to mixtures, such as motor vehicle exhaust and woodsmoke, and effects were not attributed specifically to the particulate components of the mixture.
Cohort studies evaluated in the 2019 ISA provided additional support for the relationship between long-term PM2.5 exposure and decrements in lung function growth (as a measure of lung development), indicating a robust and consistent association across study locations, exposure assessment methods, and time periods (U.S. EPA, 2019a, section 5.2.13). This relationship was further supported by a retrospective study that reports an association between declining PM2.5 concentrations and improvements in lung function growth in children (U.S. EPA, 2019a, section 5.2.11). Epidemiologic studies also examine asthma development in children (U.S. EPA, 2019a, section 5.2.3), with prospective cohort studies reporting generally positive associations, though several are imprecise ( i.e., they report wide confidence intervals). Supporting evidence is provided by studies reporting associations with asthma prevalence in children, with childhood wheeze, and with exhaled nitric oxide, a marker of pulmonary inflammation (U.S. EPA, 2019a, section 5.2.13). Additionally, the 2019 ISA includes an animal toxicological study showing the development of an allergic phenotype and an increase in a marker of airway responsiveness supports the biological plausibility of the development of allergic asthma (U.S. EPA, 2019a, section 5.2.13). Other epidemiologic studies report a PM2.5 -related acceleration of lung function decline in adults, while improvement in lung function was observed with declining PM2.5 concentrations (U.S. EPA, 2019a, section 5.2.11). A longitudinal study found declining PM2.5 concentrations are also associated with an improvement in chronic bronchitis symptoms in children, strengthening evidence reported in the 2009 ISA for a relationship between increased chronic bronchitis symptoms and long-term PM2.5 exposure (U.S. EPA, 2019a, section 5.2.11). A common uncertainty across the epidemiologic evidence is the lack of examination of copollutants to assess the potential for confounding. While there is some evidence that associations remain robust in models with gaseous pollutants, a number of these studies examining copollutant confounding were conducted in Asia, and thus have limited generalizability due to high annual pollutant concentrations.
When taken together, the 2019 ISA concludes that the epidemiologic evidence strongly supports a relationship with decrements in lung function growth asthma development in children, as well as increased bronchitis symptoms in children with asthma. Additionally, the epidemiologic Start Printed Page 16232 evidence strongly supports a relationship with an acceleration of lung function decline in adults, and with respiratory mortality and cause-specific respiratory mortality for COPD and respiratory infection (U.S. EPA, 2019a, p. 1–34). In support of the biological plausibility of associations reported in epidemiologic studies associated with respiratory health effects, animal toxicological studies evaluated in the 2019 ISA continue to provide direct evidence that long-term exposure to PM2.5 results in a variety of respiratory effects, including pulmonary oxidative stress, inflammation, and morphologic changes in the upper (nasal) and lower airways. Other results show that changes are consistent with the development of allergy and asthma, and with impaired lung development. Overall, the 2019 ISA concludes that “the collective evidence is sufficient to conclude that a causal relationship is likely to exist between long-term PM2.5 exposure and respiratory effects” (U.S. EPA, 2019a, section 5.2.13).
Short-Term PM2.5 Exposures
The 2009 ISA (U.S. EPA, 2009a) concluded that a “causal relationship is likely to exist” between short-term PM2.5 exposure and respiratory effects. This conclusion was based mainly on the epidemiologic evidence demonstrating positive associations with various respiratory effects. Specifically, the 2009 ISA described epidemiologic evidence as consistently showing PM2.5 -associated increases in hospital admissions and ED visits for COPD and respiratory infection among adults or people of all ages, as well as increases in respiratory mortality. These results were supported by studies reporting associations with increased respiratory symptoms and decreases in lung function in children with asthma, though the epidemiologic evidence was inconsistent for hospital admissions or emergency department visits for asthma. Studies examining copollutant models showed that PM2.5 associations with respiratory effects were robust to inclusion of CO or SO2 in the model, but often were attenuated (though still positive) with inclusion of O3 or NO2 . In addition to the copollutant models, evidence supporting an independent effect of PM2.5 exposure on the respiratory system was provided by animal toxicological studies of PM2.5 CAPs demonstrating changes in some pulmonary function parameters, as well as inflammation, oxidative stress, injury, enhanced allergic responses, and reduced host defenses. Many of these effects have been implicated in the pathophysiology for asthma exacerbation, COPD exacerbation, or respiratory infection. In the few controlled human exposure studies conducted in individuals with asthma or COPD, PM2.5 exposure mostly had no effect on respiratory symptoms, lung function, or pulmonary inflammation. Available studies in healthy people also did not clearly demonstrate respiratory effects following short-term PM2.5 exposures.
Epidemiologic studies evaluated in the 2019 ISA continue to provide strong evidence for a relationship between short-term PM2.5 exposure and several respiratory-related endpoints, including asthma exacerbation (U.S. EPA, 2019a, section 5.1.2.1), COPD exacerbation (U.S. EPA, 2019a, section 5.1.4.1), and combined respiratory-related diseases (U.S. EPA, 2019a, section 5.1.6), particularly from studies examining ED visits and hospital admissions. The generally positive associations between short-term PM2.5 exposure and asthma and COPD as well as ED visits and hospital admissions are supported by epidemiologic studies demonstrating associations with other respiratory-related effects such as symptoms and medication use that are indicative of asthma and COPD exacerbations (U.S. EPA, 2019a, sections 5.1.2.2 and 5.4.1.2). The collective body of epidemiologic evidence for asthma exacerbation is more consistent in children than in adults. Additionally, epidemiologic studies examining the relationship between short-term PM2.5 exposure and respiratory mortality provide evidence of consistent positive associations, demonstrating a continuum of effects (U.S. EPA, 2019a, section 5.1.9).
Epidemiologic studies evaluated in the 2019 ISA expand the assessment of potential copollutant confounding evaluated in the 2009 ISA. There is some evidence that PM2.5 associations with asthma exacerbation, combined respiratory-related diseases, and respiratory mortality remain relatively unchanged in copollutant models with gaseous pollutants including O3, NO2, SO2, and with more limited evidence for CO, as well as other particle sizes ( i.e., PM10–2.5) (U.S. EPA, 2019a, section 5.1.10.1).
Insight into whether there is an independent effect of PM2.5 on respiratory health is also partially addressed by findings from animal toxicological studies evaluated in the 2019 ISA. Specifically, short-term exposure to PM2.5 enhanced asthma-related responses in an animal model of allergic airways disease and enhanced lung injury and inflammation in an animal model of COPD (U.S. EPA, 2019a, sections 5.1.2.4.4 and 5.1.4.4.3). The experimental evidence provides biological plausibility for some respiratory-related endpoints, including limited evidence of altered host defense and greater susceptibility to bacterial infection as well as consistent evidence of respiratory irritant effects. However, animal toxicological evidence for other respiratory effects is inconsistent. A recent study evaluated in the ISA supplement by Wyatt et al. (2020) and conducted at near ambient PM2.5 concentrations, adds to the limited evidence base of controlled human exposure studies. The study, completed in healthy young adults subject to intermittent exercise, found some significant respiratory effects (including decrease in lung function), however these findings were inconsistent with the controlled human exposure studies evaluated in the 2019 ISA (U.S. EPA, 2019a, section 5.1.7.2, 5.1.2.3, and 6.1.11.2.1).
The 2019 ISA concludes that “[t]he strongest evidence of an effect of short-term PM2.5 exposure on respiratory effects is provided by epidemiologic studies of asthma and COPD exacerbation. While animal toxicological studies provide biological plausibility for these findings, some uncertainty remains with respect to the independence of PM2.5 effects” (U.S. EPA, 2019a, p. 5–155). When taken together, the 2019 ISA concludes that this evidence “is sufficient to conclude that a causal relationship is likely to exist between short-term PM2.5 exposure and respiratory effects” (U.S. EPA, 2019a, p. 5–155).
iv. Cancer
The 2009 ISA concluded that the overall body of evidence was “suggestive of a causal relationship between relevant PM2.5 exposures and cancer” (U.S. EPA, 2009a). This conclusion was based primarily on positive associations observed in a limited number of epidemiologic studies of lung cancer mortality. The few epidemiologic studies that had evaluated PM2.5 exposure and lung cancer incidence or cancers of other organs and systems generally did not show evidence of an association. Toxicological studies did not focus on exposures to specific PM size fractions, but rather investigated the effects of exposures to total ambient PM, or other source-based PM such as wood smoke. Collectively, results of in vitro studies were consistent with the larger body of evidence demonstrating that ambient PM and PM from specific combustion sources are mutagenic and genotoxic. However, animal inhalation studies Start Printed Page 16233 found little evidence of tumor formation in response to chronic exposures. A small number of studies provided preliminary evidence that PM exposure can lead to changes in methylation of DNA, which may contribute to biological events related to cancer.
Since the completion of the 2009 ISA, additional cohort studies provide evidence that long-term PM2.5 exposure is positively associated with lung cancer mortality and with lung cancer incidence, and provide initial evidence for an association with reduced cancer survival (U.S. EPA, 2019a, section 10.2.5). Re-analyses of the ACS cohort using different years of PM2.5 data and follow up, along with various exposure assignment approaches, provide consistent evidence of positive associations between long-term PM2.5 exposure and lung cancer mortality (U.S. EPA, 2019a, Figure 10–3). Additional support for positive associations with lung cancer mortality is provided by recent epidemiologic studies using individual level data to control for smoking status, as well as by studies of people who have never smoked (though such studies generally report wide confidence intervals due to the small number of lung cancer mortality cases within this population), and in additional analyses of cohorts that relied upon proxy measures to account for smoking status (U.S. EPA, 2019a, section 10.2.5.1.1). Although studies that evaluate lung cancer incidence, including studies of people who have never smoked, are limited in number, studies in the 2019 ISA generally report positive associations with long-term PM2.5 exposures (U.S. EPA, 2019a, section 10.2.5.1.2). A subset of the studies focusing on lung cancer incidence also examined histological subtype, providing some evidence of positive associations for adenocarcinomas, the predominate subtype of lung cancer observed in people who have never smoked (U.S. EPA, 2019a, section 10.2.5.1.2). Associations between long-term PM2.5 exposure and lung cancer incidence were found to remain relatively unchanged, though in some cases confidence intervals widened, in analyses that attempted to reduce exposure measurement error by accounting for length of time at residential address or by examining different exposure assignment approaches (U.S. EPA, 2019a, section 10.2.5.1.2).
To date, relatively few studies have evaluated the potential for copollutant confounding of the relationship between long-term PM2.5 exposure and lung cancer mortality or incidence. A small number of such studies have generally focused on O3 and report that PM2.5 associations remain relatively unchanged in copollutant models (U.S. EPA, 2019a, section 10.2.5.1.3). However, available studies have not systematically evaluated the potential for copollutant confounding by other gaseous pollutants or by other particle size fractions (U.S. EPA, 2019a, section 10.2.5.1.3).
Compared to total (non-accidental) mortality (U.S. EPA, 2019a, section 10.2.4.1.4), fewer studies have examined the shape of the C–R curve for cause-specific mortality outcomes, including lung cancer. Several studies of lung cancer mortality and incidence have reported no evidence of deviations from linearity in the shape of the C–R relationship (Lepeule et al., 2012; Raaschou-Nielsen et al., 2013; Puett et al., 2014), though authors provided only limited discussions of results (U.S. EPA, 2019a, section 10.2.5.1.4).
In support of the biological plausibility of an independent effect of PM2.5 on lung cancer, the 2019 ISA notes evidence from experimental and epidemiologic studies demonstrating that PM2.5 exposure can lead to a range of effects indicative of mutagenicity, genotoxicity, and carcinogenicity, as well as epigenetic effects (U.S. EPA, 2019a, section 10.2.7). For example, both in vitro and in vivo toxicological studies have shown that PM2.5 exposure can result in DNA damage (U.S. EPA, 2019a, section 10.2.2). Although such effects do not necessarily equate to carcinogenicity, the evidence that PM exposure can damage DNA, and elicit mutations, provides support for the plausibility of epidemiologic associations exhibited with lung cancer mortality and incidence. Additional supporting studies indicate the occurrence of micronuclei formation and chromosomal abnormalities (U.S. EPA, 2019a, section 10.2.2.3), and differential expression of genes that may be relevant to cancer pathogenesis, following PM2.5 exposures. Experimental and epidemiologic studies that examine epigenetic effects indicate changes in DNA methylation, providing some support that PM2.5 exposure contributes to genomic instability (U.S. EPA, 2019a, section 10.2.3). Overall, there is limited evidence that long-term PM2.5 exposure is associated with cancers in other organ systems, though there is some evidence that PM2.5 exposure may reduce survival in individuals with cancer (U.S. EPA, 2019a, section 10.2.7; U.S. EPA, 2022a, section 2.1.1.4.1).
Epidemiologic evidence for associations between PM2.5 and lung cancer mortality and incidence, together with evidence supporting the biological plausibility of such associations, contributes to the 2019 ISA's conclusion that the evidence “is sufficient to conclude that a causal relationship is likely to exist between long-term PM2.5 exposure and cancer” (U.S. EPA, 2019, section 10.2.7).
v. Nervous System Effects
Reflecting the very limited evidence available in the 2012 review, the 2009 ISA did not make a causality determination for long-term PM2.5 exposures and nervous system effects (U.S. EPA, 2009c). Since the 2012 review, this body of evidence has grown substantially (U.S. EPA, 2019, section 8.2). Animal toxicological studies assessed in in the 2019 ISA report that long-term PM2.5 exposures can lead to morphologic changes in the hippocampus and to impaired learning and memory. This evidence is consistent with epidemiologic studies reporting that long-term PM2.5 exposure is associated with reduced cognitive function (U.S. EPA, 2019a, section 8.2.5). Further, while the evidence is limited, the presence of early markers of Alzheimer's disease pathology has been demonstrated in rodents following long-term exposure to PM2.5 CAPs. These findings support reported associations with neurodegenerative changes in the brain ( i.e., decreased brain volume), all-cause dementia, or hospitalization for Alzheimer's disease in a small number of epidemiologic studies (U.S. EPA, 2019a, section 8.2.6). Additionally, loss of dopaminergic neurons in the substantia nigra, a hallmark of Parkinson disease, has been reported in mice (U.S. EPA, 2019a, section 8.2.4), though epidemiologic studies provide only limited support for associations with Parkinson's disease (U.S. EPA, 2019a, section 8.2.6). Overall, the lack of consideration of copollutant confounding introduces some uncertainty in the interpretation of epidemiologic studies of nervous system effects, but this uncertainty is partly addressed by the evidence for an independent effect of PM2.5 exposures provided by experimental animal studies.
While the findings described above are most relevant to older adults, several studies of neurodevelopmental effects in children have also been conducted. Epidemiologic studies provided limited evidence of an association between PM2.5 exposure during pregnancy and childhood on cognitive and motor development (U.S. EPA, 2019, section 8.2.5.2). While some studies report positive associations between long-term Start Printed Page 16234 exposure to PM2.5 during the prenatal period and autism spectrum disorder (ASD) (U.S. EPA, 2019, section 8.2.7.2), the interpretation of these epidemiologic studies is limited due to the small number of studies, their lack of control for potential confounding by copollutants, and uncertainty related to the critical exposure windows. Biological plausibility is provided for the ASD findings by a study in mice that found inflammatory and morphologic changes in the corpus collosum and hippocampus, as well as ventriculomegaly ( i.e., enlarged lateral ventricles) in young mice following prenatal exposure to PM2.5 CAPs.
Taken together, the 2019 ISA concludes that studies indicate long-term PM2.5 exposures can lead to effects on the brain associated with neurodegeneration ( i.e., neuroinflammation and reductions in brain volume), as well as cognitive effects in older adults (U.S. EPA, 2019a, Table 1–2). Animal toxicological studies provide evidence for a range of nervous system effects in adult animals, including neuroinflammation and oxidative stress, neurodegeneration, cognitive effects, and effects on neurodevelopment in young animals. The epidemiologic evidence is more limited, but studies generally support associations between long-term PM2.5 exposure and changes in brain morphology, cognitive decrements and dementia. There is also initial, and limited, evidence for neurodevelopmental effects, particularly ASD. The consistency and coherence of the evidence supports the 2019 ISA's conclusion that “the collective evidence is sufficient to conclude that a causal relationship is likely to exist between long-term PM2.5 exposure and nervous system effects” (U.S. EPA, 2019a, section 8.2.9).
vi. Other Effects
For other health effect categories that were evaluated for their relationship with PM2.5 exposures ( i.e., short-term PM2.5 exposure and nervous system effects and short- and long-term PM2.5 exposure and metabolic effects, reproduction and fertility, and pregnancy and birth outcomes (U.S. EPA, 2022a, Table ES–1), the currently available evidence is “suggestive of, but not sufficient to infer, a causal relationship,” mainly due to inconsistent evidence across specific outcomes and uncertainties regarding exposure measurement error, the potential for confounding, and potential modes of action (U.S. EPA, 2019a, sections 7.14, 7.2.10, 8.1.6, and 9.1.5). The causality determination for short-term PM2.5 exposure and nervous system effects in the 2019 ISA reflects a revision to the causality determination in the 2009 ISA from “inadequate to infer a causal relationship,” while this is the first-time assessments of causality were conducted for long-term PM2.5 exposure and nervous system effects, as well as short- and long-term PM2.5 exposure and metabolic effects reflect.
Recent studies evaluated in the 2019 ISA also further explored the relationship between short-and long-term UFP exposure and health effects. ( i.e., cardiovascular effects and short-term UFP exposures; respiratory effects and short-term UFP exposures; and nervous system effects and long- and short-term exposures (U.S. EPA, 2022a, Table ES–1). The currently available evidence is “suggestive of, but not sufficient to infer, a causal relationship” for short-term UFP exposure and cardiovascular and respiratory effects and for short- and long-term UFP exposure and nervous system effects, primarily due to uncertainties and limitations in the evidence, specifically, variability across studies in the definition of UFPs and the exposure metric used (U.S. EPA, 2019a, P.3.1; U.S. EPA, 2022a, section 3.3.1.6.3). The causality determinations for the other health effect categories evaluated in the 2019 ISA are “inadequate to infer a causal relationship.” Additionally, this is the first time assessments of causality were conducted for short- and long-term UFP exposure and metabolic effects and long-term UFP exposure and nervous system effects (U.S. EPA, 2022a, Table ES–1).
With the advent of the global COVID–19 pandemic, a number of recent studies evaluated in the ISA Supplement examined the relationship between ambient air pollution, specifically PM2.5 , and SARS–CoV–2 infections and COVID–19 deaths, including a few studies within the U.S. and Canada (U.S. EPA, 2022a, section 3.3.2).[59] Some studies examined whether daily changes in PM2.5 can influence SARS–CoV–2 infection and COVID–19 death (U.S. EPA, 2022a, section 3.3.2.1). Additionally, several studies evaluated whether long-term PM2.5 exposure increases the risk of SARS–CoV–2 infection and COVID–19 death in North America (U.S. EPA, 2022a, section 3.3.2.2). While there is initial evidence of positive associations with SARS–CoV–2 infection and COVID–19 death, uncertainties remain due to methodological issues that may influence the results, including: (1) The use of ecological study design; (2) studies were conducted during the ongoing pandemic when the etiology of COVID–19 was still not well understood ( e.g., specifically, there are important differences in COVID–19-related outcomes by a variety of factors such as race and SES); and (3) studies did not account for crucial factors that could influence results ( e.g., stay-at-home orders, social distancing, use of masks, and testing capacity) (U.S. EPA, 2022a, chapter 5). Taken together, while there is initial evidence of positive associations with SARS–CoV–2 infection and COVID–19 death, uncertainties remain due to methodological issues.
b. Public Health Implications and At-Risk Populations
The public health implications of the evidence regarding PM2.5 -related health effects, as for other effects, are dependent on the type and severity of the effects, as well as the size of the population affected. Such factors are discussed below in the context of our consideration of the health effects evidence related to PM2.5 in ambient air. This section also summarizes the current information on population groups at increased risk of the effects of PM2.5 in ambient air.
The information available in this reconsideration has not altered our understanding of human populations at risk of health effects from PM2.5 exposures. As recognized in the 2020 review, the 2019 ISA cites extensive evidence indicating that “both the general population as well as specific populations and lifestages are at risk for PM2.5 -related health effects” (U.S. EPA, 2019a, p. 12–1). Factors that may contribute to increased risk of PM2.5 -related health effects include lifestage (children and older adults), pre-existing diseases (cardiovascular disease and Start Printed Page 16235 respiratory disease), race/ethnicity, and SES.[60]
Children make up a substantial fraction of the U.S. population, and often have unique factors that contribute to their increased risk of experiencing a health effect due to exposures to ambient air pollutants because of their continuous growth and development.[61] Children may be particularly at risk for health effects related to ambient PM2.5 exposures compared with adults because they have (1) a developing respiratory system, (2) increased ventilation rates relative to body mass compared with adults, and (3) an increased proportion of oral breathing, particularly in boys, relative to adults (U.S. EPA, 2019a, section 12.5.1.1). There is strong evidence that demonstrates PM2.5 associated health effects in children, particularly from epidemiologic studies of long-term PM2.5 exposure and impaired lung function growth, decrements in lung function, and asthma development. However, there is limited evidence from stratified analyses that children are at increased risk of PM2.5 -related health effects compared to adults. Additionally, there is some evidence that indicates that children receive higher PM2.5 exposures than adults, and dosimetric differences in children compared to adults can contribute to higher doses (U.S. EPA, 2019a, section 12.5.1.1).
In the U.S., older adults, often defined as adults 65 years of age and older, represent an increasing portion of the population and often have pre-existing diseases or conditions that may compromise biological function. While there is limited evidence to indicate that older adults have higher exposures than younger adults, older adults may receive higher doses of PM2.5 due to dosimetric differences. There is consistent evidence from studies of older adults demonstrating generally consistent positive associations in studies examining health effects from short- and long-term PM2.5 exposure and cardiovascular or respiratory hospital admissions, emergency department visits, or mortality (U.S. EPA, 2019a, sections 6.1, 6.2, 11.1, 11.2, 12.5.1.2). Additionally, several animal toxicological, controlled human exposure, and epidemiologic studies did not stratify results by lifestage, but instead focused the analyses on older individuals, and can provide coherence and biological plausibility for the occurrence among this lifestage (U.S. EPA, 2019a, section 12.5.1.2).
Individuals with pre-existing disease may be considered at greater risk of an air pollution-related health effect than those without disease because they are likely in a compromised biological state that can vary depending on the disease and severity. With regard to cardiovascular disease, we first note that cardiovascular disease is the leading cause of death in the U.S., accounting for one in four deaths, and approximately 12% of the adult population in the U.S. has a cardiovascular disease (U.S. EPA, 2019a, section 12.3.1). Strong evidence demonstrates that there is a causal relationship between cardiovascular effects and long- and short-term exposures to PM2.5 . Some of the evidence supporting this conclusion is from studies of panels or cohorts with pre-existing cardiovascular disease, which provide supporting evidence but do not directly demonstrate an increased risk (U.S. EPA, 2019a, section 12.3.1). Epidemiologic evidence indicates that individuals with pre-existing cardiovascular disease may be at increased risk for PM2.5 -associated health effects compared to those without pre-existing cardiovascular disease. While the evidence does not consistently support increased risk for all pre-existing cardiovascular diseases, there is evidence that certain pre-existing cardiovascular diseases ( e.g., hypertension) may be a factor that increases PM2.5 -related risk. Furthermore, there is strong evidence supporting a causal relationship for long- and short-term PM2.5 exposure and cardiovascular effects, particularly for IHD (U.S. EPA, 2019a, chapter 6, section 12.3.1).
With regard to respiratory disease, we first note that the most chronic respiratory diseases in the U.S. are asthma and COPD. Asthma affects a substantial fraction of the U.S. population and is the leading chronic disease among children. COPD primarily affects older adults and contributes to compromised respiratory function and underlying pulmonary inflammation. The body of evidence indicates that individuals with pre-existing respiratory diseases, particularly asthma and COPD, may be at increased risk for PM2.5 -related health effects compared to those without pre-existing respiratory diseases (U.S. EPA, 2019a, section 12.3.5). There is strong evidence indicating PM2.5 -associated respiratory effects among those with asthma, which forms the primary evidence base for the likely to be causal relationship between short-term exposures to PM2.5 and respiratory health effects (U.S. EPA, 2019a, section 12.3.5). For asthma, epidemiologic evidence demonstrates associations between short-term PM2.5 exposures and respiratory effects, particularly evidence for asthma exacerbation, and controlled human exposure and animal toxicological studies demonstrate support for the biological plausibility for asthma exacerbation with PM2.5 exposures (U.S. EPA, 2019a, section 12.3.5.1). For COPD, epidemiologic studies report positive associations between short-term PM2.5 exposures and hospital admissions and emergency department visits for COPD, with supporting evidence from panel studies demonstration COPD exacerbation. Epidemiologic evidence is supported by some experimental evidence of COPD-related effects, which provides support for the biological plausibility for COPD in response to PM2.5 exposures (U.S. EPA, 2019a, section 12.3.5.2).
There is strong evidence for racial and ethnic disparities in PM2.5 exposures and PM2.5 -related health risk, as assessed in the 2019 ISA and with even more evidence available since the literature cutoff date for the 2019 ISA and evaluated in the ISA Supplement. There is strong evidence demonstrating that Black and Hispanic populations, in particular, have higher PM2.5 exposures than non-Hispanic White populations (U.S. EPA, 2019a, Figure 12–2; U.S. EPA, 2022a, Figure 3–38). Black populations or individuals that live in predominantly Black neighborhoods experience higher PM2.5 exposures, in comparison to non-Hispanic White populations. There is also consistent evidence across multiple studies that demonstrate increased risk of PM2.5 -related health effects, with the strongest evidence for health risk disparities for mortality (U.S. EPA, 2019a, section 12.5.4). There is also evidence of health risk disparities for both Hispanic and non-Hispanic Black populations compared to non-Hispanic White populations for cause-specific mortality and incident hypertension (U.S. EPA, 2022a, section 3.3.3.2).
Socioeconomic status (SES) is a composite measure that includes metrics such as income, occupation, or education, and can play a role in access to healthy environments as well as access to healthcare. SES may be a factor that contributes to differential risk from PM2.5 -related health effects. Studies assessed in the 2019 ISA and ISA Supplement provide evidence that lower SES communities are exposed to higher concentrations of PM2.5Start Printed Page 16236 compared to higher SES communities (U.S. EPA, 2019a, section 12.5.3; U.S. EPA, 2022a, section 3.3.3.1.1). Studies using composite measures of neighborhood SES consistently demonstrated a disparity in both PM2.5 exposure and the risk of PM2.5 -related health outcomes. There is some evidence that supports associations larger in magnitude between mortality and long-term PM2.5 exposures for those with low income or living in lower income areas compared to those with higher income or living in higher income neighborhoods (U.S. EPA, 2019a, section 12.5.3; U.S. EPA, 2022a, section 3.3.3.1.1). Additionally, evidence supports conclusions that lower SES is associated with cause-specific mortality and certain health endpoints ( i.e., HI and CHF), but less so for all-cause or total (non-accidental) mortality (U.S. EPA, 2022a, section 3.3.3.1).
The magnitude and characterization of a public health impact is dependent upon the size and characteristics of the populations affected, as well as the type or severity of the effects. As summarized above, lifestage (children and older adults), race/ethnicity and SES are factors that increase the risk of PM2.5 -related health effects. The American Community Survey (ACS) for 2019 estimates that approximately 22% and 16% of the U.S. population are children (age<18) and older adults (age 65+), respectively. For all ages, non-Hispanic Black and Hispanic populations comprise approximately 12% and 18% of the overall U.S. population in 2019. Currently available information that helps to characterize key features of these population is included in the 2022 PA (U.S. EPA, 2022b, Table 3–2).
As noted above, individuals with pre-existing cardiovascular disease and pre-existing respiratory disease may also be at increased risk of PM2.5 -related health effects. Currently available information that helps to characterize key features of populations with cardiovascular or respiratory diseases or conditions is included in the 2022 PA (U.S. EPA, 2022b, Table 3–3). The National Center for Health Statistics data for 2018 indicate that, for adult populations, older adults ( e.g., those 65 years and older) have a higher prevalence of cardiovascular diseases compared to younger adults ( e.g., those 64 years and younger). For respiratory diseases, older adults also have a higher prevalence of emphysema than younger adults, and adults 44 years or older have a higher prevalence of chronic bronchitis. However, the prevalence for asthma is generally similar across all adult age groups.
With respect to race, American Indians or Alaskan Native populations have the highest prevalence of all heart disease and coronary heart disease, while Black populations have the highest prevalence of hypertension and stroke. Hypertension has the highest prevalence across all racial groups compared to other cardiovascular diseases or conditions, ranging from approximately 22% to 32% of each racial group. Overall, the prevalence of cardiovascular diseases or conditions is lowest for Asians compared to Whites, Blacks, and American Indians or Alaskan Natives. Asthma prevalence is highest among Black and American Indian or Alaska Native populations, while the prevalence of chronic bronchitis and emphysema is generally similar across racial groups. Overall, the prevalence of respiratory diseases is lowest for Asians compared to Whites, Blacks, and American Indians or Alaskan Natives. With regard to ethnicity, cardiovascular and respiratory disease prevalence across all diseases or conditions is generally similar between Hispanic and non-Hispanic populations, although non-Hispanics have a slightly higher prevalence compared to Hispanics.
Taken together, this information indicates that the groups at increased risk of PM2.5 -related health effects represent a substantial portion of the total U.S. population. In evaluating the primary PM2.5 standards, an important consideration is the potential PM2.5 -related public health impacts in these populations.
c. PM2.5 Concentrations in Key Studies Reporting Health Effects
To inform conclusions on the adequacy of the public health protection provided by the current primary PM2.5 standards, the sections below summarize the 2022 PA's evaluation of the PM2.5 exposures, specifically the concentrations that have been examined in controlled human exposure studies, animal toxicological studies, and epidemiologic studies. The 2022 PA places the greatest emphasis on the health outcomes for which the 2019 ISA concludes that the evidence supports a “causal” or a “likely to be causal” relationship with short- or long-term PM2.5 exposures (U.S. EPA, 2022b, section 3.3.3). As described in greater detail in section II.A.2 above, this includes short- or long-term PM2.5 exposures and mortality, cardiovascular effects, and respiratory effects and long-term PM2.5 exposures and cancer and nervous system effects. While the causality determinations in the 2019 ISA are informed by studies evaluating a wide range of PM2.5 concentrations,[62] the sections below summarize the considerations in the 2022 PA regarding the degree to which the evidence assessed in the 2019 ISA and ISA Supplement supports the occurrence of PM-related health effects at concentrations relevant to informing conclusions on the primary PM2.5 standards. In so doing, the 2022 PA focuses on the available studies that are most directly informative to reaching conclusions regarding the adequacy of the current primary PM2.5 standards ( e.g., epidemiologic studies with annual mean PM2.5 concentrations near or below the level of the standard; and controlled human exposure studies at PM2.5 exposures that elicit consistent effects, as well as examining PM2.5 exposures at concentrations that are at or near the level of the standard).
i. PM2.5 Exposure Concentrations Evaluated in Experimental Studies
Evidence for a particular PM2.5 -related health outcome is strengthened when results from experimental studies demonstrate biologically plausible mechanisms through which adverse human health outcomes could occur (U.S. EPA, 2015, p. 20). Two types of experimental studies are of particular importance in understanding the effects Start Printed Page 16237 of PM exposures: controlled human exposure and animal toxicological studies. In such studies, investigators expose human volunteers or laboratory animals, respectively, to known concentrations of air pollutants under carefully regulated environmental conditions and activity levels. Thus, controlled human exposure and animal toxicological studies can provide information on the health effects of experimentally administered pollutant exposures under highly controlled laboratory conditions (U.S. EPA, 2015, p. 11).
Controlled human exposure studies have reported that PM2.5 exposures lasting from less than one hour up to five hours can impact cardiovascular function,[63] and the most consistent evidence from these studies is for impaired vascular function (U.S. EPA, 2019a, section 6.1.13.2). In addition, although less consistent, the 2019 ISA notes that studies examining PM2.5 exposures also provide evidence for increased blood pressure (U.S. EPA, 2019a, section 6.1.6.3), conduction abnormalities/arrhythmia (U.S. EPA, 2019a, section 6.1.4.3), changes in heart rate variability (U.S. EPA, 2019a, section 6.1.10.2), changes in hemostasis that could promote clot formation (U.S. EPA, 2019a, section 6.1.12.2), and increases in inflammatory cells and markers (U.S. EPA, 2019a, section 6.1.11.2). The 2019 ISA concludes that, when taken as a whole, controlled human exposure studies demonstrate that short-term exposure to PM2.5 may impact cardiovascular function in ways that could lead to more serious outcomes (U.S. EPA, 2019a, section 6.1.16). Thus, such studies can provide insight into the potential for specific PM2.5 exposures to result in physiological changes that could increase the risk of more serious effects. Table 3–4 in the 2022 PA summarizes information from the 2019 ISA and 2022 ISA supplement on available controlled human exposure studies that evaluate effects on markers of cardiovascular function following exposure to PM2.5 (U.S. EPA, 2022b). Most of the controlled human exposure studies in Table 3–4 of the 2022 PA have evaluated average PM2.5 concentrations at or above about 100 µg/m3 , with exposure durations typically up to about two hours. Statistically significant effects on one or more indicators of cardiovascular function are often, though not always, reported following 2-hour exposures to average PM2.5 concentrations at and above about 120 µg/m3 , with less consistent evidence for effects following exposures to concentrations lower than 120 µg/m3 . Impaired vascular function, the effect identified in the 2019 ISA as the most consistent across studies (U.S. EPA, 2019a, section 6.1.13.2) is shown following 2-hour exposures to PM2.5 concentrations at and above 149 µg/m3 . Mixed results are reported in the studies that evaluated longer exposure durations ( i.e., longer than 2 hours) and lower ( i.e., near-ambient) PM2.5 concentrations (U.S. EPA, 2022b, section 3.3.3.1). For example, significant effects for some outcomes were reported following 5-hour exposures to 24 µg/m3 in Hemmingsen et al. (2015b), but not for other outcomes following 5-hour exposures to 24 µg/m3 in Hemmingsen et al. (2015a) and not following 24-hour exposures to 10.5 µg/m3 in Bräuner et al. (2008). Additionally, Wyatt et al. (2020) found significant effects for some cardiovascular ( e.g., systematic inflammation markers, cardiac repolarization, and decreased pulmonary function) effects following 4-hour exposures to 37.8 µg/m3 in healthy young participants (18–35 years, n=21) who were subject to intermittent moderate exercise. The higher ventilation rate and longer exposure duration in this study compared to most controlled human exposure studies is roughly equivalent to a 2-hour exposure of 75–100 µg/m3 of PM2.5 . Therefore, dosimetric considerations may explain the observed changes in inflammation in young healthy individuals. Though this study provides evidence of some effects at lower PM2.5 concentrations, overall, there is inconsistent evidence for inflammation in other controlled human exposure studies evaluated in the 2019 ISA (U.S. EPA, 2019a, sections 5.1.7., 5.1.2.3.3, and 6.1.11.2.1; U.S. EPA, 2022a, section 3.3.1).
While controlled human exposure studies are important in establishing biological plausibility, it is unclear how the results from these studies alone and the importance of the effects observed in these studies, should be interpreted with respect to adversity to public health. More specifically, impaired vascular function can signal an intermediate effect along the potential biological pathways for cardiovascular effects following short-term exposure to PM2.5 and show a role for exposure to PM2.5 leading to potential worsening of IHD and heart failure followed potentially by ED visits, hospital admissions, or mortality (U.S. EPA, 2019a, section 6.1 and Figure 6–1). However, just observing the occurrence of impaired vascular function alone does not clearly suggest an adverse health outcome. Additionally, associated judgments regarding adversity or health significance of measurable physiological responses to air pollutants have been informed by guidance, criteria or interpretative statements developed within the public health community, including the American Thoracic Society (ATS) and the European Respiratory Society (ERS), which cooperatively updated the ATS 2000 statement What Constitutes an Adverse Health Effect of Air Pollution (ATS, 2000) with new scientific findings, including the evidence related to air pollution and the cardiovascular system (Thurston et al., 2017).[64] With regard to vascular function, the ATS/ERS statement considers the adversity of both chronic and acute reductions in endothelial function. While the ATS/ERS statement concluded that chronic endothelial and vascular dysfunction can be judged to be a biomarker of an adverse health effect from air pollution, they also conclude that “the health relevance of acute reductions in endothelial function induced by air pollution is less certain” (Thurston et al., 2017). This is particularly informative to our consideration of the controlled human exposure studies which are short-term in nature ( i.e., generally ranging from 2- to 5-hours), including those studies that are conducted at near-ambient PM2.5 concentrations.
The 2022 PA also notes that it is important to recognize that controlled human exposure studies include a small number of individuals compared to epidemiologic studies. Additionally, these studies tend to include generally healthy adult individuals, who are at a lower risk of experiencing health effects. Start Printed Page 16238 These studies, therefore, often do not include children, older adults, or individuals with pre-existing conditions. As such, these studies are somewhat limited in their ability to inform at what concentrations effects may be elicited in at-risk populations.
Nonetheless, to provide some insight into what these controlled human exposure studies may indicate regarding short-term exposure to peak PM2.5 concentrations and how concentrations relate to ambient PM2.5 concentrations, analyses in the 2022 PA (U.S. EPA, 2022b, Figure 2–19) examine monitored 2-hour PM2.5 concentrations (the exposure window most often utilized in the controlled human exposure studies) at sites meeting the current primary PM2.5 standards to evaluate the degree to which 2-hour ambient PM2.5 concentrations at such locations are likely to exceed the 2-hour exposure concentrations in the controlled human exposure studies at which statistically significant effects are reported in multiple studies for one or more indicators of cardiovascular function. At sites meeting the current primary PM2.5 standards, most 2-hour concentrations are below 10 μg/m[3] , and almost never exceed 30 μg/m[3] . The extreme upper end of the distribution of 2-hour PM2.5 concentrations is shifted higher during the warmer months (April to September), generally corresponding to the period of peak wildfire frequency in the U.S. At sites meeting the current primary PM2.5 standards, the highest 2-hour concentrations measured tend to occur during the period of peak wildfire frequency ( i.e., 99.9th percentile of 2-hour concentrations is 62 μg/m[3] during the warm season considered as a whole). Most of the sites measuring these very high concentrations are in the northwestern U.S. and California (U.S. EPA, 2022b, Appendix A, Figure A–1), where wildfires have been relatively common in recent years. When the typical fire season is excluded from the analysis, the extreme upper end of the distribution is reduced ( i.e., 99.9th percentile of 2-hour concentrations is 55 μg/m[3] ).[65] Given these results, the 2022 PA concludes that PM2.5 exposure concentrations evaluated in most of these controlled human exposure studies are well-above the 2-hour ambient PM2.5 concentrations typically measured in locations meeting the current primary standards.
With respect to animal toxicological studies, the 2019 ISA relies on animal toxicological studies to support the plausibility of a wide range of PM2.5 -related health effects. While animal toxicological studies often examine more severe health outcomes and longer exposure durations than controlled human exposure studies, there is uncertainty in extrapolating the effects seen in animals, and the PM2.5 exposures and doses that cause those effects, to human populations. The 2022 PA considers these uncertainties when evaluating what the available animal toxicological studies may indicate with regard to the current primary PM2.5 standards.
As with controlled human exposure studies, most animal toxicological studies evaluated in the 2019 ISA have examined effects following exposure to PM2.5 well above the concentrations likely to be allowed by the current PM2.5 standards. Such studies have generally examined short-term exposures to PM2.5 concentrations ranging from 100 to >1,000 μg/m3 and long-term exposures to concentrations from 66 to >400 μg/m3 ( e.g., see U.S. EPA, 2019a, Table 1–2). Two exceptions are animal toxicological studies reporting impaired lung development following long-term exposures ( i.e., 24 hours per day for several months prenatally and postnatally) to an average PM2.5 concentration of 16.8 μg/m3 (Mauad et al., 2008) and increased carcinogenic potential following long-term exposures ( i.e., 2 months) to an average PM2.5 concentration of 17.7 μg/m3 (Cangerana Pereira et al., 2011). These two studies report serious effects following long-term exposures to PM2.5 concentrations similar to the ambient concentrations reported in some PM2.5 epidemiologic studies (U.S. EPA, 2019a, Table 1–2), though still above the ambient concentrations likely to occur in areas meeting the current primary PM2.5 standards. However, noting uncertainty in extrapolating the effects seen in animals, and the PM2.5 exposures and doses that cause those effects to human populations, animal toxicological studies are of limited utility in informing decisions on the public health protection provided by the current or alternative primary PM2.5 standards. Therefore, the animal toxicological studies are most useful in providing further evidence to support the biological mechanisms and plausibility of various adverse effects.
ii. Ambient PM2.5 Concentrations in Locations of Epidemiologic Studies
As summarized in section II.A.2.a above, epidemiologic studies examining associations between daily or annual average PM2.5 exposures and mortality or morbidity represent a large part of the evidence base supporting several of the 2019 ISA's “causal” and “likely to be causal” determinations. The 2022 PA considers the ambient PM2.5 concentrations present in areas where epidemiologic studies have evaluated associations with mortality or morbidity, and what such concentrations may indicate regarding the adequacy of the primary PM2.5 standards. The use of information from epidemiologic studies to inform conclusions on the primary PM2.5 standards is complicated by the fact that such studies evaluate associations between distributions of ambient PM2.5 and health outcomes, and do not identify the specific exposures that can lead to the reported effects. Rather, health effects can occur over the entire distribution of ambient PM2.5 concentrations evaluated, and epidemiologic studies conducted to date do not identify a population-level threshold below which it can be concluded with confidence that PM2.5 -associated health effects do not occur. Therefore, the 2022 PA evaluates the PM2.5 air quality distributions over which epidemiologic studies support health effect associations (U.S. EPA, 2022b, section 3.3.3.2). In the absence of discernible thresholds, the 2022 PA considers the study-reported ambient PM2.5 concentrations reflecting estimated exposure with a focus around the middle portion of the PM2.5 air quality distribution, where the bulk of the observed data reside and which provides the strongest support for reported health effect associations. The section below, as well as in more detail in section II.B.3.b.i of the proposal (88 FR 5594, January 27, 2023), describes the consideration of the key epidemiologic studies and observations from these studies, as evaluated in the 2022 PA (U.S. EPA, 2022b, section 3.3.3.2).
As an initial matter, in considering the PM2.5 air quality distributions associated with mortality or morbidity in the key epidemiologic studies, the 2022 PA recognizes that in previous reviews, the decision framework used to judge adequacy of the existing PM2.5 standards, and what levels of any potential alternative standards should be considered, placed significant weight on epidemiologic studies that assessed associations between PM2.5 exposure and health outcomes that were most strongly supported by the body of scientific evidence. In doing so, the decision framework recognized that while there is no specific point in the air quality distribution of any Start Printed Page 16239 epidemiologic study that represents a “bright line” at and above which effects have been observed and below which effects have not been observed, there is significantly greater confidence in the magnitude and significance of observed associations for the part of the air quality distribution corresponding to where the bulk of the health events in each study have been observed, generally at or around the mean concentration. This is the case both for studies of daily PM2.5 exposures and for studies of annual average PM2.5 exposures (U.S. EPA, 2022b, section 3.3.3.2.1).
As discussed further in the 2022 PA, studies of daily PM2.5 exposures examine associations between day-to-day variation in PM2.5 concentrations and health outcomes, often over several years (U.S. EPA, 2022b, section 3.3.3.2.1). While there can be considerable variability in daily exposures over a multi-year study period, most of the estimated exposures reflect days with ambient PM2.5 concentrations around the middle of the air quality distributions examined ( i.e., “typical” days rather than days with extremely high or extremely low concentrations). Similarly, for studies of annual PM2.5 exposures, most of the health events occur at estimated exposures that reflect annual average PM2.5 concentrations around the middle of the air quality distributions examined. In both cases, epidemiologic studies provide the strongest support for reported health effect associations for this middle portion of the PM2.5 air quality distribution, which corresponds to the bulk of the underlying data, rather than the extreme upper or lower ends of the distribution. Consistent with this, as noted in the 2022 PA (U.S. EPA, 2022b, section 3.3.1.1), several epidemiologic studies report that associations persist in analyses that exclude the upper portions of the distributions of estimated PM2.5 exposures, indicating that “peak” PM2.5 exposures are not disproportionately responsible for reported health effect associations.
Thus, in considering PM2.5 air quality data from epidemiologic studies, consistent with approaches in the 2012 and 2020 reviews (78 FR 3161, January 15, 2013; U.S. EPA, 2011, sections 2.1.3 and 2.3.4.1; 85 FR 82716–82717, December 18, 2020; U.S. EPA, 2020b, sections 3.1.2 and 3.2.3), the 2022 PA evaluates study-reported means (or medians) of daily and annual average PM2.5 concentrations as indicators for the middle portions of the air quality distributions, over which studies generally provide strong support for reported associations and for which confidence in the magnitude and significance of associations observed in the epidemiologic studies is greatest (78 FR 3101, January 15, 2013). In addition to the overall study means, the 2022 PA also focuses on concentrations somewhat below the means ( e.g., 25th and 10th percentiles), when such information is available from the epidemiologic studies, which again is consistent with approaches used in previous reviews. In so doing, the 2022 PA notes, as in previous reviews, that a relatively small portion of the health events are observed in the lower part of the air quality distribution and confidence in the magnitude and significance of the associations begins to decrease in the lower part of the air quality distribution. Furthermore, consistent with past reviews, there is no single percentile value within a given air quality distribution that is most appropriate or “correct” to use to characterize where our confidence in associations becomes appreciably lower. However, and as detailed further in the 2022 PA, the range from the 25th to 10th percentiles is a reasonable range to consider as a region where there is appreciably less confidence in the associations observed in epidemiologic studies compared to the means (U.S. EPA, 2022b, p. 3–69).[66]
In evaluating the overall study-reported means, and concentrations somewhat below the means from epidemiologic studies, the 2022 PA focuses on the form, averaging time and level of the current primary annual PM2.5 standard. Consistent with the approaches used in the 2012 and 2020 reviews (78 FR 3161–3162, January 15, 2013; 85 FR 82716–82717, December 18, 2020), the annual standard has been utilized as the primary means of providing public health protection against the bulk of the distribution of short- and long-term PM2.5 exposures. Thus, the evaluation of the study-reported mean concentrations from key epidemiologic studies lends itself best to evaluating the adequacy of the annual PM2.5 standard (rather than the 24-hour standard with its 98th percentile form). This is true for the study-reported means from both long-term and short-term exposure epidemiologic studies, recognizing that the overall mean PM2.5 concentrations reported in studies of short-term (24-hour) exposures reflect averages across the study population and over the years of the study. Thus, mean concentrations from short-term exposure studies reflect long-term averages of 24-hour PM2.5 exposure estimates. In this manner, the examination of study-reported means in key epidemiologic studies in the 2022 PA aims to evaluate the protection provided by the annual PM2.5 standard against the exposures where confidence is greatest for associations with mortality and morbidity. In addition, the protection provided by the annual standard is evaluated in conjunction with that provided by the 24-hour standard, with its 98th percentile form, which aims to provide supplemental protection against the short-term exposures to peak PM2.5 concentrations that can occur in areas with strong contributions from local or seasonal sources, even when overall ambient mean PM2.5 concentrations in an area remain relatively low.
In focusing on the annual standard, and in evaluating the range of study-reported exposure concentrations for which the strongest support for adverse health effects exists, the 2022 PA examines exposure concentrations in key epidemiologic studies to determine whether the current primary annual PM2.5 standard provides adequate protection against these exposure concentrations. This means, as in past reviews, application of a decision framework based on assessing means reported in key epidemiologic studies must also consider how the study means were computed and how these values compare to the annual standard metric (including the level, averaging time and form) and the use of the monitor with the highest PM2.5 design value in an area for compliance. In the 2012 review, it was recognized that the key epidemiologic studies computed the study mean using an average across monitor-based PM2.5 concentrations. As such, the Agency noted that this decision framework applied an approach of using maximum monitor concentrations to determine compliance with the standard, while selecting the standard level based on consideration of composite monitor concentrations. Further, the Agency included analyses (Hassett-Sipple et al., 2010; Frank, 2012) that examined the differences in these two metrics ( i.e., maximum monitor concentrations and composite monitor concentrations) across the U.S. and in areas included in the key epidemiologic studies and found that the maximum design value in an area was generally higher than the monitor average across that area, with the difference varying Start Printed Page 16240 based on location and concentration. This information was taken into account in the Administrator's final decision in selecting a level for the primary annual PM2.5 standard the 2012 review and discussed more specifically in her considerations on adequate margin of safety.
Consistent with the approach taken in 2012, in assessing how the overall mean (or median) PM2.5 concentrations reported in key epidemiologic studies can inform conclusions on the primary annual PM2.5 standard, the 2022 PA notes that the relationship between mean PM2.5 concentrations and the area design value continues to be an important consideration in evaluating the adequacy of the current or potential alternative annual PM2.5 standard levels in this reconsideration. In a given area, the area design value is based on the monitor in an area with the highest PM2.5 concentrations and is used to determine compliance with the standard. The highest PM2.5 concentrations spatially distributed in the area would generally occur at or near the area design value monitor and the distribution of PM2.5 concentrations would generally be lower in other locations and at monitors in that area. As such, when an area is meeting a specific annual standard level, the annual average exposures in that area are expected to be at concentrations lower than that level and the average of the annual average exposures across that area are expected ( i.e., a metric similar to the study-reported mean values) to be lower than that level.[67]
Another important consideration is that there are a substantial number of different types of epidemiologic studies available since the 2012 review, included in both the 2019 ISA and the ISA Supplement, that make understanding the relationship between the mean PM2.5 concentrations and the area design value even more important (U.S. EPA, 2019a; U.S. EPA, 2022a). While the key epidemiologic studies in the 2012 review were all monitor-based studies, the newer studies include hybrid modeling approaches, which have emerged in the epidemiologic literature as an alternative to approaches that only use ground-based monitors to estimate exposure. As assessed in the 2019 ISA and ISA Supplement, a substantial number of epidemiologic studies used hybrid model-based methods in evaluating associations between PM2.5 exposure and health effects (U.S. EPA, 2019a; U.S. EPA, 2022a). Hybrid model-based studies employ various fusion techniques that combine ground-based monitored data with air quality modeled estimates and/or information from satellites to estimate PM2.5 exposures.[68] Additionally, hybrid modeling approaches tend to broaden the areas captured in the exposure assessment, and in so doing, tend to report lower mean PM2.5 concentrations than monitor-based approaches because they include more suburban and rural areas where concentrations are lower. While these studies provide a broader estimation of PM2.5 exposures compared to monitor-based studies ( i.e., PM2.5 concentrations are estimated in areas without monitors), the hybrid modeling approaches result in study-reported means that are more difficult to relate to the annual standard metric and to the use of maximum monitor design values to assess compliance. In addition, and to further complicate the comparison, when looking across these studies, variations exist in how exposure is estimated between such studies, which in turn affects how the study means are calculated. Two important variations across studies include: (1) Variability in spatial scale used ( i.e., averages computed across the nation (or large portions of the country) versus a focus on only CBSAs) and (2) variability in exposure assignment methods ( i.e., averaging across all grid cells [non-population weighting], averaging across a scaled-up area like a ZIP code [aspects of population weighting applied], and/or applying population weighting). To elaborate further on the variability in exposure assignment methods, studies that use hybrid modeling approaches can estimate PM2.5 concentrations at different spatial resolutions, including at 1 km x 1 km grid cells, at 12 km x 12 km grid cells, or at the census tract level. Mean reported PM2.5 concentrations can then be estimated either by averaging up to a larger spatial resolution that corresponds to the spatial resolution for which health data exists ( e.g., ZIP code level) and therefore apply aspects of population weighting. These values are then averaged across all study locations at the larger spatial resolution ( e.g., averaged across all ZIP codes in the study) over the study period, resulting in the study-reported mean 24-hour average or average annual PM2.5 concentration. Other studies that use hybrid modeling methods to estimate PM2.5 concentrations may use each grid cell to calculate the study-reported mean 24-hour average or average annual PM2.5 concentration. As such, these types of studies do not apply population weighting in their mean concentrations. In studies that use each grid cell to report a mean PM2.5 concentration and do not apply aspects of population weighting, the study mean may not reflect the exposure concentrations used in the epidemiologic study to assess the reported association. The impact of the differences in methods is an important consideration when comparing mean concentrations across studies (U.S. EPA, 2022b, section 3.3.3.2.1). Thus, the 2022 PA also considers the methods used to estimate PM2.5 concentrations, which vary from traditional methods using monitoring data from ground-based monitors [69] to those using more complex hybrid modeling approaches and how these methods calculate the study-reported mean PM2.5 concentration.[70]
Given the emergence of the hybrid model-based epidemiologic studies since the 2012 review, the 2022 PA explores the relationship between the approaches used in these studies to estimate PM2.5 concentrations and the impact that the different methods have on the study-reported mean PM2.5 concentrations. The 2022 PA further seeks to understand how the approaches and resulting mean concentrations compare across studies, as well as what the resulting mean values represent relative to the annual standard. In so doing, the 2022 PA presents analyses that compare the area annual design values, composite monitor PM2.5 concentrations, and mean concentrations from two hybrid modeling approaches, including evaluation of the means when population weighting is applied and when population weighting is not Start Printed Page 16241 applied (U.S. EPA, 2022b, section 2.3.3.1).
In the air quality analyses comparing composite monitored PM2.5 concentrations with annual PM2.5 design values in U.S. CBSAs, maximum annual PM2.5 design values were approximately 10% to 20% higher than annual average composite monitor concentrations ( i.e., averaged across multiple monitors in the same CBSA) (sections I.D.5.a above and U.S. EPA, 2022b, section 2.3.3.1, Figure 2–28 and Table 2–3). The difference between the maximum annual design value and average concentration in an area can be smaller or larger than this range (10–20%), depending on a variety of factors such as the number of monitors, monitor siting characteristics, the distribution of ambient PM2.5 concentrations, and how the average concentrations are calculated ( i.e., averaged across monitors versus across modeled grid cells). Results of this analysis suggest that there will be a distribution of concentrations across an area and the maximum annual average monitored concentration in an area (at the design value monitor, used for compliance with the standard), will generally be 10–20% higher than the average PM2.5 concentration across the other monitors in the area. Thus, in considering how the annual standard levels would relate to the study-reported means from key monitor-based epidemiologic studies, the 2022 PA generally concludes that an annual standard level that is no more than 10–20% higher than monitor-based study-reported mean PM2.5 concentrations would generally maintain air quality exposures to be below those associated with the study-reported mean PM2.5 concentrations, exposures for which the strongest support for adverse health effects occurring is available.
The 2022 PA also evaluates data from two hybrid modeling approaches (DI2019 and HA2020) that have been used in several recent epidemiologic studies (U.S. EPA, 2022b, section 2.3.3.2.4).[71] The analysis shows that the means differ when PM2.5 concentrations are estimated in urban areas only (CBSAs) versus when the averages were calculated with all or most grid cells nationwide, likely because areas included outside of CBSAs tend to be more rural and have lower estimated PM2.5 concentrations. The 2022 PA recognizes the importance of this variability in the means since the study areas included in the calculation of the mean, and more specifically whether a study is focused on nationwide, regional, or urban areas, will affect the calculation of the study mean based on how many rural areas, with lower estimated PM2.5 concentrations, are included in the study area. While the determination of what spatial scale to use to estimate PM2.5 concentrations does not inherently affect the quality of the epidemiologic study, the spatial scale can influence the calculated reported long-term mean concentration across the study area and period. The results of the analysis show that, regardless of the hybrid modeling approach assessed, the annual average PM2.5 concentrations in CBSA-only analyses are 4–8% higher than for nationwide analyses, likely as a result of higher PM2.5 concentrations in more densely populated areas, and exclusion of more rural areas (U.S. EPA, 2022b, Table 2–4). When evaluating comparisons between surfaces that estimate exposure using aspects of population weighting versus surfaces that do not calculate means using population weighting, surfaces that calculate long-term mean PM2.5 concentrations with population-weighted averages have higher average annual PM2.5 concentrations, compared to annual PM2.5 concentrations in analyses that do not apply population weighting.[72] Analyses show that average maximum annual design values are 40 to 50% higher when compared to annual average PM2.5 concentrations estimated without population weighting versus 15% to 18% higher when compared to average annual PM2.5 concentrations estimated with population weighting applied (similar to the differences observed for the composite monitor comparison values for the monitor-based epidemiologic studies) (U.S. EPA, 2022b, section 2.3.3.2.4). Given these results, it is worth noting that for the studies using the hybrid modeling approaches, the choice of methodology employed in calculating the study-reported means ( i.e., using population weighting or not), and not a difference in estimates of exposure in the study itself, can produce substantially different study-reported mean values, where approaches that do not apply population weighting leading to much lower estimated mean PM2.5 concentrations.
Based on these results, and similar to conclusions for the monitor-based studies, the 2022 PA generally concludes that study-reported mean concentrations in the studies that employ hybrid modeling approaches and calculate a population-weighted mean are associated with air quality conditions that would be achieved by meeting annual standard levels that are 15–18% higher than study-reported means. Therefore, an annual standard level that is no more than 15–18% higher than the study-reported means would generally maintain air quality exposures to be below those associated with the study-reported mean PM2.5 concentrations, exposures for which we have the strongest support for adverse health effects occurring. For the studies that utilize hybrid modeling approaches but do not incorporate population weighting in calculating the mean, the annual design values associated with these air quality conditions are expected to be much higher ( i.e., 40–50% higher) and this larger difference makes it more difficult to consider how these studies can be used to determine the adequacy of the protection afforded by the current or potential alternative annual standards. Additionally, as noted above in studies that utilize hybrid modeling approaches and that do not incorporate population weighting in calculating the mean ( e.g., use each grid cell to calculate a mean PM2.5 concentration), the study mean does not reflect the exposure concentrations used in the epidemiologic study to assess the reported association.
The 2022 PA notes that while these analyses can be useful to informing the understanding of the relationship between study-reported mean concentrations and the level of the annual standard, some limitations of this analysis must be recognized (U.S. EPA, 2022a, section 3.3.3.2.1). First, the comparisons used only two hybrid modeling approaches. Although these two hybrid modeling surfaces have been used in a number of recent epidemiologic studies, they represent just two of the many hybrid modeling approaches that have been used in epidemiologic studies to estimate PM2.5 concentrations. These methods continue to evolve, with further development and improvement to prediction models that estimate PM2.5 concentrations in epidemiologic studies. In addition to differences in hybrid modeling approaches, epidemiologic studies also use different methods to assign a population weighted average PM2.5 concentration to their study population, and the assessment presented in the Start Printed Page 16242 2022 PA does not evaluate all of the potential methods that could be used.
Additionally, while some of these epidemiologic studies also provide information on the broader distributions of exposure estimates and/or health events and the PM2.5 concentrations corresponding to the lower percentiles of those data ( e.g., 25th and/or 10th), the air quality analysis in the 2022 PA focuses on mean PM2.5 concentrations and a similar comparison for lower percentiles of data was not assessed. Therefore, any direct comparison of study-reported PM2.5 concentrations corresponding to lower percentiles and annual design values is more uncertain than such comparisons with the mean. Finally, air quality analysis presented in the 2022 PA and detailed above in section I.D.5 included two hybrid modeling-based approaches that used U.S.-based air quality information for estimating PM2.5 concentrations. As such, the analyses are most relevant to interpreting the study-reported mean concentrations from U.S. epidemiologic studies and do not provide additional information about how the mean exposures concentrations reported in epidemiologic studies in other countries would compare to annual design values observed in the U.S. In addition, while information from Canadian studies can be useful in assessing the adequacy of the annual standard, differences in the exposure environments and population characteristics between the U.S. and other countries can affect the study-reported mean value and its relationship with the annual standard level. Sources and pollutant mixtures, as well as PM2.5 concentration gradients, may be different between countries, and the exposure environments in other countries may differ from those observed in the U.S. Furthermore, differences in population characteristics and population densities can also make it challenging to directly compare studies from countries outside of the U.S. to a design value in the U.S.
As with the experimental studies discussed above, the 2022 PA focuses on epidemiologic studies assessed in the 2019 ISA and ISA Supplement that have the potential to be most informative in reaching decisions on the adequacy of the primary PM2.5 standards. The 2022 PA focuses on epidemiologic studies that provide strong support for “causal” or “likely to be causal” relationships with PM2.5 exposures in the 2019 ISA. Further, the 2022 PA also focuses on the health effect associations that are determined in the 2019 ISA and ISA Supplement to be consistent across studies, coherent with the broader body of evidence ( e.g., including animal and controlled human exposure studies), and robust to potential confounding by co-occurring pollutants and other factors.[73] In particular the 2022 PA considers the U.S. and Canadian epidemiologic studies to be more useful for reaching conclusions on the current standards than studies conducted in other countries, given that the results of the U.S. and Canadian studies are more directly applicable for quantitative considerations, whereas studies conducted in other countries reflect different populations, exposure characteristics, and air pollution mixtures. Additionally, epidemiologic studies outside of the U.S. and Canada generally reflect higher PM2.5 concentrations in ambient air than are currently found in the U.S., and are less relevant to informing questions about adequacy of the current standards.[74] However, and as noted above, the 2022 PA also recognizes that while information from Canadian studies can be useful in assessing the adequacy of the annual standard, there are still important differences between the exposure environments in the U.S. and Canada and interpreting the data ( e.g., mean concentrations) from the Canadian studies in the context of a U.S.-based standard may present challenges in directly and quantitatively informing questions regarding the adequacy of the current or potential alternative the levels of the annual standard. Lastly, the 2022 PA emphasizes multicity/multistate studies that examine health effect associations, as such studies are more encompassing of the diverse atmospheric conditions and population demographics in the U.S. than studies that focus on a single city or State. Figures 3–4 through 3–7 in the 2022 PA summarize the study details for the key U.S. and Canadian epidemiologic studies (U.S. EPA, 2022b, section 3.3.3.2.1).[75]
The key epidemiologic studies identified in the 2022 PA indicate generally positive and statistically significant associations between estimated PM2.5 exposures (short- or long-term) and mortality or morbidity across a range of ambient PM2.5 concentrations (U.S. EPA, 2022b, section 3.3.3.2.1), report overall mean (or median) PM2.5 concentrations, and include those for which the years of PM2.5 air quality data used to estimate exposures overlap entirely with the years during which health events are reported.[76] Additionally, for studies that estimate PM2.5 exposure using hybrid modeling approaches, the 2022 PA also considers the approach used to estimate PM2.5 concentrations and the approach used to validate hybrid model predictions when evaluating those studies as key epidemiologic studies [77] and focuses on those studies that use recent methods based on surfaces that are with fused with monitored PM2.5Start Printed Page 16243 concentration data (U.S. EPA, 2022b, section 3.3.3.2.1).
Figure 1 below (U.S. EPA, 2022b, Figure 3–8) highlights the overall mean (or median) PM2.5 concentrations reported in key U.S. studies that use ground-based monitors alone to estimate long- or short-term PM2.5 exposure.[78] For the small subset of studies with available information on the broader distributions of underlying data, Figure 1 below also identifies the study-period PM2.5 concentrations corresponding to the 25th and 10th percentiles of health events [79] (see Appendix B, Section B.2 of the 2022 PA for more information). Figure 2 (U.S. EPA, 2022a, Figure 3–14) presents overall means of predicted PM2.5 concentrations for key U.S. model-based epidemiologic studies that apply aspects of population-weighting, and the concentrations corresponding to the 25th and 10th percentiles of estimated exposures or health events [80] when available (see Appendix B, section B.3 for additional information).[81]
Start Printed Page 16244
Start Printed Page 16245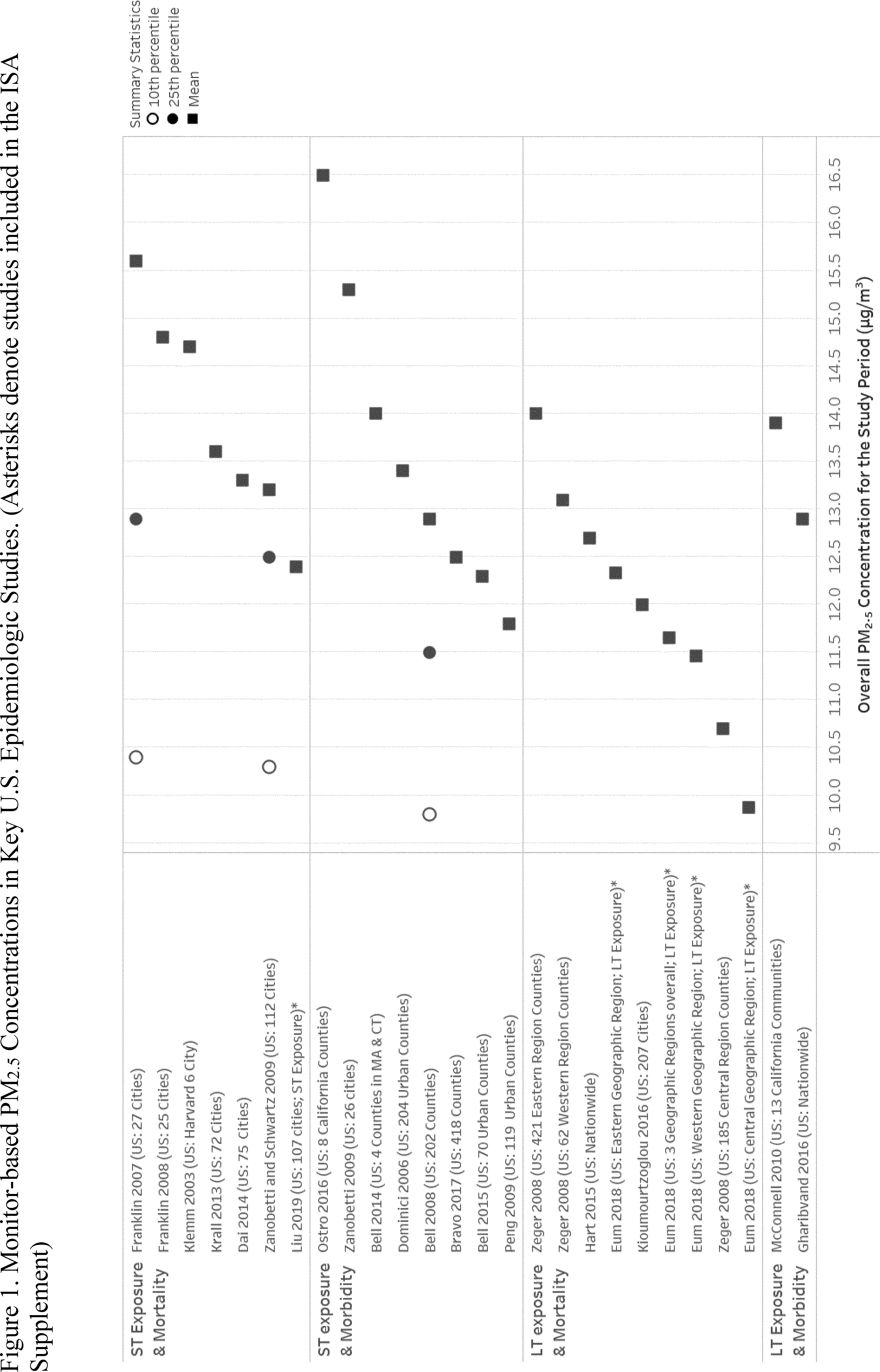

Based on its evaluation of study-reported mean concentrations, the 2022 PA notes that key epidemiologic studies conducted in the U.S. or Canada report generally positive and statistically significant associations between estimated PM2.5 exposures (short- or long-term) and mortality or morbidity across a wide range of ambient PM2.5 concentrations (U.S. EPA, 2022b, section 3.3.3.2.1). The 2022 PA makes a number of observations with regard to the study-reported PM2.5 concentrations in the key U.S. and Canadian epidemiologic studies.
The 2022 PA first considers the PM2.5 concentrations from the key U.S. epidemiologic studies. For studies that use monitors to estimate PM2.5 exposures, overall mean PM2.5 concentrations range between 9.9 μg/m[3] [82] to 16.5 μg/m3 (Figure 1 above and Start Printed Page 16246 U.S. EPA, 2022b, Figure 3–8). For key U.S. epidemiologic studies that use hybrid model-predicted exposures and apply aspects of population-weighting, mean PM2.5 concentrations range from 9.3 μg/m3 to just above 12.2 µg/m3 (Figure 2 above and U.S. EPA, 2022b, Figure 3–14). In studies that average up from the grid cell level to the ZIP code, postal code, or census tract level, mean PM2.5 concentrations range from 9.8 µg/m3 to 12.2 µg/m3 . The one study that population-weighted the grid cell prior to averaging up to the ZIP code or census tract level reported mean PM2.5 concentrations of 9.3 μg/m3 . Based on air quality analyses noted above, these hybrid modelled epidemiologic studies are expected to report means similar to those from monitor-based studies.
Other key U.S. epidemiologic studies that use hybrid modeling approaches estimate mean PM2.5 exposure by averaging each grid cell across the entire study area, whether that be the nation or a region of the country. These studies do not weight the estimated exposure concentrations based on population density or location of health events. As such, the study mean reported in these studies may not reflect the exposure concentrations used in the epidemiologic study to assess the reported association. As a result, these reported mean concentrations are the most different (and much lower) than the means reported in monitor-based studies. Due to the methodology employed in calculating the study-reported means and not necessarily a difference in estimates of exposure, these epidemiologic studies are expected to report some of the lowest mean values. For these studies, the reported mean PM2.5 concentrations range from 8.1 μg/m3 to 11.9 μg/m3 (U.S. EPA, 2022b, Figure 3–14). As noted above, for studies that utilize hybrid modeling approaches but do not incorporate population weighting into the reported mean calculation, the associated annual design values would be expected to be much higher ( i.e., 40–50% higher) than the study-reported means. This larger difference between design values and study-reported mean concentrations makes it more difficult to consider how these studies can be used to determine the adequacy of the protection afforded by the current or potential alternative annual standards (U.S. EPA, 2022b, section 3.3.3.2.1).
In addition to the mean PM2.5 concentrations, a subset of the key U.S. epidemiologic studies report PM2.5 concentrations corresponding to the 25th and 10th percentiles of health data or exposure estimates to provide insight into the concentrations that comprise the lower quartile of the air quality distributions. In studies that use monitors to estimate PM2.5 exposures, 25th percentiles of health events correspond to PM2.5 concentrations ( i.e., averaged over the study period for each study city) at or above 11.5 µg/m[3] and 10th percentiles of health events correspond to PM2.5 concentrations at or above 9.8 µg/m[3] ( i.e., 25% and 10% of health events, respectively, occur in study locations with PM2.5 concentrations below these values) (Figure 1 above and U.S. EPA, 2022b, Figure 3–8). Of the key U.S. epidemiologic studies that use hybrid modeling approaches and apply population-weighting to estimate long-term PM2.5 exposures, the ambient PM2.5 concentrations corresponding to 25th percentiles of estimated exposures are 9.1 µg/m[3] (Figure 2 and U.S. EPA, 2022b, Figure 3–14). In key U.S. epidemiologic studies that use hybrid modeling approaches and apply population-weighting to estimate short-term PM2.5 exposures, the ambient concentrations corresponding to 25th percentiles of estimated exposures, or health events, are 6.7 µg/m[3] (Figure 2 and U.S. EPA, 2022b, Figure 3–14). In key U.S. epidemiologic studies that use hybrid modeling approaches and do not apply population-weighting to estimate PM2.5 exposures, the ambient concentrations corresponding to 25th percentiles of estimated exposures, or health events, range from 4.6 to 9.2 µg/m[3] (U.S. EPA, 2022b, Figure 3–14).[83] In the key epidemiologic studies that apply hybrid modeling approaches with population-weighting and with information available on the 10th percentile of health events, the ambient PM2.5 concentration corresponding to that 10th percentile range from 4.7 µg/m3 to 7.3 µg/m3 (Figure 2 and U.S. EPA, 2022b, Figure 3–14).
The 2022 PA next considers the PM2.5 concentrations from the key Canadian epidemiologic studies. Generally, the study-reported mean concentrations in Canadian studies are lower than those reported in the U.S. studies for both monitor-based and hybrid model methods. For the majority of key Canadian epidemiologic studies that use monitor-based exposure, mean PM2.5 concentrations generally ranged from 7.0 µg/m3 to 9.0 µg/m3 (U.S. EPA, 2022b, Figure 3–9). For these studies, 25th percentiles of health events correspond to PM2.5 concentrations at or above 6.5 µg/m3 and 10th percentiles of health events correspond to PM2.5 concentrations at or above 6.4 µg/m3 (U.S. EPA, 2022b, Figure 3–9). For the key Canadian epidemiologic studies that use hybrid model-predicted exposure, the mean PM2.5 concentrations are generally lower than in U.S. model-based studies (U.S. EPA, 2022b, Figure 3–10), ranging from approximately 6.0 µg/m3 to just below 10.0 µg/m3 (U.S. EPA, 2022b, Figure 3–11). The majority of the key Canadian epidemiologic studies that used hybrid modeling were completed at the nationwide scale, while four studies were completed at the regional geographic spatial scale. In addition, all the key Canadian epidemiologic studies apply aspects of population weighting, where all grid cells within a postal code are averaged, individuals are assigned exposure at the postal code resolution, and study mean PM2.5 concentrations are based on the average of individual exposures. The majority of studies estimating exposure nationwide range between just below 6.0 µg/m3 to 8.0 µg/m3 (U.S. EPA, 2022b, Figure 3–11). One study by Erickson et al. (2020) presents an analysis related immigrant status and length of residence in Canada versus non-immigrant populations, which accounts for the four highest mean PM2.5 concentrations which range between 9.0 µg/m3 and 10.0 µg/m3 (U.S. EPA, 2022b, Figure 3–11). The four studies that estimate exposure at the regional scale report mean PM2.5 concentrations that range from 7.8 µg/m3 to 9.8 µg/m3 (U.S. EPA, 2022b, Figure 3–11). Three key Canadian epidemiologic studies report information on the 25th percentile of health events. In these studies, the ambient PM2.5 concentration corresponding to the 25th percentile is approximately 8.0 µg/m3 in two studies, and 4.3 µg/m3 in a third study (U.S. EPA, 2022b, Figure 3–11).
In addition to the expanded body of evidence from the key U.S. epidemiologic studies discussed above, there are also a subset of epidemiologic studies that have emerged that further inform an understanding of the relationship between PM2.5 exposure and health effects, including studies with the highest exposures excluded (restricted analyses), epidemiologic studies that employed statistical approaches that attempt to more extensively account for confounders and are more robust to model misspecification ( i.e., used alternative Start Printed Page 16247 methods for confounder control),[84] and accountability studies (U.S. EPA, 2019a, U.S. EPA, 2021a, U.S. EPA, 2022a).
Restricted analyses are studies that examine health effect associations in analyses with the highest exposures excluded, restricting analyses to daily exposures less than the 24-hour primary PM2.5 standard and annual exposures less than the annual PM2.5 standard. The 2022 PA presents a summary of restricted analyses evaluated in the 2019 ISA and ISA Supplement (U.S. EPA, 2022b, Table 3–10). The restricted analyses can be informative in assessing the nature of the association between long-term exposures ( e.g., annual average concentrations <12.0 µg/m3 ) or short-term exposures ( e.g., daily concentrations <35 µg/m3 ) when looking only at exposures to lower concentrations, including whether the association persists in such restricted analyses compared to the same analyses for all exposures, as well as whether the association is stronger, in terms of magnitude and precision, than when completing the same analysis for all exposures. While these studies are useful in supporting the confidence and strength of associations at lower concentrations, these studies also have inherent uncertainties and limitations, including uncertainty in how studies exclude concentrations ( e.g., are they excluded at the modeled grid cell level, the ZIP code level) and in how concentrations in studies that restrict air quality data relate to design values for the annual and 24-hour standards. Further, these studies often do not report descriptive statistics ( e.g., mean PM2.5 concentrations, or concentrations at other percentiles) that allow for additional consideration of this information. As such, while these studies can provide additional supporting evidence for associations at lower concentrations, the 2022 PA notes that there are also limitations in how to interpret these studies when evaluating the adequacy of the current or potential alternative standards.
Restricted analyses provide additional information on the nature of the association between long- or short-term exposures when analyses are restricted to lower PM2.5 concentrations and indicate that effect estimates are generally greater in magnitude in the restricted analyses for long- and short-term PM2.5 exposure compared to the main analyses. In two U.S. studies that report mean PM2.5 concentrations in restricted analyses and that estimate effects associated with long-term exposure to PM2.5 , the effect estimates are greater in the restricted analyses than in the main analyses. Di et al. (2017a) and Dominici et al. (2019) report positive and statistically significant associations in analyses restricted to concentrations less than 12.0 µg/m3 for all-cause mortality and effect estimates are greater in the restricted analyses than effect estimates reported in main analyses. In addition, both studies report mean PM2.5 concentrations of 9.6 µg/m3 . While none of the U.S. studies of short-term exposure present mean PM2.5 concentrations for the restricted analyses, these studies generally have mean 24-hour average PM2.5 concentrations in the main analyses below 12.0 µg/m3 , and report increases in the effect estimates in the restricted analyses compared to the main analyses. Additionally, in the one Canadian study of long-term PM2.5 exposure, Zhang et al. (2021) conducted analyses where annual PM2.5 concentrations were restricted to concentrations below 10.0 µg/m3 and 8.8 µg/m3 , which presumably have lower mean concentrations than the mean of 7.8 µg/m3 reported in the main analyses, though restricted analysis mean PM2.5 concentrations are not reported. Effect estimates for non-accidental mortality are greater in analyses restricted to PM2.5 concentrations less than 10.0 µg/m3 , but less in analyses restricted to <8.8 µg/m3 .
The second type of studies that have recently emerged and further inform the consideration of the relationship between PM2.5 exposure and health effects in the 2022 PA are those that employ alternative methods for confounder control. Alternative methods for confounder control seek to mimic randomized experiments through the use of study design and statistical methods to more extensively account for confounders and are more robust to model misspecification. The 2022 PA presents a summary of the studies that employ alternative methods for confounder control, and employ a variety of statistical methods, which are evaluated in the 2019 ISA and ISA Supplement (U.S. EPA, 2022b, Table 3–11). These studies reported consistent results among large study populations across the U.S. and can further inform the relationship between long- and short-term PM2.5 exposure and total mortality. Studies that employ alternative methods for confounder control to assess the association between long-term exposure to PM2.5 and mortality reduce uncertainties related to confounding and provide additional support for the associations reported in the broader body of cohort studies that examined long-term PM2.5 exposure and mortality.
Lastly, there is a subset of epidemiologic studies that assess whether long-term reductions in ambient PM2.5 concentrations result in corresponding reductions in health outcomes. These include studies that evaluate the potential for improvements in public health, including reductions in mortality rates, increases in life expectancy, and reductions in respiratory disease as ambient PM2.5 concentrations have declined over time. Some of these studies, accountability studies, provide insight on whether the implementation of environmental policies or air quality interventions result in changes/reductions in air pollution concentrations and the corresponding effect on health outcomes.[85] The 2022 PA presents a summary of these studies, which are assessed in the 2019 ISA and ISA Supplement (U.S. EPA, 2022b, Table 3–12). These studies lend support for the conclusion that improvements in air quality are associated with improvements in public health.
More specifically, of the accountability studies that account for changes in PM2.5 concentrations due to a policy or the implementation of an intervention and whether there was evidence of changes in associations with mortality or cardiovascular effects as a result of changes in annual PM2.5 concentrations, Corrigan et al. (2018), Henneman et al. (2019) and Sanders et al. (2020a) present analyses with starting PM2.5 concentrations (or concentrations prior to the policy or intervention) below 12.0 µg/m3 . Henneman et al. (2019) explored changes in modeled PM2.5 concentrations following the retirement of coal fired power plants in the U.S., and found that reductions from mean annual PM2.5 concentrations of 10.0 µg/m3 in 2005 to mean annual PM2.5 concentrations of 7.2 µg/m3 in 2012 from coal-fueled power plants resulted in corresponding reductions in the number of cardiovascular-related Start Printed Page 16248 hospital admissions, including for all cardiovascular disease, acute MI, stroke, heart failure, and ischemic heart disease in those aged 65 and older. Corrigan et al. (2018) examined whether there was a change in the cardiovascular mortality rate before (2000–2004) and after (2005–2010) implementation of the first annual PM2.5 NAAQS implementation based on mortality data from the National Center for Health Statistics and reported 1.10 (95% confidence interval (CI): 0.37, 1.82) fewer cardiovascular deaths per year per 100,000 people for each 1 μg/m3 reduction in annual PM2.5 concentrations. When comparing whether counties met the annual PM2.5 standard (attainment counties), there were 1.96 (95% CI: 0.77, 3.15) fewer cardiovascular deaths for each 1 μg/m3 reduction in annual PM2.5 concentrations between the two periods for attainment counties, whereas in non-attainment counties ( e.g., counties that did not meet the annual PM2.5 standard), there were 0.59 (95% CI: − 0.54, 1.71) fewer cardiovascular deaths between the two periods. And lastly, Sanders et al. (2020a) examined whether policy actions ( i.e., the first annual PM2.5 NAAQS implementation rule in 2005 for the 1997 annual PM2.5 standard with a 3-year annual average of 15 μg/m3 ) reduced PM2.5 concentrations and mortality rates in Medicare beneficiaries between 2000–2013. They report evidence of changes in associations with mortality (a decreased mortality rate of ~0.5 per 1,000 in attainment and non-attainment areas) due to changes in annual PM2.5 concentrations in both attainment and non-attainment areas. Additionally, attainment areas had starting concentrations below 12.0 µg/m3 prior to implementation of the annual PM2.5 NAAQS in 2005. In addition, following implementation of the annual PM2.5 NAAQS, annual PM2.5 concentrations decreased by 1.59 μg/m3 (95% CI: 1.39, 1.80) which corresponded to a reduction in mortality rates among individuals 65 years and older (0.93% [95% CI: 0.10%, 1.77%]) in non-attainment counties relative to attainment counties. In a life expectancy study, Bennett et al. (2019) reports increases in life expectancy in all but 14 counties (1325 of 1339 counties) that have exhibited reductions in PM2.5 concentrations from 1999 to 2015. These studies provide support for improvements in public health following the implementation of policies, including in areas with PM2.5 concentrations below the level of the current annual standard, as well as increases in life expectancy in areas with reductions in PM2.5 concentrations.
d. Uncertainties in the Health Effects Evidence
The 2022 PA recognizes that there are a number of uncertainties and limitations associated with the available health effects evidence. Although the epidemiologic studies clearly demonstrate associations between long- and short-term PM2.5 exposures and health outcomes, several uncertainties and limitations in the health effects evidence remain. Epidemiologic studies evaluating short-term PM2.5 exposure and health effects have reported heterogeneity in associations between cities and geographic regions within the U.S. Heterogeneity in the associations observed across epidemiologic studies may be due in part to exposure error related to measurement-related issues, the use of central fixed-site monitors to represent population exposure to PM2.5, and a limited understanding of factors including exposure error related to measurement-related issues, variability in PM2.5 composition regionally, and factors that result in differential exposures ( e.g., topography, the built environment, housing characteristics, personal activity patterns). Heterogeneity is expected when the methods or the underlying distribution of covariates vary across studies (U.S. EPA, 2019a, p. 6–221). Studies assessed in the 2019 ISA and ISA Supplement have advanced the state of exposure science by presenting innovative methodologies to estimate PM exposure, detailing new and existing measurement and modeling methods, and further informing our understanding of the influence of exposure measurement error due to exposure estimation methods on the associations between PM2.5 and health effects reported in epidemiologic studies (U.S. EPA, 2019a, section 1.2.2; U.S. EPA, 2022a). Data from PM2.5 monitors continue to be commonly used in health studies as a surrogate for PM2.5 exposure, and often provide a reasonable representation of exposures throughout a study area (U.S. EPA, 2019a, section 3.4.2.2; U.S. EPA, 2022a, section 3.2.2.2.2). However, an increasing number of studies employ hybrid modeling methods to estimate PM2.5 exposure using data from several sources, often including satellites and models, in addition to ground-based monitors. These hybrid models typically have good cross-validation, especially for PM2.5, and have the potential to reduce exposure measurement error and uncertainty in the health effect estimates from epidemiologic models of long-term exposure (U.S. EPA, 2019a, section 3.5; U.S. EPA, 2022a, section 2.3.3).
While studies using hybrid modeling methods have reduced exposure measurement error and uncertainty in the health effect estimates, these studies use a variety of approaches to estimate PM2.5 concentrations and to assign exposure to assess the association between health outcomes and PM2.5 exposure. This variability in methodology has inherent limitations and uncertainties, as described in more detail in section 2.3.3.1.5 of the 2022 PA, and the performance of the modeling approaches depends on the availability of monitoring data which varies by location. Factors that likely contribute to poorer model performance often coincide with relatively low ambient PM2.5 concentrations, in areas where predicted exposures are at a greater distance to monitors, and under conditions where the reliability and availability of key datasets ( e.g., air quality modeling) are limited. Thus, uncertainty in hybrid model predictions becomes an increasingly important consideration as lower predicted concentrations are considered.
Regardless of whether a study uses monitoring data or a hybrid modeling approach when estimating PM2.5 exposures, one key limitation that persists is associated with the interpretation of the study-reported mean PM2.5 concentrations and how they compare to design values, the metric that describes the air quality status of a given area relative to the NAAQS.[86] As discussed above in section II.B.3.b, the overall mean PM2.5 concentrations reported by key epidemiologic studies reflect averaging of short- or long-term PM2.5 exposure estimates across location ( i.e., across multiple monitors or across modeled grid cells) and over time ( i.e., over several years). For monitor-based studies, the comparison is somewhat more straightforward than for studies that use hybrid modeling methods, as the monitors used to estimate exposure in the epidemiologic studies are generally the same monitors that are used to calculate design values for a given area. It is expected that areas meeting a PM2.5 standard with a particular level would be expected to have average PM2.5 concentrations ( i.e., averaged across space and over time in the area) somewhat below that standard level., but the difference between the maximum annual design value and Start Printed Page 16249 average concentration in an area can be smaller or larger than analyses presented above in section I.D.5.a, likely depending on factors such as the number of monitors, monitor siting characteristics, and the distribution of ambient PM2.5 concentrations. For studies that use hybrid modeling methods to estimate PM2.5 concentrations, the comparison between study-reported mean PM2.5 concentrations and design values is more complicated given the variability in the modeling methods, temporal scales ( i.e., daily versus annual), and spatial scales ( i.e., nationwide versus urban) across studies. Analyses above in section I.D.5.b and detailed more in the 2022 PA (U.S. EPA, 2022b, section 2.3.3.2.4) present a comparison between two hybrid modeling surfaces, which explored the impact of these factors on the resulting mean PM2.5 concentrations and provided additional information about the relationship between mean concentrations from studies using hybrid modeling methods and design values. However, the results of those analyses only reflect two surfaces and two types of approaches, so uncertainty remains in understanding the relationship between estimated modeled PM2.5 concentrations and design values more broadly across hybrid modeling studies. Moreover, this analysis was completed using two hybrid modeling methods that estimate PM2.5 concentrations in the U.S., thus an additional uncertainty includes understanding the relationship between modeled PM2.5 concentrations and design values reported in Canada.
In addition, where PM2.5 and other pollutants ( e.g., ozone, nitrogen dioxide, and carbon monoxide) are correlated, it can be difficult to distinguish whether attenuation of effects in some studies results from copollutant confounding or collinearity with other pollutants in the ambient mixture (U.S. EPA, 2019a, section 1.5.1; U.S. EPA, 2022a, section 2.2.1). Studies evaluated in the 2019 ISA and ISA Supplement further examined the potential confounding effects of both gaseous and particulate copollutants on the relationship between long- and short-term PM2.5 exposure and health effects. As noted in the Appendix to the 2019 ISA (U.S. EPA, 2019a, Table A–1), copollutant models are not without their limitations, such as instances for which correlations are high between pollutants resulting in greater copollutant confounding bias in results. However, the studies continue to provide evidence indicating that associations with PM2.5 are relatively unchanged in copollutants models (U.S. EPA, 2019a, section 1.5.1; U.S. EPA, 2022a, section 2.2.1).
Another area of uncertainty is associated with other potential confounders, beyond copollutants. Some studies have expanded the examination of potential confounders to not only include copollutants, but also systematic evaluations of the potential impact of inadequate control from long-term temporal trends and weather (U.S. EPA, 2019a, section 11.1.5.1). Analyses examining these covariates further confirm that the relationship between PM2.5 exposure and mortality is unlikely to be biased by these factors. Other studies have explored the use of alternative methods for confounder control to more extensively account for confounders and are more robust to model misspecification that can further inform the causality determination for long-term and short-term PM2.5 and mortality and cardiovascular effects (U.S. EPA, 2019a, section 11.2.2.4; U.S. EPA, 2022a, sections 3.1.1.3, 3.1.2.3, 3.2.1.2, and 3.2.2.3). These studies indicate that bias from unmeasured confounders can occur in either direction, although controlling for these confounders did not result in the elimination of the association, but instead provided additional support for associations between long-term PM2.5 exposure and mortality when accounting for additional confounders (U.S. EPA, 2022a, section 3.2.2.2.6).
Another important limitation associated with the evidence is that, while epidemiologic studies indicate associations between PM2.5 and health effects, the currently available evidence does not identify particular PM2.5 concentrations that do not elicit health effects. Rather, health effects can occur over the entire distribution of ambient PM2.5 concentrations evaluated, and epidemiologic studies conducted to date do not identify a population-level threshold below which it can be concluded with confidence that PM2.5 -related effects do not occur.
Overall, evidence assessed in the 2019 ISA and ISA Supplement continues to indicate a linear, no-threshold C–R relationship for PM2.5 concentrations >8 μg/m3 . However, uncertainties remain about the shape of the C–R curve at PM2.5 concentrations <8 μg/m3 , with some recent studies providing evidence for either a sublinear, linear, or supralinear relationship at these lower concentrations (U.S. EPA, 2019a, section 11.2.4; U.S. EPA, 2022a, section 2.2.3.2).
There are also a number of uncertainties and limitations associated with the experimental evidence ( i.e., controlled human exposure studies and animal toxicological studies). With respect to controlled human exposure studies, the PA recognizes that these studies include a small number of individuals compared to epidemiologic studies. Additionally, these studies tend to include generally healthy adult individuals, who are at a lower risk of experiencing health effects. These studies, therefore, often do not include populations that are at increased risk of PM2.5 -related health effects, including children, older adults, or individuals with pre-existing conditions. As such, these studies are somewhat limited in their ability to inform at what concentrations effects may be elicited in at-risk populations. With respect to animal toxicological studies, while these studies often examine more severe health outcomes and longer exposure durations and higher exposure concentrations than controlled human exposure studies, there is uncertainty in extrapolating the effects seen in animals, and the PM2.5 exposures and doses that cause those effects, to human populations.
Consideration of health effects are informed by the epidemiologic, controlled human exposure, and animal toxicological studies. The evaluation and integration of the scientific evidence in the ISA focuses on evaluating the findings from the body of evidence across disciplines, including evaluating the strengths and weaknesses in the overall collection of studies across disciplines. Integrating evidence across disciplines can strengthen causal inference, such that a weak inference from one line of evidence can be addressed by other lines of evidence, and coherence of these lines of evidence can add support to a cause-effect interpretation of the association. Evaluation and integration of the evidence also includes consideration of uncertainties that are inherent in the scientific findings (U.S. EPA, 2015, pp. 13–15), some of which are described above.
3. Summary of Exposure and Risk Estimates
Beyond the consideration of the scientific evidence, discussed above in section II.B, the EPA also considers the extent to which new or updated quantitative analyses of PM2.5 air quality, exposure, or health risks could inform conclusions on the adequacy of the public health protection provided by the current primary PM2.5 standards. Additionally, the 2022 PA includes an at-risk analysis that assesses PM2.5 -attributable risk associated with PM2.5 air quality that has been adjusted to simulate air quality scenarios of policy Start Printed Page 16250 interest ( e.g., “just meeting” the current or potential alternative standards). Drawing on the summary in section II.C of the proposal, the sections below provide a brief overview of key aspects of the assessment design (II.A.3.a), key limitations and uncertainties (II.A.3.b), and exposure/risk estimates (II.A.3.c).
a. Key Design Aspects
Risk assessments combine data from multiple sources and involve various assumptions and uncertainties. Input data for these analyses includes C–R functions from epidemiologic studies for each health outcome and ambient annual or 24-hour PM2.5 concentrations for the study areas utilized in the risk assessment (U.S. EPA, 2022b, section 3.4.1). Additionally, quantitative and qualitative methods were used to characterize variability and uncertainty in the risk estimates (U.S. EPA, 2022b, section 3.4.1.7).
Concentration-response functions used in the risk assessment are from large, multicity U.S. epidemiologic studies that evaluate the relationship between PM2.5 exposures and mortality. Epidemiologic studies and concentration-response studies that were used in the risk assessment to estimate risk were identified using criteria that take into account factors such as study design, geographic coverage, demographic populations, and health endpoints (U.S. EPA, 2022b, section 3.4.1.1).[87] The risk assessment focuses on all-cause or nonaccidental mortality associated with long-term and short-term PM2.5 exposures, for which the 2019 ISA concluded that the evidence provides support for a “causal relationship” (U.S. EPA, 2022b, section 3.4.1.2).[88]
As described in more detail in the 2022 PA, the risk assessment first estimated health risks associated with air quality for 2015 adjusted to simulate “just meeting” the current primary PM2.5 standards ( i.e., the annual standard with its level of 12.0 µg/m3 and the 24-hour standard with its level of 35 µg/m3 ). Air quality modeling was then used to simulate air quality just meeting an alternative standard with a level of 10.0 µg/m3 (annual) and 30 µg/m3 (24-hour). In addition to the model-based approach, for the subset of 30 areas controlled by the annual standard linear interpolation and extrapolation were employed to simulate just meeting alternative annual standards with levels of 11.0 (interpolated between 12.0 and 10.0 μg/m3 ), 9.0 μg/m3 , and 8.0 μg/m3 (both extrapolated from 12.0 and 10.0 μg/m3 ) (U.S. EPA, 2022b, section 3.4.1.3). The 2022 PA notes that there is greater uncertainty regarding whether a revised 24-hour standard ( i.e., with a lower level) is needed to further limit “peak” PM2.5 concentration exposure and whether a lower 24-hour standard level would most effectively reduce PM2.5 -associated health risks associated with “typical” daily exposures. The risk assessment estimates health risks associated with air quality adjusted to meet a revised 24-hour standard with a level of 30 µg/m3 , in conjunction with estimating the health risks associated with meeting a revised annual standard with a level of 10.0 µg/m3 (U.S. EPA, 2022b, section 3.4.1.3). More details on the air quality adjustment approaches used in the risk assessment are described in section 3.4.1.4 and Appendix C of the 2022 PA (U.S. EPA, 2022b).
When selecting U.S. study areas for inclusion in the risk assessment, the available ambient monitors, geographic diversity, and ambient PM2.5 air quality concentrations were taken into consideration (U.S. EPA, 2022b, section 3.4.1.4). When these factors were applied, 47 urban study areas were identified, which include nearly 60 million people aged 30–99, or approximately 30% of the U.S population in this age range (U.S. EPA, 2022b, section 3.4.1.5, Appendix C, section C.1.3). Of the 47 study areas, there were 30 study areas where just meeting the current standards is controlled by the annual standard,[89] 11 study areas where just meeting the current standards is controlled by the daily standard,[90] and 6 study areas where the controlling standard differed depending on the air quality adjustment approach (U.S. EPA, 2022b, section 3.4.1.5).[91]
In addition to the overall risk assessment, the 2022 PA also includes an at-risk analysis and estimates exposures and health risks of specific populations identified as at-risk that would be allowed under the current and potential alternative standards to further inform the Administrator's conclusions regarding the adequacy of the public health protection provided by the current primary PM2.5 standards. In so doing, the 2022 PA evaluates exposure and PM2.5 mortality risk for older adults ( e.g., 65 years and older), stratified for White, Black, Asian, Native American, Non-Hispanic, and Hispanic individuals residing in the same study areas included in the overall risk assessment. This analysis utilizes a recent epidemiologic study that provides race- and ethnicity-specific risk coefficients (Di et al., 2017b).
b. Key Limitations and Uncertainties
Uncertainty in risk estimates ( e.g., in the size of risk estimates) can result from a number of factors, including the assumptions about the shape of the C–R function with mortality at low ambient PM concentrations, the potential for confounding and/or exposure measurement error in the underlying epidemiologic studies, and the methods used to adjust PM2.5 air quality. More specifically, the use of air quality modeling to adjust PM2.5 concentrations are limited as they rely on model predictions, are based on emission changes scaled by fixed percentages, and use only two of the full set of possible emission scenarios and linear interpolation/extrapolation to adjust air quality that may not fully capture potential non-linearities associated with real-world changes in air quality. Additionally, the selection of case study areas is limited to urban areas predominantly located CA and in the Eastern U.S. that are controlled by the annual standard. While the risk assessment does not report quantitative uncertainty in the risk estimates as exposure concentrations are reduced, it does provide information on the distribution of concentrations associated with the risk estimates when evaluating progressively lower alternative annual standards. Based on these data, as lower alternative annual standards are evaluated, larger proportions of the distributions in risk occur at or below 10 μg/m3 (at concentrations below or near most of the study-reported means from the key U.S. epidemiologic studies) and at or below 8 μg/m3 (the concentration at which the ISA reports increasing uncertainty in the shape of the C–R curve based on the body of epidemiologic evidence). Start Printed Page 16251
Similarly, the at-risk analysis is also subject to many of these same uncertainties noted above. Additionally, the at-risk analysis included C–R functions from only one study (Di et al., 2017b), which reported associations between long-term PM2.5 exposures and mortality, stratified by race/ethnicity, in populations age 65 and older, as opposed to the multiple studies used in the overall risk assessment to convey risk estimate variability. These and other sources of uncertainty in the overall risk assessment and the at-risk analyses are characterized in more depth in the 2022 PA (U.S. EPA, 2022b, section 3.4.1.7, section 3.4.1.8, Appendix C, section C.3).
c. Summary of Risk Estimates
Although limitations in the underlying data and approaches lead to some uncertainty regarding estimates of PM2.5 -associated risk, the risk assessment estimates that the current primary PM2.5 standards could allow a substantial number of PM2.5 -associated deaths in the U.S. For example, when air quality in the 47 study areas is adjusted to simulate just meeting the current standards, the risk assessment estimates up to 45,100 deaths in 2015 are attributable to long-term PM2.5 exposures associated with just meeting the current annual and 24-hour PM2.5 standards (U.S. EPA, 2022b, section 3.4.2.1). Additionally, as described in more detail in the 2022 PA, the at-risk analysis suggests that a lower annual standard level ( i.e., below 12 µg/m3 and down as low as 8 µg/m3 ) will help to reduce PM2.5 exposure and may also help to mitigate exposure and risk disparities in populations identified as particularly at-risk for adverse effects from PM exposures ( i.e., minority populations).
Compared to the current annual standard, meeting a revised annual standard with a lower level is estimated to reduce PM2.5 -associated health risks in the 30 study areas controlled by the annual standard by about 7–9% for a level of 11.0 µg/m3 , 15–19% for a level of 10.0 µg/m3 , 22–28% for a level of 9.0 µg/m3 , and 30–37% for a level of 8.0 µg/m3 ) (U.S. EPA, 2022b, Table 3–17). Meeting a revised annual standard with a lower level may also help to mitigate exposure and risk disparities in populations identified as particularly at-risk for adverse effects from PM exposures ( i.e., minority populations) in simulated scenarios just meeting alternative annual standards. However, though reduced, disparities by race and ethnicity persist even at an alternative annual standard level of 8 µg/m3 , the lowest alternative annual standard included in the risk assessment (U.S. EPA, 2022b, section 3.4.2.4).
Revising the level of the 24-hour standard to 30 μg/m3 is estimated to lower PM2.5 -associated risks across a more limited population and number of areas than revising the annual standard (U.S. EPA, 2022, section 3.4.2.4). Risk reduction predictions are largely confined to areas located in the western U.S., several of which are also likely to experience risk reductions upon meeting a revised annual standard. In the 11 areas controlled by the 24-hour standard, when air quality is simulated to just meet the current 24-hour standard, PM2.5 exposures are estimated to be associated with as many as 2,570 deaths annual. Compared to just meeting the current standard, air quality just meeting an alternative 24-hour standard level of 30 µg/m3 is associated with reductions in estimated risk of 9–13% (U.S. EPA, 2022b, section 3.4.2.3).
B. Conclusions on the Primary PM2.5 Standards
In drawing conclusions on the adequacy of the current primary PM2.5 standards, in view of the advances in scientific knowledge and additional information now available, the Administrator has considered the evidence base, information, and policy judgments that were the foundation of the 2012 and 2020 reviews and reflects upon the body of evidence and information newly available in this reconsideration. In so doing, the Administrator has taken into account both evidence-based and risk-based considerations, as well as advice from the CASAC and public comments. Evidence-based considerations draw upon the EPA's integrated assessment of the scientific evidence of health effects related to PM2.5 exposure presented in the 2019 ISA and ISA Supplement (summarized in the proposal in sections II.B (88 FR 5580, January 27, 2023) and II.D.2.a (88 FR 5609, January 27, 2023), and also in section II.A.2 above) to address key policy-relevant questions in the reconsideration. Similarly, the risk-based considerations draw upon the assessment of population exposure and risk (summarized in the proposal in sections II.C (88 FR 5605, January 27, 2023) and II.D.2.b (88 FR 5614, January 27, 2023), and also in section II.A.3 above) in addressing policy-relevant questions focused on the potential for PM2.5 exposures associated with mortality under air quality conditions just meeting the current and potential alternative standards.
The approach to reviewing the primary standards is consistent with requirements of the provisions of the CAA related to the review of the NAAQS and with how the EPA and the courts have historically interpreted the CAA. As discussed in section I.A above, these provisions require the Administrator to establish primary standards that, in the Administrator's judgment, are requisite ( i.e., neither more nor less stringent than necessary) to protect public health with an adequate margin of safety. Consistent with the Agency's approach across all NAAQS reviews, the EPA's approach to informing these judgments is based on a recognition that the available health effects evidence generally reflects a continuum that includes ambient air exposures for which scientists generally agree that health effects are likely to occur through lower levels at which the likelihood and magnitude of response become increasingly uncertain. The CAA does not require the Administrator to establish a primary standard at a zero-risk level or at background concentration levels, but rather at a level that reduces risk sufficiently so as to protect public health, including the health of sensitive groups, with an adequate margin of safety.
The decisions on the adequacy of the current primary PM2.5 standards described below is a public health policy judgment by the Administrator that draws on the scientific evidence for health effects, quantitative analyses of population exposures and/or health risks, and judgments about how to consider the uncertainties and limitations that are inherent in the scientific evidence and quantitative analyses. The four basic elements of the NAAQS ( i.e., indicator, averaging time, form, and level) have been considered collectively in evaluating the public health protection afforded by the current standards.
Section II.B.2 below briefly summarizes the basis for the Administrator's proposed decision, drawing from section II.D.3 of the proposal (88 FR 5617, January 27, 2023). The advice and recommendations of the CASAC and public comments on the proposed decision are addressed below in sections II.B.1 and II.B.3, respectively. The Administrator's final conclusions in this reconsideration regarding the adequacy of the current primary PM2.5 standards and whether any revisions are appropriate are described in section II.B.4.
1. CASAC Advice
As part of its review of the 2019 draft PA, the CASAC provided advice on the adequacy of the public health protection afforded by the current primary PM2.5 standards. Its advice is documented in Start Printed Page 16252 a letter sent to the EPA Administrator (Cox, 2019b). In this letter, the committee recommended retaining the current 24-hour PM2.5 standard but did not reach consensus on whether the scientific and technical information support retaining or revising the current annual standard. In particular, though the CASAC agreed that there is a long-standing body of health evidence supporting relationships between PM2.5 exposures and various health outcomes, including mortality and serious morbidity effects, individual CASAC members “differ[ed] in their assessments of the causal and policy significance of these associations” (Cox, 2019b, p. 8 of consensus responses). Drawing from this evidence, “some CASAC members” expressed support for retaining the current annual standard while “other members” expressed support for revising that standard in order to increase public health protection (Cox, 2019b, p.1 of letter). These views are summarized below.
The CASAC members who supported retaining the current annual standard expressed the view that substantial uncertainty remains in the evidence for associations between PM2.5 exposures and mortality or serious morbidity effects. These committee members asserted that “such associations can reasonably be explained in light of uncontrolled confounding and other potential sources of error and bias” (Cox, 2019b, p. 8 of consensus responses). They noted that associations do not necessarily reflect causal effects, and they contended that recent epidemiologic studies assessed in the 2019 ISA that report positive associations at lower estimated exposure concentrations mainly confirm what was anticipated or already assumed in setting the 2012 NAAQS. In particular, they concluded that such studies have some of the same limitations as prior studies and do not provide new information calling into question the existing standard. They further asserted that “accountability studies provide potentially crucial information about whether and how much decreasing PM2.5 causes decreases in future health effects” (Cox, 2019b, p. 10 of consensus responses), and they cited recent reviews ( i.e., Henneman et al., 2017; Burns et al., 2019) to support their position that in such studies, “reductions of PM2.5 concentrations have not clearly reduced mortality risks” (Cox, 2019b, p. 8 of consensus responses). Thus, the committee members who supported retaining the current annual standard advise that, “while the data on associations should certainly be carefully considered, this data should not be interpreted more strongly than warranted based on its methodological limitations” (Cox, 2019b, p. 8 of consensus responses).
These members of the CASAC further concluded that the quantitative risk assessment included in the 2019 draft PA does not provide a valid basis for revising the current standards. This conclusion was based on concerns that (1) “the risk assessment treats regression coefficients as causal coefficients with no justification or validation provided for this decision;” (2) the estimated regression concentration-response functions “have not been adequately adjusted to correct for confounding, errors in exposure estimates and other covariates, model uncertainty, and heterogeneity in individual biological (causal) [concentration-response] functions;” (3) the estimated concentration-response functions “do not contain quantitative uncertainty bands that reflect model uncertainty or effects of exposure and covariate estimation errors;” and (4) “no regression diagnostics are provided justifying the use of proportional hazards . . . and other modeling assumptions” (Cox, 2019b, p. 9 of consensus responses). These committee members also contended that details regarding the derivation of concentration-response functions, including specification of the beta values and functional forms, were not well-documented, hampering the ability of readers to evaluate these design details. Thus, these members “think that the risk characterization does not provide useful information about whether the current standard is protective” (Cox, 2019b, p. 11 of consensus responses).
Drawing from their evaluation of the evidence and the risk assessment in the 2019 draft PA, these committee members concluded that “the Draft PM PA does not establish that new scientific evidence and data reasonably call into question the public health protection afforded by the . . . 2012 PM2.5 annual standard” (Cox, 2019b, p.1 of letter).
In contrast, “[o]ther members of CASAC conclude[d] that the weight of the evidence, particularly reflecting recent epidemiology studies showing positive associations between PM2.5 and health effects at estimated annual average PM2.5 concentrations below the current standard, does reasonably call into question the adequacy of the 2012 annual PM2.5 [standard] to protect public health with an adequate margin of safety” (Cox, 2019b, p.1 of letter). The committee members who supported this conclusion noted that the body of health evidence for PM2.5 not only includes the repeated demonstration of associations in epidemiologic studies, but also includes support for biological plausibility established by controlled human exposure and animal toxicology studies. They pointed to recent studies demonstrating that the associations between PM2.5 and health effects occur in a diversity of locations, in different time periods, with different populations, and using different exposure estimation and statistical methods. They concluded that “the entire body of evidence for PM health effects justifies the causality determinations made in the Draft PM ISA” (Cox, 2019b, p. 8 of consensus responses).
The members of the CASAC who supported revising the current annual standard particularly emphasized recent findings of associations with PM2.5 in areas with average long-term PM2.5 concentrations below the level of the annual standard and studies that show positive associations even when estimated exposures above 12 μg/m3 are excluded from analyses. They found it “highly unlikely” that the extensive body of evidence indicating positive associations at low estimated exposures could be fully explained by confounding or by other non-causal explanations (Cox, 2019b, p. 8 of consensus responses). They additionally concluded that “the risk characterization does provide a useful attempt to understand the potential impacts of alternate standards on public health risks” (Cox, 2019b, p. 11 of consensus responses). These CASAC members concluded that the available evidence reasonably calls into question the protection provided by the current primary PM2.5 standards and supports revising the annual standard to increase that protection (Cox, 2019b).
As a part of this reconsideration, the CASAC reviewed the 2021 draft PA (developed to support the reconsideration as described in section I.C.5 above). As a part of their review of the 2021 draft PA, the CASAC provided advice on the adequacy of the current primary PM2.5 standards. The range of views summarized here generally reflects differing judgments as to the relative weight to place on various types of evidence, the risk-based information, and the associated uncertainties, as well as differing judgments about the importance of various PM2.5 -related health effects from a public health perspective.
In its comments on the 2021 draft PA, the CASAC stated that: “[o]verall the CASAC finds the Draft PA to be well- Start Printed Page 16253 written and appropriate for helping to `bridge the gap' between the agency's scientific assessments and quantitative technical analyses, and the judgments required of the Administrator in determining whether it is appropriate to retain or revise the National Ambient Air Quality Standards (NAAQS)” (Sheppard, 2022a, p. 1 of consensus letter). The CASAC also stated that the “[d]raft PA adequately captures and appropriately characterizes the key aspects of the evidence assessed and integrated in the 2019 ISA and Draft ISA Supplement of PM2.5 -related health effects” (Sheppard, 2022b, p. 2 of consensus letter). The CASAC also stated that “[t]he interpretation of the risk assessment for the purpose of evaluating the adequacy of the current primary PM2.5 annual standard is appropriate given the scientific findings presented” (Sheppard, 2022a, p. 2 of consensus letter).
With regard to the adequacy of the current primary annual PM2.5 standard, “all CASAC members agree that the current level of the annual standard is not sufficiently protective of public health and should be lowered” (Sheppard, 2022a, p. 2 of consensus letter). Additionally, “the CASAC reached consensus that the indicator, form, and averaging time should be retained, without revision” (Sheppard, 2022a, p. 2 of consensus letter). With regard to the level of the primary annual PM2.5 standard, the CASAC had differing recommendations for the appropriate range for an alternative level. The majority of the CASAC “judge[d] that an annual average in the range of 8–10 μg/m3 ” was most appropriate, while the minority of the CASAC members stated that “the range of the alternative standard of 10–11 μg/m3 is more appropriate” (Sheppard, 2022a, p. 16 of consensus responses). The CASAC did highlight, however, that “the alternative standard level of 10 μg/m3 is within the range of acceptable alternative standards recommended by all CASAC members, and that an annual standard below 12 μg/m3 is supported by a larger and coherent body of evidence” (Sheppard, 2022a, p. 16 of consensus responses).
In reaching conclusions on a recommended range of 8–10 μg/m3 for the primary annual PM2.5 standard, the majority of the CASAC placed weight on various aspects of the available scientific evidence and quantitative risk assessment information discussed in the 2021 draft PA (Sheppard, 2022a, p. 16 of consensus responses). In particular, these members cited recent U.S.- and Canadian-based epidemiologic studies that show positive associations between PM2.5 exposure and mortality with study-reported mean concentrations below 10 μg/m3 . Further, these members also noted that the lower portions of the air quality distribution ( i.e., concentrations below the mean) provide additional information to support associations between health effects and PM2.5 concentrations lower than the reported long-term mean concentration. In addition, the CASAC members recognized that the available evidence has not identified a threshold concentration, below which an association no longer remains, pointing to the conclusion in the draft ISA Supplement that the “evidence remains clear and consistent in supporting a no-threshold relationship, and in supporting a linear relationship for PM2.5 concentrations >8 μg/m3 ” (Sheppard, 2022a, p. 16 of consensus responses). Finally, these CASAC members placed weight on the at-risk analysis as providing support for protection of at-risk demographic groups, including minority populations.
In recommending a range of 10–11 μg/m3 for the primary annual PM2.5 standard, the minority of the CASAC emphasized that there were few key epidemiologic studies that reported positive and statistically significant health effects associations for PM2.5 air quality distributions with overall mean concentrations below 9.6 μg/m3 (Sheppard, 2022a, p. 17 of consensus responses). In so doing, the minority of the CASAC specifically noted the variability in the relationship between study-reported means and area annual design values based on the methods utilized in the studies, noting that design values are generally higher than area average exposure levels. Further, the minority of the CASAC stated that “uncertainties related to copollutants and confounders make it difficult to justify a recommendation below 10–11 μg/m3 ” (Sheppard, 2022a, p. 17 of consensus responses). Finally, the minority of the CASAC placed less weight on the risk assessment results, noting large uncertainties, including the approaches used for adjusting air quality to simulate just meeting the current and alternative standards.
With regard to the current primary 24-hour PM2.5 standard, in their review of the 2021 draft PA, the CASAC did not reach consensus regarding the adequacy of the public health protection provided by the current standard. As described further below, the majority of the CASAC members concluded “that the available evidence calls into question the adequacy of the current 24-hour standard” (Sheppard, 2022a, p. 3 of consensus letter), while the minority of the CASAC members agreed with “the EPA's preliminary conclusion [in the draft PA] to retain the current 24-hour PM2.5 standard without revision” (Sheppard, 2022a, p. 4 of consensus letter). The CASAC recommended that in future reviews, the EPA should also consider alternative forms for the primary 24-hour PM2.5 standard. Specifically, the CASAC “suggests considering a rolling 24-hour average and examining alternatives to the 98th percentile of the 3-year average,” pointing to concerns that computing 24-hour average PM2.5 concentrations using the current midnight-to-midnight timeframe could potentially underestimate the effects of high 24-hour exposures, especially in areas with wood-burning stoves and wintertime stagnation (Sheppard, 2022a, p. 18 of consensus responses).
As noted above, the majority of the CASAC favored revising the level of the primary 24-hour PM2.5 standard, suggesting that a range of 25–30 μg/m3 would be adequately protective. In so doing, the majority of the CASAC placed weight on the available epidemiologic evidence, including epidemiologic studies that restricted analyses to 24-hour PM2.5 concentrations below 25 μg/m3 . These members also placed weight on results of controlled human exposure studies with exposures close to the current standard, which they note provide support for the epidemiologic evidence to lower the standard. These members noted the limitations in using controlled human exposure studies alone in considering the adequacy of the 24-hour standard, recognizing that controlled human exposure studies preferentially recruit less susceptible individuals and have a typical exposure duration shorter than 24 hours. These members also placed “greater weight on the scientific evidence than on the values estimated by the risk assessment,” citing their concerns that the risk assessment “may not adequately capture areas with wintertime stagnation and residential wood-burning where the annual standard is less likely to be protective” (Sheppard, 2022a, p. 17 of consensus responses). Furthermore, these CASAC members “also are less confident that the annual standard could adequately protect against health effects of short-term exposures” (Sheppard, 2022a , p. 17 of consensus responses).
The minority of the CASAC agreed with the EPA's preliminary conclusion in the 2021 draft PA to retain the current primary 24-hour PM2.5 standard. In so doing, the minority of the CASAC placed greater weight on the risk assessment, noting that the risk Start Printed Page 16254 assessment accounts for both the level and the form of the current standard and the manner by which attainment with the standard is determined. Further, the minority of the CASAC stated that the “risk assessment indicates that the annual standard is the controlling standard across most of the urban study areas evaluated and revising the level of the 24-hour standard is estimated to have minimal impact on the PM2.5 -associated risks” and therefore, “the annual standard can be used to limit both long- and short-term PM2.5 concentrations” (Sheppard, 2022a, p. 18 of consensus responses). Further, the minority of the CASAC placed more weight on the controlled human exposure studies, which show “effects at PM2.5 concentrations well above those typically measured in areas meeting the current standards” and which suggest that “the current standards are providing adequate protection against these exposures” (Sheppard, 2022a, p. 18 of consensus responses).
While the CASAC members expressed differing opinions on the appropriate revisions to the current standards, they did “find that both primary standards, 24-hour and annual, are critical to protect public health given the evidence on detrimental health outcomes at both short-term and long-term exposures including peak events” (Sheppard, 2022a, p. 13 of consensus responses). The comments from the CASAC also took note of uncertainties that remain in this reconsideration of the primary PM2.5 standards and they identified a number of additional areas for future research and data gathering and dissemination that would inform future reviews of the primary PM2.5 NAAQS (Sheppard, 2022a, pp. 14–15 of consensus responses).
2. Basis for the Proposed Decision
In reaching his proposed decisions to revise the level of the primary annual PM2.5 standard from its current level of 12.0 µg/m3 to within the range of 9.0 to 10.0 µg/m3 , and to retain the current primary 24-hour PM2.5 standard (88 FR 5558, January 27, 2023), the Administrator carefully considered the assessment of the current evidence and conclusions reached in the 2019 ISA and ISA Supplement; the currently available exposure and risk information, including associated limitations and uncertainties, described in detail in the 2022 PA; the considerations and staff conclusions and associated rationales presented in the 2022 PA; the advice and recommendations from the CASAC; and public comments that had been offered up to that point (88 FR 5558, January 27, 2023).
In reaching his proposed conclusions on whether the currently available scientific evidence and quantitative risk-based information support or call into question the adequacy of the public health protection afforded by the current primary PM2.5 standards, and as is the case with NAAQS reviews in general, the extent to which the current primary PM2.5 standards are judged to be adequate will depend on a variety of factors, including science policy and public health policy judgments to be made by the Administrator on the strength and uncertainties of the scientific evidence. The factors relevant to judging the adequacy of the standards also include the interpretation of, and decisions as to the weight to place on, different aspects of the results of the risk assessment for the study areas included and the associated uncertainties. Thus, in reaching proposed conclusions of the current standards, the Administrator recognized that such a determination depends in part on judgments regarding aspects of the evidence and risk estimates, and judgments about the degree of protection that is requisite to protect public health with an adequate margin of safety.
The Administrator's full rationale for his proposed conclusions is presented in section II.D.3 of proposal (88 FR 5658, January 27, 2023), but is also briefly summarized here. In reaching the proposed decision to revise the annual standard level to 9–10 µg/m3 , the Administrator placed weight on the full body of scientific information. He noted that the 2019 ISA finds that exposure to PM2.5 causes mortality and cardiovascular effects and is likely to cause respiratory effects, cancer, and nervous system effects as detailed further in section II.B.1 of the proposal. As detailed further in section II.B.4 of the proposal, he additionally noted that the 2019 ISA identifies at-risk populations at greater risk of health effects from exposure to PM2.5, including children, older adults, people with pre-existing respiratory or cardiovascular disease, minority populations, and low socioeconomic status (SES) populations.
The Administrator also recognized that epidemiologic studies provide the strongest scientific evidence when evaluating the adequacy of the level of the annual standard. He noted that there is no specific point in the air quality distribution of any epidemiologic study that represents a `bright line' at and above which effects have been observed and below which effects have not been observed. In his proposed decision, he noted previous decision-making frameworks, which placed weight on values at or near the study-reported mean PM2.5 concentrations, which is where the most confidence in the reported association of the epidemiologic study exists. He further noted that there are a number of epidemiologic studies available in this reconsideration that use new PM2.5 exposure estimation techniques ( e.g., hybrid modeling) that were not used in epidemiologic studies that were available in previous reviews. These recent epidemiologic studies that use new exposure estimation techniques report long-term mean PM2.5 concentrations that are well below corresponding design values, which is an important consideration in reaching decisions on the level of the annual PM2.5 standard.
In reaching his proposed decision, the Administrator noted that a level of 9–10 µg/m3 would near or below the reported 25th percentiles in key U.S. based epidemiologic studies, while also recognizing that he has less confidence in the magnitude and significance of the association at even lower percentiles ( e.g., 10th percentile), where even fewer health events are observed. The Administrator also noted that a proposed level of 9–10 µg/m3 would be near the mean PM2.5 reported in Canadian based studies, though he also recognized that there are a number of factors associated with the studies in Canada ( e.g., exposure environments) that make it more difficult to compare mean concnetrations from Canadian studies to design values, which determine compliance with the standard in the U.S.
The Administrator took note of additional pieces of scientific evidence, which were not available in previous reviews, including restricted analyses, which support that the association seen in epidemiologic studies does not just occur from the peaks of the exposure distribution. Additionally, he notes that a level of 9–10 µg/m3 would be below the starting concentration in newly available accountability studies, though he did note that it is more difficult to interpret these studies in the context of selecting the level of the annual PM2.5 standard.
Further, the Administrator took into consideration the advice of the CASAC, noting that all members included 10 µg/m3 in their recommended range, and that the proposed range of 9–10 µg/m3 for the level of the primary annual PM2.5 standard was within the range recommended by the majority of the CASAC.
In reaching the proposed conclusion of a range between 9–10 µg/m3 , the Administrator noted that a level as high Start Printed Page 16255 as 11 µg/m3 might not provide an adequate margin of safety, given that 11 µg/m3 was well above many of the epidemiologic study-reported mean PM2.5 concentrations. Additionally, the Administrator noted the uncertainties associated with the scientific and quantitative information supporting a level as low as 8 µg/m3 , which call into question the potential public health improvements of a standard below 9 µg/m3 . The Administrator specifically noted the lack of key U.S. studies with mean concentrations below 9.3 µg/m3 and he further noted that the risk assessment suggests that the risk remaining under a standard of 8 µg/m3 would occur at very low concentrations ( e.g., mainly 7 µg/m3 and below).
As such, the Administrator's proposed decision noted that the current PM2.5 annual standard did not adequately provide requisite protection against exposures to PM2.5 and that a proposed range of 9–10 µg/m3 would provide an adequate margin of safety.
In his proposed decision to retain the current primary 24-hour PM2.5 standard with a level of 35 µg/m3 , the Administrator first considered the scientific information related to short-term exposures to PM2.5 and health effects. He noted that the controlled human exposure studies are the strongest line of evidence for informing his conclusions regarding the adequacy of the current 24-hour standard. In so doing, the Administrator recognized that controlled human exposure studies are conducted with healthy adult volunteers and that these studies do not include individuals who may be at increased risk of PM2.5 -related health effects ( i.e., children, older adults, people with pre-existing diseases). He also noted that the effects observed in the controlled human exposure studies ( e.g., changes in vascular function) are not effects that are judged to be clearly adverse. He recognized the most consistent evidence of effects in these studies occurs at higher concentrations ( e.g., >120 µg/m3 ) following 1–5 hour exposures, and that one study observed effects at concentrations as low as 38 µg/m3 following 4-hour exposures. However, the Administrator reiterated that these studies do not tell us at exactly what concentrations an adverse effect might occur, especially for at-risk populations. As noted above in section II.A.2.c, controlled human exposure studies tend to include generally healthy adult individuals who are at a lower risk of experiencing health effects, and often do not include at-risk populations ( e.g., children, older adults, or individuals with pre-existing conditions). As such, the Administrator recognized that these studies are somewhat limited in their ability to inform at what concentrations effects may be elicited in in at-risk populations. The Administrator also considered air quality analyses in the 2022 PA that demonstrate that there will be very few, if any, days with PM2.5 concentrations at levels evaluated in controlled human exposure studies that are associated with effects in areas that meet the current primary 24-hour PM2.5 standard.
The Administrator also noted that as, in previous PM NAAQS reviews, the protection provided by the suite of standards ( e.g., annual and 24-hour standards) is evaluated together. He noted that the annual standard is the controlling standard in most areas of the country. He also considered air quality analyses in the 2022 PA that suggest that revision of the annual standard to a level between 9–10 µg/m3 would also control 24-hour PM2.5 concentrations in most areas to, or below, 30 µg/m3 . Finally, the Administrator noted the agreement with the advice from the minority of CASAC and additionally noted the limited rationale and evidence provided by the majority CASAC's recommendation to support revision of the 24-hour standard. As such, the Administrator proposed to retain the current 24-hour standard with its level of 35 µg/m3 .
Additionally, the Administrator proposed to conclude that it is appropriate to retain all other elements ( i.e., indicator, averaging time, and form) of the annual and 24-hour standards.
3. Comments on the Proposed Decision
With respect to the adequacy of the primary annual PM2.5 standard, a number of commenters, primarily those from industry and industry groups, non-governmental organizations, and some State and local governments, disagree with the EPA's proposed decision to revise the level of the primary annual PM2.5 standard. These commenters generally expressed the view that the current standards provide the requisite degree of public health protection and should be retained, consistent with the 2020 final decision. In supporting their view, these commenters assert that the scientific evidence available in this reconsideration is essentially unchanged since the 2020 final decision and that the additional scientific evidence and quantitative risk information available for the reconsideration does not support strengthening the primary annual PM2.5 standard. These commenters also assert that uncertainties associated with the available scientific evidence have not changed since the 2020 final decision, and they note that these uncertainties were essential factors in the then-Administrator's decision to retain the primary annual PM2.5 standard. These commenters argue that, while the current Administrator acknowledges these uncertainties, he does not place enough weight on them in reaching his conclusions regarding the current standard. The commenters specifically highlight uncertainties related to exposure misclassification, confounding, and other sources of potential bias, which they claim supports retaining the current level of the annual standard. These commenters also note that these uncertainties were emphasized by the minority of the CASAC in their review of the 2021 draft PA, and the commenters further suggest that the lack of consensus from the CASAC on the appropriate level for the primary annual PM2.5 standard show that the research is unclear. The commenters contend that there is not support in this reconsideration for deviating from the then-Administrator's decision in 2020.
In contrast, other commenters, primarily from public health and environmental organizations, some State and local elected representatives, and some State and local government agencies agree with the EPA's proposed decision that the primary annual PM2.5 standard is not adequate. These commenters support revising the level of the primary annual PM2.5 standard and emphasize that the available scientific evidence, in particular epidemiologic studies, along with the CASAC's advice in their review for the 2021 draft PA, provide strong support for the proposed decision. In particular, these commenters agree with the EPA's conclusions about the strength of the scientific evidence, including uncertainties, and they emphasize that the CASAC reached consensus in their review of the 2021 draft PA that the current primary annual PM2.5 standard is not adequate. Some of these commenters also note that a revised primary annual PM2.5 standard would result in significant public health benefits by reducing morbidity and mortality associated with PM2.5 exposure, especially for at-risk populations.
The EPA agrees with commenters that the primary annual PM2.5 standard is not adequate. The EPA recognizes the longstanding body of health evidence supporting relationships between PM2.5 exposures (short- and long-term) and both mortality and serious morbidity effects. The evidence available in this reconsideration ( i.e., the studies Start Printed Page 16256 assessed in the 2019 ISA and ISA Supplement summarized above in section II.A.2.a) reaffirms, and in some cases strengthens, the conclusions from the 2009 ISA regarding the health effects of PM2.5 exposures. As noted above, epidemiologic studies demonstrate generally positive and often statistically significant associations between PM2.5 exposures and health effects. Such studies report associations between estimated PM2.5 exposures and non-accidental, cardiovascular, or respiratory mortality; cardiovascular or respiratory hospitalizations or emergency room visits; and other mortality/morbidity outcomes ( e.g., lung cancer mortality or incidence, asthma development). Recent experimental evidence, as well as evidence from epidemiologic panel studies, strengthens support for potential biological pathways through which PM2.5 exposures could lead to the serious effects reported in many population-level epidemiologic studies, including support for pathways that could lead to cardiovascular, respiratory, nervous system, and cancer-related effects. Moreover, these recent epidemiologic studies strengthen support for health effect associations at PM2.5 concentrations lower than in those evaluated in epidemiologic studies available at the time of previous reviews.
Additionally, as discussed in more detail in section I.C.5.b above, the ISA Supplement focused on studies that were most likely to inform decisions on the appropriate standard, but not to reassess areas that, based on the assessment of available science published since the cutoff date of the 2019 ISA and through 2021, were judged unlikely to have new information that would be useful for the Administrator's decision making. The ISA Supplement included U.S. and Canadian epidemiologic studies for health effect categories where the 2019 ISA concluded a causal relationship ( i.e., short- and long-term PM2.5 exposure and cardiovascular effects and mortality), as well as U.S. and Canadian epidemiologic studies that employed alternative methods for confounder control or conducted accountability analyses ( i.e., studies that examined the effect of a policy on reducing PM2.5 concentrations). These studies, summarized in section II.A.2.a above, examine both short- and long-term PM2.5 exposure and cardiovascular effects and mortality. Additionally, studies that employ alternative methods for confounder control, as described in II.A.2.a above and in Table 3–11 and of the 2022 PA (U.S. EPA, 2022b), use a variety of statistical methods to control for confounding bias. These studies consistently report positive associations, which further supports the broader body of epidemiologic evidence for both cardiovascular effects and mortality.
In addition, there are epidemiologic studies that provide supplemental information for consideration in reaching conclusions that the current suite of PM2.5 standards is not adequate. These studies include analyses that restrict annual average PM2.5 concentrations to concentrations below 12 µg/m3 and provide support for positive and statistically significant associations with mortality and cardiovascular morbidity at mean PM2.5 concentrations below the current level of the primary annual PM2.5 standard (described above in section II.A.2.c.ii and in Table 3–10 of the 2022 PA (U.S. EPA, 2022b)). Recent accountability studies that have starting annual PM2.5 concentrations at or below 12 µg/m3 suggest public health improvements may occur at concentrations below 12 µg/m3 . These studies indicate positive and statistically significant associations with mortality and morbidity ( e.g., cardiovascular hospital admissions) and reductions in PM2.5 concentrations in ambient air (described above in section II.A.2.c.ii and in Table 3–12 of the 2022 PA (U.S. EPA, 2022b)).
Thus, in considering the available scientific evidence to inform conclusions on the adequacy of the primary PM2.5 standards, the Administrator recognizes that the 2019 ISA and the ISA Supplement together provides a strong scientific foundation for concluding that the current primary PM2.5 standards are not adequate.
In addition to the scientific evidence above, the risk assessment estimates that the current primary annual PM2.5 standard could allow a substantial number of deaths in the U.S. Although the Administrator recognizes that while the risk estimates can help to place the evidence for specific health effects into a broader public health context, they should be considered along with the inherent uncertainties and limitations of such analyses when informing judgments about the potential for additional public health protection associated with PM2.5 exposures and related health effects. The Administrator takes into consideration these uncertainties, which are described in more detail in section II.A.3.b above, but notes that the general magnitude of risk estimates supports the potential for significant public health impacts, particularly for lower alternative annual standard levels.
In the CASAC's review of the 2019 draft PA, the CASAC did not reach consensus on whether the current annual standard is adequate, with the majority of the CASAC recommending that the annual standard be retained and the minority of the CASAC recommending that the standard be revised. In their review of the 2021 draft PA, the CASAC unanimously recommended that the current annual standard is not sufficiently protective of public health (Sheppard, 2022a, p. 2 of consensus letter).
The EPA disagrees with the commenters who state that the available scientific and quantitative information available in this reconsideration does not provide support for the current Administrator to reach a different decision than the then-Administrator reached in the 2020 final action. The EPA agrees with these commenters that there are uncertainties associated with the currently available scientific evidence. The EPA has considered these uncertainties extensively both in reaching conclusions in the 2022 PA (U.S. EPA, 2022b, sections 3.4.3, 3.6.1, and 4.6.3) and in the proposal (88 FR 5604, 5609, January 27, 2023), and the EPA addresses more detailed public comments about these uncertainties, including those related to copollutant confounding, unmeasured confounding, and temporal and spatiotemporal confounding, in the Response to Comments document. However, we disagree with the commenters that the evidence does not provide support for the Administrator's conclusion that the current primary annual PM2.5 standard is not adequate to protect public health with an adequate margin of safety, and should be revised. As described above, epidemiologic studies in the 2019 ISA and the ISA Supplement support and extend the evidence evaluated in the 2009 ISA, through studies conducted in diverse populations and geographic locations, using various statistical models and approaches to control for potential confounders, and using a variety of exposure assessment methodologies. Therefore, the consistent, positive associations reported across studies (U.S. EPA, 2019a, Figures 11–1 and 11–18; U.S. EPA, 2022a) are unlikely to be to be the result of unmeasured confounding and other biases are unlikely to account for the consistent positive associations observed across epidemiologic studies.
Additionally, this reconsideration includes epidemiologic studies that were not before the then-Administrator for consideration in reaching his final decisions at the time of the 2020 decision and that specifically evaluate Start Printed Page 16257 confounding using alternative methods for confounder control). These recent epidemiologic studies provide support for the current Administrator's conclusion that the suite of primary PM2.5 standards are not adequate. While confounding was an uncertainty noted by the then-Administrator in the 2020 decision, he recognized “that methodological study designs to address confounding, such as causal inference methods, are an emerging field of study” (85 FR 82710, December 18, 2020). The ISA Supplement considered studies that employed statistical approaches that attempt to more extensively account for confounders and are more robust to model misspecification ( i.e., used alternative methods for confounder control),[92] given that such studies were highlighted by the CASAC in their review of the 2019 draft PA and identified in public comments on the 2020 proposal. Since the literature cutoff date for the 2019 ISA, multiple studies that employ alternative methods for confounder control have become available for consideration in the ISA Supplement and, subsequently, in this reconsideration. For example, one study before the Administrator in this reconsideration that was not available in the 2019 ISA is Schwartz et al. (2021), which used a causal modeling approach focused on exposure changes and controls for measured confounders by design in order to evaluate the association between long-term PM2.5 exposure and mortality in the Medicare population. The study authors found significant associations of PM2.5 with increased mortality rates using a causal modeling approach robust to omitted confounding. The results of this study and other studies in the ISA Supplement that employ alternative methods to control for confounders lend support to the robustness of positive associations between PM2.5 exposure and multiple morbidity and mortality endpoints exhibited across epidemiologic studies, and also indicate that unmeasured confounding and other biases are unlikely to account for the consistent positive associations observed across epidemiologic studies (U.S. EPA, 2022b, sections 3.1.1.3, 3.1.2.3, 3.2.1.3, and 3.2.2.3).
Further, the EPA disagrees with the commenters who argue that the Administrator did not appropriately consider the strengths and limitations of the health evidence in reaching his decision to revise the current primary annual PM2.5 standard in this reconsideration. In reaching his proposed decision, the Administrator considered the entire body of evidence and how to appropriately weigh the uncertainties associated with the health evidence (88 FR 5617, January 27, 2023). Such an approach is consistent with setting standards that are neither more nor less stringent than necessary, recognizing that “Congress provided that the Administrator is to use his judgment in setting air quality standards precisely to permit him to act in the face of uncertainty,” the Administrator must set standards on “the frontiers of scientific and medical knowledge” and “Congress directed the Administrator to err on the side of caution in making the necessary decisions .” Lead Indus. Ass'n, Inc. v. EPA, 647 F.2d 1130, 1155 & n.50 (D.C. Cir. 1980) (quoting H.R. Rep. No. 95–294, at 50). As such, a determination of identifying a specific level at which the standard should be set necessarily requires the Administrator's judgement ( e.g., weighing the uncertainties and margin of safety).
Additionally, the EPA disagrees with the commenters that contend that there is no basis in this reconsideration for deviating from the previous Administrator's decision in 2020. It is well-established that in CAA section 109 Congress specifically left the determination of the requisite NAAQS to the judgment of the Administrator and, moreover, that “decisions about the appropriate NAAQS level must `necessarily . . . rest largely on policy judgments.' ” Mississippi v. EPA, 744 F.3d 1344, 1357 (D.C. Cir. 2013) (quoting Lead Industries Ass'n v. EPA, 647 F.2d 1130, 1147 (D.C. Cir. 1980)). As the Court of Appeals for the D.C. Circuit has noted, “Every time EPA reviews a NAAQS, it (presumably) does so against contemporary policy judgments and the existing corpus of scientific knowledge.” Id., at 1343.
In this reconsideration, both the existing corpus of scientific knowledge as well as the Administrator's policy judgments about how to interpret and weigh that evidence to protect public health with an adequate margin of safety have changed. The expansion of the air quality criteria to encompass additional studies, information and analyses in the ISA Supplement and 2022 PA, as well as the additional consideration of the scientific record by the CASAC and the public provided the Administrator with significant additional information on which to base his decision.[93] In addition, in this reconsideration, the Administrator is reaching different judgments about how to weigh the epidemiologic evidence, including the uncertainties in the scientific evidence, and how to ensure an adequate margin of safety to protect against uncertain harms, compared to the approach in the 2020 final decision. For example, as discussed in greater detail above in section II.A.1 and in the 2020 notice of final rulemaking (85 FR 82717, December 18, 2020), in considering the epidemiologic evidence as part of his decision to retain the current primary annual PM2.5 standard in the 2020 decision, the then-Administrator placed weight on the mean of the study-reported means (or medians) ( i.e., 13.5 µg/m3 ) from key U.S. epidemiologic studies that are monitor-based being above the level of the current primary annual PM2.5 standard of 12.0 µg/m3 . By contrast, in this reconsideration, the current Administrator has taken an approach more similar to how the EPA has considered study-reported mean PM2.5 concentrations relative to the level of the primary annual PM2.5 standard in other recent PM NAAQS reviews. In so doing, in reaching his decision to revise the level of the primary annual PM2.5 standard to 9.0 µg/m3 , he is using an approach that places weight on selecting a level for the standard that is below the study-reported mean PM2.5 concentrations reported in key U.S. epidemiologic studies, including recent epidemiologic studies that use hybrid model-based methods, as well as being near or below the 25th percentile PM2.5 concentrations in those key U.S. epidemiologic studies that report these concentrations.
As such and further detailed in section II.B.4 below, in considering the adequacy of the current primary PM standards in this reconsideration, the Administrator has carefully considered the: (1) Policy-relevant evidence and conclusions contained in the 2019 ISA and 2022 ISA Supplement; (2) the quantitative information presented and Start Printed Page 16258 assessed in the 2022 PA; (3) the evaluation of this evidence, the quantitative information, and the rationale and conclusions presented in the 2022 PA; (4) the advice and recommendations from the CASAC; and (5) public comments. The Administrator concludes that the current suite of primary PM2.5 standards are not adequate to protect public health with an adequate margin of safety.
The four basic elements of the NAAQS (indicator, averaging time, form, and level) are considered collectively in evaluating the health protection afforded by a standard. The EPA received relatively few comments on the averaging time and form for the primary PM2.5 standards, but those who did provide comments on these elements were primarily from public health and environmental organizations, State and local elected representatives, and State and local government agencies. Some commenters assert that the current 24-hour averaging time for the primary 24-hour PM2.5 standard does not adequately protect against short-term peaks. These commenters further state that the 24-hour averaging time protects against chronic exposures but does not adequately protect against serious acute risks from certain sources such as prescribed burning. Also, a few commenters explicitly recommend that a subdaily averaging time would be more appropriate, although none of the commenters recommended a specific averaging time for consideration. Additionally, some commenters cite to the CASAC's advice in their review of the 2021 draft PA that future reviews of the PM NAAQS should include evaluation of alternative forms and averaging times of the current primary 24-hour PM2.5 standard.
The EPA disagrees with commenters that the current primary 24-hour PM2.5 standard, with its 24-hour averaging time, does not adequately protect against short-term peaks and disagrees that that there is sufficient information to conclude that a subdaily averaging time would be more appropriate than a 24-hour averaging time. The EPA has reviewed the currently available scientific evidence and finds that it does not indicate that alternative averaging times would be more appropriate for the primary PM2.5 standards. Accordingly, the EPA concludes that it is appropriate to retain both the annual and 24-hour averaging times for standards meant to protect against long- and short-term PM2.5.
As noted in the proposal, the 2019 ISA and ISA Supplement found that the scientific evidence continues to provide strong support for health effect associations with both long-term ( e.g., annual or multi-year) and short-term ( e.g., mostly 24-hour) exposures to PM2.5 . Epidemiologic studies continue to provide strong support for health effects associated with short-term PM2.5 exposures based on 24-hour PM2.5 averaging periods, and we note that subdaily effect estimates are less consistent and, in some cases, smaller in magnitude (88 FR 5618, January 27, 2023). Controlled human exposure and panel-based studies of subdaily exposures typically examine subclinical effects rather than the more serious population-level effects that have been reported to be associated with 24-hour exposures ( e.g., mortality, hospitalizations). Collectively, the 2019 ISA concludes that epidemiologic studies do not indicate that subdaily averaging periods are more closely associated with health effects than the 24-hour average exposure metric (U.S. EPA, 2019a, section 1.5.2.1). Additionally, the EPA notes that while recent controlled human exposure studies provide consistent evidence for cardiovascular effects following PM2.5 exposures for less than 24 hours ( i.e., <30 minutes to 5 hours), exposure concentrations in these studies are well-above the ambient concentrations typically measured in locations meeting the current standards (U.S. EPA, 2022a, section 3.3.3.1). Therefore, this information does not indicate that a revision to the averaging time is needed to provide additional protection against subdaily PM2.5 exposures, beyond that provided by the current primary standards. This conclusion is also supported by the advice given to EPA by the CASAC in their review of the 2021 draft PA, which reached consensus that averaging times for the standards should be retained, without revision (Sheppard, 2022a, p. 2 of consensus letter).[94] For all of these reasons, the Administrator concludes that the currently available evidence does not support considering alternatives to the annual and 24-hour averaging times for standards meant to protect against long- and short-term PM2.5 exposures.
Multiple commenters, primarily from public health and environmental organizations, recommend revising the form of the primary 24-hour PM2.5 standard to a 99th percentile to provide increased public health protection against peak PM2.5 exposures, particularly for at-risk populations. These commenters express concern that the current 98th percentile form allows 7 exceedances per year and contend that a 99th percentile form that would allow half that number is more appropriate. Commenters also cite to the CASAC's advice in their review of the 2021 draft PA, which recommended that the EPA consider alternative percentiles for the form of the primary 24-hour PM2.5 standard in the future.
The EPA disagrees that the current 98th percentile form does not provide the requisite public health protection against peak PM2.5 exposures and concludes that the 98th percentile, averaged over three years, remains appropriate for the primary 24-hour PM2.5 standard. As noted in previous reviews and in the proposal, the EPA has set both an annual standard and a 24-hour standard to provide protection from health effects associated with both long- and short-term exposures to PM2.5 (62 FR 38667, July 18, 1997; 88 FR 5620, January 27, 2023). With respect to the form of the 24-hour standard, as described just above, the epidemiologic studies continue to provide strong support for health effect associations with short-term ( e.g., mostly 24-hour) PM2.5 exposures and controlled human exposure studies provide evidence for health effects following single short-term “peak” PM2.5 exposures (88 FR 5619, January 27, 2023). Both the 98th and the 99th percentile form provide a very high degree of control of peak concentrations. As the commenters point out, a 99th percentile would reduce the number of allowable exceedances to four days per year. The EPA anticipates, however, that such a revision to the form would make the attainment status of an area more subject to change from unpredictable nonanthropogenic factors, such as meteorological events. The EPA has often noted that frequent shifts in attainment status that are unrelated to long-term air quality trends is inconsistent with providing a stable target for air quality planning and risk management programs, which in turn provides for the most effective public health protection in the long run (78 FR 3127, January 15, 2013; 80 FR 65351, October 26, 2015). Thus, the EPA's interest in an appropriate degree of stability is to ensure that the State air quality programs are effective in controlling pollution and that the public health protections of the standard are achieved. As discussed above, while recent controlled human exposure studies provide consistent evidence for cardiovascular effects following PM2.5Start Printed Page 16259 exposures for less than 24 hours ( i.e., < 30 minutes to 5 hours), exposure concentrations in these studies are well-above the ambient concentrations typically measured in locations meeting the current standards (U.S. EPA, 2022a, section 3.3.3.1), and the 98th percentile form is very effective at limiting occurrences of exposures of concern. Taking into consideration the available scientific information and quantitative information, the EPA therefore concludes that the 98th percentile form provides an appropriate balance between limiting the occurrence of peak 24-hour PM2.5 concentrations and identifying a stable target for risk management programs. This conclusion is also supported by the advice given to the EPA by the CASAC in their review of the 2021 draft PA, where they reached consensus that the form for the standards should be retained, without revision (Sheppard, 2022a, p. 2 of consensus letter).[95]
Additionally, the EPA recognizes the CASAC's advice in their review of the 2021 draft PA, where they recommended “that in future reviews, the EPA provide a more comprehensive assessment of the 24-hour standard that includes the form as well as the level” (Sheppard, 2022a, p. 4 of consensus letter). This advice is reflected in the proposal by the EPA, which noted “that it would be appropriate to gather additional air quality and scientific information and further consider these issues in future reviews” (88 FR 5619, January 27, 2023). The EPA will consider the information provided by the commenters regarding the form of the 24-hour PM2.5 standard in the next review of the PM NAAQS.
A number of commenters who support revising the level of the primary annual PM2.5 standard, particularly those who support a revised level of 8 µg/m3 , disagree with how the EPA has emphasized the mean PM2.5 concentrations reported in key epidemiologic studies to inform conclusions on the level of the primary PM2.5 standard. These commenters argue that, in this reconsideration, the EPA is arbitrarily emphasizing uncertainties in key epidemiologic studies in the focus on mean concentrations. Many of these commenters recommend that the EPA consider the full distribution of PM2.5 concentrations from the key epidemiologic studies in reaching conclusions on the appropriate level for the primary annual PM2.5 standards, in particular concentrations below the mean, such as the 25th percentile. In supporting this view, commenters point to the CASAC's advice in their review of the 2021 draft PA, where the majority of the CASAC stated that the “use of the mean to define where the data provide the most evidence is conservative since robust data clearly indicate effects below the mean in concentration-response functions” (Sheppard, 2022a, p. 16 of consensus responses), and that “[e]pidemiologic studies require consideration of distribution around the mean of exposure to identify effects and thus lower levels than the mean must be considered as part of the range where the data provide higher confidence” (Sheppard, 2022a, p. 13 of consensus responses).
As an initial matter, consistent with some previous approaches and as detailed by the Administrator in reaching conclusions on the level of the primary annual PM2.5 standard in section II.B.4 below, the EPA considers the long-term study-reported mean PM2.5 concentrations from key epidemiologic studies and sets the level of the standard to somewhat below the lowest long-term mean PM2.5 concentration. Additionally, as discussed further below, the EPA also considers the available information from a subset of epidemiologic studies that report exposure estimates or health events at the 25th and 10th percentiles of PM2.5 concentrations. The Administrator gives some weight to the 25th percentile data, although he recognizes that his confidence in the magnitude and significance in the reported concentrations, and their ability to inform decisions on the appropriate level of the annual standard, decreases with reduced data (below the mean) and diminishes further at percentiles that are even further below the mean and the 25th percentile. Therefore, the Administrator places weight on the reported 25th percentiles concentrations, rather than the reported 10th percentile concentrations, for the subset of studies that report lower percentile PM2.5 concentrations in reaching his conclusions regarding the appropriate level for the primary annual PM2.5 standard.
In considering the available scientific evidence to reach decisions on the adequacy of the suite of primary PM2.5 standards, the EPA notes that in previous PM NAAQS reviews (including the 1997, 2006 and 2012 reviews), evidence-based approaches were used that focused on identifying standard levels near or somewhat below long-term mean concentrations reported in key epidemiologic studies. These approaches were supported by the CASAC in previous reviews and were supported in this reconsideration by the CASAC in their review of the 2021 draft PA.[96]
In considering the available scientific evidence, the EPA notes the strength of the epidemiologic evidence which includes multiple studies that consistently report positive associations for short- and long-term PM2.5 exposures and mortality and cardiovascular effects. Some available studies also use a variety of statistical methods to control for confounding bias and report similar associations, which further supports the broader body of epidemiologic evidence for both mortality and cardiovascular effects. Additionally, the EPA notes that recent epidemiologic studies strengthen support for health effect associations at PM2.5 concentrations lower than in those evaluated in epidemiologic studies available at the time of previous reviews.
While these epidemiologic studies evaluate associations between distributions of ambient PM2.5 concentrations and health outcomes, they do not identify the specific exposures that led to the reported effects. As such, there is no specific point in the air quality distribution of any epidemiologic study that represents a “bright line” at and above which effects have been observed and below which effects have not been observed.
Studies of daily PM2.5 exposures examine associations between day-to-day variation in PM2.5 concentrations and health outcomes, often over several years. While there can be considerable variability in daily exposures over a multi-year study period, most of the estimated exposures reflect days with Start Printed Page 16260 ambient PM2.5 concentrations around the middle of the air quality distributions examined ( i.e., “typical” days rather than days with extremely high or extremely low concentrations). Similarly, for studies of annual PM2.5 exposures, most of the health events occur at estimated exposures that reflect annual average PM2.5 concentrations around the middle of the air quality distributions examined. In both cases, epidemiologic studies provide the strongest support for reported health effect associations for this middle portion of the PM2.5 air quality distribution, which corresponds to the bulk of the underlying data, rather than the extreme upper or lower ends of the distribution. Therefore, in the absence of discernible thresholds, long-term study-reported means—that is, the study-reported ambient PM2.5 concentrations in the epidemiologic studies that reflect estimated exposures with a focus around the middle portion of the PM2.5 air quality distribution where the bulk of the observed data reside—provide the strongest support for reported health effect associations in epidemiologic studies.
Based on the air quality criteria for this reconsideration, as described in the 2019 ISA, ISA Supplement, 2022 PA and the proposal, the EPA believes it is appropriate to continue to use the mean PM2.5 concentrations from the key epidemiologic studies to inform conclusions regarding the appropriate level for the primary annual PM2.5 standard.
There are a large number of key epidemiologic studies available in this reconsideration to inform conclusions regarding the level of the primary annual PM2.5 standard. For the key U.S. epidemiologic studies, the study-reported mean PM2.5 concentrations range from 9.9–16.5 μg/m3 for monitor-based studies (Figure 1 above) and range from 9.3–12.2 μg/m3 for hybrid modeling-based studies (Figure 2 above).
In addition to the study-reported mean PM2.5 concentrations, the EPA agrees with the CASAC's advice in their review of the 2021 draft PA and public comments that information on other percentiles below the mean can also be informative, and the EPA notes that the CASAC advised that for the purpose of informing the adequacy of the standards, future reviews should include an evaluation of other metrics, including the distribution of concentrations reported in epidemiologic studies (Sheppard, 2022a, p. 9 of consensus responses). As such, in reaching conclusions in this reconsideration, the EPA takes note of the additional study-reported PM2.5 concentrations below the means ( e.g., 25th and 10th percentiles) that are available from a limited subset of key U.S. epidemiologic studies. As shown in Figures 1 and 2 above, six key U.S. epidemiologic studies report information on other percentiles ( e.g., 10th and 25th percentiles of PM2.5 concentrations or 10th and 25th percentiles of PM2.5 concentrations associated with health events) that are below the mean.[97] Three of the studies are monitor-based and three are hybrid model-based.
The key U.S. epidemiologic studies that report percentiles below the mean that are monitor based are older studies. These studies included smaller numbers of people than the newer hybrid model-based studies. For the three older, monitor-based studies, because the cohorts were smaller in size, a relatively smaller portion of the health events were observed in the lower part of the air quality distribution. As such, our confidence in the magnitude and significance of the associations begins to decrease in the lower part of the air quality distribution of those older, monitor-based studies.
The three newer, hybrid model-based studies have larger cohort sizes than the older, monitor-based studies and, as noted by commenters, have more health events in the lower part of the air quality distribution. For these reasons, the EPA notes that we have more confidence in the reported association at concentrations lower than the reported mean in these more recent hybrid model-based studies, particularly at the 25th percentile compared to the 10th percentile. While the cohort sizes in the more recent, hybrid model-based studies are larger than the older, monitor-based studies, the EPA notes that the 10th percentiles are well below the middle portion of the air quality distribution for which we have the greatest confidence, and as noted above, our confidence in the magnitude and significance of associations in the lower parts of the air quality distribution begins to decrease. While we have more confidence in the lower percentiles because of the larger cohort sizes in the more recent hybrid model-based studies, we also have more confidence in the 25th percentiles than in the 10th percentiles, which are further from the means and closer to the lower end of the air quality distribution.
In considering how the six studies that report percentiles lower than the mean can be used to inform conclusions regarding the level of the primary annual PM2.5 standard, the EPA first notes that the three monitor-based epidemiologic studies (Bell et al., 2008; Franklin et al., 2007; Zanobetti and Schwartz, 2009) report 25th percentile concentrations that are at or above 11.5 µg/m3 . For two of the more recent hybrid model-based studies (Di et al., 2017b; Wang et al., 2017), the 25th percentile of estimated PM2.5 concentrations are just above 9 µg/m3 , while one study (Di et al., 2017a) reports a PM2.5 concentrations corresponding to 25th percentiles of health events of just below 7 µg/m3 . For the Di et al. (2017a) study, the 25th percentile PM2.5 concentration (6.7 µg/m3 ) is based on the PM2.5 concentration at which the 25th percentile of deaths occur in the study, while the reported mean (11.6 µg/m3 ) is based on estimated PM2.5 exposure concentrations. Additionally, the 25th percentiles of the other two recently available hybrid model-based studies (Di et al., 2017b; Wang et al., 2017) are based on estimated PM2.5 concentrations. As such, the PM2.5 concentration at which the 25th percentile of health events occur may be different from the estimated 25th percentile PM2.5 concentration in this study (Di et al., 2017a), creating an uncertain basis for comparison with the studies by Di et al. (2017b) and Wang et al. (2017). The 25th percentiles from these studies, in particular those that are more recently available, help to inform the Administrator's judgments regarding the appropriate level for the primary annual PM2.5 standard.
Some commenters disagree with the EPA's consideration of the relationship between mean PM2.5 concentrations reported in the key epidemiologic studies and design values to inform conclusions on the appropriate level for the primary annual PM2.5 standards. Commenters contend that setting the level of the primary annual standard below the design values in the epidemiologic studies, rather than below the study-reported mean concentrations, might keep overall mean PM2.5 concentrations throughout an area below the study-reported means but allow PM2.5 concentrations in some parts of the area, including near the “design value monitor” to remain above the study-reported mean PM2.5 concentrations, which are the concentrations where the evidence of health effects is strongest. Commenters contend that such a decision framework would not result in a standard that would provide requisite protection with an adequate margin of safety, Start Printed Page 16261 particularly for at-risk populations. These commenters further support this view by citing the CASAC's advice in their review of the 2021 draft PA, where the majority of CASAC stated that “even if a design value is somewhat higher than the area average, it reflects actual exposure levels and thus any portion of the population living near the design value monitor does experience exposures at that level and consequent health effects of exposure to that higher concentration” (Sheppard, 2022a, p. 14 of consensus responses). Additionally, these commenters suggest that the EPA should not deviate from the approach taken in the 2012 review, which was to set the standard at a level “somewhat below” the lowest mean PM2.5 concentration in the key epidemiologic studies.
To the extent that commenters are suggesting that the EPA is setting the level of the primary annual PM2.5 standard below the design values in the epidemiologic studies, rather than below the study-reported mean PM2.5 concentrations, we disagree with the commenters. In reaching conclusions on the level of the primary annual PM2.5 standard, the EPA considers the long-term study-reported mean PM2.5 concentrations from key epidemiologic studies and sets the level of the standard to somewhat below the lowest long-term mean PM2.5 concentration, not below the design values in the epidemiologic studies. Additionally, the EPA also considers the available information from a subset of epidemiologic studies that report exposure estimates or health events at the 25th and 10th percentiles of PM2.5 concentrations. The EPA particularly considers the 25th percentile data, while recognizing that our confidence in the magnitude and significance in the reported concentrations, and the ability of the lower percentile PM2.5 concentrations to inform decisions on the appropriate level of the annual standard, decreases with reduced data (below the mean) and diminishes further at percentiles that are even further below the mean and the 25th percentile.
However, the EPA notes that it is important to understand, and to not ignore, the relationship between the study-reported mean PM2.5 concentrations reported in key epidemiologic studies and the area design value. As an initial matter, the NAAQS consists of all four elements of the standard (indicator, averaging time, form, and level) and setting a standard that is requisite to protect public health includes consideration of all four elements together. Following implementation of the NAAQS, the design value is the metric used to determine compliance with the standard and is the statistic that describes the air quality status of a given location relative to the level of the primary annual PM2.5 NAAQS. The design value is different from the study-reported mean PM2.5 concentrations. This is because the study-reported mean PM2.5 concentrations are an annual average PM2.5 concentration, similar to the level of the standard, but the epidemiologic studies do not report statistics that take into account the other elements of the standard ( i.e., averaging time and form). Therefore, when considering the appropriate revisions to the annual PM2.5 standard, the EPA must consider the protection provided by a revised standard taking into account all of the elements of the standard, not just the annual average PM2.5 concentration alone.
In considering the annual standard, and in assessing the range of study-reported exposure concentrations for which we have the strongest support for adverse health effects observed in epidemiologic studies, the EPA focuses on whether the current primary annual PM2.5 standard provides adequate protection against these exposure concentrations or if the level of the standard should be revised to provide the appropriate public health protection. This means that, as in some previous reviews, it is important to consider how the study means were computed and how these concentrations compare to the annual standard metric (including the level, averaging time and form) which must be met at the monitor with the highest PM2.5 design value in an area for compliance with the NAAQS. This approach is based on the application of a decision framework based on assessing means (as well as the lower distribution of reported PM2.5 concentration, as noted above) reported in key epidemiologic studies. In the 2012 review, the available key epidemiologic studies computed the mean PM2.5 concentrations using an average across monitor-based PM2.5 concentrations. As such, at that time, the decision framework used an approach based on maximum monitor concentrations to determine compliance with the standard, while selecting the standard level based on consideration of composite monitor concentrations ( i.e., selecting the standard level of 12.0 µg/m3 was just below the long-term study-reported mean PM2.5 concentrations in key epidemiologic studies). Further, the EPA conducted analyses that examined the differences in these two metrics ( i.e., maximum monitor concentrations, which is how compliance with the standard is assessed and composite monitor concentrations, which is how key epidemiologic studies report their mean concentrations) across the U.S. and in areas included in the key epidemiologic studies and found that the maximum design value in an area was generally higher than the monitor average across that area, with the amount of difference between the two metrics varying based on location and concentration (Hassett-Sipple et al., 2010; Frank, 2012). This information was taken into account by the then-Administrator's final decision in selecting a level of 12.0 µg/m3 for the primary annual PM2.5 standard in the 2012 review and discussed more specifically in her considerations on adequate margin of safety.
The relationship between the mean PM2.5 concentrations and the area design value continues to be an important consideration in evaluating the adequacy of the current or potential alternative annual standard levels in this reconsideration. Again, in a given area, the area design value is based on the monitor in an area with the highest PM2.5 concentrations and is used to determine compliance with the standard, including the averaging time and form of the standard ( i.e., an annual average over 3-years must not exceed the level of the of the annual PM2.5 standard). The highest PM2.5 concentrations spatially distributed in the area would generally occur at or near the area design value monitor and the distribution of PM2.5 concentrations would generally be lower in other locations and at monitors in that area. As such, when an area is meeting a specific annual standard level ( e.g., 9.0 µg/m3 ), we would expect the annual average exposures ( i.e., a metric similar to the study-reported mean values) in that area to be at concentrations lower than that level ( e.g., lower than 9.0 µg/m3 ).
However, as described in section II.A.2.c.ii, we note that there are a substantial number of different types of epidemiologic studies available since the 2012 review, as assessed in both the 2019 ISA and the ISA Supplement, that make understanding the relationship between the mean PM2.5 concentrations and the area design value an even more important consideration in this reconsideration (U.S. EPA, 2019a; U.S. EPA, 2022a). While the key epidemiologic studies in the 2012 review were all monitor-based studies, the recent epidemiologic studies in this reconsideration include hybrid modeling approaches that have emerged in the epidemiologic literature as an Start Printed Page 16262 alternative to approaches that only use ground-based monitors to estimate PM2.5 exposure. As assessed in the 2019 ISA and ISA Supplement, a substantial number of epidemiologic studies used hybrid model-based methods in evaluating associations between PM2.5 exposure and health effects. Hybrid model-based studies employ various fusion techniques that combine ground-based monitored data with air quality modeled estimates and/or information from satellites to estimate PM2.5 exposures. While these studies provide a broader estimation of PM2.5 exposures compared to monitor-based studies ( i.e., PM2.5 concentrations are estimated in areas without monitors), the hybrid modeling approaches result in study-reported means that are more difficult to relate to the annual standard metric and to the maximum monitor design values used to assess compliance. In addition, to further complicate the comparison, when looking across these studies, we find variations in how exposure is estimated between such studies, and thus, how the study means are calculated. Two important variations across studies include: (1) Variability in spatial scale used ( i.e., averages computed across the national (or large portions of the country) versus a focus on only CBSAs); and (2) variability in exposure assignment methods ( i.e., averaging across all grid cells, averaging across a scaled-up area like a ZIP code, and population weighting). The differences in these approaches can result in studies reporting different study means, even though the association between PM2.5 exposure and health effects outcomes are similar.
To emphasize the importance of the differences between the studies, we revisit the simplified example in the State of Georgia from the 2022 PA that evaluates monitors and hybrid modeling approaches, noting that this example is useful to exhibit how the differences in the methods used to estimate exposure can lead to differences in the reported mean concentrations (U.S. EPA, 2022b, p. 3–71). In this example, for all monitors within the Atlanta-Sandy Springs-Roswell CBSA, the average PM2.5 concentration is 9.3 µg/m3 , while the area design value (based on the highest monitored PM2.5 concentration in the area) is 10.4 µg/m3 . This comparison helps to illustrate the fact that composite monitor values tend to be somewhat lower than the highest area monitor values, consistent with the key points made in the 2012 review. This example also illustrates how monitors are sited to represent the higher concentrations within the area and that the area's annual design value, which is used for compliance with the standard, is calculated based on the highest monitor in the area. Next, in this example, mean PM2.5 concentrations were calculated using similar approaches to those used in hybrid modeling-based epidemiologic studies to compute study-reported means, including (1) the average concentration across the entire State of Georgia; (2) the population-weighted average across the entire State; (3) the average concentration across the Atlanta-Sandy Springs-Roswell CBSA; and (4) the population-weighted average across the Atlanta-Sandy Springs-Roswell CBSA. At the urban level ( e.g., Atlanta-Sandy Springs-Roswell CBSA), the average PM2.5 concentration when taking the mean of all grid cells is 9.2 µg/m3 , whereas the population-weighted mean is 9.6 µg/m3 . Across Georgia, the average PM2.5 concentration using the hybrid approach and averaged across each grid cell is 8.3 µg/m3 , which is lower than the population-weighted statewide average of 9.1 µg/m3 . While this is a simple example completed in one State and one CBSA, it suggests that the lowest mean values tend to result from the approaches that use concentrations from all or most grid cells ( e.g., did not apply population weighting), both urban and rural, across the study area to compute the mean. Higher mean values are observed when the approach focuses on the urban areas alone or when the approach incorporates population weighting. Overall, this example suggests that the means from studies using hybrid modeling approaches are generally lower than the means from monitor-based approaches, and means from both approaches are lower than the annual design values for the same area. Population weighting tends to increase the calculated mean concentration, likely because more densely populated areas also tend to have higher PM2.5 concentrations. In other words, this simplified example exhibits how not all reported mean PM2.5 concentrations from key epidemiologic studies are the same; some reported means are from monitored studies and some reported means are from hybrid modeling studies, while some reported means include only urban areas, and other reported means include both urban and rural areas, and some reported means include aspects of population weighting while others do not.
As detailed above in section I.D.5, in the air quality analyses comparing composite monitored PM2.5 concentrations with annual PM2.5 design values in U.S. CBSAs, maximum annual PM2.5 design values were approximately 10% to 20% higher than annual average composite monitor concentrations ( i.e., averaged across multiple monitors in the same CBSA). Based on these results, this analysis suggests that there will be a distribution of concentrations and the maximum annual average monitored concentration in an area (at the design value monitor, used for compliance with the standard), will generally be 10–20% higher than the average across the other monitors in the area. Thus, in considering how the annual standard levels would relate to the study-reported means from monitor-based studies, we can generally conclude that an annual standard level that is no more than 10–20% higher than monitor-based study-reported mean PM2.5 concentrations would generally maintain air quality exposures to be below those associated with the study-reported mean PM2.5 concentrations, exposures for which we have the strongest support for adverse health effects occurring.
Air quality analyses described in section I.D.5 above also consider information from the epidemiologic studies that utilized the hybrid modeling approaches. Analyses show that average maximum annual design values are 40–50% higher when compared to annual average PM2.5 concentrations estimated without population weighting and are 15–18% higher when compared to average annual PM2.5 concentrations with population weighting applied. Given these results, it is worth noting that for the studies using the hybrid modeling approaches, the choice of methodology employed in calculating the study-reported means ( i.e., using population weighting versus not applying aspects of population weighting), and not a difference in estimates of exposure in the study itself, can produce substantially different study-reported mean values, with the approach that does not employ population weighting producing a much lower reported mean PM2.5 concentration. Therefore, the impact of the differences in methods is an important consideration when comparing mean concentrations across studies.
Because of the differences in the methods employed by the key epidemiologic studies, and as demonstrated by the example and air quality analyses above, the application of any decision framework that considers the study-reported mean PM2.5 concentrations, and evaluates whether the current annual standard provides adequate protection against these reported exposure concentrations, is more complicated than the Start Printed Page 16263 approaches used in past reviews. As such, the EPA disagrees with commenters who argue that the EPA's consideration of the relationship between mean PM2.5 concentrations reported in key epidemiologic studies and design values is not appropriate and should be ignored.
In considering the information from the epidemiologic studies, while the EPA does not dispute the reported associations of epidemiologic studies in hybrid modeling studies that report long-term mean concentrations and do not apply aspects of population weighting, using the reported long-term mean concentration from these studies in informing an appropriate level of the annual PM2.5 standard is more uncertain. Given this, hybrid modeling studies that do not apply aspects of population weighting provide less information on conclusions regarding the appropriate level of the primary annual PM2.5 standard. In support of this, some commenters also noted this consideration and suggested that the Administrator place lower weight on U.S. studies that did not use population weighting.
In considering the relationship between study-reported mean PM2.5 concentrations and the design values, the EPA agrees with commenters that setting the level of the primary annual standard below the design values, rather than below the study-reported mean concentrations, might allow PM2.5 concentrations in some part of the area near the design value monitor to remain above the study-reported mean PM2.5 concentration, where evidence of health effects is strongest. As discussed in the proposal and in section II.B.4 below, the Administrator specifically notes that that the highest PM2.5 concentrations spatially distributed in the area would generally occur at or near the area design value monitor and that PM2.5 concentrations will be equal to or lower at other monitors in the area. Furthermore, since monitoring strategies aim to site monitors in areas with higher PM2.5 concentrations, monitored areas will generally have higher concentrations compared to areas without monitors. Therefore, by setting the level of the standard to 9.0 µg/m3 and just below the lowest study-reported mean PM2.5 concentration ( e.g., 9.3 µg/m3 ), the highest possible design value in a given area would be just below the study-reported mean PM2.5 concentration, the concentration where we have the most confidence in the reported health effect association, and we anticipate that, based on our assessment of air quality data, the distribution of PM2.5 concentrations would decrease even further with distance from the highest monitor ( i.e., the “design value monitor”) (see, for example, U.S. EPA, 2022a, section 2.3.3.2.4 and pp. 3–71 to 3–77). The Administrator further notes that when an epidemiologic study reports a mean PM2.5 concentration that reflects the average of annual average monitor-based concentrations across an area, the area design value will generally be higher than the study-reported mean. Similarly, he observes that when a study reports a mean that reflects the average of annual average concentrations estimated at across an area using a hybrid modeling approach, the area design value will generally be higher. As such, by evaluating the difference between the study-reported mean PM2.5 concentrations and design values, the Administrator seeks to set the level of the standard below the lowest study-reported mean, while ensuring that the primary annual PM2.5 standard, including its averaging time and form, provides protection against the exposures associated with health effects observed in the key epidemiologic studies.
Additionally, the EPA disagrees with commenters who contend that the approach taken may allow PM2.5 near the design value monitor to remain above the study-reported mean PM2.5 concentrations. In following this approach of setting the annual standard level somewhat below the lowest reported mean PM2.5 concentration, setting a standard level that requires the design value monitor (which is the highest monitor in an area) to be just below the lowest study-reported mean across key studies will generally result in distributions of even lower concentrations of PM2.5 across the entire area, such that even those people living near an area design value monitor (where PM2.5 concentrations are generally highest) will be exposed to PM2.5 concentrations below the PM2.5 concentrations reported in the epidemiologic studies where there is the highest confidence of an association. In their review of the 2021 draft PA, the majority of the CASAC had some concerns about the approach for comparing study means and design values, questioning whether such an approach would provide adequate protection for people who live in areas with higher concentrations, such as those living in areas with higher concentrations ( e.g., near the design value monitor) (Sheppard, 2022a, p. 8 of consensus responses). The minority of the CASAC, in considering the relationship between the study-reported mean PM2.5 concentration and design values, stated that “the form of the standard and the way attainment with the standard is determined ( i.e., highest design value in the CBSA) are important factors when determining the appropriate level for the standard” and noted that that design values are generally higher than area average exposure levels (Sheppard, 2022a, p. 17 of consensus responses). For all of the reasons discussed above, and consistent with the minority of the CASAC's advice in their review of the 2021 draft PA, we disagree with the commenters that areas near the design value monitors would be expected to experience PM2.5 concentrations above the study-reported mean concentrations.
Several commenters assert that epidemiologic studies that restrict PM2.5 concentration to below 12 µg/m3 provide additional support for revising the level of the primary annual PM2.5 standard to 8 µg/m3 . Some commenters disagree with the EPA's assertion that the studies that employ restricted analyses do not provide enough information to understand how the studies were restricted to certain PM2.5 concentrations, with commenters providing additional information on the methods for restricted analyses. The commenters state that for the long-term studies at issue here, the study authors simply examined their database that linked subjects to long-term PM2.5 concentrations above 12 μg/m3 , removed those data from the analysis, and reran the analysis. Additionally, one commenter provided an explanation of how the restricted analyses were conducted in studies for which he was an author. The commenter notes that for each year a subject was in the study, annual PM2.5 concentrations were assigned at the ZIP code level. If they moved, they were assigned the ZIP code level PM2.5 concentration for the new ZIP code. The commenter notes that these restricted analyses only included subjects whose annual PM2.5 exposure never exceeded that restricted concentration for any year of follow-up in the study. The commenter suggested that the EPA may be concerned as to how PM2.5 concentrations in restricted analyses related to a design value since these are exposures for individuals who may have relocated during the study but argue that that is not the point. The commenters assert that while the analyses were restricted to people never exposed above certain concentrations over longer periods of time, the actual PM2.5 exposure was one year of exposure in most of these studies. Commenters also suggest that, since the Start Printed Page 16264 EPA has deviated from its approach from the 2012 review for considering study-reported mean PM2.5 concentrations, the EPA should dismiss its concerns regarding being able to relate the mean PM2.5 concentrations from these studies to design values.
First, the EPA agrees with commenters that studies that employ restricted analyses can be used for informing conclusions regarding the appropriate level of the primary annual PM2.5 standard. However, the EPA disagrees that the information provided by the commenters provides a sufficient basis for an annual standard level of 8 μg/m3 . Restricted analyses provide additional support for effects at lower concentrations, exhibiting associations for mean concentrations presumably below the mean concentrations for the main analyses. However, even though commenters note that any individual with exposures over the restricted analyses is excluded from restricted analyses, uncertainties remain with regard to how the mean PM2.5 concentrations in restricted analyses compare to design values, particularly in light of the removal of entire ZIP codes from analyses. Design values are calculated based on all measured PM2.5 concentrations. When an analysis is restricted below a certain level, some parts of the air quality distribution are removed, but comparing the restricted mean to a design value is not possible because these are two different metrics. For example, in a study that restricts concentrations below 12 µg/m3 , that represents only part of the air quality distribution, whereas a design value for that study area would include all PM2.5 concentrations, not just the ones below 12 µg/m3 . Therefore, in contrast to means from the main (unrestricted) analysis, it is not possible to compare mean concentrations from restricted analyses to design values. Further, it is unclear how one could evaluate such a relationship between design values and mean PM2.5 concentrations from studies that use restricted analyses because the standard is set based on all of its elements (indicator, averaging time, form, and level) and removing PM2.5 concentrations from the calculation of the design value for such a comparison would result in a metric that is no longer a design value that would provide the intended protection of the standard. This leads to greater uncertainty in how to use the mean PM2.5 concentrations from these studies that use restricted analyses in a similar decision framework as the epidemiologic studies that report long-term mean PM2.5 concentrations for health effect associations for the full distribution of PM2.5 concentrations.
As described in reaching his conclusions in the section below, the Administrator judges that, despite these uncertainties and limitations, studies that use restricted analyses can provide supplemental information for consideration in reaching conclusions regarding both the adequacy and level of the standard. He notes two studies (Di et al., 2017b and Dominici et al., 2019) are available in this reconsideration that report means in their restricted analyses (restricting annual average PM2.5 exposure below 12 μg/m3 ) and used population-weighted approaches to estimate PM2.5 exposures and these studies report mean PM2.5 concentrations of 9.6 µg/m3 . He recognizes that these studies are just one line of evidence for consideration and that along with the broader evidence base, including the key epidemiologic studies, these studies provide support that the level of the primary annual PM2.5 standard should be set below 10 µg/m3 .
We disagree with the commenters that concerns about relating the mean PM2.5 concentrations from restricted analyses to design values are not valid. As an initial matter, restricted analyses were not available and did not inform the 2012 decision to revise the annual PM2.5 standard level to 12.0 µg/m3 . The approach in 2012 in revising the annual standard was to set the level to somewhat below the mean of key epidemiologic studies. As noted above, while the EPA believes that restricted analyses can help inform conclusions regarding the adequacy and the level of the primary annual PM2.5 standard, in the context of placing the studies in a decision framework to inform the appropriate level of the annual PM2.5 standard, the EPA has not deviated from its approach from the 2012 review. Given that restricted analyses are new since the 2012 review, the EPA disagrees with commenters that uncertainties associated with these studies should not be considered, and that these studies should be used in a similar manner to their main analyses in taking an approach to set a level of the standard somewhat below the lowest long-term reported mean PM2.5 concentration. Specifically, as detailed above there are uncertainties and limitations associated with relating the mean PM2.5 concentrations from these studies to design values for studies that use restricted analyses, and many of these studies did not expressly report a mean PM2.5 concentration for the restricted analysis which makes it impossible to make such a comparison.
Several commenters contend that in considering the accountability studies, the EPA inappropriately reached conclusions regarding the level of the primary annual PM2.5 standard based on the starting PM2.5 concentrations of these studies, rather than the ending concentrations ( i.e., concentrations after a policy was implemented). The commenters assert that these studies provide support for revising the level of the primary annual PM2.5 standard to below the proposed range of 9–10 µg/m3 to protect public health with an adequate margin of safety.
Accountability studies examine the effect of a policy on reducing PM2.5 concentrations in ambient air and evaluate whether such reductions were observed to also lead to reductions in PM2.5 - associated health outcomes ( e.g., mortality). Additionally, accountability studies can reduce uncertainties related to residual confounding of temporal and spatial factors (U.S. EPA, 2022a, p. 3–25). Prior to implementation of the policies, three accountability studies newly available in this reconsideration and assessed in the ISA Supplement, report mean PM2.5 concentrations below the level of the current annual standard level (12.0 µg/m3 ) and ranged from 10.0 µg/m3 to 11.1 µg/m3 (Sanders et al., 2020b; Corrigan et al., 2018; and Henneman et al., 2019). These studies suggest that public health improvements may occur following the implementation of a policy that reduces annual average PM2.5 concentrations below the level of the current standard of 12.0 µg/m3 , and potentially below the lowest “starting” concentrations in these studies of 10.0 µg/m3 . However, while the small number of studies may provide limited information related to informing the adequacy and level of the annual PM2.5 standard, we note that accountability studies are only one line of evidence, and that these studies provide supplemental information for consideration in addition to the full body of evidence. Further, the EPA does not believe it would be appropriate to determine the level of the standard by reference to ending concentrations in accountability studies. Accountability studies are most informative in demonstrating that public health improvements may occur following the implementation of a policy that reduces annual average PM2.5 concentrations below the level of the current standard of 12.0 µg/m3 , and potentially below the lowest “starting” concentrations in these studies of 10.0 µg/m3 . However, the EPA finds the available information from accountability studies is too limited to support a conclusion that the Start Printed Page 16265 appropriate level at which to set the primary annual PM2.5 standard would be equal to the ending concentrations of those studies, as the commenters suggest. These studies demonstrate that there are reductions in health outcomes when PM2.5 concentrations are reduced in these studies from the starting concentration to the ending concentration, but do not provide support for health effect associations at or below the ending concentrations that would warrant a more stringent standard.
Commenters disagree with the Administrator placing less weight on the epidemiologic studies conducted in Canada when reaching conclusions regarding the level of the primary annual PM2.5 standard. These commenters argue that the Canadian epidemiologic studies provide support for setting the level at the lowest end of the proposed range ( i.e., 8 µg/m3 ) because they report mean PM2.5 concentrations, in some cases, below 8 µg/m3 . Commenters disagree with the EPA's reasoning for placing less weight on the Canadian epidemiologic studies, suggesting it conflicts with the approaches in previous PM NAAQS reviews and arguing that the findings of the Canadian epidemiologic studies can be directly translated into a primary annual PM2.5 standard. Additionally, while the commenters disagree with the EPA's approach for considering the study-reported mean PM2.5 concentrations and design values in general, they note that the CASAC, in their review of the 2021 PA, noted that “while there may be no design value in Canada, there are data that indicate what a U.S. design value would be if an area average like that found in the Canadian studies were to occur in the U.S.” (Sheppard, 2022a, p. 13 of consensus responses). The commenters contend that the EPA failed to acknowledge this advice from the CASAC, specifically noting that the majority of the CASAC highlighted Canadian epidemiologic studies as a part of their rationale for revising the level of the primary annual PM2.5 standard to within the range of 8–10 µg/m3 .
In considering the information from the epidemiologic studies in reaching his conclusions, the Administrator considered the full body of evidence, including studies conducted in the U.S. and Canada. However, as described in the proposal and in section II.B.4 below, the Administrator also recognizes that the exposure environments in the U.S. are different from those in Canada. In particular, the U.S. population density is approximately 43 people per square kilometer in the contiguous U.S.[98] compared to Canada, which has one of the lowest population densities on the Earth with 4.2 people per square kilometer (Statistics Canada, 2023). This difference in population density between the U.S. and Canada was not as apparent, and did not need to be highlighted, in the 2012 review given that the available Canadian epidemiologic studies used population-weighting and focused on urban areas where monitors were available and population densities were more comparable with those in the U.S. Given this, the study-reported mean concentrations from U.S. and Canadian studies in the 2012 review were very similar. The recent epidemiologic evidence available in this reconsideration, however, includes studies that utilize approaches that highlight the importance of considering the differences between the two exposure environments in the U.S. versus Canada. When focusing on the recently available Canadian monitor-based epidemiologic studies in this reconsideration, the information indicates that these studies, unlike the studies available in the 2012 review, do not apply population weighting ( e.g., Lavigne et al., 2018; Liu et al., 2019). As noted in responding to other public comments above, the absence of population weighting is an important consideration that limits the utility of these studies in informing the appropriate level of the primary annual PM2.5 standard. In addition, there are recently available studies in the 2019 ISA and ISA Supplement that expand the geographical extent of the epidemiologic study areas by estimating exposure concentrations in areas where there are no monitors. To do this, these studies use either a statistical extrapolation of monitored values or use air quality modeling and other forms of data ( e.g., hybrid model-based approaches). For these Canadian studies, the EPA notes two important considerations in using the information to directly translate to policy decisions regarding the level of the annual standard in the U.S. The first is that in incorporating a larger portion of Canada into these recent studies, more rural areas are included, and as such, the population densities and exposure environment differences become more important. The second is that in analyses that evaluate and validate hybrid models, there is less certainty in PM2.5 exposure estimates in more rural areas, which are further from air quality monitors and where PM2.5 concentrations in the ambient air tend to be lower (U.S. EPA, 2022b, pp. 2–51 and 2–63). Additionally, it is unclear what portion of the PM2.5 concentrations from rural areas are contributing to the study reported mean. Given this, studies that incorporate more rural areas into the epidemiologic studies highlight the importance of considering the differences between the population exposures in the studies themselves and in the U.S. versus Canadian study areas, as well as the influence these differences have on the interpretation of the epidemiologic study results. For these reasons, while the Canadian epidemiologic studies provide additional support for associations between PM2.5 concentrations and health effects, the long-term means from Canadian epidemiologic studies are a less certain basis for informing the EPA's selection of the annual standard level, given that it is a U.S.-based standard.
With respect to the CASAC's advice in their review of the 2021 draft PA, the EPA recognizes that the majority of the CASAC pointed to the Canadian studies as supporting their recommendation to revise the annual standard level to within the range of 8–10 µg/m3 . However, the EPA also notes that the CASAC did not advise the EPA to revise the annual standard to a level that was below the study-reported means in the key Canadian epidemiologic studies. Indeed, the CASAC noted that some of the Canadian studies showed associations below 8 µg/m3 , but did not recommend that the Administrator consider levels below 8 µg/m3 for the annual standard. Further, based on the CASAC's advice, the Administrator is not excluding Canadian studies from his consideration in this reconsideration, but he is considering them in light of the limitations and challenges presented and in the context of the full body of available scientific evidence.
Lastly, the EPA disagrees with commenters that the findings of the Canadian epidemiologic studies can be directly translated into a primary annual PM2.5 standard based on the evaluation of the relationship between U.S. study-reported mean PM2.5 concentrations and U.S. design values. It is unclear whether the relationship between U.S. study-reported mean PM2.5 concentrations and U.S. design values (which, in the case of U.S. hybrid model-based studies, indicates that design values are 15–18% greater than area mean PM2.5 concentrations) would apply to the Canadian epidemiologic studies and their reported mean PM2.5Start Printed Page 16266 concentrations, given that these studies generally report lower PM2.5 concentrations than the U.S.-based studies. As such, interpreting the study-reported mean concentrations from the Canadian studies in the context of a U.S.-based standard may present challenges in directly and quantitatively informing decisions regarding potential alternative levels of the annual standard, particularly noting the different in exposure relationships in the U.S. versus Canada given the large difference in population densities between the two countries. Further, as mentioned above, while the CASAC advised the EPA to consider the Canadian studies as relevant evidence and found that placing weight on the Canadian studies supported their recommendation to revise the annual standard level to within the range of 8–10 µg/m3 , the lower end of their recommended range for the level of the annual standard did not extend below the lower study-reported means from those studies.
Commenters who supported retaining and revising the primary annual PM2.5 standard both raised concerns regarding how the EPA used the scientific evidence and quantitative risk assessment related to disparities in PM2.5 exposure and risk in informing conclusions on the standard. Commenters who supported retaining the standard assert that the available scientific evidence that demonstrates disparities for minority populations do not support revising the standard, noting that these studies are in areas that tend to have large minority populations and more sources of PM. These commenters contend that because the studies conclude that minority populations experience more effects than others living in the same area that something other than PM2.5 concentrations in ambient air is causing the disproportionate impact on minority populations, providing proximity to a source as an example. The commenters note that it is unclear how a national standard will reduce exposure disparities for population groups living in the same area, and further assert that studies of exposure disparities among minority populations were considered in reaching the 2020 final decision to retain the standards.
Conversely, commenters who support revising the standard assert that the at-risk analyses conducted in the 2022 PA provide support for revising the primary annual PM2.5 standard to a level of 8 μg/m3 . In particular, these commenters state that the at-risk analysis demonstrated that while disparities in mortality risk remain at a standard level of 9.0 μg/m3 , disparities in exposure are significantly reduced for an alternative standard level of 8.0 μg/m3 (U.S. EPA, 2022b, p. 3–162).
As discussed in section I above, the primary (health-based) NAAQS are established at a level that is requisite to protect public health, including the health of sensitive or at-risk groups, with an adequate margin of safety.[99] In so doing, decisions on the NAAQS are based on an explicit and comprehensive assessment of the current scientific evidence and associated risk analyses. More specifically, the EPA expressly considers the available information regarding health effects among at-risk populations in decisions on the primary NAAQS. Where populations with disparities in exposure and risk are among the at-risk populations, the decision on the standards is based on providing requisite protection for these and other at-risk populations and lifestages.
The Administrator expressly considered the available information regarding health effects among at-risk populations in reaching the proposed decisions that the current primary annual PM2.5 standard is not requisite to protect public health with an adequate margin of safety, and should be revised. The 2019 ISA and ISA Supplement identified children, older adults, people with pre-existing diseases (cardiovascular disease and respiratory disease), minority populations, and low SES populations as at-risk populations. The Administrator is thus, in his final decision, establishing primary PM2.5 standards which, in his judgment, will provide protection for these at-risk populations, including minority populations, with an adequate margin of safety.
With respect to the risk assessment, while the EPA notes that the analyses support the conclusion that the primary PM2.5 standards are not adequate, as detailed further in the proposal and above in section II.A.3, the EPA also cautions against an over-interpretation of the absolute results. The quantitative risk assessment provides estimates of PM2.5 -attributable mortality based on input data that include C–R functions from epidemiologic studies that do not quantitatively account for uncertainties in associations between PM2.5 exposure and health effects at lower concentrations and are based on an air quality adjustment approach that incorporates proportional decreases in PM2.5 concentrations to meet lower alternative standard levels. As a result, simulated air quality improvements used in the risk assessment will always lead to proportional decreases in risk ( i.e., each additional µg/m3 reduction produces additional benefits with no clear stopping point), without considering the substantially greater uncertainties associated with the relationship between PM2.5 exposures and health effects at lower concentrations.
The same is true for the new at-risk analysis in the risk assessment presented in the 2022 PA that is based on a recent epidemiologic study that is available in this reconsideration that provides mortality risk coefficients for older adults ( i.e., 65 years and older) based on PM2.5 exposure and stratified by racial and ethnic demographics. Generally, the results of at-risk analyses can vary greatly depending on the inputs to the analyses, including the representativeness of the populations and demographics captured by the study areas that are a part of the analyses, as well as the available C–R functions from epidemiologic studies that stratify by race and ethnicity and the air quality adjustment approaches that are used to simulate air quality at different standard levels. In fact, for this at-risk analysis, the results are even more uncertain than similar estimates from the overall risk assessment due to additional sources of uncertainty specific to the at-risk analysis, such as using C–R functions derived from smaller epidemiologic sample sizes along with the sources of uncertainty that apply to the overall risk assessment (U.S. EPA, 2022b, section 3.4.1.8). Additionally, in characterizing at-risk populations, the at-risk analysis only used one of the air quality adjustment approaches used in the overall risk assessment, which decreases the potential representativeness of the PM2.5 concentrations across the study areas (U.S. EPA, 2022b, section 3.4.1.8). Lastly, this at-risk analysis relies on the stratified risk coefficients from only one epidemiologic study.[100] For these reasons, the Administrator places little Start Printed Page 16267 weight on the absolute results of the risk assessment, including the at-risk analysis, for purposes of selecting the level of the annual standard that is requisite.
While there are substantial uncertainties in the absolute results of the quantitative risk assessment, the EPA also notes that recent scientific evidence evaluated in the ISA Supplement, which built upon the 2019 PM ISA conclusions, found that the evidence “[c]ontinue[s] to support disparities in PM2.5 exposure and health risks by race and ethnicity” while studies of SES “provide additional support indicating there may be disparities in PM2.5 exposure and health risk by SES” (U.S. EPA, 2022a, p. 5–4). Thus, in light of the statutory requirement to provide protection for at-risk populations, it is not surprising that the stratified population results of the risk assessment suggest that meeting a revised standard would result in higher risk reductions for minority and low SES populations.
In conclusion, the EPA recognizes that the at-risk analysis was based on one epidemiologic study that stratified by race/ethnicity for older adults ( e.g., 65+ years old) and that there is increasing uncertainty in quantitative estimates of stratified risk estimates at the lower end of the range of standard levels assessed. Moreover, the EPA finds that the goal of the NAAQS is to provide the requisite protection to at-risk groups, and where minority populations are included among the at-risk groups, providing requisite protection to minority populations will also result in protecting the public health of other populations. Thus, in setting the NAAQS to protect the health of at-risk groups with an adequate margin of safety, the Administrator is selecting the standard that will provide requisite protection, including for minority populations and other at-risk populations, which also generally results in protecting the public health of other populations and reducing risk disparities.
A number of commenters, primarily from industries and industry groups and some States, support the EPA's proposed decision to retain the primary 24-hour PM2.5 standard. Many of these commenters contend that the available scientific evidence and quantitative information has not significantly changed since the 2020 final decision and note that important uncertainties remain. The commenters agree with the EPA's conclusions regarding the controlled human exposure studies and their relationship to short-term peak PM2.5 concentrations in ambient air. These commenters also noted the primary annual and 24-hour PM2.5 standards work together to provide public health protection, with the 98th percentile form of the 24-hour standard effectively limiting peak daily concentrations. The commenters agree with the EPA that the current suite of standards maintain subdaily concentrations below the higher concentrations in controlled human exposure studies where more consistent health effects are observed. Commenters also agree with the EPA's conclusions that the epidemiologic studies are not useful for informing decisions on the level of the primary 24-hour PM2.5 standard because the standard focuses on reducing peak exposures with its 98th percentile form, while the epidemiologic studies often focus on the mean or median as the percentile for which associations with short-term exposures are observed. These commenters also agree with the EPA's focus on U.S.-based studies because of differences compared to Canadian studies. The commenters also generally agree with the Administrator's judgment that it was appropriate to place less weight on the risk assessment, noting that the annual standard is controlling in most areas of the country and revising the annual standard would have the most potential to reduce risk related to PM2.5 exposures and would reduce both average (annual) and peak (daily) PM2.5 concentrations. Finally, these commenters note that the CASAC did not reach consensus on whether the current primary 24-hour PM2.5 standard should be revised, and they agree with the minority of the CASAC's recommendation in their review of the 2021 draft PA that the primary 24-hour primary PM2.5 standard should be retained. These commenters also note the CASAC's support in their review of the 2019 draft PA for retaining the primary 24-hour PM2.5 standard.
A number of commenters, primarily from public health and environmental organizations and some States, oppose the EPA's proposed decision to retain the primary 24-hour PM2.5 standard. These commenters support revising the level of the primary 24-hour PM2.5 standard, contending that a more stringent standard is necessary to provide requisite public health protection with an adequate margin of safety, particularly for at-risk groups. In so doing, these commenters place weight on the same aspects of the available scientific evidence as the majority of the CASAC in their review of the 2021 draft PA, and generally advocate for revising the level of the standard to within the range of 25–30 µg/m3 as recommended by the majority of the CASAC. Some of these commenters support a level no higher than 25 µg/m3 and others support a level of 20 µg/m3 . These commenters generally cite to the available scientific evidence, including evidence of disproportionate exposures and risks for certain at-risk groups, and the CASAC's advice in support for their recommendation. Some of these commenters also suggest that decisions regarding the primary 24-hour PM2.5 standard should not be related to decisions on the primary annual PM2.5 standard.
As an initial matter, the EPA disagrees with commenters who suggest that decisions regarding the primary 24-hour PM2.5 standard should not be related to decisions on the primary annual PM2.5 standard. In reviewing the adequacy of the public health protection afforded by the primary PM2.5 standards, the Administrator's consistent past practice has been to evaluate the combination of the annual and 24-hour standards together. In 2012, the then-Administrator concluded that the most effective and efficient way to reduce total population risk associated with both long- and short-term PM2.5 exposures was to set a generally controlling annual standard, and to provide supplemental protection by means of a 24-hour standard set at the appropriate level. In so doing, the then-Administrator explicitly recognized that potential air quality changes associated with meeting a revised annual standard (with a level of 12 µg/m[3] ) would result in lowering risks associated with both long- and short-term PM2.5 exposures by lowering the overall distribution of air quality concentrations, and that retaining a 24-hour standard at the appropriate level would ensure an adequate margin of safety against short-term effects in areas with high peak-to-mean ratios (78 FR 3163, January 15, 2013). In this reconsideration, also, the Administrator considers it appropriate to rely on the annual standard (arithmetic mean, averaged over three years) for targeting protection against both long- and short-term PM2.5 exposures, noting that the annual standard is typically controlling, while the 24-hour standard (98th percentile, averaged over three years) can provide supplemental protection against the occurrence of peak 24-hour PM2.5 concentrations (U.S. EPA, 2022b, section 3.6.3). Further, the Administrator notes that, as in the 2012 review, changes in PM2.5 air quality to meet a revised annual standard would Start Printed Page 16268 affect the entire distribution of long- and short-term concentrations, thus likely resulting not only in lower short- and long-term PM2.5 concentrations near the middle of the air quality distribution, but also in fewer and lower short-term peak PM2.5 concentrations.[101] Thus, the Administrator continues to conclude it is appropriate to consider whether the annual and 24-hour standards together provide requisite protection of public health, rather than considering each standard in isolation.
Regarding the appropriate basis for determining the level of the 24-hour standard, a number of commenters who support revising the primary 24-hour PM2.5 standard to a lower level contend that the EPA should not rely on the controlled human exposure studies in evaluating the adequacy of the public health protection afforded by the primary 24-hour PM2.5 standard. These commenters support this view by citing the CASAC comments in their review of the 2019 draft PA which advised that controlled human exposure studies have limitations that may impact their ability to inform conclusions on the adequacy of the public health protection afforded by the primary 24-hour PM2.5 standard. Commenters noted that these studies do not include the most vulnerable populations and often involve exposure to only one pollutant to elicit a response, and therefore are not representative of real-world exposures.
Other commenters support the EPA's use of the controlled human exposure studies to inform the adequacy of the public health protection and note that the 24-hour standard must at least provide protection against the health effects observed in controlled human exposure studies. Some of the commenters cite the Wyatt et al. (2020) study that demonstrated cardiovascular effects following 2-hour exposures to 120 µg/m3 and 4-hour exposures to 37.8 µg/m3 . Some of these commenters contend that the current primary 24-hour PM2.5 standard allows PM2.5 exposures comparable to those observed to elicit effects in the controlled human exposure studies, and therefore, the EPA must revise the level of the current standard to protect public health. To support this view, some commenters submitted an analysis of monitoring data from 2017–2020, which compares the number of days per year where maximum daily PM2.5 concentrations exceed 120 µg/m3 and 37.8 µg/m3 .
Additionally, other commenters assert that the EPA should focus less on peak PM2.5 concentrations “typically measured” in areas meeting the current primary PM2.5 standards even if they do not exceed the concentrations in the controlled human exposure studies because, in their view, the standard needs to protect against atypical exposures to atypical peak PM2.5 concentrations. These commenters conclude that, when considered together, the controlled human exposure studies and the epidemiologic studies warrant strengthening the level of the primary 24-hour PM2.5 standard.
The EPA generally disagrees with commenters who contend that it is inappropriate to rely on the controlled human exposures studies in evaluating the adequacy of the public health protection afforded by the primary 24-hour PM2.5 standard. The Agency considers these studies informative both for establishing biological plausibility and for determining an appropriate level for the 24-hour standard. When looking to the experimental studies, the EPA finds that the 2019 ISA and ISA Supplement included controlled human exposure studies that report statistically significant effects on one or more indicators of cardiovascular function following 2-hour exposures to PM2.5 concentrations at and above 120 μg/m[3] (and at and above 149 μg/m[3] for vascular impairment, the effect shown to be most consistent across studies). As noted in the 2019 ISA, these studies are important in establishing biological plausibility for PM2.5 exposures causing more serious health effects, such as those seen in short-term exposure epidemiologic studies, and they provide support that more adverse effects may be experienced following longer exposure durations and/or exposure to higher concentrations. Additionally, one controlled human exposure study assessed in the ISA Supplement reports evidence of some effects for cardiovascular markers at lower PM2.5 concentrations, 4-hour exposures to 37.8 µg/m[3] (Wyatt et al., 2020). However, there is inconsistent evidence for inflammation in other controlled human exposure studies evaluated in the 2019 ISA. The EPA notes that although the controlled human exposure studies do not provide a threshold below which no effects occur, the observed effects in these controlled human exposures studies are ones that signal an intermediate effect in the body, likely due to short-term exposure to PM2.5, and typically would not, by themselves, be judged as adverse (88 FR 5620, January 27, 2023) [102 103]
The EPA notes that the majority of the CASAC, in their review of the 2021 draft PA, commented that these controlled human exposure studies generally do not include populations with substantially increased risk from exposure to PM2.5 , such as children, older adults, or those with more severe underlying illness, and often involve exposure to only one pollutant to elicit a response. However, both the majority and the minority of the CASAC explained that, even taking into consideration their limitations, the controlled human exposure studies provide some support for assessing the adequacy of the 24-hour standard.[104]
The EPA agrees with the CASAC that the controlled human exposure studies generally do not include populations with substantially increased risk from exposure to PM2.5, like children, older adults, or those with pre-existing severe illness, like cardiovascular effects. As such, and as an initial note, these Start Printed Page 16269 studies are therefore somewhat limited in their ability to inform at what concentrations effects may be elicited in at-risk populations. In spite of this limitation, the EPA also agrees with the CASAC, that even taking into consideration the limitations of the controlled human exposure studies, these studies can provide some support for evaluating the adequacy of the 24-hour standard. However, the EPA further notes that while the controlled human exposure studies are important in establishing biological plausibility, the health outcomes observed in these controlled human exposure studies are often “intermediate” outcomes ( i.e., not always clearly adverse) and therefore it is unclear how the importance of the effects observed in the studies should be interpreted with respect to adversity to public health. The EPA finds that it is appropriate to consider these study limitations in assessing the information provided by controlled human exposure studies in evaluating the adequacy of the primary 24-hour PM2.5 standard.
The EPA agrees with commenters that the primary 24-hour PM2.5 standard must at least provide protection against the health effects consistently observed in controlled human exposure studies. As discussed in the proposal, the EPA looks at whether the exposures that elicit a response following exposure to PM2.5 in the controlled human exposure studies occur under recent air quality conditions in areas meeting the current standards. Based on these air quality analyses, the EPA concludes that these types of exposures very rarely occur when the current standards are being met.
The EPA did receive multiple comments questioning these results and the approach in the EPA's analyses. For example, some commenters submitted an analysis of monitoring data from 2017–2020, which compares the number of days per year where maximum daily PM2.5 concentrations exceed 120 µg/m3 and 37.8 µg/m3 and evaluate the number of days subset by groups of monitors with 4-year average PM2.5 concentrations close to the levels of combinations of current and proposed annual (+/− 0.2 µg/m3 ) and 24-hour (+/−2 µg/m3 ) PM2.5 standards. To support their view that the primary PM2.5 standards should be revised, the commenters describe decreases in days per monitor per year with 2-hour maximum concentrations greater than 120 µg/m3 and 4-hour maximum concentrations greater than 37.8 µg/m3 when comparing monitors that achieve close to 10 and 30 µg/m3 versus monitors that meet close to 8 µg/m3 and 25 µg/m3 . The commenters noted decreases in the number of days per monitor per year with 2-hour maximum concentrations over 120 µg/m3 and 4-hour max concentration over 37.8 µg/m3 were also seen when comparing monitors close to achieving 24-hour standards with levels of 35 µg/m3 versus 25 µg/m3 .
First, the EPA notes that this analysis submitted by commenters was limited to a very small number of monitors and did not include a national perspective. Second, the EPA notes that this analysis focused on number of days (rather than the number of times) where there was a 2-hour maximum concentration over 120 µg/m[3] or a 4-hour max concentration over 37.8 µg/m[3] . In order to evaluate the protection provided by the current 24-hour standard against peak exposures, including exposures with 2-hour concentrations greater than 120 µg/m[3] and 4-hour concentrations greater than 37.8 µg/m[3] , the EPA considers it more informative and appropriate from a public health perspective to assess the number of times a subdaily exposure of concern occurs in a year, rather than the number of days on which they occur because the former identifies more potential exposures of concern and provides more information about the scale and scope of the occurrences of those exposures. Lastly, the analyses allowed monitors somewhat above the standards to be included. Therefore, it is unclear whether the exceedances of the 2-hour or 4-hour benchmarks would still have occurred if the area had actually been meeting the current primary PM2.5 standards. However, in considering the analyses submitted by the commenters, the EPA conducted new analyses [105] that looked at all individual monitors across the U.S. and evaluated the percentage of times the monitors experienced a 2-hour maximum concentration over 120 µg/m3 or a 4-hour max concentration over 37.8 µg/m3 when that monitor was meeting the current standards. Further, given that the Administrator concludes that the level of the current primary annual PM2.5 is not adequate and that it should be revised to 9.0 µg/m3 , the new analysis evaluates the percentage of times during a recent 3-year period ( i.e. 2019–2021) that individual monitors experienced a 2-hour maximum concentration over 120 µg/m3 or a 4-hour max concentration over 37.8 µg/m3 when that monitor was meeting the current primary 24-hour PM2.5 standard with its level of 35 µg/m3 and a revised primary annual PM2.5 standard of 9.0 µg/m3 .
In evaluating the results from the new analyses, it is important to keep in mind that the 2019 ISA and ISA Supplement concluded that the most consistent evidence from the controlled human exposures studies is for impaired vascular function following 2-hour exposures to average PM2.5 concentrations at and above about 120 µg/m3 , with less consistent evidence for effects following exposures to concentrations lower than 120 µg/m3 . The new analyses show that across all monitors, on average, only 0.029 percent of 2-hour observations reach PM2.5 concentrations higher than 120 µg/m3 in areas meeting the current 24-hour standard and a revised annual standard of 9.0 µg/m3 . Further, recognizing that one purpose of the 24-hour standard is to protect against exposure in areas with high peak-to-mean ratios, when assessing the monitors individually across the U.S. under these same conditions, the monitors reporting the highest PM2.5 concentrations have only 0.47 percent of 2-hour observations reach PM2.5 concentrations higher than 120 µg/m3 .
Additionally, the analyses also evaluated the frequency of reporting a 4-hour maximum concentration over 37.8 µg/m3 when monitors were meeting the current 24-hour standard and a revised annual standard of 9.0 µg/m3 . For this part of the analysis, the EPA finds that across all monitors, on average, only 0.41 percent of 4-hour observations reach PM2.5 concentrations higher than 37.8 µg/m3 in areas meeting the current 24-hour standard and a revised annual standard of 9.0 µg/m3 . Further, when assessing the monitors individually across the U.S. under these same conditions, the monitors reporting the highest PM2.5 concentrations have only 2.6 percent of 4-hour observations reach PM2.5 concentrations higher than 37.8 µg/m3 . Thus, the EPA disagrees with commenters that the current primary 24-hour PM2.5 standard typically allows PM2.5 exposures at or above those observed to cause health effects in controlled human exposure studies. Furthermore, the EPA notes that in light of the small number of occurrences and the intermediate nature of the effects observed in Wyatt et al. (2020) at concentrations of 37.8 µg/m3 ( i.e., effects that typically would not, by themselves, be judged as adverse), there is substantial basis to doubt whether further improvements in public health Start Printed Page 16270 would be achieved by further reducing these exposures. In drawing this conclusion, the EPA notes the lack of evidence of effects from controlled human exposure studies at levels below the current 24-hour standard and the fact that the results of Wyatt et al. (2020) are inconsistent with other currently available studies, and this study only observes intermediate effects.
In response to commenters that cited the majority of the CASAC's view that, in general, “[t]here is . . . less confidence that the annual standard could adequately protect against health effects of short-term exposures” (Sheppard, 2022a, p. 4 of consensus letter), the EPA disagrees with the majority of CASAC, noting that the results of the EPA's analysis suggest that high peak concentrations are extremely infrequent in areas meeting an annual standard of 9.0 µg/m3 , occurring less than 0.029–0.41 percent of the time (for 2-hour concentrations >120 µg/m3 and 4-hour concentrations >37.8 µg/m3 , respectively). This suggests that in most locations, even the upper tail of the distribution would be controlled quite well under a revised annual standard. With regard to the likelihood that the current standards would allow peak concentrations that are clearly of concern from a health perspective, therefore, the EPA concludes that such occurrences are extremely infrequent—and will be even less frequent under the improved air quality conditions associated with meeting a revised annual PM2.5 standard of 9.0 µg/m3 .
A number of commenters who support revising the primary 24-hour PM2.5 standard to a lower level suggest that the available epidemiologic evidence provides support for such a revision. To support their view, the commenters note that the currently available evidence, including a number of epidemiologic studies that demonstrate associations between short-term PM2.5 exposures and health effects, provides support for causal relationships for short-term PM2.5 exposures and health effects as described in the 2019 ISA and ISA Supplement. The commenters further note that the available epidemiologic studies include diverse populations that are broadly representative of the U.S. population, including at-risk populations, which they assert is an advantage over the controlled human exposure studies and the risk assessment, which are not as broadly representative.
These commenters highlight a number of specific epidemiologic studies that they suggest provide support for revising the level of the 24-hour standard. Additionally, commenters contend that there are epidemiologic studies using restricted analyses that show that positive and statistically significant associations between short-term PM2.5 exposure and mortality persist at daily mean concentrations below 25 µg/m3 . The commenters also cite several studies that provide no evidence of a threshold. These commenters also point to the CASAC advice in their review of the 2021 draft PA, where the majority of the CASAC cited epidemiologic studies using restricted analyses as offering support for revision. The commenters argue that the EPA cannot base discretion on uncertainties related to the methods used in restricted analyses in the epidemiologic studies. In so doing, these commenters disagree with the EPA that it is important to take into consideration that these studies do not consider the form or averaging time of the 24-hour standard. Finally, the commenters claim that while the EPA stated that the study-reported means from epidemiologic studies that use restricted analyses are more useful for identifying impacts from typical 24-hour exposures than for peak 24-hour exposures, the commenters assert that the studies also indicate that there are health risks at relatively high concentrations below the current level of the primary 24-hour PM2.5 standard that must be addressed.
As noted by the commenters, epidemiologic studies that show positive and statistically significant associations between short-term PM2.5 exposure and mortality provide support for the causal determination in the 2019 ISA. The EPA also agrees that the available epidemiologic studies include diverse populations that are broadly representative of the U.S. population, including at-risk populations. Further, the EPA agrees that studies evaluated in the 2019 ISA and the ISA Supplement continue to provide evidence of linear, no-threshold concentration-response relationships, but with less certainty in the shape of the curve at lower concentrations ( i.e., below about 8 µg/m3 ), with some recent studies providing evidence for either a sublinear, linear, or supralinear relationship at these lower concentrations (U.S. EPA, 2019a, section 11.2.4; U.S. EPA, 2022a, section 2.2.3.2).
However, findings of positive, significant associations in short-term epidemiologic studies do not directly indicate that short-term effects would occur in areas meeting the 24-hour standard and therefore, do not directly address the question of whether the current 24-hour standard is adequate. While short-term epidemiologic studies evaluate associations between distributions of ambient PM2.5 and health outcomes, they do not identify the specific exposures ( i.e., a specific 24-hour concentration) that can lead to the reported effects. Short-term epidemiologic studies evaluate the association between day-to-day variation in daily (24-hour) PM2.5 exposure and health endpoints ( e.g., mortality) to understand how these changes in air pollution concentrations are associated with changes in health outcomes. But these studies do not report daily concentrations; rather, they report the long-term mean concentration of the 24-hour PM2.5 concentrations over the entire multi-year period of the study, and typically report their results as a relative risk ( e.g., for each 10 µg/m[3] increase in PM2.5, the risk of mortality or cardiovascular hospital admissions increases by a certain percentage, across the full range of the 24-hour PM2.5 concentrations in the study). This means that there is no specific point in the air quality distribution of any epidemiologic study that represents a “bright line” at and above which effects have been observed and below which effects have not been observed. Nor, as noted above, do these studies allow for any direct inferences about health impacts associated with the short-term “peak” exposures that the primary 24-hour standard is designed to protect against. While there can be considerable variability in daily exposures over a multi-year study period, most of the estimated exposures in these epidemiologic studies reflect days with ambient PM2.5 concentrations around the mean or middle of the air quality distributions examined ( i.e., “typical” days rather than days with extremely high or extremely low concentrations). This is true of long-term epidemiologic studies as well. The difference between epidemiologic studies examining associations with long-term exposures and short-term exposures is comparing different levels of exposure over different exposure durations ( i.e., long-term studies exposures are defined as those that are annual or multi-year, while short-term exposures are defined as those that are mostly 24-hour) (U.S. EPA, 2019a, section P.3.1). Thus, in both cases, and in the absence of a discernible threshold, epidemiologic studies of short-term and long-term exposures provide the strongest support and confidence for reported health effect associations around the middle portion of the PM2.5 air quality distribution ( e.g., the study-reported mean PM2.5Start Printed Page 16271 concentration), which corresponds to the bulk of the underlying data, rather than at the extreme upper or lower ends of the distribution. However, the difference between the annual standard and the 24-hour standard, aside from averaging times, is that the form of the annual standard is a mean PM2.5 concentration, which is based on the bulk of the air quality data, while the form of the 24-hour standard is a 98th percentile form, which is based on peak concentrations. Both long-term and short-term epidemiologic studies are informative for determining the appropriate level of the annual PM2.5 standard, which is designed to control “typical” daily exposures and risks, because these studies most often report long-term mean (or median) PM2.5 concentrations that are representative of “typical” exposures that are associated with health effects. In contrast, while the short-term epidemiologic studies examine health effects associated with shorter exposure durations ( e.g., mostly 24-hour exposures), these studies are less informative for determining the appropriate level of the 24-hour PM2.5 standard because these studies do not report the 98th percentile PM2.5 concentrations,[106] which is more directly comparable to the form of the 24-hour standard. Additionally, if the 98th percentile of data were reported, the EPA would consider the peak concentrations observed in these studies (which by definition rarely occur) in conjunction with other supporting evidence. However, as already noted, there is an absence of new information in this reconsideration (either from controlled human exposure studies or epidemiologic studies) suggesting that peak concentrations just below the level of the current 24-hour standard (with its level of 35 µg/m3 ) are associated with adverse effects. Instead, the evidence links risk to more typical daily exposures near the middle of the air quality distribution—exposures most effectively controlled through a strengthening of the annual standard. As noted in the 2012 final rule, “reducing the annual standard is the most efficient way to reduce the risks from short-term exposures . . . as the bulk of the risk comes from the large number of days across the bulk of the air quality distribution, not the relatively small number of days with peak concentrations” (78 FR 3156, January 15, 2013).
As noted above, in evaluating the adequacy of the current standards, the EPA has consistently considered the annual standard (based on arithmetic mean concentrations) and 24-hour standard (based on 98th percentile concentrations) together in evaluating the public health protection provided by the standards against the full distribution of short- and long-term PM2.5 exposures. Moreover, the EPA has previously noted that the annual standard is generally controlling in most parts of the country, providing an effective and efficient way to reduce total population risk to both long- and short-term PM2.5 exposures, while the 24-hour standard, with its 98th percentile form, provides supplemental protection, particularly for areas with high peak-to-mean ratios of 24-hour PM2.5 concentrations (78 FR 3158, January 15, 2013). In such areas, annual average PM2.5 concentrations could be quite low, and the 24-hour standard provides a means of ensuring control of episodic peaks possibly associated with strong local or seasonal sources, or PM2.5 -related effects that may be associated with shorter-than daily exposure periods. The approach taken in evaluating the adequacy and alternative levels of the annual standard has been to evaluate the long-term mean PM2.5 concentrations of both long-term and short-term key epidemiologic studies, where we have the most confidence in the reported health effects association, while also giving some consideration to lower percentiles of the air quality distribution ( e.g., 25th percentiles). However, using a similar approach to evaluate the adequacy of the current and any potential alternative levels of the 24-hour standard with short-term epidemiologic studies, as the majority of CASAC and some commenters are suggesting, presents challenges.
Short-term epidemiologic studies, including those that use restricted analyses, often report metrics that include mean PM2.5 concentrations, with some studies also reporting lower percentiles, such as the 25th percentile. As previously noted above, for studies of daily PM2.5 exposure, which examine associations between day-to-day variation in PM2.5 concentrations and health outcomes, often over several years, most of the estimated exposures reflect days with ambient PM2.5 concentrations around the middle of the air quality distributions examined ( i.e., the mean or median). However, there is not a metric or statistic reported in short-term epidemiologic studies that allows for a direct comparison to the current 24-hour PM2.5 standard and its 98th percentile form. While a 98th percentile of PM2.5 concentrations is a metric that might be more closely compared to the 24-hour standard level, 98th percentile PM2.5 concentrations were not reported in key epidemiologic studies. Consistent with the Administrator's final decision in 2012, the EPA notes that even if 98th percentile values were reported, it would be inappropriate to focus on these concentrations without also considering the impact of a revised annual standard on short-term concentrations, since many areas would be expected to experience decreasing short- and long-term PM2.5 concentrations in response to a revised annual standard (78 FR 3156, January 15, 2013). Furthermore, in light of the scarcity of days at the very upper end of the distribution, and to avoid placing undue reliance on the peak concentrations observed in these studies (which by definition rarely occur), the EPA finds that such values would need to be considered in conjunction with other supporting evidence. In addition, as described above, the other lines of evidence available for consideration by the EPA do not indicate that the current primary 24-hour standard requires revision to protect public health with an adequate margin of safety. The EPA notes again the lack of corroborating evidence from controlled human exposure studies. While the EPA agrees with the CASAC that the controlled human exposure studies are limited in their ability to speak to the concentrations at which effects may be elicited in at-risk populations, as discussed above the lowest concentration associated with effects is 37.8 µg/m3 and the effects observed were “intermediate” outcomes that are not by themselves considered adverse. We also note that, as detailed in section II.A.2.a above, the study that observed intermediate effects at concentrations of 37.8 µg/m3 was evaluated in the ISA Supplement and the results of this study were inconsistent with the controlled human exposure studies evaluated in the 2019 ISA. Additionally, as noted above, the EPA finds that across all monitors, on average, only 0.41 percent of 4-hour observations reach PM2.5 concentrations higher than 38 µg/m3 in areas meeting the current 24-hour Start Printed Page 16272 standard and a revised annual standard of 9.0 µg/m3 . Given the rarity of these occurrences and the fact that the effects associated with exposures to this PM2.5 concentration have not been found to be adverse in and of themselves, the EPA finds it reasonable to conclude that this pattern of air quality will protect at-risk populations, even though such populations were not in the study groups. The EPA concludes that further evidence would be needed at specific short-term ( i.e., hourly or daily) concentrations below the level of the current 24-hour standard to support any revision to the current 24-hour standard.
With regard to the data that are available from the short-term epidemiologic studies (which, as noted, do not include 98th percentile values), the EPA considers it inappropriate to utilize the study-reported means from the short-term epidemiologic evidence to assess the adequacy of the 24-hour standard, with its 98th percentile form, considering that the study-reported mean concentrations do not provide meaningful insight regarding the frequency or health significance of peak concentrations occurring during the study period. As indicated in the 2022 PA, the study-reported means of short-term epidemiologic studies do not serve a purpose in determining a level at which we can confidently attribute effects to the impact of “peak” exposures. The 24-hour standard is intended to provide supplemental protection against short-term peak exposures and while there is a general relationship between mean concentrations and 98th percentile concentrations in individual locations, such relationships vary by location and there is not an established relationship that can be relied upon to predict 98th percentile concentrations based on mean PM2.5 concentrations reported in multi-city epidemiologic studies. Instead, mean concentrations from short-term epidemiologic studies are more useful in addressing questions regarding the effects of “typical” or average 24-hour exposures, which are addressed through the annual standard. For this reason, the EPA does consider the mean concentrations of short-term studies (as well as the means from the long-term studies) in evaluating the level of the annual standard, which the EPA recognizes as the generally controlling standard for both long- and short-term exposures. However, the EPA does not agree with commenters that it is appropriate to use means from short-term epidemiologic studies as the basis for a decision-making framework to determine the adequacy of the current 24-hour standard, with its 98th percentile form.
As described in the proposal (88 FR 5613, January 27, 2023), the 2022 PA also noted the epidemiologic studies that restrict 24-hour average PM2.5 concentrations to values of less than 35 µg/m3 , and in some cases less than 25 µg/m3 , and annual average PM2.5 concentrations less than 12 µg/m3 . Restricted analyses use a subset of data from their main analyses and conduct an epidemiologic study with health events that occur at concentrations below a certain concentration ( e.g., 25 µg/m3 ). While some of these studies do not report the mean PM2.5 concentration for the restricted analysis, the mean of the restricted analysis is presumably less than the mean PM2.5 concentration in the main analysis. Restricted analyses from long-term and short-term exposure epidemiologic studies are informative in providing support that the health effects associations are not driven by just the upper peaks of the PM2.5 air quality distributions and provide support for revision to the level of the annual PM2.5 standard. Short-term restricted analyses also report positive associations between short-term PM2.5 exposure and morbidity and mortality. As an example, in a restricted analysis evaluating the association between short-term exposures and PM2.5 concentrations less than 25 µg/m3 , Di et al. (2017a) removed 6.3 percent of the data from their main analyses, ( i.e., all PM2.5 concentrations greater than 25 µg/m3 ), and still found a positive and significant association between short-term PM2.5 exposure and mortality. This study provides additional support that the association between short-term exposure to PM2.5 and mortality in the main epidemiologic analysis is not driven by the upper peaks of the PM2.5 air quality distribution, which in turn supports the conclusion that lowering the entire distribution of air quality concentrations through a revised annual standard is an appropriate means of protecting against adverse effects from short-term exposure, as discussed further below.
In their review of the 2021 draft PA, the majority of the CASAC highlighted three U.S.-based epidemiologic studies that restricted 24-hour average PM2.5 concentrations below 25 μg/m3 as a part of their rationale for recommending that the EPA revise the level of the primary 24-hour PM2.5 standard. Similarly, in evaluating positive associations in restricted analyses, some commenters also suggest that because an association exists at 24-hour concentrations below 25 µg/m3 , the 24-hour standard level should be set at the concentration at which the analysis was restricted ( e.g., 25 µg/m3 ). However, the EPA notes that neither the CASAC nor public commenters provided any detail regarding, how, in their view, these studies demonstrate that the level of the current 24-hour standard is not adequate, and/or how these studies demonstrate what revised level of the 24-hour standard would provide requisite public health protection with an adequate margin of safety. The EPA considers that such an approach would have several important limitations. First, the approach assumes that a specific point on the air quality distribution ( e.g., the point at which the analysis was restricted) is where health effects are exhibited and where we have the most confidence in the reported association. However, in addition to the limitations associated with the short-term epidemiologic studies outlined above, the EPA does not agree that it would be appropriate to identify the requisite level of the primary 24-hour PM2.5 standard based on the specific concentration at which the analyses restrict their studies. The choice to restrict the data at a particular concentration is in effect arbitrary, and does not establish that any particular effects are attributable to that concentration as opposed to other concentrations within the restricted analysis.
Further, these restricted analyses do not report the PM2.5 concentration at the 98th percentile of data or other metrics relating to the upper end of the distribution that could provide information about health risks associated with peak exposures. For example, the CASAC does not provide a discussion of what the comparable 98th percentile concentration is in the distribution of remaining 24-hour PM2.5 concentrations of restricted analyses (because such data is not reported by the study authors) and what degree of confidence the Administrator should place on those upper percentile values ( e.g., 98th percentile values). In order to identify a level of the 24-hour standard based on associations between the “upper end” of exposures, either in the unrestricted or the restricted analyses, and adverse health effects, it would be necessary to have both greater detail on the distribution of air quality in the study and greater confidence in the reported association at the peak concentrations such as the 98th percentile—in other words, a better understanding of how specific 24-hour concentrations correspond to the frequency and total number of observed health events in the study.
Further, the EPA notes that when resulting analyses based on the Start Printed Page 16273 restricted dataset continue to find positive associations between the remaining air quality distribution and health effects, it suggests that the relationship was in fact not driven primarily by the upper tail (now removed from the dataset) but rather by lower portions of the distribution of air quality. In other words, we have no confidence that the remaining upper end of the air quality distribution is driving the remaining associations reported in the restricted analyses, as opposed to the vast array of health events at and around the mean PM2.5 concentration. In fact, it is reasonable to conclude that to effectively address the health effects observed in the study, it is necessary to control not just the peak concentrations but to reduce the bulk of the exposures (occurring near the mean), a task more effectively achieved, as noted above through a tightening of the annual standard, which has the effect of shifting the entire distribution of PM2.5 concentrations downward (both peaks and means). Therefore, while the EPA agrees that both short- and long-term epidemiologic studies that completed restricted analyses and reported the resulting study means could be used to inform conclusions regarding the adequacy of the annual standard, given that the resulting study means (when reported) could be evaluated in the context of the decision framework described above for informing decisions on the level of the annual standard, the EPA considers that current short-term epidemiologic studies that restrict analyses are subject to the same limitations outlined above for current short-term epidemiologic studies in how they can be used in a decision-making framework to inform the adequacy and alternative level of the primary 24-hour PM2.5 standard. As such, while the available short-term epidemiologic studies that restrict their analyses are useful for informing conclusions regarding the strength of the associations for health outcomes, they are not, as currently designed, as useful for informing conclusions regarding the adequacy of the current primary 24-hour PM2.5 standard. In reaching this conclusion, the EPA notes that the majority of the CASAC did not address the limitations of these studies outlined in the 2021 draft PA, particularly in the context of the 24-hour standard with its 98th percentile form. Among the future research needs identified by the EPA in the 2022 final PA, the Agency noted a number of gaps in the currently available information reported in the epidemiologic studies of short-term exposure, including “descriptive statistics of PM2.5 concentrations at individual percentiles from the 95th percentile to the 99th percentile, as well as the number of days of concentrations and/or health events within each of these percentiles” and other descriptive statistics and details regarding analytical design in studies employing restricted analyses (U.S. EPA, 2022b, pp. 3–225 to 3–226). Such information could significantly improve the EPA's ability to draw conclusions from these studies with regard to the adequacy of the current primary 24-hour PM2.5 standard.
Due to the limitations and uncertainties outlined above, in reaching his decision on the primary 24-hour PM2.5 standard, the Administrator judges that the information from currently available short-term epidemiologic studies, including those that use restricted analyses, is inadequate to inform decisions regarding the adequacy of the current 24-hour standard. Additionally, consistent with the final decision in 2012, the EPA continues to view an approach that focuses on setting a generally controlling annual standard as the most effective and efficient way to reduce total population risk associated with both long- and short-term PM2.5 exposures. Potential air quality changes associated with meeting an annual standard level of 9.0 µg/m3 will result in lowering risk associated with both long- and short-term PM2.5 exposure by lowering the overall air quality distribution. As discussed above, reducing the annual standard is the most efficient way to reduce the risks from short-term exposures identified in the epidemiologic studies, as the available evidence suggests the bulk of the risk comes from the large number of days across the bulk of the air quality distribution, not the relatively small number of days with peak concentrations. However, as in the 2012 review, the Administrator recognizes that an annual standard alone would not be expected to offer sufficient protection with an adequate margin of safety against the effects of short-term PM2.5 exposures in all parts of the country, particularly in areas with high peak-to-mean ratios, and concludes that it is appropriate to continue to provide supplemental protection by means of a 24-hour standard. In so doing, the Administrator concludes that retaining the level of the primary 24-hour PM2.5 standard of 35 µg/m3 will provide requisite protection against short-term peak PM2.5 concentrations, in conjunction with a revised annual standard level of 9.0 µg/m3 .
4. Administrator's Conclusions
This section summarizes the Administrator's considerations and conclusions related to the adequacy of the current primary PM2.5 standards and presents his decision to revise the primary annual PM2.5 standard to a level of 9.0 µg/m3 and retain the primary 24-hour PM2.5 standard. In establishing primary standards under the Act that are “requisite” to protect public health with an adequate margin of safety, the Administrator is seeking to establish standards that are neither more nor less stringent than necessary for this purpose. He recognizes that the requirement to provide an adequate margin of safety was intended to address uncertainties associated with inconclusive scientific and technical information and to provide a reasonable degree of protection against hazards that research has not yet identified. However, the Act does not require that primary standards be set at a zero-risk level; rather, the NAAQS must be sufficiently protective, but not more stringent than necessary.
Given these requirements, the Administrator's final decision in this reconsideration is a public health policy judgment drawing upon scientific and technical information examining the health effects of PM2.5 exposures, including how to consider the range and magnitude of uncertainties inherent in that information. This public health policy judgment is based on an interpretation of the scientific and technical information that neither overstates nor understates its strengths and limitations, nor the appropriate inferences to be drawn, and is informed by the Administrator's consideration of advice from the CASAC and public comments received on the proposal.
The initial issue to be addressed in the reconsideration of the primary PM2.5 standards is whether, in view of the advances in scientific knowledge and other information reflected in the 2019 ISA, ISA Supplement, and 2022 PA, the current standards are requisite to protect public health with an adequate margin of safety. In considering the adequacy of the current suite of primary PM2.5 standards, the Administrator has considered the large body of evidence presented and assessed in the 2019 ISA and ISA Supplement, the conclusions presented in the 2022 PA, the views expressed by the CASAC, and public comments. The Administrator has taken into account both evidence- and risk-based considerations in developing final conclusions on the adequacy of the current primary PM2.5 standards. The Administrator has additionally Start Printed Page 16274 considered the associated public health policy judgments and judgments about the uncertainties inherent in the scientific evidence and quantitative analyses that are integral to the conclusions on the adequacy of the current primary PM2.5 standards.
In evaluating the adequacy of the current standards, the Administrator first recognizes the longstanding body of health evidence supporting relationships between PM2.5 exposures (short- and long-term) and mortality and serious morbidity effects. The evidence available in this reconsideration ( i.e., that assessed in the 2019 ISA and ISA Supplement) and summarized above in section II.A.2.a reaffirms, and in some cases strengthens, the conclusions from the 2009 ISA regarding the health effects of PM2.5 exposures. Recent epidemiologic studies demonstrate generally positive and often statistically significant associations between PM2.5 exposures and a number of health effects, including non-accidental, cardiovascular, or respiratory mortality; cardiovascular or respiratory hospitalizations or emergency room visits; and other mortality/morbidity outcomes ( e.g., lung cancer mortality or incidence, asthma development). Recent controlled human exposure and animal toxicological studies, as well as evidence from epidemiologic panel studies, strengthens support for potential biological pathways through which PM2.5 exposures could lead to the serious effects reported in many population-level epidemiologic studies, including support for pathways that could lead to cardiovascular, respiratory, nervous system, and cancer-related effects. In considering the available scientific evidence, and consistent with approaches employed in past NAAQS reviews, the Administrator places the most weight on evidence supporting “causal” or “likely to be causal” relationship with long or short-term PM2.5 exposures. In addition, the Administrator also takes note of those populations identified to be at greater risk of PM2.5 -related health effects, as characterized in the 2019 ISA and ISA Supplement, and the potential public health implications.
In evaluating what existing or revised standards may be requisite to protect public health, as described above in section II.A.2, the Administrator's approach recognizes that the current annual standard (based on arithmetic mean concentrations) and 24-hour standard (based on 98th percentile concentrations), together, are intended to provide public health protection against the full distribution of short- and long-term PM2.5 exposures. This approach recognizes that changes in PM2.5 air quality designed to meet either the annual or the 24-hour standard would likely result in changes to both long-term average and short-term peak PM2.5 concentrations.
Further, consistent with the approach adopted in 2012, the Administrator concludes that the most effective and efficient way to reduce total population risk associated with both long- and short-term PM2.5 exposures is to set a generally controlling annual standard, and to provide supplemental protection against the occurrence of peak 24-hour PM2.5 concentrations by means of a 24-hour standard set at the appropriate level. In reaching this conclusion, the Administrator explicitly recognizes that air quality changes associated with meeting a revised annual standard would result in lowering risks associated with both long- and short-term PM2.5 exposures by lowering the overall distribution of air quality concentrations, leading to not only in lower short- and long-term PM2.5 concentrations near the middle of the air quality distribution, but also in fewer and lower short-term peak PM2.5 concentrations. Similarly, the Administrator recognizes that changes in air quality to meet a 24-hour standard, would result not only in fewer and lower peak 24-hour PM2.5 concentrations, but also in lower annual average PM2.5 concentrations. However, as noted in 2012, he also recognizes that an approach that relies on setting the level of the 24-hour standard such that the 24-hour standard is generally controlling would be less effective and result in less uniform protection across the U.S. than an approach that focuses on setting a generally controlling annual standard. Thus, he concludes that relying on a revised annual standard as the controlling standard will reduce aggregate risks associated with both long- and short-term exposures more consistently than a generally controlling 24-hour standard. He further concludes that retaining a 24-hour standard at the appropriate level will ensure an adequate margin of safety against short-term effects in areas with high peak-to-mean ratios.
In light of his focus on the annual standard as the generally controlling standard, in considering whether the primary PM2.5 standards are adequate, the Administrator first considers information available to inform his final conclusions regarding the primary annual PM2.5 standard. In so doing, he notes that in this reconsideration, a large number of key U.S. epidemiologic studies report positive and statistically significant associations for air quality distributions with overall mean PM2.5 concentrations that are well below the current level of the annual standard of 12.0 μg/m3 . He further recognizes that there is additional scientific evidence assessed in the 2019 ISA and newly assessed in this reconsideration in the ISA Supplement that can provide supplemental information to inform his decisions. In addition to the key U.S. epidemiologic studies, the Administrator also recognizes that key Canadian epidemiologic studies also demonstrate positive and statistically significant associations at concentrations below 12 μg/m3 . He also recognizes that epidemiologic studies that restrict annual average PM2.5 concentrations to below 12 μg/m3 also provide support for positive and statistically significant associations at lower mean PM2.5 concentrations, as do accountability studies that also suggest public health improvements may occur at concentrations below 12 μg/m3 .
With regard to the available scientific evidence to inform his final decisions on the adequacy of the current 24-hour standard, the Administrator finds that there is less information available to support decisions on the 24-hour standard than that summarized above for the annual standard. The Administrator first notes that controlled human exposure studies, including those newly available in this reconsideration, demonstrate effects following short-term PM2.5 exposures at concentrations higher than the current 24-hour standard. The Administrator also considers air quality analyses conducted in the 2022 PA and in responding to public comments, as described above in section II.B.3, that evaluate PM2.5 concentrations in ambient air for similar durations to the controlled human exposure studies. As noted above, these air quality analyses indicate that the current 24-hour standard, particularly in conjunction with the revised level of the annual standard, provides a high degree of protection against subdaily PM2.5 concentrations that have been shown to elicit effects in controlled human exposure studies. The Administrator considers a limited number of available epidemiologic studies that report associations with health effects when the analyses are restricted to daily PM2.5 concentrations below 35 μg/m3 . As described above, although these studies are useful in demonstrating that health effects are associated with exposure to daily PM2.5 concentrations in the lower part of the air quality distribution, they do not provide information about health effects associated with the short-term Start Printed Page 16275 “peak” exposures that the 24-hour standard is designed to protect against. Accordingly, these studies have limited relevance in informing a decision about the appropriate level of the 24-hour standard.
In addition to the scientific evidence, the Administrator also considers the information from the risk assessment. In so doing, he notes that the risk assessment estimates that the current primary annual PM2.5 standard could allow a substantial number of deaths in the U.S. With respect to the 24-hour standard, the Administrator recognizes that there are only a small number of study areas where the 24-hour standard is controlling and changes in the 24-hour standard level are estimated to have a much smaller impact on public health. The Administrator recognizes that while the risk estimates can help to place the evidence for specific health effects into a broader public health context, they should be considered along with the inherent uncertainties and limitations of such analyses when informing judgments about the potential for additional public health protection associated with PM2.5 exposure and related health effects. While the Administrator recognizes that these uncertainties are important, he also notes that the general magnitude of the risk estimates provide support for significant public health impacts, particularly for lower alternative annual standard levels.
In reaching his final conclusions regarding the adequacy of the primary PM2.5 standards, the Administrator also considers the CASAC's advice and recommendations, as well as public comments. With respect to the CASAC's advice, the Administrator recognizes that, in their review of the 2021 draft PA, the CASAC reached consensus that the current primary annual PM2.5 standard is not adequate and that it is not sufficiently protective of public health. The Administrator also takes note of the CASAC's advice in their review of the 2019 draft PA, where the CASAC did not reach consensus on the adequacy of the primary annual PM2.5 standard, with the minority recommending revision and the majority recommending the standard be retained. Furthermore, he recognizes that in reviewing the 2019 draft PA, the CASAC reached consensus regarding the adequacy of the primary 24-hour PM2.5 standard, concluding that the standard should be retained. Conversely, in their review of the 2021 draft PA, the majority of the CASAC advised that the current primary 24-hour PM2.5 standard is not adequate and recommended revising the level of the standard, while the minority of the CASAC concluded that the standard was adequate and should be retained. However, in considering the advice of the CASAC collectively in the context of this reconsideration, the Administrator recognizes that the 2021 draft PA included scientific evidence and quantitative risk information that was not available in the 2019 draft PA, and therefore, the advice and recommendations of the CASAC in their review of the 2021 draft PA are based on consideration of the full body of scientific evidence available in this reconsideration, including the evidence evaluated in the 2019 ISA and the ISA Supplement.
The Administrator recognizes that much of the scientific evidence available in this reconsideration was also available in the 2019 ISA and was considered by the then-Administrator when he decided that the current primary PM2.5 standards are requisite to protect public health with an adequate margin of safety. However, as described in section I.C.5.b above, in reaching his decision to reconsider the 2020 final decision, the Administrator also recognized that there were a number of studies published since the literature cutoff date of the 2019 ISA that were raised by some members of the CASAC in their review of the 2019 draft PA, in public comments on the 2020 proposal, and in the petitions for reconsideration. As such, the expansion of the air quality criteria in this reconsideration to encompass both the 2019 ISA and the additional scientific evidence evaluated in the ISA Supplement, along with evidence and updated quantitative analyses in the 2022 PA also provided an expanded record for the CASAC's review and public comments as a part of this reconsideration. Taken together, the 2019 ISA, ISA Supplement, and 2022 PA, along with the CASAC's advice and recommendations and public comments, provide the Administrator with additional information for consideration in reaching his final conclusions in this reconsideration. As a result, the record before him notably expands upon and strengthens the basis for the conclusions of the 2019 ISA while reducing some uncertainties that were identified in the 2020 final action.
In considering the available information in this reconsideration, the current Administrator reached different conclusions regarding the appropriate weight to place on certain aspects of the evidence than the then-Administrator in the 2020 final decision. For example, in reaching his conclusions on the primary annual PM2.5 standard in 2020, the then-Administrator concluded that it was appropriate to place more weight on epidemiologic studies that used ground-based monitors and to place less weight on the studies that used hybrid model-based approaches, citing to increased uncertainties associated with this new and emerging approach to estimating exposure. In placing more weight on the key U.S. monitor-based studies, the then-Administrator noted that the majority of these studies had mean concentrations at or above the level of the annual standard (12.0 µg/m3 ). However, unlike the approach for considering such studies in the 2012 review, the then-Administrator concluded that it was appropriate to consider the study-reported means collectively, and in so doing, he placed weight on the average of the study-reported means (or medians) across the U.S. monitor-based studies of 13.5 µg/m3 , and noted that this concentration was above the level of the standard (85 FR 82717, December 18, 2020). In contrast, in this reconsideration, the current Administrator judges that it is appropriate to consider the individual study-reported mean PM2.5 concentrations from not only the U.S. monitor-based epidemiologic studies, but also the U.S. hybrid model-based epidemiologic studies, which are an advancement in the available science since the completion of the 2009 ISA. The current Administrator also adopts an approach similar to some previous approaches for the PM NAAQS in which he judges it most appropriate to set the level of the standard to somewhat below the lowest long-term study-reported mean PM2.5 concentration reported in key U.S. epidemiologic studies, which is 9.3 µg/m3 . The study that reports the long-term mean PM2.5 concentration of 9.3 µg/m3 is newly available in this reconsideration and is evaluated in the ISA Supplement. In the 2019 ISA, the lowest long-term study-reported mean PM2.5 concentrations for U.S.-based studies that use ground-based monitors and hybrid model-based approaches are 9.9 µg/m3 and 10.7 µg/m3 , respectively. In judging that it is appropriate to consider both monitor- and hybrid model-based epidemiologic studies and that it is appropriate to adopt an approach to set the level of the standard to somewhat below the lowest long-term mean PM2.5 concentration, the current Administrator judges that the available scientific evidence—evaluated in both the 2019 ISA and in the ISA Supplement—provide support for his conclusion that that current primary Start Printed Page 16276 PM2.5 standard is not adequate and should be revised.
In addition to adopting a different approach than the previous Administrator for considering the long-term mean PM2.5 concentrations from key U.S. epidemiologic studies (one more consistent with the approach of the EPA in other prior reviews), the current Administrator both has information newly available in this reconsideration before him and is reaching different conclusions about how to weigh the evidence before him in reaching his final conclusions. For example, in reaching his final decision in 2020, the then-Administrator was concerned about placing too much weight on epidemiologic studies to inform his conclusions on the adequacy of the primary PM2.5 standards, noting that the epidemiologic studies do not identify particular PM2.5 concentrations that cause effects and cannot alone identify a specific level at which to set the standard. In so doing, the then-Administrator placed greater weight on the uncertainties and limitations associated with the epidemiologic studies, including exposure measurement error, potential confounding by copollutants, increased uncertainty of associations at lower PM2.5 concentrations, and heterogeneity of effects across different cities or regions (85 FR 82716, December 18, 2020). The Administrator recognizes that in reaching these judgments, the then-Administrator took into consideration the views of some members of the CASAC, who, in their advice on the 2019 draft PA, expressed the view that the current PM NAAQS should be retained because reported associations between short- and long-term PM2.5 exposures and adverse health outcomes “can reasonably be explained in light of uncontrolled confounding and other potential sources of error and bias” (Cox, 2019b, p. 8 of consensus responses).
In this reconsideration, the current Administrator notes that the ISA Supplement evaluates additional studies that employed statistical approaches that attempted to more extensively account for confounders and are more robust to model misspecification ( i.e., used alternative methods for confounder control, which are sometimes referred to as causal modeling or causal inference methods) that build upon those studies available and evaluated in the 2019 ISA (U.S. EPA, 2019, sections 11.1.2.1 and 11.2.2.4). These studies report consistent positive associations between long-term and short-term PM2.5 exposure and total mortality and cardiovascular effects (U.S. EPA, 2022a, section 3.2.2.3). In considering the epidemiologic evidence evaluated in the 2019 ISA, along with the newly available studies evaluated in the ISA Supplement, the current Administrator also recognizes that there are uncertainties and limitations associated with the epidemiologic studies, but judges that it is appropriate to place less weight on these uncertainties than the then-Administrator placed on them in reaching his final decision in 2020, given the strength of the longstanding large body of epidemiologic evidence, employing a variety of study designs, that demonstrates associations between long- and short-term PM2.5 exposures and health effects across multiple U.S. cities and in diverse populations, including in studies examining populations and lifestages that may be at comparatively higher risk of experiencing a PM2.5 -related health effect ( e.g., older adults, children).
In reaching this final decision, the Administrator recognizes he is differing not only with the prior Administrator but also with the advice some members of the CASAC provided during their review of the 2019 draft PA. Specifically, taking into consideration the strength of the evidence providing support for causality determinations, the advice of other members of the CASAC and the need to protect public health with an adequate margin of safety, the current Administrator disagrees with these members of CASAC regarding the weight to be given to epidemiologic evidence “based on its methodological limitations” (Cox, 2019b, p. 8 of consensus responses), such as the possibility “that such associations could reasonably be explained by uncontrolled confounding and other potential sources of error and bias” (Cox, 2019b, p. 8 of consensus responses).
As another example of information that was not available to the CASAC in providing advice to the Administrator in reaching his final decision in 2020, the then-Administrator noted in his final decision that, while some members of the CASAC and public commenters highlighted a number of accountability studies that examined past reductions in ambient PM2.5 concentrations and the degree to which those reductions have resulted in public health improvements, the small number of available accountability studies did not examine air quality with starting concentrations meeting the primary annual PM2.5 standard of 12.0 µg/m3. The then-Administrator took into consideration the absence of such accountability studies, as part of his consideration of the full body of scientific evidence, in reaching his judgment that there was considerable uncertainty in the potential for increased public health protection from further reductions in ambient PM2.5 concentrations beyond those achieved under the existing primary PM2.5 NAAQS (85 FR 82717, December 18, 2020). However, there are several accountability studies available since the literature cutoff date of the 2019 ISA and evaluated in the ISA Supplement in this reconsideration that have starting concentrations (or concentrations prior to the policy or intervention) below 12.0 µg/m3 (Corrigan et al, 2018; Henneman et al., 2019; Sanders et al., 2020a). The current Administrator concludes that, while the number of available accountability studies is limited, he recognizes that these studies provide supplemental information for consideration for informing decisions on the appropriate level of the primary annual PM2.5 standard along with the full body of evidence.
As EPA has frequently noted throughout this document, the extent to which the current primary PM2.5 standards are judged to be adequate depends in part on science policy and public health policy judgments to be made by the Administrator on the strength and uncertainties of the scientific evidence, such as how to consider epidemiologic evidence and the need for an adequate margin of safety in setting the standards. Thus, it would be pure speculation to guess whether the then-Administrator would have reached the same or different conclusions in the 2020 final decision had the record before him included the newly available information in this reconsideration.[107] However, the current Administrator concludes that, for the reasons explained herein that, in his judgment, based on the record before him in this reconsideration, it is necessary and appropriate to revise the primary annual PM2.5 NAAQS to provide requisite protection of public health with an adequate margin of safety.
Based on the available scientific evidence and quantitative information, as well as consideration of the CASAC's advice and public comments, the Administrator concludes that the Start Printed Page 16277 current primary annual PM2.5 standard is not adequate to protect public health with an adequate margin of safety. In addition, he finds the available information insufficient to call into question the adequacy of the public health protection afforded by the current primary 24-hour PM2.5 standard.
In considering how to revise the current suite of primary PM2.5 standards in order to achieve the requisite protection for public health, with an adequate margin of safety, against long- and short-term PM2.5 exposures the Administrator considers the four basic elements of the NAAQS (indicator, averaging time, form, and level) collectively. With respect to indicator, the Administrator recognizes that the scientific evidence in this reconsideration, as in previous reviews, continues to provide strong support for health effects associated with PM2.5 mass. He notes the 2022 PA conclusion that the available information continues to support the PM2.5 mass-based indicator and remains too limited to support a distinct standard for any specific PM2.5 component or group of components, and too limited to support a distinct standard for the ultrafine fraction of PM (U.S. EPA, 2022b, section 3.6.3.2.1). In its advice on the adequacy of the current primary PM2.5 standards in their review of the 2021 draft PA, the CASAC reached consensus that the PM2.5 mass-based indicator should be retained, without revision (Sheppard, 2022a, p. 2 of consensus letter).[108] Additionally, there was no information in the public comments that provided a rationale for an alternative indicator. For all of these reasons, the Administrator concludes that it is appropriate to retain PM2.5 mass as the indicator for the primary standards for fine particles.
Consistent with his proposed conclusions regarding averaging time, the Administrator notes that the scientific evidence continues to provide strong support for health effect associations with both long- and short-term PM2.5 exposures (88 FR 5618, January 27, 2023). Epidemiologic studies continue to provide strong support for health effects associated with short-term PM2.5 exposures based on 24-hour averaging periods, and associations in epidemiologic studies with subdaily estimates are less consistent and, in some cases, smaller in magnitude (88 FR 5618, January 27, 2023). Taken together, the 2019 ISA concludes that epidemiologic studies do not indicate that subdaily averaging periods are more closely associated with health effects than the 24-hour average exposure metric (U.S. EPA, 2019a, section 1.5.2.1). In addition, controlled human exposure and panel-based studies of subdaily exposures typically examine subclinical effects rather than the more serious population-level effects that have been reported to be associated with 24-hour exposures ( e.g., mortality, hospitalizations). While recent controlled human exposure studies provide consistent evidence for cardiovascular effects following PM2.5 exposures for less than 24 hours ( i.e., <30 minutes to 5 hours), air quality analyses have shown that the current averaging times can effectively protect against the exposure concentrations in these studies. This information does not indicate that a revision to the averaging time is necessary to provide additional protection against subdaily PM2.5 exposures, beyond that provided by the current primary annual and 24-hour PM2.5 standards. The Administrator also notes that this conclusion is also support by the CASAC's advice in their review of the 2021 draft PA where they reached consensus that averaging times for the primary PM2.5 standards should be retained, without revision (Sheppard, 2022a, p. 2 of consensus letter).[109] The Administrator also considers the relatively few public comments received that support a subdaily averaging time, but concludes that the currently available information does not provide support for an alternate averaging time. Consistent with his proposed decision, the Administrator concludes that it is appropriate to retain the annual and 24-hour averaging times for the primary PM2.5 standards to protect against long- and short-term PM2.5 exposures.
With regard to form, the Administrator first notes that the EPA has set both an annual standard and a 24-hour standard to provide protection from health effects associated with both long- and short-term exposures to PM2.5 (62 FR 38667, July 18, 1997; 88 FR 5620, January 27, 2023). With regard to the form of the annual standard, the Administrator recognizes that a large majority of the recently available epidemiologic studies continue to report associations between health effects and annual average PM2.5 concentrations. These studies of annual average PM2.5 concentrations provide support for retaining the current form of the annual standard to provide protection against long- and short-term PM2.5 exposures. In its review of the 2021 draft PA, the CASAC reached consensus that the form of the annual standard ( i.e., annual mean, averaged over 3 years) should be retained, without revision (Sheppard, 2022a, p. 2 of consensus letter).[110] The Administrator also notes that there were no public comments that recommended an alternative form for the primary annual PM2.5 standard.
With regard to the form of the 24-hour standard (98th percentile, averaged over three years), epidemiologic studies continue to provide strong support for health effect associations with short-term ( e.g., mostly 24-hour) PM2.5 exposures, and controlled human exposure studies provide evidence for health effects following single short-term “peak” PM2.5 exposures (88 FR 5618, January 27, 2023). Therefore, the Administrator concludes that the evidence supports retaining a standard focused on providing supplemental protection against short-term peak exposures and supports a 98th percentile form for a 24-hour standard, in combination with a primary annual PM2.5 standard with its annual mean averaged over three years form. As described in the proposal and in responding to comments in section II.B.3 above, the Administrator further notes that the 98th percentile, averaged over three years, form also provides an appropriate balance between limiting the occurrence of peak 24-hour PM2.5 concentrations and identifying a stable target for risk management programs (U.S. EPA, 2022b, section 3.6.3.2.3). Furthermore, the Administrator notes that the multi-year percentile form ( i.e., averaged over three years) offers greater stability to the air quality management process by reducing the possibility that statistically unusual indicator values will lead to transient violations of the standard. This conclusion is also supported by the CASAC's advice in their review of the 2021 draft PA, where they reached consensus that the form for the primary PM2.5 standards should be retained, without revision (Sheppard, 2022a, p. 2 of consensus letter).[111]
The Administrator also recognizes that the CASAC recommended that in future reviews, the EPA also consider alternative forms for the primary 24-hour PM2.5 standard (Sheppard, 2022a, Start Printed Page 16278 p. 18 of consensus responses). Based on the CASAC's advice, the proposal solicited comment on alternatives to the current form for consideration in future reviews (88 FR 5619, January 27, 2023). The Administrator recognizes that there were a limited number of public comments related to the form of the primary PM2.5 standards as discussed in section II.D.3 above and in the Response to Comments document, and notes that, the EPA will consider the information provided by the commenters regarding the form of the 24-hour PM2.5 standard in the next review of the PM NAAQS. Consistent with his proposed decision, in considering the information summarized above, the Administrator concludes that it is appropriate to retain the forms of the current annual and 24-hour PM2.5 standards.
In considering how to revise the current suite of PM2.5 standards to provide the requisite public health protection with an adequate margin of safety, the Administrator next evaluates the appropriate levels of the primary PM2.5 standards, beginning with the annual PM2.5 standard. In having carefully considered public comments related to the primary annual PM2.5 standard, the Administrator believes that the fundamental conclusions regarding the scientific evidence and quantitative information that supported his proposed conclusions (as described in the 2019 ISA, ISA Supplement, 2022 PA, and the proposal) remain valid. In considering the level at which the primary annual PM2.5 standard should be set, the Administrator considers the entire body of evidence and information, giving appropriate weight to each part of that body of evidence and information. He continues to place the greatest weight in this reconsideration on the available scientific evidence that provides support for associations between health effects and long- and short-term PM2.5 exposures. In conjunction with his decisions to retain the current indicator, averaging time, and form as described above, the Administrator is revising the level of the primary annual PM2.5 standard to 9.0 µg/m3 . In so doing, he is selecting a primary annual PM2.5 standard that, together with the primary 24-hour PM2.5 standard, provides requisite public health protection with an adequate margin of safety, based on his judgments about and interpretation of the scientific evidence and quantitative risk information.
The Administrator's decision to revise the level of the primary annual PM2.5 standard to 9.0 µg/m3 builds upon his conclusion that the overall body of scientific evidence and quantitative risk information calls into question the adequacy of public health protection afforded by the current standard, particularly for at-risk populations. Consistent with his consideration of the available information in reaching his proposed decisions, the Administrator's final decision on the level of the primary annual PM2.5 standard places the greatest emphasis on key U.S. epidemiologic studies that report associations between long- and short-term PM2.5 exposures and mortality and morbidity. As in the proposal, and as discussed further below, he views additional epidemiologic studies ( i.e., studies that employ alternative methods for confounding control, studies that employ restricted analyses, and accountability studies), the controlled human exposure studies, and the risk assessment as providing supplemental information in support of his decision to revise the current annual standard, but recognizes that some of these lines of evidence and information provide a more limited basis for selecting a particular standard level among a range of options. See Mississippi, 744 F. 3d at 1351–52 (studies can legitimately support a decision to revise the standard, but not provide sufficient information to justify their use in setting the level of a revised standard).
Given his consideration of the scientific evidence, quantitative risk information, advice from the CASAC, and public comments, the Administrator judges that a primary annual PM2.5 standard with a level of 9.0 µg/m3 is requisite to protect public health with an adequate margin of safety. He notes that the determination of what constitutes an adequate margin of safety is expressly left to the judgment of the EPA Administrator. See Lead Industries Association v. EPA, 647 F.2d at 1161–62; Mississippi, 744 F.3d at 1353. He further notes that in evaluating how particular standards address the requirement to provide an adequate margin of safety, it is appropriate to consider such factors as the nature and severity of the health effects, the size of the at-risk populations, and the kind and degree of the uncertainties present. In considering the need for an adequate margin of safety, the Administrator notes that a primary annual PM2.5 standard with a level of 9.0 µg/m3 would be expected to provide substantial improvements in public health compared to the current annual standard, including for at-risk groups such as children, older adults, people with preexisting conditions, minority populations, and low SES populations.
Consistent with his conclusions on the need for revision of the current annual standard, in reaching a decision on level, the Administrator places the most weight on information from epidemiologic studies. In so doing, the Administrator notes that these studies provide consistent evidence of positive and statistically significant associations between long- and short-term exposure to PM2.5 and mortality and morbidity (88 FR 5624, January 27, 2023). The Administrator recognizes that placing weight on the information from the epidemiologic studies allows for examination of the entire population, including those that may be at comparatively higher risk of experiencing a PM2.5 -related health effects ( e.g., children, older adults, minority populations) (88 FR 5624, January 27, 2023). The Administrator also recognizes that recent epidemiologic studies continue to support a no-threshold relationship, meaning that there is no “bright line” below which no effects have been found. These studies also support a linear relationship between health effects and PM2.5 exposures at PM2.5 concentrations greater than 8 μg/m3 , though uncertainties remain about the shape of the C–R curve at PM2.5 concentrations less than 8 μg/m3 , with some recent studies providing evidence for either a sublinear, linear, or supralinear relationship at these lower concentrations (U.S. EPA, 2019a, section 11.2.4; U.S. EPA, 2022a, section 2.2.3.2; 88 FR 5625, January 27, 2023).
As at the time of proposal, the Administrator notes that some recent epidemiologic studies have adopted a broad range of approaches to examine confounding and the results of those examinations support the robustness of reported associations seen in epidemiologic studies. These include studies that employ alternative methods for confounder control and studies that evaluate the uncertainty related to exposure measurement error, both of which continue to support associations between PM2.5 exposures and health effects while taking approaches to address uncertainties.
In considering the epidemiologic evidence, the Administrator judges that, in reaching his decision on an appropriate level for the annual standard that will protect public health with an adequate margin of safety, in the absence of any discernible population-level thresholds, and in recognizing the need to weigh uncertainties associated with the epidemiologic evidence, it is most appropriate to examine where the evidence of associations observed in the Start Printed Page 16279 epidemiologic studies is strongest and, conversely, to place less weight where he has less confidence in the associations observed in the epidemiologic studies. As at the time of proposal, the Administrator notes that in previous reviews, evidence-based approaches noted that the evidence of an association in any epidemiologic study is “strongest at and around the long-term average where the data in the study are most concentrated” (78 FR 3140, January 15, 2013). Given this, these approaches focused on identifying standard levels near or somewhat below long-term mean concentrations reported in key epidemiologic studies. These approaches were supported by previous CASAC advice as well as the CASAC's advice in their review of the 2021 draft PA as a part of this reconsideration.
Additionally, the Administrator acknowledges that in the 2020 final action, the then-Administrator decided to retain the standard based in part on concerns about placing reliance on the epidemiologic studies and his judgment that even if he did rely on them, the majority of the studies had means or medians, as well as the mean of all of the key study-reported means or medians, above the level of the current annual standard. However, after considering the evidence, the advice of CASAC, and public comments the Administrator judges that this approach is insufficient to protect public health with an adequate margin of safety. The Administrator's decision to reach a different judgment about the appropriate level of the annual standard reflects the updated and expanded scientific record available to the Administrator in this reconsideration, as well as the additional advice from the CASAC and the public comments based on this newly available information. In addition, the Administrator observes the decision in this action to place weight on the epidemiologic studies, and to revise the annual primary standard to a level below the lowest long-term mean in the U.S.-based epidemiologic studies, is consistent with the EPA's past practice in PM NAAQS reviews.
In this reconsideration, the Administrator is considering the scientific record which has been expanded and updated since the 2020 final action, as well as the additional advice from the CASAC and the public comments that are based on the newly available information that expands upon the information previously available. In addition, the Administrator is exercising his judgment about how to interpret and weigh the expanded evidence in a way that is more consistent with the approaches used in prior PM NAAQS reviews. As a result, the Administrator has concluded on reconsideration that the level of the primary annual standard is not adequate and should be revised to protect public health with an adequate margin of safety.
Consistent with his proposed decisions, in reaching conclusions on the level of the primary annual PM2.5 standard, the Administrator considers the long-term [112] study-reported mean PM2.5 concentrations from key long- and short-term epidemiologic studies and sets the level of the standard to somewhat below the lowest long-term mean PM2.5 concentration.[113] He notes that in previous PM NAAQS reviews (including the 1997, 2006 and 2012 reviews), evidence-based approaches focused on identifying standard levels near or somewhat below long-term mean concentrations reported in key long- and short-term epidemiologic studies. These approaches were supported by the CASAC in previous reviews and were supported in this reconsideration by the CASAC in their review of the 2021 draft PA. In considering the available scientific evidence to inform such an approach, the Administrator notes the strength of the epidemiologic evidence which includes multiple studies that consistently report positive associations for short- and long-term PM2.5 exposure and mortality and cardiovascular effects. Some available studies also use a variety of statistical methods to control for confounding bias and report similar associations, which further supports the broader body of epidemiologic evidence for both mortality and cardiovascular effects. Additionally, he notes that recent epidemiologic studies available for consideration in reaching his final decision strengthen support for health effect associations at PM2.5 concentrations lower than in those evaluated in epidemiologic studies available at the time of previous reviews. The Administrator does recognize, however, that while these epidemiologic studies evaluate associations between distributions of ambient PM2.5 concentrations and health outcomes, they do not identify the specific exposures that led to the reported effects. As such, he notes that there is no specific point in the air quality distribution of any epidemiologic study that represents a “bright line” at and above which effects have been observed and below which effects have not been observed. The Administrator further notes that the epidemiologic studies provide the strongest support for reported health effect associations for this middle portion of the PM2.5 air quality distribution, which corresponds to the bulk of the underlying data, rather than the extreme upper or lower ends of the distribution, and concludes that the long-term study-reported means from both long- and short-term studies provide the strongest support for reported health effect associations in epidemiologic studies. For these reasons, as described in the proposal and in responding to public comments in section II.B.3 above, the Administrator concludes that it is appropriate to continue to employ an approach that focuses on the mean PM2.5 concentrations from the key epidemiologic studies to inform his conclusions regarding the appropriate level for the primary annual PM2.5 standard.
In adopting such an approach, the Administrator considers the long-term mean concentrations reported in two types of key epidemiologic studies: (1) Monitor-based studies [114] (epidemiologic studies that used ground-based monitors to estimate exposure, similar to approaches used in past reviews), and (2) hybrid modeling-based studies [115] (epidemiologic studies that used hybrid modeling approaches and apply aspects of population weighting to estimate exposures). In reaching conclusions regarding the level of a standard that would provide requisite protection with an adequate margin of safety, the Administrator recognizes that he must use his judgment regarding the appropriate weight to place on the available evidence and technical information, including uncertainties. As shown in Figures 1 and 2 above, for the key U.S. monitor-based epidemiologic studies, Start Printed Page 16280 the study-reported mean concentrations range from 9.9–16.5 μg/m3 , and for the key U.S. hybrid modeling-based epidemiologic studies, the mean concentrations range from 9.3–12.2 μg/m3 . The Administrator also recognizes that, in their review of the 2021 draft PA, both the majority and minority of the CASAC emphasized the epidemiologic studies in support of their recommendations for the level of the annual standard, but they weighed the studies in different ways (Sheppard, 2022a, p. 16–17 of consensus responses).
Based on this information, and in considering the CASAC's advice in their review of the 2021 draft PA, the Administrator judges that it is appropriate to set the level of the primary PM2.5 standard at least as low as the lowest mean PM2.5 concentration from these key U.S.-based epidemiologic studies, which is 9.3 µg/m[3] . The Administrator additionally notes that setting the annual standard level at 9.0 µg/m[3] , which is below the lowest study-reported mean PM2.5 concentration of 9.3 µg/m[3] , would be expected to shift the distribution of PM2.5 concentrations in an area such that the area's highest monitor would generally be at or below 9.0 µg/m[3] annually, when meeting the annual standard. In this situation, the resulting average or mean PM2.5 concentration for the entire area (measured across a number of monitors) would be even further below the study-reported means,[116] and will provide adequate protection not only in areas where the highest allowable concentrations would be expected ( i.e., near design value monitors) but also in other parts of the area where PM2.5 concentrations would be expected to be maintained even lower.
As noted above, however, the Administrator must exercise his judgment regarding the appropriate weight to place on the available scientific evidence and quantitative information, including uncertainties, in determining what level of the annual standard is sufficient to protect public health with an adequate margin of safety. In so doing, he considers other information available in this reconsideration to inform his judgments, including study-reported PM2.5 concentrations at lower percentiles in key epidemiologic studies, supplemental information from other types of epidemiologic studies, study-reported PM2.5 concentrations from key Canadian epidemiologic studies, and the results from the quantitative risk assessment.
In weighing the evidence in considering the requisite level of the annual standard, the Administrator also takes into account additional information from the key long- and short-term U.S. epidemiologic studies available that provide study-reported PM2.5 concentrations below the mean and, in particular, the subset of epidemiologic studies that report 25th and 10th percentile concentrations. Consistent with his proposed conclusions, as well as the CASAC's advice in their review of the 2021 draft PA and public comments, the Administrator judges that it is appropriate to place some weight on these lower percentiles in reaching his conclusions on the level of the primary annual standard. There are six key U.S. epidemiologic studies that report information on other percentiles ( e.g., 10th and 25th percentiles of PM2.5 concentrations or 10th and 25th percentiles of PM2.5 concentrations associated with health events) that are below the mean.[117] In considering the information from these studies, the Administrator first notes that the three older, monitor-based studies that report lower percentiles of PM2.5 concentrations have smaller cohort sizes than the three hybrid model-based studies. Thus, the Administrator recognizes that the older, monitor-based studies had a relatively smaller portion of the health events that were observed in the lower part of the air quality distribution because of the generally smaller size of the cohorts. He further notes that the recent hybrid model-based studies have larger cohort sizes than the older, monitor-based studies, and therefore, have more health events in the lower part of the air quality distribution. Because of the larger cohort sizes and having a larger portion of health events that are observed across the air quality distribution, the Administrator has more confidence in the magnitude and significance of the associations in the lower parts of the air quality distribution for the recent, hybrid model-based studies compared to the older, monitor-based studies. Given this, the Administrator judges that it is appropriate to place weight on the 25th percentile concentrations reported in the recently available hybrid model-based studies in reaching his conclusions regarding the appropriate level for the primary annual PM2.5 standard. However, the Administrator also recognizes that his confidence in the magnitude and significance in the reported concentrations, and their ability to inform decisions on the appropriate level of the annual standard, starts to diminish at percentiles that are even further below the mean and the 25th percentile. For these reasons, the Administrator places weight on the reported 25th percentiles concentrations in the recent hybrid model-based studies, rather than the reported 10th percentile concentrations, in reaching his conclusions regarding the appropriate level for the primary annual PM2.5 standard.
In considering the information from these studies, as described in section II.A.2.c and in responding to public comments in section II.B.3 above, the Administrator notes that there are two hybrid model-based studies with large cohort sizes that apply population weighting and report lower percentile values. These studies are Di et al. (2017b) and Wang et al. (2017) and the reported 25th percentile concentration is 9.1 µg/m[3] for both studies.[118] In considering these studies, the Administrator concludes that it is appropriate to place weight on the 25th percentile concentrations of these newer hybrid model-based studies (of 9.1 µg/m3 ) such that setting the level of the standard near these 25th percentile concentrations would provide requisite protection. The Administrator observes that an annual standard level of 9.0 µg/m3 would be near the reported 25th percentile concentrations in these studies.
As at the time of proposal, the Administrator also takes note of the study-reported long-term mean PM2.5 concentrations in long- and short-term Canadian epidemiologic studies, which ranged from 6.9 to 13.3 µg/m3 for monitor-based studies and 5.9 to 9.8 µg/m3 for hybrid model-based studies. While the Administrator notes that these studies provide additional support for associations between PM2.5 concentrations and health effects, he is also mindful that there are important differences between the exposure environments in the U.S. and Canada and that interpreting the data ( e.g., study-reported mean concentrations) Start Printed Page 16281 from the Canadian studies in the context of a U.S.-based standard may present challenges in directly and quantitatively informing decisions regarding potential alternative levels of the annual standard. For example, in terms of people per square kilometer, the U.S. population density is nearly 10 times in the contiguous U.S. compared to Canada. As described in more detail in responding to public comments in section II.B.3 above, in this reconsideration, the Administrator recognizes that this difference in population density between the U.S. and Canada is more apparent than in previous reviews because the studies available in this reconsideration use different approaches than those previously available. In the 2012 review, the available Canadian epidemiologic studies used population-weighting and focused on urban areas where monitors were available and population densities were more comparable with those in the U.S., and at that time, the U.S. and Canadian studies reported similar mean PM2.5 concentrations. However, in this reconsideration, the Administrator takes note that for the new Canadian epidemiologic studies: (1) The Canadian monitor-based studies available in this reconsideration do not apply population weighting as the previously available studies did; and (2) some of the studies now use hybrid modeling approaches for estimating exposure. The Administrator recognizes that these differences are important to consider in reaching conclusions on how these Canadian epidemiologic studies should be interpreted regarding decisions on the requisite level of the primary annual PM2.5 standard. Specifically, the Administrator notes that the more recent Canadian studies that use hybrid modeling incorporate larger portions of the country, and therefore include more rural areas. The more rural areas that are included in the study using the hybrid modeling approaches, the more important it is to consider how the population densities and exposure environments differ between the U.S. and Canada. Additionally, the Administrator notes that for hybrid modeling-based studies there is less certainty in PM2.5 exposure estimates in more rural areas, which are further from air quality monitors and where PM2.5 concentrations in the ambient air tend to be lower. For these hybrid model-based studies, the portion of the rural areas that are contributing to the study-reported mean PM2.5 concentrations in these studies is unclear. For these reasons, the Administrator concludes that it is important to consider the differences between the population exposures in the U.S. and Canadian study areas and how these differences influence the interpretation of the epidemiologic study results.
Thus, the Administrator considers the Canadian studies to inform his judgments on what level for the annual standard is requisite in light of the limitations and challenges presented. The Administrator also recognizes that the majority of the CASAC in their review of the 2021 draft PA, as well as a number of public commenters, place weight on the Canadian epidemiologic studies in recommending that the level of the primary annual PM2.5 standard be revised to 8–10 µg/m3 . The Administrator further notes while the majority of the CASAC advised the EPA to consider the Canadian studies in revising the annual standard level to within the range of 8.0–10.0 µg/m3 , they did not advise the EPA to set the annual standard level below the study-reported means from those studies. Given these considerations, the Administrator judges that it is appropriate to set the level of annual standard within the range of 8–10 µg/m3 to be consistent with the majority of the CASAC's advice in their consideration of these studies.
The Administrator also recognizes that information from epidemiologic studies that included analyses that restrict annual average PM2.5 concentrations to concentrations below the level of the current annual standard can be useful for informing conclusions regarding the appropriate level of the primary annual PM2.5 standard. In so doing, he particularly notes the two key U.S. epidemiologic studies (Di et al., 2017b and Dominici et al., 2019) that restrict annual average PM2.5 concentrations to less than 12 µg/m3 and report positive and statistically significant associations with all-cause mortality and mean PM2.5 concentrations of 9.6 µg/m3 . He also considers these results along with the uncertainties and limitations associated with studies that restricted analyses below certain PM2.5 concentrations. As described in responding to comments in section II.B.3 above, uncertainties associated with how the studies exclude PM2.5 concentrations from the analyses ( e.g., at what spatial resolution are concentrations being excluded), make it difficult to understand how to interpret the results of the restricted analyses in the context of the approach employed in this reconsideration, which takes into consideration the relationship between mean PM2.5 concentrations and design values.
The Administrator also recognizes that, in their review of the 2021 draft PA, the CASAC noted that epidemiologic studies that restrict analyses below certain PM2.5 concentrations represent one area for which the evidence has expanded in this reconsideration, stating that these studies provide support for mortality effects at concentrations below the current PM NAAQS (Sheppard, 2022a, p. 5 of consensus responses). In their recommendations on alternative levels for the primary annual PM2.5 standard, the majority of the CASAC cited to studies that restrict PM2.5 concentrations to below 12 µg/m3 as a part of their rationale for supporting a level within the range of 8–10 µg/m3 (Sheppard, 2022a p. 16 of consensus responses). Additionally, the Administrator notes that some members of the CASAC, in their review of the 2019 draft PA, concluded that the epidemiologic studies that restrict analyses below 12 µg/m3 and show positive associations with health effects, along with other aspects of the scientific evidence, provide support for their conclusion that the primary annual PM2.5 standard is not adequate (Cox, 2019b, p. 9 of consensus responses). Furthermore, the Administrator takes note of public commenters who also noted that the epidemiologic studies that restrict PM2.5 concentrations to below the current standard provide support, along with the other available information, for lowering the level of the primary annual PM2.5 standard. In considering the studies that include restricted analyses, along with the CASAC's advice and public comments on these types of studies, the Administrator concludes that, although there are inherent uncertainties associated with this limited body of evidence, these studies that apply restricted analyses provide support for serious effects ( e.g., mortality) at concentrations below 10.0 µg/m3 . Given this, the Administrator concludes that it is appropriate to place some weight on these studies, and in doing so, notes that a standard level of 9.0 µg/m3 would be below the reported mean PM2.5 concentrations of 9.6 µg/m3 in these studies and would, thus, be expected to provide protection against exposures related to these reported mean concentrations.
The Administrator also takes into consideration recent U.S. accountability studies, which assess the health effects associated with actions that improve air quality ( e.g., air quality policies or implementation of an intervention). These types of studies can also reduce uncertainties related to residual confounding of temporal and spatial factors (U.S. EPA, 2022a, p. 3–25). The Start Printed Page 16282 Administrator notes that in the 2020 review, the available accountability studies had “starting” annual average PM2.5 concentrations ( i.e., mean concentration prior to reductions being evaluated) from 13.2–31.5 µg/m3 , and the then-Administrator cited the lack of accountability studies in areas where the “starting” concentration met the current primary PM2.5 standards as part of his rationale for retaining the standards. As at the time of proposal, the current Administrator notes that in three studies newly available in this reconsideration and assessed in the ISA Supplement, prior to implementation of the policies, mean PM2.5 concentrations in these studies were below the level of the current annual standard level (12.0 µg/m3 ) and ranged from 10.0 µg/m3 to 11.1 µg/m3 . These studies report positive and significant associations between mortality and cardiovascular morbidity and reductions in ambient PM2.5 following the implementation of a policy (Henneman et al., 2019; Corrigan et al., 2018; Sanders et al., 2020a; 88 FR 5627, January 27, 2023). These studies suggest that public health improvements may occur following the implementation of a policy that reduces annual average PM2.5 concentrations below the level of the current standard of 12.0 µg/m3 . The Administrator recognizes that in their review of the 2021 draft PA, the CASAC noted that the availability of recent accountability studies was one area where the evidence had been strengthened and that the studies assessed in the ISA Supplement provide evidence of mortality effects at annual average PM2.5 concentrations below the current NAAQS (Sheppard, 2022a, p. 5 of consensus responses). The Administrator recognizes that the CASAC also concluded that, along with other lines of evidence, the accountability studies with starting concentrations below the levels of the current standards are appropriate to consider for informing conclusions on alternative standard levels (Sheppard, 2022a, p. 13 of consensus responses). The Administrator also notes the advice of the CASAC in their review of the 2019 draft ISA, where they suggested that accountability studies be taken into account and such studies provide potentially crucial information about whether and how much decreasing PM2.5 causes decreases in future health effects, which reflects the primary purpose of the NAAQS (Cox, 2019b, p. 8 and 10 of consensus responses). The Administrator also notes that in their review of the 2019 draft ISA, some members of the CASAC cautioned against placing more weight on the data from accountability studies based on the methodological limitations of the studies (Cox, 2019b, p. 8 of consensus responses). The Administrator notes that the CASAC did not explicitly cite to accountability studies in their reviews of the 2019 draft PA or 2021 draft PA as support for their recommendations on the adequacy of the primary annual PM2.5 standard or potential alternative standard levels. A number of public commenters who support revising the level of the standard to 8 µg/m3 cite these accountability studies, along with the broader evidence base, as support for a more protective standard. The Administrator, in considering the evidence, the advice from the CASAC, and public comment, first recognizes that accountability studies are just one line of evidence to be considered in the broader evaluations of the information available to inform conclusions on the level of the standard. In so doing, he notes that public health improvements may occur following the implementation of a policy that reduces annual average PM2.5 concentrations below the level of the current standard of 12.0 µg/m3 , and potentially below the lowest “starting” concentrations in these studies of 10.0 µg/m3 . However, the Administrator concludes that the limited number of accountability studies provide limited information for informing decisions on the appropriate level of the primary annual PM2.5 standard but recognizes that these studies provide supplemental information for consideration along with the full body of evidence. Taken together, the Administrator notes a revised annual standard level of 9.0 µg/m3 is at or below the lowest starting concentration of these accountability studies ( i.e., 10.0 µg/m3 ), and judges that it is appropriate to place some weight on these studies, particularly for informing his public policy judgments regarding an adequate margin of safety.
In addition to his consideration of and conclusions regarding the available scientific evidence, the Administrator also considers the results of the quantitative risk assessment to inform his conclusions regarding the appropriate level for the primary annual PM2.5 standard. The Administrator recognizes that the risk estimates can help to place the evidence for specific health effects into a broader public health context, but should be considered along with the inherent uncertainties and limitations of such analyses when informing judgments about the potential for additional public health protection associated with PM2.5 exposure and related health effects. The Administrator recognizes that the overall risk assessment estimates suggest that the current primary annual PM2.5 standard could allow a substantial number of PM2.5 -associated deaths in the U.S. The Administrator also recognizes that the CASAC concurred with the 2021 draft PA's assessment that meaningful risk reductions will result from lowering the annual PM2.5 standard (Sheppard, 2022a, p. 16 of consensus responses).
Additionally, with respect to the results of the quantitative risk assessment, the Administrator recognizes that the 2022 PA also provides information on the distribution of concentrations associated with the estimated mortality risk at each alternative standard level assessed (U.S. EPA, 2022b, sections 3.4.2.2 and 3.6.2.2, Figure 3–18 and 3–19). When meeting an annual standard of 9.0 µg/m3 at the design value monitor, the exposure concentrations within an area are estimated to be below 9 µg/m3 , with the majority of those exposures being at concentrations of below 8 µg/m3 . The Administrator notes that this range of concentrations is below the lowest means in the key long- and short-term epidemiologic studies (concentrations at which the evidence is the strongest in supporting an association between exposure to PM2.5 and adverse health effects observed in the key epidemiologic studies available in this reconsideration). Thus, the Administrator concludes that the results of the quantitative risk assessment suggest that a revised annual standard level of 9.0 µg/m3 is estimated to reduce PM2.5 exposures to fall within the range of concentrations in which there is the most confidence in the associations and thus, confidence that estimated risk reductions will actually occur.
The Administrator also notes the information provided by the quantitative risk assessment on the distribution of concentrations associated with the estimated mortality risk for a higher annual standard level of 10.0 µg/m3 and a lower standard level of 8.0 µg/m3 (U.S. EPA, 2022b, sections 3.4.2.2 and 3.6.2.2, Figure 3–18 and 3–19). The Administrator finds that, for an annual standard level of 10.0 µg/m3 , the quantitative risk assessment estimates that the standard would allow multiple exposures at concentrations above the lowest means in the key epidemiologic studies, and therefore, calls into question whether a standard level of 10.0 µg/m3 would provide enough public health protection. Additionally, the Administrator also finds that, for a lower annual standard level of 8.0 µg/ Start Printed Page 16283 m3 , the quantitative risk assessment estimates the exposure concentrations to be below 8 µg/m3 , with the majority of those exposures being at concentrations of below 7 µg/m3 . The Administrator observes that the majority of exposure concentrations under this air quality scenario are estimated to fall outside of the range of concentrations in which he has the most confidence in the associations and that the additional risk reductions will actually occur.
Recognizing and building upon the above considerations and judgments, and with consideration of advice from the CASAC and public comment, the Administrator concludes that the current body of scientific evidence and quantitative risk assessment support his judgment that the level of the primary annual PM2.5 standard should be revised to a level of 9.0 µg/m3 . Revising the level of the primary annual PM2.5 standard will, in the Administrator's judgment, provide requisite public health protection with an adequate margin of safety.
The Administrator recognizes that placing weight on the information from the epidemiologic studies allows for examination of the entire population, including those that may be at comparatively higher risk of experiencing a PM2.5 -related health effects ( e.g., children, older adults, minority populations) (88 FR 5624, January 27, 2023). In considering the epidemiologic evidence, the Administrator judges that, in reaching his decision on an appropriate level for the annual standard that will protect public health with an adequate margin of safety, in the absence of any discernible population-level thresholds, and in recognizing the need to weigh uncertainties associated with the epidemiologic evidence, it is most appropriate to examine where the evidence of associations observed in the epidemiologic studies is strongest and, conversely, to place less weight where he has less confidence in the associations observed in the epidemiologic studies. The Administrator notes that in previous reviews, evidence-based approaches noted that the evidence of an association in any epidemiologic study is “strongest at and around the long-term average where the data in the study are most concentrated” (78 FR 3140, January 15, 2013). These approaches were supported by previous CASAC advice as well as the CASAC's advice in their review of the 2021 draft PA as a part of this reconsideration. Given this, the Administrator notes that in revising the annual PM2.5 standard to a level of 9.0 µg/m[3] , he is setting the standard at a level below the long-term mean PM2.5 concentrations in the key long- and short-term epidemiologic studies, including the lowest study reported mean of 9.3 µg/m[3] , following an approach that is consistent with previous PM NAAQS reviews. The Administrator additionally notes that air quality analyses in the 2022 PA demonstrate that areas meeting a revised annual standard of 9.0 µg/m[3] would be expected to shift the distribution of PM2.5 exposure concentrations in an area such that the area's highest monitor would generally be at or below 9.0 µg/m[3] annually, and most of the resulting PM2.5 concentrations across the area would be even further below the study-reported means.[119 120] Thus, a standard level of 9.0 µg/m3 is expected to provide sufficient protection not only in areas where the highest allowable concentration would be located ( i.e., near design value monitors) but also in other parts of the area where PM2.5 concentrations would be expected to be maintained even lower.
Furthermore, the Administrator recognizes the CASAC's advice in their review of the 2021 draft PA, as well as public comments, that weight should be placed on study-reported PM2.5 concentrations that are somewhat below the mean, particularly for some of the newer epidemiologic studies with larger cohort sizes. In weighing uncertainties associated with using these data to inform a revised annual standard level, as well as noting the limited studies for which this information is available, the Administrator judges that some weight should be placed on these data, but they should not receive the same weight as the study-reported mean concentrations. Thus, the Administrator concludes that it would be appropriate to set the annual standard level near the 25th percentile PM2.5 concentrations in the two newer key epidemiologic studies for which these values were reported. In doing so, the Administrator notes that a decision to revise the annual standard to 9.0 µg/m3 would set a level of the standard near and somewhat below the reported 25th percentile PM2.5 concentrations of 9.1 µg/m3 in these two more recent hybrid model-based studies.
The Administrator also takes note of the study-reported long-term mean PM2.5 concentrations in the key Canadian epidemiologic studies. While the Administrator notes that these studies provide additional support for associations between PM2.5 concentrations and health effects, he is also mindful that there are important differences between the exposure environments in the U.S. and Canada that affect interpretation of the data in the context of informing decisions regarding potential alternative levels of the annual standard. The Administrator also recognizes that the majority of the CASAC in their review of the 2021 draft PA, as well as a number of public commenters, placed weight on the Canadian epidemiologic studies in recommending that the level of the primary annual PM2.5 standard be revised to 8–10 µg/m3 . The Administrator notes that a decision to revise the annual standard to 9.0 µg/m3 would set the level of the standard within the range of levels recommended by the majority of CASAC in their consideration of these studies.
Additionally, the Administrator also considers the information provided by epidemiologic studies that use restricted analyses, as well as accountability studies. With respect to the restricted analyses, the Administrator, in considering the CASAC's advice in their review of the 2021 draft PA and many public comments on these types of studies, concludes that, although there are inherent uncertainties associated with this limited body of evidence, the studies that apply restricted analyses provide support for serious effects ( e.g., mortality) at concentrations below 10.0 µg/m3 . Additionally, in considering accountability studies, the Administrator concludes that while the small number of these studies provide limited information for informing decisions on the appropriate level of the primary annual PM2.5 standard, these studies provide supplemental information for consideration along with the full body of evidence. The Administrator further notes that these studies suggest that public health improvements may occur following the implementation of a policy that reduces annual average PM2.5 concentrations below the level of the current standard of 12.0 µg/m3 , and potentially below the lowest “starting” concentrations in these studies of 10.0 µg/m3 . Taken together, the Administrator judges that it is appropriate to place some weight on these types of studies, particularly for informing his public policy judgments regarding an adequate margin Start Printed Page 16284 of safety, and notes that a revised annual standard level of 9.0 µg/m3 is below the lowest starting concentration of the accountability studies ( i.e., 10.0 µg/m3 ), and below the concentration at which studies that apply restricted analyses provide support for serious effects ( i.e., 9.6 µg/m3 ).
The Administrator also judges that the results of the quantitative risk assessment provide support for a primary annual PM2.5 standard with a level of 9.0 µg/m3 . The results of the risk assessment suggest that when meeting an annual standard of 9.0 µg/m3 , PM2.5 exposures are maintained below 9 µg/m3 at the design value monitor, with the majority of those exposures being at concentrations below 8 µg/m3 . Thus, the Administrator notes that an annual standard level of 9.0 µg/m3 would be expected to provide protection from exposures where he has the greatest confidence in the associations between health effects and PM2.5 exposures ( i.e. the long-term mean PM2.5 concentrations in the key U.S. epidemiologic studies, of which the lowest is 9.3 µg/m3 ) and would provide an adequate margin of safety by maintaining most PM2.5 exposures even further below 9.0 µg/m3 .
When considering adequate margin of safety, the Administrator notes that in his decision to revise the annual standard level to 9.0 µg/m3 , he is placing weight on the information from the epidemiologic studies which allows for examination of the entire population, including those that may be at comparatively higher risk of experiencing a PM2.5 -related health effects ( e.g., children, older adults, minority populations). Additionally, as discussed above, the Administrator also recognizes that setting the annual standard level at 9.0 µg/m3 , which is below concentrations at which the evidence is the strongest in supporting an association between exposure to PM2.5 and adverse health effects observed in the key epidemiologic studies available in this reconsideration, would be expected to shift the distribution of PM2.5 exposure concentrations in an area such that the area's highest monitor would generally be at or below 9.0 µg/m3 annually, and most of the resulting PM2.5 concentrations across the area would be even lower. In considering these air quality relationships, the Administrator judges that a revised annual standard level of 9.0 µg/m3 would provide requisite protection with adequate margin of safety, for all populations, including those most at-risk.
In reaching this conclusion, the Administrator recognizes that in establishing primary standards under the Act that are requisite to protect public health with an adequate margin of safety, he is seeking to establish standards that are neither more nor less stringent than necessary for this purpose. The Act does not require that primary standards be set at a zero-risk level or to protect the most sensitive individual, but rather at a level that avoids unacceptable risks to public health. In this context, the Administrator's conclusion is that revised primary annual standard, in conjunction with the 24-hour standard, provides the appropriate degree of protection, and that more or less stringent standards would not be requisite.
In considering the requirement for an adequate margin of safety, the Administrator notes that the determination of what constitutes an adequate margin of safety is expressly left to the judgment of the EPA Administrator. See Lead Industries Association v. EPA, 647 F.2d at 1161–62; Mississippi, 744 F.3d at 1353. He further notes that in evaluating how particular standards address the requirement to provide an adequate margin of safety, it is appropriate to consider such factors as the nature and severity of the health effects, the size of sensitive population(s) at risk, and the kind and degree of the uncertainties present. Consistent with past practice and long-standing judicial precedent, and as described in this section, the Administrator takes the need for an adequate margin of safety into account as an integral part of his decision making on a standard. See, e.g., NRDC v. EPA, 902 F. 2d 962, 973–74 (D.C. Cir. 1990).
Given all of the evidence and information discussed above, the Administrator judges that a standard with a level of 9.0 µg/m3 is requisite to protect public health with an adequate margin of safety. In so doing, he first recognizes that a less stringent standard would allow the occurrence of higher long- and short-term PM2.5 concentrations at a level at or above the mean PM2.5 concentrations in key U.S. epidemiologic studies. That is, a less stringent standard would be expected to allow more PM2.5 exposures at concentrations at or above which the key U.S. epidemiologic studies have reported associations between mean PM2.5 concentrations and serious health effects and would deviate from some past approaches for selecting the appropriate level of the annual standard. A less stringent standard would also not provide requisite protection with an adequate margin of safety against PM2.5 exposures in the lower percentiles of the air quality distribution ( i.e., 25th percentile) for which associations with health effects have been observed in a limited number of epidemiologic studies. Furthermore, the Administrator notes that the primary annual and 24-hour PM2.5 standards, together, are intended to provide public health protection against the full distribution of long- and short-term PM2.5 exposures. As noted above, the Administrator recognizes that the changes in PM2.5 air quality designed to meet a less stringent annual standard would likely result in higher exposures across the distribution of air quality, including both higher average (or typical) concentrations as well as higher short-term peak PM2.5 concentrations. Taking into consideration both the full evidence base for associations of PM2.5 with mortality and other adverse health effects, including the reported mean PM2.5 concentrations from key long- and short-term U.S. epidemiologic studies, information from epidemiologic studies that report 25th percentile PM2.5 concentrations, supplemental information from other epidemiologic studies ( i.e., epidemiologic studies that use restricted analyses, accountability studies, and Canadian epidemiologic studies), and the results of the risk assessment, as well as the advice from the CASAC and public comments, the Administrator concludes that a less stringent standard would allow risks of mortality and other adverse health effects that are too great, and thus would not provide sufficient protection for public health as required by the CAA.
Additionally, in considering a less stringent standard, the Administrator recognizes that through its control of long- and short-term PM2.5 concentrations, the annual standard provides a margin of safety for less well-studied exposure levels and population groups for which the evidence is limited or lacking. In so doing, he recognizes that our understanding of the relationships between the presence of a pollutant in ambient air and associated health effects is based on a broad body of information encompassing not only more established aspects of the evidence, such as the conclusion that long- and short-term exposures to PM2.5 are causally related to mortality and cardiovascular effects and likely to be causally related to respiratory effects, but also aspects with which there may be substantial uncertainty. In particular, the Administrator notes that there are other categories of effects with causality determinations that are suggestive of, but not sufficient to infer, a causal Start Printed Page 16285 relationship between PM2.5 exposure and health outcomes. These include, but are not limited t,o short-term exposure and nervous system effects, as well as long- and short-term exposure and pregnancy and birth outcomes, where the evidence is less certain but which represent potentially substantial additional risk to public health from exposure to PM2.5 . He recognizes the CAA requirement that requires primary standards to provide an adequate margin of safety was intended to address uncertainties associated with inconclusive scientific and technical information as well as to provide a reasonable degree of protection against hazards that research has not yet identified and in his judgment, the primary NAAQS must be set at a level that is adequately protective against these and other effects which research has not yet identified. Thus, even if the Administrator had somewhat greater concerns about the possibility of confounding, error and bias in the epidemiologic studies, which reduced his confidence in finding that PM2.5 is causally related to mortality and cardiovascular effects, he would still find it appropriate to set the primary NAAQS below the means of key U.S. epidemiologic studies given the strength of the evidence providing support for the association, as well as additional evidence linking PM2.5 to other endpoints of substantial public health concern, and the need to protect public health with an adequate margin of safety. In considering the uncertainties in both the epidemiologic evidence and the controlled human exposures studies, the Administrator recognizes that collectively, the health effects evidence generally reflects a continuum, consisting of levels at which scientists generally agree that health effects are likely to occur, through lower levels at which the likelihood and magnitude of the response become increasingly uncertain. In light of these uncertainties, the Administrator recognizes that the CAA requirement that primary standards provide an adequate margin of safety, as summarized in section I.A above, is intended to address uncertainties associated with inconclusive scientific and technical information, as well as to provide a reasonable degree of protection against hazards that research has not yet identified. The Administrator has taken the need to provide for an adequate margin of safety into account as an integral part of his decision-making on the appropriate standards in setting the standard at a level below the level where available epidemiologic studies, which include diverse populations that are broadly representative of the U.S. population including at-risk populations, have provided the strongest evidence supporting effects, and in other ways as well. For example, consideration of a margin of safety is reflected in the approach of setting the level of the annual standard near and somewhat below the 25th percentile PM2.5 concentrations from key U.S. epidemiologic studies ( i.e., 9.1 µg/m3 ), as well as recognition that attaining a design value will generally result in significantly broader and greater improvements of air quality across an area (including but certainly not limited to areas near the design value monitor) (U.S. EPA, 2022a, sections 2.3.3.2.4 and 3.3.3.2.1, Table 3–5). Based on all of the considerations noted here, and considering the current body of evidence, including the associated limitations and uncertainties, in combination with the exposure/risk information, the Administrator concludes that a less stringent standard than the current standard would not provide the requisite protection of public health, including an adequate margin of safety.
Having concluded that a less stringent standard would not provide the requisite protection of public health, the Administrator next considers whether a more stringent standard would be appropriate. In so doing, he notes that a decision to set the level of the annual standard to below 9.0 µg/m3 would place a large amount of the emphasis on potential public health importance of further reducing the occurrence of PM2.5 concentrations of concern, though the exposures about which he is most concerned are well controlled with an annual standard level of 9.0 µg/m3 , as demonstrated by the quantitative risk assessment. Such a decision would also place greater weight on (1) further reducing ambient PM2.5 concentrations relative to those observed in long-and short-term epidemiologic studies, including those that he had judged to have significant uncertainties, including Canadian studies, studies using restricted analyses, and accountability studies; (2) shifting the air quality distribution in areas such that the highest exposure concentrations are reduced to below PM2.5 concentrations observed in epidemiologic studies to be in the 25th or lower percentile, for which the evidence is limited; and (3) further shifting exposure concentrations to those shown at the lower end of the distribution in the quantitative risk assessment, despite the important uncertainties in the overall risk assessment. As discussed in this section and in responses to significant comments above and in the Response to Comments document, the Administrator has concluded that placing a large emphasis on these factors and revising the standard to a level below 9.0 µg/m3 would result in a standard that is more stringent than the evidence indicates to be sufficient to protect public health with an adequate margin of safety. Compared to a primary annual PM2.5 standard set at a level of 9.0 µg/m3 , the Administrator concludes that the extent to which lower standard levels could result in further public health improvements becomes notably less certain.
Thus, having carefully considered the scientific evidence, quantitative information, CASAC advice, and public comments relevant to his decision on the level of the primary annual PM2.5 standard, as discussed above and in the Response to Comments document, the Administrator is revising the level of the primary annual PM2.5 standard to 9.0 µg/m3 . In the Administrator's judgment, based on the currently available evidence and information, an annual standard set at this level and using the specified indicator, averaging time, and form, in conjunction with the other primary PM standards, would be requisite to protect public health with an adequate margin of safety. The Administrator judges that such a standard would protect, with an adequate margin of safety, the health of at-risk populations, including children, older adults, those with pre-existing cardiovascular and respiratory diseases, minority populations, and low SES populations. The Administrator believes that a standard set at 9.0 µg/m3 would be sufficient to protect public health with a margin of safety, and believes that a lower standard would be more than what is necessary to provide this degree of protection. This judgment by the Administrator appropriately considers the degree of protection that is neither more nor less stringent than necessary for this purpose and recognizes that the CAA does not require that primary standards be set at a zero-risk level, but rather at a level that reduces risk sufficiently so as to protect public health with an adequate margin of safety.
In reaching his conclusions on adequacy of the current suite of primary PM2.5 standards, based on consideration of the available scientific evidence and quantitative information, the CASAC's advice and public comments, the Administrator finds that the available information is insufficient to call into question the adequacy of the public Start Printed Page 16286 health protection afforded by the current primary 24-hour PM2.5 standard. As described earlier in this section, the Administrator concludes that it is appropriate to retain the current indicator (PM2.5), averaging time (24-hour), and form (98th percentile, averaged over three years) for the primary 24-hour PM2.5 standard and below explains the basis for his final decision that is also appropriate to retain the current level of the primary 24-hour PM2.5 standard.
In reaching his conclusion to retain the current primary 24-hour PM2.5 standard the Administrator does so in light of the conclusion that the epidemiologic evidence supports associations between short- and long-term PM2.5 exposures and adverse health effects, but that the epidemiologic evidence does not identify specific concentrations at which those effects occur and the Administrator has greatest confidence in effects where the bulk of the data is reported ( i.e., the mean PM2.5 concentration, with some consideration for the 25th percentile of the air quality distribution). Thus, in considering the epidemiologic evidence, the Administrator concludes it is appropriate to focus on setting a generally controlling annual standard as the most effective and efficient way to reduce total population risk associated with both long- and short-term PM2.5 exposures, and that it is appropriate to revise the level of the annual standard level to 9.0 µg/m3 . In addition to the epidemiologic evidence, the Administrator also considers the available controlled human exposure studies, which provide evidence for health effects following single, short-term PM2.5 exposures to concentrations that typically correspond to upper end of the PM2.5 air quality distribution in the U.S. ( i.e., “peak” concentrations). In so doing, the Administrator notes that these studies report statistically significant effects on one or more indicators of cardiovascular function following 2-hour exposures to PM2.5 concentrations at and above 120 μg/m3 and at and above 149 μg/m3 for vascular impairment, the effect shown to be most consistent across studies. In particular, the Administrator notes that a single study is assessed in the ISA Supplement that reports effects following 4-hour exposures at 37.8 µg/m3 , although the results of this study are inconsistent with the results of the controlled human exposure studies assessed in the 2019 ISA. Along with the inconsistent results from the controlled human exposure studies, the Administrator also recognizes that effects observed in these studies are intermediate effects which are not typically considered adverse and that the study participants were healthy individuals. Taking into consideration the available scientific evidence, including the uncertainties and limitations, along with the CASAC's advice, the Administrator concludes that it is appropriate to maintain a primary 24-hour PM2.5 standard to protect against peak exposures.
Thus, the Administrator considers what primary 24-hour PM2.5 standard is requisite to provide supplemental protection against peak exposures. While having confidence that the revised annual standard will result in lowering risk associated with both long- and short-term PM2.5 exposure by lowering the overall air quality distribution, as in the 2012 review, the Administrator recognizes that an annual standard alone would not be expected to offer sufficient protection with an adequate margin of safety against the effects of short-term PM2.5 exposures in all parts of the country. Therefore, he continues to conclude that it is appropriate to continue to provide supplemental protection by means of a 24-hour standard, in conjunction with a revised annual standard level of 9.0 µg/m3 .
In considering the available scientific evidence assessed in the 2019 ISA and ISA Supplement, the Administrator first considers the controlled human exposure studies for informing his decisions on the primary 24-hour PM2.5 standard. In so doing, he notes that in their review of the 2021 draft PA, the majority of CASAC members expressed the view that controlled human exposure studies are not the best evidence to use for justifying retaining the 24-hour standard without revision, in part because these studies preferentially recruit less susceptible individuals and have a typical exposure duration much shorter than 24 hours. Thus, in the view of the majority, “the evidence of effects from controlled human exposure studies with exposures close to the current 24-hour standard supports epidemiological evidence for lowering the standard” (Sheppard, 2022a, p. 3–4 of consensus letter). In reviewing the controlled human exposure studies, the Administrator agrees with the majority of CASAC that these controlled human exposure studies generally do not include populations with substantially increased risk from exposure to PM2.5, such as children, older adults, or those with more severe underlying illness. However, he disagrees with any conclusion that they should not be used to inform a decision about the adequacy of the current standard. The Administrator finds the information available from these studies to be useful, noting that the recently available controlled human exposure studies provide evidence for health effects following single, short-term exposures to PM2.5 concentrations that are greater than those allowed under the current standard. The results of the controlled human exposure studies are inconsistent, particularly at lower PM2.5 concentrations, but some studies do report statistically significant effects on one or more indicators of cardiovascular function following 2-hour exposures to PM2.5 concentrations at and above 120 μg/m3 (and at and above 149 μg/m3 for vascular impairment, the effect shown to be most consistent across studies). Additionally, one controlled human exposure study assessed in the ISA Supplement reports evidence of some effects for cardiovascular markers following 4-hour exposures to 37.8 µg/m3 (Wyatt et al., 2020). However, there is inconsistent evidence for inflammation in other controlled human exposure studies evaluated in the 2019 ISA. The Administrator finds these studies are important in establishing biological plausibility for PM2.5 exposures causing more serious health effects, such as those seen in short-term exposure epidemiologic studies, and they provide support that more adverse effects may be experienced following longer exposure durations and/or exposure to higher concentrations. As described in more detail in responding to public comments in section II.B.3 above, he notes that although the controlled human exposure studies do not provide a threshold below which no effects occur, the observed effects in these controlled human exposures studies are ones that signal an intermediate effect in the body, likely due to short-term exposure to PM2.5, and typically would not, by themselves, be judged as adverse. As noted in sections II.A.2 and II.B.3 above, associated judgments regarding adversity or health significance of measurable physiological responses to air pollutants in previous NAAQS reviews have been informed by guidance, criteria or interpretative statements developed within the public health community. This type of information on adversity of effects is particularly informative to the Administrator's judgments regarding the adversity of the effects observed in the controlled human exposure studies which are short-term in nature ( i.e., generally ranging from 2- to 5-hours), including those studies that are Start Printed Page 16287 conducted at near-ambient PM2.5 concentrations. Based on the observation that the effects observed in Wyatt et al. (2020) are not by themselves adverse, and the fact that the findings of this study are inconsistent with other currently available evidence regarding the level at which effects are observed, the Administrator disagrees with the view expressed by the majority of CASAC that this study supports epidemiologic evidence for lowering the 24-hour standard.
Consistent with his approach in reaching his proposed decision and taking into consideration these points as well as balancing these limitations ( i.e., that the health outcomes observed in these controlled human exposure studies are not clearly adverse and that the studies generally do not include those at increased risk from PM2.5 exposure), the Administrator still considers it appropriate to ensure that the 24-hour PM2.5 standard provides protection against health effects consistently observed in the controlled human exposure studies. He next examines the air quality analyses, described in more detail in section II.A.c.i above, to assess whether during recent air quality conditions, areas meeting the current standards would experience PM2.5 concentrations reported in these controlled human exposure studies. He observes that air quality analyses demonstrate that the PM2.5 exposures shown to cause consistent effects in the controlled human exposure studies are well above the ambient concentrations typically measured in locations meeting the current primary standards, and therefore suggest that the current primary PM2.5 standards provide protection against these “peak” concentrations. In fact, at air quality monitoring sites meeting the current primary PM2.5 standards ( i.e., the 24-hour standard of 35 μg/m[3] and the annual standard of 12 μg/m[3] ), the 2-hour concentrations generally remain below 10 μg/m[3] , and rarely exceed 30 μg/m[3] . Though two-hour concentrations are higher at monitoring sites violating the current standards, they generally remain below 16 μg/m[3] and rarely exceed 80 μg/m[3] , still below concentrations in CHE studies where consistent effects are observed ( e.g., greater than 120 μg/m[3] ) (U.S. EPA, 2022b, section 2.3.2.2.3, Figure 2–19, and section 3.3.3.1). Additionally, and in response to public comments, the Administrator notes additional air quality analyses conducted by the EPA,[121] that provide a more refined analysis of whether areas that meet the current standards experience peak concentrations reported in controlled human exposure studies. He notes that 2-hour observations greater than 120 μg/m3 and 4-hour observations greater than 38 μg/m3 rarely occur ( e.g., 0.025% of rolling 2-hour observations are greater than 120 μg/m3 and 0.78% of rolling 4-hour observations greater than 38 μg/m3 ). Based on this information, the Administrator finds that the current suite of standards maintains subdaily concentrations of PM2.5 in ambient air far below the exposure concentrations in controlled human exposure studies where consistent effects have been observed, and notes that while these studies generally do not include the most at-risk individuals, the exposure concentrations in these studies also do not elicit adverse effects.
Further, in light of the Administrator's emphasis on the annual standard as the controlling standard, with the 24-hour standard providing supplemental protection against peak concentrations, he next considers the potential impact of a revised annual standard of 9.0 µg/m[3] on the occurrence of peak sub-daily PM2.5 concentrations. Specifically, the Administrator takes note of the new air quality analyses [122] where he observes that lower percentages of concentrations greater than 120 µg/m3 and 38 µg/m3 occur in areas meeting an annual standard of 9.0 µg/m3 and a 24-hour standard of 35 µg/m3 , versus an annual standard of 12.0 µg/m3 and a 24-hour standard of 35 µg/m3 . Thus, he concludes that an annual standard that is controlling across most areas of the country will continue to effectively limit peak daily concentrations in conjunction with the existing 24-hour standard, with its level of 35 µg/m3 and 98th percentile form, which continues to provide supplemental protection against peak concentrations.
In addition, the Administrator also notes that the majority of the CASAC in their review of the 2021 draft PA, as well as a number of public commenters, support their recommendation to revise the current 24-hour standard by pointing to “substantial epidemiologic evidence from both morbidity and mortality studies” which “includes three U.S. air pollution studies with analyses restricted to 24-hour concentrations below 25 μg/m3 ” (Sheppard, 2022a, p. 17 consensus responses). The Administrator notes that the epidemiologic evidence available in this reconsideration, including the studies that restrict short-term PM2.5 exposures ( i.e., 24-hour PM2.5 concentrations) to levels below 25 μg/m3 , provides support for positive and statistically significant associations between short-term exposure to PM2.5 and all-cause mortality (Di et al., 2017a) and CVD hospital admissions (deSouza et al., 2021; Di et al., 2017a). He agrees that these studies help to provide additional support for reaching conclusions on causality in the 2019 ISA. He further agrees that the available epidemiologic studies provide important information that it is appropriate to consider in this reconsideration, including information on associations between health effects and PM2.5 exposures in diverse populations that are broadly representative of the U.S. population, and include populations identified as at-risk ( e.g., older adults, minority populations), as well as evidence of linear, no-threshold concentration-response relationships in those associations, although with less certainty in the shape of the curve at long-term average concentrations below about 8 μg/m3 .
However, the Administrator also notes significant limitations in the currently available epidemiologic information that limit his ability to draw conclusions from the key short-term studies, including those that employ restricted analyses, to inform his decision regarding the level of the 24-hour PM2.5 standard. As a result of these limitations, the Administrator does not find that the short-term epidemiologic studies, or the other evidence such as the controlled human exposure studies or the risk assessment, provide a sufficient justification for revising the 24-hour standard.
First, he notes that short-term epidemiologic studies examine associations between day-to-day variations in PM2.5 concentrations and health outcomes, often over multi-year study periods. As such, these studies report long-term mean 24-hour PM2.5 concentrations ( e.g., mean 24-hour PM2.5 concentrations over multi-year study periods), rather than at specific points in the distribution ( i.e., 90th or 98th percentile 24-hour concentrations) at which effects occur. Further, he notes Start Printed Page 16288 that while there can be considerable variability in daily exposures over a multi-year study period, the bulk of the observations reflect days with ambient PM2.5 concentrations in the middle of the air quality distribution ( i.e., “typical” days rather than days with extremely low or extremely high concentrations). As a result, the results of these studies are more directly applicable to decisions regarding the annual standard (which is based on the long-term mean of both short- and long-term epidemiologic studies), and the fact that they do not report other air quality statistics, such as the 98th percentile concentrations which might be more directly compared to the level of the 24-hour standard, makes them less useful for informing decisions on the 24-hour standard. As discussed in responding to comments above, the form of the annual standard is based on the annual mean PM2.5 concentration averaged over three years,[123] which makes it better suited as a basis for controlling air quality to avoid effects observed in both long-term and short-term epidemiologic studies. By contrast, the form of the 24-hour standard is the 98th percentile averaged over three years, which makes it appropriate for controlling short-term peak concentrations. However, based on the available air quality information, including distribution statistics of PM2.5 concentrations and health events reported in the short-term epidemiologic studies, these studies are too limited in their ability to identify health effects attributable to specific short-term peak concentrations that are necessary to evaluate whether the 24-hour standard with its 98th percentile form should be revised ( e.g., restricted epidemiologic studies do not report the number or the percentile of health events or the percentile of PM2.5 concentrations across the highest part of the restricted air quality distribution, including the 98th percentile). Thus, the Administrator does not consider it appropriate to use the reported means from short-term studies to determine the appropriate level for a 24-hour standard with a 98th percentile form.
Similarly, the Administrator does not consider the results of the restricted analyses to be well suited to informing the choice of level for a 24-hour standard. Restricted analyses use a subset of data from their main analyses to evaluate health events that occur at concentrations below a certain concentration ( e.g., 25 μg/m[3] ). The Administrator notes that the associations between the health effects ( e.g., mortality and cardiovascular morbidity) and PM2.5 concentrations remain even after excluding higher concentrations in the restricted analyses, and he also recognizes that the magnitude of the effect is generally greater in the restricted analyses compared to the associations reported in the main analysis. He considers such analyses to be informative in indicating that the health effects association reported in the main (unrestricted) analysis are not driven only by the upper peaks of the PM2.5 air quality distribution, but rather persist at lower portions of the distribution (consistent with his emphasis on the annual standard, which is focused on exposures near the mean concentration, where the bulk of the exposure distribution is concentrated). Indeed, he notes that if peak concentrations were the principal driver of health effects associated with PM2.5 exposure, one might expect the associations to become weaker as the upper portion of the data is excluded in the restricted analyses, which is not what is reported by the analyses ( e.g., the restricted analyses generally report associations that are greater in magnitude compared to the main analyses). However, he disagrees with the assertion by the CASAC in their review of the 2021 draft PA and some public commenters that it would be appropriate to focus on the specific PM2.5 concentration ( e.g., 25 or 30 μg/m[3] ) at which the analysis was restricted as the basis for choosing a 24-hour standard level. The Administrator recognizes that in restricted analyses, while an association continues to persist across the full range of the air quality distribution, and that the cutpoint concentration at which the analysis was restricted ( e.g., 25 or 30 µg/m[3] ) becomes the maximum PM2.5 concentration in the distribution, he also notes that these studies do not provide information related to the distribution of health events and PM2.5 concentrations, and as such, he is more uncertain where the bulk of the data are and where he has confidence in the reported association.[124] He notes that no evidence exists to support a conclusion that the PM2.5 concentration chosen as the cutpoint in a restricted analysis has any bearing on the concentration at which effects are likely to occur (or not occur). He notes that, as with long-term studies, the evidence does not suggest there is a specific point in the air quality distribution of these short-term studies that represents a “bright line” at and above which effects have been observed and below which effects have not been observed. In order to identify a level of the 24-hour standard based on associations between the “upper end” of exposures, either in the unrestricted or the restricted analyses, and adverse health effects, it would be necessary to have a better understanding of how specific 24-hour concentrations correspond to the frequency and total number of observed health events in the study. Currently, such information, including 98th percentile statistics, are not reported in the key short-term epidemiologic studies (and if they were reported, the Administrator would have to carefully consider how to weigh the data). As such, in reaching his decision on the primary 24-hour PM2.5 standard, the Administrator judges that the currently available information from short-term epidemiologic studies, including those that employ restricted analyses, does not provide a sufficient basis to revise the current 24-hour standard, given that the 24-hour standard focuses on reducing “peak” exposures (with its 98th percentile form), but rather that such information supports his judgment that it is appropriate to focus on revising the annual standard for purposes of reducing all exposures, across the entire distribution of air quality, to increase public health protection.
In reaching final decisions regarding the adequacy of the primary 24-hour PM2.5 standard, the Administrator continues to view an approach that focuses on setting a generally controlling annual standard as the most effective and efficient way to reduce total population risk associated with both long- and short-term PM2.5 exposures. Additionally, he emphasizes that improvements in air quality associated with meeting an annual standard level of 9.0 µg/m3 will result in lowering risk associated with both long- and short-term PM2.5 exposure by lowering the overall air quality distribution. The Administrator concludes that reducing the annual standard is the most efficient way to reduce the risks from short-term exposures identified in the epidemiologic studies, as the available evidence suggests the bulk of the risk comes from the large number of days across the bulk of the air quality distribution, not the relatively small number of days with peak concentrations. However, as in the 2012 Start Printed Page 16289 review, the Administrator recognizes that an annual standard alone would not be expected to offer sufficient protection with an adequate margin of safety against the effects of short-term PM2.5 exposures in all parts of the country and concludes that, in conjunction with a revised annual standard level of 9.0 µg/m3 , it is appropriate to continue to provide supplemental protection by means of a 24-hour standard, particularly for areas with high peak-to-mean ratios possibly associated with strong local or seasonal sources.
In selecting the level of a 24-hour standard designed to provide supplemental protection against peak exposures (in conjunction with a revised annual standard of 9.0 µg/m3 ), the Administrator considers the information from the controlled human exposure studies and the EPA's analysis of peak concentrations observed in areas meeting the current standard of 35 µg/m3 in conjunction with a revised standard of 9.0 µg/m3 to be of particular relevance. He notes the controlled human exposure evidence includes studies reporting effects on one or more indicators of cardiovascular function following 2-hour exposures at and above 120 µg/m3 , including effects reported at and above 149 µg/m3 for vascular impairment, the effect shown to be most consistent across studies, and less consistent effects at lower concentrations, including a single study at near ambient concentrations (Wyatt et al., 2020) reporting effects following 4-hour exposures at 37.8 µg/m3 . He recognizes that the effects observed (in those studies that observed effects) are ones that signal an intermediate effect in the body, likely due to short-term exposure to PM2.5, and typically would not, by themselves, be judged as adverse, and the study participants were healthy individuals.
He notes in particular that, in the EPA's analysis, in areas meeting the current 24-hour standard and the revised annual standard 0.029 percent of 2-hour observations and 0.41 percent of 4-hour observations reach PM2.5 concentrations higher than 120 µg/m3 and 37.8 µg/m3 , respectively. He also notes the lack of evidence of effects from controlled human exposure studies at levels below the current 24-hour standard and the fact that the results of Wyatt et al. (2020) are inconsistent with other available studies, as well as the intermediate nature of effects observed in this study. In his judgment, the small number of occurrences of peak exposures indicate that, in conjunction with a revised annual standard of 9.0 µg/m3 , the current 24-hour standard of 35 µg/m3 remains requisite to protect public health with an adequate margin of safety, and that there is substantial basis to doubt whether further improvements in public health would be achieved by further reducing these exposures. Furthermore, the Administrator concludes that due to the limitations and uncertainties outlined above, the information from recent short-term epidemiologic studies, including those that use restricted analyses, is inadequate to inform decisions regarding the adequacy of the current 24-hour standard. Thus, in reaching his decision on the primary 24-hour PM2.5 standard, the Administrator concludes that currently available evidence does not call into question the adequacy of the current standard.
In addition to the scientific evidence, the Administrator also considers the risk assessment in evaluating the appropriate level of the 24-hour PM2.5 standard. The risk assessment indicates that the annual standard is the controlling standard across most of the urban study areas evaluated ( i.e., when air quality related to the annual average PM2.5 concentrations decrease, daily average PM2.5 concentrations are also expected to decrease). When air quality is adjusted to just meet an alternative 24-hour standard level of 30 μg/m3 in the areas where the 24-hour standard is controlling, the risk assessment estimates reductions in PM2.5 -associated risks across a more limited population and number of areas compared to when air quality is adjusted to simulate alternative levels for the annual standard ( i.e., where the annual standard is controlling), and these predictions are largely confined to areas located in the western U.S., several of which are also likely to experience risk reductions upon meeting a revised annual standard. With respect to the CASAC's advice in their review of the 2021 draft PA, the Administrator notes that the minority of CASAC advised that these results suggest that the annual standard can be used to limit both long- and short-term PM2.5 concentrations and views these risk assessment results as supporting the conclusion that the current 24-hour standard is adequate (Sheppard, 2022a, p. 4 of consensus letter). In contrast, the majority of CASAC members in their review of the 2021 draft PA, as well as a number of public commenters that support revision of the 24-hour standard, placed greater weight on the evidence-based considerations ( e.g. scientific evidence, like the restricted analyses) than on the values estimated by the risk assessment, noting the potential for uncertainties in how the risk assessment was able to “capture areas with wintertime stagnation and residential wood-burning where the annual standard is less likely to be protective” (Sheppard, 2022a, p. 4 of consensus letter).
In considering the application of the risk assessment to judgments about the adequacy of the current primary 24-hour PM2.5 standard, the Administrator again notes that the risk assessment analyses of PM2.5 -attributable mortality use input data that include C–R functions from epidemiologic studies that have no threshold and a linear C–R relationship down to zero, as well an air quality adjustment approach that incorporates proportional decreases in PM2.5 concentrations to meet lower standard levels. As such, the Administrator notes that this quantitative approach does not incorporate any elements of uncertainty in associations of health effects at lower concentrations and that simulated air quality improvements will always lead to proportional decreases in risk ( i.e., each additional µg/m[3] reduction produces additional benefits with no clear stopping point at any PM2.5 concentration). Therefore, the Administrator recognizes that while the risk estimates can help to place the evidence for specific health effects into a broader public health context, the results should be considered along with the inherent uncertainties and limitations of such analyses when informing judgments about the potential for additional public health protection associated with PM2.5 exposure and related health effects. Further, the Administrator notes additionally that air quality analyses have also been considered in looking at the adequacy of the 24-hour standard in controlling peak PM2.5 concentrations of potential concern,[125] and that those analyses included monitoring information from across the entire U.S., specifically highlighting areas with higher peak concentrations and including areas impacted by wintertime stagnation and residential wood-burning. Thus, while the risk assessment may have focused on a subset of areas across the U.S. based on the study area selection criteria, the Administrator is considering a broader set of information in reaching his conclusions regarding the appropriateness of the current 24- Start Printed Page 16290 hour standard to control peak concentrations.
The Administrator also considers the advice from the CASAC in their reviews of the 2019 draft PA and 2021 draft PA. In their review of the 2019 draft PA, the CASAC “agrees with the EPA and finds that the available evidence does not call into question the adequacy of public health protection afforded by the current 24-hour PM2.5 standard and concurs that it be retained” (Cox, 2019b, p. 3 of letter). He also notes that in their review of the 2021 draft PA, the CASAC did not reach consensus on whether the current 24-hour standard is adequate, with the majority of the CASAC recommending that the 24-hour standard be revised and the minority of the CASAC recommending that the standard be retained. The majority of the CASAC members further stated that “[t]here is also less confidence that the annual standard could adequately protect against health effects of short-term exposures. A range of 25–30 μg/m3 for the 24-hour PM2.5 standard would be adequately protective” (Sheppard, 2022a, p. 4 of consensus letter). The Administrator also acknowledges that some public commenters agreed with the majority of the CASAC in supporting a revision to the level of the 24-hour standard to a range between 25–30 µg/m3 . These commenters cite a number of reasons, including: (1) Results from controlled human exposure studies at near ambient concentrations; (2) aspects of the scientific evidence, including restricted analyses that report positive and significant associations below 35 µg/m3 ; and (3) quantitative risk analyses that show decreasing risk with decreasing PM2.5 concentrations. In responding to these comments, the Administrator recognizes that some commenters have different interpretations of the evidence, air quality information, and quantitative results from the risk assessment in this review and would make different judgments about the weight to place on the relative strength and limitations of the currently available scientific evidence and information and how such information could be used in making public health policy decisions on the 24-hour standard. However, as outlined above, the Administrator has carefully considered the information available from controlled human exposure studies and short-term epidemiologic studies, and weighed the strengths and limitations of this evidence in formulating his decisions. Furthermore, as discussed above the Administrator has noted significant uncertainties and limitations inherent in the risk estimates, as well as noting that very few areas were included. In addition, he has given careful consideration to the majority of the CASAC's advice in their review of the 2021 draft PA, but has drawn different conclusions with respect to how currently available evidence and air quality information inform the selection of level for the 24-hour primary PM2.5 standard.
In considering the advice of the majority of CASAC, the Administrator notes that a decision to set the level of the 24-hour standard to below 35 µg/m3 would place a large amount of emphasis on the potential public health importance of further reducing the occurrence of peak PM2.5 concentrations. However, the Administrator concludes that there is insufficient basis to conclude that a more stringent standard to further reduce peak concentrations is needed or would benefit public health. As discussed above, he judges that the PM2.5 exposures in controlled human exposure studies that correspond to peak concentrations will already be well controlled via the combination of the revised annual standard, with a level of 9.0 µg/m3 , and the 24-hour standard with its level 35 µg/m3 and its 98th percentile form. Taking into consideration the inconsistent results reported in controlled human exposure studies, the intermediate nature of the health effects observed in the controlled human exposure studies that are not typically considered adverse, the health status of the study participants, and how infrequently peak concentrations of potential concern are anticipated to occur in areas meeting the revised primary annual PM2.5 standard, he judges that the current 24-hour standard is requisite to protect against the effects reported in these studies with an adequate margin of safety. Likewise, he judges that neither the epidemiologic studies (including the studies that use restricted analyses) nor the risk assessment provide a sufficient basis for revising the 24-hour standard. As discussed above, the epidemiologic studies, including short-term studies and those with restricted analyses, are not well-suited for identifying a level for a 24-hour standard to address health effects associated with peak concentrations. The restricted analyses support the conclusion that the health effects associated with PM2.5 is not associated primarily with exposure to higher concentrations of the main analyses, but like other epidemiologic studies they typically report only long-term mean 24-hour concentrations ( e.g., restricted epidemiologic studies do not report the number or the percentile of health events or the percentile of PM2.5 concentrations across the highest part of the restricted air quality distribution, including the 98th percentile) and do not identify any particular concentration within the air quality distribution above which effects have been observed and below which effects have not been observed. Similarly, the risk assessment highlights that the annual standard is controlling across much of the U.S. and is generally more effective at reducing risk than the 24-hour standard and, taking into account the limitations and assumptions of the risk assessment discussed above, does not provide a basis for revising the 24-hour standard. For the reasons discussed herein, the Administrator judges that the uncertainties as to whether there would be public health benefits from a more stringent 24-hour standard are too great to justify revising the standard.
Thus, having carefully considered the scientific evidence, quantitative information, CASAC advice, and public comments, the Administrator is retaining the current primary 24-hour PM2.5 standard, with its level of to 35 µg/m3 and its 98th percentile form. In the Administrator's judgment, based on the currently available evidence and information, a 24-hour standard set at this level and using the specified indicator, averaging time, and form would be requisite to protect public health with an adequate margin of safety, in conjunction with the annual standard. As noted, in evaluating the adequacy of the current standards, the Administrator focuses on evaluating the public health protection afforded by the annual and 24-hour standards, taken together, against adverse health effects associated with long- or short-term PM2.5 exposures. A 24-hour standard set at a level of 35 µg/m3 , in conjunction with a revised annual standard level of 9.0 µg/m3 , in the judgment of the Administrator, provides an appropriate level of public health protection, for both long- and short-term PM2.5 exposures. The Administrator believes that a 24-hour standard set at 35 µg/m3 would continue to be sufficient to protect public health with a margin of safety, and believes that a lower standard would be more than what is necessary to provide this degree of protection when considered in conjunction with a revised annual standard. The Administrator concludes the current 24-hour standard at a level of 35 µg/m3 , in conjunction with a revised annual standard level of 9.0 µg/m3 , will provide appropriate protection Start Printed Page 16291 in areas in which the long-term mean concentrations are already relatively low ( i.e., below 9 µg/m3 ) but where there may be elevated short-term peak PM2.5 concentrations, often associated with strong local or seasonal sources. This judgment by the Administrator appropriately considers the degree of protection that is neither more nor less stringent than necessary for this purpose and recognizes that the CAA does not require that primary standards be set at a zero-risk level, but rather at a level that reduces risk sufficiently so as to protect public health with an adequate margin of safety.
In making this decision to retain the current level of the primary PM2.5 24-hour standard at 35 µg/m3 in conjunction with revising the annual standard level from 12.0 µg/m3 to 9.0 µg/m3 , given all of the evidence and information discussed above, the Administrator judges that the revised suite of primary PM2.5 standards and the rationale supporting these levels appropriately reflects consideration of the strength of the available evidence and other information and its associated uncertainties as well as the advice of CASAC and consideration of public comments. He additionally judges that this suite of primary PM2.5 standards is requisite to protect public health, including at-risk populations, with an adequate margin of safety from effects associated with long and short-term exposures to fine particles. This judgment by the Administrator appropriately considers the requirement for standards that are requisite to protect public health but are neither more nor less stringent than necessary.
C. Decisions on the Primary PM2.5 Standards
For the reasons discussed above, and taking into account the information and assessments presented in the 2019 ISA and ISA Supplement, the scientific and quantitative risk information in the 2022 PA, the advice and recommendations of the CASAC, and public comments, the Administrator revises the current suite of primary PM2.5 standards. Specifically, the Administrator revises the level of the primary annual PM2.5 standard to 9.0 µg/m3 while retaining its form, indicator and averaging time. In conjunction with revising the primary annual PM2.5 standard level to provide protection from effects associated with long- and short-term PM2.5 exposures, the Administrator retains the level of 35 µg/m3 and the 98th percentile form, indicator and averaging time of the primary 24-hour PM2.5 standard to continue to provide supplemental protection for areas with high peak PM2.5 concentrations. The Administrator concludes that this suite of standards is requisite to protect public health with an adequate margin of safety against health effects potentially associated with long- and short-term PM2.5 exposures.
III. Rationale for Decisions on the Primary PM 10 Standard
This section presents the rationale for the Administrator's decision to retain the existing primary PM10 standard. This decision is based on a thorough review of the latest scientific information, published through January 2018 [126] and evaluated in the 2019 ISA, on human health effects associated with PM10–2.5 in ambient air. As described in section I above and in section 1.2 of the ISA Supplement, the scope of the updated scientific evaluation of the health effects evidence is based on those PM size fractions, exposure durations, and health effects category combinations where the 2019 ISA concluded a causal relationship exists (U.S. EPA, 2019a, U.S. EPA, 2022b).). Therefore, because the 2019 ISA did not conclude a causal relationship for PM10–2.5 for any exposure durations or health effect categories, the ISA Supplement does not include an evaluation of additional studies for PM10–2.5 . As a result, the 2019 ISA continues to serve as the scientific foundation for assessing the adequacy of the primary PM10 standard in this reconsideration of the 2020 final decision (U.S. EPA, 2019a, section 1.7; U.S. EPA, 2022a). The Administrator's decision also takes into account the 2022 PA evaluation of the policy-relevant information in the 2019 ISA, CASAC advice and recommendations, and public comments.
In presenting the rationale for the Administrator's final decision and its foundations, Section III.A provides background on the 2020 final decision to retain the primary PM10 and a brief summary of key aspects of the currently available health effects information. Section III.B summarizes the CASAC advice and the Administrator's proposed conclusions to retain the existing primary PM10 standard, addresses public comments received on the proposal, and presents the Administrator's conclusions on the adequacy of the current standard, drawing on consideration of information in the 2019 ISA and the 2022 PA, advice from the CASAC, and comments from the public. Section III.C summarizes the Administrator's decision on the primary PM10 standard.
A. Introduction
The general approach for this reconsideration of the 2020 final decision on the primary PM10 standard relies on the scientific information available for this review, as well as the Administrator's judgments regarding the available public health effects evidence, and the appropriate degree of public health protection for the existing standards. With the 2020 decision, the then-Administrator retained the existing primary 24-hour PM10 standard, with its level of 150 µg/m3 and its one-expected-exceedance form on average over three years, to continue to provide public health protection against short-term exposures to PM10–2.5 (85 FR 82725, December 18, 2020).
1. Background on the Current Standard
Consistent with the 2009 ISA, the 2019 ISA concluded that the available epidemiologic, controlled human exposure, and animal toxicological studies, including uncertainties, provided support for the causality determinations of “suggestive of, but not sufficient to infer, a causal relationship” between short-term exposures to PM10–2.5 and cardiovascular effects, respiratory effects, and mortality (U.S. EPA, 2019a, section 1.4.2). The 2019 ISA also reached the conclusion that the evidence supports a “suggestive of, but not sufficient to infer, a causal relationship” between short-term PM10–2.5 exposures and metabolic effects, an endpoint that was not evaluated in the 2009 ISA (U.S. EPA, 2019a, section 1.4.2).
Compared to the 2009 ISA, the 2019 ISA includes expanded evidence for the relationships between long-term exposures and cardiovascular effects, metabolic effects, nervous system effects, cancer, and mortality. The 2019 ISA concluded that the small number of epidemiologic and experimental studies, including uncertainties, contribute to the determination that, “the evidence is suggestive of, but not sufficient to infer, a causal relationship between long-term PM10–2.5 exposure and cardiovascular effects, metabolic effects, nervous system effects, cancer, and mortality and cancer (U.S. EPA, 2019a, p. 10–87). For long-term exposures and cardiovascular effects, Start Printed Page 16292 cardiovascular effects, and cancer, this is an upgrade from the “inadequate to infer the presence or absence of a causal relationship” conclusions in the 2009 ISA (U.S. EPA, 2019a, section 1.4.2). This determination is also the first for long-term exposures and metabolic effects, as the 2009 ISA did not include metabolic effects as an endpoint (U.S. EPA, 2019a section 1.4.2).
In considering the available body of evidence, it was noted in the 2020 review there were considerable uncertainties and limitations associated with the experimental evidence for PM2.5 exposures and health effects, and as such more weight was placed on the available epidemiologic evidence. Therefore, the primary focus in the 2020 review was on multi-city and single-city epidemiologic studies that evaluated associations between short-term PM10–2.5 and mortality, cardiovascular effects (hospital admissions and emergency department visits, as well as blood pressure and hypertension), and respiratory effects. Despite differences in the approaches [127] used to estimate ambient PM10–2.5 concentrations, the majority of the studies reported positive, though often not statistically significant, associations with short-term PM10–2.5 exposures. Most PM10–2.5 effect estimates remained positive in copollutant models that included either gaseous pollutants or other particulate matter size fractions ( e.g., PM2.5). In U.S. study locations likely to have met the PM10 standard during the study period, a few studies reported positive associations between PM10–2.5 and mortality that were statistically significant and remained so in copollutant models (U.S. EPA, 2019a). In addition to the epidemiologic studies, there were a small number of controlled human exposure studies evaluated in the 2019 ISA that reported alterations in heart rate variability or increased pulmonary inflammation following short-term exposure to PM10–2.5, providing some support for the associations in the epidemiologic studies. Animal toxicological studies examined the effect of short-term PM10–2.5 exposures using non-inhalation ( e.g., intratracheal instillation) route.[128] Therefore, these studies provided limited evidence for the biological plausibility of PM10–2.5 -induced effects (U.S. EPA, 2019a). Although the scientific evidence available in the 2019 ISA expanded the understanding of health effects associated with PM10–2.5 exposures, a number of important uncertainties remained. These uncertainties, and their implications for interpreting the scientific evidence, include the following:
• The potential for confounding by copollutants, notably PM2.5, was addressed with copollutant models in a relatively small number of PM10–2.5 epidemiologic studies (U.S. EPA, 2019a). This was particularly important given the relatively small body of experimental evidence ( i.e., controlled human exposure and animal toxicological studies) available to support the independent effect of PM10–2.5 on human health. This increases the uncertainty regarding the extent to which PM10–2.5 itself, rather than one or more copollutants, is responsible for the mortality and morbidity effects reported in epidemiologic studies.
• There was greater spatial variability in PM10–2.5 concentrations than PM2.5 concentrations, resulting in the potential for increased exposure error for PM10–2.5 (U.S. EPA, 2019a). Available measurements did not provide sufficient information to adequately characterize the spatial distribution of PM10–2.5 concentrations (U.S. EPA, 2019a). The limitations in estimates of ambient PM10–2.5 concentrations “would tend to increase uncertainty and make it more difficult to detect effects of PM10–2.5 in epidemiologic studies” (U.S. EPA, 2019a).
• Estimation of PM10–2.5 concentrations over which reported health outcomes occur remain highly uncertain. When compared with PM2.5, there is uncertainty spanning all epidemiologic studies examining associations with PM10–2.5 including deficiencies in the existing monitoring networks, the lack of a systematic evaluation of the various methods used to estimate PM10–2.5 concentrations and the resulting uncertainty in the spatial as well as the temporal variability in PM10–2.5 concentration (U.S. EPA, 2019a).). Given these limitations in routine monitoring, epidemiologic studies employed a number of different approaches for estimating PM10–2.5 concentrations, including (1) calculating the difference between PM10 and PM2.5 at co-located monitors, (2) calculating the difference between county-wide averages of monitored PM10 and PM2.5 based on monitors that are not necessarily co-located, and (3) direct measurement of PM10–2.5 using a dichotomous sampler (U.S. EPA, 2019a, section 1.4.2). Given the relatively small number of PM10–2.5 monitoring sites, the relatively large spatial variability in ambient PM10–2.5 concentrations, the use of different approaches to estimating ambient PM10–2.5 concentrations across epidemiologic studies, and the limitations inherent in such estimates, the distributions of PM10–2.5 concentrations over which reported health outcomes occur remain highly uncertain (U.S. EPA, 2019a).
There was relatively little information available to characterize potential exposure differences that may inform the apparent variability in associations between short-term PM10–2.5 exposures and health effects across study locations (U.S. EPA, 2019a). Specifically, the potential spatial and temporal variability in PM10–2.5 exposures complicates the interpretation of results between study locations as well as the relative lack of information on the chemical and biological composition of PM10–2.5 (U.S. EPA, 2009a U.S. EPA, 2019a).
In reaching his decision in 2020 to retain the existing 24-hour primary PM10 standard, the then-Administrator specifically noted that, while the health effects evidence was somewhat expanded since the prior reviews, the overall conclusions in the 2019 ISA, including uncertainties and limitations, were generally consistent with what was considered in the 2012 review (85 FR 82725, December 18, 2020). In addition, the then-Administrator recognized that there were still a number of uncertainties and limitations associated with the available evidence.
With regard to the evidence on PM10–2.5 -related health effects, the then-Administrator noted that epidemiologic studies continued to report positive associations with mortality and morbidity in cities across North America, Europe, and Asia, where PM10–2.5 sources and composition were expected to vary widely. While significant uncertainties remained in the 2020 review, the then-Administrator recognized that this expanded body of evidence had broadened the range of effects that have been linked with PM10–2.5 exposures. The studies evaluated in the 2019 ISA expanded the scientific foundation presented in the 2009 ISA and led to revised causality determinations (and new determinations) for long-term PM10–2.5Start Printed Page 16293 exposures and mortality, cardiovascular effects, metabolic effects, nervous system effects, and cancer (85 FR 82726, December 18, 2020). Drawing from his consideration of this evidence, the then-Administrator concluded that the scientific information available since the time of the last review supported a decision to maintain a primary PM10 standard to provide public health protection against PM10–2.5 exposures, regardless of location, source of origin, or particle composition (85 FR 82726, December 18, 2020). With regard to uncertainties in the available evidence, the then-Administrator first noted that a number of limitations were identified in the 2012 review related to: (1) Estimates of ambient PM10–2.5 concentrations used in epidemiologic studies; (2) limited evaluation of copollutant models to address the potential for confounding; and (3) limited experimental studies supporting biological plausibility for PM10–2.5 -related effects. Despite the expanded body of evidence for PM10–2.5 exposures and health effects, the then-Administrator recognized that uncertainties in the 2020 review continued to include those associated with the exposure estimates used in epidemiologic studies, the independence of the PM10–2.5 health effect associations, and the biologically plausible pathways for PM10–2.5 health effects (85 FR 82726, December 18, 2020). These uncertainties contributed to the 2019 ISA determinations that the evidence is at most “suggestive of, but not sufficient to infer” causal relationships (85 FR 82726, December 18, 2020). In considering the available evidence in his basis for the decision, the then-Administrator emphasized evidence supporting “causal” and “likely to be causal” relationships, and therefore, judged that the PM10–2.5 -related health effects evidence provided an uncertain scientific foundation for making standard-setting decisions. He further judged limitations in the evidence raised questions as to whether additional public health improvements would be achieved by revising the existing PM10 standard (85 FR 24126, April 30, 2020). In the 2020 decision, for all of the reasons discussed above and recognizing the CASAC conclusion that the evidence provided support for retaining the current standard, the then-Administrator concluded that it was appropriate to retain the existing primary PM10 standard, without revision. His decision was consistent with the CASAC advice related to the primary PM10 standard. Specifically, the CASAC agreed with the 2020 PA conclusions that, while these effects are important, the “evidence does not call into question the adequacy of the public health protection afforded by the current primary PM10 standard” and “supports consideration of retaining the current standard in this review” (Cox, 2019b, p. 3 of consensus letter). Thus, the then-Administrator concluded that the primary PM10 standard (in all of its elements ( i.e., indicator, averaging time, form, and level)) was requisite to protect public health with an adequate margin of safety against effects that have been associated with PM10–2.5 . In light of this conclusion, the EPA retained the existing PM10 standard.
2. Overview of the Health Effects Evidence
The information summarized here is based on the scientific assessment of the health effects evidence available in this reconsideration; this evaluation is documented in the 2019 ISA and its policy implications are discussed further in the 2022 PA. As noted above, the ISA Supplement does not include an evaluation of studies for PM10–2.5, and the 2019 ISA continues to serve as the scientific foundation for this reconsideration.
a. Nature of Effects
For the health effect categories and exposure duration combinations evaluated, the 2019 ISA concludes that the evidence supports causality determinations for PM10–2.5 that are at most “suggestive of, but not sufficient to infer, a causal relationship”. While the evidence supporting the causal nature of relationships between exposure to PM10–2.5 has been strengthened for some health effect categories since the completion of the 2009 ISA, the 2019 ISA concludes that overall “the uncertainties in the evidence identified in the 2009 ISA have, to date, still not been addressed” (U.S. EPA, 2019a, section 1.4.2, p. 1–41; U.S. EPA, 2022b, section 4.3.1). Specifically, epidemiologic studies available in the 2012 review relied on various methods to estimate PM10–2.5 concentrations, and these methods had not been systematically compared to evaluate spatial and temporal correlations in PM10–2.5 concentrations. Methods included: (1) Calculating the difference between PM10 and PM2.5 concentrations at co-located monitors, (2) calculating the difference between county-wide averages of monitored PM10 - and PM2.5 -based on monitors that are not necessarily co-located, and (3) direct measurement of PM10–2.5 using a dichotomous sampler (U.S. EPA, 2019a, section 1.4.2). As described in the 2019 ISA, there continues to be variability across epidemiologic studies in the approaches used to estimate PM10–2.5 concentrations. Additionally, some studies estimate long-term PM10–2.5 exposures as the difference between PM10 and PM2.5 concentrations based on information from spatiotemporal or land use regression (LUR) models, in addition to monitors. The various methods used to estimate PM10–2.5 concentrations have not been systematically evaluated (U.S. EPA, 2019a, section 3.3.1.1), contributing to uncertainty regarding the spatial and temporal correlations in PM10–2.5 concentrations across methods and in the PM10–2.5 exposure estimates used in epidemiologic studies (U.S. EPA, 2019a, section 2.5.1.2.3). Given the greater spatial and temporal variability of PM10–2.5 and the lower number of PM10–2.5 monitoring sites, compared to PM2.5, this uncertainty is particularly important for the coarse size fraction. Beyond the uncertainty associated with PM10–2.5 exposure estimates in epidemiologic studies, the limited information on the potential for confounding by copollutants and the limited support available for the biological plausibility of health effects following PM10–2.5 exposures also continue to contribute to uncertainty in the PM10–2.5 health evidence. Uncertainty related to potential confounding stems from the relatively small number of epidemiologic studies that have evaluated PM10–2.5 health effect associations in copollutants models with both gaseous pollutants and other PM size fractions. On the other hand, uncertainty related to the biological plausibility of effects attributed to PM10–2.5 exposures results from the small number of controlled human exposure and animal toxicological studies that have evaluated the health effects of experimental PM10–2.5 inhalation exposures. The evidence supporting the 2019 ISA's “suggestive of, but not sufficient to infer, a causal relationship” causality determinations for PM10–2.5, including uncertainties in this evidence, is summarized below in sections III.B.1.a through III.B.1.f.
i. Mortality
Due to the dearth of studies examining the association between long-term PM10–2.5 exposure and mortality, the 2009 ISA concluded that the evidence was “inadequate to determine if a causal relationship exists” (U.S. EPA, 2009a). As reported in the 2019 ISA, some cohort studies conducted in the U.S. and Europe report positive associations between long-term PM10–2.5 exposure and total (nonaccidental) Start Printed Page 16294 mortality, though results are inconsistent across studies (U.S. EPA, 2019a, Table 11–11). The examination of copollutant models in these studies remains limited and, when included, PM10–2.5 effect estimates are often attenuated after adjusting for PM2.5 (U.S. EPA, 2019a, Table 11–11). Across studies, PM10–2.5 exposure concentrations are estimated using a variety of approaches, including direct measurements from dichotomous samplers, calculating the difference between PM10 and PM2.5 concentrations measured at collocated monitors, and calculating difference of area-wide concentrations of PM10 and PM2.5 . As discussed above, temporal and spatial correlations between these approaches have not been evaluated, contributing to uncertainty regarding the potential for exposure measurement error (U.S. EPA, 2019a, section 3.3.1.1 and Table 11–11). The 2019 ISA concludes that this uncertainty “reduces the confidence in the associations observed across studies” (U.S. EPA, 2019a, p. 11–125). The 2019 ISA additionally concludes that the evidence for long-term PM10–2.5 exposures and cardiovascular effects, respiratory morbidity, and metabolic disease provide limited biological plausibility for PM10–2.5 -related mortality (U.S. EPA, 2019a, sections 11.4.1 and 11.4). Taken together, the 2019 ISA concludes that, “this body of evidence is suggestive, but not sufficient to infer, that a causal relationship exists between long-term PM10–2.5 exposure and total mortality” (U.S. EPA, 2019a, p. 11–125).
With regard to short-term PM10–2.5 exposures and mortality, the 2009 ISA concluded that the evidence is “suggestive of a causal relationship between short-term exposure to PM10–2.5 and mortality” (U.S. EPA, 2009a). The 2019 ISA included multicity epidemiologic studies conducted primarily in Europe and Asia that continue to provide consistent evidence of positive associations between short-term PM10–2.5 exposure and total (nonaccidental) mortality (U.S. EPA, 2019a, Table 11–9). Although these studies contribute to increasing confidence in the PM10–2.5 -mortality relationship, the use of various approaches to estimate PM10–2.5 exposures continues to contribute uncertainty to the associations observed. Recent studies expand the assessment of potential copollutant confounding of the PM10–2.5 -mortality relationship and provide evidence that PM10–2.5 associations generally remain positive in copollutant models, though associations are attenuated in some instances (U.S. EPA, 2019a, section 11.3.4.1, Figure 11–28, Table 11–10). The 2019 ISA concludes that, overall, the assessment of potential copollutant confounding is limited due to the lack of information on the correlation between PM10–2.5 and gaseous pollutants and the small number of locations in which copollutant analyses have been conducted. Associations with cause-specific mortality ( i.e., cardiovascular and respiratory mortality) provide some support for associations with total (nonaccidental) mortality, though associations with respiratory mortality are more uncertain ( i.e., wider confidence intervals) and less consistent (U.S. EPA, 2019a, section 11.3.7). The 2019 ISA concludes that the evidence for PM10–2.5 -related cardiovascular effects provides only limited support for the biological plausibility of a relationship between short-term PM10–2.5 exposure and cardiovascular mortality (U.S. EPA, 2019a, section 11.3.7). Based on the overall evidence, the 2019 ISA concludes that, “this body of evidence is suggestive, but not sufficient to infer, that a causal relationship exists between short-term PM10–2.5 exposure and total mortality” (U.S. EPA, 2019a, p. 11–120).
ii. Cardiovascular Effects
In the 2009 ISA, the evidence describing the relationship between long-term exposure to PM10–2.5 and cardiovascular effects was characterized as “inadequate to infer the presence or absence of a causal relationship.” The limited number of epidemiologic studies reported contradictory results and experimental evidence demonstrating an effect of PM10–2.5 on the cardiovascular system was lacking (U.S. EPA, 2019a, section 6.4).
The evidence relating long-term PM10–2.5 exposures to cardiovascular mortality remains limited, with no consistent pattern of associations across studies and, as discussed above, uncertainty stemming from the use of various approaches to estimate PM10–2.5 concentrations (U.S. EPA, 2019a, Table 6–70). The evidence for associations with cardiovascular morbidity has grown and, while results across studies are not entirely consistent, some epidemiologic studies report positive associations with ischemic heart disease (IHD) and MI (U.S. EPA, 2019a, Figure 6–34); stroke (U.S. EPA, 2019a, Figure 6–35); atherosclerosis (U.S. EPA, 2019a, section 6.4.5); venous thromboembolism (VTE) (U.S. EPA, 2019a, section 6.4.7); and blood pressure and hypertension (U.S. EPA, 2019a, Section 6.4.6). PM10–2.5 cardiovascular mortality effect estimates are often attenuated, but remain positive, in copollutants models that adjust for PM2.5 . For morbidity outcomes, associations are inconsistent in copollutant models that adjust for PM2.5, NO2, and chronic noise pollution (U.S. EPA, 2019a, p. 6–276). The lack of toxicological evidence for long-term PM10–2.5 exposures represents a data gap (U.S. EPA, 2019a, section 6.4.10), resulting in the 2019 ISA conclusion that “evidence from experimental animal studies is of insufficient quantity to establish biological plausibility” (U.S. EPA, 2019a, p. 6–277). Based largely on the observation of positive associations in some epidemiologic studies, the 2019 ISA concludes that “evidence is suggestive of, but not sufficient to infer, a causal relationship between long-term PM10–2.5 exposure and cardiovascular effects” (U.S. EPA, 2019a, p. 6–277).
With regard to short-term PM10–2.5 exposures and cardiovascular effects, the 2009 ISA found that the available evidence for short-term PM10–2.5 exposure and cardiovascular effects was “suggestive of a causal relationship.” This conclusion was based on several epidemiologic studies reporting associations between short-term PM10–2.5 exposure and cardiovascular effects, including IHD hospitalizations, supraventricular ectopy, and changes in heart rate variability (HRV). In addition, dust storm events resulting in high concentrations of crustal material were linked to increases in total cardiovascular disease emergency department visits and hospital admissions. However, the 2009 ISA noted the potential for exposure measurement error primarily due to the different methods used across studies to estimate PM10–2.5 concentrations and copollutant confounding in these epidemiologic studies. In addition, there was only limited evidence of cardiovascular effects from a small number of experimental studies ( e.g. animal toxicological studies and controlled human exposure studies) that examined short-term PM10–2.5 exposures (U.S. EPA, 2009a, section 6.2.12.2). In the 2019 ISA, key uncertainties included the potential for exposure measurement error, copollutant confounding, and limited evidence of biological plausibility for cardiovascular effects following inhalation exposure (U.S. EPA, 2019a, section 6.3.13).
The evidence for short-term PM10–2.5 exposure and cardiovascular outcomes has expanded since the 2009 ISA, though important uncertainties remain. The 2019 ISA notes that there are a small number of epidemiologic studies reporting positive associations between short-term exposure to PM10–2.5 and cardiovascular-related morbidity Start Printed Page 16295 outcomes. However, the 2019 ISA notes that there is limited evidence to support that these associations are biologically plausible, or independent of copollutant confounding. The 2019 ISA also concludes that it remains unclear how the approaches used to estimate PM10–2.5 concentrations in epidemiologic studies compare amongst one another and subsequently how exposure measurement error varies between each method. Specifically, it is unclear how well-correlated PM10–2.5 concentrations are both temporally and spatially across these methods and therefore whether exposure measurement error varies across these methods. Taken together, the 2019 ISA concludes that “the evidence is suggestive of, but not sufficient to infer, a causal relationship between short-term PM10–2.5 exposures and cardiovascular effects” (U.S. EPA, 2019a, p. 6–254).
iii. Respiratory Effects
With regard to short-term PM10–2.5 exposures and respiratory effects, the 2009 ISA (U.S. EPA, 2009a) concluded that the relationship between short-term exposure to PM10–2.5 and respiratory effects is “suggestive of a causal relationship” based on a small number of epidemiologic studies observing associations with some respiratory effects and limited evidence from experimental studies to support biological plausibility. Epidemiologic findings were consistent for respiratory infection and combined respiratory-related diseases, but not for COPD. Studies were characterized by overall uncertainty in the exposure assignment approach and limited information regarding potential copollutant confounding. Controlled human exposure studies of short-term PM10–2.5 exposures found no lung function decrements and inconsistent evidence for pulmonary inflammation. Animal toxicological studies were limited to those using non-inhalation ( e.g., intra-tracheal instillation) routes of PM10–2.5 exposure.
Recent epidemiologic findings consistently link PM10–2.5 exposure to asthma exacerbation and respiratory mortality, with some evidence that associations remain positive (though attenuated in some studies of mortality) in copollutant models that include PM2.5 or gaseous pollutants. Epidemiologic studies provide limited evidence for positive associations with other respiratory outcomes, including COPD exacerbation, respiratory infection, and combined respiratory-related diseases (U.S. EPA, 2019a, Table 5–36). As noted above for other endpoints, an uncertainty in these epidemiologic studies is the lack of a systematic evaluation of the various methods used to estimate PM10–2.5 concentrations and the resulting uncertainty in the spatial and temporal variability in PM10–2.5 concentrations compared to PM2.5 (U.S. EPA, 2019a, sections 2.5.1.2.3 and 3.3.1.1). Specifically, the existing monitoring networks do not provide a good characterization of how well correlated concentrations are both spatially and temporally across the PM10–2.5 estimation methods and overall spatial and temporal patterns in PM10–2.5 concentrations. Taken together, the 2019 ISA concludes that “the collective evidence is suggestive of, but not sufficient to infer, a causal relationship between short-term PM10–2.5 exposure and respiratory effects” (U.S. EPA, 2019a, p. 5–270).
iv. Cancer
In the 2012 review, little information was available from studies of cancer following inhalation exposures to PM10–2.5 . Thus, the 2009 ISA determined the evidence was “inadequate to evaluate the relationship between long-term PM10–2.5 exposures and cancer” (U.S. EPA, 2009a). The scientific information evaluated in the 2019 ISA of long-term PM10–2.5 exposure and cancer remains limited, with a few recent epidemiologic studies reporting positive, but imprecise, associations with lung cancer incidence (U.S. EPA, 2019a). Moreover, uncertainty remains in these studies with respect to exposure measurement error due to the use of PM10–2.5 predictions that have not been validated by monitored PM10–2.5 concentrations (U.S. EPA, 2019a, sections 3.3.2.3 and 10.3.4). Relatively few experimental studies of PM10–2.5 have been conducted, though available studies indicate that PM10–2.5 exhibits two key characteristics of carcinogens: genotoxicity and oxidative stress. While limited, such experimental studies provide some evidence of biological plausibility for the findings in a small number of epidemiologic studies (U.S. EPA, 2019a, section 10.3.4).
Taken together, the small number of epidemiologic and experimental studies, along with uncertainty with respect to exposure measurement error, contribute to the determination in the 2019 ISA that, “the evidence is suggestive of, but not sufficient to infer, a causal relationship between long-term PM10–2.5 exposure and cancer” (U.S. EPA, 2019a, p. 10–87).
v. Metabolic Effects
The 2009 ISA did not make a causality determination for PM10–2.5 -related metabolic effects. One epidemiologic study in the 2019 ISA reports an association between long-term PM10–2.5 exposure and incident diabetes, while additional cross-sectional studies report associations with effects on glucose or insulin homeostasis (U.S. EPA, 2019a, section 7.4). As discussed above for other outcomes, uncertainties with the epidemiologic evidence include the potential for copollutant confounding and exposure measurement error due to the different methods used across studies to estimate PM10–2.5 concentrations (U.S. EPA, 2019a, Tables 7–14 and 7–15). The evidence base to support the biological plausibility of metabolic effects following PM10–2.5 exposures is limited, but a cross-sectional study that investigated biomarkers of insulin resistance and systemic and peripheral inflammation may support a pathway leading to type 2 diabetes (U.S. EPA, 2019a, sections 7.4.1 and 7.4.3). Based on the expanded, though still limited evidence base, the 2019 ISA concludes that, “[o]verall, the evidence is suggestive of, but not sufficient to infer, a causal relationship between [long]-term PM10–2.5 exposure and metabolic effects” (U.S. EPA, 2019a, p. 7–56).
vi. Nervous System Effects
The 2009 ISA did not make a causality determination for PM10–2.5 -related nervous system effects. In the 2019 ISA, available epidemiologic studies report associations between PM10–2.5 and impaired cognition and anxiety in adults in longitudinal analyses (U.S. EPA, 2019a, Table 8–25, section 8.4.5). Associations of long-term exposure with neurodevelopmental effects are not consistently reported in children (U.S. EPA, 2019a, sections 8.4.4 and 8.4.5). Uncertainties in these studies include the potential for copollutant confounding, as no studies examined copollutants models (U.S. EPA, 2019a, section 8.4.5), and for exposure measurement error, given the use of various methods to estimate PM10–2.5 concentrations (U.S. EPA, 2019a, Table 8–25). In addition, there is limited animal toxicological evidence supporting the biological plausibility of nervous system effects (U.S. EPA, 2019a, sections 8.4.1 and 8.4.5). Overall, the 2019 ISA concludes that, “the evidence is suggestive of, but not sufficient to infer, a causal relationship” between long-term PM10–2.5 exposure and nervous system effects (U.S. EPA, 2019a, p. 8–75). Start Printed Page 16296
B. Conclusions on the Primary PM10 Standard
In drawing conclusions on the adequacy of the current primary PM10 standard, in view of the advances in scientific knowledge and additional information now available, the Administrator has considered the evidence base, information, and policy judgments that were the foundation of the 2020 review and reflects upon the body of information and evidence available in this reconsideration. In so doing, the Administrator has taken into account both evidence-based and quantitative information-based considerations, as well as advice from the CASAC and public comments. Evidence-based considerations draw upon the EPA's integrated synthesis of the scientific evidence from animal toxicologic, controlled human exposure, and epidemiologic studies evaluating health effects related to exposures to PM10–2.5 as presented in the 2019 ISA and discussed in section III.A.2. In addition to the evidence, the Administrator has weighed a range of policy-relevant considerations as discussed in the 2022 PA and summarized in sections III.B and III.C of the proposal and summarized in section III.B.2 below. These considerations, along with the advice from the CASAC (section III.B.1) and public comments (section III.B.3), are discussed below. A more detailed summary of all significant comments, along with the EPA's responses in the Response to Comments document, can be found in the docket for this rulemaking (Docket No. EPA–HQ–OAR–2015–00072). This document is available for review in the docket for this rulemaking and through EPA's NAAQS website (link). The Administrator's conclusions in this reconsideration regarding the adequacy of the current primary PM10 standard and whether any revisions are appropriate are described in section III.B.4.
1. CASAC Advice
As described in section I.X, the EPA decided to prepare a revised PA for the reconsideration of the 2020 final decision. The CASAC's advice on the 2019 draft PA and the 2021 draft PA was documented in letters to the prior and current Administrators (Cox, 2019b; Sheppard, 2022a) and is summarized below. In reviewing both the 2019 draft PA and the 2021 draft PA, the CASAC agreed with the EPA's preliminary conclusion that the available scientific evidence, including its uncertainties and limitations, does not call into question the adequacy of the current primary PM10 standard and that the standard should be retained, without revision.
In its review of the 2019 draft PA, the CASAC concurred with the overall preliminary conclusion that it is appropriate to consider retaining the current primary PM10 standard, without revision. In their agreement with the conclusions in the 2019 draft PA, the CASAC stated that “that key uncertainties identified in the last review remain” (Cox, 2019b) and that “none of the identified health outcomes linked to PM10–2.5 ” were judged to be causal or likely to be causal (Cox, 2019b, p. 12 of consensus responses). Moreover, to reduce these uncertainties in future reviews, the CASAC recommended improvements to PM10–2.5 exposure assessment, including a more extensive network for direct monitoring of the PM10–2.5 fraction (Cox, 2019b, p. 13 of consensus responses). The CASAC also recommended additional controlled human exposure and animal toxicological studies of the PM10–2.5 fraction to improve the understanding of biological mechanisms and pathways (Cox, 2019b, p. 13 of consensus responses). Overall, the CASAC agreed with the EPA's preliminary conclusion in the 2019 draft PA that “. . . the available evidence does not call into question the adequacy of the public health protection afforded by the current primary PM10 standard and that evidence supports consideration of retaining the current standard in this review” (Cox, 2019b, p. 3 of letter).
In its review of the 2021 draft PA, the CASAC provided advice on the adequacy of the current primary PM10 standard in the context of its review of the revised PA for this reconsideration (Sheppard, 2022a) [129] .) [130] . In this context, the CASAC supported the preliminary conclusion in the 2021 draft PA that the evidence reviewed in the 2019 ISA does not call into question the public health protection provided by the current primary PM10 standard against PM10–2.5 exposures and concurs with the 2021 draft PA's overall preliminary conclusion that it is appropriate to consider retaining the current primary PM10 standard (Sheppard, 2022a, p. 4 of consensus letter). Additionally, the CASAC concurred that “. . . at this time, PM10 is an appropriate choice as the indicator for PM10–2.5 ” and “that it is important to retain the level of protection afforded by the current PM10 standard” (Sheppard, 2022a, p. 4 of consensus letter). The CASAC also recognized uncertainties associated with the scientific evidence, including “compared to PM2.5 studies, the more limited number of epidemiology studies with positive statistically significant findings, and the difficulty in extracting the sole contribution of coarse PM to observed adverse health effects” (Sheppard, 2022a, p. 19 of consensus responses).
The CASAC recommended several areas for additional research to reduce uncertainties in the PM10–2.5 exposure estimates used in the epidemiologic studies, to evaluate the independence of PM10–2.5 health effect associations, to evaluate the biological plausibility of PM10–2.5 -related effects, and to increase the number of studies examining PM10–2.5 -related health effects in at-risk populations (Sheppard, 2022a, p. 20 of consensus responses). Furthermore, the CASAC “recognizes a need for, and supports investment in research and deployment of measurement systems to better characterize PM10–2.5 ” and to “provide information that can improve public health” (Sheppard, 2022a, p. 20 of consensus responses).
2. Basis for the Proposed Decision
At the time of the proposal, the Administrator carefully considered the assessment of the current evidence and conclusions reached in the 2019 ISA, considerations and staff conclusions and associated rationales presented in the 2020 PA and 2022 PA, and advice and recommendations of the CASAC (88 FR 5634, January 27, 2023). Consistent with previous reviews, the Administrator first considered the available scientific evidence for PM10–2.5 -related exposures and health effects, as evaluated in the 2019 ISA. As an initial matter, the Administrator recognized that the scientific evidence for PM10–2.5 -related effects available in this reconsideration is the same body of evidence that was available at the time of the 2020 review, as evaluated in the 2019 ISA and summarized in section III.A.2 above. The 2019 ISA concludes that the evidence supports “suggestive of, but not sufficient to infer” causal relationships between short- and long-term exposures to PM10–2.5 and cardiovascular effects, cancer, and mortality and long-term PM10–2.5 exposures and metabolic effects and nervous system effects (U.S. EPA, 2019a). The Administrator noted that Start Printed Page 16297 the evidence for several PM10–2.5 -related health effects has expanded since the completion of the 2009 ISA, but important uncertainties remain. The uncertainties in the epidemiologic studies contribute to the determinations in the 2019 ISA that the evidence for short and long-term PM10–2.5 exposures and mortality, cardiovascular effects, metabolic effects, nervous system effects, and cancer is “suggestive of, but not sufficient to infer” causal relationships (U.S. EPA, 2019a; U.S. EPA, 2022b, section 4.3.1). Drawing from the evidence evaluated in the 2019 ISA and consideration of the scientific evidence in the 2022 PA, the Administrator noted that, consistent with previous reviews, the 2019 ISA and the 2022 PA highlight a number of uncertainties associated with the evidence, including: (1) PM10–2.5 exposure estimates used in epidemiologic studies, (2) independence of PM10–2.5 health effect associations, and (3) biological plausibility of the PM10–2.5 -related effects. These uncertainties contribute to the determinations in the 2019 ISA that the evidence for short-term PM10–2.5 exposures and key health effects is “suggestive of, but not sufficient to infer” causal relationships. In considering the available scientific evidence, consistent with approaches employed in past NAAQS reviews, the Administrator placed the most weight on evidence supporting “causal” and “likely to be causal” relationships. In so doing, he noted that the available evidence for short- and long-term PM10–2.5 exposures and health effects does not support causality determinations of a “causal relationship” or “likely to be causal relationship.” Furthermore, the Administrator recognized that, because of the uncertainties and limitations in the evidence base, the 2022 PA does not include a quantitative assessment of PM10–2.5 exposures and risk that might further inform decisions regarding the adequacy of the current 24-hour primary PM10 standard. Therefore, in light of the 2019 ISA conclusions that the evidence supports “suggestive of, but not sufficient to infer” causal relationships. The Administrator judged that there are substantial uncertainties that raise questions regarding the degree to which additional public health improvements would be achieved by revising the existing PM10 standard. In considering the available evidence for long-term PM10–2.5 exposures, the Administrator noted that there is limited evidence that would support consideration of an annual standard to provide protection against such effects, in conjunction with the current primary 24-hour PM10 standard. He preliminarily concluded that the current primary 24-hour PM2.5 standard that reduces 24-hour exposures also likely reduces long-term average exposures, and therefore provides some margin of safety against the health effects associated with long-term PM10–2.5 exposures.
In reaching his proposed decision on the adequacy of the current primary 24-hour PM10 standard, the Administrator also considered advice from the CASAC. As noted above in section III.B.1, the CASAC recognized uncertainties associated with the scientific evidence and agreed with the 2019 draft PA and 2021 draft PA conclusions that the scientific evidence does not call into question the adequacy of the primary PM10 standard and supports consideration of retaining the current standard.
When considering the above information together, the Administrator proposed to conclude that the available scientific evidence continues to support a PM10 standard to provide some measure of protection against PM10–2.5 exposures. Additionally, he recognized that there are important uncertainties and limitations associated with the available evidence for PM10–2.5 -related health effects, for both short and long-term exposure, as evaluated in the 2019 ISA. Consistent with the decisions in the previous reviews, the Administrator proposed to conclude that these limitations lead to considerable uncertainty regarding the potential public health implications of revising the level of the current primary 24-hour PM10 standard. Thus, based on his consideration of the evidence and associated uncertainties and limitations for PM10–2.5 -related health effects and his consideration of CASAC advice on the primary PM10 standard, the Administrator proposed to retain the current primary PM10 standard, without revision.
3. Comments on the Proposed Decision
Of the public comments received on the proposal, very few commenters provided comments on the primary PM10 standard. Of those commenters who did provide comments on the primary PM10 standard, the majority agree with the EPA's proposed decision to retain the primary PM10 standard. In so doing, these commenters agree with the EPA's rationale regarding the available scientific information, including uncertainties and limitations, for informing decisions on the standard. These commenters state that no new scientific evidence or quantitative information has emerged since the 2020 decision to retain the current standard. Furthermore, these commenters note that the EPA did not evaluate any new scientific evidence related to PM10–2.5 exposures and health effects as a part of the 2022 ISA Supplement developed for this reconsideration, nor did the revised 2022 PA consider any new or different information from the 2020 PA, and therefore, the EPA reached the same conclusion as is the 2020 PA that the current standard is adequate and should be retained. This group includes industries and industry groups, as well as some State and local governments. All of these commenters generally note their agreements with the rationale provided in the proposal and the CASAC concurrence with the 2021 draft PA conclusion that the available information does not call into question the adequacy of the current standard, and therefore, does not support revision and that the current standard should be retained.
Some commenters, including those from environmental and public health organizations and groups, some states, and individuals, disagreed with the Administrator's proposed decision to retain the current primary PM10 standard. These commenters recommend that the EPA revise the primary PM10 standard to a lower level to provide increased public health protection, citing to the available scientific evidence, as well as the proposed revision to the primary PM2.5 standard.
Commenters who disagreed with the proposal to retain the current standard state that revision to the primary PM10 standard is necessary to protect public health with an adequate margin of safety. In their recommendations for revising the standard, some commenters contend that the current standard, with its indicator of PM10 to target exposures to PM10–2.5, has become less protective as ambient concentrations of PM2.5 have been reduced with revisions to that standard. These commenters assert that the current primary PM10 standard allows increased exposure to PM10–2.5 in ambient air because retaining the primary PM10 would allow proportionately more PM10–2.5 mass as the PM2.5 standard has been revised downward. Moreover, in support of their recommendations, the commenters note that the available evidence of PM10–2.5 -related health effects has been expanded and strengthened since the time of the last review. Taken together, the commenters contend that the primary PM10 standard should be revised and failure to do so would be arbitrary and capricious. Some of these Start Printed Page 16298 commenters assert that the level of the primary PM10 standard should be revised to 140 or 145 µg/m3 , concurrent with a strengthened primary 24-hour PM2.5 standard, while other commenters recommend revising the level of the standard to within the range of 65–75 µg/m3 , to provide increased public health protection.
We disagree with the commenters that the primary PM10 standard should be revised because of reductions in ambient concentrations of PM2.5 . As an initial matter, we note that overall, ambient concentrations of both PM10 and PM2.5 have declined significantly over time. Ambient concentrations of PM10 have declined by 46% across the U.S. from 2000 to 2019,[131] while PM2.5 concentrations in ambient air have declined by 43% during this same time period.[132] As noted in the 2022 PA (p. 2–41), the majority of PM10–2.5 sites have generally remained steady and do not exhibit a trend of increasing or decreasing concentrations during this time period, reflecting the relatively consistent level of dust emission across the U.S. from 2000 to 2019 (U.S. EPA, 2022b).
The 2019 ISA provides a comparison of the relative contribution of PM2.5 and PM10–2.5 to PM10 concentrations by region and season using the more comprehensive monitoring data from the NCore network available in this reconsideration (U.S. EPA, 2019, section 2.5.1.1.4). The data indicate that, for urban areas, there are roughly equivalent amounts of PM2.5 and PM10–2.5 contributing to PM10 in ambient air, while rural locations have a slightly higher contribution of PM10–2.5 contributing to PM10 concentrations than PM2.5 (U.S. EPA, 2019, section 2.5.1.1.4, Table 2–7). There is generally a greater contribution from the PM2.5 fraction in the East and a greater contribution from the PM10–2.5 fraction in the West and Midwest.
The EPA recognizes that when the primary annual PM2.5 standard was revised from 15.0 µg/m3 to 12.0 µg/m3 while leaving the 24-hour PM2.5 standards unchanged at 35 µg/m3 and the 24-hour PM10 standard unchanged at 150 µg/m3 , the PM10–2.5 fraction of PM10 could increase in some areas as the PM2.5 fraction decreases (78 FR 3085, March 03, 2013). As described in the 2019 ISA, PM10 has become considerably coarser across the U.S. compared to similar observations in the 2009 ISA such that, in urban areas, the mass of the coarse fraction of PM is similar to or greater than the mass of the fine fraction of PM (U.S. EPA, 2019, section 2.5.1.1.4; U.S. EPA, 2009c). However, in considering recent air quality data, the EPA notes that in most areas of the country PM2.5 and PM10 concentrations have declined and are well below their respective 24-hour standards. While the contribution of fine and coarse PM to PM10 mass concentrations may vary spatially and temporally, based on the trends in recent air quality data, the Administrator concludes that the current primary 24-hour PM10 standard is maintaining air quality at level that provides requisite protection against PM10–2.5 . That is, recent air quality data does not suggest that PM10–2.5 concentrations have been increasing as PM2.5 concentrations have been decreasing. In considering the available PM10–2.5 health effects evidence in this reconsideration, there continue to be significant uncertainties and limitations, specifically with respect to the exposure assessment methods used to estimate PM10–2.5 concentrations, that make it difficult to fully assess the public health implications of revising the primary PM10 standard even considering the possibility for additional variability in the relative ratio of PM2.5 to PM10–2.5 in current PM10 air quality across the U.S. As described in detail above in section III.A.2 and in the proposal (85 FR 5558, January 27, 2023), the uncertainties and limitations in the health effects evidence for PM10–2.5 contributed to the determinations in the 2019 ISA that the evidence for key PM10–2.5 health effects is “suggestive of, but not sufficient to infer, a causal relationship” or “inadequate to infer the presence, or absence of a causal relationship” (U.S. EPA, 2019a). While the evidence base for PM10–2.5 -related health effects has somewhat expanded since the 2009 ISA, the Administrator concludes that the evidence remains too limited to inform judgments regarding whether a more protective primary PM10 standard is warranted at this time.
Beyond the uncertainties and limitations associated with the available scientific evidence, the EPA also notes that, while the NCore monitoring network has been expanded since the time of the last review, epidemiologic studies available in this review do not use PM10–2.5 NCore data in evaluating associations between PM10–2.5 in ambient air and long- or short-term exposures. In the absence of such evidence, the public health implications of changes in ambient PM10–2.5 concentrations as PM2.5 concentrations decrease remain unclear. Therefore, the EPA continues to recognize this as an area for future research, to address the existing uncertainties (U.S. EPA, 2022b, section 4.6), and inform future reviews of the PM NAAQS. Taken together, as at the time of proposal, the Administrator concludes that these and other limitations in the PM10–2.5 evidence raised questions as to whether additional public health improvements would be achieved by revising the existing PM10 standard, particularly when considering such judgments along with his decision to retain the current primary 24-hour PM2.5 standard. Therefore, the EPA does not agree with the commenters that the currently available air quality information or scientific evidence support revisions to the primary PM10 standard in this reconsideration.
Consistent with their comments on the 2020 proposal, some commenters disagreed with the Administrator's proposed conclusion to retain the current primary PM10 standard, primarily focusing their comments on the need for revisions to the form of the standard or the level of the standard. With regard to comments on the form of the standard, some commenters assert that the EPA should revise the standard by adopting a separate form (or a “compliance threshold” in their words)—the 99th percentile, averaged over three years—for the primary PM10 standard for continuous monitors, which provide data every day, while maintaining the current form of the standard (one exceedance, averaged over three years) for 1-in-6 samplers, given the increased use of continuous monitoring and to ease the burden of demonstrating exceptional events. These commenters, in support of their comment, contend that the 99th percentile would effectively change the form from the 2nd highest to the 4th highest and would allow no more than three exceedances per year, averaged over three years. These commenters additionally highlight the EPA's decision in the 1997 review to adopt a 99th percentile form, averaged over three years, citing to advantages of a percentile-based form in the Administrator's rationale in that review. The comments further assert that a 99th percentile form for the primary PM10 standard is still more conservative than the form for other short-term NAAQS ( e.g., PM2.5 and NO2). Start Printed Page 16299
First, the EPA has long recognized that the form is an integral part of the NAAQS and must be selected together with the other elements ( i.e., indicator, averaging time, level) of the NAAQS to ensure the appropriate stringency and requisite degree of public health protection. Thus, if the EPA were to change the form according to the monitoring method it would be establishing two different NAAQS, varying based on the monitoring method. The EPA has not done this to date, did not propose such an approach, and declines to adopt it for the final rule, as we believe such a decision in this final rule is beyond the scope of the proposal, and that each PM standard should have a single form, indicator, level and averaging time, chosen by the Administrator as necessary and appropriate. While certain continuous monitors may be established and approved as a Federal Equivalent Method (FEM) for PM10, as an alternative to a Federal Reference Method (FRM), the use of an FEM is intended as an alternative means of determining compliance with the NAAQS, not as authorizing a different NAAQS.
Even if the commenters had asked that the change in form be made without regard to monitoring method, the EPA does not believe such a change would be warranted. The change in form for continuous monitors suggested by the commenters, without also lowering the level of such a standard, would allow more exceedances and thereby reduce the public health protection provided against exposures to PM10–2.5 in ambient air, resulting in a less stringent primary PM10 standard than the current standard. These commenters have not provided new evidence or analyses to support their conclusion that an appropriate degree of public health protection could be achieved by allowing the use of an alternative form ( i.e., 99th percentile), while retaining the other elements of the standard.
With regard to the commenters' assertion that an alternate form of the standard would ease the burden of demonstrating exceptional events, the EPA recognizes, consistent with the CAA, that it may be appropriate to exclude monitoring data influenced by “exceptional” events when making certain regulatory determinations. However, the EPA notes that the cost of implementation of the standards may not be considered by the EPA in reviewing the standards. The EPA continues to update and develop documentation and tools to facilitate the implementation of the 2016 Exceptional Events Rule, including new PM2.5 implementation focused products under development that are intended to assist air agencies with the development of demonstrations for specific types of exceptional events. With regard to the commenters' specific concerns for wildfires or high winds, the EPA released updated guidance documents on the preparation of exceptional event demonstrations related to wildfires in September 2016, high wind dust events in April 2019, and prescribed fires in August 2019. These guidance documents outline the regulatory requirements and provide examples for air agencies preparing demonstrations for wildfires, high wind dust, and prescribed fire events. For all of the reasons discussed above, the EPA does not agree with the commenters that the form of the primary PM10 standard should be revised to a 99th percentile for continuous monitors.
4. Administrator's Conclusions
This section summarizes the Administrator's considerations and conclusions related to the current primary PM10 standard. In establishing primary standards under the Act that are “requisite” to protect the public health with an adequate margin of safety, the Administrator is seeking to establish standards that are neither more nor less stringent than necessary for this purpose. In so doing, the Administrator notes that his final decision in this reconsideration is a public health policy judgment that draws upon scientific information, as well as judgments about how to consider the range and magnitude of uncertainties that are inherent in the information. Accordingly, he recognizes that his decision requires judgments based on the interpretation of the evidence that neither overstates nor understates the strength or limitations of the evidence nor the appropriate inferences to be drawn. He recognizes, as described in section I.A above, that the Act does not require that primary standards be set at a zero-risk level; rather, the NAAQS must be sufficient but not more stringent than necessary to protect public health, including the health of sensitive groups with an adequate margin of safety.
Given these requirements, and consistent with the primary PM2.5 standards discussed above (section II.C.3), the Administrator's final decision in this reconsideration of the current primary PM10 standard will be a public health policy judgment that draws upon the scientific information examining the health effects of PM10–2.5 exposures, including how to consider the range and magnitude of uncertainties inherent in that information. The Administrator's final decision is based on an interpretation of the scientific evidence that neither overstates nor understates its strengths and limitations, nor the appropriate inferences to be drawn.
Having carefully considered advice from the CASAC and public comments, as discussed above, the Administrator notes that the fundamental scientific conclusions on health effects of PM10–2.5 in ambient air that were reached in the 2019 ISA and summarized in the 2020 PA and 2022 PA remain valid. Additionally, the Administrator believes the judgments he proposed (85 FR 5558, January 27, 2023) with regard to the evidence remain appropriate. Further, in considering the adequacy of the current primary PM10 standard in this reconsideration, the Administrator has carefully considered the policy-relevant evidence and conclusions contained in the 2019 ISA; the rationale and conclusions presented in the 2020 PA and 2022 PA; the advice and recommendations from the CASAC in their reviews of the 2019 draft PA and 2021 draft PA; and public comments, as addressed in section III.B.3 above and in the RTC document. In the discussion below, the Administrator gives weight to the conclusions in the 2020 PA and 2022 PA, with which the CASAC has concurred, as summarized in section III.C of the proposal and takes note of the key aspects of the rationale for those conclusions that contribute to his decision in this review. In considering this information, the Administrator concludes that the preliminary conclusions and policy judgments supporting his proposed decision remain valid, and that the current primary PM10 standard provides requisite protection of public health with an adequate margin of safety and should be retained. In considering the 2020 PA and 2022 PA evaluations and conclusions, the Administrator notes that, while the health effects evidence is somewhat expanded since the 2009 ISA as described in section III.A.2 above, the overall conclusions are generally consistent with those reached in the 2009 ISA (U.S. EPA, 2020b, section 4.4). In so doing, he additionally notes that the CASAC supported the preliminary conclusion in the 2019 draft PA and 2021 draft PA that the evidence reviewed in the 2019 ISA does not call into question the public health protection provided by the current primary PM10 standard against PM10–2.5 exposures and concurs that it is appropriate to consider retaining the current primary PM10 standard (Cox, Start Printed Page 16300 2019b, p. 13 of consensus responses; Sheppard, 2022a, p. 4 of consensus letter).
As noted below, the scientific evidence for PM10–2.5 -related health effects has expanded somewhat since the 2012 review, in particular for long-term exposures. The Administrator recognizes, however, that there are a number of uncertainties and limitations associated with the available information, as described in the proposal (85 FR 5558, January 27, 2023) and below. With regard to the current evidence on PM10–2.5 -related health effects, the Administrator takes note of recent epidemiologic studies that continue to report positive associations with mortality and morbidity in cities across North America, Europe, and Asia, where PM10–2.5 sources and composition are expected to vary widely. While significant uncertainties remain, as described below, the Administrator recognizes that this expanded body of evidence has broadened the range of effects that have been linked with PM10–2.5 exposures. These studies provide an important part of the scientific foundation supporting the 2019 ISA's revised causality determinations (and new determinations) for long-term PM10–2.5 exposures and mortality, cardiovascular effects, metabolic effects, nervous system effects, and cancer (U.S. EPA, 2019a; U.S. EPA, 2022b, section 4.2). Drawing from his consideration of this evidence, the Administrator concludes that the available scientific information supports a decision to maintain a primary PM10 standard to provide public health protection against PM10–2.5 exposures, regardless of location, source of origin, or particle composition. With regard to uncertainties in the evidence, the Administrator first notes that a number of limitations were identified in the 2012 review related to: (1) Estimates of ambient PM10–2.5 concentrations used in epidemiologic studies; (2) limited evaluation of copollutant models to address the potential for confounding; and (3) limited experimental studies supporting biological plausibility for PM10–2.5 -related effects. Despite the expanded body of evidence for PM10–2.5 exposures and health effects assessed in the 2019 ISA, the Administrator recognizes that uncertainties remain, similar to those in the 2012 review. As summarized in section III.A.2 above and in responding to public comments, uncertainties in the available scientific evidence continue to include those associated with the exposure estimates used in epidemiologic studies, the independence of the PM10–2.5 health effect associations, and the biologically plausible pathways for PM10–2.5 health effects (U.S. EPA, 2022b, section 4.3). These uncertainties contribute to the 2019 ISA determinations that the evidence is “suggestive of, but not sufficient to infer” causal relationships (U.S. EPA, 2019a). The Administrator recognizes that the NAAQS must allow for a margin of safety but also places emphasis on evidence supporting “causal” or “likely to be causal” relationships (as described in sections II.A.2 and III.A.2 above). Finding that there is too much uncertainty that a more stringent standard would improve public health, the Administrator judges that the available evidence provides support for his conclusion that the current standard provides the requisite level of protection from the effects of PM10–2.5 . In making this judgment, the Administrator considers whether this level of protection is more than what is requisite and whether a less stringent standard would be appropriate to consider. He notes that there continues to be uncertainty associated with the evidence, as reflected by the “suggestive of, but not sufficient to infer” causal determinations. The Administrator recognizes that the CAA requirement that primary standards provide an adequate margin of safety, as summarized in section I.A above, is intended to address uncertainties associated with inconclusive scientific evidence and technical information, as well as to provide a reasonable degree of protection against hazards that research has not yet identified. In light of these considerations and the current body of evidence, including uncertainties and limitations, the Administrator concludes that a less stringent standard would not provide the requisite protection of public health, including an adequate margin of safety. The Administrator also considers whether the level of protection associated with the current standard is less than what is requisite and whether a more stringent standard would be appropriate to consider. In so doing, the Administrator considers, as discussed above, the level of protection offered from exposures for which public health implications are less clear. In so doing, he again notes the significant uncertainties and limitations that persist in the scientific evidence. In particular, he notes limitations in the approaches used to estimate ambient PM10–2.5 concentrations in epidemiologic studies, limited examination of the potential for confounding by co-occurring pollutants, and limited support for the biological plausibility of the serious effects reported in many epidemiologic studies that are reflected by the “suggestive of, but not sufficient to infer” causal determinations. Thus, in light of the currently available information, including the uncertainties and limitations of the evidence base available to inform his judgments regarding protection against PM10–2.5 -related effects, the Administrator does not find it appropriate to increase the stringency of the standard in order to provide the requisite public health protection. Rather, he judges it appropriate to maintain the level of protection provided by the current primary PM10 standard for PM10–2.5 exposures and he does not judge that the available information and the associated uncertainties indicate the need for a greater level of public health protection.
In reaching his conclusions on the primary PM10 standard, the Administrator also considers advice from the CASAC. In their comments, the CASAC noted that uncertainties that were identified in the 2012 review persist in the evidence for PM10–2.5 -related health effects (Cox, 2019b, p. 13 of consensus responses; Sheppard, 2022a, p. 4 of consensus letter) In considering these comments, the Administrator takes note of the CASAC consideration of the evidence, and associated uncertainties, and its conclusion that the evidence reviewed in the 2019 ISA does not call into question the adequacy of the public health protection afforded by the current primary PM10 standard (Cox, 2019b, p. 3 of letter; Sheppard, 2022a, p. 4 of consensus letter). The Administrator further notes the unanimous conclusions of the CASAC that evidence supports consideration of retaining the current primary PM10 standard (Cox, 2019b, p. 3 of consensus letter; Sheppard, 2022a, p. 4 of consensus letter). In addition to the CASAC's advice, the Administrator also considers public comments, the majority of which supported retaining the primary PM10 standard, citing to and agreeing with the Administrator's rationale for his proposed decision. The Administrator also recognizes that a few public commenters supported revising the primary PM10 standard in order to provide increased protection against PM10–2.5 -related health effects.
The Administrator also notes that the scientific record for his decision on the primary PM10 standard is the same as the record before the then-Administrator in 2020, as the scope of the ISA Supplement focused on health effect categories where the 2019 ISA concluded a causal relationship ( i.e.,Start Printed Page 16301 short- and long-term PM2.5 exposure and cardiovascular effects and mortality). Therefore, because no health outcome categories for short- or long-term PM10–2.5 exposure in the 2019 ISA were greater than “suggestive of, but not sufficient to infer, a causal relationship”, the ISA Supplement did not evaluate studies published after the literature cutoff date of the 2019 ISA related to PM10–2.5 exposures and health effects. The Administrator further notes his decision is consistent with the decision of the prior Administrator in 2020 to retain the primary PM10 standard.
With regard to the indicator for the primary PM10 standard, the Administrator recognizes that the 2022 PA notes that the evidence continues to support retaining the PM10 indicator to provide public health protection against PM10–2.5 -related effects. He notes that, consistent with the approaches in previous reviews, a standard with a PM10 mass-based indicator, in conjunction with a PM2.5 mass-based standard, will result in controlling allowable concentrations of PM10–2.5 . The Administrator also takes note of the 2019 ISA comparison that showed that the relative contribution of PM2.5 and PM10–2.5 to PM10 concentrations can vary across the U.S. by region and season, with urban locations having a somewhat higher contribution of PM2.5 contributing to PM10 concentrations than PM10–2.5 (U.S. EPA, 2019a, section 2.5.1.1.4, Table 2–7). In these urban locations, where PM2.5 concentrations are somewhat higher than in rural locations, the toxicity of the PM10 may be higher due to contaminating PM2.5 . Further, although uncertainties with the evidence persist, the strongest health effects evidence associated with PM10–2.5 comes from epidemiologic studies conducted in urban areas. He also notes that the CASAC agreed with the EPA's conclusions that a PM10 indicator remained appropriate (Cox, 2019b, p. 13 of consensus responses; Sheppard, 2022a, p. 4 of letter). In light of this information, the Administrator concludes that the PM10 indicator remains appropriate and provides protection from exposure to all coarse PM, regardless of location, source of origin, or particle composition.
Similarly, with regard to averaging time, form, and level of the standard, the Administrator takes note of uncertainties in the available evidence and information and continues to find that the current standard, as defined by in all of its elements, is requisite. As an initial matter, the Administrator notes that the current primary PM10 standard, with its level of 150 µg/m3 , 24-hour averaging time, not to be exceeded more than once per year on average over three years, is intended to protect against short-term peak PM10–2.5 exposures. In so doing, while the Administrator notes that changes in PM2.5 concentrations in ambient air can influence the contribution of the fine and coarse fractions to PM10 mass, such that reductions in PM2.5 concentrations can lead to more allowable PM10–2.5 under the current primary PM10 standard, he recognizes that there is no new information available in this reconsideration to suggest that the public health protection provided by the current standard is not requisite or that a more stringent standard is warranted at this time. The Administrator concludes that, particularly in light of his decision to retain the primary 24-hour PM2.5 standard with its level of 35 µg/m3 as described in section II.B.4 above, the primary PM10 standard would be expected to maintain PM10–2.5 concentrations in ambient air below those that have been considered to be associated with serious health effects in past NAAQS reviews. The Administrator also notes that while the scientific evidence available in the 2019 ISA has expanded since the completion of the 2009 ISA, he concludes that this information does not provide support for the causal or likely to be causal relationships upon which he places the greatest weight in considering the adequacy of the current standards. He further concludes that the uncertainties and limitations of the scientific evidence, along with the absence of information to inform a quantitative exposure or risk assessment, make it difficult to reach decisions regarding whether a more protective standard is warranted at this time. He has additionally considered the public comments regarding revisions to these elements of the standard and continues to judge that the existing level and the existing form, in all its aspects, together with the other elements of the existing standard provide an appropriate level of public health protection. For all of the reasons discussed above and recognizing the CASAC's conclusion that the current evidence provides support for retaining the current standard, the Administrator concludes that the current primary PM10 standard (in all of its elements) is requisite to protect public health with an adequate margin of safety from effects of PM10–2.5 in ambient air and should be retained without revision.
C. Decision on the Primary PM10 Standard
For the reasons discussed above and considering information and assessments presented in the 2019 ISA and the 2022 PA, the advice from the CASAC, and public comments, the Administrator concludes that the current primary PM10 standard is requisite to protect public health with an adequate margin of safety, including the health of at-risk populations, and is retaining the current standard without revision.
IV. Communication of Public Health
A. Air Quality Index Overview
Information about the public health implications of ambient concentrations of criteria pollutants is communicated to the public using the Air Quality Index (AQI) reported on the EPA's AirNow website.[133] The current AQI has been in use since its inception in 1999.[134] It provides useful, timely, and easily understandable information about the daily degree of pollution. The goal of the AQI is to establish a nationally uniform system of indexing pollution concentrations for ozone, carbon monoxide, nitrogen dioxide, PM, and sulfur dioxide. The AQI is recognized internationally as a proven tool to effectively communicate air quality information to the public as demonstrated by the fact that many countries have created similar indices based on the AQI.
The AQI converts an individual pollutant concentration in a community's air to a number on a scale from 0 to 500. Reported AQI values for specific pollutants enable the public to know whether air pollution levels in a particular location are characterized as good (0–50), moderate (51–100), unhealthy for sensitive groups (101–150), unhealthy (151–200), very unhealthy (201–300), or hazardous (301+). Across criteria pollutants, the AQI value of 100 typically corresponds to the level of the short-term ( e.g., 24-hour, 8-hour, or 1-hour standard) NAAQS for each pollutant. Below an index value of 100, an intermediate value of 50 is defined either as the level of the annual standard if an annual standard has been established ( e.g., PM2.5, nitrogen dioxide), a Start Printed Page 16302 concentration equal to one-half the value of the 24-hour standard used to define an index value of 100 ( e.g., carbon monoxide), or a concentration based directly on health effects evidence ( e.g., ozone). An AQI value greater than 100 means that a pollutant is in one of the unhealthy categories ( i.e., unhealthy for sensitive groups, unhealthy, very unhealthy, or hazardous). An AQI value at or below 100 means that a pollutant concentration is in one of the satisfactory categories ( i.e., moderate or good). The scientific evidence on pollutant-related health effects for each NAAQS review support decisions related to pollutant concentrations at which to set the various AQI breakpoints, which delineate the AQI categories for each individual pollutant ( i.e., the pollutant concentrations corresponding to index values of 150, 200, 300, and 500). The AQI is reported three ways by the EPA and State, local and Tribal agencies, all of which are useful and complementary. The daily AQI is reported for the previous day and used to observe trends in community air quality, the AQI forecast helps people plan their outdoor activities for the next day, and the near-real-time AQI, or NowCast AQI, tells people whether it is a good time for outdoor activity.
Historically, State and local agencies have primarily used the AQI to provide general information to the public about air quality and its relationship to public health. For more than two decades, many State and local agencies, as well as the EPA and other Federal agencies, have been developing new and innovative programs and initiatives to provide more information related to air quality and health messaging to the public in a more timely way. These initiatives, including air quality forecasting, near real-time data reporting through the AirNow website, use of data from air quality sensors on the EPA and U.S. Forest Service's (USFS) Fire and Smoke Map, and air quality action day programs, provide useful, up-to-date, and timely information to the public about air pollution and its health effects. Such information can help the public learn when their well-being may be compromised, so they can take actions to avoid or to reduce exposures to ambient air pollution at concentrations of concern. This information can also encourage the public to take actions that will reduce air pollution on days when concentrations are projected to be of concern to local communities ( e.g., air quality action day programs can encourage individuals to drive less or carpool).
B. Air Quality Index Category Breakpoints for PM2.5
Recognizing the scientific information available and current AQI reporting practices, the EPA proposed several revisions to the AQI PM2.5 breakpoints. EPA solicited and received comments on these proposed revisions. Upon reviewing the information in the proposal and considering the comments received EPA is making final revisions to the AQI category breakpoints for PM2.5. This section summarizes the proposed revisions, which can be read in full in the proposal (88 FR 5638, January 27, 2023), significant comments, and final revisions.
1. Summary of Proposed Revisions
One purpose of the AQI is to communicate to the public when air quality is poor and thus when they should consider taking actions to reduce their exposures. The higher the AQI value, the higher the level of air pollution and the greater the health concern. In recognition of the scientific information available that is informing the reconsideration of the 2020 final decision on the primary PM2.5 standards, including a number of new controlled human exposure and epidemiologic studies published since the completion of the 2009 ISA, as well as additional epidemiologic studies from other peer reviewed documents that evaluate the health effects of wildfire smoke exposure and that can inform the selection of AQI breakpoints at higher PM2.5 concentrations,[135] the EPA proposed to make two sets of changes to the PM2.5 sub-index of the AQI. First, the EPA proposed to continue to use the approach used in the revisions to the AQI in 2012 (77 FR 38890, June 29, 2012) of setting the lower breakpoints (50, 100 and 150) to be based on the levels of the primary PM2.5 annual and 24-hour standards and proposed to revise the lower breakpoints to be consistent with changes to the primary PM2.5 standards that are part of this reconsideration. Second, the EPA proposed to revise the upper AQI breakpoints (200 and above) and to replace the linear-relationship approach used in 1999 to set these breakpoints, with an approach that more fully considers the PM2.5 health effects evidence from controlled human exposure and epidemiologic studies that have become available in the last 20 years (64 FR 42530, August 4, 1999).
a. Air Quality Index Values of 50, 100 and 150
With respect to the lower AQI breakpoints in the proposal (88 FR 5638, January 27, 2023), the EPA proposed to conclude that it is appropriate to continue setting these breakpoints to be consistent with the primary annual and 24-hour PM2.5 standard levels. The lowest AQI value of 50 provides the breakpoint between the “good” and “moderate” categories. At and below this concentration, air quality is considered “good” for everyone. Above this concentration, in the “moderate” category, the AQI contains advisories for unusually sensitive individuals. The EPA has historically set this breakpoint at the level of the primary annual PM2.5 standard. In doing so, the EPA has recognized that: (1) The annual standard is set to provide protection to the public, including at-risk populations, from PM2.5 concentrations, which, when experienced on average for a year, have the potential to result in adverse health effects; and (2) the AQI exposure period represents a shorter exposure period ( e.g., 24-hour (or less)) while focusing on the most sensitive individuals. The EPA saw no basis for deviating from this approach in this reconsideration. Thus, the EPA proposed to set the AQI value of 50 at a daily ( i.e., 24-hour) average concentration equal to the level of the primary annual PM2.5 standard that is promulgated.
The historical approach to setting an AQI value of 100, which is the breakpoint between the “moderate” and “unhealthy for sensitive groups” categories, and above which advisories are generated for sensitive groups, is to set it at the same level as the primary 24-hour PM2.5 standard. In so doing, the EPA has recognized that the primary 24-hour PM2.5 standard is set to provide protection to the public, including at-risk populations, from short-term exposures to PM2.5 concentrations that have the potential to result in adverse health effects. Given this, it is appropriate to generate advisories for sensitive groups at concentrations above this level. In the past, State, local, and Tribal air quality agencies have expressed strong support for this approach (78 FR 3086, January 15, 2013). The EPA saw no basis to deviate Start Printed Page 16303 from this approach in this reconsideration. In the proposal (88 FR 5638, January 27, 2023), the EPA proposed to retain the current primary 24-hour PM2.5 standard with its level of 35 μg/m3 but took comment on revising the level of that standard to 25 μg/m3 (section II.D.3.b). Thus, the EPA proposed to retain the AQI value of 100 set at the level of the current primary 24-hour PM2.5 standard concentration of 35 μg/m3 ( i.e., 24-hour average).
With respect to an AQI value of 150, which is the breakpoint between the “unhealthy for sensitive groups” and “unhealthy categories,” this breakpoint concentration in this reconsideration is based upon the considering the same health effects information, as assessed in the 2019 ISA and ISA Supplement and described in section II above, that informs the proposed decisions on the level of the 24-hour standard and the AQI value of 100. Previously, the Agency has used a proportional adjustment in which the AQI value of 150 was set proportionally to the AQI value of 100. This proportional adjustment inherently recognizes that the available epidemiologic studies provide no evidence of discernible thresholds, below which effects do not occur in either sensitive groups or in the general population, that could inform conclusions regarding concentrations at which to set this breakpoint. Given that the epidemiologic evidence continues to be the most relevant health effects evidence for informing this range of AQI values, the EPA saw no basis to deviate from this approach in this reconsideration. Therefore, the EPA proposed to set an AQI value of 150 proportionally, depending on the breakpoint concentration of the AQI value of 100 ( i.e., 55.4 for a 24-hour standard of 35 μg/m3 ).
b. Air Quality Index Values of 200 and Above
In the proposal (88 FR 5639, January 27, 2023), the EPA summarized the history of setting the AQI values of 300 and above in the 1999 rule (64 FR 42530, August 4, 1999) and established breakpoints for PM2.5 in that range. In general, the AQI values between 100 and 500 were based on PM2.5 concentrations that generally reflected a linear relationship between increasing index values and increasing PM2.5 concentrations.[136] It was found that this linear relationship was generally consistent with the health effects evidence, which suggested that as PM2.5 concentrations increase, increasingly larger numbers of people are likely to experience serious health effects in this range of PM2.5 concentrations (64 FR 42536, August 4, 1999). For the AQI breakpoint of 500, the concentration was based on the method used to establish a previously existing PM10 breakpoint that was informed by studies conducted in London using the British Smoke method, which uses a different particle size cutpoint as noted in the proposal (88 FR 5639, January 27, 2023). Due to limited ambient PM2.5 monitoring data available at that time, the decision on the 500 value concentration for PM2.5 was based on the stated assumption that PM concentrations measured by the British Smoke method were approximately equivalent to PM2.5 concentrations (64 FR 42530, August 4, 1999). Given that the British Smoke method has a larger particle size cutpoint than the current PM2.5 monitoring method, which has a cutpoint of 2.5 microns, a concentration of 500 μg/m3 based on the British Smoke method would be equivalent to a lower PM2.5 concentration. With respect to the upper breakpoints of the AQI, the EPA has historically been concerned about establishing these upper breakpoints using evidence based on larger size fractions of PM, given that PM2.5 is the indicator for the AQI. While monitoring data for higher PM2.5 concentrations in ambient air has been available for many years, the health effects evidence has only recently become available for consideration in informing decisions on the upper breakpoints of the AQI.
As part of this reconsideration, the EPA recognized that the health effects evidence associated with PM2.5 exposure has greatly expanded in recent years. Multiple controlled human exposure studies have become available that provide information about health effects across a range of concentrations. While many of the new studies evaluated in the 2019 ISA focused on examining health effects associated with exposure to lower PM2.5 concentrations, there are also several new controlled human exposure studies that provide information about the health effects observed in study participants at concentrations well above the standard levels. Additionally, there are also epidemiologic studies now available and evaluated in other Agency peer-reviewed documents that can inform health effects associated with higher PM2.5 concentrations (U.S. EPA, 2021b).[137] Thus, the EPA concluded that it is appropriate to reevaluate the upper AQI breakpoints, taking into account the expanded body of scientific evidence, particularly given several new epidemiologic studies conducted during high pollution events like wildfires and multiple controlled human exposure studies. While it remains unclear the exact PM2.5 concentrations at which specific health effects occur, the more recent studies do provide more refined information about the concentration range in which these effects might occur in some populations. These studies provide support for coherence of effects across scientific disciplines and potentially biologically plausible pathways for the overt population-level health effects observed in epidemiologic studies. Therefore, taking into account the short exposure time period in these studies ( e.g., 1–6 hours) and that the studies generally do not include at-risk (or sensitive) populations, but rather young, healthy adults, these studies, in conjunction with information from epidemiologic studies, the EPA preliminarily concluded it would be appropriate to be more cautionary and offer advisories to the public for reducing exposures at lower concentrations than recommended with the current AQI breakpoints.
The AQI value of 200 is the breakpoint between the “unhealthy” and “very unhealthy” categories. At AQI values above 200, the AQI would be providing a health warning that the risk of anyone experiencing a health effect following short-term exposures to these PM2.5 concentrations has increased. To inform proposed decisions on this breakpoint, the EPA takes note of studies indicating the potential for respiratory or cardiovascular effects that are on their own representative of or are on the biologically plausible pathway to more serious health outcomes ( e.g., emergency department visits, hospital admissions). The controlled human exposure studies evaluated in the 2009 and 2019 ISAs provide evidence of inflammation as well as cardiovascular effects in healthy subjects at and above 120 µg/m3 . For example, Ramanathan et al. (2016) observed a transient reduction in antioxidant/anti-inflammatory function after exposing healthy young subjects to a mean concentration of 150 µg/m3 of PM2.5 for 2 hours. Urch et al. Start Printed Page 16304 (2010) also reported increased markers of inflammation when exposing both asthmatic and non-asthmatic subjects to a mean concentration of 140 µg/m3 of PM2.5 for 3 hours. In studies specifically examining cardiovascular effects, Ghio et al. (2000) and Ghio et al. (2003) exposed healthy subjects to a mean concentration of 120 µg/m3 for 2 hours and reported significantly increased levels of fibrinogen, a marker of coagulation that increases during inflammation. Sivagangabalan et al. (2011) exposed healthy subjects to a mean concentration of 150 µg/m3 of PM2.5 for 2 hours and noted an increased QT interval (3.4 ± 1.4) indicating some evidence for conduction abnormalities, an indicator of possible arrhythmias. Lastly, Brook et al. (2009) reported a transient increase of 2.9 mm Hg in diastolic blood pressure in healthy subjects during the 2-hour exposure to a mean concentration of 148 µg/m3 of PM2.5.
In addition to epidemiologic studies evaluated in the 2019 ISA that analyzed exposures at ambient PM2.5 concentrations, there are a number of recent epidemiologic studies focusing on wildfire smoke that have become available that were evaluated in the EPA's recently released peer-reviewed assessment on wildland fire (U.S. EPA, 2021b). One of these studies, Hutchinson et al. (2018), conducted a bidirectional case-crossover analysis to examine associations between wildfire-specific PM2.5 exposure and respiratory-related healthcare encounters ( i.e., ED visits, inpatient hospital admissions, and outpatient visits) prior and during the 2007 San Diego wildfires. This study found positive and significant associations to PM2.5 exposures and respiratory-related healthcare encounters. Further, during the initial 5-day period of the wildfire event, the study observed that there was evidence of increases in a number of respiratory-related outcomes particularly ED visits for asthma, upper respiratory infection, respiratory symptoms, acute bronchitis, and all respiratory-related visits (Hutchinson et al., 2018). When examining the air quality during the wildfire event, PM2.5 concentrations were highest during the initial five days of the wildfire, with 24-hour average PM2.5 concentrations of 89.1 µg/m3 across all zip codes and with the highest 24-hour average of 160 µg/m3 on the first day (Hutchinson et al., 2018).
When considering this collective body of evidence from controlled human exposure and epidemiologic studies, the Agency proposed to set an AQI value of 200 at a daily ( i.e., 24-hour average) concentration of PM2.5 of 125 μg/m3 . As discussed above and in the proposal (88 FR 5640, January 27, 2023), this concentration is at the lower end of the concentrations consistently shown to be associated with respiratory and cardiovascular effects in controlled human exposure studies following short-term exposures ( e.g., 2–3 hours) and in young, healthy adults (Ghio et al., 2000; Ghio et al., 2003; Urch et al., 2010; Ramanathan et al., 2016; Sivagangabalan et al., 2011; and Brook et al., 2009) and also within the range of 5-day average and maximum concentrations observed to be associated with respiratory-related outcomes following exposure to wildfire smoke (Hutchinson et al., 2018).
The AQI value of 300 denotes the breakpoint between the “very unhealthy” and “hazardous” categories, and thus marks the beginning of the “hazardous” AQI category. At AQI values above 300, the AQI provides a health warning that everyone is likely to experience effects following short-term exposures to these PM2.5 concentrations. To inform decisions on this AQI breakpoint, the EPA takes note of controlled human exposure studies that consistently show subclinical effects which are often associated with more severe cardiovascular outcomes. As discussed above, Brook et al. (2009) reported a transient increase of 2.9 mm Hg in diastolic blood pressure in healthy subjects during the 2-hour exposure to a mean concentration of 148 µg/m[3] of PM2.5 . Bellavia et al. (2013) exposed healthy subjects to an average PM2.5 concentration of 242 µg/m[3] for 2 hours and reported increased systolic blood pressure (2.53 mm Hg). Tong et al. (2015) exposed healthy subjects to an average PM2.5 concentration of 253 µg/m[3] for 2 hours and observed a significant increase in diastolic blood pressure (2.1 mm Hg) and a nonsignificant increase in systolic blood pressure (2.5 mm Hg). Lucking et al. (2011) reported impaired vascular function and increased potential for coagulation when exposing healthy subjects to diesel exhaust (DE) with an average PM2.5 concentration of 320 µg/m[3] for a duration of 1 hour.[138] These studies all provided evidence of impaired vascular function, including vasodilatation impairment and increased thrombus formation, with Tong et al. (2015), Bellavia et al. (2013), Brook et al. (2009) all reporting increases in blood pressure. Additionally, Behbod et al. (2013) reported increased inflammatory markers following a 2-hour exposure to an average PM2.5 concentration of 250 µg/m3 in healthy subjects.
In addition to the controlled human exposure studies discussed above, the epidemiologic study conducted by DeFlorio-Barker et al. (2019) examined the relationship between wildfire smoke and cardiopulmonary hospitalizations among adults 65 years of age and older from 2008–2010 in 692 U.S. counties. The authors reported a 2.22% increase in all-cause respiratory hospitalizations on wildfire smoke days for a 10 µg/m3 increase in 24-hour average PM2.5 concentrations (DeFlorio-Barker et al., 2019). The maximum 24-hour average concentration in this study on wildfire smoke days was 212.5 µg/m3 (DeFlorio-Barker et al., 2019). In considering this study, the EPA notes the increased probability that even healthy adults experience effects at this maximum exposure concentration, particularly given that this maximum concentration is near the exposure concentrations in controlled human exposure studies that consistently reported evidence of impaired vascular function and several that reported increases in blood pressure in healthy adults following 2-hour exposures.
Based on the information discussed above and in the proposal (88 FR 5640, January 27, 2023), the EPA proposed to revise the 300 level of the AQI, which marks the beginning of the “hazardous” AQI category, to a concentration that is consistent with the PM2.5 concentrations associated with health effects as reported in the controlled human exposure (Brook et al., 2009; Bellavia et al., 2013; Tong et al., 2015; Behbod et al., 2013) and epidemiologic studies (DeFlorio-Barker et al. (2019). Specifically, the Agency proposed to set an AQI value of 300 at a daily ( i.e., 24-hour average) PM2.5 concentration of 225 μg/m3 . This concentration falls between the 2-hour average concentrations reported in controlled human exposure studies found to be consistently associated, in healthy adults, with impaired vascular function and/or increases in blood pressure, which could both be a precursor to more severe cardiovascular effects following short-term (1- to 2-hour) exposures, and the maximum 24-hour average PM2.5 concentrations on wildfire smoke days reported in the epidemiologic study conducted by DeFlorio-Barker et al. (2019). Start Printed Page 16305
c. Air Quality Index Value of 500
Lastly, the EPA also proposed revisions to the 500 value of the AQI. The 500 value of the AQI is within the “hazardous” category but is specified and used to calculate the slope of the AQI values in the “hazardous category” above and below AQI values of 500. In the past, this breakpoint had a very prominent role in determining the current upper AQI values given that it was used as part of the linear relationship with the concentration at the AQI value of 100 to determine the AQI values of 200 and 300 in 1999 (64 FR 42530, August 4, 1999).
As discussed above and in the proposal (88 FR 5641, January 27, 2023), the current breakpoint concentration for the 500 value of the AQI was set in 1999 at a 24-hour average PM2.5 concentration of 500 μg/m[3] and was based on studies conducted in London using the British Smoke method, which used a different particle size cutpoint and likely overestimated the PM2.5 concentration. In looking to improve upon that approach, the EPA considered several recent controlled human exposure studies that observe health effects that are on the biologically plausible pathway to more severe cardiovascular outcomes and note that these seem to follow exposures to high PM2.5 concentrations that are well above those typically observed in ambient air. More specifically, in controlled human exposure studies, Vieira et al. (2016a) and Vieira et al. (2016b) exposed healthy subjects and subjects with heart failure to diesel exhaust (DE) with a mean PM2.5 concentration of 325 µg/m[3] for 21 minutes and reported decreased stroke volume, and increased arterial stiffness (an indicator of endothelial dysfunction) in both healthy and heart failure subjects.[139] Also as summarized above and discussed in the proposal (88 FR 5641, January 27, 2023), Lucking et al. (2011) exposed healthy subjects to DE with a mean PM2.5 concentration of 320 µg/m[3] for 1 hour.[140] Epidemiologic studies have linked the types of cardiovascular effects observed in these controlled human exposure studies with the exacerbation of ischemic heart disease (IHD) and heart failure as well as myocardial infarction (MI) and stroke.
In addition to the controlled human exposure studies discussed in the proposal (88 FR 5641, January 27, 2023) and summarized above, recent epidemiologic studies examining the relationship between concentrations of PM2.5 during wildfires and respiratory health also informed the proposed decisions on the concentration for the AQI value of 500. As discussed in the proposal (88 FR 5641, January 27, 2023) and summarized earlier in this section, Hutchinson et al. (2018) reported increases in a number of respiratory-related ED visits for asthma, upper respiratory infection, respiratory symptoms, acute bronchitis, and all combined respiratory-related visits based on data from Medi-Cal claims for emergency department presentations, inpatient hospitalizations, and outpatient visits during the initial 5-day period of the 2007 San Diego fire. During the initial 5-day window, PM2.5 concentrations were found to be at their highest with the 95th percentile of 24-hour average concentrations of 333 µg/m3 .
Although studies of short-term ( i.e., daily) exposures to wildfire smoke are more informative in considering alternative level for the AQI value of 500 since they mirror the 24-hour exposure timeframe, additional information from epidemiologic studies of longer-term exposures ( i.e., over many weeks) during wildfire events can provide supporting information. As discussed in the proposal (88 FR 5641, January 27, 2023) and summarized here, Orr et al. (2020) conducted a longitudinal study that reported exposure to wildfire smoke from a multi-month fire resulted in reduced lung function in subsequent years and concluded that exposure to high PM2.5 concentrations during a multi-week fire event may lead to health consequences, such as declines in lung function. During the 2017 wildfire event (August 1 to September 19, 2017), Orr et al. (2020) reported that many days during the multi-month fire had PM2.5 concentrations above 300 µg/m3 , resulting in a daily average PM2.5 concentration of 220.9 μg/m3 with a maximum PM2.5 concentration of 638 µg/m3 .
The controlled human exposure studies provide biological plausibility for results of epidemiologic studies that document increases in respiratory-related health care events during the wildfires. The collective evidence from controlled human exposure and epidemiologic studies, which includes decreases in stroke volume, increased arterial stiffness, impaired vascular function and respiratory-related healthcare encounters provide health-based evidence that informed the proposed decisions on the level of the AQI value of 500. Given the concentrations observed in these studies, the Agency proposed to revise the AQI value of 500 to a level set at a daily ( i.e., 24-hour average) PM2.5 concentration of 325 μg/m3 . This concentration is at or below the lowest concentrations observed in the controlled human exposure studies associated with more severe effects discussed above and also at the low end of the daily concentrations observed in the epidemiologic studies conducted by Hutchinson et al. (2018) and Orr et al. (2020).
Table 1 below summarizes the proposed breakpoints for the PM2.5 sub-index.
Table 1—Proposed Breakpoints for PM 2.5 Sub-Index
AQI category Index values Proposed breakpoints (μg/m3 , 24-hour average) Good 0–50 0.0–(9.0–10.0) Moderate 51–100 (9.1–10.1)–35.4 Unhealthy for Sensitive Groups 101–150 35.5–55.4 Unhealthy 151–200 55.5–125.4 Very Unhealthy 201–300 125.5–225.4 Start Printed Page 16306 Hazardous 1 301+ 225.5 1 AQI values between breakpoints are calculated using equation 1 in appendix G. For AQI values in the hazardous category, AQI values greater than 500 should be calculated using equation 1 and the PM 2.5 concentration specified for the AQI value of 500. 2. Summary of Significant Comments on Proposed Revisions
The EPA received many comments on the proposed changes to the PM2.5 AQI breakpoints. Many commenters generally supported all the proposed revisions to the AQI breakpoints based on the revisions to the primary annual and daily PM2.5 standards and recent scientific evidence discussed in the proposal (88 FR 5558, January 27, 2023). However, we received specific comments on proposed revisions to the breakpoints in the lower end of the AQI, related to their linkage to the annual and daily PM2.5 standards, and proposed revisions to the breakpoints at the upper end of the AQI, based on EPA's interpretation of available health effects evidence.
a. Air Quality Index Values of 50, 100, and 150
Some commenters agreed with using the historical approach of setting the 50, 100 and 150 breakpoints of the AQI to be consistent with the primary PM2.5 standards. Some cited the reason that this approach creates consistent communication with respect to air quality and the standards, and this is how the other AQI sub-indices are set. A few commenters disagreed with the historical approach and suggested instead that the 50 breakpoint of the AQI should not be revised at all, or that the 50 and 100 breakpoints of the AQI should be supported directly by health data similar to the basis for the proposed 200, 300 and 500 breakpoints.
The few commenters that disagreed with the historical approach of the 50 breakpoint of the AQI noted that setting a short-term breakpoint to annual standard was not logical since it is a long-term standard and not meant to be interpreted for short-term messaging with the AQI, in particular when reported hourly via the NowCast. These commenters also noted that additional studies are needed to identify the health impacts of short-term exposures at low concentrations. They also noted that lowering the 50 breakpoint of the AQI in conjunction with the annual standard may cause confusion with the public because some State programs and policy decisions are connected to the AQI while others are based on PM concentrations, which could lead to inconsistent messaging reducing the public's trust. These comments were supported by noting that revised breakpoints could lead to more moderate days than in the past, but the monitor values would be the same as before when the commenters considered it “healthy,” possibly eroding trust in air agencies' messaging. Commenters also noted if the breakpoints are revised, the public will not visually be able to detect the difference between what was considered a good AQI day versus a now moderate AQI day.
The EPA disagrees with these commenters. With respect to setting a short-term breakpoint to the level of a much longer-term (annual) standard, setting the lower AQI breakpoints at the level of the annual and daily PM2.5 standards for communication purposes was discussed in the proposed reconsideration (88 FR 5558, January 27, 2023) and previously supported by State organizations in the 2012 PM Final Rule (77 FR 38890, June 29, 2012). Both the AQI and the Pollutant Standards Index, which came before it, have historically been normalized across pollutants by defining an index value of 50 and 100 as the numerical level of the annual (when defined) and short-term ( i.e., averaging time of 24-hours or less) primary NAAQS for each pollutant. This approach clearly communicates the air quality to the public. The EPA considers this approach to be appropriate given the available evidence and structure of the standard. As discussed in section II.B above and in the notice of final rulemaking for the 2012 review (77 FR 38890, June 29, 2012), the primary annual and 24-hour PM2.5 standards work together in concert to provide public health protection. The annual PM2.5 standard is generally viewed as the principal means of providing public health protection against “typical” daily and annual PM2.5 exposures, while the 24-hour PM2.5 standard is generally viewed as a means of providing protection against short-term exposures to “peak” PM2.5 concentrations, such as can occur in areas with strong contributions from local or seasonal sources, even when annual average PM2.5 concentrations remain relatively low. Because the annual standard provides public health protection for typical daily PM2.5 exposures, the EPA thinks it is appropriate to use that level for the 50 breakpoint of the AQI and describe daily air quality at and below the level of the annual standard “Good.” Since an annual standard allows for days with air quality above that level, it is appropriate to call days just above it “Moderate.” If the 50 breakpoint of the AQI was set at a level above the annual standard, it would be possible for the majority of days to be called “good” in a year when an area exceeds the annual standard. This could cause confusion with the public about air quality if the general perception is that local air quality is “good,” but the area fails to meet the annual standard. In addition, the EPA continues to find it appropriate to use the NowCast with the PM2.5 AQI index to provide more real-time information to the public. As discussed in the AQI Technical Assistance Document, while the NowCast algorithm is approximating a 24-hour average exposure, it can reflect concentrations observed over shorter averaging times when air quality is changing rapidly (U.S. EPA, 2018a). The EPA continues to consider the use of the primary annual standard level suitable in the NowCast given the health evidence supporting the standard and given that the reported concentrations are an approximation of “typical” daily exposure. Additionally, the EPA reflects the nature of the NowCast in the associated health messaging.
With regard to the commenter stating the public may not be able to visually detect a difference in the air quality, the EPA notes that the AQI is intended to be a communication tool for public awareness precisely because it is generally difficult for the public to visually judge air quality risks when air pollution is “moderate.” Moreover, since the establishment of the AQI, the EPA and State and local air agencies and organizations have developed experience in educating the public about changes in the standards and, Start Printed Page 16307 concurrently, related changes to AQI breakpoints and advisories. When the standards change, the EPA and State and local agencies have sought to help the public understand that air quality is not getting worse, it's that the health evidence underlying the standards and the AQI has changed. The EPA's Air Quality System (AQS), the primary repository for air quality monitoring data, is also adjusted to reflect the revised breakpoints. Specifically, all historical AQI values in AQS are recomputed with the revised breakpoints, so that all data queries and reports downstream of AQS will show appropriate trends in AQI values over time. If any State, local or Tribal air agency is concerned that people are or will be confused on a moderate AQI day, then they could use the communication information that has been developed with this rulemaking.
Some commenters stated that the AQI should not necessarily be linked to the primary PM2.5 standards. One example is the comment that if the annual standard is not lowered to 8 µg/m3 , the EPA should lower the 50 breakpoint of the AQI to that level to better inform the public of the need for behavioral modifications to reduce the harm to health from PM2.5 exposure. Similar to the reasons discussed above, the EPA concludes that setting the 50 breakpoint of the AQI at the level of the annual PM2.5 standard is appropriate from a health perspective and for communication purposes. The Administrator has judged the primary annual standard (in conjunction with the other primary standards) as revised in this final action to be requisite to protect public health with an adequate margin of safety, based on the health evidence discussed in section II.A.2. Setting the 50 breakpoint lower than the annual standard also has the potential to cause confusion with the public since it does not reflect the standards and the Administrator's judgments about the standards as well.
With regard to the 100 breakpoint of the AQI, several commenters expressed the view that the level of the 24-hour PM2.5 standard and an AQI value of 100 should be set at 25 μg/m3 based on the body of evidence and lower end of the range recommended by CASAC. These commenters noted that if the current 24-hour standard and AQI value of 100 is retained at 35 μg/m3 then the public will not be able to make informed decisions about actions to take to protect their health. Many of these commenters further recommended that the AQI value of 100 should be lowered to 25 μg/m3 even if the standard is retained. Commenters expressed the view that this would more adequately allow the public to take health-protective actions.
The EPA disagrees with these commenters and notes that many State, Tribal and local air agencies have expressed strong support for aligning the 100 breakpoint of the AQI with the short-term 24-hour primary PM2.5 standards as discussed in the proposal (88 FR 5558, January 27, 2023). The EPA agrees with the view, expressed by State, local and Tribal entities, that aligning the lower breakpoints with the standards enables clear communication of the standards. This alignment approach is also utilized in the other AQI sub-indices lower breakpoints and taking a different approach with the PM2.5 AQI could cause confusion. Additionally, the Administrator has judged that it is appropriate to retain the 24-hour standard at a level of 35 μg/m3 (in conjunction with the other primary standards) to protect public health with an adequate margin of safety, based on the health evidence discussed in section II.A.2. Thus, EPA disagrees that it is necessary or appropriate to set the 100 breakpoint at a lower concentration to provide further information to the public. The 50 breakpoint, which is set at a level below 25 μg/m3 , will continue to provide information to members of the public particularly concerned about exposures to PM2.5. As with the 50 breakpoint, aligning the breakpoint with the standard both reflects the Administrator's judgment about the health risks and eliminates the potential to cause confusion in the public about those risks.
b. Air Quality Index Values of 200 and Above
Some commenters supported the proposed revisions to the 200, 300 and 500 breakpoints that recognize the expanded body of scientific evidence, particularly several new epidemiologic studies conducted during high pollution events such as wildfires and multiple controlled human exposure studies. A few commenters agreed with incorporating the expanded body of scientific evidence into the 200, 300 and 500 breakpoints, but suggested a modified linear approach between 200 (115 μg/m3 ) and 500 (312 μg/m3 , setting the 300 breakpoint to 187 μg/m3 ) based on recent epidemiologic wildfire smoke studies.
Other commenters disagreed with the proposed revisions and suggested the EPA should continue using the previous breakpoints that follow the 1999 linear approach (64 FR 42530, August 4, 1999), because not changing the breakpoints would simplify communications. A few commenters stated the proposed revisions to the AQI upper breakpoints are not justified because the scientific evidence supporting the revisions is inadequate. To support this view, the commenters suggest that only three epidemiologic studies were used in determining the upper breakpoints and none of them were representative of potential effects in the general public; of the 13 studies cited only three were near the proposed revised breakpoints; four of the studies involved exposure to PM from diesel and traffic pollution, which is different than PM from wildfire smoke; and the data supporting the revisions only indicated “mild” health effects that were mostly in sensitive populations.
The EPA agrees with the majority of commenters that supported utilizing the expanded body of scientific evidence to revise the 200, 300 and 500 breakpoints of the AQI. The EPA appreciates the suggestion of using a revised linear approach from 200 to 500. But rather than using the available evidence to only set the breakpoint of 500, the EPA finds it appropriate to set the breakpoints for 200, 300 and 500 using an evidence-based approach, by relying on information presented in both controlled human exposure studies and epidemiologic studies that examine relationships between high PM2.5 exposure episodes ( i.e., periods of wildfire smoke) and various health outcomes. Setting these breakpoints based directly on health effects evidence, which can be communicated, is more useful and appropriate than using a linear approach, because it can better describe the potential health effects and symptoms which also helps the public better understand why more health protective actions are needed. By its nature, a linear approach does not evaluate and identify associated health effects and risk factors.
The EPA disagrees with the commenters that expressed the view that these upper breakpoints should not be revised based largely on the numerous peer-reviewed studies published since the 200, 300 and 500 breakpoints were originally established in 1999 (64 FR 42530, August 4, 1999). As discussed in the proposal (88 FR 5641, January 27, 2023), the rationale behind the proposed revisions is rooted in the fact the upper AQI breakpoints are based on outdated scientific evidence. Specifically, the traditional linear approach was predicated on the 500 value of the AQI, which was estimated using health studies that used the British Smoke Method. The British Smoke Method is based on a particle size fraction (4.5 microns) that is larger Start Printed Page 16308 than PM2.5 . Given that the British Smoke method has a larger particle size cutpoint than the current PM2.5 monitoring method, which has a cutpoint of 2.5 microns, a concentration of 500 μg/m3 based on the British Smoke method would be equivalent to a lower PM2.5 concentration (88 FR 5641, January 27, 2023). The combination of a larger particle size fraction informing previous decisions around upper AQI breakpoints and more recent scientific evidence than the London Fog Episode, on the potential health consequences of what we currently consider to be high PM2.5 exposures, provides the underlying basis for revising the upper breakpoints to better inform the public about air quality to allow the public to take health protective actions as appropriate. Moreover, as discussed above, until recently there was limited information upon which to base the breakpoints between 150 and 500, so the linear approach was a reasonable substitute. While not changing the breakpoints may be easier because there is no change to communicate, using a health-based approach is more appropriate, because it helps the public better understand that more health protective actions are needed.
The Agency disagrees that the scientific evidence discussed in the proposal is inadequate to revise the 200, 300 and 500 breakpoints of the AQI (88 FR 5640, January 27, 2023). The EPA disagrees that these studies should not be considered because they “indicated mild health effects in sensitive populations.” The EPA notes that many of the subclinical effects discussed in the proposal (88 FR 5640, January 27, 2023) that informed the breakpoints are on the biologically plausible pathway (see 2019 ISA, section 6.1.1 and Figure 6–1) to more severe cardiovascular outcomes, such as ED visits, hospital admissions, and death as depicted in the large number of epidemiologic studies evaluated in the 2019 ISA and ISA Supplement. From a public health perspective, the purpose of the AQI is to inform the public when air quality could adversely affect their health. The scientific evidence informed revisions to the breakpoints at the upper end of the AQI allow it to better reflect the risk of experiencing health effects at higher PM2.5 concentrations. In addition, the EPA disagrees with the commenter that the effects reported at these higher concentrations were observed only in sensitive populations as these effects were also reported in healthy populations (Ghio et al., 2000; Ghio et al., 2003; Urch et al., 2010; Ramanathan et al., 2016; Sivagangabalan et al., 2011; Brook et al., 2009; Bellavia et al. (2013); Tong et al. (2015); Behbod et al. (2013); Vieira et al. (2016a) Vieira et al. (2016b); and Lucking et al. (2011)).
c. Other Comments
The EPA received a few additional comments on elements of the PM2.5 AQI, including the averaging time. Some commenters expressed the view that the 24-hour averaging time was not useful when informing the public how to protect their health, particularly during rapidly changing conditions such as wildfire smoke events. Instead, they suggested a subdaily averaging time of 1–3 hours would be more effective because it more closely aligns with how people breathe.
A few of these commenters suggested that instead of changing the AQI averaging time, which aligns with the short-term standard, the EPA could create a public health warning system for unhealthy PM2.5 levels. The commenters noted that aligning the AQI averaging time with the short-term standard could be useful for consistent communication with the standards and attainment but suggested that a subdaily warning system could better allow the public to take health protective actions.
The EPA disagrees that a shorter averaging period for the PM2.5 AQI sub-index would be better. The health effects evidence supporting a subdaily metric is limited and inconsistent. As part of its review of the health effects evidence, the 2019 ISA evaluated whether a subdaily metric would be more closely related to health effects. Most epidemiologic studies that examined the relationship between short-term PM2.5 exposures and health effects evaluated an exposure metric averaged over 24-hours. Some recent studies, focusing on respiratory and cardiovascular effects and mortality, have examined whether there is evidence that subdaily exposure metrics are more closely related to health effects than a traditional 24-hour average metric. After evaluating this limited newer evidence, the 2019 ISA concluded that “collectively, the available evidence does not indicate that subdaily averaging periods for PM2.5 are more closely associated with health effects than the 24-hour avg exposure metric,” (2019 ISA, chapter 1, section 1.5.2.1, pp. 146–147; U.S. EPA, 2022a).
In addition, there are communication benefits to aligning the averaging time of the AQI with the daily standard, as some of these commenters note, such as providing consistent messages about when it may be beneficial for people to take actions to reduce PM2.5 exposures. Furthermore, with regard to an additional warning system, the EPA is concerned that having two air quality communication systems operating at the same time would likely be confusing to the public and reduce the effectiveness of the systems.
At the same time, the EPA recognizes that when air quality is rapidly changing, such as during wildfire smoke events, reporting information based on a 24-hour metric may not be as useful for the public as reporting more frequently would be. The EPA has balanced concerns about being able to provide timely communication of air quality hazards when conditions are changing quickly with the goal of limiting the number of air quality communications systems and its judgment that the evidence supports a 24-hour-based metric linked to the daily standard by establishing the NowCast, which takes into consideration subdaily PM2.5 concentrations and provides a near real-time AQI value based on the AQI colors and scale. Specifically, the NowCast shows air quality conditions for the most current hour of PM2.5 data available by using a calculation that involves multiple hours of past data. As noted in the AQI Technical Assistance Document, the NowCast currently uses longer averages during periods of stable air quality and shorter averages (down to a 3-hour average) when air quality is changing rapidly, such as during a wildfire (U.S. EPA, 2018a). As discussed further in section IV.D.2 of this notice, the EPA uses the NowCast to approximate the complete daily AQI (24-hour average) during any given hour. This means the subdaily NowCast is approximating a 24-hour average exposure, which aligns with the health evidence and the existing AQI communications network, while also being capable of communicating rapidly changing conditions to the public.
3. Summary of Final Revisions
Upon reviewing and considering the comments on the proposed revisions (summarized above in Section IV.C) along with the scientific evidence outlined in the proposal (88 FR 5639, January 27, 2023) and summarized above in section IV.A, the EPA is finalizing the proposed changes to the AQI.
Thus, as discussed in section IV of the preamble (88 FR 5639, January 27, 2023) to the proposed rule, the EPA is taking final action to revise the AQI value of 50 to 9.0 μg/m3 , 24-hour average, consistent with the final decision on the primary annual PM2.5 standard level as summarized in section II.C of the Start Printed Page 16309 preamble to the final rule; retain the AQI value of 100 at 35 μg/m3 , 24-hour average, consistent with the final decision on the primary 24-hour PM2.5 standard level as summarized in section II.C of the preamble to the final rule; and retain the AQI value of 150 at 55 μg/m3 , 24-hour average. The EPA is also taking action to revise the AQI value of 200 to 125 μg/m3 , 24-hour average; 300 to 225 μg/m3 , 24-hour average; and 500 to 325 μg/m3 , 24-hour average, consistent with the rationale discussed above and the health evidence discussed in section IV of the preamble (88 FR 5639, January 27, 2023) to the proposed rule. The EPA has prepared communications materials to assist States with adjusting to the revised AQI and looks forward to working with, and learning from the experiences of, State, local, and Tribal governments in implementing these changes.
C. Air Quality Index Category Breakpoints for PM10
The EPA proposed to retain the PM10 sub-index of the AQI consistent with the proposed decision to retain the primary PM10 standard, and consistent with the health effects information that supports this proposed decision, as discussed in section III.D of the proposal (88 FR 5632, January 27, 2023). EPA did not receive comments on this and is taking final action to retain the PM10 sub-index of the AQI for the reasons stated in the preamble to the proposed rule (88 FR 5642, January 27, 2023).
D. Air Quality Index Reporting
With respect to the reporting requirements for the AQI and as noted in the proposal (88 FR 5642, January 27, 2023) there have been many technological advances in air quality monitoring and data reporting since the appendix G to 40 CFR part 58 was last revised in 1999. Federal, State, local, and Tribal agencies have used these changes to make health information and air quality data more readily available and easier to access. Given this, it is useful to update the reporting requirements and recommendations to match current practices and ensure the public has the most useful and timely information to take health-protective behaviors.
1. Summary of Proposed Revisions
Currently, appendix G defines daily reporting as five days per week. When this reporting requirement was originated in 1999 the technology available at that time was not sufficient to calculate and report the AQI more than five days per week without requiring additional staffing on the weekends. Since that time, advances in technology have allowed for reporting seven days per week automatically without expending additional resources on weekends. As a result, most State, local, and Tribal air agencies now report the AQI seven days per a week. Given these technological advances and noting that reporting agencies currently report the AQI seven days per week, the EPA proposed that State, local, and Tribal agencies that report the AQI be required to report it seven days a week, ensuring that the members of the public continue to have access to daily air quality and health information that they can use to take steps to protect their health.
Improvements in monitoring networks and modeling capabilities have also enabled the ability to report the AQI in near real-time. This allows State, local, and Tribal air agencies to provide timely air quality information to the public for making health-protective decisions and to help satisfy AQI reporting requirements. The availability of near real-time AQI data also allows for more timely responses by the public when air quality conditions are changing rapidly, such as during wildfire smoke events. Subdaily reporting of the AQI can be critical when there are rapidly change conditions and/or high pollution events so that the public is able to make informed decisions to protect their health. Many State, local, and Tribal air agencies currently report the AQI hourly to ensure that the public has access to accurate and timely information. In recognition of these advances, and to continue to provide for near-real time AQI reporting that the public has come to rely on, the EPA proposed to recommend that State, local, and Tribal agencies report the AQI in near-real time.
In lieu of or along with reporting the near-real-time AQI directly to the public, most State/local and Tribal agencies submit hourly air quality data to the EPA. The EPA and some State, local and Tribal air quality agencies use this near-real-time data to create products for use by the public, weather service providers and the media as discussed in the proposal (88 FR 5643, January 27, 2023). To continue to ensure the availability of the products that the public and many stakeholders rely upon, the EPA proposed to recommend that State, local, and Tribal air quality agencies submit hourly data to the EPA's air quality database. Submitting hourly data to the EPA for use on the AirNow website and in other products also enables State, local, and Tribal air quality agencies to meet the recommendation to report the AQI in near-real-time.
In addition to the proposed updates to the reporting requirements and recommendations for near-real-time reporting and data submission recommendations, the Agency also proposed reformatting the question-and-answer format used in appendix G to align with the current standard formatting used in the Code of Federal Regulations. In proposing to update the format, the EPA did not reopen the language that has merely been moved or rearranged as there are no substantive changes.
Another change the EPA proposed to make to appendix G is with regard to Table 2—Breakpoints for the AQI for purposes of clarity. As discussed in the proposal (88 FR 5642, January 27, 2023) and summarized here, the EPA proposed to collapse the two rows presented for the Hazardous Category into one. The two rows in the current table specify pollutant concentrations for two AQI ranges within the Hazardous category (301–400 and 401–500), with an intermediate break at 400. The 400 breakpoint for all criteria pollutants in the current Table 2 is set at the proportional pollutant concentration approximately halfway between the Index values of 300 and 500. In proposing updated AQI breakpoints for PM2.5, the EPA considered adjusting the 400 breakpoint similarly. However, the EPA concluded that collapsing the two rows into a single range (301–500) would provide a more transparent and easy-to-follow presentation of the pollutant concentrations corresponding to the AQI range for the Hazardous category. Moreover, collapsing the Hazardous category into a single row in Table 2 has no substantive effect on the Emergency Episode program in 40 CFR part 51, appendix L. Thus, the EPA proposed to remove the breakpoint of 400 from the table in appendix G but this change would not substantively affect the derivation of the AQI for any pollutant.
In addition, the EPA proposed to move some information currently in appendix G into the Technical Assistance Document for the Reporting of Daily Air Quality, or TAD (U.S. EPA, 2018a), so that it can be updated in a more timely manner to reflect current scientific and health effects evidence and current communication methods, thereby assisting State, local, and Tribal agencies in providing accurate and timely information to the public. Information that was proposed to be moved from appendix G to the TAD included the definitions of the sensitive (at-risk) populations for each pollutant. Start Printed Page 16310 This definition is typically evaluated and updated, as warranted, in most NAAQS reviews, even if the standard is not revised. Generally, if the standard is not revised in a review of the NAAQS, then appendix G is also not revised. Moving the definitions of sensitive groups to the TAD allows them to be updated even when a NAAQS is not revised to be consistent with the definitions of the sensitive (at-risk) populations identified in the ISA for that NAAQS review. Also, the proposal (88 FR 5642, January 27, 2023) recognized that the ways that air quality and health information is supplied to the news media and public changes regularly and thus proposed that information about suggested approaches for public communication be taken out of appendix G and discussed in the TAD.
2. Summary of Significant Comments on the Proposed Revisions
The EPA received many comments on the proposed changes to AQI reporting, many of which supported the proposed revisions. EPA discusses several of the topics that received the most attention from commenters below. Discussion of other comments received on the proposed changes to the AQI can be found in section IV of the Responses to Significant Comments on the 2023 Proposed Reconsideration of the National Ambient Air Quality Standards for Particulate Matter.
Most commenters expressed support for revising the definition of “daily reporting” from five days a week to seven days a week. A commenter did not support this change and recommended the EPA maintain the definition of daily as five days per week, noting that State and local air agencies do not routinely work seven days per week and would not be available to perform quality control of this data and report it reliably on weekends.
The EPA appreciates the support for this proposed revision and disagrees that the proposed change would require personnel to perform quality control of AQI data on weekends. 40 CFR part 58 Appendix D defines continuous monitoring requirements for agencies participating in the State/Local Air Monitoring Stations (SLAMS) network, and Appendix G states that agencies “ . . . must use concentration data from State/Local Air Monitoring Stations (SLAMS) required by 40 CFR 58.10” when reporting the AQI. Therefore, as noted in Appendix D and G, Agencies are required to report the AQI using monitors within SLAMS, which are not subject to daily quality control/validation.
A few commenters noted that the proposal preamble language mentioned AQI is reported three ways (88 FR 5637, 5638, January 27, 2023): “The AQI is reported three ways all of which are useful and complementary. The daily AQI is reported for the previous day and used to observe trends in community air quality, the AQI forecast helps people plan their outdoor activities for the next day, and the near-real-time AQI, or NowCast AQI, tells people whether it is a good time for outdoor activity.” These commenters suggested that the NowCast is being codified in 40 CFR part 58 Appendix G as a method of calculating the AQI, which they oppose, saying that codifying its use is inappropriate given the shortest averaging period of the PM2.5 NAAQS remains at 24-hours. Some stated that NowCast values have no direct correlation to the AQI calculation methodology codified in 40 CFR part 58 Appendix G. These commenters say that codifying the NowCast would impose a significant burden on States' forecasting staff.
However, some other commenters noted they appreciate the public-friendly format and near real-time data the NowCast provides and use it in their clinical encounters with patients. One air agency recognized the importance of the NowCast near real-time AQI during high pollution events and suggested the EPA should provide more “concrete” health messaging for these short-term spikes.
The EPA disagrees that the preamble language proposed to codify the NowCast or to impose a burden on reporting agencies. The preamble to the proposed rule references the AQI being reported in three ways and it does so because the EPA and many State, local and Tribal air quality agencies already report it these three ways. However, text included in the preamble is generally explanatory and does not alter regulatory provisions. Comments that State that EPA is codifying the NowCast into Appendix G are incorrect. Further, in proposed revisions to 40 CFR part 58 Appendix G, the EPA recommended, but did not propose to require, the use of air quality forecasts and a subdaily AQI. Consistent with the proposal, the EPA is therefore not finalizing any additional requirement or burden on States' forecasting staff relative to forecasts or a subdaily AQI.
The EPA disagrees with the comment that the NowCast values have no direct correlation to the AQI calculation methodology codified in 40 CFR part 58 Appendix G. As noted in the AQI Technical Assistance Document (Technical Assistance Document for the Reporting of Daily Air Quality—the Air Quality Index (AQI)), the NowCast algorithm is based on the AQI methodology but provides more real-time information to the public (U.S. EPA, 2018a). While the NowCast algorithm is approximating a 24-hour average exposure, it can reflect concentrations observed over shorter averaging times when air quality is changing rapidly (U.S. EPA, 2018a). The EPA reflects the nature of the NowCast in the health messaging provided there.
As noted in the above discussion of the AQI, air quality can change quickly during the day. A central purpose of the AQI is to help the public know when it is prudent to take action to reduce their exposure to pollution. Accordingly, the EPA developed the NowCast to estimate the 24-hour AQI for the current hour to give people information and tools to reduce their exposures to protect their health, particularly when air quality may be changing. The NowCast gives people the knowledge and ability to take timely action. They can use this information to reduce their exposure—reducing exposures if PM2.5 is high only during a few hours a day will help reduce a person's 24-hour exposure—or be active when air quality is better.
The first NowCast method was developed in 2003 and was designed so “current conditions” represent the 24-hour PM2.5 standard as closely as possible. This method proved to be slow to respond during rapid air quality changes. In 2013, the EPA developed an updated NowCast method for PM2.5 [141] that responds more quickly to rapidly changing air quality conditions, such as those we see during wildfires, to make air quality alerts more timely. We analyzed millions of data points in developing this NowCast method and presented this information to State, local and Tribal air agencies. The updated NowCast, which is still in use, was launched August 1, 2013, on AirNow.gov. It was designed to represent a shorter average (target 3-hour) when air quality is changing rapidly, in part because 3-hour averages from some continuous monitors are more stable than 1-hour averages. The NowCast reflects a longer-term (12-hour) average when air quality is stable.
After evaluating the 2013 NowCast method, the EPA concluded that it matched the desired characteristics. The NowCast method responds to rapid changes in air quality yet still reflects a Start Printed Page 16311 longer-term average when air quality is stable; will work in any location with adequate air quality data and for any air quality situation; gives people the best possible estimate of a 24-hour exposure; allows the EPA to caution people in time for them to take protective action and reduce their 24-hour exposure; and ensures that AQI maps on AirNow more closely match what people see.
The AQI is designed to allow people to reduce their exposure when pollution levels are higher and be active outdoors when pollution levels are lower. Since air quality almost always changes during the day, that level of granularity is not possible with a 24-hour forecast. If the public has only the 24-hour forecast, they may miss the times to be active outdoors when air quality is better and may be active outdoors when air quality is worse.
Also as noted above, many entities appreciate the near real-time reporting of the AQI that the NowCast provides and suggested more specific messaging is needed. The EPA appreciates this insight and will continue to consider ways to communicate air quality information most effectively to the public. For example, in light of recent wildfire events, the EPA worked with the USFS to pilot the AirNow Fire and Smoke Map.
3. Summary of Final Revisions
Upon reviewing and considering the comments on the proposed revisions (summarized above in Section IV.C) along with the rationale outlined in the proposal (88 FR 5638, January 27, 2023) and summarized above in section IV.C, the EPA is finalizing the proposed changes to the AQI reporting requirements. Thus, as discussed in section IV of the preamble to the proposed rule, the EPA is taking final action to require the AQI be reported seven days a week; recommend that State, local, and Tribal agencies report the AQI in near-real time; recommend that State, local, and Tribal air quality agencies submit hourly data to the EPA's air quality database; reformat appendix G to align with the current standard formatting used in the Code of Federal Regulations; collapse the two rows in Table 2 presented for the Hazardous Category into one by removing the 400 breakpoint; and move some information currently in appendix G into the Technical Assistance Document for the Reporting of Daily Air Quality, or TAD (U.S. EPA, 2018a) such as including the definitions of the sensitive (at-risk) populations for each pollutant and suggested approaches for public communication as stated in the revised Appendix G.
Table 2 below summarizes the breakpoints for the PM2.5 sub-index.
Table 2—Breakpoints for PM 2.5 Sub-Index
AQI category Index values Breakpoints (μg/m3 , 24-hour average) Good 0–50 0.0–9.0 Moderate 51–100 9.1–35.4 Unhealthy for Sensitive Groups 101–150 35.5–55.4 Unhealthy 151–200 55.5–125.4 Very Unhealthy 201–300 125.5–225.4 Hazardous 1 301+ 225.5 1 AQI values between breakpoints are calculated using equation 1 in appendix G. For AQI values in the hazardous category, AQI values greater than 500 should be calculated using equation 1 and the PM 2.5 concentration specified for the AQI value of 500. V. Rationale for Decisions on the Secondary PM Standards
This section presents the rationale for the Administrator's decision that no change to the current secondary PM standards is required at this time to provide requisite protection against the public welfare effects of PM within the scope of this reconsideration ( i.e., visibility, climate, and materials effects).[142] This decision is based on a thorough review of the scientific evidence generally published through December 2017,[143] as presented in the 2019 ISA (U.S. EPA, 2019a), on the non-ecological public welfare effects of PM pertaining to the presence of PM in ambient air, specifically visibility, climate, and materials effects. Additionally, this decision is based on a thorough evaluation of some studies that became available after the literature cutoff date of the 2019 ISA that could either further inform the adequacy of the current PM NAAQS or address key scientific topics that have evolved since the literature cutoff date for the 2019 ISA, generally through March 2021, as presented in the ISA Supplement [144] (U.S. EPA, 2022a). The selection of welfare effects evaluated within the ISA Supplement was based on the causality determinations reported in the 2019 ISA and the subsequent use of scientific evidence in the 2020 PA. 145 Start Printed Page 16312 Specifically, for welfare effects, the focus within the ISA Supplement is on visibility effects. The ISA Supplement does not include an evaluation of studies on climate or materials effects. The Administrator's decision also takes into account the 2022 PA evaluation of the policy-relevant information in the 2019 ISA and ISA Supplement and presentation of quantitative analysis of air quality related to visibility impairment; CASAC advice and recommendations, as reflected in discussions of the drafts of the ISA Supplement and 2022 PA at public meetings and in the CASAC's letters to the Administrator; and public comments received on the proposal.
In presenting the rationale for the Administrator's final decision and its foundations, section V.A provides background on the 2020 final decision to retain the secondary PM standards (section V.A.1), and also provides brief summaries of key aspects of the currently available welfare effects evidence (section V.A.2) and quantitative information (section V.A.3). Section V.B summarizes the CASAC's advice (section V.B.1) and the proposed conclusions (section V.B.2), addresses public comments received on the proposal (section V.B.3), and presents the Administrator's conclusions on the adequacy of the current standards (section V.B.4), drawing on consideration of the available scientific and quantitative information, advice from the CASAC, and comments from the public. Section V.C summarizes the Administrator's decision on the secondary PM standards.
A. Introduction
The general approach for this reconsideration of the 2020 final decision on the secondary PM standards relies on the EPA's assessments of the current scientific evidence and associated quantitative analyses to inform the Administrator's judgments regarding secondary standards that are requisite to protect the public welfare from known or anticipated adverse effects associated with the pollutant's presence in the ambient air. The EPA's assessments are primarily documented in the 2019 ISA, ISA Supplement, and 2022 PA, which builds on the 2020 PA, all of which have received CASAC review and public comment (83 FR 53471, October 23, 2018; 83 FR 55529, November 6, 2018; 85 FR 4655, January 27, 2020; 86 FR 52673, September 22, 2021; 86 FR 54186, September 30, 2021; 86 FR 56263, October 8, 2021; 87 FR 958, January 7, 2022; 87 FR 22207, April 14, 2022; 87 FR 31965, May 26, 2022). In bridging the gap between the scientific assessments of the 2019 ISA and ISA Supplement and the judgments required of the Administrator in determining whether the current standards provide the requisite public welfare protection, the 2022 PA evaluates policy implications of the evaluation of the current evidence in the 2019 ISA and ISA Supplement, and the quantitative information documented in the 2022 PA. In evaluating the public welfare protection afforded by the current standards against PM-related effects within the scope of this reconsideration, the four basic elements of the NAAQS (indicator, averaging time, level, and form) are considered collectively.
The final decision on the adequacy of the current secondary standards is a public welfare policy judgment to be made by the Administrator. In reaching conclusions with regard to the standard, the decision draws on the scientific information and analyses about welfare effects, and associated public welfare significance, as well as judgments about how to consider the range and magnitude of uncertainties that are inherent in the scientific evidence and analyses. This approach is based on the recognition that the available evidence generally reflects a continuum that includes ambient air exposures at which scientists agree that effects are likely to occur through lower levels at which the likelihood and magnitude of responses become increasingly uncertain. This approach is consistent with the requirements of the provisions of the Clean Air Act related to the review of NAAQS and with how the EPA and the courts have historically interpreted the Act. These provisions require the Administrator to establish secondary standards that, in the judgment of the Administrator, are requisite to protect public welfare from known or anticipated adverse effects associated with the presence of the pollutant in the ambient air. In so doing, the Administrator seeks to establish standards that are neither more nor less stringent than necessary for this purpose. The Act does not require that standards be set at a zero-risk level, but rather at a level that reduces risk sufficiently so as to protect the public welfare from known or anticipated adverse effects.
1. Background on the Current Standards
The current secondary PM standards were retained in 2020 based on the scientific and technical information available at that time, as well as the then-Administrator's judgments regarding the available welfare effects evidence, the appropriate degree of public welfare protection for the existing standards, and available air quality information on visibility impairment that may be allowed by such a standard (85 FR 82684, December 18, 2020). With the 2020 decision, the then-Administrator retained the secondary 24-hour PM2.5 standard, with its level of 35 µg/m3 , the annual PM2.5 standard, with its level of 15.0 µg/m3 , and the 24-hour PM10 standard, with its level of 150 µg/m3 . The subsections below focus on the key considerations and the then-Administrator's conclusions in the 2020 final decision for climate and materials effects (section V.A.1.a) and visibility effects (section V.A.2.b).
a. Non-Visibility Effects
In light of the robust evidence base, the 2019 ISA concluded there to be causal relationships between PM and climate effects and materials effects (U.S. EPA, 2019a, sections 13.3.9 and 13.4.2). The 2020 final decision was based on a thorough review in the 2019 ISA of the scientific information on PM-induced climate and materials effects. The decision also took into account: (1) Assessments in the 2020 PA of the most policy-relevant information in the 2019 ISA regarding evidence of adverse effects of PM to climate and materials, (2) uncertainties in the available evidence to inform a quantitative assessment of PM-related climate and materials effects, (3) CASAC advice and recommendations, and (4) public comments received during the development of these documents and on the proposal document.
In considering non-visibility welfare effects in the 2020 decision, the then-Administrator concluded that, while it is important to maintain an appropriate degree of control of fine and coarse particles to address non-visibility welfare effects, “it is generally appropriate to retain the existing standards and that there is insufficient information to establish any distinct secondary PM standards to address climate and materials effects of PM” (85 FR 82744, December 18, 2020).
With regard to climate, the then-Administrator recognized that there were a number of improvements and refinements to climate models since the 2012 review. However, while the evidence continued to support a causal relationship between PM and climate effects, the then-Administrator noted that significant limitations continued to exist related to quantifying the contributions of direct and indirect Start Printed Page 16313 effects of PM and PM components on climate forcing (U.S. EPA, 2020b, sections 5.2.2.1.1 and 5.4). He also recognized that the models continued to exhibit considerable variability in estimates of PM-related climate impacts at regional scales ( e.g., ~100 km) as compared to simulations at global scales. Therefore, the resulting uncertainty led the then-Administrator to conclude in the 2020 decision that the available scientific information remained insufficient to quantify climate impacts associated with particular concentrations of PM in ambient air (U.S. EPA, 2020b, section 5.2.2.2.1) or to evaluate or consider a level of PM air quality in the U.S. to protect against climate effects and that there was insufficient information available to base a national ambient standard on climate impacts (85 FR 82744, December 18, 2020).
With regard to materials effects, the then-Administrator noted that the evidence available in the 2019 ISA continued to support a causal relationship between materials effects and PM deposition (U.S. EPA, 2019a, section 13.4). He recognized that the deposition of fine and coarse particles to materials can lead to physical damage and/or impaired aesthetic qualities. Particles can contribute to materials damage by adding to the natural weathering processes and by promoting the corrosion of metals, the degradation of building materials, and the weakening of material components. While some new information was available in the 2019 ISA, the information was from studies primarily conducted outside of the U.S. in areas where PM concentrations in ambient air are higher than those observed in the U.S. (U.S. EPA, 2020b, section 13.4). Additionally, the information assessed in the 2019 ISA did not support quantitative analyses of PM-related materials effects in the 2020 PA (U.S. EPA, 2020b, section 5.2.2.2.2). Given the limited amount of information available and its inherent uncertainties and limitations, the Administrator concluded that he was unable to relate soiling or damage to specific levels of PM in ambient air or to evaluate or consider a level of air quality to protect against such materials effects, and that there was insufficient information available to support a distinct national ambient standard based on materials effects (85 FR 82744, December 18, 2020).
In reviewing the 2019 draft PA, the CASAC agreed with staff conclusions that, while these effects are important, “the available evidence does not call into question the protection afforded by the current secondary PM standards” and recommended that the secondary standards “should be retained” (Cox, 2019b, p. 3 of letter). In reaching a final decision in 2020, for all of the reasons discussed above and recognizing the CASAC conclusion that the evidence provided support for retaining the current secondary PM standards, the then-Administrator concluded that it was appropriate to retain the existing secondary PM standards, without revision. For climate and materials effects, this conclusion reflected his judgment that, although it remains important to maintain secondary PM2.5 and PM10 standards to provide some degree of control over long- and short-term concentrations of both fine and coarse particles, there was insufficient information to establish distinct secondary PM standards to address non-visibility PM-related welfare effects (85 FR 82744, December 18, 2020).
b. Visibility Effects
The 2019 ISA concluded that, “the evidence is sufficient to conclude that a causal relationship exists between PM and visibility impairment” (U.S. EPA, 2019a, section 13.2.6). The 2020 decision on the adequacy of the secondary standards with regard to visibility effects was a public welfare policy judgment made by the then-Administrator, which drew upon the available scientific evidence for PM-related visibility effects and on analyses of visibility impairment, as well as judgments about the appropriate weight to place on the range of uncertainties inherent in the evidence and analyses. The 2020 final decision was based on a thorough review in the 2019 ISA of the scientific information on PM-related visibility effects. The decision also took into account: (1) Assessments in the 2020 PA of the most policy-relevant information in the 2019 ISA regarding evidence of adverse effects of PM on visibility; (2) air quality analyses of the PM2.5 visibility index and design values based on the form and averaging time of the existing secondary 24-hour PM2.5 standard; (3) CASAC advice and recommendations; and (4) public comments received during the development of these documents and on the 2020 proposal document.
In considering the visibility effects in the 2020 review, the then-Administrator noted the long-standing body of evidence for PM-related visibility impairment. This evidence, which is based on the fundamental relationship between light extinction and PM mass, demonstrated that ambient PM can impair visibility in both urban and remote areas, and had changed very little since the 2012 review (U.S. EPA, 2019a, section 13.1; U.S. EPA, 2009a, section 9.2.5). The evidence related to public perception of visibility impairment was from studies from four areas in North America.[146] These studies provided information to inform our understanding of levels of visibility impairment that the public judged to be “acceptable” (U.S. EPA, 2010b; 85 FR 24131, April 30, 2020). In considering these public preference studies, the then-Administrator noted that no new visibility studies conducted in the U.S. were discussed in the 2019 ISA, and there was little newly available information with regard to acceptable levels of visibility impairment in the U.S. The Administrator recognized that visibility impairment can have implications for people's enjoyment of daily activities and their overall well-being, and therefore, considered the degree to which the current secondary standards protect against PM-related visibility impairment.
Consistent with the 2012 review, in the 2020 review, the then-Administrator first concluded that a target level of protection for a secondary PM standard is most appropriately defined in terms of a visibility index that directly takes into account the factors ( i.e., species composition and relative humidity) that influence the relationship between PM2.5 in ambient air and PM-related visibility impairment. In defining a target level of protection, the then-Administrator considered the specific aspects of such an index, including the appropriate indicator, averaging time, form and level (78 FR 82742–82744, December 18, 2020).
First, with regard to indicator, the then-Administrator noted that in the 2012 review, the EPA used an index based on estimates of light extinction by PM2.5 components calculated using an adjusted version of the IMPROVE algorithm, which allows the estimation of the light extinction using routinely monitored components of PM2.5, PM10–2.5 mass, and estimates of relative humidity. The then-Administrator recognized that, while there have been some revisions to the IMPROVE algorithm since the time of the 2012 Start Printed Page 16314 review, our fundamental understanding of the relationship between PM in ambient air and light extinction had changed little and the various IMPROVE algorithms appropriately reflected this relationship across the U.S. In the absence of a monitoring network for direct measurement of light extinction, he concluded that a calculated light extinction indicator that utilizes the IMPROVE algorithms continued to provide a reasonable basis for defining a target level of protection against PM-related visibility impairment (78 FR 82742–82744, December 18, 2020).
In further defining the characteristics of a visibility index, the then-Administrator next considered the appropriate averaging time, form, and level of the index. Given the available scientific information the review, and in considering the CASAC's advice and public comments, the then-Administrator concluded that, consistent with the decision in the 2012 review, a visibility index with a 24-hour averaging time and a form based on the 3-year average of annual 90th percentile values remained reasonable. With regard to the averaging time and form of such an index, the Administrator noted analyses conducted in the last review that demonstrated relatively strong correlations between 24-hour and subdaily ( i.e., 4-hour average) PM2.5 light extinction (78 FR 3226, January 15, 2013), indicating that a 24-hour averaging time is an appropriate surrogate for the subdaily time periods of the perception of PM-related visibility impairment and the relevant exposure periods for segments of the viewing public. This decision in the 2020 review also recognized that a 24-hour averaging time may be less influenced by atypical conditions and/or atypical instrument performance (78 FR 3226, January 15, 2013). The then-Administrator recognized that there was no new information to support updated analyses of this nature, and therefore, he believed these analyses continued to provide support for consideration of a 24-hour averaging time for a visibility index in this review. With regard to the statistical form of the index, the Administrator noted that, consistent with the 2012 review: (1) A multi-year percentile form offers greater stability from the occasional effect of interannual meteorological variability (78 FR 3198, January 15, 2013; U.S. EPA, 2011, p. 4–58); (2) a 90th percentile represents the median of the distribution of the 20 percent worst visibility days, which are targeted in Federal Class I areas by the Regional Haze Program; and (3) public preference studies did not provide information to identify a different target than that identified for Federal Class I areas (U.S. EPA, 2011, p. 4–59). Therefore, the then-Administrator judged that a visibility index based on estimates of light extinction, with a 24-hour averaging time and a 90th percentile form, averaged over three years, remained appropriate (78 FR 82742–82744, December 18, 2020).
With regard to the level of a visibility index, consistent with the 2012 review, the then-Administrator judged that it was appropriate to establish a target level of protection of 30 deciviews (dv),[147 148] reflecting the upper end of the range of visibility impairment judged to be acceptable by at least 50% of study participants in the available public preference studies (78 FR 3226, January 15, 2013). The 2011 PA identified a range of levels from 20 to 30 dv based on the responses in the public preference studies available at that time (U.S. EPA, 2011, section 4.3.4). At the time of the 2012 review, the then-Administrator noted a number of uncertainties and limitations in public preference studies, including the small number of stated preference studies available, the relatively small number of study participants, the extent to which the study participants may not be representative of the broader study area population in some of the studies, and the variations in the specific materials and methods used in each study. In considering the available preference studies in 2012, with their inherent uncertainties and limitations, the then-Administrator concluded that the substantial degree of variability and uncertainty in the public preference studies should be reflected in a target level of protection based on the upper end of the range of candidate protection levels (CPLs).
Given that there were no new preference studies in the 2019 ISA, the then-Administrator's judgments in 2020 were based on the same studies, with the same range of levels, available in the 2012 review. The 2020 PA (U.S. EPA, 2020b, section 5.5), discussed a number of limitations and uncertainties associated with these studies. In considering the scientific information, with its uncertainties and limitations, as well as public comments on the level of the target level of protection against visibility impairment, the then-Administrator concluded that it was appropriate to again use a level of 30 dv for the visibility index (78 FR 82742–82744, December 18, 2020).
Having concluded that the protection provided by a standard defined in terms of a PM2.5 visibility index, with a 24-hour averaging time, and a 90th percentile form, averaged over 3 years, set at a level of 30 dv, was requisite to protect public welfare with regard to visual air quality, the Administrator next considered the degree of protection from visibility impairment afforded by the existing suite of secondary PM standards.
In this context, the then-Administrator considered the updated analyses of visibility impairment presented in the 2020 PA (U.S. EPA, 2020b, section 5.2.1.2), which reflected a number of improvements since the 2012 review. Specifically, the updated analyses examined multiple versions of the IMPROVE equation, including the version incorporating revisions since the time of the 2012 review. These updated analyses provided a further understanding of how variation in the inputs to the algorithms affect the estimates of light extinction (U.S. EPA, 2020b, Appendix D). Additionally, for a subset of monitoring sites with available PM10–2.5 data, the updated analyses better characterized the influence of coarse PM on light extinction than in the 2012 review (U.S. EPA, 2020b, section 5.2.1.2).
The results of the updated analyses in the 2020 PA were consistent with those from the 2012 review. Regardless of which version of the IMPROVE equation was used, the analyses demonstrated that, based on 2015–2017 data, the 3-year visibility metric was at or below about 30 dv in all areas meeting the current 24-hour PM2.5 standard, and below 25 dv in most of those areas. In locations with available PM10–2.5 monitoring, which met both the current 24-hour secondary PM2.5 and PM10 standards, 3-year visibility index metrics were at or below 30 dv regardless of whether the coarse fraction was included as an input to the algorithm for estimating light extinction (U.S. EPA, 2020b, section 5.2.1.2). While the inclusion of the coarse fraction had a relatively modest impact on the estimates of light extinction, the then-Administrator recognized the continued importance of the PM10 standard given the potential for larger impacts on light extinction in areas with higher coarse particle concentrations, which were not included in the analyses in the 2020 PA due to a lack of available data (U.S. EPA, 2019a, section 13.2.4.1; U.S. EPA, 2020b, section 5.2.1.2). He Start Printed Page 16315 noted that the air quality analyses showed that all areas meeting the existing 24-hour PM2.5 standard, with its level of 35 µg/m3 , had visual air quality at least as good as 30 dv, based on the visibility index. Thus, the secondary 24-hour PM2.5 standard would likely be controlling relative to a 24-hour visibility index set at a level of 30 dv. Additionally, areas would be unlikely to exceed the target level of protection for visibility of 30 dv without also exceeding the existing secondary 24-hour PM2.5 standard. Thus, the then-Administrator judged that the 24-hour PM2.5 standard provided sufficient protection in all areas against the effects of visibility impairment, i.e., that the existing 24-hour PM2.5 standard would provide at least the target level of protection for visual air quality of 30 dv which he judged appropriate (78 FR 82742–82744, December 18, 2020).
2. Overview of Welfare Effects Evidence
The information summarized here is based on the scientific assessment of the welfare effects evidence available in this reconsideration; this assessment is documented in the 2019 ISA and ISA Supplement and its policy implications are further discussed in the 2022 PA. While the 2019 ISA provides the broad scientific foundation for this reconsideration, additional literature has become available since the cutoff date of the 2019 ISA that expands the body of evidence related to visibility effects that can inform the Administrator's judgment on the adequacy of the current secondary PM standards. As such, the ISA Supplement builds on the information in the 2019 ISA with a targeted identification and evaluation of new scientific information regarding visibility effects. As described in the ISA Supplement and the 2022 PA, the selection of welfare effects to evaluate within the ISA Supplement were based on the causality determinations reported in the 2019 ISA and the subsequent use of scientific evidence in the 2020 PA (U.S. EPA, 2019a, section 1.2; U.S. EPA, 2022a, section 1.4.2). The ISA Supplement focuses on U.S. and Canadian studies that provide new information on public preferences for visibility impairment and/or developed new methodologies or conducted quantitative analyses of light extinction (U.S. EPA, 2022a, section 1.2). Such studies of visibility effects and quantitative relationships between visibility impairment and PM in ambient air were considered to be of greatest utility in informing the Administrator's conclusions on the adequacy of the current secondary PM standards. The visibility effects evidence presented within the 2019 ISA, along with the targeted identification and evaluation of new scientific information in the ISA Supplement, provides the scientific basis for the reconsideration of the 2020 final decision on the secondary PM standards for visibility effects. For climate and materials effects, the 2020 PA concluded that there were substantial uncertainties associated with the quantitative relationships with PM concentrations and the concentration patterns that limited the ability to quantitatively assess the public welfare protection provided by the standards from these effects. Therefore, the evaluation of the information related to these effects draws heavily from the 2019 ISA and 2020 PA. The subsections below briefly summarize the nature of PM-related visibility (section V.B.1.a), climate (section V.B.1.b), and materials (section V.B.1.c) effects.
a. Nature of Effects
Visibility impairment can have implications for people's enjoyment of daily activities and for their overall sense of well-being (U.S. EPA, 2009a, section 9.2). The strongest evidence for PM-related visibility impairment comes from the fundamental relationship between light extinction and PM mass (U.S. EPA, 2009a), which confirms a well-established “causal relationship exists between PM and visibility impairment” (U.S. EPA, 2009a, p. 2–28). Beyond its effects on visibility, the 2009 ISA also identified a causal relationship “between PM and climate effects, including both direct effects of radiative forcing and indirect effects that involve cloud and feedbacks that influence precipitation formation and cloud lifetimes” (U.S. EPA, 2009a, p. 2–29). The evidence also supports a causal relationship between PM and effects on materials, including soiling effects and materials damage (U.S. EPA, 2009a, p. 2–31).
The evidence available in this reconsideration is consistent with the evidence available at the time of the 2012 and 2020 reviews and supports the conclusions of causal relationships between PM and visibility, climate, and materials effects (U.S. EPA, 2019a, chapter 13). Evidence newly available in this reconsideration augments the previously available evidence of the relationship between PM and visibility impairment (U.S. EPA, 2019a, section 13.2; U.S. EPA, 2022a, section 4), climate effects (U.S. EPA, 2019a, section 13.3), and materials effects (U.S. EPA, 2019a, section 13.4).
i. Visibility
The fundamental relationship between light extinction and PM mass, and the EPA's understanding of this relationship, has changed little since the 2009 ISA (U.S. EPA, 2009a). The combined effect of light scattering and absorption by particles and gases is characterized as light extinction, i.e., the fraction of light that is scattered or absorbed per unit of distance in the atmosphere.[149] Light extinction is measured in units of 1/distance, which is often expressed in the technical literature as visibility per megameter (abbreviated Mm−1). Higher values of light extinction (usually given in units of Mm−1 or dv) correspond to lower visibility. When PM is present in the air, its contribution to light extinction is typically much greater than that of gases (U.S. EPA, 2019a, section 13.2.1). The impact of PM on light scattering depends on particle size and composition, as well as relative humidity. All particles scatter light, as described by the Mie theory, which relates light scattering to particle size, shape, and index of refraction (U.S. EPA, 2019a, section 13.2.3; Mie, 1908, Van de Hulst, 1981). Fine particles scatter more light than coarse particles on a per unit mass basis and include sulfates, nitrates, organics, light-absorbing carbon, and soil (Malm et al., 1994). Hygroscopic particles like ammonium sulfate, ammonium nitrate, and sea salt increase in size as relative humidity increases, leading to increased light scattering (U.S. EPA, 2019a, section 13.2.3).
As at the time of the 2012 and 2020 reviews, direct measurements of PM light extinction, scattering, and absorption continue to be considered more accurate for quantifying visibility than PM mass-based estimates because measurements do not depend on assumptions about particle characteristics ( e.g., size, shape, density, component mixture, etc.) (U.S. EPA, 2019a, section 13.2.2.2). Measurements of light extinction can be made with high time resolution, allowing for characterization of subdaily temporal patterns of visibility impairment. A number of measurement methods have been used for visibility impairment ( e.g.,Start Printed Page 16316 transmissometers, integrating nephelometers, teleradiometers, telephotometers, and photography and photographic modeling), although each of these methods has its own strengths and limitations (U.S. EPA, 2019a, Table 13–1). While some recent research confirms and adds to the body of knowledge regarding direct measurements as is described in the 2019 ISA and ISA Supplement, no major new developments have been made with these measurement methods since prior reviews (U.S. EPA, 2019a, section 13.2.2.2; U.S. EPA, 2022a, section 4.2).
In the absence of a robust monitoring network for the routine measurement of light extinction across the U.S., estimation of light extinction based on existing PM monitoring can be used. The theoretical relationship between light extinction and PM characteristics, as derived from Mie theory (U.S. EPA, 2019a, Equation 13.5), can be used to estimate light extinction by combining mass scattering efficiencies of particles with particle concentrations (U.S. EPA, 2019a, section 13.2.3; U.S. EPA, 2009a, sections 9.2.2.2 and 9.2.3.1). This estimation of light extinction is consistent with the method used in previous reviews. The algorithm used to estimate light extinction, known as the IMPROVE algorithm,[150] provides for the estimation of light extinction (bext ), in units of Mm-1 , using routinely monitored components of fine (PM2.5) and coarse (PM10–2.5) PM. Relative humidity data are also needed to estimate the contribution by liquid water that is in solution with the hygroscopic components of PM. To estimate each component's contribution to light extinction, their concentrations are multiplied by extinction coefficients and are additionally multiplied by a water growth factor that accounts for their expansion with moisture. Both the extinction efficiency coefficients and water growth factors of the IMPROVE algorithm have been developed by a combination of empirical assessment and theoretical calculation using particle size distributions associated with each of the major aerosol components (U.S. EPA, 2019a, sections 13.2.3.1 and 13.2.3.3).
At the time of the 2012 review, two versions of the IMPROVE algorithm were available in the literature—the original IMPROVE algorithm (Lowenthal and Kumar, 2004, Malm and Hand, 2007, Ryan et al., 2005) and the revised IMPROVE algorithm (Pitchford et al., 2007). As described in detail in the 2022 PA (U.S. EPA, 2022b, section 5.3.1.1) and the 2019 ISA (U.S. EPA, 2019a, section 13.2.3), the algorithm has been further evaluated and refined since the time of the 2012 review (Lowenthal and Kumar, 2016), particularly for PM characteristics and relative humidity in remote areas. All three versions of the IMPROVE algorithm were considered in evaluating visibility impairment in this reconsideration.
Consistent with the evidence available at the time of the 2012 and 2020 reviews, our understanding of public perception of visibility impairment comes from visibility preference studies conducted in four areas in North America.[151] The detailed methodology for these studies are described in the 2022 PA (U.S. EPA, 2022b, section 5.3.1.1), the 2019 ISA (U.S. EPA, 2019a), and the 2009 ISA (U.S. EPA, 2019a). In summary, the study participants were queried regarding multiple images that were either photographs of the same location and scenery that had been taken on different days on which measured extinction data were available or digitized photographs onto which a uniform “haze” had been superimposed. Results of the studies indicated a wide range of judgments on what study participants considered to be acceptable visibility across the different study areas, depending on the setting depicted in each photograph. Based on the results of the four cities, a range encompassing the PM2.5 visibility index values from images that were judged to be acceptable by at least 50 percent of study participants across all four of the urban preference studies was identified (U.S. EPA, 2010b, p. 4–24; U.S. EPA, 2020b, Figure 5–2). Much lower visibility (considerably more haze resulting in higher values of light extinction) was considered acceptable in Washington, DC, than was in Denver, and 30 dv reflected the level of impairment that was determined to be “acceptable” by at least 50 percent of study participants (78 FR 3226–3227, January 15, 2013).
Since the completion of the 2009 and 2019 ISAs, there has been only one public preference study that has become available in the U.S. This study uses images of the Grand Canyon, AZ, described in the ISA Supplement (U.S. EPA, 2022a). The Grand Canyon study, conducted by Malm et al. (2019), has a similar study design to that used in the public preference studies discussed above; however, there are several important differences that make it difficult to directly compare the results of the Malm et al. (2019) study with other public preference studies. As an initial matter, the Grand Canyon study was conducted in a Federal Class I area, as opposed to in an urban area, with a scene depicted in the photographs that did not include urban features.[152] We recognize that public preferences with respect to visibility in Federal Class 1 areas may well differ from visibility preferences in urban areas and other contexts, although there is currently a lack of information to on such questions. Further, the Malm et al. (2019) study also used a much lower range of superimposed “haze” than the preference studies discussed above.[153] It is unclear whether the participant preferences are a function in part of the range of potential values presented, such that the participant preferences for the Grand Canyon were generally lower [154] than the other preference studies in part because of the lower range of superimposed “haze” for the images in that study, or if their preferences would vary if presented with images with a range of superimposed “haze” more comparable to the levels used in the other studies ( i.e., more “haze” superimposed on the images).
The Malm et al. (2019) study also explored alternate methods for evaluating “acceptable” levels of visual air quality from the preference studies, including the use of scene-specific visibility indices as potential indicators of visibility levels as perceived by the observer (Malm et al., 2019). In addition to measures of atmospheric haze, such Start Printed Page 16317 as atmospheric extinction, used in previously available preference studies, other indices for visual air quality include color and achromatic contrast of single landscape figures, average and equivalent contrast of an entire scene, edge detection algorithms such as the Sobel index, and just-noticeable difference or change indexes. The results reported by Malm et al. (2019) suggest that scene-dependent metrics, such as contrast, may be useful alternate predictors of preference levels compared to universal metrics like light extinction (U.S. EPA, 2022a, section 4.2.1). This is because extinction alone is not a measure of “haze,” but of light attenuation per unit distance, and visible “haze” is dependent on both light extinction and distance to a landscape feature (U.S. EPA, 2022a, section 4.2.1). However, there are very few studies available that use scene-dependent metrics ( i.e., contrast) to evaluate public preference information, which makes it difficult to evaluate them as an alternative to the light extinction approach.
ii. Climate
The available evidence continues to support the conclusion of a causal relationship between PM and climate effects (U.S. EPA, 2019a, section 13.3.9). Since the 2012 review, climate impacts have been extensively studied and recent research reinforces and strengthens the evidence evaluated in the 2009 ISA. Recent evidence provides greater specificity about the details of radiative forcing effects [155] and increases the understanding of additional climate impacts driven by PM radiative effects. The Intergovernmental Panel on Climate Change (IPCC) assesses the role of anthropogenic activity in past and future climate change, and since the completion of the 2009 ISA, has issued the Fifth IPCC Assessment Report (AR5; IPCC, 2013), which summarizes any key scientific advances in understanding the climate effects of PM since the previous report. As in the 2009 ISA, the 2019 ISA draws substantially on the IPCC report to summarize climate effects. As discussed in more detail in the 2022 PA (U.S. EPA, 2022b, section 5.3.2.1.1), the general conclusions are similar between the IPCC AR4 and AR5 reports with regard to effects of PM on global climate. Consistent with the evidence available in the 2012 review, the key components, including sulfate, nitrate, organic carbon (OC), black carbon (BC), and dust, that contribute to climate processes vary in their reflectivity, forcing efficiencies, and direction of forcing. Since the completion of the 2009 ISA, the evidence base has expanded with respect to the mechanisms of climate responses and feedbacks to PM radiative forcing; however, the recently published literature assessed in the 2019 ISA does not reduce the considerable uncertainties that continue to exist related these mechanisms.
As described in the proposal (88 FR 5650, January 27, 2023), PM has a very heterogeneous distribution globally and patterns of forcing tend to correlate with PM loading, with the greatest forcings centralized over continental regions. The climate response to this PM forcing, however, is more complicated since the perturbation to one climate variable ( e.g., temperature, cloud cover, precipitation) can lead to a cascade of effects on other variables. While the initial PM radiative forcing may be concentrated regionally, the eventual climate response can be much broader spatially or be concentrated in remote regions, and may be quite complex, affecting multiple climate variables with possible differences in the direction of the forcing in different regions or for different variables (U.S. EPA, 2019a, section 13.3.6). The complex climate system interactions lead to variation among climate models, which have suggested a range of factors that can influence large-scale meteorological processes and may affect temperature, including local feedback effects involving soil moisture and cloud cover, changes in the hygroscopicity of the PM, and interactions with clouds (U.S. EPA, 2019a, section 13.3.7). As a result, there remains insufficient evidence to related climate effects to specific PM levels in ambient air or to establish a quantitative relationship between PM and climate effects, particularly at a regional scale. Further research is needed to better characterize the effects of PM on regional climate in the U.S. before PM climate effects can be quantified.
iii. Materials
Consistent with the evidence assessed in the 2009 ISA, the available evidence continues to support the conclusion that there is a causal relationship between PM deposition and materials effects. Effects of deposited PM, particularly sulfates and nitrates, to materials include both physical damage and impaired aesthetic qualities, generally involving soiling and/or corrosion (U.S. EPA, 2019a, section 13.4.2). Because of their electrolytic, hygroscopic, and acidic properties and their ability to sorb corrosive gases, particles contribute to materials damage by adding to the effects of natural weathering processes, by potentially promoting or accelerating the corrosion of metals, degradation of painted surfaces, deterioration of building materials, and weakening of material components.[156] There is a limited amount of recently available data for consideration in this review from studies primarily conducted outside of the U.S. on buildings and other items of cultural heritage. However, these studies involved concentrations of PM in ambient air greater than those typically observed in the U.S. (U.S. EPA, 2019a, section 13.4).
Building on the evidence available in the 2009 ISA, and as described in detail in the proposal (88 FR 5650, January 27, 2023) and in the 2019 ISA (U.S. EPA, 2019a, section 13.4), research has progressed on (1) the theoretical understanding of soiling of items of cultural heritage; (2) the quantification of degradation rates and further characterization of factors that influence damage of stone materials; (3) materials damage from PM components besides sulfate and black carbon and atmospheric gases besides SO2; (4) methods for evaluating soiling of materials by PM mixtures; (5) PM-attributable damage to other materials, including glass and photovoltaic panels; (6) development of dose-response relationships for soiling of building materials; and (7) damage functions to quantify material decay as a function of pollutant type and load. While the evidence of PM-related materials effects has expanded somewhat since the completion of the 2009 ISA, there remains insufficient evidence to relate soiling or damage to specific PM levels in ambient air or to establish a quantitative relationship between PM and materials degradation. The recent evidence assessed in the 2019 ISA is generally similar to the evidence available in the 2009 ISA, including Start Printed Page 16318 associated limitations and uncertainties and a lack of evidence to inform quantitative relationships between PM and materials effects, therefore leading to similar conclusions about the PM-related effects on materials.
3. Summary of Air Quality and Quantitative Information
Beyond the consideration of the scientific evidence, as discussed in section V.A.2 above, quantitative analyses of PM air quality, when available, can also inform conclusions on the adequacy of the public welfare protection provided by the current secondary PM standards.
a. Visibility Effects
In the 2012 and 2020 reviews, quantitative analyses for PM-related visibility effects focused on daily visibility impairment, given the short-term nature of PM-related visibility effects. The evidence and information available in this reconsideration continues to provide support for the short-term ( i.e., hourly or daily) nature of PM-related visibility impairment. As such, the quantitative analyses presented in the 2022 PA continue to focus on daily visibility impairment and utilize a two-phase assessment approach for visibility impairment, consistent with the approaches taken in past reviews. First, the 2022 PA considers the appropriateness of the elements (indicator, averaging time, form, and level) of the visibility index for providing protection against PM-related visibility effects. Second, recent air quality was used to evaluate the relationship between the current secondary 24-hour PM2.5 standard and the visibility index. The information available since the 2012 review includes an updated equation for estimating light extinction, summarized in the 2022 PA (U.S. EPA, 2022b, section 5.3.1.1) and described in the 2019 ISA (U.S. EPA, 2019a, section 13.2.3.3), as well as more recent air monitoring data, that together allow for development of an updated assessment of PM-related visibility impairment in study locations in the U.S.
i. Target Level of Protection in Terms of a PM2.5 Visibility Index
In evaluating the adequacy of the current secondary PM standards, the 2022 PA first evaluates the appropriateness of the elements (indicator, averaging time, form, and level) identified for a visibility index to protect against visibility effects. In previous reviews, the visibility index as set at a level of 30 dv, with estimated light extinction as the indicator, a 24-hour averaging time, and a 90th percentile form, averaged over three years.
With regard to an indicator for the visibility index, the 2022 PA recognizes the lack of availability of methods and an established network for directly measuring light extinction (U.S. EPA, 2022b, section 5.3.1.1). Therefore, consistent with previous reviews, the 2022 PA concludes that a visibility index based on estimates of light extinction by PM2.5 components derived from an adjusted version of the original IMPROVE algorithm to be the most appropriate indicator for the visibility index in this reconsideration. As described in section 5.3.1.1 of the 2022 PA, the IMPROVE algorithm estimates light extinction using routinely monitored components of PM2.5 and PM10–2.5, along with estimates of relative humidity (U.S. EPA, 2022b, section 5.3.1.1).
With regard to averaging time, the 2022 PA notes that the evidence continues to provide support for the short-term nature of PM-related visibility effects. Given that there is no new information available regarding the time periods during which visibility impairment occurs or public preferences related to specific time periods for visibility impairment, the 2022 PA concludes that it is appropriate to continue to focus on daily visibility impairment. In so doing, the 2022 PA relies on analyses that were conducted in the 2012 review that showed relatively strong correlations between 24-hour and subdaily ( i.e., 4-hour average) PM2.5 light extinction that indicated that a 24-hour averaging time is an appropriate surrogate for the subdaily time periods relevant for visual perception (U.S. EPA, 2011, Figures G–4 and G–5; Frank, 2012). These analyses continue to provide support for a 24-hour averaging time for the visibility index in this reconsideration. Consistent with previous reviews, the 2022 PA also notes that the 24-hour averaging time may be less influenced by atypical conditions and/or atypical instrument performance than a subdaily averaging time (85 FR 82740, December 18, 2020; 78 FR 3226, January 15, 2013).
With regard to the form for the visibility index, the available information continues to provide support for a 3-year average of annual 90th percentile values. Given that there is no new information to inform selection of an alternate form, as in previous reviews, the 2022 PA notes that the 3-year average form provides stability from the occasional effect of inter-annual meteorological variability that can result in unusually high pollution levels for a particular year (85 FR 82741, December 18, 2020; 78 FR 3198, January 15, 2013; U.S. EPA, 2011, p. 4–58). In so doing, the 2022 PA considers the evaluation in the 2010 Urban-Focused Visibility Assessment (UFVA) of three different statistical forms: 90th, 95th, and 98th percentiles (U.S. EPA, 2010b, Chapter 4).). In considering this evaluation of statistical forms from the 2010 UFVA, consistent with the 2011 PA, the 2022 PA notes that the Regional Haze Program targets the 20 percent most impaired days for visibility improvements in visual air quality in Federal Class I areas and that the median of the distribution of these 20 percent most impaired days would be the 90th percentile. The 2011 PA also noted that strategies that are implemented so that 90 percent of days would have visual air quality that is at or below the level of the visibility index would reasonably be expected to lead to improvements in visual air quality for the 20 percent most impaired days. Additionally, as in the 2011 PA, the 2022 PA recognizes that the available public preference studies do not address frequency of occurrence of different levels of visibility (U.S. EPA, 2022b, section 5.3.1.2). Therefore, the analyses and consideration for the form of a visibility index from the 2011 PA continue to provide support for a 90th percentile form, averaged across three years, in defining the characteristics of a visibility index in this reconsideration.
With regard to the level for the visibility index, the 2022 PA recognizes that there is an additional public preference study (Malm et al., 2019) available in this reconsideration. As noted above, however, this study differs from the previously available public preference studies in several ways, which makes it difficult to integrate this newly available study with the previously available studies. Most significantly, this study was evaluated public preferences for visibility in the Grand Canyon, perhaps the most notable Class I area in the country for visibility purposes. Therefore, the 2022 PA concludes that the Grand Canyon study is not directly comparable to the other available preferences studies and public preferences of visibility impairment in the Malm et al. (2019) study are not appropriate to consider in identifying a range of levels for the target level of protection against visibility impairment for this reconsideration of the secondary PM NAAQS. Start Printed Page 16319
Therefore, the 2022 PA continues to rely on the same studies [157] and the range of 20 to 30 dv identified from those studies in previous reviews. With regard to selecting the appropriate target level of protection for visibility impairment within this range, the 2022 PA notes that in previous reviews, a level at the upper end of the range ( i.e., 30 dv) was selected given the uncertainties and limitations associated with the public preference studies (U.S. EPA, 2022b, section 5.3.1.1). However, the 2022 PA also recognizes that (1) the degree of protection provided by a secondary PM NAAQS is not determined solely by any one element of the standard but by all elements ( i.e., indicator, averaging time, form, and level) being considered together, and (2) decisions regarding the adequacy of the current secondary standards is a public welfare policy judgment to be made by the Administrator. As such, the Administrator may judge that a target level of protection below the upper end of the range ( i.e., less than 30 dv) is appropriate, depending on his public welfare policy judgments, which draw upon the available scientific evidence for PM-related visibility effects and on analyses of visibility impairment, as well as judgments about the appropriate weight to place on the range of uncertainties inherent in the evidence and analyses.
In considering the available public preference studies, consistent with past reviews, the 2022 PA concludes that it is reasonable to consider a range of 20 to 30 dv for selecting a target level of protection, including a high value of 30 dv, a midpoint value of 25 dv, and a low value of 20 dv. A target level of protection at or in the upper end of the range would focus on the Washington, DC, preference study results (Abt Associates, 2001; Smith and Howell, 2009), which identified 30 dv as the level of impairment that was determined to be “acceptable” by at least 50 percent of study participants. The public preferences of visibility impairment in the Washington, DC, study are likely to be generally representative of urban areas that do not have valued scenic elements ( e.g., mountains) in the distant background. This would be more representative of areas in the middle of the country and many areas in the eastern U.S., as well as possibly some areas in the western U.S.
A target level of protection in the middle of the range would be most closely associated with the level of impairment that was determined to be “acceptable” by at least 50 percent of study participants in the Phoenix, AZ, study (BBC Research & Consulting, 2003), which was 24 dv. This study, while methodologically similar to the other public preference studies, included participants that were selected as a representative sample of the Phoenix area population [158] and used computer-generated images to depict specific uniform visibility impairment conditions. This study yielded the best results of the four public preference studies in terms of the least noisy preference results and the most representative selection of participants. Therefore, based on this study, the use of 25 dv to represent a midpoint within the range of target levels protection is well supported.
A target level of protection at or just above the lower end of the range would focus on the Denver, CO, study, but may not be as strongly supported as higher levels within the range (Ely et al., 1991). Older studies, such as those conducted in Denver, CO (Ely et al., 1991), and British Columbia, Canada (Pryor, 1996), used photographs that were taken at different times of the day and on different days to capture a range of light extinction levels needed for the preference studies. Compared to studies that used computer-generated images ( i.e., those in Phoenix, AZ, and Washington, DC) there was more variability in scene appearance in these older studies that could affect preference rating and includes uncertainties associated with using ambient measurements to represent sight path-averaged light extinction values rather than superimposing a computer-generated amount of haze onto the images. When using photographs, the intrinsic appearance of the scene can change due to meteorological conditions ( i.e., shadow patterns and cloud conditions) and spatial variations in ambient air quality that can result in ambient light extinction measurement not being representative of the sight-path-averaged light extinction. Computer-generated images, such as those generated with WinHaze, do not introduce such uncertainties, as the same base photograph is used ( i.e., there is no intrinsic change in scene appearance) and the modeled haze that is superimposed on the photograph is determined based on uniform light extinction throughout the scene.
In addition to differences in preferences that may arise from photographs versus computer-generated images, urban visibility preference may differ by location, and such differences may arise from differences in the cityscape scene that is depicted in the images. These differences are related to the perceived value of objects and scenes that are included in the image, as objects at a greater distance have a greater sensitivity to perceived visibility changes as light extinction is changed compared to similar scenes with objects at shorter distances. For example, a person (regardless of their location) evaluating visibility in an image with more scenic elements such as mountains or natural views may value better visibility conditions in these images compared to the same level of visibility impairment in an image that only depicts urban features such as buildings and roads. That is, if a person was shown the same level of visibility impairment in two images depicting different scenes—one with mountains in the background and urban features in the foreground and one with no mountains in the background and nearby buildings in the image without mountains in the distance—may find the amount of haze to be unacceptable in the image with the mountains in the distance because of a greater perceived value of viewing the mountains, while finding the amount of haze to be acceptable in the image with the buildings because of a lesser value of viewing the cityscape or an expectation that such urban areas may generally have higher levels of haze in general. This is consistent when comparing the differences between the Denver, CO, study results (which found the 50% acceptance criteria occurred at the best visual air quality levels among the four cities) and the Washington, DC, results (which found the 50% acceptability criteria occurred at the worst visual air quality levels among the four cities). These results may occur because the most prominent and picturesque feature of the cityscape of Denver is the visible snow-covered mountains in the distance, while the prominent and Start Printed Page 16320 picturesque features of the Washington, DC, cityscape are buildings relatively nearby without prominent and/or valued scenic features that are more distant. Given these variabilities in preferences it is unclear to what extent, the available evidence provides strong support for a target level of protection at the lower end of the range. Future studies that reduce sources of noisiness and uncertainty in the results could provide more information that would support selection of a target level of protection at or just above the lower end of the range.
Taken together, the 2022 PA concludes that available information continues to support a visibility index with estimated light extinction as the indicator, a 24-hour averaging time, and a 90th percentile form, averaged over three years, with a level within the range of 20 to 30 dv.
ii. Relationship Between the PM2.5 Visibility Index and the Current Secondary 24-Hour PM2.5 Standard
The 2022 PA presents quantitative analyses based on recent air quality that evaluate the relationship between recent air quality and calculated light extinction. As in previous reviews, these analyses explored this relationship as an estimate of visibility impairment in terms of the 24-hour PM2.5 standard and the visibility index. Generally, the results of the updated analyses are similar to those based on the data available at the time of the 2012 and 2020 reviews (U.S. EPA, 2022b, section 5.3.1.2). As discussed in section V.C.1.a above, the 2022 PA concludes that the available evidence continues to support a visibility index with estimated light extinction as the indicator, a 24-hour averaging time, and a 90th percentile form, averaged over three years, with a level within the range of 20 to 30 dv. These analyses evaluate visibility impairment in the U.S. under recent air quality conditions, particularly those conditions that meet the current standards, and the relative influence of various factors on light extinction. Given the relationship of visibility with short-term PM, we focus particularly on the short-term PM standards.[159] Compared to the 2012 review, updated analyses incorporate several refinements, including (1) the evaluation of three versions of the IMPROVE equation to calculate light extinction (U.S. EPA, 2022b, Appendix D, Equations D–1 through D–3) in order to better understand the influence of variability in equation inputs; [160] (2) the use of 24-hour relative humidity data, rather than monthly average relative humidity as was used in the 2012 review (U.S. EPA, 2022b, section 5.3.1.2, Appendix D); and (3) the inclusion of the coarse fraction in the estimation of light extinction (U.S. EPA, 2022b, section 5.3.1.2, Appendix D). The analyses in the reconsideration are updated from the 2012 and 2020 reviews and include 60 monitoring sites that measure PM2.5 and PM10 and are geographically distributed across the U.S. in both urban and rural areas (U.S. EPA, 2022b, Appendix D, Figure D–1).
When light extinction was calculated using the revised IMPROVE equation, in areas that meet the current 24-hour PM2.5 standard for the 2017–2019 time period, all sites have light extinction estimates at or below 26 dv (U.S. EPA, 2022b, Figure 5–3). For the four locations that exceed the current 24-hour PM2.5 standard, light extinction estimates range from 22 dv to 27 dv (U.S. EPA, 2022b, Figure 5–3). These findings are consistent with the findings of the analyses using the same IMPROVE equation in the 2012 review with data from 102 sites with data from 2008–2010 and in the 2020 review with data from 67 sites with data from 2015–2017. The analyses presented in the 2022 PA indicate similar findings to those from the analyses in the 2012 and 2020 reviews, i.e., the updated quantitative analysis shows that the 3-year visibility metric was no higher than 30 dv [161] at sites meeting the current secondary PM standards, and at most such sites the 3-year visibility index values are much lower ( e.g., an average of 20 dv across the 60 sites).[162]
When light extinction was calculated using the revised IMPROVE equation,[163] the resulting 3-year visibility metrics are nearly identical to light extinction estimates calculated using the original IMPROVE equation (U.S. EPA, 2022b, Figure 5–4), but some sites are just slightly higher. Using the revised IMPROVE equation, for those sites that meet the current 24-hour PM2.5 standard, the 3-year visibility metric is at or below 26 dv. For the four locations that exceed the current 24-hour PM2.5 standard, light extinction estimates range from 22 dv to 29 dv (U.S. EPA, 2022b, Figure 5–4). These results are similar to those for light extinction calculated using the original IMPROVE equation,[164] and those from previous reviews.
When light extinction was calculated using the refined equation from Lowenthal and Kumar (2016), the resulting 3-year visibility metrics are slightly higher at all sites compared to light extinction estimates calculated using the original IMPROVE equation (U.S. EPA, 2022b, Figure 5–5).[165] These higher estimates are to be expected, given the higher OC multiplier included in the IMPROVE equation from Lowenthal and Kumar (2016), which reflects the use of data from remote areas with higher concentrations of organic PM when validating the equation. As such, it is important to note that the Lowenthal and Kumar (2016) version of the equation may overestimate light extinction in non-remote areas, including the urban areas in the updated analyses in this reconsideration.
Nevertheless, when light extinction is calculated using the Lowenthal and Start Printed Page 16321 Kumar (2016) equation for those sites that meet the current 24-hour PM2.5 standard, the 3-year visibility metric is generally at or below 28 dv. For those sites that exceed the current 24-hour PM2.5 standard, three of these sites have a 3-year visibility metric ranging between 26 dv and 30 dv, while one site in Fresno, California that exceeds the current 24-hour PM2.5 standard and has a 3-year visibility index value of 32 dv (compared to 29 dv when light extinction is calculated with the original IMPROVE equation) (see U.S. EPA, 2022b, Appendix D, Table D–3). At this site, it is likely that the 3-year visibility metric using the Lowenthal and Kumar (2016) equation would be below 30 dv if PM2.5 concentrations were reduced such that the 24-hour PM2.5 level of 35 µg/m3 was attained.
In considering visibility impairment under recent air quality conditions, the 2022 PA recognizes that the differences in the inputs to equations estimating light extinction can influence the resulting values. For example, given the varying chemical composition of emissions from different sources, the 2.1 multiplier for converting OC to organic matter (OM) in the Lowenthal and Kumar (2016) equation may not be appropriate for all source types. At the time of the 2012 review, the EPA judged that a 1.6 multiplier was more appropriate, for the purposes of estimating visibility index at sites across the U.S., than the 1.4 or 1.8 multipliers used in the original and revised IMPROVE equations, respectively. A multiplier of 1.8 or 2.1 would account for the more aged and oxygenated organic PM that tends to be found in more remote regions than in urban regions, whereas a multiplier of 1.4 may underestimate the contribution of organic PM found in remote regions when estimating light extinction (78 FR 3206, January 15, 2013; U.S. EPA, 2012, p. IV–5). The available scientific information and results of the air quality analyses indicate that it may be appropriate to select inputs to the IMPROVE equation ( e.g., the multiplier for OC to OM) on a regional basis rather than a national basis when calculating light extinction. This is especially true when comparing sites with localized PM sources (such as sites in urban or industrial areas) to sites with PM derived largely from biogenic precursor emissions (that contribute to widespread secondary organic aerosol formation), such as those in the southeastern U.S. The 2022 PA notes, however, that conditions involving PM from such different sources have not been well studied in the context of applying a multiplier to estimate light extinction, contributing uncertainty to estimates of light extinction for such conditions.
At the time of the 2012 review, the EPA noted that PM2.5 is the size fraction of PM responsible for most of the visibility impairment in urban areas (77 FR 38980, June 29, 2012). Data available at the time of the 2012 review suggested that, generally, PM10–2.5 was a minor contributor to visibility impairment most of the time (U.S. EPA, 2010b) although the coarse fraction may be a major contributor in some areas in the desert southwestern region of the U.S. Moreover, at the time of the 2012 review, there were few data available from PM10–2.5 monitors to quantify the contribution of coarse PM to calculated light extinction. Since that time, an expansion in PM10–2.5 monitoring efforts has increased the availability of data for use in estimating light extinction with both PM2.5 and PM10–2.5 concentrations included as inputs in the equations. The analysis in the 2020 PA addressed light extinction at 20 of the 67 PM2.5 sites where collocated PM10–2.5 monitoring data were available. Since that time, PM10–2.5 monitoring data are available at more locations and the analyses presented in the 2022 PA include those for light extinction estimated with coarse and fine PM at all 60 sites. Generally, the contribution of the coarse fraction to light extinction at these sites is minimal, contributing less than 1 dv to the 3-year visibility metric (U.S. EPA, 2020b, section 5.2.1.2). However, the 2022 PA notes that in the updated quantitative analyses, only a few sites were in locations that would be expected to have high concentrations of coarse PM, such as the Southwest. These results are consistent with those in the analyses in the 2019 ISA, which found that mass scattering from PM10−2.5 was relatively small (less than 10%) in the eastern and northwestern U.S., whereas mass scattering was much larger in the Southwest (more than 20%) particularly in southern Arizona and New Mexico (U.S. EPA, 2019a, section 13.2.4.1, p. 13–36).
Overall, the findings of these updated quantitative analyses are generally consistent with those in the 2012 and 2020 reviews. The 3-year visibility metric was generally below 26 dv in most areas that meet the current 24-hour PM2.5 standard. Small differences in the 3-year visibility metric were observed between the variations of the IMPROVE equation, which may suggest that it may be more appropriate to use one version over another in different regions of the U.S. based on PM characteristics such as particle size and composition to more accurately estimate light extinction.
b. Non-Visibility Effects
Consistent with the evidence available at the time of the 2012 and 2020 reviews, and as described in detail in the 2022 PA (U.S. EPA, 2022b, section 5.3.2.2), the data remain insufficient to conduct quantitative analyses for PM effects on climate and materials. For PM-related climate effects, as explained in more detail in the proposal (88 FR 5654, January 27, 2023), our understanding of PM-related climate effects is still limited by significant key uncertainties. The recently available evidence does not appreciably improve our understanding of the spatial and temporal heterogeneity of PM components that contribute to climate forcing (U.S. EPA, 2022b, sections 5.3.2.1.1 and 5.5). Significant uncertainties also persist related to quantifying the contributions of PM and PM components to the direct and indirect effects on climate forcing, such as changes to the pattern of rainfall, changes to wind patterns, and effects on vertical mixing in the atmosphere (U.S. EPA, 2022b, sections 5.3.2.1.1 and 5.5). Additionally, while improvements have been made to climate models since the completion of the 2009 ISA, the models continue to exhibit variability in estimates of the PM-related climate effects on regional scales ( e.g., ~100 km) compared to simulations at the global scale (U.S. EPA, 2022b, sections 5.3.2.1.1 and 5.5). While our understanding of climate forcing on a global scale is somewhat expanded since the 2012 review, significant limitations remain to quantifying potential adverse PM-related climate effects in the U.S. and how they would vary in response to incremental changes in PM concentrations across the U.S. As such, while recent research is available on climate forcing on a global scale, the remaining limitations and uncertainties are significant, and the recent global scale research does not translate directly for use at regional spatial scales. Therefore, the evidence does not provide a clear understanding at the necessary spatial scales for quantifying the relationship between PM mass in ambient air and the associated climate-related effects in the U.S. that would be necessary to evaluate or consider a level of air quality to protect against such effects and for informing consideration of a national PM standard on climate in this reconsideration (U.S. EPA, 2022b, section 5.3.2.2.1; U.S. EPA, 2019a, section 13.3). Start Printed Page 16322
For PM-related materials effects, as explained in more detail in the 2022 PA (U.S. EPA, 2022b, section 5.3.2.2), the available evidence has been somewhat expanded to include additional information about the soiling process and the types of materials impacted by PM. This evidence provides some limited information to inform dose-response relationships and damage functions associated with PM, although most of these studies were conducted outside of the U.S. where PM concentrations in ambient air are typically above those observed in the U.S. (U.S. EPA, 2022b, section 5.3.2.1.2; U.S. EPA, 2019a, section 13.4). The evidence on materials effects characterized in the 2019 ISA also includes studies examining effects of PM on the energy efficiency of solar panels and passive cooling building materials, although the evidence remains insufficient to establish quantitative relationships between PM in ambient air and these or other materials effects (U.S. EPA, 2022b, section 5.3.2.1.2). While the available evidence assessed in the 2019 ISA is somewhat expanded since the time of the 2012 review, quantitative relationships have not been established for PM-related soiling and corrosion and frequency of cleaning or repair that further the understanding of the public welfare implications of materials effects (U.S. EPA, 2022b, section 5.3.2.2.2; U.S. EPA, 2019a, section 13.4). Therefore, there is insufficient information to inform quantitative analyses assessing materials effects to inform consideration of a national PM standard on materials in this reconsideration (U.S. EPA, 2022b, section 5.3.2.2.2; U.S. EPA, 2019a, section 13.4).
B. Conclusions on the Secondary PM Standards
In drawing conclusions on the adequacy of the current secondary PM standards, in view of the advances in scientific knowledge and additional information now available, the Administrator has considered the evidence base, information, and policy judgments that were the foundation of the 2020 decision and reflects upon the body of information and evidence available in this reconsideration. In so doing, the Administrator has taken into account both evidence-based and quantitative information-based considerations, as well as advice from the CASAC and public comments. Evidence-based considerations draw upon the EPA's assessment and integrated synthesis of the scientific evidence from studies evaluating welfare effects related to visibility, climate, and materials associated with PM in ambient air as discussed in the 2022 PA (summarized in sections V.B and V.D.2 of the proposal, section V.A.2 above). The quantitative information-based considerations draw from the results of the quantitative analyses of visibility impairment presented in the 2022 PA (as summarized in section V.C of the proposal and V.A.3 above) and consideration of these results in the 2022 PA.
Consideration of the scientific evidence and quantitative information in the 2022 PA and by the Administrator is framed by consideration of a series of policy-relevant questions. Section V.B.2 below summarizes the rationale for the Administrators proposed decision, drawing from section V.D.3 of the proposal. The advice and recommendations of the CASAC and public comments on the proposed decision are addressed below in sections V.B.1 and V.B.3, respectively. The Administrator's conclusions in this reconsideration regarding the adequacy of the secondary PM standards and whether any revisions are appropriate are described in section V.D.4.
1. CASAC Advice
In comments on the 2019 draft PA, the CASAC concurred with the staff's overall preliminary conclusions that it is appropriate to consider retaining the current secondary standards without revision (Cox, 2019b). The CASAC “finds much of the information . . . on visibility and materials effects of PM2.5 to be useful, while recognizing that uncertainties and controversies remain about the best ways to evaluate these effects” (Cox, 2019b, p. 13 of consensus responses). Regarding climate, while the CASAC agreed that research on PM-related effects has expanded since the 2012 review, it also concluded that “there are still significant uncertainties associated with the accurate measurement of PM to the direct and indirect effects of PM on climate” (Cox, 2019b, pp. 13–14 of consensus responses). The committee recommended that the EPA summarize the “current scientific knowledge and quantitative modeling results for effects of reducing PM2.5 ” on several climate-related outcomes (Cox, 2019b, p. 14 of consensus responses), while also recognizing that “it is appropriate to acknowledge uncertainties in climate change impacts and resulting welfare impacts in the United States of reductions in PM2.5 levels” (Cox, 2019b, p. 14 of consensus responses). When considering the overall body of scientific evidence and technical information for PM-related effects on visibility, climate, and materials, the CASAC agreed with the EPA's preliminary conclusions in the 2019 draft PA, stating that “the available evidence does not call into question the protection afforded by the current secondary PM standards and concurs that they should be retained” (Cox, 2019b, p. 3 of letter).
In this reconsideration, the CASAC provided its advice regarding the current secondary PM standards in the context of its review of the 2021 draft PA (Sheppard, 2022a). In its comments on the 2021 draft PA, the CASAC first recognized that the scientific evidence is sufficient to support a causal relationship between PM and visibility effects, climate effects and materials effects.
With regard to visibility effects, the CASAC recognized that the identification of a target level of protection for the visibility index is based on a limited number of studies and suggested that “additional region- and view-specific visibility preference studies and data analyses are needed to support a more refined visibility target” (Sheppard, 2022a, p. 21 of consensus responses). While the CASAC did not recommend revising either the target level of protection for the visibility index or the level of the current 24-hour PM2.5 standard, they did state that a visibility index of 30 deciviews “needs to be justified” and “[i]f a value of 20–25 deciviews is deemed to be an appropriate visibility target level of protection, then a secondary 24-hour PM2.5 standard in the range of 25–35 µg/m3 should be considered” (Sheppard, 2022a, p. 21 of consensus responses).
The CASAC also recognized the limited availability of monitoring methods and networks for directly measuring light extinction. As such, they suggest that “[a] more extensive technical evaluation of the alternatives for visibility indicators and practical measurement methods (including the necessity for a visibility FRM) is need for future reviews” (Sheppard, 2022a, p. 22 of consensus letter). The majority of the CASAC “recommend[ed] that an FRM for a directly measured PM2.5 light extinction indicator be developed” to inform the consideration of the protection afforded by the secondary PM standards against visibility impairment, the minority of the CASAC “believe that a light extinction FRM is not necessary to set a secondary standard protective of visibility” (Sheppard, 2022a, p. 22 of consensus responses). Start Printed Page 16323
With regard to climate, the CASAC noted that “there is a causal relationship between PM and climate change, but large uncertainties remain” and recommended additional research (Sheppard, 2022a, p. 22 of consensus responses). With respect to materials damage, the CASAC noted that “[q]uantitative information on the relationship between PM and material damage is lacking” and suggested some additional studies and research approaches that could provide additional information on the effects of PM on materials and the quantitative assessment of the relationship between materials effects and PM in ambient air (Sheppard, 2022a, p. 23 of consensus responses).
2. Basis for the Proposed Decision
In reaching his proposed conclusions, the Administrator first recognized that, consistent with the scope of this reconsideration, his decision in this reconsideration will be focused only and specifically on the adequacy of public welfare protection provided by the secondary PM standards from effects related to visibility, climate, and materials. He then considered the assessment of the current evidence and conclusions reached in the 2019 ISA and ISA Supplement; the currently available quantitative information, including associated limitations and uncertainties, described in detail and characterized in the 2022 PA; considerations and staff conclusions and associated rationales presented in the 2022 PA; and the advice and recommendations from the CASAC (88 FR 5655, January 27, 2023).
With respect to visibility, the Administrator noted the longstanding body of evidence that demonstrates a causal relationship between ambient PM and effects on visibility (U.S. EPA, 2019a, section 13.2). and that visibility impairment can have implications for people's enjoyment of daily activities and for their overall sense of well-being. Therefore, as in previous reviews, he considered the degree to which the current secondary standards protect against PM-related visibility impairment. In so doing, and consistent with previous reviews, the Administrator considered the protection provided by the current secondary standards against PM-related visibility impairment in conjunction with the Regional Haze Program [166] for protecting visibility in Class I areas,[167] which together would be expected to achieve appropriate visual air quality across all areas (88 FR 5658, January 27, 2023). The Administrator proposed to conclude that addressing visibility impairment in Class I areas is beyond the scope of the secondary PM NAAQS and that setting the secondary PM NAAQS at a level that would remedy visibility impairment in Class I areas would result in standards that are more stringent than is requisite.
In further considering what standards are requisite to protect against adverse public welfare effects from visibility impairment, the Administrator adopted an approach consistent with the approach used in previous reviews (88 FR 5645, January 27, 2023). That is, he first identified an appropriate target level of protection in terms of a PM visibility index that accounts for the factors that influence the relationship between particles in the ambient air and visibility ( i.e., size fraction, species composition, and relative humidity). He then considered air quality analyses examining the relationship between this PM visibility index and the current secondary 24-hour PM2.5 standard in locations meeting the current 24-hour PM2.5 and PM10 standards (U.S. EPA, 2022b, section 5.3.1.2; 88 FR 5650, January 27, 2023).
To identify a target level of protection, the Administrator first considered the characteristics of the visibility index and defines its elements (indicator, averaging time, form, and level). With regard to the indicator for the visibility index, the Administrator recognized that there is a lack of availability of methods and an established network for directly measuring light extinction, consistent with the conclusions reached in the 2022 PA (U.S. EPA, 2022b, section 5.3.1.1) and with the CASAC's recommendation for additional research on direct measurement methods for light extinction in their review of the 2021 draft PA (Sheppard, 2022a, p. 22 of consensus responses). Consistent with the approaches used in reaching decisions in 2012 and 2020, given the lack of such monitoring data, the Administrator preliminarily judged that estimated light extinction, as calculated using one or more versions of the IMPROVE algorithms, continues to be the most appropriate indicator for the visibility index in this reconsideration (88 FR 5659, January 27, 2023).
In further defining the characteristics of a visibility index based on estimates of light extinction, the Administrator considered the appropriate averaging time, form, and level of the index. With regard to the averaging time and form, the Administrator noted that in previous reviews, a 24-hour averaging time was selected and the form was defined as the 3-year average of annual 90th percentile values. The Administrator recognized that the evidence available in this reconsideration and described in the 2022 PA continue to provide support for the short-term nature of PM-related visibility effects. Considering the available analyses of 24-hour and subdaily PM2.5 light extinction, and noting that the CASAC did not provide advice or recommendations with regard to the averaging time of the visibility index, the Administrator preliminarily judged that the 24-hour averaging time continues to be appropriate for the visibility index (88 FR 5659, January 27, 2023).
With regard to the form of the visibility index, the Administrator noted that, consistent with the approach taken in other NAAQS, including the current secondary 24-hour PM2.5 NAAQS, a multi-year percentile form offers greater stability to the air quality management process by reducing the possibility that statistically unusual indicator values will lead to transient violations of the standard. Using a 3-year average provides stability from the occasional effects of inter-annual meteorological variability that can result in unusually high pollution levels for a particular year (88 FR 5659, January 27, 2023). In considering the percentile that would be appropriate with the 3-year average, the Administrator first noted that the Regional Haze Program targets the 20% most impaired days for improvements in visual air quality in Class I areas.[168] Based on analyses examining 90th, 95th, and 98th percentile forms, the Administrator preliminarily judged that a focus similar to the Regional Haze Program focused on improving the 20% most impaired days suggest that the 90th percentile, which represents the median of the 20% most impaired days, such that 90% of days have visual air quality that is at or below the target level of protection of the visibility Start Printed Page 16324 index, would be reasonably expected to lead to improvements in visual air quality for the 20% most impaired days (88 FR 5659, January 27, 2023). In the analyses of percentiles, the results suggest that a higher percentile value could have the effect of limiting the occurrence of days with peak PM-related light extinction in areas outside of Federal Class I areas to a greater degree. However, the Administrator preliminarily concluded that it is appropriate to balance concerns about focusing on the group of most impaired days with concerns about focusing on the days with peak visibility impairment. Additionally, the Administrator noted that the CASAC did not provide advice or recommendations related to the form of the visibility index. Therefore, the Administrator preliminarily judged that it remains appropriate to define a visibility index in terms of a 24-hour averaging time and a form based on the 3-year average of annual 90th percentile values (88 FR 5659, January 27, 2023).
With regard to the level of the visibility index, the Administrator first noted that the scientific evidence that is available to inform the level of the visibility index is largely the same as in previous reviews, and continues to provide support for a level within the range of 20 to 30 dv (88 FR 5659–5660, January 27, 2023). The Administrator recognized that significant uncertainties and limitations remained, in particular those related to the public preference studies, including methodological differences between the studies, and that the available studies may not capture the full range of visibility preferences in the U.S. population (88 FR 5659–5660, January 27, 2023). The Administrator also noted that, in their review of the 2021 draft PA, the CASAC recognized that a judgment regarding the appropriate target level of protection for the visibility index is based on a limited number of visibility preference studies, with studies conducted in the western U.S. reporting public preferences for visibility impairment associated with the lower end of the range of levels, while studies conducted in the eastern U.S. reporting public preferences associated with the upper end of the range (Sheppard, 2022a, p. 21 of consensus responses). The Administrator noted that there have long been significant questions about how to set a national standard for visibility that is not overprotective for some areas of the U.S. In establishing the Regional Haze Program to improve visibility in Class I areas, Congress noted that “as a matter of equity, the national ambient air quality standards cannot be revised to adequately protect visibility in all areas of the country.” H.R. Rep. 95–294 at 205. Thus, in reaching his proposed conclusion, the Administrator recognized that there are substantial uncertainties and limitations in the public preference studies that should be considered when selecting a target level of protection for the visibility index and took the uncertainties and variability inherent in the public preference studies into account. In so doing, the Administrator first preliminarily judged that, consistent with similar judgments in past reviews, it is appropriate to recognize that the secondary 24-hour PM2.5 standard is intended to address visibility impairment across a wide range of regions and circumstances, and that the current standard works in conjunction with the Regional Haze Program to improve visibility, and therefore, it is appropriate to establish a target level of protection based on the upper end of the range of levels. In considering the information available in this reconsideration and the CASAC's advice, the Administrator proposed to conclude that the protection provided by a visibility index based on estimated light extinction, a 24-hour averaging time, and a 90th percentile form, averaged over 3 years, set at a level of 30 dv (the upper end of the range of levels) would be requisite to protect public welfare with regard to visibility impairment (88 FR 5660, January 27, 2023).
In preliminarily concluding that it remains appropriate in this reconsideration to define the target level of protection in terms of a visibility index based on estimated light extinction as described above ( i.e., with a 24-hour averaging time; a 3-year, 90th percentile form; and a level of 30 dv), the Administrator next considered the degree of protection from visibility impairment afforded by the existing secondary standards. He considered the updated analyses of PM-related visibility impairment presented in the 2022 PA (U.S. EPA, 2022b, section 5.3.1.2), which reflect several improvements over the analyses conducted in the 2012 review. Specifically, the updated analyses examine multiple versions of the IMPROVE algorithm, including the version incorporating revisions since the 2012 review (section V.B.1.a), which provides an improved understanding of how variation in equation inputs impacts calculated light extinction (U.S. EPA, 2022b, Appendix D). In addition, unlike the analyses in the 2012 review and the 2020 PA, all of the sites included in the analyses had PM10–2.5 data available, which allows for better characterization of the influence of the coarse fraction on light extinction (U.S. EPA, 2022b, section 5.3.1.2).
The Administrator noted that the results of these updated analyses are consistent with the results from the 2012 and 2020 reviews (88 FR 5660, January 27, 2023). Regardless of the IMPROVE equation used, these analyses demonstrate that the 3-year visibility metric is at or below 28 dv in all areas meeting the current 24-hour PM2.5 standard (section V.C.1.b). Given the results of these analyses, the Administrator preliminarily concluded that the updated scientific evidence and technical information support the adequacy of the current secondary PM2.5 and PM10 standards to protect against PM-related visibility impairment. While the inclusion of the coarse fraction had a relatively modest impact on calculated light extinction in the analyses presented in the 2022 PA, he nevertheless recognized the continued importance of the PM10 standard given the potential for larger impacts in locations with higher coarse particle concentrations, such as in the southwestern U.S., for which only a few sites met the criteria for inclusion in the analyses in the 2022 PA (U.S. EPA, 2019a, section 13.2.4.1; U.S. EPA, 2022b, section 5.3.1.2).
With regard to the adequacy of the secondary 24-hour PM2.5 standard, the Administrator noted that the CASAC stated that “[i]f a value of 20–25 deciviews is deemed to be an appropriate visibility target level of protection, then a secondary 24-hour PM2.5 standard in the range of 25–35 µg/m3 should be considered” (Sheppard, 2022a, p. 21 of consensus responses). The Administrator recognized that the CASAC recommended that the Administrator provide additional justification for a visibility index target of 30 dv but did not specifically recommend that he choose an alternative level for the visibility index. The Administrator considered the CASAC's advice, together with the available scientific evidence and quantitative information, in reaching his proposed conclusions. He recognized conclusions regarding the appropriate weight to place on the scientific and technical information examining PM-related visibility impairment including how to consider the range and magnitude of uncertainties inherent in that information is a public welfare policy judgment left to the Administrator. As such, the Administrator noted his conclusion on Start Printed Page 16325 the appropriate visibility index ( i.e., with a 24-hour averaging time; a 3-year, 90th percentile form; and a level of 30 dv) and his conclusions regarding the quantitative analyses of the relationship between the visibility index and the current secondary 24-hour PM2.5 standard. In so doing, he proposed to conclude that the current secondary standards provide requisite protection against PM-related visibility effects (88 FR 5661, January 27, 2023).
In reaching his proposed conclusions, the Administrator also recognized that the available evidence on visibility impairment generally reflects a continuum and that the public preference studies did not identify a specific level of visibility impairment that would be perceived as “acceptable” or “unacceptable” across the whole U.S. population. However, he noted that a judgment regarding the appropriate target level of protection would take into consideration the appropriate weight to place on the individual public preference studies. In so doing, he noted that placing more weight on the public preference study from Washington, DC, could provide support for a target level of protection at or near 30 dv, whereas placing more weight on the public preference study performed in the Phoenix, AZ, study could provide support for a target level of protection below 30 dv and down to 25 dv. While the Administrator noted that, in their review of the 2021 draft PA, the CASAC did not recommend revising the level of the current 24-hour PM2.5 standard, the Administrator recognized that they did recommend greater justification for a target level of protection of 30 dv, and noted that if a target level of protection of 20–25 dv was identified, then a secondary 24-hour PM2.5 standard in the range of 25–35 μg/m3 should be considered (Sheppard, 2022a, p. 21 of consensus responses). For these reasons, the Administrator solicited comment on his proposed decision to retain the current secondary 24-hour PM2.5 standard, as well as the appropriateness of a target level of protection for visibility below 30 dv and as low as 25 dv, and on revising the level of the current secondary 24-hour PM2.5 standard to a level as low as 25 µg/m3 .
With respect to climate effects, the Administrator recognized that a number of improvements and refinements have been made to climate models since the time of the 2012 review. However, despite continuing research and the strong evidence supporting a causal relationship with climate effects (U.S. EPA, 2019a, section 13.3.9), the Administrator noted that there are still significant limitations in quantifying the contributions of the direct and indirect effects of PM and PM components on climate forcing (U.S. EPA, 2022b, sections 5.3.2.1.1 and 5.5). He also recognized that models continue to exhibit considerable variability in estimates of PM-related climate impacts at regional scales ( e.g., ~100 km), compared to simulations at the global scale (U.S. EPA, 2022b, sections 5.3.2.1.1 and 5.5). As noted above, the CASAC recognized a causal relationship between PM and climate effects but also the large uncertainties associated with quantitatively assessing such effects, particularly on a national level in the context of a U.S.-based standard. These uncertainties led the Administrator to preliminarily conclude that the scientific information available in this reconsideration remains insufficient to quantify, with confidence, the impacts of ambient PM on climate in the U.S. (U.S. EPA, 2022b, section 5.3.2.2.1) and that there is insufficient information at this time to revise the current secondary PM standards or to promulgate a distinct secondary standard to address PM-related climate effects (88 FR 5661, January 27, 2023).
With respect to materials effects, the Administrator noted that the available evidence continues to support the conclusion that there is a causal relationship with PM deposition (U.S. EPA, 2019a, section 13.4). He recognized that deposition of particles in the fine or coarse fractions can result in physical damage and/or impaired aesthetic qualities. Particles can contribute to materials damage by adding to the effects of natural weathering processes and by promoting the corrosion of metals, the degradation of painted surfaces, the deterioration of building materials, and the weakening of material components. While some recent evidence on materials effects of PM is available in the 2019 ISA, the Administrator noted that this evidence is primarily from studies conducted outside of the U.S. in areas where PM concentrations in ambient air are higher than those observed in the U.S. (U.S. EPA, 2019a, section 13.4). The CASAC also noted the lack of quantitative information relating PM and material effects. Given the limited amount of information on the quantitative relationships between PM and materials effects in the U.S., and uncertainties in the degree to which those effects could be adverse to the public welfare, the Administrator preliminarily judged that the scientific information available in this reconsideration remains insufficient to quantify, with confidence, the public welfare impacts of ambient PM on materials and that there is insufficient information at this time to revise the current secondary PM standards or to promulgate a distinct secondary standard to address PM-related materials effects (88 FR 5661, January 27, 2023).
Taken together, the Administrator proposed to conclude that the scientific and technical information for PM-related visibility impairment, climate impacts, and materials effects, with its attendant uncertainties and limitations, supports the current level of protection provided by the secondary PM standards as being requisite to protect against known and anticipated adverse effects on public welfare. For visibility impairment, this proposed conclusion reflected his consideration of the evidence for PM-related light extinction, together with his consideration of updated analyses of the protection provided by the current secondary PM2.5 and PM10 standards. For climate and materials effects, this conclusion reflected his preliminary judgment that, although it remains important to maintain secondary PM2.5 and PM10 standards to provide some degree of control over long- and short-term concentrations of both fine and coarse particles, it is generally appropriate not to change the existing secondary standards at this time and that it is not appropriate to establish any distinct secondary PM standards to address PM-related climate and materials effects at this time. As such, the Administrator recognized that current suite of secondary standards ( i.e., the 24-hour PM2.5, 24-hour PM10, and annual PM2.5 standards) together provide such control for both fine and coarse particles and long- and short-term visibility and non-visibility ( e.g., climate and materials) [169] effects related to PM in ambient air. His proposed conclusions on the secondary standards were consistent with advice from the CASAC, which noted substantial uncertainties remain in the scientific evidence for climate and materials effects. Thus, based on his consideration of the evidence and analyses for PM-related welfare effects, as described above, and his consideration of CASAC advice on the secondary standards, the Administrator proposed not to change those standards ( i.e., the current 24-hour and annual PM2.5 standards, 24-hour PM10 standard) at this time (88 FR 5662, January 27, 2023).
Start Printed Page 163263. Comments on the Proposed Decision
Of the public comments received on the proposal, very few were specific to the secondary PM standards. Of those commenters who did provide comments on the secondary PM standards, the majority support the Administrator's proposed decision to retain the current standards. Some commenters disagree with the Administrator's proposed conclusion to retain the current secondary standards, primarily focusing their comments on the need for a revised standard to protect against visibility impairment. In addition to the comments addressed in this notice, the EPA has prepared a Response to Comments document that addresses other specific comments related to setting the secondary PM standards. This document is available for review in the docket for this rulemaking and through the EPA's NAAQS website ( https://www.epa.gov/naaqs/particulate-matter-pm-air-quality-standards).
We first note that some commenters raise questions about the protection provided by the secondary PM standards for ecological effects ( e.g., effects on ecosystems, ecosystem services, or species). However, consistent with the 2016 IRP and as described in the proposal (88 FR 5643, January 27, 2023), other welfare effects of PM, such as the ecological effects identified by commenters, are being considered as part of the separate, ongoing review of the secondary standards for oxides of sulfur, oxides of nitrogen and PM, and thus, those comments are beyond the scope of this action.
Of the comments addressing the proposed decision for the secondary PM standards, many of the commenters support the Administrator's proposed decision to retain the current secondary PM standards, without revision. This group includes industries and industry groups and State and local governments and organizations. All of these commenters generally note their agreement with the rationale provided in the proposal, with a focus on the strength of the available scientific evidence for PM-related welfare effects. Most also recognize that the scientific evidence and quantitative information available in this reconsideration have not substantially altered our previous understanding of PM-related effects on non-ecological welfare effects ( i.e., visibility, climate, and materials) and do not call into question the adequacy of the current secondary standards. They find the proposed decision not to change the standards at this time to be well supported and a reasonable exercise of the Administrator's public welfare policy judgment under the CAA. The EPA agrees with these comments regarding the adequacy of the current secondary PM standards and the lack of support for revision of these standards at this time.
The EPA received relatively few comments on the proposed decision that it is not appropriate to establish any distinct secondary PM standards to address PM-related climate effects. Several commenters agree that the available scientific evidence provides support for the 2019 conclusion that there is a causal relationship between PM and climate effects, and the commenters also agree with the EPA that the currently available information is not sufficient for supporting quantitative analyses for the climate effects of PM in ambient air. These commenters support the Administrator's proposed decision not to set a distinct standard for climate.
There were also very few commenters who commented on the proposed decision that it is not appropriate to establish any distinct secondary PM standards to address PM-related materials effects. As with comments on climate effects, commenters generally agree with the EPA that the evidence is not sufficient to support quantitative analyses for PM-related materials effects. However, some commenters contend that EPA failed to explain in the proposal how the current standard is appropriate to protect materials from the effects of PM. These commenters disagree with the EPA's conclusion that quantitative relationships have not been established for PM-related soiling and corrosion and frequency of cleaning or repair of materials, and cite to several studies conducted outside the U.S. that they contend that the EPA should consider since the same materials are present in the U.S. They further contend that, in discussing the available scientific evidence in the 2019 ISA for studies conducted outside of the U.S., the EPA did not provide references to these studies and, therefore, the public is unable to comment on these studies. They further State that EPA failed to consider the following information: (1) Recent work related to soiling of photovoltaic modules and other surfaces, and; (2) damage and degradation resulting from oxidant concentrations and solar radiation for a number of materials, including polymeric materials, plastic, paint, and rubber. These commenters further assert that the EPA failed to propose a standard that provides requisite protection against materials effects attributable to PM.
As an initial matter, we note that the commenters submitted the same comments related to materials effects during the 2020 review. Consistent with our response in the 2020 notice of final rulemaking (85 FR 82737, December 18, 2020), we disagree with the commenters that the EPA failed to consider the relevant scientific information about materials effects available in this reconsideration. The 2019 ISA considered and included studies related to materials effects of PM, including studies conducted in and outside of the U.S., on newly studied materials including photovoltaic modules that were published prior to the cutoff date for the literature search.[170] These include the Besson et al. (2017) study referenced by the commenters (U.S. EPA, 2019a, section 13.4.2). The Grøntoft et al. (2019) study referenced by the same commenters was published after the cutoff date for the literature search for the 2019 ISA. However, the EPA provisionally considered new studies in responding to comments in the 2020 review, including the new studies highlighted by the commenters in their comments on the 2020 notice of proposed rulemaking, in the context of the findings of the 2019 ISA (see Appendix in U.S. EPA, 2020a).[171] Based on the provisional consideration, the EPA concluded in the 2020 review that the new studies are not sufficient to alter the conclusions reached in the 2019 ISA regarding PM and materials effects. For example, the Grøntoft et al. (2019) study was based on European air pollution which as the EPA has noted has higher concentrations (as well as diversity in sources, such as light duty diesel engines) compared to the U.S.. Thus, the EPA did not find it necessary or appropriate to reopen the air quality criteria to consider this study because it would not have been an adequate basis on which to set a NAAQS. As discussed in section I, when the EPA decided to reconsider the standards, it also decided to reopen the air quality criteria to a limited degree, based on its judgment that certain new studies were likely to be useful in reconsidering the standards. Start Printed Page 16327 Based on the provisional consideration in the 2020 review and the significant data gaps that existed at that time, the EPA did not include these studies within the scope of the 2022 ISA Supplement because, although these studies provide additional support for PM-related materials, the studies would not support quantitative analyses or alternative conclusions regarding these effects. As described in section I.C.5.b above, the ISA Supplement focuses on a thorough evaluation of some studies that became available after the literature cutoff date of the 2019 ISA that could either further inform the adequacy of the current PM NAAQS or address key scientific topics that have evolved since the literature cutoff date for the 2019 ISA. In developing the ISA Supplement, the EPA focused on the non-ecological welfare effects for which the evidence supported a “causal relationship” and for which quantitative analyses could be supported by the evidence because those were the welfare effects that were most useful in informing conclusions in the 2020 PA. While the 2020 PA considered the broader set of evidence for materials effects, it concluded that there remained `substantial uncertainties with regard to the quantitative relationships with PM concentrations and concentration patterns that limit[ed] [the] ability to quantitatively assess the public welfare protection provided by the standards from these effects' (U.S. EPA, 2020b).” Therefore, the ISA Supplement did not include an evaluation of scientific evidence for PM-related materials effects. However, the EPA has once again provisionally considered new studies in this reconsideration, including the studies highlighted by the commenters, in the context of the 2019 ISA and concludes that, as in the 2020 review, these studies are not sufficient to alter the conclusions reached in the 2019 ISA regarding PM and materials effects or to provide sufficient information on which to base a secondary NAAQS. The EPA agrees there is a causal relationship between the presence of PM in the ambient air and materials effects, but to set a standard, the EPA needs not only to understand at what point materials effects become adverse to public welfare but to be able to relate specific concentrations of ambient PM to those levels of materials effects. Given the significant gaps in the evidence, particularly given that the majority of the recent evidence has been conducted outside of the U.S., establishing any quantitative relationships between particle size, concentration, chemical components, and specific measures of materials damage, such as frequency of painting or repair of materials, the EPA finds the evidence is insufficient to support a secondary NAAQS to protect against materials effects.
With regard to studies conducted outside of the U.S., including those referenced by the commenters, as described in the proposal, in reaching his proposed conclusion, the Administrator recognized that while there was some newly available information related to materials effects of PM included in the 2019 ISA, “this evidence is primarily from studies conducted outside of the U.S. in areas where PM concentrations in ambient air are higher than those observed in the U.S. (U.S. EPA, 2019a, section 13.4)” (88 FR 5661, January 27, 2023). We disagree with the commenters that EPA did not provide references for these studies, nor that the lack of references inhibited the public's ability to provide comment on this proposed conclusion. First, the reference to section 13.4 in the 2019 ISA is a direct citation to the evaluation of newly available studies on PM-related materials effects, which includes citations for all materials effects evidence considered in the 2020 review and in this reconsideration. Second, section 5.3.2.1.2 of the 2022 PA considers the available scientific evidence for PM-related materials effects—including citations to the studies newly available in the 2019 ISA—and how that evidence informs conclusions regarding the adequacy of the standard (U.S. EPA, 2022b, section 5.3.2.1.2). Therefore, the EPA disagrees that the proposal failed to provide the proper references to the studies conducted outside of the U.S., and that the public was not provided the opportunity to provide comment on these studies.
Moreover, we disagree with the commenters that the EPA failed to consider quantitative information from studies available in this reconsideration. As detailed in sections 5.3.2.1.2 and 5.3.2.2 of the 2022 PA, and consistent with the information available in the 2020 review, a number of new studies are available that apply new methods to characterize PM-related effects on previously studied materials; however, the evidence remains insufficient to relate soiling or damage to specific levels of PM in ambient air or to establish quantitative relationships between PM and materials degradation. The uncertainties in the evidence identified in the 2012 review persist in the evidence in the 2020 review and in this reconsideration, with significant uncertainties and limitations to establishing quantitative relationships between particle size, concentration, chemical components, and frequency of painting or repair of materials. While some new evidence is available in the 2019 ISA, overall, the data are insufficient to conduct quantitative analyses for PM-related materials effects. Quantitative relationships have not been established between characteristics of PM and frequency of repainting or cleaning of materials, including photovoltaic panels and other energy-efficient materials, that would help inform our understanding of the public welfare implications of soiling in the U.S. (U.S. EPA, 2022b, section 5.3.2.2.2; U.S. EPA, 2019a, section 13.4). Similarly, the information does not support quantitative analyses between microbial deterioration of surfaces and the contribution of carbonaceous PM to the formation of black crusts that contribute to soiling (U.S. EPA, 2022b, section 5.3.2.2.2; U.S. EPA, 2019a, section 13.4). We also note that quantitative relationships are difficult to assess, in particular those characterized using damage functions as these approaches depend on human perception of the level of soiling deemed to be acceptable and evidence in this area remains limited in this reconsideration (U.S. EPA, 2022b, section 5.3.2.1.2). Additionally, we note the CASAC's concurrence with conclusions in the 2020 PA (Cox, 2019b, p. 13 of consensus responses) and the 2022 PA (Sheppard, 2022a, p. 23 of consensus responses) that uncertainties remain about the best way to evaluate materials effects of PM in ambient air. Further, no new studies are available in this reconsideration to link human perception of reduced aesthetic appeal of buildings and other objects to materials effects and PM in ambient air. Finally, uncertainties remain about deposition rates of PM in ambient air to surfaces and the interaction of PM with copollutants on these surfaces (U.S. EPA, 2022b, section 5.6).
With respect to the commenters' assertion that the EPA failed to consider information related to materials damage and degradation from oxidant concentrations and solar radiation for a variety of materials, we first note that, even assuming these sources of materials damage are within the scope of this review of the PM NAAQS, the commenter did not provide any references to the scientific studies that they suggest that the EPA did not consider. Despite the lack of a list of specific references from the commenter, we note that the 2019 ISA considered a number of studies that examined the Start Printed Page 16328 relationships between PM and several of the materials listed by the commenters ( e.g., paint, plastic, rubber). However, as described in the 2022 PA, these studies did not provide additional information regarding quantitative relationships between PM and materials that could inform quantitative analyses (U.S. EPA, 2022b, sections 5.3.2.1.2 and 5.3.2.2.2), nor did they alter conclusions regarding the adequacy of the current standard (U.S. EPA, 2022b, section 5.5).
As summarized above and in the proposal, the evidence in the 2020 review and in this reconsideration for PM-related effects on materials is not substantively changed from that in the 2012 review. There continues to be a lack of evidence related to materials effects that establishes quantitative relationships and supports quantitative analyses of PM-related materials soiling or damage. While the information available in the 2020 review and in this reconsideration continues to support a causal relationship between PM in ambient air and materials effects (U.S. EPA, 2019a, section 13.4), the EPA is unable to relate soiling or damage to specific levels of PM in ambient air and is unable to evaluate or consider a level of air quality to protect against such materials effects. Although the EPA did not propose a distinct level of air quality or a national standard based on air quality impacts (88 FR 5662, January 27, 2023), we did identify data gaps that prevented us from doing so. The EPA identified a number of key uncertainties and areas of future research (U.S. EPA, 2022b, section 5.6) that may inform consideration of the materials effects of PM in ambient air in future reviews of the PM NAAQS. The EPA notes that one commenter objected to the Administrator's proposed conclusion in the proposal (88 FR 5661, January 27, 2023) that in light of the available evidence for PM-related impacts on climate and on materials that it is appropriate not to change the existing secondary standards at this time. The EPA has explained, in both the proposal and this final action, the basis for its conclusion that there is insufficient evidence to identify any particular secondary standard or standards that would provide requisite protection against climate effects or materials damage. The EPA acknowledges that, as a result, the adoption of any distinct secondary PM standards for those effects would be inconsistent with the requirements of the CAA. The EPA is clarifying that it is not basing its decisions on secondary standards in this reconsideration to address these welfare effects because it has concluded that the available scientific evidence is insufficient to allow the Administrator to make a reasoned judgment about what specific standard(s) would be requisite to protect against known or anticipated adverse effects to public welfare from PM-related materials damage or climate effects.
Some commenters agree with the Administrator's proposed conclusion that a target level of protection for visibility of 30 dv and the level of the secondary 24-hour PM2.5 standard of 35 µg/m3 continues to be adequate to protect visibility, highlighting improvements in visibility in the U.S. Other commenters who disagree with the proposed decision indicated support for a more stringent standard for visibility impairment, although some of these commenters did not necessarily specify the alternative standard that would, in their judgment, address their concerns related to various aspects of the EPA's proposal, including the available public preference studies, specific aspects of the visibility index, and the target level of protection identified by the Administrator. Rather, most commenters focused on particular aspects of the visibility metric underlying the current secondary 24-hour PM2.5 standard, including the form, averaging time, and target level of protection necessary to protect against visibility impairment.
With regard to the commenters' assertion that the current secondary standards are inadequate to protect the public welfare from PM-related visibility impairment, the EPA disagrees that the currently available information is sufficient to suggest that a more stringent standard is warranted. The EPA identified and addressed in great detail the limitations and uncertainties associated with the public preference studies as a part of the 2012 review (78 FR 3210, January 15, 2013). Given that the evidence related to public preferences has not substantially changed since the 2012 review, the EPA reiterated the limitations and uncertainties inherent in the evidence as a part of the 2020 PA (U.S. EPA, 2020b, section 5.5), as well as in the 2022 PA for this reconsideration (U.S. EPA, 2022b, section 5.6). The 2022 PA highlights key uncertainties associated with public perception of visibility impairment and identifies areas for future research to inform future PM NAAQS reviews, including those raised by the commenters (U.S. EPA, 2022b, section 5.6). Specifically, the EPA agrees with commenters that there are several areas where additional information would reduce uncertainty in our interpretation of the available information for purposes of characterizing visibility impairment. As described in more detail in the 2020 PA (U.S. EPA, 2020b, p. 5–41) and the 2022 PA (U.S. EPA, 2022b, p. 5–53), briefly, these areas include: (1) Expanding the number and geographic coverage of preference studies in urban, rural, and Class I areas; (2) evaluating visibility preferences of the U.S. population today, given that the preference studies were conducted more than 15 years ago, during which time air quality in the U.S. has improved; (3) accounting for the influence of varying study methods may have on an individual's response as to what level of visibility impairment is acceptable, and; (4) information on people's judgments on acceptable visibility based on factors that can influence their perception of visibility ( e.g., duration of impairment experiences, time of day, frequency of impairment).
However, the EPA disagrees with the commenters that the current secondary PM standards are inadequate and should be made more stringent because of the limitations and uncertainties associated with the available public preference studies. The EPA does not view the limitations of the preference studies and other available evidence as so significant as to render the EPA unable to identify a secondary standard to protect against the adverse effects of PM on visibility, but the EPA also does not believe that the limitations themselves mean that the standards are inadequate. In fact, there is a limited amount of recently available scientific evidence to further inform our understanding of public preferences and visibility impairment is recognized by the Administrator in reaching his proposed decision not to change the current secondary PM standards at this time, given that the evidence base is largely the same as at the time of the 2012 and 2020 reviews.
These same commenters further contend that the EPA failed to use the latest science to develop a visibility index, stating that the EPA failed to consider the contrast of distance methodology employed in a recent meta-analysis of available preference studies (Malm et al., 2019). Commenters claim that the EPA draws conclusions from the Malm et al. (2019) study about how to relate contrast to acceptable visibility preferences in the 2022 ISA Supplement, yet ignores the findings of the study and fails to consider the “contrast of distance” methodology in the 2022 PA and the proposal, thereby, in their view, departing from the CASAC's advice to consider this evidence in setting the secondary Start Printed Page 16329 standard. Finally, the commenters assert that the EPA did not explain why the available public preference studies are adequate for analysis using a light extinction approach but not using the contrast of distance approach, and that such differential treatment is arbitrary.
We disagree with the commenters that the EPA did not use the latest science in evaluating the visibility index, and that the EPA failed to consider the contrast of distance methodology used in Malm et al. (2019). As the commenters state, the Malm et al. (2019) study was included in the ISA Supplement (U.S. EPA, 2022a, section 4.2.1). However, the EPA disagrees with the assertion that the ISA Supplement reached conclusions about how to relate contrast to acceptable visibility preferences. The ISA Supplement provided an overview of the Malm et al. (2019) study, stating that “[t]he main conclusion of this study was that the level of acceptable visual air quality is more consistent across studies using metrics that evaluate the distinction of an object from a background than using metrics that evaluate the greatest distance at which an object can be observed.” Furthermore, the statements that the commenters are referencing in support of this statement ( i.e., U.S. EPA, 2022b, pp. 4–5–4–6) are in fact the conclusions of the study itself, rather than conclusions of the EPA. For example, the ISA Supplement notes that “Malm et al. (2019) suggested that scene-dependent metrics like contrast, which integrate the effects of bext along the sight paths between observers and landscape features, are better predictors of preference levels than universal metrics like light extinction.” The suggestion that the contrast of distance methodology is a better predictor than light extinction is one of the study authors, not the EPA. The EPA has not reached a conclusion on whether contrast of distance methodology would be a more appropriate indicator for a visibility index than estimated light extinction because the EPA finds that there is insufficient information in the record at this time to support that it is practical to evaluate, much less adopt, the contrast of distance methodology on a national basis. Specifically, the Malm et al. (2019) study does not provide as a part of their publication the specific input values to the equation to calculate the contrast of distance associated with the available public preference studies ( e.g., sight paths from the images), nor do the preference studies present or make publicly available these data in their publications. In the absence of additional studies or publicly available data to further evaluate the contrast of distance methodology, the EPA is unable to consider contrast of distance as an alternative to estimated light extinction in this reconsideration, although we note that it may be appropriate to evaluate it more closely in future reviews.
In reaching conclusions regarding the appropriate indicator for the visibility index, the 2022 PA specifically notes “that limited new research is available on methods of characterizing visibility or on how visibility is valued by the public, such as visibility preference studies. Thus, while limited new research has further informed our understanding of the influence of atmospheric components of PM2.5 on light extinction, the available evidence to inform consideration of the public welfare implications of PM-related visibility impairment remains relatively unchanged” (U.S. EPA, 2022b, p. 5–50). The EPA again notes in the proposal that “there are very few studies available that use scene-dependent metrics ( i.e., contrast) to evaluate public preference information, which makes it difficult to evaluate them as an alternative to the light extinction approach” (88 FR 5649–5650, January 27, 2023). To further expand on this statement, the Malm et al. (2019) study does not provide enough information to replicate the results of their contrast of distance approach to allow for a comprehensive evaluation of the potential use of this methodology in considering the results of the public preference studies for determining the target level of protection for visibility.
Some commenters suggests that the methodology could be approximated by simply ensuring that people could always see distant scenic elements, and that characterizing typical average and/or maximal viewing distances cross different geographical areas and regions would be a straightforward Geographical Information Systems (GIS) exercise. The EPA disagrees that this assessment would be straightforward, given the lack of data establishing viewing distances in the available scientific record and the diversity of distance to scenic elements across different areas and regions of the U.S., and finds that this approach is also not practical to adopt in this reconsideration. Finally, while the Malm et al. (2019) study is using an alternative approach for evaluating public preferences and acceptability, we note that this study is evaluating the same public preference studies that have been available for the past several decades. For these reasons, the EPA disagrees with the commenters' allegation that the EPA ignored the findings of the Malm et al. (2019) study and failed to consider the contrast of distance methodology in the 2022 PA and the proposal, and ignored the CASAC's advice to consider this study. The ISA Supplement and the 2022 PA considered the Malm et al. (2019) study, along with the full body of available scientific evidence, and took into account the uncertainties and limitations associated with the evidence for visibility preferences, in reaching conclusions regarding the adequacy of the secondary 24-hour PM2.5 standard (U.S. EPA, 2022b, pp. 5–24–5.25, 5–50).
Several comments in support of revising the secondary 24-hour PM2.5 standard to protect against visibility generally recommend revisions to the elements of the standard and visibility index (indicator, averaging time, form, and level) consistent with those supported by the CASAC and public comments in previous PM NAAQS reviews. Some commenters assert that the EPA's approach in the 2022 PA and in the proposal for this reconsideration did not evaluate options for alternative secondary PM standards and thereby is flawed. We address comments on the elements of a visibility index and a revised standard for visibility effects below.
As an initial matter, the EPA disagrees to the extent commenters are suggesting that the PA is legally required to analyze options for alternative standards. The PA is a document developed by the EPA in order to assist the Administrator and the CASAC in reaching conclusions regarding the adequacy of the current standards, and its scope is determined by the EPA. Moreover, the 2022 PA did assess a wide range of information relevant to the Administrator's decision and considered a range of potential standards.
First, in developing the 2022 PA and in responding to CASAC's advice and recommendations during its review of the 2021 draft PA, the EPA expanded upon its discussion of determining the target level of protection for the visibility index and considered the extent to which the available scientific information would alter regarding the visibility index and the appropriate target level of protection against PM-related visibility effects (U.S. EPA, 2022b, pp. 5–27–5–29). This detailed discussion expands the consideration of the target level of protection for the visibility index presented in the 2020 PA (U.S. EPA, 2020b) and the 2021 draft PA (U.S. EPA, 2021c), neither of which specifically considered the elements of the visibility index in determining the appropriate target level of protection. In Start Printed Page 16330 considering the available information in the 2022 PA, the EPA concluded that the available information continued to provide support for a visibility index with a level of 30 dv, with estimated light extinction as the indicator, a 24-hour averaging time, and a 90th percentile form, averaged over three years.
Additionally, in summarizing the air quality and quantitative information in the proposal for this reconsideration, the EPA further expands upon the discussion added to the 2022 PA related to the target level of protection in terms of a PM2.5 visibility index. In so doing, the EPA considers even more extensively the available public preference studies and quantitative analyses (88 FR 5651–5652, January 27, 2023). In particular, there is a more detailed discussion of the public preference studies, including the levels of impairment determined to be “acceptable” by at least 50 percent of study participants and the methodologies used in the studies, including uncertainties and limitations associated with the methodologies (88 FR 5652, January 27, 2023). In reaching a proposed decision regarding the adequacy of the secondary PM standards, as well as the appropriate target level of protection for the visibility index, the Administrator considered the available scientific evidence and quantitative analyses, as well as judgments about how to consider the range and magnitude of uncertainties that are inherent in the scientific evidence and analyses. In so doing, the Administrator proposed to conclude that the protection provided by a visibility index based on estimated light extinction, a 24-hour averaging time, and a 90th percentile form, averaged over 3 years, set at a level of 30 dv would be requisite to protect public welfare with regard to visibility impairment (88 FR 5660, January 27, 2023).
Having provisionally concluded that it was appropriate to define the target level of protection in terms of a visibility index based on estimated light extinction as described above ( i.e., with a 24-hour averaging time; a 3-year, 90th percentile form; and a level of 30 dv), the Administrator next considered the degree of protection from visibility afforded by the current secondary PM standards. In so doing, he considered the updated analyses of PM-related visibility impairment presented in the 2022 PA (U.S. EPA, 2022b, section 5.3.1.2) and described in more detail in the proposal (88 FR 5656, January 27, 2023), which included estimating light extinction using multiple versions of the IMPROVE algorithm and inclusion of PM10-2.5 data at all sites to allow for better characterization of the influence of the coarse fraction of PM on light extinction. The Administrator noted that the results of the analyses in the 2022 PA were consistent with those from the 2012 and 2020 reviews. He also recognized that, regardless of the IMPROVE equation that was used, the analyses demonstrated that the 3-year visibility metric is at or below 28 dv in all areas meting the current 24-hour PM2.5 standard (88 FR 5657, January 27, 2023). The Administrator also noted that, in their review of the 2021 draft PA, the CASAC stated that “[i]f a value of 20–25 deciviews is deemed to be an appropriate visibility target level of protection, then a secondary 24-hour standard in the range of 25–35 µg/m3 should be considered (Sheppard, 2022a, p. 21 of consensus responses). The Administrator recognized that while the CASAC recommended that additional justification be provided for a visibility index target level of protection of 30 dv, they did not specifically recommend that he choose an alternative level for the visibility index. Therefore, the Administrator considered the available scientific evidence, quantitative information, and the CASAC's advice in reaching his proposed conclusions. The Administrator recognized conclusions regarding the appropriate weight to place on the scientific and technical information, including how to consider the range and magnitude of uncertainties inherent in that information, is a public welfare policy judgment left to the Administrator. As such, the Administrator noted his preliminary conclusion on the appropriate visibility index ( i.e., with a 24-hour averaging time; a 3-year, 90th percentile form; and a level of 30 dv) and his preliminary conclusions regarding the quantitative analyses of the relationship between the visibility index and the current secondary 24-hour PM2.5 standard. In so doing, he proposed to conclude that the current secondary standards provide requisite protection against PM-related visibility effects (88 FR 5661, January 27, 2023).
However, the Administrator additionally recognized that the available evidence on visibility impairment generally reflects a continuum and that the public preference studies did not identify a specific level of visibility impairment that would be perceived as “acceptable” or “unacceptable” across the whole U.S. population. He noted a judgment of a target level of protection, below 30 dv and down to 25 dv, could be supported if more weight was put on the public preference study performed in the Phoenix, AZ, study (BBC Research & Consulting, 2003). As described above, while the Administrator noted that the CASAC did not recommend revising the level of the current 24-hour PM2.5 standard in their review of the 2021 draft PA, they did state that, should an alternative level be considered for the visibility index, revisions to the secondary 24-hour PM2.5 standard should also be considered (Sheppard, 2022a, p. 21 of consensus responses). Thus, the Administrator solicited comment on the appropriateness of a target level of protection for visibility below 30 dv and down as low as 25 dv, and of revising the level of the current secondary 24-hour PM2.5 standard to a level as low as 25 µg/m3 (88 FR 5662, January 27, 2023), and the Administrator considered these public comments in reaching his final decision on the secondary standards. Thus, the EPA disagrees that the 2022 PA and the proposal did not adequately consider options for revising the secondary PM NAAQS.
With regard to the elements of the visibility index, in considering the adequacy of the current secondary 24-hour PM2.5 standard to protect against visibility impairment, as described in the proposal (88 FR 5658–5660, January 27, 2023), the Administrator first defined an appropriate target level of protection in terms of a PM visibility index. In considering the information available in this reconsideration and the CASAC's advice, the Administrator proposed to conclude that the protection provided by a visibility index based on estimated light extinction, a 24-hour averaging time, and 90th percentile form, averaged over 3 years, set at a level of 30 dv, would be requisite to protect public welfare with regard to visibility impairment (88 FR 5660, January 27, 2023).
In defining this target level of protection, the Administrator first considered the indicator of such an index. He noted that, given the lack of availability of methods and an established network for directly measuring light extinctions, a visibility index based on estimates of light extinction by PM2.5 components derived from an adjusted version of the original IMPROVE algorithm would be most appropriate, consistent with the 2012 and 2020 reviews. As described in the proposal (88 FR 5649, January 27, 2023) and above (section V.A.2), the IMPROVE algorithm estimates light extinction using routinely monitored components of PM2.5 and PM10–2.5, along with estimates of relative humidity. The Start Printed Page 16331 Administrator, while recognizing that some revisions to the IMRPOVE algorithm were newly available in the 2020 review, noted that the fundamental relationship between ambient PM and light extinction has changed very little and the different versions of the IMPROVE algorithms can appropriately reflect this relationship across the U.S. (88 FR 5658–5659, January 27, 2023). As such, he judged that defining a target level of protection in terms of estimated light extinction continues to be a reasonable approach in this reconsideration.
Some commenters who criticized the EPA's interpretation and application of the Malm et al. (2019) study also contend that an indicator based on the contrast of distance would be a significant improvement over the current indicator for the visibility index and would more accurately evaluate public preferences. However, as described in the 2022 PA (U.S. EPA, 2022b, section 5.3.1.1), while scene-dependent metrics, such as contrast, may be useful alternative predictors of preferences compared to universal metrics like light extinction, there are a very limited number of studies that use such metrics to evaluate public preferences of visibility impairment and there is a lack of scientific evidence that supports one metric over another. Moreover, the EPA finds that even if the Administrator agreed that the contrast of distance methodology was an improvement over light extinction, there is insufficient information available to evaluate and adopt contrast of distance as an indicator for a national visibility target at this time. While, in its review of the 2021 draft PA the CASAC suggested that the EPA consider this method in developing the secondary PM standards, the CASAC also noted that “more extensive technical evaluation of the alternatives for visibility indicators and practical measurement methods” is needed to inform future reviews of the secondary PM standards (Sheppard, 2022a, p. 22 of consensus responses). The CASAC did not recommend using a different indicator for this reconsideration, with the majority of CASAC members reiterated past advice recommending development of a visibility FRM for a directly measured PM2.5 light extinction indicator (Sheppard, 2022a, p. 22 of consensus responses), a recommendation that was supported by other public commenters as well, and the minority of the CASAC suggested that such an FRM is not necessary. For these reasons, the EPA does not consider it feasible or appropriate to define the visibility index in terms of a contrast of distance indicator at this time.
With regard to averaging time, some commenters suggested to the EPA that a secondary standard with a different form than the primary standard may be a more relevant for welfare effects. While they do not recommend a specific alternative form, the commenters point to CASAC advice in past reviews where the CASAC stated that a subdaily standard based on daylight hours better reflects visibility impairment.
In defining the characteristics of a visibility index, the EPA continues to believe that a 24-hour averaging time is reasonable. This is in part based on analyses conducted in the 2012 review that showed relatively strong correlations between 24-hour and subdaily ( i.e., 4-hour average) PM2.5 light extinction (88 FR 5659, January 27, 2023; 85 FR 82740, December 18, 2020; 78 FR 3226, January 15, 2013), indicating that a 24-hour averaging time is an appropriate surrogate for the subdaily time periods relevant for visual perception. The EPA believes that these analyses continue to provide support for a 24-hour averaging time for the visibility index in this reconsideration. The EPA also recognizes that the longer averaging time may be less influenced by atypical conditions and/or atypical instrument performance (88 FR 5659, January 27, 2023; 85 FR 82740, December 18, 2020; 78 FR 3226, January 15, 2013). When taken together, the available scientific information and updated analyses of calculated light extinction available in this reconsideration continue to support that a 24-hour averaging time is appropriate when defining a target level of protection against visibility impairment in terms of a visibility index.
Moreover, the EPA disagrees with commenters that a secondary PM2.5 standard with a 24-hour averaging time does not provide requisite protection against the public welfare impacts of visibility impairment. At the time of the 2012 review, the EPA recognized that hourly or subdaily ( i.e., 4- to 6-hour) averaging times, within daylight hours and excluding hours with high relative humidity, are more directly related to the short-term nature of visibility impairment and the relevant viewing periods for segments of the viewing public than a 24-hour averaging time. At the time of the 2012 review, the EPA agreed that a subdaily averaging time would generally be preferable. However, the Agency noted significant data quality uncertainties associated with the instruments that would provide hourly PM2.5 mass concentrations necessary to inform a subdaily averaging time. These uncertainties, as described in the 2012 review, included short-term variability in hourly data from available continuous monitoring methods, which would prohibit establishing a subdaily averaging time (78 FR 3209, January 15, 2013). For all of these reasons, and consistent with the 2020 review, the EPA continues to believe that a subdaily averaging time is not supported by the information available in this reconsideration.
With regard to the form of the visibility index, some commenters contend that the form used in evaluating visibility impairment is not appropriate. First, commenters contend that the EPA incorrectly stated that the CASAC did not provide advice on the 3-year, 90th percentile form of the visibility index and that the CASAC specifically recommended that the EPA further justify the metric and form, and by not doing so, the proposal arbitrarily departs from the CASAC's recommendations. The commenters also contend that the EPA fails to explain how averaging the form over three years is protective given that the public does not perceive visibility in three-year averages.
We disagree with the commenters that the EPA departed from the CASAC's recommendations that “[t]he final PA should provide a robust justification for the daily light extinction percentile used in the analysis” (Sheppard, 2022a, p. 22 of consensus responses). In this statement, the CASAC did not make explicit recommendations for revisions to the form of the visibility index, as the commenters assert, but rather requested additional justification for the percentile selected for the visibility index in the 2022 PA. In response to the CASAC's recommendation after reviewing the 2021 draft PA, the EPA included a new section in the 2022 PA that explicitly discusses the elements ( i.e., indicator, averaging time, form, and level) of the visibility index, including additional justification for the conclusions regarding the appropriate elements for the index (U.S. EPA, 2022b, pp. 5–27–5–29). In so doing, the 2022 PA recognizes that there is no new information available in this reconsideration to inform selection of an alternative form of the visibility index, and therefore, relied on the analyses presented in the 2010 UFVA that evaluated the different statistical forms of the visibility index. The 2022 PA also discusses the approach to improving visual air quality in Federal Class I areas as a part of the Regional Haze Program (U.S. EPA, 2022b, p. 5–28). Furthermore, as reflected in responding to public comments below, and in Start Printed Page 16332 reaching his final conclusions in section V.B.4 below, the Administrator further considers the available scientific and quantitative information, the CASAC's advice, and public comments in informing his final conclusions regarding the appropriate target level of protection for the visibility index. With regard to the commenters' assertion that the EPA did not justify why averaging the form over three years is protective, we agree with the commenters that people do not perceive visibility impairment in three year averages. As described in the 2022 PA, visibility-related effects and perceived impairment are often associated with short-term PM concentrations, and therefore, the focus of the visibility analyses is centered on the adequacy of the 24-hour PM2.5 standard (U.S. EPA, 2022b, p. 5–29). However, as described in the 2022 PA, the 3-year average form provides stability from the occasional effect of inter-annual meteorological variability that can result in unusually high pollution levels for a particular year (U.S. EPA, 2022b, p. 5–28). Occasional meteorological variability is of particular concern for the visibility index, which can be impacted by not only PM concentrations in ambient air but also relative humidity. The D.C. Circuit has previously recognized that it is legitimate for the EPA to consider overall stability of the standard and its resulting promotion of overall effectiveness of NAAQS control programs in setting a standard. See American Trucking Ass'ns v. Whitman, 283 F.3d 355, 375–76 (D.C. Cir. 2002). The 2022 PA concluded that the available information continues to provide support for a 90th percentile form, averaged over three years, and the inclusion of additional justification for the elements of the visibility index responds to the CASAC's recommendation (U.S. EPA, 2022b, section 5.3.1.2).
Some commenters suggest that the 90th percentile form is too low and would result in 36 days being excluded annually, presuming that the public only finds it objectionable when visibility is worse than the standard on 37 or more days per year. The commenters also contend that the EPA's approach of using a 90th percentile form for the visibility index is inconsistent with the goals of the Regional Haze Program. In so doing, the commenters note that the Regional Haze Rule focuses on improving conditions on the worst days, while they argue that a 90th percentile form for the visibility index would ignore the 36 worst visibility days, rather than identifying them and reducing pollution on those days.
In reaching conclusions regarding the appropriate form of the visibility index, the EPA is following the same approach employed in past reviews of the secondary PM NAAQS, including those in the 2012 and 2020 rulemakings. In reaching conclusions regarding the appropriate form of the visibility index in the 2011 PA, the EPA considered the percentile forms of the visibility index assessed in the 2010 PA ( i.e., 90th, 95th, 98th) along with the approach for improving visual air quality under the Regional Haze Program. In so doing, the 2011 PA notes that the Regional Haze Program targets the 20% most impaired days for improvements in visual air quality in Federal Class I areas ( i.e., the days more impaired than the 80th percentile). The 2011 PA recognized that to increase the likelihood of improving visual air quality on the worst days, the form of the visibility index should be set well above the 80th percentile. The 2011 PA further concluded that a 90th percentile form would represent the median of the distribution of the 20% most impaired days, and meeting a visibility index with a 90th percentile form would mean that 90% of the days have visual air quality that is at or below the level of the visibility index and would reasonably expected to lead to improvements in visual air quality for the 20% most impaired days (U.S. EPA, 2011, p. 4–59). The 2022 PA noted that there is no new information from public preference studies that would inform the Administrator's consideration of the appropriate form for the visibility target index, and reached conclusions consistent with those of 2011 PA. However, as discussed below, the EPA disagrees that a focus on the 90th percentile “ignores” any days with worse visibility. It is possible to examine past patterns of air quality to judge the relationship between the 90th percentile and higher percentiles, and to assess whether achieving a 90th percentile visibility target will also result in air quality improvements, where necessary, at higher percentiles. Based on its assessment of past air quality and potential alternative percentiles for the form, the EPA judged that a 90th percentile would appropriately achieve improved air quality both above and below that percentile.
Some commenters suggest that the analyses conducted in the 2010 UFVA are based on a different metric than the 24-hour average being considered in the reconsideration, that the analyses are outdated and irrelevant. Therefore, the commenters assert that relying on the analyses in the 2010 UFVA is not a rational justification for the use of a 90th percentile for the visibility index in this reconsideration. Moreover, these commenters state that, in past reviews, both the EPA and the CASAC have considered and recommended a 98th percentile form, but the proposal does not consider the 98th percentile.
Start Printed Page 16333These commenters assert that the 2010 UFVA was not considering the same metric under consideration here. However, the EPA was citing to the 2010 UFVA for the conclusion that there are correlations between different statistical forms of the visibility index. To confirm whether these correlations occur under recent air quality, we conducted additional air quality analyses evaluating the visibility index using the current percentile form ( i.e., 90th) and two alternative forms ( i.e., 95th and 98th).[172] While a higher percentile form would further limit the number of days with peak PM-related light extinction, the analyses confirm that a 90th percentile form is effective in limiting visibility impairment at higher percentiles. Based on these analyses, depending on which version of the IMPROVE equation is used to estimate light extinction, the differences in the 3-year averages of estimated light extinction for the 90th, 95th, and 98th percentile forms are small. For example, in areas that meet the current 24-hour PM2.5 standard, for light extinction estimated using the original IMPROVE equation, all sites have light extinction estimates for a 90th percentile form at or below 26 dv, for a 95th or 98th percentile form at or below 29 dv.[173] In most locations, when estimating light extinction based on the original IMPROVE equation, the difference between a 95th or 98th percentile form and a 90th percentile form is generally less than 3 dv.[174] As noted in previous reviews, a change of 1 to 2 dv in light extinction under many viewing conditions will be perceived as a small, but noticeable, change in the appearance of a scene, regardless of the initial amount of visibility impairment (88 FR 5657, January 27, 2023; U.S. EPA, 2004b; U.S. EPA, 2010b). Thus, differences between a 90th percentile form and a 95th or 98th percentile form remain small, and for any of these forms of the visibility index, the estimated light extinction based on the original IMPROVE equation in areas meeting the current secondary 24-hour PM2.5 standard is below the upper end of the range of the levels considered for the visibility index ( i.e., below 30 dv).
Some commenters disagree with the EPA's proposed conclusion that a level of 30 dv is appropriate for the visibility index and support a lower level in order to provide increased protection against visibility impairment. Commenters who support a revised level for the visibility index state that a target level of protection of 30 dv would mean that less than 10% of participants in the public preference studies, other than the Washington, DC, study, would accept visibility conditions above 29 dv. These commenters further suggest that a 75% acceptability, rather than 50% acceptability, is requisite to protect visibility sources, which would be on average a level of 21 dv when using the light extinction method or 18 dv when using the contrast of distance method. These commenters argue that, based on the available information, a target level of protection for the visibility index of approximately 20 dv would be more appropriate, and therefore, the level of the secondary 24-hour PM2.5 standard should be strengthened to 25 μg/m3 . Other commenters who support a revised level for the visibility index suggest that public preference studies with longer sight paths to distant landscape features or with lower target levels than those in the Washington, DC study, such as the Phoenix study, would support a lower level. These commenters support revising the target level of protection for the visibility index to a 25 dv, and revising the level of the secondary 24-hour PM2.5 standard to a level as low as 25 μg/m3 , suggesting that in low relative humidity environments, 25 dv is consistent with PM2.5 concentrations of less than 25 μg/m3 .
Some commenters state that EPA's justification for setting a target level of protection at the upper end of the 20 to 30 dv range is arbitrary. These commenters state that the EPA's reliance on the standard operating in many regions and circumstances as support for the upper end of the range is irrational and illegal. Moreover, these commenters contend that EPA provided no rational connection between the Regional Haze Program and the proposed decision to set the target level of protection at the upper end of the range. They suggest that the EPA proposed to rely exclusively on the Regional Haze Program to protect visibility in Class I areas and to give visibility in these areas no weight in considering the secondary PM standard and that it is not rational to entirely ignore visibility in Class I areas when setting the secondary standard. These commenters assert that the Regional Haze Program provides no rational basis for a target level of protection at the upper end of the range, nor does the EPA identify one.
Some commenters contend that the EPA failed to justify the adequacy of the current secondary annual PM2.5 standard, noting that the secondary 24-hour and annual PM2.5 standards work together to provide protection against short- and long-term effects of PM2.5 . These commenters point to CASAC comments on the 2021 draft PA and the comments of an individual CASAC member's support for strengthening the secondary annual PM2.5 standard to provide increased protection against climate and materials effects over time. They contend that EPA arbitrarily failed to discuss the secondary annual PM2.5 standard not only in the proposal, but also in the 2022 PA and in the 2020 final decision.
The EPA recognizes that the selection of the target level of protection for the visibility index is fundamentally a public welfare policy judgment for the Administrator. The Administrator is tasked by the CAA to judge when visibility impairment becomes an adverse effect on public welfare. It is clear that visibility impairment can become adverse to public welfare, but the Administrator does not consider that every deciview of impairment is adverse to public welfare. In considering the point at which visibility impairment becomes adverse to public welfare, such that the attainment of the secondary PM NAAQS would prevent the adverse effect, the Administrator gives weight to the public preference studies as to when visibility impairment is unacceptable. At the same time, the Administrator recognizes the limitations of these studies, which have been detailed in the proposal and the 2022 PA. Similarly, the EPA discussed the Regional Haze program in the proposal to highlight that there is a distinct program to protect against visibility impairment in Class I areas, and the existence of that program is relevant to the Administrator's judgment about the level of visibility impairment that is adverse to public welfare under CAA 109(d), because in determining what is requisite the Administrator is primarily considering visibility impairment outside of Class I areas. Start Printed Page 16334
In considering how to use the results of the public preference studies, the Administrator concludes that a 50th acceptability criterion is an appropriate tool. The Administrator's task is to set standards that are neither more stringent nor less stringent than necessary, and a 50% acceptability criterion seems most appropriate to use in judging when visibility impairments become adverse, because it should more closely represent when the median person would find the impairment to be adverse. The Administrator notes this conclusion is consistent with the approach adopted in the Denver study by Ely et al. (1991) where the 50% acceptability criterion for urban visibility was first presented. This study discussed the use of the 50% acceptability criteria as a reasonable basis for setting a standard to protect visibility in urban areas. In doing so, Ely et al. (1991) noted that the 50% acceptability criterion divided the slides into two groups—those judged acceptable and those judged unacceptable by a majority of people in the study—and therefore, was reasonable since it defines the point where the majority of the study participants began to judge levels of visibility impairment as unacceptable (Ely et al., 1991).
In considering the appropriate target level of protection, we next look to the available public preference studies, noting that the selecting of the range of 20 to 30 dv for the target level of protection for the visibility index is informed by the 50% acceptability values from these studies. The Denver, CO, (Ely et al., 1991) and British Columbia, Canada, (Pryor, 1996) studies met the 50% acceptability criteria at 20 dv and 19–23 dv, respectively (U.S. EPA, 2022b, Table D–8). As described in the proposal, these studies used photographs that were taken at different times of the day and on different days to capture a range of light extinction levels needed for the preference studies (88 FR 5652, January 27, 2023). Compared to studies that used computer-generated images ( i.e., those in Phoenix, AZ, and Washington, DC) there was more variability in scene appearance in these older studies that could affect preference rating and includes uncertainties associated with using ambient measurements to represent sight path-averaged light extinction values rather than superimposing a computer-generated amount of haze onto the images. When using photographs, the intrinsic appearance of the scene can change due to meteorological conditions ( i.e., shadow patterns and cloud conditions) and spatial variations in ambient air quality that can result in ambient light extinction measurement not being representative of the sight-path-averaged light extinction. Computer-generated images, such as those generated with WinHaze, do not introduce such uncertainties, as the same base photograph is used ( i.e., there is no intrinsic change in scene appearance) and the modeled haze that is superimposed on the photograph is determined based on uniform light extinction throughout the scene. Because of the uncertainties and limitations associated with the Denver, CO, and British Columbia, Canada, the EPA concludes that it is appropriate to place less weight on these studies, and to instead focus on the public preference studies that were designed to reduce these uncertainties and limitations.
In so doing, we focus on the public preference studies that use computer-generated images ( i.e., those in the Phoenix, AZ, and Washington, DC) studies. As described in the proposal, the use of computer-generated images have less variability in scene appears than in those studies that use photographs taken on different days and at different times of the days ( i.e., those in the Denver, CO, study) that would be likely to influence preference rating and introduces uncertainties associated with using ambient measurements to present sight path-averaged light extinction values rather than superimposing a computer-generated amount of haze onto the images (88 FR 5652, January 27, 2023).
The Phoenix, AZ, public preference study (BBC Research & Consulting, 2003) had several strengths compared to some of the other public preference studies. The Phoenix, AZ, study had the largest number of participants (385 in 27 separate focus group sessions) of all of the public preference studies, with a sample group designed to be demographically representative of the Phoenix population at that time. The age range in the Phoenix study was also more inclusive (18–65+), with the distribution of the study participants corresponding reasonably well to the overall age distribution in the 2000 U.S. Census for the Phoenix area (BBC Research & Consulting, 2003). Furthermore, the 21 images used in the Phoenix, AZ, study were developed using the WinHaze software with visual air quality ranging from 15 to 35 dv, and the view was toward the southwest, including downtown Phoenix, with the Sierra Estrella Mountains in the background at a distance of 25 miles. This study had the least noisy preference results, perhaps because a larger, more representative group of participants combined with the use of computer-generated images resulted in the smoother distribution of responses of “acceptable” visual air quality. Based on the EPA's evaluation of the public preference studies in the 2012 review, the 50% “acceptable” criteria was met at approximately 24 dv (U.S. EPA, 2010, Table 2–3).
We also consider the public preferences for the Washington, DC, studies (Abt Associates, 2001; Smith and Howell, 2009). The 2001 Washington, DC study included nine participants, and the 2009 Washington, DC, study replicated the 2001 study with 26 additional participants. Similar to the Phoenix study, the Washington, DC, studies also had the strength of having the 20 images included in the study generated using WinHaze with visual air quality ranging from 9 to 45 dv. The study depicted a scene of a panoramic view of the Potomac River, the National Mall, and downtown Washington, DC. All of the distinct buildings in the scene were within four miles and the higher elevations in the background were less than 10 miles from where the image was taken from the Arlington National Cemetary in Virginia. The 50% “acceptable” criteria was met at approximately 29 dv (U.S. EPA, 2010, Table 2–3).
As described in more detail in the proposal, visibility preferences can vary by location, and such differences may arise based on the differences in the cityscape scene that is depicted in the images (88 FR 5652, January 27, 2023). In considering the geographical differences between the public preference studies, we recognize that the methodological differences between the studies may influence the resulting “acceptable” level of visibility impairment. In the Phoenix, AZ, study, the image depicted mountains in the background and urban features in the foreground, whereas the Washington, DC, study depicted nearby buildings in the image without mountains in the distance. As an initial matter, we note that the object of interest to the study participant could differ across the studies based on the scenes included in the images being evaluated—with the mountains being of greater interest in the images in the Phoenix, AZ, study, despite also depicting buildings that are similar to those shown and presumed to be of interest in the images in the Washington, DC, study (88 FR 5652, January 27, 2023). We also agree with the commenters that the distance between the object of interest and the camera is an important consideration in Start Printed Page 16335 evaluating the public preference studies. Objects at greater distances from the camera location (such as those in the Phoenix, AZ, study which had a maximum distance of 42 km (U.S. EPA, 2022b, Table D–8)) have a greater sensitivity to light extinction, which alone could explain differences in preferences but coupled with an object of greater interest results in lower acceptable levels of visibility impairment. Conversely, objects at closer distances from the camera location (such as those in the Washington, DC, study which had a maximum distance of 8 km (U.S. EPA, 2022b, Table D–8)) have less sensitivity to light extinction, which coupled with objects of interest (compared to the mountainous views in the Phoenix, AZ, study) result in higher acceptable levels of visibility impairment. These studies clearly demonstrate that there are differences in the public preferences across the studies depending on the images that are used, in particular the object of interest to the study participant depicted in the image and the distance of the sight path to the object, and that such differences can influence preference results.
However, we note that these uncertainties and limitations have persisted from past reviews, and there is very little new information to inform conclusions regarding the interpretation of these results with regard to the target level of protection. In selecting a target level of protection, and in considering the CASAC's advice in their review of the 2021 draft PA and public comments, we conclude that it is appropriate to consider the information from the public preference studies in Washington, DC, and Phoenix, AZ, and in so doing, that it is appropriate to place weight on both of these studies in reaching conclusions on the appropriate target level of protection. The EPA recognizes that the scenes depicted in these two studies are different and may influence public preferences of visibility impairment, but notes these studies can be considered together as providing information about different areas across the U.S. with variations in the scenes that people are likely to most commonly encounter. The scene depicted in the images used in the Washington, DC, study have a mix of buildings, landmarks, and open space. On the other hand, the scene depicted in the Phoenix, AZ, study included a mix of buildings in the foreground and with more distant mountains in the background. The Administrator considers it appropriate to consider these studies together because in combination, they provide a greater diversity of scenes, which is more likely to be representative of scenes people typically experience around the country ( e.g., not only in eastern metropolitan statistical areas, but also in western areas with different vistas). In considering these two studies together, the EPA recognizes that, first, the “object of interest” is a subjective judgment left to the participants of the public preference studies, and second, the images in these two studies may differ in terms of sensitivity to changes in light extinction because of the distance between the object of interest in the scene and the camera. As noted by the public commenters, the sight path for the images in the public preference studies is an important consideration in reaching conclusions regarding the appropriate target level of protection for the visibility index. In addition, the Administrator judges that giving weight to multiple studies is a more appropriate approach than focusing on a single study, particularly where the study design (including the representativeness of the participants and the scenes depicted in the images) may be important for interpreting the results of the public preference studies for informing conclusions regarding the visibility index. Given these considerations and taking into consideration public comments on the target level of protection for the visibility index, the Administrator recognizes that it is more appropriate to consider a broader range of public preferences, reflecting a broader range of scenes, by putting significant weight on both the Washington, DC, and Phoenix, AZ, studies. In so doing, he reaches the conclusion that it would be appropriate to identify secondary PM standards that generally limit visibility impairment to a level between the two studies.
The Administrator next considers what target level of protection would be appropriate based on the available information from these public preference studies. He first recognizes that, in the 2012 and 2020 final decisions, the then-Administrators selected a target level of protection of 30 dv, based on the upper end of the range. In so doing, the then-Administrators judged that it was appropriate to place more weight on the uncertainties associated with the public preference studies in reaching their conclusions. However, in this reconsideration, the current Administrator, while continuing to recognize that substantial uncertainties remain and that there is relatively limited new information regarding public preferences of visibility impairment, judges that it is important to balance the weight placed on uncertainties with the strength of the scientific evidence. As such, the Administrator concludes that it is appropriate to consider a target level of protection within the range of 20 to 30 dv. He further concludes that in selecting a target level within that range it is appropriate to place weight on both the mid-point of the range, as supported by the study in Phoenix, AZ, as well as the upper end, as supported by the Washington, DC, study. The Administrator notes that these two studies both employ similar methodologies that are subject to fewer uncertainties than older public preference studies (including their use of WinHaze to reduce uncertainties in the preference solicitations) although he notes that the Phoenix, AZ, study yielded the best results of the four public preference studies in terms of the least noisy preference results and the most representative selection of participants. Furthermore, he notes the differences between the scenes used for each study and finds that consideration of these studies together is more appropriate in selecting a national target for visibility protection than considering either study alone. Thus, in considering this information, along with the uncertainties and limitations of the public preference studies, the Administrator judges that it would be appropriate to select a target level of protection based on placing equal weight on the upper end of the range ( i.e., 30 dv) and the middle of the range ( i.e., 24 dv based on the Phoenix, AZ, study) in order to identify a nationwide target for protection against visibility impairment. In so doing, the Administrator concludes that a visibility index with a target level of protection of 27, defined in terms of estimated light extinction, with a 24-hour averaging time and a 3-year, 90th percentile form, would provide adequate protection against PM-related visibility effects on public welfare. Such a target level of protection balances the information from two key studies reflecting different participant preferences for different vistas in different parts of the country, appropriately weighting both near-field and more distant landscape features that may be of importance to public perceptions of visibility.
The Administrator notes that the available evidence indicates that the relationship between PM and light extinction is complex, depending on factors such as PM composition, size fraction, and age of the particles in ambient air, as well as relative Start Printed Page 16336 humidity. These factors can vary across the country based on differences in regional influences, as well as meteorological conditions that can vary spatially and temporally in different areas. The Administrator also recognizes that this variability, coupled with the age of the PM depending on the distance from the source to the monitor location, also complicates the selection of which IMPROVE equation is most appropriate in different areas, although he notes that different IMPROVE equations will yield similar, but not identical, results. In so doing, the Administrator takes note of the figures presented in the 2022 PA, which depict the comparisons using the original IMPROVE equation (Figure 5–3), the revised IMPROVE equation (Figure 5–4), and the Lowenthal & Kumar equation (Figure 5–6), as well as the estimated light extinction values for the three different equations presented in Table D–7.
The Administrator notes that when light extinction is calculated using the original IMPROVE equation, all 60 sites have 3-year visibility metrics below 28 dv, 58 sites are at or below 25 dv, 26 sites are at or below 20 dv, and of the two sites above 25 dv one is at 26 dv and the other has a 24-hour PM2.5 design value of 56 μg/m[3] ( i.e., well above the current 24-hour standard). Results are similar for other IMPROVE equations.[175] Based on these analyses, and consistent with the results of similar analyses in the 2012 review and the 2020 PA, the Administrator concludes that the current secondary 24-hour PM2.5 standard, with its level of 35 μg/m3 , maintains the visibility index below 27 dv, and in fact, the current standard maintains air quality such that many areas have visibility index values that range between 15 and 25 dv for all three IMPROVE equations. In the areas that meet the secondary 24-hour PM2.5 standard, all locations were below 27 dv when using the original and revised IMPROVE equation and all but three locations were at or below 27 dv when using the Lowenthal & Kumar IMPROVE equation. Three locations (two in California and one in Utah) had air quality that was at 28 dv when the Lowenthal & Kumar IMPROVE equation was used. As described in more detail in section V.A.1.3, we recognize that there are differences in the inputs for the three IMPROVE equations that can influence the resulting estimated light extinction values. The higher multiplier for converting OC to OM in the Lowenthal & Kumar IMPROVE equation ( i.e., a multiplier of 2.1) may be more appropriate in more remote locations where there is more aged and oxygenated organic PM than in urban locations. The three locations with air quality at 28 dv are all in urban areas (downtown Los Angeles, CA; Rubidoux, CA; Salt Lake City, UT) and tend to have higher levels of nitrate and OC, especially during the wintertime when peak PM2.5 concentrations typically occur. In these locations, it may be more appropriate to use either the original or revised IMPROVE equation, which have multipliers of 1.4 and 1.8, respectively, in order to refine the inputs such that estimated light extinction in these locations is more accurately characterized based on site-specific characteristics.
We also note that the four areas that exceed the secondary 24-hour PM2.5 standard also generally had air quality that was below 27 dv in terms of the visibility index, with only two locations experiencing a visibility index above 27 dv. One location that exceeds the secondary 24-hour PM2.5 standard had a visibility index of 29 dv using the original IMPROVE equation, while two locations were 30 and 32 dv using the Lowenthal & Kumar IMPROVE equation. We believe attainment and maintenance of the secondary 24-hour PM2.5 standard will result in improved air quality in these areas, such that the visibility index values for these areas will decrease even further.
The Administrator recognizes that in concluding that it is appropriate to identify secondary PM standards that generally limit visibility impairment to as low as 27 dv in terms of the visibility index, the current secondary PM standards continue to provide protection against visibility impairment associated with a visibility index as low as, or even lower than, 27 dv. In so doing, he notes that when meeting the current 24-hour PM2.5 standard, all sites have a visibility index at or below 27 dv with the original and revised IMPROVE equations, and all but three sites at or below 27 dv with the Lowenthal and Kumar IMPROVE equation. Furthermore, the Administrator notes that this conclusion is consistent with the CASAC's advice who, in their review the 2021 draft PA, stated that “[i]f a value of 20–25 deciviews is deemed to be an appropriate visibility target level of protection, then a secondary 24-hour PM2.5 standard in the range of 25–35 μg/m3 should be considered” (Sheppard, 2022a, p. 21 of consensus responses).
Thus, the Administrator concludes that weight on both the upper end of the range of target levels of protection for the visibility index identified in previous reviews and the mid-point of the range, as presented by the Phoenix, AZ, public preference study, and focusing on a target level of protection of 27 dv, he still judges the current secondary 24-hour PM2.5 standard requisite to achieve that target because the standard generally maintains the visibility index at or below 27 dv such that more stringent standards are not warranted.
The EPA agrees with the commenters that the secondary PM standards work together to provide protection against short- and long-term effects of both fine and coarse particles (U.S. EPA, 2022b, section 5.5; 88 FR 5661, January 27, 2023). However, the EPA disagrees with commenters that we failed to discuss the secondary annual PM2.5 standard in the proposal, 2022 PA, and the 2020 final notice and that we failed to justify the adequacy of the secondary annual PM2.5 standard. As described in the 2022 PA and the proposal, we recognize that PM2.5 is the size fraction of PM responsible for most of the visibility impairment in urban areas (U.S. EPA, 2022b, section 5.3.1.2; 88 FR 5654, January 27, 2023). Analyses in the 2019 ISA found that mass scattering from PM10–2.5 was relatively small (less than 10%) in the eastern and northwestern U.S., whereas mass scattering was much larger in the Southwest (more than 20%), particularly in southern Arizona and New Mexico (U.S. EPA, 2019, section 13.2.4.1, p. 13–36). Given the relationship between visibility and PM2.5 along with the short-term nature of visibility effects, we focus more on the adequacy of the secondary 24-hour PM2.5 standard for providing protection against visibility impairment (U.S. EPA, 2022b, section 5.3.1.2; 88 FR 5653, January 27, 2023). In reaching his proposed conclusions, the Administrator clearly states that he “recognizes that the current suite of secondary standards ( i.e., the 24-hour PM2.5, 24-hour PM10, and annual PM2.5 standards) together provide . . . control for both fine and coarse particulates and long- and short-term visibility and non-visibility ( e.g., climate and materials) effects related to PM in ambient air” (88 FR 5661, January 27, 2023). Thus, by explaining how the secondary standards work together to provide protection from adverse effects, why we focus on the secondary 24-hour PM2.5 standard as Start Printed Page 16337 most relevant to visibility impairment, and how the Administrator selected the target level of protection for the visibility index, we have addressed the CASAC's request to support the proposed decision to revise the secondary 24-hour PM2.5 standard while retaining the secondary annual PM2.5 standard. The commenters also cite to an individual CASAC member's comments for the review of the 2021 draft PA who stated “[f]or the limited scope of this reconsideration review, I see no reason to not simply set the Secondary equal to the Primary PM Standards, whatever they may be” (Sheppard, 2022a, p. A–3). This CASAC member did not provide a supporting rationale for revising the secondary standards to levels equal to the primary standards. Although areas across the country are required to attain both the primary and secondary PM2.5 standards so air quality is unaffected by the Administrator's decision not to revise the secondary standards to be equal to the primary standards, as described in responding to comments above, the CAA provisions require the Administrator to establish secondary standards that, in the judgment of the Administrator, are requisite to protect public welfare from known or anticipated adverse effects associated with the presence of the pollutant in ambient air. In so doing, the Administrator seeks to establish standards that are neither more nor less stringent than necessary for this purpose. The Act does not require that standards be set at a zero-risk level, but rather at a level that reduces risk sufficiently so as to protect the public welfare from known or anticipated adverse effects. The final decision on the adequacy of the current secondary standards is a public welfare policy judgment to be made by the Administrator. In reaching his proposed and final decisions regarding the adequacy of the current secondary PM standards, the Administrator considered the available scientific information and analyses about welfare effects, and associated public welfare significance, as well as judgments about how to consider the range and magnitude of uncertainties that are inherent in the scientific evidence and analyses. In so doing, the Administrator concluded that the currently available scientific evidence and quantitative analyses, including uncertainties and limitations, do not call into question the adequacy of the current secondary PM standards and that the current secondary PM standards should be retained, without revision. The Administrator's judgments and decisions on the primary and secondary standards are independent and consider different aspects of the available scientific evidence and information in reaching conclusions regarding the adequacy of the standards in protecting against PM-related health and welfare effects.
4. Administrator's Conclusions
This section summarizes the Administrator's considerations and conclusions related to the current secondary PM2.5 and PM10 standards and presents the rationale for his decision that no change is required for those standards at this time. The CAA provisions require the Administrator to establish secondary standards that, in the judgment of the Administrator, are requisite to protect public welfare from known or anticipated adverse effects associated with the presence of the pollutant in the ambient air. In so doing, the Administrator seeks to establish standards that are neither more nor less stringent than necessary for this purpose. The Act does not require that standards be set at a zero-risk level, but rather at a level that reduces risk sufficiently so as to protect the public welfare from known or anticipated adverse effects. The final decision on the adequacy of the current secondary standards is a public welfare policy judgment to be made by the Administrator. The decision should draw on the scientific information and analyses about welfare effects, and associated public welfare significance, as well as judgments about how to consider the range and magnitude of uncertainties that are inherent in the scientific evidence and analyses. This approach is based on the recognition that the available evidence generally reflects a continuum that includes ambient air exposures at which scientists agree that effects are likely to occur through lower levels at which the likelihood and magnitude of responses become increasingly uncertain. This approach is consistent with the requirements of the provisions of the Clean Air Act related to the review of NAAQS and with how the EPA and the courts have historically interpreted the Act.
Given these requirements, the Administrator's final decision in this reconsideration is a public welfare policy judgment that draws upon the scientific and technical information examining PM-related visibility impairment, climate effects and materials effects, including how to consider the range and magnitude of uncertainties inherent in that information. The Administrator recognizes that his final decision is based on an interpretation of the scientific evidence and technical analyses that neither overstates nor understates their strengths and limitations, or the appropriate inferences to be drawn. In particular, the Administrator notes that the assessment of when visibility impairment is adverse to public welfare requires a public welfare policy judgment informed by available scientific and quantitative information.
In considering the adequacy of the current secondary PM standards in this reconsideration, the Administrator has carefully considered the: (1) Policy-relevant evidence and conclusions contained in the 2019 ISA and 2022 ISA Supplement; (2) the quantitative information presented and assessed in the 2022 PA; (3) the evaluation of this evidence, the quantitative information, and the rationale and conclusions presented in the 2022 PA; (4) the advice and recommendations from the CASAC; and (5) public comments. In the discussion below, the Administrator gives weight to the 2022 PA conclusions, with which the CASAC generally concurred during their review of the 2019 draft PA and 2021 draft PA, as summarized in section IV.B.1 of the 2020 final notice and section V.D.1 of the 2022 proposal, and takes note of key aspects of the rationale for those conclusions that contribute to his decision in this reconsideration. After giving careful consideration to all of this information, the Administrator judges that no change is required for the secondary PM standards at this time.
In considering the 2022 PA evaluations and conclusions, the Administrator takes note of the overall conclusions that the non-ecological welfare effects evidence and quantitative information are generally consistent with what was considered in the 2020 final decision and in the 2012 review (U.S. EPA, 2022b, section 5.5). The scientific evidence for non-ecological welfare effects in this reconsideration is largely the same as that available in the 2019 ISA and 2020 PA. As described in section I.C.5.b above, the 2022 ISA Supplement included a limited number of newly available studies on PM-related visibility effects. This newly available evidence on visibility effects, along with the full body of non-ecological welfare effects evidence assessed in the 2019 ISA, reaffirms conclusions on the visibility, climate, and materials effects recognized in the 2020 final decision and in the 2012 review, including key conclusions on which the standards are based. Further, as discussed in more Start Printed Page 16338 detail above, the updated quantitative analyses of visibility impairment for areas meeting the current standards in the 2022 PA support the adequacy of the current secondary PM standards to protect against PM-related visibility impairment. The Administrator also recognizes that uncertainties and limitations continue to be associated with the available scientific evidence and quantitative information.
With regard to the current evidence on visibility effects, as summarized in the 2022 PA and discussed in detail in the 2019 ISA and ISA Supplement, the Administrator notes the long-standing body of evidence for PM-related visibility impairment. As in previous reviews, this evidence continues to demonstrate a causal relationship between PM in ambient air and effects on visibility (U.S. EPA, 2019a, section 13.2). The Administrator recognizes that visibility impairment can have implications for people's enjoyment of daily activities and for their overall sense of well-being. Therefore, as in previous reviews, he considers the degree to which the current secondary standards protect against PM-related visibility impairment and the degree to which PM-related visibility impairment is adverse to public welfare. In particular, in recognizing the short-term nature of visibility impairment along with the fact that PM2.5 is the size fraction that contributes most to light extinction, the Administrator especially focuses on the adequacy of the current secondary 24-hour PM2.5 standard in providing protection against PM-related visibility effects judged to be adverse. The Administrator also considers the protection provided by the current secondary 24-hour PM2.5 standard against PM-related visibility impairment in conjunction with the Regional Haze Program as a means of achieving appropriate levels of protection against PM-related visibility impairment in urban, suburban, rural, and Federal Class I areas across the U.S. Programs implemented to meet the secondary PM standards, along with the requirements of the Regional Haze Program established for protecting against visibility impairment in Class I areas, would be expected to improve visual air quality across all areas of the country.
As described in the proposal (88 FR 5658, January 27, 2023), the Administrator recognizes that the Regional Haze Program was established by Congress specifically to achieve “the prevention of any future, and the remedying of existing, impairment of visibility in mandatory Class I areas, which impairment results from man-made air pollution,” and that Congress established a long-term program to achieve that goal (CAA section 169A). In adopting section 169, Congress set a goal of eliminating anthropogenic visibility impairment at Class I areas, as well as a framework for achieving that goal which extends well beyond the planning process and timeframe for attaining the secondary PM NAAQS. Recognizing that the Regional Haze Program will continue to contribute to reductions in visibility impairment in Class I areas, consistent with his proposed conclusions, the Administrator concludes that addressing visibility impairment in Class I areas is largely beyond the scope of the secondary PM standards and that setting the secondary 24-hour PM2.5 standard at a level that would remedy visibility impairment in Class I areas would result in standards that are more stringent than is requisite.
In further considering what standards are requisite to protect against adverse public welfare effects from visibility impairment, the Administrator concludes that it is appropriate to use an approach consistent with the approach used past reviews (88 FR 5650, January 27, 2023). He first identifies an appropriate target level of protection in terms of a PM visibility index that takes into account the factors that influence the relationship between PM in ambient air and visibility ( i.e., size fraction, species composition, and relative humidity). He then considers the air quality analyses conducted in the 2022 PA that examine the relationship between the PM visibility index and the current secondary 24-hour PM2.5 standard in locations that meet the current 24-hour PM2.5 and PM10 standards (U.S. EPA, 2022b, section 5.3.1.2).
In reaching conclusions regarding the target level of protection, the Administrator first considers the characteristics of the visibility index and defines its elements (indicator, averaging time, form, and level). With regard to the indicator for the visibility index, the Administrator continues to recognize that, consistent with the conclusions of the 2022 PA and the CASAC's advice in their review of the 2021 draft PA, there is a lack of availability of methods and an established network for directly measuring light extinction. Therefore, the Administrator concludes that it continues to be appropriate to using an index based on estimates of light extinction by PM2.5 components based on the IMPROVE algorithm. In so doing, the Administrator recognizes that the fundamental understanding of the relationship between ambient PM and light extinction has generally changed very little over time; however, several versions of the IMPROVE equation have been developed and evaluated that could be used to estimate light extinction. As at the time of the proposal, the Administrator recognizes that the results of the quantitative analyses in the 2022 PA that examined three versions of the IMPROVE equation indicate that there are very small differences in estimates of light extinction between the equations, and that it is not always clear that one version of the IMPROVE equation is more appropriate for estimating light extinction across the U.S. than other versions of the IMPROVE algorithm (88 FR 5659, January 27, 2023). He also recognizes that the selection of inputs to the IMPROVE equation ( e.g., the multiplier for OC to OM) may be more appropriate on a regional basis rather than a national basis when calculating light extinction, and notes the CASAC's advice that PM-visibility relationships are region specific (Sheppard, 2022a, p. 21 of consensus responses). The Administrator further notes that neither the CASAC nor public commenters recommended a specific IMPROVE equation or an approach for using different IMPROVE equations across the U.S. Therefore, given the absence of a robust monitoring network to directly measure light extinction, the Administrator concludes that light estimated light extinction, as calculated using one or more versions of the IMPROVE algorithms, continues to be the most appropriate indicator for the visibility index.
Having reached the conclusion that estimated light extinction is the appropriate indicator for the visibility index, the Administrator next considers the appropriate averaging time and form of the index. With regard to the averaging time and form, the Administrator notes that in previous reviews, a 24-hour averaging time was selected and the form was defined as the 3-year average of annual 90th percentile values. As at the time of proposal, the Administrator recognizes that the available information continues to provide support for the short-term nature of visibility effects. He further recognizes that no new information is available in this reconsideration to inform his conclusions regarding averaging time, and therefore, he considers past analyses of 24-hour and subdaily PM2.5 light extinction to inform his conclusions on averaging time. As described in the proposal (88 FR 5659, January 27, 2023) and in responding to comments in section V.B.3 above, prior Start Printed Page 16339 analyses demonstrated that there are strong correlations between 24-hour and subdaily ( i.e., 4-hour average) PM2.5 light extinction, indicating that a 24-hour averaging time is an appropriate surrogate for the subdaily time periods associated with when individuals experience visibility impairment and that a longer averaging time may also be less influenced by atypical conditions and/or atypical instrument performance. The Administrator also notes that the CASAC did not provide advice or recommendations with regard to the averaging time of the visibility index, although some public commenters referenced CASAC advice in past reviews that a subdaily standard based on daylight hours would better reflect the public welfare effects of public perceptions of visibility impairment than a 24-hour standard. However, in considering the available scientific and quantitative information, as well as the CASAC's advice in their reviews of the 2019 draft PA and 2021 draft PA, the Administrator concludes that the 24-hour averaging time continues to be appropriate for the visibility index because it is an appropriate surrogate for subdaily time periods and results in a more stable target.
With regard to the form of the visibility index, the Administrator notes the approach in other NAAQS that a multi-year percentile form offers greater stability to the air quality management process by reducing the possibility that statistically unusual indicator values will lead to transient violations of the standard. He recognizes that using a 3-year average provides stability from the occasional effects of inter-annual meteorological variability (including relative humidity) that can result in unusually high pollution levels for a particular year (88 FR 5659, January 27, 2023) and recognizes that a stable standard contributes to the benefits of the NAAQS by ensuring that attainment strategies are designed to address non-transient problems and achieve durable air quality improvements. For these reasons, he concludes that a 3-year average continues to be appropriate.
In considering the percentile that would be appropriate with the 3-year average, the Administrator recognizes that there is very little new information available in this reconsideration to inform selection of an alternative form of the visibility index and that the appropriate form requires the exercise of public welfare policy judgment. In selecting the appropriate target level of protection for the visibility index, the Administrator is required to assess when visibility impairment becomes adverse to public welfare, weighing both the degree of visibility impairment (in dv) and the frequency of such impairment (through the form). As with the mass-based PM air quality standard, the target level of protection for the visibility index must be selected in conjunction with the form to determine the appropriate stringency. In so doing, consistent with approaches in past reviews, the Administrator first notes that the Regional Haze Program targets the 20% most impaired days for improvements in visual air quality in Class I areas, which are the days above the 80th percentile form of the visibility index. The Administrator concludes that a percentile form set at the 80th percentile would not be likely to sufficiently improve visual air quality on the worst days based on the visibility index. In considering the information available in past reviews regarding the form of the visibility index, as well as the analysis of alternative forms based on recent air quality discussed above, the Administrator notes that a 90th percentile form would represent the median of the distribution of the 20% most impaired days, and meeting a visibility index with a 90th percentile form would reasonably be expected to lead to improvements in visual air quality for days both above and below the 90th percentile (88 FR 5660, January 27, 2023). In reaching his conclusion that a 90th percentile would appropriately achieve improved air quality both above and below that percentile, the Administrator took into consideration assessments of air quality data and potential alternative percentiles for the form. The Administrator further notes that, consistent with the conclusions in the 2011 PA and 2020 PA, the 2022 PA concluded that there is no new information from public preference studies that would suggest that a 90th percentile form is not appropriate. The Administrator also considers air quality analyses described above in responding to public comments regarding the percentile form of the visibility index. In particular, the Administrator notes that while a higher percentile form ( i.e., 95th or 98th) would somewhat further limit the number of days with peak PM-related light extinction, the differences in the 3-year averages of estimated light extinction for the 90th, 95th, and 98th percentile forms are small. For example, he notes that for the original IMPROVE equation, in areas that meet the current 24-hour PM2.5 standard, all sites have light extinction estimates for a 90th percentile form at or below 26 dv, and for a 95th or 98th percentile form light extinction estimates are at or below 29 dv.[176] He further notes that, in most locations when estimating light extinction based on the original IMPROVE equation, the difference between a 95th or 98th percentile form and a 90th percentile form is generally less than 3 dv.[177] Moreover, the Administrator concludes that a 90th percentile form achieves a very high degree of control but appropriately targets the group of worst days, rather than the few very worst days. Based on the available information and these analyses, the Administrator concludes that the information does not indicate that it would be appropriate to consider limiting the occurrence of days with peak PM-related light extinction to a greater degree, nor did the CASAC provide advice or recommendations related to the form of the visibility index. Therefore, the Administrator judges that it remains appropriate to define a visibility index in terms of a 24-hour averaging time and form based on the 3-year average of annual 90th percentile values.
With regard to the level of the visibility index, as at the time of proposal, the Administrator continues to recognize that there is very little new information available to inform his judgment regarding the range of levels of visibility impairment judged to be acceptable by at least 50% of study participants in the visibility preference studies,[178] and therefore, the range of 20 to 30 dv identified in the 2022 PA remains appropriate for considering the level of the visibility index. The Administrator also recognizes that the uncertainties and limitations associated with the public preferences identified in the 2012 and 2020 reviews continue to persist, and that these limitations and uncertainties contributed to the decisions in 2012 and 2020 that a level at the upper end of the range ( i.e., 30 dv) was selected. The Administrator specifically notes that, while the studies Start Printed Page 16340 are methodologically similar, there are a number of factors that can influence comparability across the studies and that the available studies may not capture the full range of visibility preferences in the U.S. population, as described in more detail in section V.D.3 of the 2022 proposal (88 FR 5659–5660, January 27, 2023). The Administrator also notes the CASAC's advice in their review of the 2021 draft PA that there are a limited number of visibility preference studies available to inform the Administrator's judgment regarding the appropriate target level of protection for the visibility index (Sheppard, 2022a, p. 21 of consensus responses). In considering the available information, including uncertainties and limitation, and the CASAC's advice, the Administrator proposed to conclude that it is appropriate to consider a target level of protection for the visibility index within the range of 20 to 30 dv, and that establishing a target level of protection at the upper end of the range was appropriate. In so doing, the Administrator proposed to conclude that the protection provided by a visibility index based on estimated light extinction, a 24-hour averaging time, and a 90th percentile form, averaged over 3 years, set to a level of 30 dv would be requisite to protect public welfare with regard to visibility impairment.
However, at the time of proposal, the Administrator recognized that the available evidence on visibility impairment generally reflects a continuum and that the public preference studies do not provide information about the specific level for which visibility impairment would be “acceptable” or “unacceptable” across the country, and that alternative target levels of protection could be supported. At that time, in soliciting public comments, the Administrator recognized that other interpretations, assessments, and judgments based on the available welfare effects evidence for this reconsideration could be possible (88 FR 5662, January 27, 2023).
With regard to the appropriate target level of protection for the visibility index, the Administrator first notes that while the public preference studies were conducted in several geographical areas across the U.S., and they provide insight into regional preferences for visibility impairment, none of the studies identify a specific level of visibility impairment that would be perceived as “acceptable” or “unacceptable” across the whole U.S. population. He also noted that there have been significant questions about how to set a standard for visibility that is neither overprotective nor underprotective for some areas of the U.S. As described in the proposal (88 FR 5660, January 27, 2023), in establishing the Regional Haze Program to improve visibility in Class I areas, Congress noted that “as a matter of equity, the national ambient air quality standards cannot be revised to adequately protect visibility in all areas of the country.” H.R. Rep. 95–294 at 205. For the reasons noted above, in reaching his proposed decision regarding visibility impairment, the Administrator recognized that he is not seeking to set a standard that would eliminate visibility impairment in Class I areas, but significant uncertainties remain regarding how to judge when visibility impairment becomes adverse to public welfare across the range of daily outdoor activities for Americans across the country.
In reaching final conclusions regarding the available information, along with the CASAC's advice and public comments, the Administrator again considers what constitutes an appropriate target level of protection, and in particular considers whether a target level of protection below 30 dv is warranted. In so doing, he first notes the variability in public preferences of visibility impairment as demonstrated by the available public preferences, which support a range of potential target levels of protection for the visibility index from 20 to 30 dv. He also notes that this range informed the 2012 and 2020 then-Administrators final decisions that a target level of protection at the upper end of the range ( i.e., 30 dv) would be most appropriate, given the uncertainties and limitations associated with the public preference studies. As described in in section V.B.3 above in responding to public comments, the Administrator recognizes that a number of factors can influence public preferences across studies, in particular due to the types of scenes depicted in the images as well as the distances at which the objects of interest are located from the camera. Furthermore, the Administrator recognizes the small number of public preference studies currently available makes precise interpretations of their results challenging for determining a nationally appropriate target level of visibility protection. The Administrator also recognizes that the CASAC, in their review of 2021 draft PA, reiterated that PM-visibility relationships are region-specific based on aerosol composition, and that several public commenters emphasized the importance of the sight path distance in the images when considering how to interpret the public preference studies.
In this reconsideration, the Administrator judges that in determining when visibility impairment becomes adverse to public welfare for purposes of the secondary NAAQS, while continuing to recognize that substantial uncertainties remain and that there is relatively limited new information regarding public preferences of visibility impairment, it is important to balance the weight placed on uncertainties with the strength of the scientific evidence. In so doing, the Administrator first concludes that, consistent with previous reviews and his proposed decision, it remains appropriate to consider a target level of protection within the range of 20 to 30 dv. However, in further considering the available scientific and quantitative information, CASAC advice, and public comments, he further concludes that in selecting a target level within that range it is appropriate to place weight on both the middle of the range, as supported by the study in Phoenix, AZ, as well as the upper end, as supported by the Washington, DC, study. In so doing, he notes that the Washington, DC, and Phoenix, AZ, studies employ similar methodologies that are subject to fewer uncertainties than older public preference studies (including their use of WinHaze to reduce uncertainties in the preference solicitations) although he does note that the Phoenix, AZ, study yielded the best results of the four public preference studies in terms of the least noisy preference results and the most representative selection of participants. Further, the Administrator judges that this approach would take into account scenes that are similar to both the Washington, DC, study and Phoenix, AZ, study, which would be more representative of the “typical” scenes encountered across more areas of the U.S. than an approach that places weight on just one study or on studies conducted in certain geographical areas of the country. In considering this information, along with the uncertainties and limitations of the public preference studies, the Administrator judges that it would be appropriate to select a target level of protection based on placing equal weight on the upper end of the range ( i.e., 30 dv) and the middle of the range ( i.e., 24 dv based on the Phoenix, AZ, study) in order to provide protection against visibility impairment in different geographical areas of the U.S. For these reasons, the Administrator concludes that a visibility index with a target level of protection of 27 dv, Start Printed Page 16341 defined in terms of estimated light extinction, with a 24-hour averaging time and a 3-year, 90th percentile form, would provide adequate protection against PM-related visibility effects. In reaching this conclusion, the Administrator judges that such a target level of protection balances the information from these two key public preference studies in such a way appropriately weighs both near-field and more distant landscape features that may be of importance to public perceptions of visibility.
In further considering the appropriate target level of protection for the visibility index, the Administrator again recognizes the complexity of the relationship between PM and light extinction which is dependent on a number of factors, including PM composition, size fraction, and age of the particles in ambient air, as well as relative humidity. As noted in responding to comments above, these factors can vary geographically across the U.S. and local or regional meteorological conditions can also vary spatially and temporally. These factors are critical inputs to the IMPROVE equation and can influence the resulting estimated light extinction such that it is not a straightforward comparison between estimated light extinction in one area of the country versus another. Moreover, the Administrator recognizes that there is variability in estimated light extinction depending on the version of the IMPROVE equation that is used. As described in more detail in the 2022 PA and the proposal, and in reaching his decisions on the indicator of the visibility index above, the Administrator notes that the 2022 PA concluded that one version of the IMPROVE equation is not more accurate or precise in estimating light extinction, and that difference in locations may support the selection of inputs into the IMPROVE equation or of the appropriate IMPROVE equation to estimate light extinction on a regional basis rather than on a national basis.
In considering the available information, including variations in both public preferences of visibility impairment and estimates of light extinction using one or more IMPROVE equation, as well as the CASAC's advice in their review of the 2019 draft PA and 2021 draft PA and public comments, the Administrator judges that a target level of protection of 27 dv would be appropriate. In so doing, he concludes that a target level of protection above 27 dv would not provide adequate protection against PM-related visibility impairment based on the 50% acceptability values when both the Washington, DC, and Phoenix, AZ, studies are considered. However, he also notes that when considering the 50% acceptability values from studies conducted in different areas of the U.S. and with different scenes and images depicted, the available public preference studies do not provide a “bright line” at and above which visibility impairment is considered adverse to public welfare. He further recognizes that, as discussed just above, there are a number of region-specific factors that can influence light extinction, and thereby influence visibility impairment, as well as variations in public preferences of visibility impairment based on the available studies, that complicate selection of a single target level of protection that would be appropriate for a national visibility index. While the Administrator recognizes that the uncertainties and limitations associated with public preferences of visibility and estimating light extinction have persisted over the last several PM NAAQS reviews, he also recognizes that in reaching conclusions regarding the appropriate target level of protection for the visibility index also involves public welfare policy judgments regarding how to appropriately consider the particular uncertainties around identifying when visibility impairment becomes adverse to public welfare, and the limitations on relying on the public preference studies.
The Administrator also places weight on the high degree of spatial and temporal variability in PM composition and relative humidity across the U.S. in considering a target level of protection. This approach of establishing a target level of protection that takes into account 50% acceptability values from both eastern and western sites is a more appropriate basis for determining the requisite level of protection against known or anticipated adverse effects on public welfare across diverse locations, i.e., a standard that is neither more nor less stringent than necessary nationwide. Specifically, the Administrator judges that a target level of protection for the visibility index focused on maintaining estimated light extinction between the upper end of the range of the target levels of protection ( i.e., 30 dv based on the Washington, DC, study) and the middle of the range ( i.e., 24 dv based on the Phoenix, AZ, study) to be more appropriate for a nationwide standard to protect against visibility impairment compared to a value derived from one location or one type of scene alone. For these reasons, in selecting a target level of protection, the Administrator concludes that a target level of protection somewhere between the upper end and middle of the range is appropriate because he judges that this approach, in conjunction with the Regional Haze program, is sufficient, but not more stringent than necessary, to protect against adverse effects on public welfare. Thus, he concludes a secondary 24-hour PM2.5 NAAQS should be evaluated based on its ability to provide protection against visibility impairment associated with estimated light extinction of 27 dv based on estimated light extinction, a 24-hour averaging time, and a 90th percentile form, averaged over 3 years.
Having concluded that it is appropriate to identify a target level of protection in terms of a visibility index based on estimated light extinction as described above, the Administrator next considers the degree of protection from visibility impairment afforded by the current secondary PM standards. He considers the updated analyses of PM-related visibility impairment presented in the 2022 PA (U.S. EPA, 2022b, section 5.3.1.2) and described in section V.B.1.a of the proposal, and notes that the results of the analyses are consistent with the results from the 2012 and 2020 reviews.
Taking into consideration the full body of scientific evidence and technical information concerning the known and anticipated effects of PM on visibility impairment, the Administrator concludes that the current secondary PM2.5 and PM10 standards are requisite to protect against PM-related visibility impairment. While the inclusion of the coarse fraction had a relatively modest impact on calculated light extinction in the analyses presented in the 2022 PA, he recognizes the continued importance of the PM10 standard given the potential for larger impacts in locations with higher coarse particle concentrations, such as in the southwestern U.S., for which only a few sites met the criteria for inclusion in the analyses in the 2022 PA (U.S. EPA, 2019a, section 13.2.4.1; U.S. EPA, 2022b, section 5.3.1.2).
With regard to the adequacy of the secondary 24-hour PM2.5 standard, the Administrator notes that, in their review of the 2021 draft PA, the CASAC stated that “[i]f a value of 20–25 deciviews is deemed to be an appropriate visibility target level of protection, then a secondary 24-hour PM2.5 standard in the range of 25–35 µg/m3 should be considered” (Sheppard, 2022a, p. 21 of consensus responses). The Administrator recognizes that the CASAC recommended that the Administrator provide additional justification for a visibility index target Start Printed Page 16342 of 30 dv but did not specifically recommend that he choose an alternative level for the visibility index. The Administrator carefully considered the advice of CASAC and the public comments and concluded that a lower target level of visibility was appropriate in order to properly reflect both a broader set of studies and a broader range of vistas that were the subject of those studies. However, in their review of the 2021 draft PA, the CASAC recognized that even a visibility index target in the range of 20–25 dv could still warrant retention of the current secondary 24-hour PM2.5 standard. The Administrator also considers the advice from the CASAC in their review of the 2019 draft PA, who “recogniz[ed] that uncertainties. . .remain about the best way to evaluate” PM-related visibility effects (Cox, 2019b, p. 13 consensus responses). The Administrator considered the CASAC's advice, together with the available scientific evidence and quantitative information, in reaching his conclusions.
The Administrator recognizes that conclusions regarding the appropriate weight to place on the scientific and technical information examining PM-related visibility impairment, including how to consider the range and magnitude of uncertainties inherent in that information, is a public welfare policy judgment left to the Administrator. In reaching his final decision in 2020, the then-Administrator noted that the available evidence regarding visibility effects had changed very little since the 2012 review, specifically recognizing that, as evaluated in the 2019 ISA, there were no new visibility studies that were conducted in the U.S. and there was little new information available with regard to acceptable levels of visibility impairment in the U.S. (85 FR 82742, December 18, 2020). As such, the then-Administrator concluded that the protection provided by a standard defined in terms of a PM2.5 visibility index, with a 24-hour averaging time, a 90th percentiles form averaged over three years, set at a level of 30 dv, was requisite to protect public welfare against visibility impairment (85 FR 82743, December 18, 2020). He also recognized that there was some new information to inform quantitative analyses of light extinction, but that the results of the analyses conducted in the 2020 PA were consistent with those from the 2012 review. The then-Administrator recognized that the analyses demonstrated that the 3-year visibility metric was at or below about 30 dv in all areas that met the current secondary 24-hour PM2.5 standard, and was below 25 dv in most of those areas (85 FR 82743, December 18, 2020). Therefore, the Administrator judged that the secondary 24-hour PM2.5 standard provided sufficient protection for visual air quality of 30 dv, which he judged appropriate (88 FR 82744, December 18, 2020). In this reconsideration, the ISA Supplement evaluated newly available studies on public preferences for visibility impairment and/or development methodologies or conducted quantitative analyses of light extinction. In considering the available scientific and quantitative information, including that newly available in this reconsideration, the current Administrator reached the same preliminary conclusions in the notice of proposed rulemaking regarding the 3-year visibility index and the current secondary PM standards as the then-Administrator in the 2020 final decision. However, in light of public comments on the proposal, the Administrator has further considered the available scientific evidence and information, as well as the CASAC's advice regarding visibility effects in their review of the 2021 draft PA. In so doing, the Administrator judges that it is appropriate to place more weight on certain aspects of the evidence that he had placed less weight on in reaching his proposed conclusions ( i.e., he focused on the both the middle and the upper end of the range of the 50% acceptability values from the available public preference studies). As such, the Administrator notes his conclusion on the appropriate visibility index ( i.e., with a 24-hour averaging time; a 3-year, 90th percentile form; and a level of 27 dv), which takes into account the regional variations in public preferences and equations for estimating light extinction, and his conclusions regarding the quantitative analyses of the relationship between the visibility index and the current secondary 24-hour PM2.5 standard. In so doing, the Administrator concludes that the current secondary standards provide requisite protection against PM-related visibility effects.
With respect to climate effects, as at the time of proposal, the Administrator recognizes that a number of improvements and refinements have been made to climate models since the time of the 2012 review. However, despite continuing research and the strong evidence supporting a causal relationship with climate effects (U.S. EPA, 2019a, section 13.3.9), the Administrator notes that there are still significant limitations in quantifying the contributions of the direct and indirect effects of PM and PM components on climate forcing (U.S. EPA, 2022b, sections 5.3.2.1.1 and 5.5). He also recognizes that models continue to exhibit considerable variability in estimates of PM-related climate impacts at regional scales ( e.g., ~100 km), compared to simulations at the global scale (U.S. EPA, 2022b, sections 5.3.2.1.1 and 5.5). Moreover, the effects of PM on climate are diverse as well as uncertain. Depending on the circumstances, the radiative forcing effects of PM in the atmosphere can vary, such that positive forcing could result in warming of the Earth's surface, whereas a negative forcing could result in cooling (U.S. EPA, 2019a, section 13.3.2.2). The resulting uncertainty leads the Administrator to conclude that the scientific information available in this reconsideration remains insufficient to quantify, with confidence, the impacts of ambient PM on climate in the U.S. (U.S. EPA, 2022b, section 5.3.2.2.1) and that there is not an adequate scientific basis to link attainment of any particular PM concentration in ambient air in the U.S. to specific climate effects. Consequently, the Administrator judges that there is insufficient information at this time to revise the current secondary PM standards or to promulgate a distinct secondary standard to address PM-related climate effects.
With respect to materials effects, the Administrator notes that the available evidence continues to support the conclusion that there is a causal relationship with PM deposition (U.S. EPA, 2019a, section 13.4). He recognizes that deposition of particles in the fine or coarse fractions can result in physical damage and/or impaired aesthetic qualities. Particles can contribute to materials damage by adding to the effects of natural weathering processes and by promoting the corrosion of metals, the degradation of painted surfaces, the deterioration of building materials, and the weakening of material components. While some recent evidence on materials effects of PM is available in the 2019 ISA, the Administrator notes that this evidence is primarily from studies conducted outside of the U.S. in areas where PM concentrations in ambient air are higher than those observed in the U.S. (U.S. EPA, 2019a, section 13.4). Given the limited amount of information on the quantitative relationships between PM and materials effects in the U.S., and uncertainties in the degree to which those effects could be adverse to the public welfare, the Administrator judges that the available scientific information Start Printed Page 16343 remains insufficient to quantify, with confidence, the public welfare impacts of ambient PM on materials and that there is insufficient information at this time to revise the current secondary PM standards or to promulgate a distinct secondary standard to address PM-related materials effects.
Taken together, the Administrator concludes that the scientific and quantitative information for PM-related non-ecological welfare effects ( i.e., visibility, climate, and materials),[179] along with the uncertainties and limitations, supports the current level of protection provided by the secondary PM standards as being requisite to protect against known and anticipated adverse effects on public welfare. For visibility impairment, this conclusion reflects his consideration of the evidence for PM-related light extinction, together with his consideration of updated air quality analyses of the relationship between the visibility index and the current secondary 24-hour PM2.5 standard and the protection provided by the current secondary PM2.5 and PM10 standards. For climate and materials effects, this conclusion reflects his judgment that, although it remains important to maintain secondary PM2.5 and PM10 standards to provide some degree of control over long- and short-term concentrations of both fine and coarse particles, it is appropriate not to change the existing secondary standards at this time and that it is not appropriate to establish any distinct secondary PM standards to address PM-related climate and materials effects at this time. As such, the Administrator recognizes that current suite of secondary standards ( i.e., the 24-hour PM2.5, 24-hour PM10, and annual PM2.5 standards) together provide such control for both fine and coarse particles and long- and short-term visibility and non-visibility ( e.g., climate and materials) effects related to PM in ambient air. His conclusions on the secondary standards are consistent with advice from the CASAC, which noted substantial uncertainties remain in the scientific evidence for climate and materials effects, as well as the majority of public comments on the secondary PM standards. Thus, based on his consideration of the evidence and analyses for PM-related welfare effects, as described above, and his consideration of CASAC advice and public comments on the secondary standards, the Administrator concludes that it is appropriate not to change those standards ( i.e., the current 24-hour and annual PM2.5 standards, 24-hour PM10 standard) at this time.
C. Decision on the Secondary PM Standards
For the reasons discussed above and taking into account information and assessments presented in the 2019 ISA, ISA Supplement, and 2022 PA, advice from the CASAC, and consideration of public comments, the Administrator concludes that the current secondary PM standards are requisite to protect public welfare from known or anticipated adverse effects and is not changing the standards at this time.
VI. Interpretation of the NAAQS for PM
The EPA is finalizing revisions on data calculations in appendix K for PM10 and appendix N for PM2.5 . Revisions to appendix K make the PM10 data handling procedures for the 24-hour PM10 standards more consistent with those of other NAAQS pollutants and codify existing practices. Revisions to appendix N update references to the revision(s) of the standards and change data handling provisions related to combining data from nearby monitoring sites to codify existing practices that are currently being implemented as the EPA standard operating procedures.
A. Amendments to Appendix K: Interpretation of the NAAQS for Particulate Matter
The EPA proposed to modify its data handling procedures for the 24-hour PM10 standard in appendix K to part 50 (88 FR 5662, January 27, 2023). The proposed modifications include: (1) Revising design value calculations to be on a site-level basis, (2) codifying site combinations to maintain a continuous data record, and (3) clarifying daily validity requirements for continuous monitors. The purpose of these modifications is to make the data handling procedures for the 24-hour PM10 standard more consistent with those of other NAAQS pollutants and codify existing practices that are currently being implemented as EPA standard operating procedures.
The EPA received few comments on these proposed appendix K revisions, the majority of which were supportive.
One commenter was not supportive of the proposed appendix K revision to site-level PM10 design values, asserting that it would amount to an imposition of a more stringent PM10 standard due to the potential high bias of FEMs. The EPA disagrees with this assertion because site-level design values would combine data from any high biased FEM with other monitors at the site rather than calculate a monitor-level design value with data solely from that high-biased FEM. The EPA tested the impact of calculating site-level PM10 design values for the 2019–2021 period by assigning the lowest parameter occurrence code as the primary monitor and calculating site-level design values. Most resulting site-level design values were either identical to or in-between the multiple monitor-level design values at the site. Combining data from two or more monitors also has the benefit of increasing the number of valid sample days at many sites. For the 2019–2021 test period, approximately 10% of the sites with more than one monitor went from having multiple invalid design values to a single valid design value.
One commenter was not supportive of a footnote in the preamble of the NPRM stating that in the absence of a designated primary monitor at a given site, the default primary monitor would be one with the most complete data record (88 FR 5662, January 27, 2023). Because the procedure for calculating PM10 design values on a site-level basis being finalized here will require monitoring agencies to designate a primary monitor for each site in their annual network plans (88 FR 5694, January 27, 2023; App. K, 1.0(b)), the EPA agrees with the commenter that this footnote was unnecessary.
Therefore, the EPA is finalizing these appendix K revisions as proposed.
B. Amendments to Appendix N: Interpretation of the NAAQS for PM2.5
The EPA proposed to modify its data handling procedures for the annual and 24-hour PM2.5 standards in appendix N to part 50 (88 FR 5663, January 27, 2023). These proposed revisions include: (1) Updating references to the revisions of the standards rather than stating the specific level, and (2) codifying site combinations to maintain a continuous data record. The purpose of both modifications is to codify existing practices that are currently being implemented as the EPA standard operating procedures.
The EPA received few comments on these revisions in the proposed rule, with most supportive of the appendix N revisions.
Although the EPA did not propose or request comment on this issue, one commenter suggested that appendix N be revised to only allow data from the primary monitor to be used in PM2.5 NAAQS designations asserting that it would add flexibility. The EPA disagrees with the commenter's assertion that this would add flexibility because it could force agencies to run Start Printed Page 16344 their FRMs on a daily schedule or potentially lead to invalid design values if manual sampling interruptions or laboratory issues impact FRM data completeness. This change would also be undesirable because it could reduce by two-thirds the number of days used in calculations for the annual and 24-hour PM2.5 design values at many sites.
Therefore, the EPA is finalizing these appendix N revisions as proposed.
VII. Amendments to Ambient Monitoring and Quality Assurance Requirements
The EPA is finalizing revisions to ambient air monitoring requirements for PM to improve the usefulness of and appropriateness of data used in regulatory decision making. These changes focus on ambient monitoring requirements found in 40 CFR parts 50 (appendix L), 53, and 58 with associated appendices (A, B, C, D, and E). These changes include addressing updates in the approval of reference and equivalent methods, updates in quality assurance statistical calculations to account for lower concentration measurements, updates to support improvements in PM methods, a revision to the PM2.5 network design to account for at-risk populations, and updates to the Probe and Monitoring Path Siting Criteria for NAAQS pollutants. The EPA also took comment on how to incorporate data from next generation technologies into Agency efforts. A summary of the comments received is included in this section.
A. Amendment to 40 CFR Part 50 (Appendix L): Reference Method for the Determination of Fine Particulate Matter as PM2.5 in the Atmosphere—Addition of the Tisch Cyclone as an Approved Second Stage Separator
The EPA proposed a change to the FRM for PM2.5 (40 CFR part 50, appendix L), the addition of an alternative PM2.5 particle size separator to that of the Well Impactor Ninety-Six (WINS) and the Very Shape Cut Cyclone (VSCC) size separators (88 FR 5663, January 27, 2023). The new separator is the TE–PM2.5 C cyclone manufactured by Tisch Environmental Inc.,[180] Cleves Ohio, which has been shown to have performance equivalent to that of the originally specified WINS impactor with regards to aerodynamic cutpoint and PM2.5 concentration measurement. In addition, the new TE–PM2.5 C has a significantly longer service interval than the WINS and is comparable to that of the VSCC separator. Generally, the TE–PM2.5 C is also physically interchangeable with the WINS and VSCC where both are manufactured for the same sampler. The proposed change would allow either the WINS, VSCC, or TE–PM2.5 C to be used in a PM2.5 FRM sampler. As is the case for the WINS and VSCC, the TE–2.5C is now also an approved size separator for candidate PM2.5 FEMs. Currently, the EPA has designated one PM2.5 sampler configured with TE–PM2.5 C separator as a Class II PM2.5 equivalent method and one as a PM10-2.5 equivalent method. Upon promulgation of this change to appendix L, these instruments would be redesignated as PM2.5 and PM10-2.5 FRMs, respectively. Owners of such samplers should contact the sampler manufacturer to receive a new reference method label for the samplers.
The EPA received only one comment regarding this proposed change, which was supportive. Therefore, the EPA is finalizing this change to Appendix L as proposed.
B. Issues Related to 40 CFR Part 53 (Reference and Equivalent Methods)
The EPA proposed to clarify the regulations associated with FRM and FEM applications for review by the EPA (88 FR 5664, January 27, 2023). Revisions were also proposed in instances where current regulatory specifications are no longer pertinent and require updating. In addition, the EPA proposed to correct a compiled a list of noted minor errors in the regulations associated with the testing requirements and acceptance criteria for FRMs and FEMs in part 53. These errors are typically not associated with the content of Federal Register documents but often relate to transcription errors and typographical errors in the electronic CFR (eCFR) and printed versions of the CFR.
1. Update to Program Title and Delivery Address for FRM and FEM Applications
The EPA proposed a change to 40 CFR 53.4(a) to update the delivery address for FRM and FEM Applications and Modification Requests, as well as update the name of the program responsible for their review (88 FR 5664, January 27, 2023). These revisions are due solely to organizational changes and do not affect the structure or role of the Reference and Equivalent Methods Designation Program in reviewing new FRM and FEM application requests and requests to modify existing designated instruments. The EPA received no comments on this revision and, therefore, the EPA is finalizing this revision as proposed.
2. Requests for Delivery of a Candidate FRM or FEM Instrument
The EPA proposed a change to 40 CFR 53.4(d), which currently allows the EPA to request only candidate PM2.5 FRMs and Class II or Class III equivalent methods for testing purposes as part of the applicant review process (88 FR 5664, January 27, 2023). The EPA proposed to revise this section to enable requesting any candidate FRM, FEM, or a designated FRM or FEM associated with a Modification Request, regardless of NAAQS pollutant type or metric. The EPA received no comments on these revisions; therefore, the EPA is finalizing this revision as proposed.
3. Amendments to Requirements for Submission of Materials in 40 CFR 53.4(b)(7) for Language and Format
The EPA proposed a change to 40 CFR 53.4(b)(7) to specify that all written FRM and FEM application materials must be submitted to the EPA in English in MS Word format and that submitted data must be submitted in MS Excel format (88 FR 5664, January 27, 2023). The EPA received no comments on these revisions; therefore, the EPA is finalizing this section as proposed.
4. Amendment to Designation of Reference and Equivalent Methods
The EPA proposed a change to 40 CFR 53.8(a) to clarify the terms of new FRM and FEM methods to ensure that candidate samplers and analyzers are not publicly announced, marketed, or sold until the EPA's approval has been formally announced in the Federal Register (88 FR 5664, January 27, 2023). The EPA received no comments on these revisions; therefore, the EPA is finalizing this section as proposed.
5. Amendment to One Test Field Campaign Requirement for Class III PM2.5 FEMs
The EPA proposed a change to 40 CFR 53.35(b)(1)(ii)(D) that involves field comparability tests for candidate Class III PM2.5 FEMs, including the requirement that a total of five field campaigns must be conducted at four separate sites, A, B, C, and D (88 FR 5664, January 27, 2023). The existing Site D specifications require that the site “shall be in a large city east of the Mississippi River, having characteristically high sulfate concentrations and high humidity levels.” However, dramatic decreases in ambient sulfate concentration make it difficult for applicants to routinely meet the high sulfate concentration requirement. Therefore, the EPA proposed to revise the Site D specifications to read “shall be in a large Start Printed Page 16345 city east of the Mississippi River, having characteristically high humidity levels.” Only one comment was received on this proposed revision, which was supportive. Therefore, the EPA is finalizing the revision to 40 CFR 53.35(b)(1)(ii)(D), as proposed.
6. Amendment to Use of Monodisperse Aerosol Generator
The EPA proposed a change to 40 CFR 53.61(g), 53.62(e), and Table F–1 that involves the wind tunnel evaluation of candidate PM10 inlets and candidate PM2.5 fractionators under static conditions, which requires the generation and use of monodisperse calibration aerosols of specified aerodynamic sizes (88 FR 5664, January 27, 2023). In the current regulations, the TSI Incorporated Vibrating Orifice Aerosol Generator (VOAG) is the only monodisperse generator that is approved for this purpose. However, TSI Incorporated no longer manufacturers nor supports the VOAG. Therefore, a commercially available monodisperse aerosol generator (Model 1520 Fluidized Monodisperse Aerosol Generator, MSP Corporation, Shoreview, MN) has been added to list of approved generators for this purpose. No comments were received on this revision; therefore, the EPA is finalizing this revision as proposed.
7. Corrections to 40 CFR Part 53 (Reference and Equivalent Methods)
Certain provisions of 40 CFR 53.14, Modification of a reference or equivalent method, incorrectly state an EPA response deadline of 30 days for receipt of modification materials in response to an EPA notice. Per a 2015 amendment (80 FR 65460, 65416, Oct. 26, 2015), all EPA response deadlines for modifications of reference or equivalent methods are 90 days from day of receipt. Thus, the EPA proposed a correction to specify the correct 90-day deadline (88 FR 5664, January 27, 2023).
Requirements for Reference and Equivalent Methods for Air Monitoring of Criteria Pollutants identifies the applicable 40 CFR part 50 appendices and 40 CFR part 53 subparts for each criteria pollutant. The four rows in the section for PM10–2.5 erroneously do not include the footnote instruction that the aforementioned pollutant alternative Class III requirements may be substituted in regard to Appendix O to Part 50—Reference Method for the Determination of Coarse Particulate Matter as PM10–2.5 in the Atmosphere.
Table B–1 specifies that the interference equivalent for each interferent is ±0.005 ppm for both the standard-range and lower-range limits, with the exception of nitric oxide (NO) for the lower-range limit per note 4. When testing the lower range of SO2, the limit for NO is ±0.003 ppm, therefore, an incorrect lower limit (±0.0003) is currently stated in note 4 for this exception to the SO2 lower range limit. Thus, the EPA proposed a correction to Table B–1 to specify the correct limit in note 4 (88 FR 5664, January 27, 2023).
After the EPA received an inquiry regarding the interaction of NO and O3, the EPA investigated the interferent testing requirements stated by 40 CFR part 53, subpart B. The EPA has determined that during the 2011 SO2 amendment and subsequent 2015 O3 amendment, several typographical errors were introduced into Table B–3, the most significant of which is the omission of note 3, which instructs the applicant to not mix the pollutant with the interferent. Thus, the EPA proposed revisions to Table B–3 to correct these errors (88 FR 5664, January 27, 2023).
Additionally, appendix A to subpart B of part 53 provides figures depicting optional forms for reporting test results. Figure B–3 lists an incorrect formula: the lower detectible limit section is missing the proper operator in the LDL calculation formula and Figure B–5 lists an incorrect calculation metric, and there is a typesetting error in the calculation of the standard deviation. The EPA proposed to correct the typesetting errors and noted other errors to be corrected in several formulas provided throughout § 53.43 (88 FR 5664, January 27, 2023).
The EPA proposed a revision to 40 CFR 53.43(a)(2)(xvi), 53.43(b)(2)(iv), and 53.43(b)(2)(iv) to correct typographical errors in equations.
The EPA proposed a revision to Table C–4 of part 53 Subpart C (88 FR 5700). This change is related to field comparability tests of candidate PM2.5, PM10–2.5, and PM10 FEMs, which requires testing at wide range of ambient concentrations. For this reason, Table C–4 specifies a minimum number of valid sample sets to be conducted at specified high concentrations. However, due to the dramatic decrease in ambient PM concentrations in the past two decades, these number of valid test days at high concentrations has been difficult to achieve. Accordingly, the EPA proposed to revise the testing specifications for high concentration events in Table C–4 to reflect current levels of ambient PM for all three PM metrics. In addition to the revision of the ambient PM concentration specifications to Table C–4, there are also several entry errors that required correction.
The EPA received no comments on these proposed revisions; therefore, the EPA is finalizing the changes as proposed.
C. Changes to 40 CFR Part 58 (Ambient Air Quality Surveillance)
1. Quality Assurance Requirements for Monitors Used in Evaluations for National Ambient Air Quality Standards
In the proposal, the EPA described how we evaluated the quality system as part of the PM NAAQS reconsideration (88 FR 5665, January 27, 2023). In this section, the EPA identified several areas for improvement in steadily declining average ambient PM2.5 concentrations across the country and the final decision to revise primary annual PM2.5 NAAQS described in section II above. We assessed PM2.5 concentration data across a range of values to determine if any changes to the statistical calculations used to evaluate the data quality in the PM2.5 network were warranted. This section describes the EPA's assessment, comments received, and the EPA's final decisions on the proposed changes. Other changes in this section include clarifications and other improvements that will facilitate consistency and the operation of quality assurance programs by State, local, and Tribal (SLT) agencies nationwide.
a. Quality System Requirements
The EPA reconsidered the appendix A, section 2.3.1.1 goal for acceptable measurement uncertainty (88 FR 5665, January 27, 2023) for automated and manual PM2.5 methods for total bias. The existing total bias goal is an upper 90 percent confidence limit for the coefficient of variation (CV) of 10 percent and ±10 percent for total bias. The intent of the proposal was to investigate if this bias goal is still realistic given updated precision and bias statistic. The EPA received one comment that bias reevaluation may be premature, since the final NAAQS standard had not yet been determined at the time of the proposal. The EPA acknowledges this comment but clarifies that the proposed new bias statistic was evaluated at a range of levels including the range of proposed PM2.5 standards in the technical memorandum, “Task 16 on PEP/NPAP Task Order: Bias and Precision DQOs for the PM2.5 Ambient Air Monitoring Network.” [181] Considering the Start Printed Page 16346 justification in the technical memorandum and the lack of adverse comments regarding this part of the proposal, the EPA is retaining the appendix A, section 2.3.1.1, goal for acceptable measurement uncertainty for automated and manual PM2.5 methods for total bias.
The EPA also proposed to update and clarify ambient air monitoring requirements found in 40 CFR part 58, appendix A, section 2.6.1 pertaining to EPA Protocol Gas standards used for ambient air monitoring and the Ambient Air Protocol Gas Verification Program (PGVP) (88 FR 5665, January 27, 2023). The EPA proposed to revise appendix A to clarify that in order to participate in the Ambient Air PGVP, producers of Protocol Gases must adhere to the requirements of 40 CFR 75.21(g), and only regulatory ambient air monitoring programs may submit cylinders for assay verification to the EPA Ambient Air PGVP. The EPA received mixed comments in support of and in opposition to this proposed revision. The sole commenter opposing the proposed revision indicated that the proposed PGVP requirements would be additional and is concerned with an increased resource burden. But the EPA responds that the PGVP requirements that were proposed to be added are consistent with the existing PGVP requirements in 40 CFR 75.21(g), and PGVP has been defined as a regulatory requirement since 2016 (81 FR 17263, March 28, 2016), so the proposed part 58 changes are not “additional” to existing regulations. After consideration of the comments, the EPA is finalizing the update and clarification of ambient air monitoring requirements found in appendix A, section 2.6.1 pertaining to EPA Protocol Gas standards used for ambient air monitoring and the Ambient Air PGVP as proposed.
b. Measurement Quality Check Requirements
The EPA proposed to remove section 3.1.2.2 from appendix A, which allows NO2 compressed gas standards to be used to generate audit standards (88 FR 5665, January 27, 2023). The EPA received one comment supporting this change. As a result of the comment received and other general supportive comments regarding quality assurance, the EPA is finalizing the removal of section 3.1.2.2 from appendix A as proposed.
The EPA proposed to revise the requirement in Appendix A, section 3.1.3.3 changing the National Performance Audit Program (NPAP) requirement for annual verification of gaseous standards to the ORD-recommended certification periods identified in Table 2–3 of the EPA Traceability Protocol for Assay and Certification of Gaseous Calibration Standards (appendix A, section 6.0(4)) (88 FR 5665). The EPA received one comment supporting this change. As a result of the comment received and other general supportive comments regarding quality assurance, the EPA is finalizing the updated NPAP gaseous certification requirement in section 3.1.3.3 as proposed.
The EPA proposed to adjust the minimum value required by appendix A, section 3.2.4, to be considered valid sample pairs for the PM2.5 Performance Evaluation Program (PEP) from 3 μg/m[3] to 2 μg/m[3] (88 FR 5665, January 27, 2023). The EPA received comments in support and against the change. In the only opposing comment, the commenter expressed concern that the method detection limit (MDL) for PM2.5 is 2 μg/m[3] . The commenter also indicated that the MDL “typically has minimal value per the definition of the MDL.” 40 CFR part 50, appendix L states, “The lower detection limit of the mass concentration measurement range is estimated to be approximately 2 μg/m[3] , based on noted mass changes in field blanks in conjunction with the 24 m[3] nominal total air sample volume specified for the 24-hour sample.” The EPA notes that field blanks currently average less than 10 μg nationally, and when divided by the 24 m[3] nominal total air sample volume specified for a 24-hour sample, the result is 0.4 μg/m[3] . The appendix L MDL referenced by the commenter was part of the 1997 PM NAAQS rulemaking (62 FR 38652, July 18, 1997); current data shows that the MDL is substantially lower than the EPA's original estimate. After review of the comments, and in consideration of the recently calculated detection limit for the PM2.5 FRM that is substantially lower than our original estimate,[182] the EPA is finalizing the revised minimum value for valid sample pairs for the PM2.5 Performance Evaluation Program (PEP) from 3 μg/m3 to 2 μg/m3 in appendix A, section 3.2.4 as proposed.
c. Calculations for Data Quality Assessments
The EPA proposed to change Equations 6 and 7 of appendix A, section 4.2.1 that are used to calculate the Collocated Quality Control Sampler Precision Estimate for PM10, PM2.5and Pb (88 FR 5666, January 27, 2023). The proposed new statistics are designed to address the high imprecision values that result from using these calculations to compare low concentrations that are now more routinely observed in the networks. The EPA received several comments in support of this change in general, but some commenters indicated that they believed there was an error in the new calculation that may result in high imprecision from the calculation of the equation. The EPA reviewed the technical memorandum and confirmed that a multiplier of 100 was unintentionally left in the proposed relative difference equation, Equation 6. Also, equation 6 was corrected from a normalized percent difference to a normalized relative percent difference that is appropriate for comparing collocated pairs at low concentrations. The technical memorandum titled “Task 16 on PEP/NPAP Task Order: Bias and Precision DQOs for the PM2.5 Ambient Air Monitoring Network” has been amended to correct the error and is included in the docket for this action.[183]
Equation 6 as proposed at 88 FR 5666 (January 27, 2023) was:
Start Printed Page 16347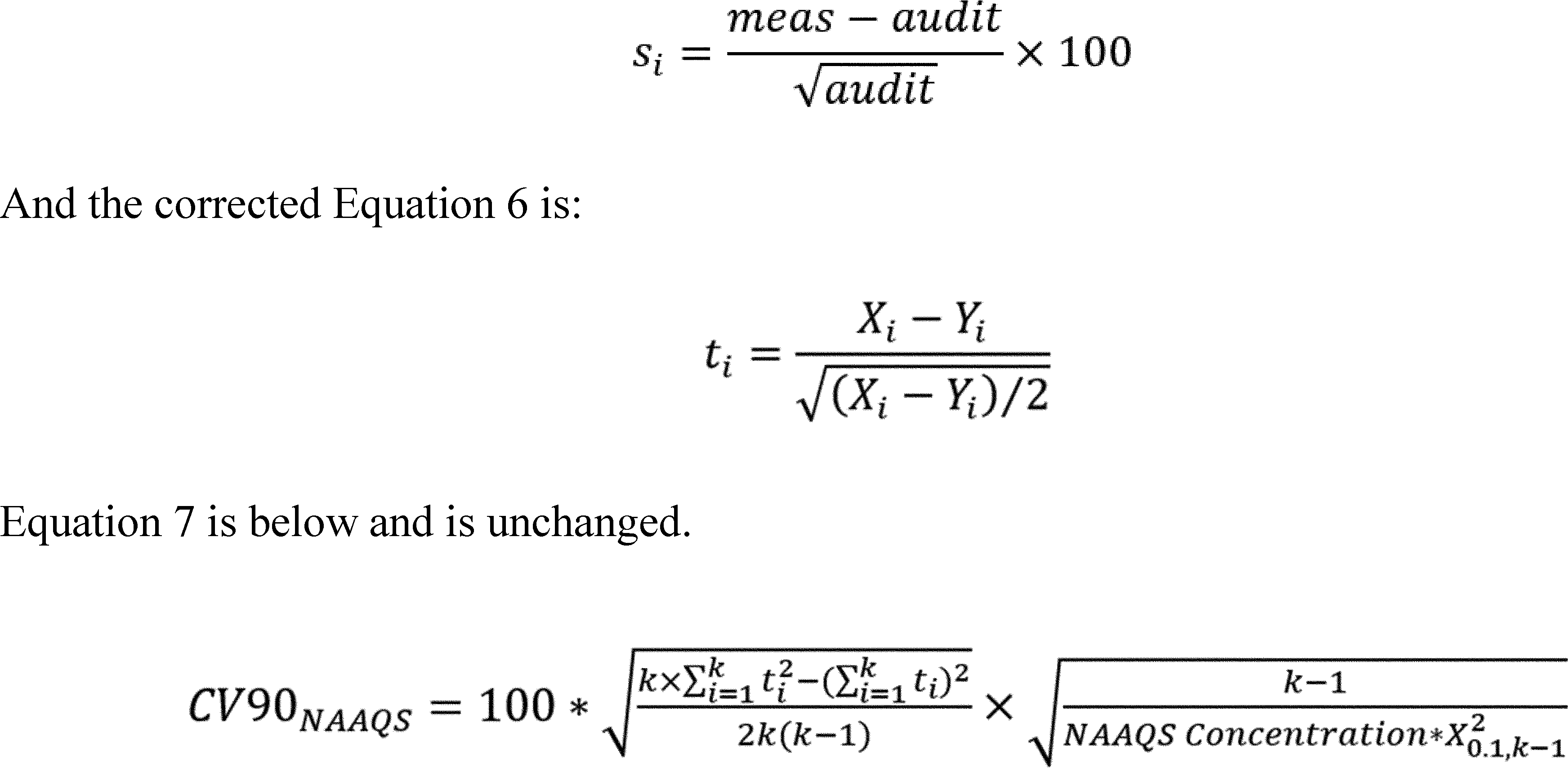
As a result of the positive comments received and the correction to the equation made in response to some comments, the EPA is finalizing the updated Equation 6 as described and is finalizing Equation 7 as proposed for the calculation of the Collocated Quality Control Sampler Precision Estimate for PM10, PM2.5, and Pb in section 4.2.1.
The EPA proposed to update the appendix A, section 4.2.5, Equation 8, calculation for the Performance Evaluation Program Bias Estimate for PM2.5 (88 FR 5666–67, January 27, 2023). Because average ambient PM concentrations across the nation have steadily declined since the promulgation of the PM2.5 standard, the EPA proposed to replace the current percent difference equation with a relative difference equation. The EPA received several comments in support of this change in general, but some commenters identified a potential error in the new calculation that resulted in an artificially high estimate, which they do not support. The EPA reviewed the technical memorandum and discovered that a multiplier of 100 was left in the new relative difference equation used in the bias equation. The technical memorandum, “Task 16 on PEP/NPAP Task Order: Bias and Precision DQOs for the PM2.5 Ambient Air Monitoring Network” has been amended to correct the error and is included in the docket.[184] The proposed Equation 8 proposed at 88 FR 5667 (January 27, 2023) was:
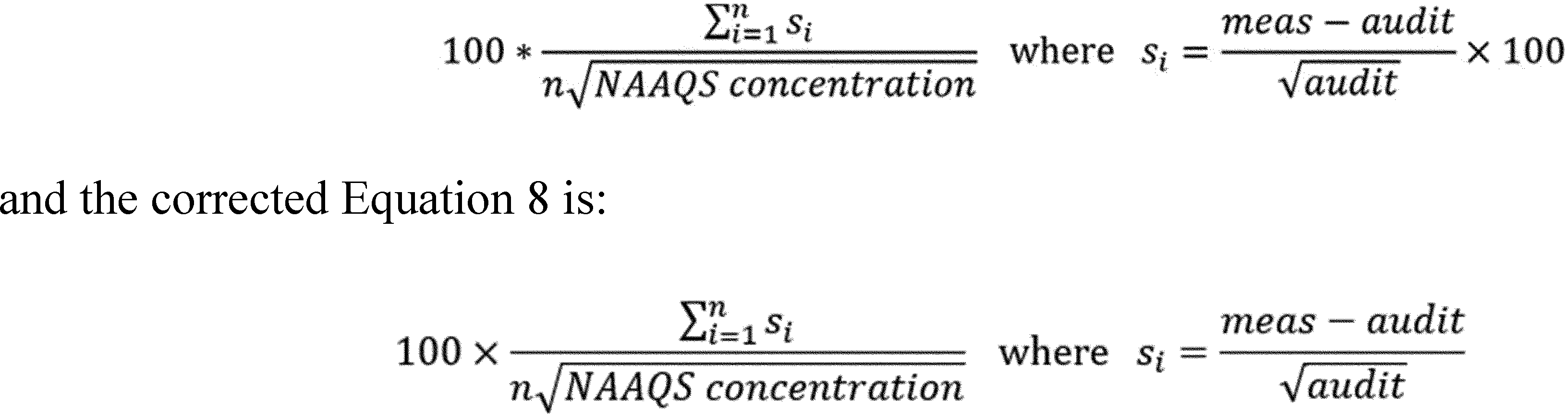
As a result of the supportive comments received and the correction to the equation in response to some comments, the EPA is updating and finalizing Equation 8 as described for the calculation for the Performance Evaluation Program Bias Estimate for PM2.5, in section 4.2.5.
d. References
The EPA proposed to update the references and hyperlinks in appendix A, section 6 (88 FR 5667, January 27, 2023) to provide accuracy in identifying and locating essential supporting documentation and delete references to historical documents that do not represent current practices. The EPA received only favorable comments, and as a result, the EPA is finalizing the updated the references and hyperlinks in appendix A, section 6, as proposed.
The EPA also proposed to add a footnote to Table A–1 of part 58, appendix A—Minimum Data Assessment Requirements for NAAQS Related Criteria Pollutant Monitors (88 FR 5669, January 27, 2023). The proposed footnote clarifies the allowable time ( i.e., every two weeks, once a month, once a quarter, once every six months, or distributed over all four quarters depending on the check) between checks and encourages monitoring organizations to perform data assessments at regular intervals. The EPA received two comments regarding this proposed footnote. One commenter indicated that this change is inconsistent with the QA Handbook for Air Pollution Measurement Systems: “Volume II: Ambient Air Quality Monitoring Program QA Handbook.” The EPA agrees with the commenter; because the QA Handbook is guidance, Start Printed Page 16348 the EPA will revise it after this action is finalized to be consistent with the updated CFR provision. Another commenter does not support the addition of the footnote due to concerns about limiting flexibility. In response, the EPA reiterates that the proposed revision is intended to clarify intent and does not make any changes to the required frequencies or acceptance criteria for data assessment. A “weight of evidence” narrative is still found in 40 CFR part 58, appendix A, section 1.2.3. As a result of the comments received and the rationale discussed above, the EPA is finalizing the addition of the new footnote to Table A–1 of part 58, appendix A—Minimum Data Assessment Requirements for NAAQS Related Criteria Pollutant Monitors as proposed.
2. Quality Assurance Requirements for Prevention of Significant Deterioration (PSD) Air Monitoring
The EPA proposed to revise appendix B, Quality Assurance Requirements for Prevention of Significant Deterioration (PSD) Air Monitoring (88 FR 5667, January 27, 2023), in parallel to the proposal to revise appendix A. Thus, this section of the proposal included similar detail and proposed revisions related to evaluating quality system statistical calculations for PM2.5, clarifications and other improvements that would facilitate consistency and the operation of quality assurance programs for PSD by SLT agencies nationwide.
a. Quality System Requirements
The EPA reconsidered the goal in appendix B, section 2.3.1.1 for acceptable measurement uncertainty for automated and manual PM2.5 methods for total bias (88 FR 5668, January 27, 2023).[185] The current total bias goal is an upper 90 percent confidence limit for the coefficient of variation (CV) of 10 percent and ±10 percent for total bias. The EPA's intent was to investigate if this goal is still realistic given updated precision and bias statistics. The EPA received one comment that bias reevaluation may be premature, since the final NAAQS standard had not yet been determined at the time of the proposal. The EPA acknowledges this comment but clarifies that the proposed new bias statistic was evaluated at a range of levels including the proposed range of PM2.5 standards in the technical memorandum, “Task 16 on PEP/NPAP Task Order: Bias and Precision DQOs for the PM2.5 Ambient Air Monitoring Network.” [186] Considering the justification in the technical memorandum and the lack of adverse comments regarding the substantive proposal, the EPA is retaining the appendix B, section 2.3.1.1, goal for acceptable measurement uncertainty for automated and manual PM2.5 methods for total bias.
The EPA also proposed to update and clarify ambient air monitoring requirements found in 40 CFR part 58, appendix B, section 2.6.1 pertaining to EPA Protocol Gas standards used for ambient air monitoring and the Ambient Air PGVP (88 FR 5668, January 27, 2023). The EPA proposed to revise appendix B to clarify that in order to participate in the Ambient Air PGVP, producers of Protocol Gases must adhere to the requirements of 40 CFR 75.21(g), and only regulatory ambient air monitoring programs may submit cylinders for assay verification to the EPA Ambient Air PGVP. The EPA received comments in support of and in opposition to this proposed revision. The commenter opposing the revision indicated that the proposed PGVP requirements would be additional and is concerned with an increased resource burden. However, the EPA disagrees with the commenter because that the proposed PGVP requirements are consistent with the existing PGVP requirements in 40 CFR 75.21(g). PGVP has been defined as a regulatory requirement since 2016 (81 FR 17263, March 28, 2016), so the proposed part 58 changes are not “additional” to existing regulations. After consideration of the comments, the EPA is finalizing the update and clarification of ambient air monitoring requirements found in appendix B, section 2.6.1 pertaining to EPA Protocol Gas standards used for ambient air monitoring and the Ambient Air PGVP as proposed.
b. Measurement Quality Check Requirements
The EPA proposed to remove section 3.1.2.2 from appendix B, which allows NO2 compressed gas standards to be used to generate audit standards (88 FR 5668, January 27, 2023). The EPA received one comment supporting this change. As a result of the comment received and other general supportive comments regarding quality assurance, the EPA is finalizing the removal of section 3.1.2.2 from appendix B as proposed.
The EPA proposed to revise the requirement in Appendix B, section 3.1.3.3 changing the National Performance Audit Program (NPAP) requirement for annual verification of gaseous standards to the ORD-recommended certification periods identified in Table 2–3 of the EPA Traceability Protocol for Assay and Certification of Gaseous Calibration Standards (appendix B, section 6.0(4)) (88 FR 5668, January 27, 2023). The EPA received one comment supporting this change. As a result of the comment received and other general supportive comments regarding quality assurance, the EPA is finalizing the updated NPAP gaseous certification requirement in section 3.1.3.3 as proposed.
The EPA proposed to adjust the minimum value required by appendix B, section 3.2.4, to be considered valid sample pairs for the PM2.5 Performance Evaluation Program (PEP) from 3 μg/m3 to 2 μg/m3 (88 FR 5668, January 27, 2023). The EPA received comments in support and against the change. In the only opposing comment, the commenter expressed concern that the method detection limit (MDL) for PM2.5 is 2 μg/m3 . The commenter also indicated that the MDL “typically has minimal value per the definition of the MDL.” 40 CFR part 50, appendix L states, “The lower detection limit of the mass concentration measurement range is estimated to be approximately 2 μg/m3 , based on noted mass changes in field blanks in conjunction with the 24 m3 nominal total air sample volume specified for the 24-hour sample”. The EPA notes that field blanks currently average less than 10 μg nationally, and when divided by the 24 m3 nominal total air sample volume specified for a 24-hour sample, the result is 0.4 μg/m3 . The appendix L MDL referenced by the commenter was part of the 1997 PM NAAQS rulemaking more than 20 years ago (62 FR 38652, July 18, 1997); current data shows that the MDL is substantially lower than EPA's original estimate. After review of the comments, and in consideration of the recently calculated Start Printed Page 16349 detection limit for the PM2.5 FRM that is substantially lower than our original estimate, the EPA is revising the minimum value for valid sample pairs for the PM2.5 Performance Evaluation Program (PEP) from 3 μg/m3 to 2 μg/m3 in appendix B, section 3.2.4 as proposed.
c. Calculations for Data Quality Assessments
The EPA proposed to change Equations 6 and 7 of appendix B, section 4.2.1 used for calculating the Collocated Quality Control Sampler Precision Estimate for PM10, PM2.5and Pb (88 FR 5707, January 27, 2023). These new statistics are designed to address the high imprecision values that result from using these calculations to compare low concentrations that are now more routinely observed in the networks. The EPA received several comments in support of this change in general, but a couple commenters indicated that there could be an error in the new calculation that resulted in high imprecision from the calculation of the equation. The EPA reviewed the technical memorandum and discovered that a multiplier of 100 was unintentionally left in the proposed relative difference equation, Equation 6. Also, equation 6 was corrected from a normalized percent difference to a normalized relative percent difference that is appropriate for comparing collocated pairs at low concentrations. The technical memorandum titled “Task 16 on PEP/NPAP Task Order: Bias and Precision DQOs for the PM2.5 Ambient Air Monitoring Network” was amended to correct the error and is included in the docket.[187]
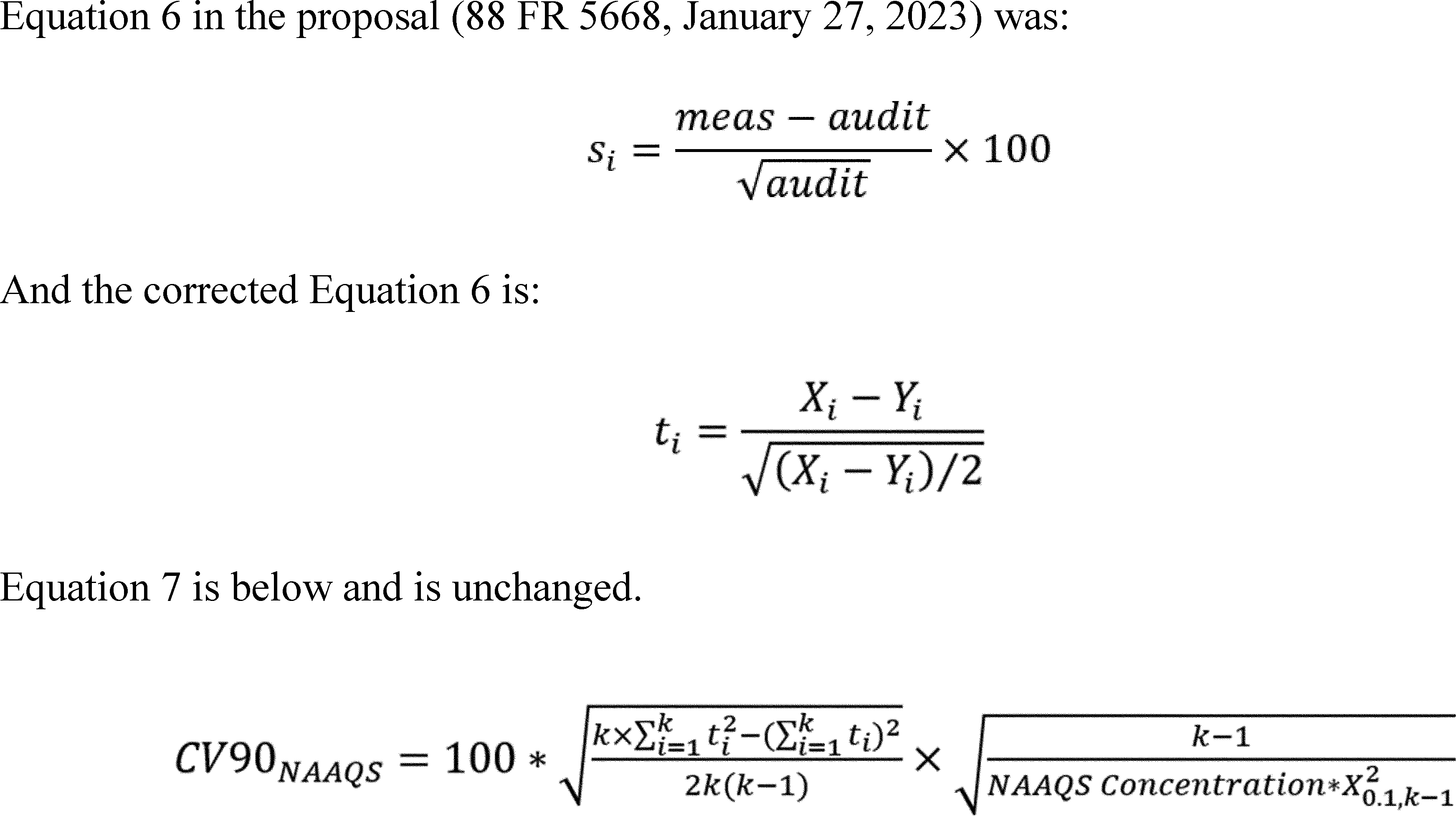
As a result of the positive comments received and the correction to the equation made in response to those comments, the EPA is finalizing the update to Equation 6 and retaining Equation 7 as proposed for the calculation of the Collocated Quality Control Sampler Precision Estimate for PM10, PM2.5and Pb in section 4.2.1.
The EPA proposed to update the appendix B, section 4.2.5, Equation 8, calculation for the Performance Evaluation Program Bias Estimate for PM2.5 (88 FR 5668–59, January 27, 2023). Because average ambient PM concentrations across the nation have steadily declined since the promulgation of the PM2.5 standard, the EPA proposed to replace the current percent difference equation with a relative difference equation. The EPA received several comments in support of this change in general, but some commenters identified a potential error in the new calculation that resulted in an artificially high estimate, which they do not support. The EPA reviewed the technical memorandum and discovered that a multiplier of 100 was left in the new relative difference equation used in the bias equation. The technical memorandum, “Task 16 on PEP/NPAP Task Order: Bias and Precision DQOs for the PM2.5 Ambient Air Monitoring Network” has been amended to correct the error and is included in the docket. The proposed Equation 8 (88 FR 5669, January 27, 2023) was:
Start Printed Page 16350
As a result of the supportive comments received and the correction to the equation in response to some comments, the EPA is updating and finalizing Equation 8 as described for the calculation for the Performance Evaluation Program Bias Estimate for PM2.5, in section 4.2.5.
d. References
The EPA proposed to update the references and hyperlinks in appendix B, section 6 (88 FR 5669, January 27, 2023) to provide accuracy in identifying and locating essential supporting documentation and delete references to historical documents that do not represent current practices. The EPA received only favorable comments, and as a result, the EPA is finalizing the updated the references and hyperlinks in appendix B, section 6, as proposed.
The EPA also proposed to add a footnote to Table B–1 of part 58, appendix B—Minimum Data Assessment Requirements for NAAQS Related Criteria Pollutant PSD Monitors (88 FR 5669, January 27, 2023). The proposed footnote clarifies the allowable time ( i.e., every two weeks, once a month, once a quarter, once every six months, or distributed over all four quarters depending on the check) between checks and encourages monitoring organizations to perform data assessments at regular intervals. The EPA received two comments regarding this proposal. One commenter indicated that this change is inconsistent with the QA Handbook. The EPA agrees with the commenter; because the QA Handbook is guidance, the EPA will revise it after this action is finalized to be consistent with the updated CFR provision. Another commenter does not support the addition of the footnote due to concerns about limiting flexibility. In response, the EPA reiterates that the proposed revision is intended to clarify intent and does not make any changes to the required frequencies or acceptance criteria for data assessment. A “weight of evidence” narrative is still found in 40 CFR part 58, appendix B, section 1.2.3. As a result of the comments received and the rationale discussed above, the EPA is adding the new footnote to Table B–1 of part 58, appendix B—Minimum Data Assessment Requirements for NAAQS Related Criteria Pollutant PSD Monitors as proposed.
3. Amendments to PM Ambient Air Quality Methodology
a. Revoking Approved Regional Methods (ARMs)
The EPA proposed to remove provisions for approval and use of Approved Regional Methods (ARMs) throughout parts 50 and 58 of the CFR (88 FR 5669, January 27, 2023). ARMs are continuous PM2.5 methods that have been approved specifically within a State or local air agency monitoring network for purposes of comparison to the NAAQS and to meet other monitoring objectives. Currently, there are no approved ARMs. There are, however, more than a dozen approved Federal Equivalent Methods (FEMs) for PM2.5. These approved FEMs are eligible for comparison to the NAAQS and to meet other monitoring objectives.
The EPA received comments from multiple State air programs in support of the proposal to remove provisions for approval and use of ARMs. One commenter cites that there are multiple FEMs available for monitoring agencies to work with and that the agency was never able to get a candidate ARM to meet the requirements for approval. With the availability of multiple FEMs that now work in the monitoring agency's network, the commenting agency does not anticipate the need to ever pursue an ARM in the future and, therefore, suggests that the ARM provision is no longer needed. Another commenter strongly supported the proposed changes to remove the ARM provisions. The EPA also received comments from a few agencies that supported retaining the ARM provisions instead. One commenter cited the need to consider the rapid advancement of various new technologies and that, in some cases, approved continuous FEMs may have shortcomings, meaning that losing the ability to propose an ARM in the future may limit useful alternative options to monitoring agencies. Another commenter suggested that the removal of the ARM would take away the ability and right to use locally derived correction factors.
After considering the comments for and against removing the provisions for ARMs, the EPA believes it is most appropriate to remove the ARM provisions. As described in the proposal, when the EPA first proposed the process for approving and using ARMs, there were no continuous FEMs approved. There are now over a dozen approved PM2.5 continuous FEMs and no approved ARMs. Therefore, the EPA is finalizing the removal of ARMs throughout 40 CFR parts 50 and 58 as proposed.
b. Calibration of PM Federal Equivalent Methods (FEMs)
The EPA proposed to modify its specifications for PM FEMs in appendix C to Part 58 (88 FR 5670–73, January 27, 2023). Specifically, the EPA proposed that valid State, local, and Tribal (SLT) air monitoring data from Federal Reference Methods (FRMs) generated in routine networks and submitted to the EPA may be used to improve the PM concentration measurement performance of approved FEMs. This approach, initiated by instrument manufacturers, would be implemented as a national solution in factory calibrations of approved FEMs through a firmware update. This could apply to any PM FEM methods ( i.e., PM10, PM2.5, and PM10–2.5).
The EPA proposed this modification because there are some approved PM FEMs that are not currently meeting bias measurement quality objectives (MQOs) when evaluating data nationally as described in the 2022 PA (U.S. EPA, 2022b, section 2.2.3.1), meaning that an update to factory calibrations may be appropriate; however, there is no clearly defined process to update the calibration of FEMs. While there are several types of data available to use as the reference for such updates ( e.g., routinely operated FRMs, audit program FRMs, and chemical speciation sampler Start Printed Page 16351 data), we proposed to use routinely operated SLT FRMs as the basis of comparison upon which to calibrate FEMs. The goal of updating factory calibrations would be to increase the number of routinely operating FEMs meeting bias MQOs across the networks in which they are operated. While there are other approaches that could improve data comparability between PM FEMs and collocated FRMs, the EPA believes that the proposed modification to calibrate PM FEMs represents the most reliable approach to update FEM factory calibrations, since the existing FRM network data that meet MQOs would be used to set updated factory calibrations.
While the Agency proposed to add this language to more expressly define a process to update factory calibrations of approved PM FEMs, the EPA believes that the existing rules for updating approved FRMs and FEMs found at 40 CFR 53.14 may also continue to be utilized for this purpose, as appropriate. 40 CFR 53.14 allows instrument manufactures to submit to the EPA a “Modification of a reference or equivalent method.” Submitting a modification request may be appropriate to ensure an approved FEM continues to meet 40 CFR 53.9, “Conditions of designation.” Specifically, 40 CFR 53.9(c) requires that, “Any analyzer, PM10 sampler, PM2.5 sampler, or PM10–2.5 sampler offered for sale as part of an FRM or FEM shall function within the limits of the performance specifications referred to in § 53.20(a), § 53.30(a), § 53.35, § 53.50, or § 53.60, as applicable, for at least 1 year after delivery and acceptance when maintained and operated in accordance with the manual referred to in § 53.4(b)(3).” Thus, instrument manufacturers are encouraged to seek improvements to their approved FEM methods as needed to continue to meet data quality needs as operated across the network.
There are several technical components to EPA's proposed modification, including: the reference data to be used in the calibrations; implementing as a national solution in factory calibrations of approved FEMs through firmware updates; application to any PM FEM methods ( i.e., PM10, PM2.5, and PM10–2.5); the appropriate range of data to be used to develop and test new factory calibrations, from just the most representative concentrations up to all available concentrations; the representative set of geographic locations that can be used; whether outliers may be included or not included; that new factory calibrations should be developed using data from at least 2 years and tested on data from a separate year or years; that updates to factory calibrations can occur as often as needed; that calibrations should be evaluated by monitoring agencies as part of routine data assessments, e.g., during certification of data and 5-year assessments; the EPA's recognition that only data from existing operating sites is available; and finally, that an updated factory calibration does not have to work with the original field study data submitted that led to the original FEM designation.
With the proposed modification, the EPA solicited input on these technical issues as well as the overall approach and any alternatives that could lead to more sites meeting the bias MQO with automated FEMs, especially for those sites that are near the level of the primary annual PM2.5 NAAQS, as proposed to be revised in section II above. In response, the EPA received comments from about two dozen entities, most of which were SLT air programs or Multi-Jurisdictional Organizations (MJOs) comprised of these entities.
Overall, there was broad and strong support from a majority of commenters for the proposed requirement to use FRM data generated in routine networks and submitted to the EPA to update factory calibrations included as part of approved FEMs. There were a smaller number of critical comments on the proposed process as well as some commentors that supported the proposed requirement but also provided additional suggestions for the EPA's consideration. Below, we address each of the areas on which the EPA requested comment regarding the calibration of PM FEMs, as well as a few additional areas where multiple commenters offered input on other areas related to our proposal.
A majority of the commenters on the proposed PM FEM calibration process support the process to use valid State, local, and Tribal FRM data generated in routine networks and submitted to the EPA to improve the PM concentration measurement performance of approved FEMs. Some commenters suggested that this action is needed to ensure that data reported from FRMs and FEMs are comparable and correction methods applied to data from FEM monitors are defensible across the national PM monitoring network. Others stated that they agree with the EPA that this is a critical step in the right direction to account for the discrepancies between PM2.5 FRM data and PM2.5 FEM data. Some commented that applying corrections includes a recognition that, while different measurement principles may produce differences in the resulting data, having an approach that minimizes bias is extremely important. Finally, some stated their belief that a correction factor is necessary to preserve data integrity with the FRM.
The EPA also received comments suggesting ways that the PM FEM correction could be performed, including through detailed analysis of data; by having PM FEM instrument manufacturers evaluate nationally available valid FRM data to update factory calibrations; and, by having the instrument manufacturers implement calibration adjustments at the factory.
The EPA also received supportive comments on the PM FEMs calibration relating to comparability to the NAAQS. For example, a commenter stated that it is important to ensure bias MQOs are met for FEMs run at sites potentially affected by revised standards as well as the need to accurately designate areas as attaining or not attaining the NAAQS. There were comments supporting the correction of PM FEM data as helping the EPA and SLT monitoring programs continue to evolve toward more automated methods. For example, one commenter appreciates the EPA's support for the ongoing move from filter-based PM2.5 FRMs to use of continuous FEMs, stating that they concur with the EPA's assessment that there is monitoring bias between FRMs and FEMs, and commending EPA for recognizing ongoing data quality issues for FEMs and for taking action to improve these issues in collaboration with instrument manufacturers and SLT agencies.
A small number of commenters were critical of the proposed FEM calibration approach. One commenter noted that EPA should further examine the handling of FEM PM2.5 data when used for comparison to the NAAQS. In response, we note that monitoring agencies and the EPA will continue to examine the comparability and use of FEM data used in comparison to the NAAQS. Another commenter suggested that the calibration process for a designated PM monitor should not be altered following Class III designation approval. The EPA disagrees as we believe it is appropriate for FEMs to be calibrated with routinely operated FRMs, because doing so is an efficient way to work towards FEM data meeting the bias MQO across the networks in which the FEMs are currently being operated. Also, having continuous PM FEMs meeting bias MQOs allows the use of the data in a variety of other ways that manually operated FRMs samplers cannot support. Another commenter stated that, if a particular FEM designated make or model of Start Printed Page 16352 instruments fails to meet MQOs, then that make or model should be removed from the designations altogether. The EPA agrees and clarifies that the modification would not prevent removal of FEM designation from a make or model of instrument under the existing 40 CFR 53.11—Cancellation of reference or equivalent method designation. This may be appropriate if there are no other solutions to improve the method such that it achieves bias MQOs.
A few commenters provided specific recommendations for how the regulatory language could be improved. These included comments that the new regulatory language proposed for 40 CFR part 58, appendix C, section 2.2 must ensure consistency and transparency when requesting changes to the factory calibration; that the EPA should incorporate binding regulatory language in 40 CFR part 58, appendix C, section 2.2 ( i.e., it currently lacks “shall” or “must”) to ensure the language is not open to inconsistency and does not provide unique deference to instrument manufacturers without a mechanism for transparent communication of the changes being made and the supporting technical analysis. A commenter also requested that the EPA define the core requirements needed to ensure all requests for updating factory calibrations are required to follow the same process, using data of the same known quality, and evaluating the effectiveness of the resulting correction factors consistently.
In response to these comments, while the EPA agrees that the proposed regulatory language for 40 CFR part 58, appendix C, section 2.2 must ensure consistency and transparency when entities request changes to factory calibrations, the EPA disagrees that the regulations cannot also provide some flexibility. For example, we believe that a degree of flexibility is appropriate regarding whether outliers in the data to be used for factory calibration should or should not be included, the range of data to be included, and in utilizing collocated FRM and FEM data for updated calibrations from a representative set of geographic areas in which it is produced. The EPA believes that the proposal defined the core requirements needed to ensure all requests for updating FEM factory calibrations will follow the same process, using data of the same known quality and evaluating the effectiveness of the resulting correction factors consistently.
In its proposal, the EPA identified that while there are several types of data available to use as the reference for FEM calibration updates, including data from routinely operated FRMs, audit program FRMs, and PM2.5 chemical speciation samplers, the EPA proposed to use routinely operated State, local, and Tribal FRMs as the basis of comparison upon which to calibrate FEMs (88 FR 5670–71, January 27, 2023). Importantly, routine SLT agency FRM data form the largest portion of the monitored air quality data used in epidemiologic studies that are being used to inform proposed decisions regarding the adequacy of the public health protection afforded by the primary PM2.5 NAAQS, as discussed in section II above.
Overall, there was broad and strong support for utilizing collocated FRM data from routine SLT networks to provide calibrations of the continuous FEMs. For example, several commenters agree that valid SLT air monitoring data generated in routine networks and submitted to the EPA will improve the PM concentration measurement performance of approved FEMs. Another commenter provided support for PM FEM instrument manufacturers to evaluate nationally available valid FRM data as well as other data sets such as the performance evaluation audit program to update factory calibrations. The EPA believes that the routinely operated PM FRMs represent the best and largest source of data to calibrate continuous PM FEMs, and that performance evaluation audit program data should be kept independent of the calibration process. This will mean that assessments of the routine monitoring operations, including both the FRM and any future updated PM FEMs, will appropriately remain independent in evaluating whether updated methods are meeting bias MQOs. The EPA is, therefore, finalizing its approach to use routinely operated SLT FRMs as the basis of comparison upon which to calibrate continuous PM FEMs as proposed.
Regarding the EPA's proposed requirement to utilize factory calibrations (88 FR 5670–71, January 27, 2023), several commenters agreed that factory calibrations provide the best option to improve PM FEMs. For example, one commenter stated that the correction factors are necessary to preserve data integrity with the FRM, and they support the proposal that the approach be initiated by instrument manufacturers and implemented as a national solution through firmware updates.
Regarding the proposed requirement that calibrations be initiated by instrument manufacturers (88 FR 5671, January 27, 2023), most commenters were supportive of the proposed approach that recalibration of FEM PM instruments be initiated by instrument manufacturers. For example, one commenter stated they support allowing instrument companies submit improvements to their existing FEMs, as vendors should be encouraged to improve their methods. Another commenter noted that having a methodology initiated by the manufacturer will have nationwide consistency. A few of commenters recommended that SLT air agencies should have the additional ability to petition the EPA Administrator to initiate factory calibrations of FEMs to better meet MQOs when data collected by their agencies indicate disparities, because the monitoring agencies are responsible for the quality of the data from the specific makes and models of instrumentation used in their networks. While the EPA believes that, in most cases, the instrument companies should be the ones to initiate the process for calibration of FEMs to routinely operated FRMs, we agree with the commenters who suggested that other options should be available, including allowing monitoring agencies or MJOs to work independently or together to pursue improvements to designated FEMs. However, the EPA believes that any such improvements initiated by monitoring agencies or MJOs should still be facilitated through the responsible instrument company. Also, any such effort to improve data quality should be employed across all the networks in which the methods are operated and not limited to the networks operated by the agency(s) pursuing such improvements.
Regarding how frequently factory calibrations should be updated, our proposal identified that it would be most appropriate to not define a specific time period for updates; rather, updates should be based on whether or not quality data is being produced across a given network (88 FR 5672, January 27, 2023). Regarding this issue, one commenter recommended that instrument manufacturers be required to evaluate and, if necessary, adjust PM FEMs factory calibrations on an ongoing basis at regular intervals. The EPA notes that while it does not have the authority to require instrument companies to evaluate the quality of data from operating FEMs under 40 CFR part 58, the EPA does routinely participate in conferences and workshops and makes assessments of data quality specific to instrument makes and models publicly available. The EPA also regularly summarizes relevant FRM and FEM data Start Printed Page 16353 quality in documents such as the 2022 PA (U.S. EPA, 2022b). Therefore, consistent with the proposal, we are not finalizing any specifics regarding how frequently factory calibrations should be updated but commit to continue to routinely provide information to SLT agencies regarding FEM data quality.
The EPA proposed that the calibration of FEMs could apply to any of the PM FEM method indicators ( i.e., PM10, PM2.5, and PM10–2.5) (88 FR 5670, January 27, 2023). The EPA received only supportive comments. All comments that included a discussion of three PM metrics support their inclusion for calibration of PM FEMs. Therefore, the EPA is finalizing the inclusion of all three PM indicators ( i.e., PM10, PM2.5, and PM10–2.5) as proposed.
The EPA proposed that either all data available or a range of data up to 125% of the 24-hour NAAQS for the PM indicator of interest may be used to establish new factory calibrations, (88 FR 5671–73, January 27, 2023). The EPA received many comments supportive of the proposal and one comment offering a different approach on the range of data to use. One commenter recommends that the EPA should consider using all “validated” data because how these instruments behave under normal operating ranges may be just as important as how they behave when monitoring conditions are low or elevated, and that the full range of data should be used when determining the appropriate level of the standard, just as the full range of data is used in determining if an area is attaining the standard. In response to this comment, the EPA believes that making allowances for some flexibilities will increase the likelihood of instrument companies pursuing such improvements. Also, even though there is flexibility, the EPA will still be able to evaluate the appropriateness of a range of concentration data included as part of each application submitted. Also, the EPA notes that in certain circumstances, States do petition the EPA to set aside data under the Exceptional Events Rule (§ 50.14, “Treatment of air quality monitoring data influenced by exceptional events”). Where approved, exceptional event data are set aside from use in regulatory decisions. Thus, there is a process to set aside certain high concentration data for certain purposes. Therefore, the EPA is finalizing the provision that factory calibrations may be based on a range of valid data as proposed.
The EPA solicited comment on the representative set of geographic locations to use in the calibration of FEMs compared to collocated FEMs (88 FR 5671, January 27, 2023). Most commenters were supportive of the approach of using representative sites in SLT networks from across the country. For example, several commenters provided their support for PM FEM instrument manufacturers to evaluate nationally available valid FRM data to update factory calibrations. Commenters disagreeing with a national geographic approach preferred to allow local solutions to correct data. For example, one commenter suggested having a local or regional option because PM instruments are impacted by, and respond differently to, a variety of local factors, including relative humidity, temperature, concentration levels, and particle composition. The EPA agrees that there are challenges in the response of PM FEMs to a variety of local factors; however, this can be true of many methods and are not specific to PM FEMs and, therefore, does not provide a reason to reject this approach in this instance. Another commenter stated that the proposed national correction factor is a “flawed concept,” suggesting that it is “widely understood throughout the monitoring community that monitors perform best with a local correction factor.” This commentor offered no record or citation supporting this point. The EPA counters that while monitoring agencies may statistically correct data from a PM continuous monitor for AQI purposes (40 CFR part 58, appendix G), there are both examples of well performing statistically corrected PM continuous monitors being used for AQI purposes; however, without proper attention and updates, there are also examples of poorly performing ones. Finally, another commenter believes that a national correction factor cannot possibly incorporate data to represent all the scenarios across the nation that have an impact on monitor performance and data quality. Although the EPA agrees that there are a variety of local scenarios that could affect monitor performance, the overall benefits of having nationally consistent measurement of PM concentrations and national calibration of data outweigh the potential advantages of locally specific calibrations.
Several commenters also disagreed with using local and regional calibrations of data, including some monitoring agencies that asserted being unable to reinvest in the operation of FRMs that would be required to locally calibrate their own PM FEMs. Further, every approved PM FEM method designated today is effectively calibrated through demonstration of field testing in the areas in which it was required to be tested (40 CFR 53.35(b)(1)). Moreover, the EPA proposed to require instrument manufacturers to demonstrate that they can improve the number of sites meeting bias MQOs by initiating a recalibration of an FEM. Thus, the use of a national set of sites where the methods are operated is essentially a fine-tuning of the PM FEMs performance across all sites where it is used.
After considering all the comments received, the EPA believes it is appropriate to finalize as proposed with a representative set geographic locations at SLT sites to calibrate PM FEMs. Identification of such sites would be made by the applicant of the planned updated calibration, subject to EPA approval, and submitted to the EPA in accordance with the requirements and application instructions in 40 CFR part 58, appendix C, sections 2.2 and 2.7. The EPA encourages early communication between an applicant seeking a method update and the EPA to facilitate the most appropriate sites are included in any updated application of the methods calibration.
The EPA proposed that instrument companies may, but are not required to, check for and exclude any potential outliers that may exist in the validated State, local, and Tribal agency network data available from AQS that would be used to establish new factory calibrations. The EPA received two comments regarding potential outlier approaches. One commenter disagreed with the proposed approach and instead recommended the use of all “validated” data, because how these instruments behave under normal operating ranges may be just as important as how they behave when monitoring conditions are low or elevated. The EPA acknowledges this point; however, the proposal on outliers allows flexibility in using standard outlier tests if needed to include or exclude such data as part of the calibration process. Ultimately, the true test of success for an updated method calibration will be that a higher number of sites are meeting bias MQOs in the areas in which the method is used, which will include all routine valid data including any potential outliers. Another commenter asserted concerns with the ability of instrument manufacturers to analyze data within individual monitoring agencies. The EPA disagrees with the commenter because decisions whether to include or exclude outliers should be flexible and made on a case-by-case basis. Moreover, the expected substantially larger dataset from routinely operated collocated FRMs and FEMs compared to what was Start Printed Page 16354 used in the original FEM designation testing (§ 53.35 Test procedure for Class II and Class III methods for PM2.5 and PM10–2.5) will minimize the effect of any potential outliers.
In contrast to these two comments, the EPA received many comments supportive of the proposed outlier approach overall. Therefore, the EPA is finalizing this part of the proposal that instrument companies may, but are not required to, check for and exclude any potential outliers that may exist in the validated State, local, and Tribal agency network data available from AQS that would be used to establish new factory calibrations.
Several commenters offered input on statistical criteria and initial testing requirements for approval of candidate PM FEMs and the role of instrument manufacturers in this process. The EPA did not propose any changes related to these issues; however, these comments have been considered below.
One commenter suggested that data quality objectives, bias, and precision estimators for different monitoring methods should be based on averages at both national and regional levels for purposes of comparison. Another commenter asked to strengthen the criteria for Class 3 Equivalency standards for candidate PM instrumentation. On testing requirements, one commenter recommended that the EPA consider updating the 40 CFR part 53 process for approving FEMs so that the testing process more closely reflects the regulatory deployment and data handling that generates NAAQS-comparable data. Another commenter asked that the results from “summer” and “winter” field evaluations not be averaged together because it allows agencies to minimize the error of biased instruments by averaging poor results with data often biased in the other direction. The same commenter also recommended that candidate instruments data sets should not be averaged together as is done currently where data from triplicate instruments are averaged for each day. Another commenter asked that the EPA require FEM field comparability tests in the northwest ( e.g., in EPA Region 10) in areas where particulate derived from biomass predominates to ensure that certified instruments will perform reliably in regions influenced by these sources. Related to the different measurement principles and the instrument companies' role in PM FEMs, one commenter noted that FEMs may never align perfectly with the FRMs due to the use of different measurement principles. Another commenter asked that manufacturers of FEM instruments be held accountable for ensuring that they continue to meet FEM criteria, whether through calibration updates and/or follow-up evaluations. Another commenter suggested that instrument manufacturers should be required to further evaluate the FEM monitoring data at defined intervals including, but not limited to, the 2-year and 5-year approval anniversaries.
The EPA did not propose to make modifications to the statistical criteria or testing requirements; however, we did solicit comment on any alternatives that would lead to more sites meeting the bias MQO with automated FEMs, especially for those sites that are near the level of the primary annual PM2.5 NAAQS as proposed (88 FR 5672–73, January 27, 2023). While the comments requesting that the statistical criteria be strengthened may have merit, doing so would not address the large inventory of already deployed PM FEMs used throughout the country. Also, without performing a detailed Data Quality Objective (DQO) design process, it is unclear how changing one or more statistical criteria would help improve the number of sites meeting the bias MQO now or in the future. Similarly, while the comments asking for changes to the locations of testing may also have merit, the EPA believes this could be a deterrent for instrument manufactures to seek additional improvements since more testing would be required, at least for candidate methods. Regarding the comment on the different measurement principles, the EPA concurs that different measurement principles may never align perfectly. Also, the EPA notes that the Agency has longstanding goals for acceptable measurement uncertainty of automated and manual PM2.5 methods in 40 CFR part 58, appendix A, section 2.3.1.1. Therefore, while having different measurement principles align is useful, meeting the goal for acceptable measurement uncertainty is the objective.
Regarding the comments related to the instrument companies' role in PM FEMs, the EPA notes that FEMs are already required to meet 40 CFR 53.9, “Conditions of designation.” Specifically, 40 CFR 53.9(c) requires that, “Any analyzer, PM10 sampler, PM2.5 sampler, or PM10–2.5 sampler offered for sale as part of an FRM or FEM shall function within the limits of the performance specifications referred to in § 53.20(a), § 53.30(a), § 53.35, § 53.50, or § 53.60, as applicable, for at least 1 year after delivery and acceptance when maintained and operated in accordance with the manual referred to in § 53.4(b)(3).” The EPA does not have the authority to require instrument manufacturers to further evaluate the FEM monitoring data at defined intervals, including but not limited to the 2-year and 5-year approval anniversaries, as one commenter suggested.
In addition to these few recommendations, the EPA received many comments supportive of the proposal that valid State, local, and Tribal air monitoring data from FRMs generated in routine networks and submitted to the EPA may be used to improve the PM concentration measurement performance of approved FEMs; therefore, consistent with the proposal we are not finalizing any updates to the statistical criteria, testing requirements, or requirements on instrument manufactures as proposed.
The EPA proposed that any new factory calibration should be developed using data from at least 2 years and tested on a separate year(s) of data (88 FR 5672, January 27, 2023). Comments on this part of the proposal were generally supportive. One commenter requested that at least a 3-year dataset, rather than the proposed 2 years, be used for a representative design value comparison of the FEM and FRM datasets to be evaluated. Another commenter pointed out that as large a data set as possible should be used, but EPA should not limit it to only data collected by instruments that have operated for more than 2 years.
In response to these comments, the EPA notes the broad support for the proposal as written. Also, the EPA notes that the 2-year period for using data to develop a factory calibration is a minimum, and that more years may be used as appropriate. Therefore, the EPA is finalizing its approach that any new factory calibration should be developed using data from at least 2 years and tested on a separate year(s) of data as proposed.
The EPA proposed several aspects of the FEM calibration on which we did not receive specific comments, including a provision that FEM methods should be evaluated by monitoring agencies as part of routine data assessments, such as during certification of data and 5-year assessments; the fact that the EPA recognizes only data from existing operating sites are available for use in factory calibrations; and recognition that an updated factory calibration does not have to work with the original field study data submitted that led to the designation as an FEM. With the broad general support from commenters summarized above, the EPA is finalizing each of these Start Printed Page 16355 individual aspects of the FEM calibration as proposed.
In the proposal, the EPA identified that we should expect a lag between the date when an already designated method is approved with a new factory calibration as an updated method by the EPA and when it can be implemented in the field. The EPA solicited comment on how to approach the data produced during this lag. Commenters provided input not only on how to address data during the lag, but also regarding how to address data already collected prior to a method update that has the potential to be used in regulatory decision making, particularly where such collected data do not meet the bias MQO. In response to this solicitation of comment, there was a consistent recommendation that calibrations of data associated with method updates should be applied to all relevant PM data prior to the EPA using it for designations under a final NAAQS.
While the EPA appreciates these comments and recognizes their support for retroactive data correction, at this time and following this final rule, monitoring agencies should continue to report PM FEM data as measured. This component of this final rule is focused only on revising 40 CFR part 53, appendix C to implement an updated calibration for approved PM FEMs. The issue of how prior and future monitoring data will be used in the implementation of this NAAQS, such as for designations, and for air quality regulatory programs is outside the scope of this rulemaking and will therefore be addressed by the EPA in a subsequent relevant action or actions.
The EPA received comments on whether updates to PM FEM methods should be required to be implemented or there would flexibility in when and if a monitoring agency implemented them. The commenters asked that EPA be flexible in allowing the use of updated method correction factors intended to improve the data comparability between the FRMs and FEMs.
In most cases, the EPA expects that updating the FEMs will result in improved data quality and more sites meeting bias MQOs; however, the EPA is not finalizing an update requirement in this action. Monitoring agencies can assess their data and make decisions on an update based on whether they are meeting the bias MQOs. Such decisions on whether or not to update a method may efficiently be included in those agencies' annual monitoring network plans under 40 CFR 58.10, “Annual monitoring network plan and periodic assessment,” which are already subject to EPA Regional office approval. In some circumstances, it is possible the original PM FEM may be revised in a manner where only the updated method has an active approved designation. In these cases, monitoring agencies would need to address updating their PM FEM in a timely manner.
The EPA solicited input on any alternative approaches that could lead to more sites meeting the bias MQO with automated PM FEMs, especially for those sites that are near the level of the primary annual PM2.5 NAAQS as proposed to be revised in section II above. A few commentors provided input on potential options for alternative approaches and several others offered input on how a local or regional calibration of an FEM could work. Among alternative approaches, one commenter suggested that manufacturers of FEMs could provide settings that would allow for adjustments to make FEM data more “FRM-like.” Another commenter suggested working with the manufacturers of FEM equipment to diagnose the cause of the bias and then to address it appropriately.
The EPA received several comments on how to implement a local or regional calibration of FEMs. One commenter suggested that EPA could allow for SLT agencies to adjust FEM data to be more “FRM-like” prior to submitting data to AQS. Another commenter suggested using a rolling 3-month linear regression based on a comparison of FEM data to PM2.5 levels measured by a 1-in-6-day FRM. Another commenter recommended that the EPA allow the application of a correction factor that is from an area with a similar climate and other conditions. Another commenter suggested that, for metropolitan statistical areas (MSAs) where the re-calibrated FEMs still do not meet equivalency criteria, monitoring agencies should be able to use the rolling linear regression technique to further calibrate the FEMs within an MSA. Another commenter suggested that developing a simple linear regression could establish the relationship between FEM data and FRM data and be used to adjust the FEM data at each site where they are collocated. Another commenter suggested that averaging the results within a MSA and applying it on an MSA basis with the previous 2 years of data could provide an adjustment method for sites without a collocated FRM. Another commenter identified that a regional correction factor potentially could improve instrument accuracy to biomass sources, which are a large component of PM in many communities.
Among the alternative approaches suggested, having settings that would allow for adjustments to make FEM data more “FRM-like” has merit, but assuming this was within a PM FEM itself, it would need to be separately incorporated into each make and model of FEM. If EPA were to pursue this alternative approach, the suggestion could be incorporated into a future regulatory action as a potential condition of designation because, without having the opportunity to thoughtfully consider how every step of such an approach would need to work, including what such requirements would look like and how potential settings adjustments would be made, it is not appropriate for the EPA to require the availability of such settings now, nor would it address the inventory of currently available PM FEMs already operating.
Regarding the suggestion that the EPA and SLTs should work with the manufacturers of FEM equipment to diagnose the cause of any biases and then to address them appropriately, the EPA supports this recommendation, but does not believe a regulatory change is required to allow the monitoring community (EPA and SLTs) to work with instrument manufacturers in this way.
Regarding the several comments on how to implement a local or regional calibration of FEMs, the EPA acknowledges the desire for this flexibility but believes that any such provisions for local or regional calibration of FEMs would need to be thoroughly thought out and proposed for consideration across the monitoring community. While several commenters support such an approach, the EPA also received adverse comments on the potential for local and regional calibration of PM FEMs instead of national. Most of the criticism of local and regional calibration of PM FEMs centered on both the lack of existing operating PM FRMs in commenters' networks and monitoring agencies' inability to staff the higher number of operating FRMs that would have to be collocated with PM FEMs to calibrate. Thus, the commenters that oppose local and regional calibrations of data prefer to utilize the national calibration of FEM data as proposed. Acknowledging all of these viewpoints, the EPA believes that it would not be appropriate to institute such an approach at this time. As discussed throughout this section, this final rule, the EPA is embarking on a new national approach to calibration of FEMs where valid State, local, and Start Printed Page 16356 Tribal air monitoring data from FRMs generated in routine networks and submitted to the EPA may be used to improve the PM concentration measurement performance of approved FEMs. The EPA and the community of SLT monitoring agencies can further consider other solutions to improving PM FEM methods, including local and regional scale calibration of FEMs, in a future review of the PM NAAQS.
In summary, the EPA is finalizing its proposal to allow valid State, local, and Tribal air monitoring data from PM FRMs and FEMs generated in routine networks and submitted to the EPA to update factory calibrations included as part of approved FEMs (40 CFR part 58, appendix C, sections 2.2 and 2.7). This approach, which will typically be initiated by instrument manufacturers but can also be spurred by monitoring agencies, MJOs of monitoring agencies, and the EPA itself, is to be implemented as a national solution in factory calibrations of approved FEMs through a firmware update, subject to EPA approval. FEM calibrations can apply to any PM FEM methods ( i.e., PM10, PM2.5, and PM10–2.5). As part of this process, the EPA is finalizing that a range of data based on the most representative concentrations up to all available concentrations may be used in developing and testing a new factory calibration; that a representative set of geographic locations can be used; that outliers may be included or not included; that a new factory calibration should be developed using data from at least 2 years and tested on a separate year(s) of data; that updates to factory calibrations can occur as often as needed and should be evaluated by monitoring agencies as part of routine data assessments such as during certification of data and 5-year assessments; that the EPA recognizes only data from existing operating sites is available; and that an updated factory calibration does not have to work with the original field study data submitted that led to the designation as an FEM. The EPA is finalizing this approach as proposed with the intention of having more sites meet the bias MQOs with automated PM FEMs.
4. Revisions to the PM2.5 Monitoring Network Design Criteria To Address At-Risk Communities
To enhance protection of air quality in communities subject to disproportionate air pollution risk, particularly in light of the proposed range for a revised primary annual PM2.5 standard, the EPA proposed to modify the PM2.5 monitoring network design criteria to include an environmental justice (EJ) factor that accounts for proximity of at-risk populations ( i.e., those identified in the 2019 ISA and ISA Supplement as being at increased risk of adverse health effects from PM2.5 exposures to sources of concern), consistent with the statutory requirement that the NAAQS protect the health of at-risk populations (88 FR 5673, January 27, 2023). Specifically, the EPA proposed to modify the existing requirement at 40 CFR part 58, appendix D, section 4.7.1(b)(3)): “For areas with additional required SLAMS, a monitoring station is to be sited in an area of poor air quality,” to additionally address at-risk communities with a focus on anticipated exposures from local sources of emissions. The scientific evidence evaluated in the 2019 ISA and ISA Supplement indicates that sub-populations at potentially greater risk from PM2.5 exposures include children, lower socioeconomic status (SES) [188] populations, minority populations (particularly Black populations), and people with certain preexisting diseases (particularly cardiovascular disease and asthma). The EPA proposed that communities with relatively higher proportions of sub-populations at greater risk from PM2.5 exposure within the jurisdiction of a State or local monitoring agency should be considered “at-risk communities” for these purposes.
The PM2.5 network design criteria have led to a robust national network of PM2.5 monitoring stations. These monitoring stations are largely in Core-Based Statistical Areas (CBSAs) [189] across the country that include many PM2.5 monitoring sites in at-risk communities. Many of the epidemiologic studies evaluated in the 2019 ISA and ISA Supplement, including those that provide evidence of disparities in PM2.5 exposure and health risk in minority populations and low-SES populations, often use data from these existing PM2.5 monitoring sites. However, we anticipate that with the more protective annual NAAQS finalized in section II above, characterizing localized air quality issues around local emission sources may become even more important. The EPA believes that adding a network design requirement to locate monitors in at-risk communities will improve our characterization of exposures for at-risk communities where localized air quality issues may contribute to air pollution exposures. Requiring that PM2.5 monitoring stations be sited in at-risk communities will allow other methods to be operated alongside PM2.5 measurements to support multiple monitoring objectives per 40 CFR part 58, appendix D, section 1.1. The EPA believes that it is appropriate to formalize the monitoring network's characterization of PM2.5 concentrations in communities at increased risk to provide such areas with the level of protection intended with the PM2.5 NAAQS. The addition of this requirement will also lead to enhanced local data that will allow air quality regulators help communities reduce exposures and inform future implementation and reviews of the NAAQS.
The EPA received comments concerning the proposed requirement to modify the PM2.5 monitoring network design criteria to include an EJ factor that accounts for the proximity of populations at increased risk of adverse health effects from PM2.5 exposures to sources of concern. Commenters included State, local, and Tribal air agencies and multijurisdictional organizations (MJOs) comprised of those agencies; industry and industry groups; other Federal, State, and local government entities; public health, medical, and environmental nongovernmental organizations (NGOs); and private citizens. The EPA proposed to require that sites located in at-risk communities (particularly those whose air quality is potentially affected by local sources of concern) should nonetheless meet the requirements to be considered representative of “areawide” air quality as this is consistent with all other minimally required sites. There were several other technical components of the proposed requirement for which we asked for comment, including: how to identify at-risk communities; the PM sources of concern important to consider; the datasets that can be used to identify communities with high exposures; the most useful measurement methods to collocate with PM2.5 in at-risk communities; and the timeline to implement any new or moved sites.
Overall, most commenters were very supportive of the EPA's proposed modification to the PM2.5 monitoring Start Printed Page 16357 network design criteria to include an EJ factor that accounts for proximity of populations at increased risk of adverse health effects from PM2.5 exposures to sources of concern. A few commenters offered detailed supporting comments. For example, one commenter recommended targeting investment in regulatory monitors in EJ communities, opining that there is presently a lack of equitable distribution of these monitors in low-income and minority communities. Another commenter supports the inclusion of an EJ factor in PM2.5 monitoring network design criteria as a means to assess whether disparities in exposure are reduced in the future. The EPA appreciates the support for the proposed requirement and acknowledges the desirability of a goal to assess if disparities in exposure are reduced in the future as a result of these monitoring efforts.
Some commenters were generally supportive of the proposed requirement but suggested that the EPA should recast the approach in a more specific way or offered additional examples of sources of concern. For example, one commenter stated that PM2.5 emissions from residential and commercial wood burning result in localized hotspots that are often not revealed by community air monitoring. Another commenter asked that the EPA adopt a strategy to monitor EJ communities near both larger well-known point sources of PM2.5 and along traffic corridors as well as smaller sources that, when taken together, may create a large amount of emissions and health harms in the area. Another commenter stated that the national network of monitors operated by the EPA captures data used for generalized modeling, but overall monitoring is not as granular as one would expect, especially in urban areas. For instance, the commenter suggested that EPA could monitor suspected “hot spots” ( e.g., residential development adjacent to highways and active construction sites) to better manage and mitigate PM2.5 pollution at their sites of origin, and that more extensive and granular monitoring data would also facilitate essential research and inform future evaluations and adjustments of the NAAQS. The EPA acknowledges these comments identifying other sources of concern, and we address these and other potential sources of concern below.
Among adverse comments, a few commenters stated that “at-risk communities” is not well defined. The EPA disagrees and directs those commenters to the numerous places where this definition is covered, including in Section II.B.2 of the proposal where we explained the term related to a variety of at-risk populations (88 FR 5591–92, January 27, 2023) as well as section 12.5 of the 2019 ISA (U.S. EPA, 2019a) and section 3.3.3 of the ISA Supplement (U.S. EPA, 2022a). Other commenters oppose the addition of the proposed monitoring because they feel it would reduce flexibility for agencies in deciding where they should site monitors, advocating that monitoring agencies should be afforded maximum flexibility to identify where to site monitors for at-risk areas. Because the EPA recognizes the challenges cited by these commenters related to establishing new ambient air monitoring stations, the EPA is finalizing the modified requirement on PM2.5 monitoring network design criteria intended to address at-risk communities that allows flexibility regarding which EJ communities should be monitored. Finally, one commenter asked that the EPA clarify a specific metric to judge how to site monitors in at-risk communities. Instead, the EPA believes it is appropriate for agencies to recommend what they believe to be the most important things to consider for their sites to meet the PM2.5 network design requirements and, thus, applying a new metric could take away from local priorities for at-risk communities.
A few commenters asked that the EPA require more monitoring than proposed. One commenter stated that it would be more beneficial to overburdened communities if air monitoring were required in all at-risk communities. A few commenters asked that EPA require additional monitoring for attainment of PM2.5 NAAQS in EJ communities. In response to these comments, the EPA supports the SLT agencies' initiatives to conduct additional monitoring beyond the minimum monitoring requirements and network design criteria. In addition, the EPA supports agencies' use of alternative datasets such as sensors and sensors networks, satellites, and other non-regulatory monitoring where appropriate for non-regulatory data uses. The EPA notes that many monitoring agencies already operate more monitoring sites than are minimally required, and we expect this to continue as agencies consider siting monitors in at-risk communities.
However, the EPA also received substantial concerns from monitoring agencies about their resource constraints, including staffing to support any potential new monitoring. The EPA also notes that the existing and robust network of almost 1,000 PM2.5 sites nationally is designed to continue to protect all populations at the level of the NAAQS discussed in section II of this final action by always having at least one site in the area of expected maximum concentration for each CBSA where monitoring is required. As a result of the revisions to the annual PM2.5 NAAQS being finalized in this action, a small number of new monitoring sites will also be required under EPA's current minimum monitoring requirements. With the monitoring network design changes finalized in this rule, many of these existing and new sites will form an important sub-component of the PM2.5 network by better characterizing air quality in at-risk communities, particularly with respect to sources of concern.
The EPA concludes that the requirements in this final rule for siting of monitoring in at-risk communities will meaningfully improve the PM2.5 monitoring network and its characterization of air quality in at-risk communities, without placing substantial new resource burdens on States and their monitoring agencies that would be associated with requirements for additional monitoring sites. Therefore, the EPA is finalizing this part of the proposed action without requiring additional monitoring sites beyond what would be associated with the revised annual PM2.5 NAAQS described in section II as they pertain to the minimum requirements associated with Table D–5 of Appendix D to Part 58—PM2.5 Minimum Monitoring Requirements.
A few commenters asked that the EPA enhance monitoring in smaller cities and rural areas. One commenter asked for the EPA to extend the proposed monitoring network to Micropolitan Statistical Areas with populations of 10,000–50,000 and to rural areas. Another commenter pointed out that current air quality monitoring networks focus on urban and densely populated areas; therefore, rural areas are often not captured in this existing monitoring infrastructure, despite well-documented examples of high PM concentration in rural communities. The commenter believes this results in inadequate assessment of air pollution exposures for a substantial segment of the U.S. population. The EPA disagrees that there needs to be additional requirements for small CBSA's and rural areas. Regarding these comments, the EPA points out that we have a long-standing requirement for each State to monitor at background and transport sites (40 CFR part 58, appendix D, section 4.7.3—Requirement for PM2.5 Background and Transport Sites). Also, if an agency deems it appropriate to do so, monitoring coverage of rural areas can be accomplished with other tools Start Printed Page 16358 such as sensors and sensors networks, satellites, and other non-regulatory monitoring. Although there may be short-term high exposures in rural areas, there is no evidence that long-term averages are higher in rural areas compared to urban areas with significantly higher density of populations and emissions. For smaller cities or rural areas that may have concentrations near the level of the PM2.5 NAAQS finalized in section II above, monitoring agencies are encouraged to monitor and address emissions as appropriate.
Some commenters disagree that the proposed revision to the PM2.5 monitoring network design criteria to address at-risk communities is needed. One commenter stated that including an EJ factor is not necessary because the current network is designed to protect all citizens. Another commenter stated that EJ factors could be cumbersome to implement. Another commenter asserted the proposal to add SLAMS in at-risk communities with higher PM2.5 concentrations might create more granular data and provide for a greater margin of safety for those communities and monitors in such a way that data from those areas could misrepresent the larger area represented by the network. In response to the comment on the current network protecting all citizens, the EPA agrees that by measuring in the community with the highest concentration of PM2.5 we protect other citizens; however, as stated in the proposal, the EPA believes that adding a requirement for sites with an EJ factor near sources of concern will enhance the overall network to the benefit of all citizens. Also, we anticipate that with the more protective annual NAAQS finalized in section II above, characterizing localized air quality issues will become even more important around local emission sources. As for EJ factors being cumbersome to implement, the EPA disagrees because there are many such locations already operating successfully in the current network. Regarding the comment that sites in at-risk communities may misrepresent the larger area represented by a particular network, the EPA notes that pursuant to 40 CFR part 58, minimally required sites in a given network are to represent area-wide air quality; therefore, sites in at-risk communities, by definition, would be representative of the communities within the network in which they are sited for the level of protection intended under the annual PM2.5 NAAQS.
In the proposal, the EPA identified that, in light of the evidence of increased risk to at-risk communities, it would be appropriate to better characterize exposures for communities in proximity to local sources of concern (88 FR 5673–76, January 27, 2023). Thus, the EPA proposed that enhanced networks should include representation of at-risk communities living near emission sources of concern ( e.g., major ports, rail yards, airports, industrial areas, or major transportation corridors). The EPA requested comment on the types of sources of concern most important to consider. In addition to supporting the types of sources the EPA identified in the proposal, commenters also identified several additional localized sources such as railroads, stationary sources, transportation facilities, and communities with high numbers of wood stoves.
A few commenters suggested the inclusion of sources that are often considered line and/or area sources, e.g., traffic corridors and emissions from federally regulated facilities, military installations, and national forests. Commenters also identified other sources usually associated with long-range transport such as smoke from wildfire and prescribed fires and long-distance transport of PM, for example from Saharan dust and other international transport. As explained in the proposal, the site with the highest expected PM2.5 is already required to have a monitor by our long-standing requirement that monitors be placed “. . . in the area of expected maximum concentration” (§ 58.1 and appendix D, section 4.7.1(b)(1)). The EPA expects that both sites with the expected maximum concentration and sites specifically placed in at-risk communities would be impacted by any long-range transport in the area. Therefore, the EPA believes any emphasis on the sources of concern should prioritize localized sources, including point, area, and line sources of concern impacting the at-risk community of interest. Therefore, based upon the comments, the EPA is finalizing a broader example list of sources of concern to include localized sources such as point sources and transportation facilities, since these are the most commonly expected additional sources of concern. In response to the other sources of concern suggested by commenters, the EPA notes that while it has provided examples, the siting of monitors in EJ communities would not be limited to these examples. Thus, the revised set of examples would include “a major industrial area, point source(s), port, rail yard, airport, or other transportation facility or corridor.” In finalizing this modified list of examples, the EPA is not looking to prioritize one type of source category over another; rather, we intend to further illustrate the types of localized sources of pollution that might impact at-risk communities such that the siting of monitors nearby may be appropriate.
One commenter noted that the proposal may have unintentionally taken out the requirement related to specific design criteria for PM2.5 in 40 CFR part 58, appendix D, 4.7.1(b)(3) that, for an area with a requirement for an additional SLAMS monitor, it should “be sited in an area of poor air quality.” Thus, the language as proposed neither requires that such monitors be sited in areas of poor air quality, nor does it require that the monitor be sited in an area that is anticipated to experience poor air quality from unspecified (and thus potentially relatively insignificant) sources in the area. The EPA agrees that this was not our intention; the EPA wants to protect populations in at-risk communities by ensuring they are protected by the NAAQS when there are sources of concern that may be impacting them ( i.e., not insignificant sources). Thus, the EPA is reinstating this requirement in the network design language and combining it with the examples of the types of localized sources of concern: “For areas with additional required SLAMS, a monitoring station is to be sited in an at-risk community with poor air quality, particularly where there are anticipated effects from sources in the area ( e.g., a major industrial area, point source(s), port, rail yard, airport, or other transportation facility or corridor).”
To ensure minimally required monitoring sites appropriately represent exposures in at-risk communities, the EPA proposed that sites represent “area-wide” air quality near local sources of concern (88 FR 5674, January 27, 2023). Sites representing “area-wide” air quality are those monitors sited at neighborhood, urban, and regional scales, as well as those monitors sited at either micro- or middle-scale that are identified as being representative of many such locations in the same Metropolitan Statistical Area (MSA).[190] Most existing—as well as new or moved sites—are expected to be neighborhood-scale, which means that the monitoring stations would typically represent conditions throughout some reasonably homogeneous urban sub-region with dimensions of a few kilometers per part 58, appendix D, section 4.7.1(c)(3). Additionally, as described in § 58.30, Start Printed Page 16359 sites representing “area-wide” air quality have a long-standing applicability to both the annual and 24-hour PM2.5 NAAQS. Our proposed requirement for siting monitors in communities representing “area-wide” air quality is consistent with other network design objectives pursuant to which we seek to have monitors located where people live, work, and play.
The EPA received a few comments on its proposed requirement that minimally required sites represent “area-wide” air quality. One commenter stated that the inclusion of a provision for EJ would narrow the location of monitors to certain communities that may not best represent “areawide” air quality. Another commenter asked the EPA to consider removing requirements that sites be area-wide, since 24-hour and annual averaging times would miss short, elevated pollution events. A couple commenters had concerns with the difference in the scale of representation between EJ monitors using small scale and other NAAQS monitors using area-wide scale, in that area-wide scale would not protect those most at risk. However, another commenter agreed with the EPA that sites representing at-risk communities should represent area-wide air quality. In addition to these comments, the EPA received many comments with support for its proposed modifications to the network design criteria as whole.
Regarding whether narrowing the location to certain communities may not best represent “area-wide” air quality, the EPA notes that sites are either identified as being area-wide or not; the EPA did not suggest it was seeking a best “area-wide” location. In response to the comment that area-wide site may miss short, elevated pollution events, the EPA is aware that there can be local, short-term spikes in PM2.5 concentrations. However, the network design criteria associated with minimally required sites is applicable to both the annual and 24-hour PM2.5 NAAQS, and the EPA believes it is appropriate to continue to ensure all minimally required sites have the most utility and remain applicable to both forms of the PM2.5 NAAQS. The identification of unique micro- and middle-scale sites was directed at discretionary efforts of any monitoring agency, with the recognition that such sites, ( i.e., relatively unique micro-scale, or localized hot spot, or unique middle-scale impact sites), are not applicable to the annual NAAQS as described in § 58.30—Special consideration for data comparison to the NAAQS.
After considering all the comments on this topic, the EPA is finalizing this part of the modification to the network design criteria to maintain, consistent with our long-standing network design criteria, that all minimally required sites are to represent area-wide air quality.
In addition to using data from the robust network of almost 1,000 PM2.5 sites for NAAQS and AQI purposes, having a stable network of long-term sites is especially valuable to examine trends and to inform long-term health and epidemiology studies that support reviews of the PM NAAQS. Therefore, while we proposed to add a PM2.5 network design criterion to address at-risk communities, many sites are likely already in valuable locations meeting one of the existing network design criteria ( i.e., being in an area-wide area of expected maximum concentration or collocated with near-road sites) and supporting multiple monitoring objectives. Also, in many communities, there may already be sites meeting the network design criterion we proposed for at-risk communities. Thus, acknowledging the value of having long-term data from a consistent set of network sites, the EPA believes that moving sites should be minimized, especially in MSAs with a small number of sites. However, because a small number of new sites are expected to be required due to the existing minimum monitoring requirements (40 CFR part 58, appendix D, Table D–5) [191] and the revised primary annual PM2.5 NAAQS detailed in section II, and because sites occasionally have to be moved—due to, for example, loss of access to a site or a site no longer meeting siting criteria—the EPA believes it is appropriate to prioritize establishing sites in at-risk communities near sources of concern, whenever new sites are established, whether because it is a new site or a replacement for a prior site that must be moved. The EPA accordingly proposed that annual monitoring network plans (40 CFR 58.10(a)(1)) and 5-year assessments (40 CFR 58.10(d)) that include any of the few new sites that will be required include a commitment to examine the ability of existing and proposed sites to support air quality characterization for areas with at-risk populations in the community and the objective discussed herein.
In the proposal, the EPA identified that assessing and prioritizing at-risk communities for monitoring can be accomplished through several approaches (88 FR 5675). The most critical aspect of prioritizing which communities to monitor is their representation of the at-risk populations described earlier in this section. The other major consideration is whether the community is near a source or sources of concern. While many CBSAs have one or more sources of concern described above, some CBSAs will not have a quantity of emissions from sources of concern that result in an elevated level of measured PM2.5 concentrations in surrounding communities. The siting criteria to be “in the area of expected maximum concentration,” § 58.1 & appendix D, section 4.7.1(b)(1) ensures there is a monitoring site in the community with the highest exposure in each CBSA with a monitoring requirement. Some CBSAs may also have a requirement to collocate a PM2.5 monitor at a near-road NO2 station. Therefore, the EPA believes that for cases where an additional PM2.5 site is required, we should include a criterion that the site be in an at-risk community when there are no sources of concern identified in that CBSA, or such sources do exist but are not expected to lead to elevated levels of measured PM2.5 concentrations.
In its proposal, the EPA highlighted that tools such as the EPA's EJSCREEN [192] are available to identify the at-risk communities intended for monitoring as part of the proposed revision to the PM2.5 network design criteria (88 FR 5675–76, January 27, 2023). The EPA solicited comment on other tools and/or datasets that can be utilized to identify at-risk communities. In addition to support for using EJSCREEN, commenters identified several other options to identify at-risk communities intended for monitoring as part of the proposed revision to the PM2.5 network design criteria. Among similar tools, one commentor suggesting using CalEnviroScreen.[193] Commenters also identified different options for models including InMAP,[194] satellite-derived models that can be employed to help identify EJ communities, and hybrid models. A few commenters also suggested using sensors and sensor networks such as the BlueSky [195] and PurpleAir [196] sensors.
The EPA supports the use of other State and local tools designed to help identify the at-risk communities that Start Printed Page 16360 should be monitored to meet the revised network design criteria. The EPA additionally agrees with commenters that the use of models as well as sensors and sensor networks may be appropriate and helpful in identifying the most appropriate at-risk communities in which to locate monitors.
For at-risk communities, monitoring agencies need data that can best inform where there may be elevated levels of exposures from sources of concern. While we use FRMs and FEMs to determine compliance with the NAAQS, data from these methods will only be available at existing sites. However, there are several additional datasets available that may be useful in evaluating the potential for elevated levels of exposure to communities near sources of concern. In the proposal, EPA identified potential non-regulatory monitoring datasets such as CSN, IMPROVE, and AQI non-regulatory PM2.5 continuous monitors; modeling data that utilizes emission inventory and meteorological data; emerging sensor networks such as those that comprise EPA and the USFS's Fire and Smoke Map; [197] and satellites that measure radiance and, with computational algorithms, can be used to estimate PM2.5 from aerosol optical depth (AOD) (88 FR 5675–76, January 27, 2023). The EPA solicited comment on datasets most useful to identify communities with high exposures for PM2.5 NAAQS ( i.e., annual or 24-hour). In addition to providing information about datasets that can inform the NAAQS comparison, commenters additionally identified several types of datasets that may be useful to identify where there may be elevated levels of exposures from sources of concern. These datasets include satellite measurements, sensors, and sensor network data, which may all be useful to find hot spots in communities. Commenters also identified EJScreen and CalEnviroScreen, which are screening and mapping tools that utilize several datasets. Another commenter stated that to better understand exposure differences in disadvantaged communities, shorter measurement intervals should be measured and reported.
In considering the datasets identified in the proposal as well as the ones commenters provided, the EPA believes all the datasets have value to help inform where there may be elevated levels of exposures from sources of concern. However, each of them may also have limitations and, therefore, users should be careful not to rely solely on one dataset versus another for all purposes. Fortunately, many of the available datasets are becoming easier to work with and more accessible, which will allow interested parties and monitoring agencies the opportunity to efficiently review the datasets and determine best applicability. For all of these reasons, the EPA is not finalizing a requirement to use a specific dataset or tool to identify at risk communities; however, whatever datasets a monitoring agency elects to use, its plan to use such data for purposes of meeting the network design requirements will be subject to EPA approval as part of the 40 CFR 58.10 annual monitoring network plan. Regarding the comment recommending shorter measurement intervals in measuring and reporting data to better understand exposure differences in disadvantaged communities, the EPA agrees and generally supports use of continuous methods. While we generally support use of continuous methods, approved filter-based technologies and methods also provide valuable air quality information. Therefore, the EPA is not requiring the use of automated continuous methods beyond what is already required in 40 CFR part 58, appendix D, section 4.7.2—Requirement for Continuous PM2.5 Monitoring.
The monitoring methods appropriate for use at required PM2.5 sites in at-risk communities are FRMs and automated continuous FEMs (88 FR 5675–76, January 27, 2023). These are the methods eligible to compare to the PM2.5 NAAQS, which is the primary objective for collecting this data. There are several other monitoring objectives that would benefit from the use of automated continuous FEMs. For example, having hourly data available from automated continuous FEMs would allow sites to provide data in near-real time to support forecasting and near real-time reporting of the AQI. Automated continuous methods are also useful to support evaluation of other methods such as low-cost sensors. When used in combination with on-site wind speed and wind direction measurements, automated FEMs can provide useful pollution roses, which help in identifying the origin of emissions that affect a community. Additionally, when collocated with continuous carbon methods such as an aethalometer, automated FEMs can help identify potential local carbon sources contributing to increased exposure in the community. While either FRMs or automated FEMs may be used at a site for comparison to the PM2.5 NAAQS, the EPA supports use of automated continuous FEMs at sites in at-risk communities.
The EPA requested comment on the measurement methods most useful to collocate with PM2.5 in at-risk communities (88 FR 5675–76, January 27, 2023), and a few commenters provided input. One commenter recommended that the EPA should employ supplemental technologies and systems to increase coverage of the regulatory monitoring network and obtain more complete data to further protect public health and address environmental injustice in air pollution exposure. Another commenter recommended that the EPA invest in community-led monitoring and mobile air quality monitoring with a goal of recording block-level variabilities in data. And another commenter cited the value of community-deployed PM2.5 monitoring.
The EPA appreciates the comments provided on the measurement methods most useful to collocate with PM2.5 monitoring sites in at-risk communities. Because the use of methods beyond the required PM2.5 FRMs or FEMs or other criteria pollutant measurements meeting a NAAQS monitoring requirement is voluntary, the establishment of PM2.5 NAAQS comparable sites in at-risk communities will allow for collaboration at multiple levels. The EPA strongly encourages such collaboration with impacted communities, and the measurement methods discussed here should be considered for use as appropriate.
In the proposal, the EPA identified that, to meet the revised network design criteria, there will be only a few new sites required,[198] plus any potentially moved sites in cases where an existing site lease is lost or otherwise requires relocation (88 FR 5675–76, January 27, 2023). To handle these new or relocated sites, the EPA proposed to build upon our existing regulatory process for selecting and approving these sites under 40 CFR 58.10 (88 FR 5676, January 27, 2023). In the proposal, we stated it would be appropriate to provide at least 12 months from the effective date of the final rule to allow monitoring agencies to initiate planning to implement these measures by seeking input from communities and other interested parties and considering whether to revise their PM2.5 networks Start Printed Page 16361 or explain how their existing networks meet the objectives of the proposed modification to the network design criteria. Thus, the EPA proposed that monitoring agencies should address their approach to the question of whether any new or moved sites are needed and identify the potential communities in which the agencies are considering adding monitoring, if applicable, as well as identifying how they intend to meet the revised criteria for PM2.5 network design to address at-risk communities in the agencies' annual monitoring network plans due to each applicable EPA Regional office no later than July 1, 2024 (see 40 CFR 58.10). Specifics on the resulting new or moved sites for PM2.5 network design to address at-risk communities were proposed to be detailed in the annual monitoring network plans due to each applicable EPA Regional office no later than July 1, 2025 (40 CFR 58.10). The EPA proposed that any new or moved sites would be required to be implemented and fully operational no later than 24 months from the date of approval of a plan or January 1, 2027, whichever comes first, but the EPA solicited comment on whether less time is needed ( e.g., 12 months from plan approval and/or January 1, 2026).
The EPA received a few comments on its proposed timeline for monitoring agencies to identify, propose, and ultimately bring any new or moved sites online. One commenter asked that the timeline give states more time to start or move sites. A few commenters asked that the EPA only require meeting a timeline for identifying whether any new or moved sites are needed after the EPA has provided the monitoring agencies with guidance on the priority of the potential at-risk communities. One of those commenters further requests that the EPA allow at least 24 months from the date of approval of a § 58.10 monitoring plan identifying any relocation of monitoring sites or establishment of new monitoring sites to implement any changes to the network, citing the need for more time to work with local officials, procure monitoring equipment, and contract for services, all of which can cause significant delays in establishing a monitoring site. Another commenter asked that the EPA remain attentive to the challenges that States, and air agencies face regarding recruiting and retaining the specialized staff needed to support their existing regulatory monitoring networks and the capital resources needed to implement and sustain new monitoring stations in areas that are clearly meeting the existing PM NAAQS or any revised PM NAAQS. Another commenter stated that the July 1, 2024, timeline for a network evaluation this complex is insufficient, noting that they submit their draft annual monitoring network plan for public review and comment in mid-April for 30 days. Because the final plan is due July 1 and must include all comments and responses and describe any changes based on those comments, the timeline does not take these requirements into consideration by allowing for the more extensive assessment of changes that may be needed to meet the proposed new monitoring requirements. The commenter stated that it would be appropriate to provide at least 12 months from the effective date of this final rule for monitoring agencies to initiate planning to implement these measures, seek input, consider revisions to their PM2.5 networks, and explain how their existing networks meets the objectives of the final rule. The commenter notes that that SLT agencies should be provided a minimum of 18 months after the final recommendation is published to add this information to their § 58.10 annual monitoring network plans. Another commenter encourages the EPA to retain the proposed deadline for any newly required monitoring stations in at-risk communities to be operational ( i.e., 24 months after the July 2025 network plan approval or January 1, 2027, whichever is earlier). While the need for this data is urgent, the commenter stated that the process for procuring instrumentation, securing leases, and building permits, and other logistics in constructing new monitoring sites can take a significant amount of time, some of which are outside of agencies' control.
As stated earlier, the EPA received strong support for our proposal to modify the PM2.5 monitoring network design criteria to include an EJ factor that accounts for proximity of populations at increased risk of adverse health effects from PM2.5 exposures to sources of concern from a wide range of commenters. A few commenters support the timeline proposed, a few others support starting any new or moved sites sooner than proposed, while other commenters asked for more time or offered conditions regarding how to establish an appropriate timeline.
The EPA disagrees with the commenter that suggested the EPA should only require agencies to meet a timeline to identify whether any new or moved sites are needed after the EPA has provided the monitoring agencies with guidance on the priority of the potential at-risk communities, because the regulatory text provides all the guidance required for agencies to begin this process. As we explained above, the EPA does not anticipate that many new or moved sites will be required based on the final rule because we think most sites are already in suitable locations and long-term sites are highly valued. Also, monitoring agencies have discretion to provide to the EPA their recommendations regarding how they intend to meet the modifications to the PM2.5 monitoring network design criteria to include an EJ factor that accounts for proximity of populations at increased risk of adverse health effects from PM2.5 exposures to sources of concern. Overall, the EPA believes that having sites in the areas of expected maximum concentrations will best ensure that all communities are protected. Since there may be multiple choices for sites in EJ areas near sources of concern, the EPA acknowledges that there may be many locations that can meet the revised PM2.5 network design criteria. While, as we explained earlier, we want such sites to also be in areas of poor air quality, the sites in the area of maximum concentration will ensure that all communities are protected, there can be more flexibility afforded in the selection amongst at-risk communities to meet the revised requirements, since any alternative at-risk communities would already be protected.
The EPA considered both the concerns and support for the timeline proposed and clarifies that the component of the proposed requirement regarding the need to identify potential new sites or an intention to move sites to be included in the annual monitoring network plan due to EPA on July 1, 2024, would be satisfied with a statement of intent to pursue a new site per the revised network design criteria and in consideration of the minimum monitoring requirements. While monitoring agencies may provide as much detail as they deem appropriate regarding the revised PM2.5 network design criteria in their annual monitoring network plans due on July 1, 2024, there is no expectation that any details on site-specific information would be included at that stage. We encourage agencies to provide their initial thinking on the communities they are most interested in monitoring pursuant to the revised network design criteria. Therefore, the EPA is finalizing the timeline as proposed, including the provision that monitoring agencies report their intention to add or move sites, where required, in their annual monitoring network plans due to each applicable EPA Regional office no later than July 1, 2024 (40 CFR 58.10). The Start Printed Page 16362 monitoring agencies will then provide specifics on any new or moved sites for PM2.5 network design to address at-risk communities in the annual monitoring network plans due to each applicable EPA Regional office no later than July 1, 2025 (40 CFR 58.10). And any new or moved sites shall be implemented and fully operational no later than 24 months from the date of approval of a § 58.10 plan, or January 1, 2027, whichever comes first.
In summary, the EPA is finalizing modifications to the PM2.5 network design criteria to include an EJ factor to address at-risk communities with a focus on exposures from sources of concern in areas of poor air quality. While this modification to the PM2.5 network design requires sites to be located in at-risk communities, particularly those whose air quality is potentially affected by local sources of concern, such sites must still meet the requirement for being considered “area-wide” air quality. In finalizing this modification to the PM2.5 network design requirement, the EPA is making two changes in the final rule response to the comments received. First, the EPA is broadening our examples of “sources of concern” to include localized sources such as point sources and major transportation facilities or corridors. Second, the EPA is reinstating “poor air quality” in our requirement for the modified network design criteria, meaning the revised PM2.5 network design requirement now states: “For areas with additional required SLAMS, a monitoring station is to be sited in an at-risk community with poor air quality, particularly where there are anticipated effects from sources in the area ( e.g., a major industrial area, point source(s), port, rail yard, airport, or other transportation facility or corridor).” All other aspects of the PM2.5 network design requirements are being finalized as proposed.
5. Revisions to Probe and Monitoring Path Siting Criteria
The EPA proposed changes to monitoring requirements in the Appendix E—Probe and Monitoring Path Siting Criteria for Ambient Air Quality Monitoring (88 FR 5676–78, January 27, 2023). Since 2006, the EPA finalized multiple rule revisions to establish siting requirements for PM10–2.5 and O3 monitoring sites (71 FR 2748, January 17, 2006), Near-Road NO2 monitoring sites (75 FR 6535, February 9, 2010), Near-Road CO monitoring sites (76 FR 54342, August 31, 2011), and Near-Road PM2.5 monitoring sites (78 FR 3285, January 15, 2013). Through these previous revisions to the regulatory text, some requirements were inadvertently omitted, and, over time, the clarity of this appendix was reduced through those omissions that, in a few instances, led to unintended and conflicting regulatory requirements. The EPA proposed to reinstate portions of previous Probe and Monitoring Path Siting Criteria Requirements from previous rulemakings, where appropriate, to restore the original intent.
The EPA only received a few comments on the proposed rulemaking pertaining to the proposed changes regarding probe and monitoring path siting criteria for ambient air quality monitoring, most of which were supportive of the proposed revisions. One commenter noted that the image for Figure E–1 in Appendix E to part 58 was distorted and of extremely poor quality, rendering the text in places almost unreadable (88 FR 5712, January 27, 2023). The EPA makes several references to Figure E–1, which provides detailed information needed for assessing a range of acceptable probe distances from roadways based on a monitor's spatial scale. The commenter also stated that a higher quality image is needed for the figure so that agencies can fully interpret the figure to the extent that EPA requires. The EPA agrees with the commenter that a higher quality image for Figure E–1 is important and needed. Based on this comment, the EPA is finalizing the revision to Figure E–1 to clearly communicate the requirements of appendix E.
The EPA is revising appendix E in its entirety as proposed (88 FR 5709–5717, January 27, 2023) for clarity and as described in detail below.
a. Separate Section for Open Path Monitoring Requirements
The EPA proposed to relocate all open path monitor siting criteria requirements to a separate section in appendix E from those requirements for siting samplers and monitors that utilize probe inlets (88 FR 5676, January 27, 2023). Separate sections for these distinct monitoring method types allows the EPA to more clearly articulate minimum technical siting requirements for each.
The EPA received one supportive comment to adopt this change and received no adverse comments. Another commenter stated the regulatory text of the proposal improves the clarity of the appendix but encouraged the EPA to break the summary tables down further into more manageable components (perhaps by pollutant). The commenter stated that summary tables for the proposed appendix continue to be a “jumbled mess of regulatory requirements.” The EPA agrees that the summary tables E–3 and E–6 in the proposal could be improved further. Also, the EPA found that footnote 3 of Table E–6 in the proposed rule was incomplete and corrected this editorial error.
Therefore, the EPA is making editorial changes to both summary tables E–3 and E–6 and finalizing the remainder of the language as proposed with the open path monitor siting criteria requirements placed into a separate section of the appendix.
b. Distance Precision for Spacing Offsets
The EPA proposed to require that when rounding is performed to assess compliance with these siting requirements, the distance measurements will be rounded such as to retain at least two significant figures (88 FR 5676, January 27, 2023). The EPA proposed to communicate this rounding requirement in the regulatory text using footnotes in the tables of this appendix.
The EPA received two supportive comments and no adverse comments regarding this proposed change. While supportive of the proposal, one of the two supporting comments suggested it would be clearer if EPA explicitly defined a decimal in the distance values and round to the nearest tenths place for these assessments. The EPA disagrees with this recommendation because in some cases it would be more restrictive and burdensome than the proposed requirement that was intended to provide both clarity and flexibility. Therefore, the EPA is finalizing the language as proposed.
c. Summary Table of Probe Siting Criteria
The EPA proposed to provide additional specificity and flexibility to the summary table for probe siting criteria by changing the “>” (greater than) symbols to “≥” (greater than or equal to) symbols in the summary table E–4 (88 FR 5676, January 27, 2023). Because one commenter pointed out to the EPA that in the prior version of the rule there was no table E–4, as a clerical matter, we have renumbered this summary table to table E–3 in the final rule. This proposed minor revision to the summary table more clearly expresses the EPA's intent that the distance offsets provided in the summary tables in appendix E are acceptable for NAAQS compliance monitoring.
The EPA received one comment supporting the proposal. The EPA received no adverse comments. Because Start Printed Page 16363 one commenter pointed out to the EPA that in the prior version of the rule there was no table E–4, as a clerical matter, we have renumbered this summary table to table E–3 in the final rule. Therefore, the EPA is updating the table numbering and otherwise finalizing the tables as proposed.
d. Spacing From Minor Sources
The EPA proposed to clarify and provide flexibility regarding siting monitors near minor sources by changing a requirement to a goal (88 FR 5676–77, January 27, 2023). To accomplish this, the EPA proposed to replace the “must” in the regulation with a “should.” While the EPA proposed to change this requirement to a goal, the EPA reiterated in the proposal that it recommends that sites with minor sources be avoided whenever practicable and probe inlets should be spaced as far from minor sources as possible when alternative monitoring stations are not suitable.
The EPA received one comment supporting the proposed revision and received no adverse comments. Therefore, the EPA is finalizing the language as proposed.
e. Spacing From Obstructions and Trees
The EPA proposed to clarify and redefine that the minimum arc required to be free of obstructions for a probe inlet or monitoring path is 270-degrees and that probe inlets must be no closer than 10-meters to the driplines of any trees (88 FR 5677, January 27, 2023). These changes were proposed because of inconsistencies introduced into the rule with the 2006 rulemaking. Both are discussed in more detail in the following sections.
The majority of comments received were supportive of these proposed siting amendments and clarifications. Two commenters were not supportive of this proposal. One adverse comment focused on the potential that site modifications would be required if the minimum arc required to be free of obstructions for a probe inlet is 270-degrees. The second adverse comment pertained to the proposal to clarify distance requirements from tree driplines. The commenter stated they would expect significant challenges in meeting the proposed 20-meter tree dripline distance. This comment is not a substantive negative comment because the 20-meter distance provided in the proposal is a goal and not a requirement. As such, monitoring organizations should not expect additional challenges in meeting the probe siting requirements. One supportive commenter on the 270-degree minimum arc proposal also requested that the EPA acknowledge that some cases exist where monitoring is desired or necessary to protect the public health, but siting criteria cannot be met.
Based on the only two negative comments received from monitoring agencies or organizations, one of which was not substantive, the EPA believes most sites already meet these proposed requirements related to the arc and distance from dripline. However, the EPA also acknowledges that there may be limited cases where this proposed revision may require site modifications, and some sites may not be able to be achieve the proposed siting requirements, even with modifications to the site. For cases where long-term trend sites or monitors that determine the design value for their area cannot reasonably meet these regulatory siting requirements, the EPA encourages monitoring organizations to work with their respective EPA Regional offices to determine if a waiver from this siting criteria would be appropriate under appendix E, section 10.
These siting requirements are discussed in more detail below in sections VII.B.5.f and VII.B.5.h.
f. Reinstating Minimum 270-Degree Arc and Clarified 180-Degree Arc
The EPA proposed to correct identified inconsistencies in the 270-degree requirement for unrestricted airflow to the probe inlet by reinstating the requirement stated in appendix E, paragraph 4(b), and to clarify that the continuous 180-degree minimum arc of unrestricted airflow provision is reserved for monitors sited on the side of a building or wall to comply with network design criteria requirements specified in appendix D of part 58 (88 FR 5677, January 27, 2023).
The EPA received two comments regarding this proposal, with one being supportive and one being negative. The adverse comment focused on the potential that site modifications would be required if this revision was made. The commenter supporting the proposal also requested that the EPA acknowledge that some cases exist where monitoring is desired or necessary to protect the public health, but siting criteria cannot be met. The EPA agrees with both commenters and acknowledges that there does exist limited cases where this proposal would require site modifications and some sites may not be able to be achieve the proposed siting requirement even with modifications to the site. For these cases, and especially when long-term trend sites or monitors that determine the design value for their area cannot reasonably meet these regulatory siting requirements, the EPA encourages monitoring organizations to work with their respective EPA Regional Offices to determine if a waiver from this siting criteria is appropriate through the provisions found in Section 10 of this appendix.
Based on the EPA only receiving a single negative comment regard the 270-degree and 180-degree provisions the EPA thinks most sites already meet these proposed requirements. Additionally, as stated above, the EPA is also retaining waiver provisions from these siting requirements for the remaining cases that can be exercised when appropriate. Therefore, the EPA is finalizing the language as proposed.
g. Obstacles That Act as Obstructions
The EPA proposed to clarify the definitions of “obstructions” and “obstacles” in the regulatory text (88 FR 5677, January 27, 2023). Stating that, “[o]bstructions to the air flow of the probe inlet are those obstacles that are horizontally closer than twice the vertical distance the obstacle protrudes above the probe inlet and can be reasonably thought to scavenge reactive gases or to restrict the airflow for any pollutant,” the EPA proposed to reiterate that the EPA does not generally consider objects or obstacles such as flag poles or site towers used for NOy convertors and meteorological sensors, etc., to be deemed obstructions.
The EPA received one comment supporting the proposal and received no adverse comments. Therefore, the EPA is finalizing the definitions as proposed.
h. 10-Meter Tree Dripline Requirement
The EPA proposed to reconcile the conflicting requirements in 5(a) and the prior table E–4 footnote 3 by clarifying that the probe inlet must always be no closer than 10 meters to the tree dripline (88 FR 5677, January 27, 2023). The EPA also proposed to reinstate the goal “that monitor probe inlets should be at least 20-meters from the driplines of trees,” a goal that was inadvertently omitted during previous rule revisions. In addition, the EPA proposed to clarify that if a tree or group of trees is considered an “obstruction,” section 4(a) will apply.
As described above, the majority of comments received were supportive of the EPA proposed amendments and clarification, with two commenters focused on the possibility that monitoring agencies may not be able to meet the revised siting requirements. Specific to the proposed dripline requirement, the EPA reiterates that the Start Printed Page 16364 20-meter tree dripline offset is not a requirement, but rather a goal. Monitoring programs should as much as practicable attempt to meet this 20-meter tree dripline offset goal but are only required to be at least 10 meters removed from tree driplines. If these requirements cannot be met, the EPA encourages monitoring organizations to contact their respective EPA Regional offices to determine if a waiver from this siting criteria would be appropriate under appendix E, section 10.
Another commenter recommended that the proposal should also include an elevation specification. For instance, if a monitor is on the roof of a shelter, a tree below that roof should not be considered an obstruction no matter the distance to the dripline. The EPA considers this scenario to occur in practice only rarely. The EPA agrees that when the overall tree height is less than the height of the probe inlet, the tree is not obstructing the airflow to the probe inlet. However, a tree in such proximity to the probe inlet in many cases is not likely to remain at a height lower than the probe inlet. The EPA considers a scenario such as this to be best addressed in the waiver provisions of this appendix due both to the rarity of this occurring as well as the need for the EPA to periodically reassess whether tree growth has adversely impacted the site conditions.
For these reasons, the EPA is finalizing the language as proposed.
i. Spacing Requirement for Microscale Monitoring
The EPA proposed to require that microscale sites for any pollutant shall have no trees or shrubs blocking the line-of-sight fetch between the monitor's probe inlet and the source under investigation (88 FR 5677, January 27, 2023). This proposed revision would bring consistency between near-road monitoring stations and other microscale monitoring.
The EPA received one comment on this proposed requirement expressing concerns regarding its practicality and legality. The commenter stated agencies may at times want to site a monitor close to a source, but the closest location will have trees in the line of sight on private property. Additionally, in some cases, the trees may have been planted for the purpose of reducing off-property emissions from a source such as a Concentrated Animal Feeding Operation (CAFO). The commenter further stated that the proposal mandates that State agencies order the removal of trees from private property to collect valid data.
The EPA disagrees that the proposed requirement is impractical or unlawful. The proposed requirement would not require, mandate, or otherwise empower monitoring agencies to force the removal of trees on private property. The EPA agrees with the commenter that trees may at times be planted as part of control strategies to reduce offsite emissions and thus protect the public, but the EPA disagrees with the commenter that the trees must be removed to perform ambient air monitoring in these locations. Rather, if trees or shrubs block the line-of-sight fetch between the monitor's probe inlet and the source under investigation, it is the EPA's position that, for most cases, a microscale designation does not accurately reflect the monitoring scale for this location, and instead the EPA would recommend that the monitoring scale be designated to a more representative monitoring scale such as middle scale or neighborhood scale.
Moreover, for cases where long-term trend sites or monitors that determine the design value for an area cannot reasonably meet this regulatory siting requirement, the EPA encourages monitoring organizations to work with their respective EPA Regional offices to determine if a waiver from this siting criteria may be appropriate under appendix E, section 10.
For these reasons, the EPA is finalizing the language as proposed.
j. Waiver Provisions
The EPA proposed to maintain the appendix E, section 10 waiver provisions in the current regulation for siting criteria, but to modify section 10.3 to require that waivers from the probe-siting criteria must be reevaluated and renewed minimally every 5 years (88 FR 5677–78, January 27, 2023).
The EPA received one comment supporting the proposal and no adverse comments. Therefore, the EPA is finalizing the language as proposed.
k. Acceptable Probe Materials
The EPA proposed to expand the list of acceptable probe materials for sampling reactive gases in appendix E, section 9, from just borosilicate glass and fluorinated ethylene propylene (FEP) Teflon®, or their equivalents. The EPA proposed to add polyvinylidene fluoride (PVDF), also known as Kynar®, polytetrafluoroethylene (PTFE), and perfluoroalkoxy (PFA) to the list of approved materials for efficiently transporting gaseous criteria pollutants, and the use of NafionTM upstream of ozone analyzers (88 FR 5678, January 27, 2023). Mention of trade names or commercial products does not constitute endorsement.
The EPA received two comments supporting the proposal and received no adverse comments. Therefore, the EPA is finalizing the language as proposed.
D. Incorporating Data From Next Generation Technologies
In the proposal, the EPA requested comment on how to incorporate data from next generation technologies into Agency efforts (88 FR 5678–80, January 27, 2023). The near real-time integration of data from PM2.5 continuous monitors, sensors, and satellites has allowed the EPA to use data in certain informational applications such as EPA and USFS's Fire and Smoke Map.[199] This mapping product uses Application Program Interfaces (APIs) where data sets are automatically shared on prespecified computer servers. Given the success of the Fire and Smoke Map, the EPA indicated interest in exploring the use of next-generation technologies to develop additional approaches, products, and applications to help address important non-regulatory air quality data needs. Therefore, the EPA solicited comment on the most important data uses and data sets to consider in such future initiatives. Such approaches and/or products could utilize historical or near real-time data. The EPA sought this input and prioritization on use of next generation technologies to help improve the utility of data to better support air quality management to improve public health and the environment.
The EPA received comments from about two dozen entities on its request for comments on how to incorporate data from next generation technologies. The entities that provided comment included federal agencies; representatives of industry and industry groups; public health, medical, and environmental organizations; State, local and related multi-state organizations involved in air program management; Tribes and Tribal organizations involved in air program management; and other State and local governments.
While there were some differences across commenters, a majority of the commenters support use of next generation data for non-regulatory purposes, but not for regulatory decision making due to their inherent uncertainties and limitations. The EPA also received comments from some environmental organizations support using alternative data for regulatory decision making. Start Printed Page 16365
Many commenters pointed out that they are already successfully using sensor data and networks in supplemental and informational applications and support further expansion of these capabilities. Across many commenters, there was support for using next generation data as “fit for purpose,” filling in gaps, finding hot spots, identifying and addressing EJ concerns, and evaluating and informing network siting. The EPA acknowledges the successful examples of sensor data and networks for non-regulatory purposes. A few commenters support expanding the use of sensor data to provide real-time AQI; the EPA is interested in this use of next generation data as well. A few commenters pointed the need for the EPA to work closely with them and their communities to understand and use next generation data, while others expressed a desire for help developing best practices around collecting and using next generation data, developing products with data analysis/visualization, and developing appropriate QA/QC for sensor data. The EPA acknowledges each of these requests and expects to continue to work closely with SLTs and other stakeholders to understand and develop information on the collection and use of next generation data.
A few commenters offered more detailed comments. Some recommended that the EPA repropose implementation provisions related to next generation technologies with greater clarity to provide for meaningful comment. For example, the use of low-cost sensor and satellite data could be used in drawing nonattainment area boundaries or identifying sources for emissions control, but doing so would be such a significant change from prior EPA policy that it warrants a more specific proposal, beyond the scope of this request for comment. In response to this comment, the EPA notes it did not propose or change the use of non-regulatory measurement data as part of this proposal, but instead opened an opportunity to comment about the use of next generation technologies.
Another commenter stated that while low-cost sensor data can be invaluable for some purposes, the potentially overwhelming amount of data produced by sensors may present additional challenges to communities without the resources or expertise to analyze it. Cost is another concern associated with some next generation technologies of which some communities may not be aware, as the initial cost of the sensor alone is not indicative of the total cost of operation, which can include costs of internet access and servers. The EPA appreciates the need to consider all the costs of implementing and maintaining sensor data.
Another commenter stated that having a dense sensor network collocated with FRMs and FEMs could help ensure timely maintenance of the regulatory measurements in the event there appears to be a divergence of data. The EPA appreciates the comment that emphasizes how sensors could be used to complement the FRM and FEM data with regard to ensuring timely maintenance.
Another commentor strongly opposes incorporating sensor data into any EPA systems unless robust quality assurance (QA) practices are widely established and managed by qualified personnel. The EPA agrees that QA is necessary, and notes that the “fit for purpose” aspect of using sensor data will inform the appropriate QA associated with the intended use of such data.
In summary, the EPA invited comment on how we should consider incorporating data from next generation technologies into our air monitoring efforts. In seeking comment on this topic, the EPA did not propose to add, edit, or delete any regulatory language associated with the PM NAAQS. The EPA received comments from a variety of entities that largely support using next generation data for a variety of purposes that supplement, but cannot replace, the measurement data from monitoring methods required ( i.e., FRMs and FEMs) for regulatory decision making. Across many commenters, there was support for using next generation technologies and data as “fit for purpose,” filling in gaps, finding hot spots, identifying, and addressing EJ concerns, and evaluating and informing network siting. Quality assurance of the data will be an important component in the use of next generation technology data. The EPA will consider these comments as it continues its work with the co-regulated community comprised of SLT agencies and other stakeholders to understand and use next generation data and joint efforts to manage the nation's ambient air.
VIII. Clean Air Act Implementation Requirements for the Revised Primary Annual PM 2.5 NAAQS
The EPA's revision to the primary annual PM2.5 NAAQS discussed in section II above triggers a number of implementation related activities that were described in the NPRM. The two most immediate implementation impacts following a final new or revised NAAQS are related to stationary source permitting and the initial area designations process. Permitting implications are discussed below in section VIII.E. With regard to initial area designations, the EPA is separately issuing a memorandum regarding the Initial Area Designations for the Revised Primary Annual Fine Particle National Ambient Air Quality Standard Memorandum (the “Annual PM2.5 NAAQS Designations Memorandum”) that will provide information about the statutory schedule for the designations process. For other implementation related implications, please refer back to the NPRM section VIII.
The NPRM also referred to the PM2.5 State Implementation Plan (SIP) Requirements Rule (81 FR 58010, August 24, 2016), which specifies planning requirements for areas designated as nonattainment for purposes of the PM2.5 NAAQS and includes a number of key recommendations for areas to consider implications of environmental justice through the attainment planning process, consistent with the identification of at-risk groups in the 2019 ISA and ISA Supplement and the statutory requirement to protect the health of at-risk groups. As stated in the NPRM, State and local air agencies are encouraged to consider how they might develop implementation plans that encourage early emission reductions.
A. Designation of Areas
As discussed in section II, with respect to the PM2.5 NAAQS, the EPA is finalizing: (1) Revisions to the level of the primary annual PM2.5 NAAQS and retaining the current primary 24-hour PM2.5 NAAQS (section II.B.4); and (2) no change to the current secondary annual and 24-hour PM2.5 NAAQS at this time (section V.B.4). Upon promulgation of a new or revised NAAQS, States and the EPA must initiate the process for initial designations.
The timeline for initial area designations begins with promulgation of the revised primary annual PM2.5 NAAQS, as stated in the CAA section 107(d)(1)(B)(i). Through this process, which provides for input from States and others at various stages, the EPA identifies areas of the country that either meet or do not meet the revised primary annual PM2.5 NAAQS, along with the nearby areas contributing to NAAQS violations. The following includes additional information regarding the designations process described in the CAA.
Section 107(d)(1) of the CAA states that, “By such date as the Administrator may reasonably require, but not later than 1 year after promulgation of a new or revised national ambient air quality standard for any pollutant under section Start Printed Page 16366 109, the Governor of each State shall . . . submit to the Administrator a list of all areas (or portions thereof) in the State” and make recommendations for whether the EPA should designate those areas as nonattainment, attainment, or unclassifiable.[200] The CAA provides the EPA with discretion to require States to submit their designations recommendations within a reasonable amount of time not exceeding one additional year.[201] Section 107(d)(1)(A) of the CAA also states that “the Administrator may not require the Governor to submit the required list sooner than 120 days after promulgating a new or revised national ambient air quality standard.” Section 107(d)(1)(B)(i) further provides, “Upon promulgation or revision of a NAAQS, the Administrator shall promulgate the designations of all areas (or portions thereof) . . . as expeditiously as practicable, but in no case later than 2 years from the date of promulgation. Such period may be extended for up to one year in the event the Administrator has insufficient information to promulgate the designations.” With respect to the NAAQS setting process, courts have interpreted the term “promulgation” to be signature and widespread dissemination of a final rule.[202]
If the EPA agrees with the designations recommendation of the State, then it may proceed to promulgate the designations for such areas. If, however, the EPA disagrees with the State's recommendation, then the EPA may elect to make modifications to the recommended designations. By no later than 120 days prior to promulgating the final designations, the EPA is required to notify States of any intended modifications to the State designation recommendations for any areas or portions thereof, including the boundaries of areas, as the EPA may deem necessary. States then have an opportunity to comment on the EPA's intended modification and tentative designation decision. If a State elects not to provide designation recommendations for any area, then the EPA must itself promulgate the designation that it deems appropriate.
While section 107(d) of the CAA specifically addresses the designations process for States, the EPA intends to follow the same process for Tribes to the extent practicable, pursuant to section 301(d) of the CAA regarding Tribal authority, and the Tribal Authority Rule (63 FR 7254, February 12, 1998). To provide clarity and consistency in doing so, the EPA issued a guidance memorandum to our Regional Offices on working with Tribes during the designations process.[203]
Consistent with the process used in previous area designations efforts, the EPA will evaluate each area on a case-by-case basis considering the specific facts and circumstances unique to the area to support area boundary decisions for the revised standard. The EPA intends to issue a designations memorandum which will provide information regarding the designations process. In broad overview, the EPA has historically used area-specific analyses to support nonattainment area boundary recommendations and final boundary determinations by evaluating factors such as air quality data, emissions and emissions-related data ( e.g., population density and degree of urbanization, traffic and commuting patterns), meteorology, geography/topography, and jurisdictional boundaries. We expect to follow a similar process when establishing area designations for this revised PM2.5 NAAQS. CAA section 107(d) explicitly requires that the EPA designate as nonattainment not only the area that is violating the pertinent standard, but also those nearby areas that contribute to the violation in the violating area. In the PM2.5 NAAQS Designations Memorandum, the EPA intends to include information regarding consideration of federal land boundaries that may be fully or partially included within the bounds of a county otherwise identified as nonattainment.
As with past revisions of the PM2.5 NAAQS, the EPA intends to make the designations decisions for the revised primary annual PM2.5 NAAQS based on the most recent three years of quality-assured, certified air quality data in the EPA's Air Quality System (AQS). Accordingly, the EPA recommends that States base their initial area designation recommendations on the most current available three years of complete and certified air quality data at the time of the recommendations. The EPA will then base the final designations on the most recent three consecutive years of complete, certified air quality monitoring data available at the time of final designations.[204]
Monitoring data are currently available from numerous existing PM2.5 Federal Equivalent Methods (FEM) and Federal Reference Methods (FRM) sites to determine violations of the revised primary annual PM2.5 NAAQS. As described in section VII.C.3.b, the EPA took comment on how to deal with cases where an FEM is approved by the EPA with an update and when it can be implemented in the field. The EPA took comment on how to approach the data produced during this lag and received input from over a dozen commenters. The commenters asked that the EPA be flexible in allowing the use of updated method correction factors intended to improve the data comparability between the FRMs and FEMs. The EPA will address any data correction issues between the FRMs and FEMs through a future Notice of Data Availability (NOA).
Consistent with past practice and as noted in the NPRM, the EPA intends to provide additional information concerning the designations process, including information about the schedule and recommendations for determining area boundaries in the forthcoming Annual PM2.5 NAAQS Designations Memorandum. Other topics addressed in this memorandum include the schedule for preparing and submitting exceptional events initial notification and exceptional events demonstrations relevant to the designations process, and information related to wildfire and prescribed fire on wildlands as it pertains to initial area designations, as well as addressing back-correction of PM FEM data when a method has an approved factory calibration as part of a method update. The Annual PM2.5 NAAQS Designations Memorandum is intended to assist States and Tribes in formulating their area recommendations.[205]
As discussed in the proposal, the “Treatment of Data Influenced by Exceptional Events; Final Rule,” (81 FR 68216, October 3, 2016) and codified at 40 CFR 50.1, 40 CFR 50.14, and 40 CFR 51.930, contains instructions and requirements for air agencies that may Start Printed Page 16367 flag air quality data for certain days in the Air Quality System due to potential impacts from exceptional events ( i.e., such as prescribed fires on wildland, wildfires, or high wind dust storms). Accordingly, for purposes of initial area designations for a new or revised NAAQS, an air agency may submit to the EPA an exceptional events demonstration with supporting information and analyses for each monitoring site and day the air agency claims the EPA should exclude from design value calculations for designations purposes.
The EPA has provided tools to assist air agencies in preparing adequate exceptional events demonstrations.[206] Further, the EPA will continue to work with air agencies as they identify exceptional events that may influence decisions related to the initial area designations process, and to prepare and submit exceptional events demonstrations if appropriate. Importantly, air quality monitoring data may be influenced by emissions from prescribed fires on wildland and wildfires. The EPA's Exceptional Events Rule provides for both of these types of events to be considered as exceptional events, provided the affected air agencies submit exceptional events demonstrations that meet the procedural and technical requirements of the EPA's Exceptional Events Rule. To that end, the EPA has issued guidance addressing development of exceptional events demonstrations for both wildfire and prescribed fires on wildland.[207] In light of the growing frequency and severity of wildfire events, and expected increases in the application of prescribed fire as a means to achieve long-term reductions in high severity wildfire risk and associated smoke impacts, the EPA seeks to ensure that the Agency's exceptional events process provides an efficient and clear pathway for excluding data that may be affected by such events in a manner that is consistent with the Clean Air Act and the public health objectives of the NAAQS. Accordingly, the EPA is continuing to explore opportunities to develop additional tools that could assist air agencies in preparing exceptional events demonstrations for wildfires and prescribed fires on wildland. In addition, EPA intends to continue engaging with the U.S. Department of Agriculture, U.S. Department of the Interior, air agencies, and other stakeholders on these issues. For more information regarding the exceptional events demonstration submission deadlines for the area designations process, please see Table 2 to 40 CFR 50.14(c)(2)(vi)—“Schedule for Initial Notification and Demonstration Submission for Data Influenced by Exceptional Events for Use in Initial Area Designations.”
B. Section 110(a)(1) and (2) Infrastructure SIP Requirements
As discussed in the NPRM, the CAA directs States to address basic SIP requirements to implement, maintain, and enforce the NAAQS. Under CAA sections 110(a)(1) and (2), states are required to have State implementation plans that provide the necessary air quality management infrastructure that provides for the implementation, maintenance, and enforcement of the NAAQS. After the EPA promulgates a new or revised NAAQS, States are required to make a new SIP submission to establish that they meet the necessary structural requirements for such new or revised NAAQS or make changes to do so. The EPA refers to this type of SIP submission as an “infrastructure SIP submission.” Under CAA section 110(a)(1), all States are required to make these infrastructure SIP submissions within three years after the effective date of a new or revised primary standard. While the CAA authorizes the EPA to set a shorter time for States to make these SIP submissions, the EPA is requiring submission of infrastructure SIPs within three years of the effective date of this revised primary annual PM2.5 NAAQS.
The EPA has provided general guidance to States concerning its interpretation of these requirements of CAA section 110(a)(1) and (2) in the context of infrastructure SIP submissions for a new or revised NAAQS.[208] The EPA encourages States to use this guidance when developing their infrastructure SIPs for this revised primary annual PM2.5 NAAQS.
As a reminder, the EPA notes that States are not required to address nonattainment plan requirements for purposes of the revised primary annual PM2.5 NAAQS on the same schedule as infrastructure SIP requirements. The EPA interprets the CAA such that two elements identified in section 110(a)(2) are not subject to the 3-year submission deadline of section 110(a)(1) and thus States are not required to address them in the context of an infrastructure SIP submission. The elements pertain to part D, in title I of the CAA, which addresses additional SIP requirements for nonattainment areas. Therefore, for the reasons explained below, the following section 110(a)(2) elements are considered by the EPA to be outside the scope of infrastructure SIP actions: (1) The portion of section 110(a)(2)(C), programs for enforcement of control measures and for construction or modification of stationary sources that applies to permit programs applicable in designated nonattainment areas (known as “nonattainment new source review”) under part D; and (2) section 110(a)(2)(I), which requires a SIP submission pursuant to part D, in its entirety.
Accordingly, the EPA does not expect States to address the requirement for a new or revised NAAQS in the infrastructure SIP submissions to include regulations or emissions limits developed specifically for attaining the relevant standard in areas designated nonattainment for the revised primary annual PM2.5 NAAQS. States are required to submit infrastructure SIP submissions for the revised primary annual PM2.5 NAAQS before they will be required to submit nonattainment plan SIP submissions to demonstrate attainment with the same NAAQS. States are required to submit nonattainment plan SIP submissions to provide for attainment and maintenance of a revised primary annual PM2.5 NAAQS within 18 months from the effective date of nonattainment area designations as required under CAA section 189(a)(2)(B). The EPA reviews and acts upon these later SIP submissions through a separate process. For this reason, the EPA does not expect States to address new nonattainment area emissions controls per section 110(a)(2)(I) in their infrastructure SIP submissions.
One of the required infrastructure SIP elements is that each State SIP must contain adequate provisions to prohibit, consistent with the provisions of title I of the CAA, emissions from within the State that will significantly contribute to nonattainment in, or interfere with maintenance by, any other State of the primary or secondary NAAQS.[209] This Start Printed Page 16368 element is often referred to as the “good neighbor” or “interstate transport” provision.[210] The provision has two prongs: significant contribution to nonattainment (prong 1), and interference with maintenance (prong 2). The EPA and States must give independent significance to prong 1 and prong 2 when evaluating downwind air quality problems under CAA section 110(a)(2)(D)(i)(I).[211] Further, case law has established that the EPA and States must implement requirements to meet interstate transport obligations in alignment with the applicable statutory attainment schedule of the downwind areas impacted by upwind-state emissions.[212] Thus, the EPA anticipates that States will need to address interstate transport obligations associated with this revised PM NAAQS, in alignment with the provisions of subpart 4 of part D of the CAA, as discussed in more detail in section VIII.C below. Specifically, States must implement any measures required to address interstate transport obligations as expeditiously as practicable and no later than the next statutory attainment date, i.e., for this NAAQS revision as expeditiously as practicable, but no later than the end of the sixth calendar year following nonattainment area designations. See CAA section 188(c). States may find it efficient to make SIP submissions to address the interstate transport provisions separately from other infrastructure SIP elements.
Each State has the authority and responsibility to review its air quality management program's existing SIP provisions in light of a new or revised NAAQS to determine if any revisions are necessary to implement the new or revised NAAQS. Most States have revised and updated their SIPs in recent years to address requirements associated with other revised NAAQS. For certain infrastructure elements, some States may believe they already have adequate State regulations adopted and approved into the SIP to address a particular requirement with respect to the revised primary annual PM2.5 NAAQS.
If a State determines that existing SIP-approved provisions are adequate in light of this revised primary annual PM2.5 NAAQS with respect to a given infrastructure SIP element (or sub-element), then the State may make an infrastructure SIP submission “certifying” that the existing State's existing EPA approved SIP already contains provisions that address one or more specific section 110(a)(2) infrastructure elements.[213] In the case of such a submission, the State does not have to include a copy of the relevant provision ( e.g., rule or statute) itself. Rather, this certification submission should provide citations to the SIP-approved State statutes, regulations, or non-regulatory measures, as appropriate, in or referenced by the already EPA-approved SIP that meet particular infrastructure SIP element requirements. The State's infrastructure SIP submission should also include an explanation as to how the State has determined that those existing provisions meet the relevant requirements.
Like any other SIP submission, that State can make such an infrastructure SIP submission certifying that it has already met some or all of the applicable requirements only after it has provided reasonable notice and opportunity for public hearing. This “reasonable notice and opportunity for public hearing” requirement for infrastructure SIP submissions is to meet the requirements of CAA sections 110(a) and 110(l). Under the EPA's regulations at 40 CFR part 51, if a public hearing is held, an infrastructure SIP submission must include a certification by the State that the public hearing was held in accordance with the EPA's procedural requirements for public hearings. See 40 CFR part 51, appendix V, section 2.1(g), and see 40 CFR 51.102.
In consultation with the EPA's Regional office, a State should follow all applicable EPA regulations governing infrastructure SIP submissions in 40 CFR part 51— e.g., subpart I (Review of New Sources and Modifications), subpart J (Ambient Air Quality Surveillance), subpart K (Source Surveillance), subpart L (Legal Authority), subpart M (Intergovernmental Consultation), subpart O (Miscellaneous Plan Content Requirements), subpart P (Protection of Visibility), and subpart Q (Reports). For the EPA's general criteria for infrastructure SIP submissions, refer to 40 CFR part 51, appendix V, Criteria for Determining the Completeness of Plan Submissions. For additional information on infrastructure SIP submission requirements, refer to the EPA's 2013 guidance entitled “Guidance on Infrastructure State Implementation Plan (SIP) Elements under Clean Air Act Sections 110(a)(1) and 110(a)(2).” The EPA recommends that States electronically submit their infrastructure SIPs to the EPA through the State Plan Electronic Collaboration System (SPeCS),[214] an online system available through the EPA's Central Data Exchange.
C. Implementing Revised Primary Annual PM2.5 NAAQS in Nonattainment Areas
As discussed in the NPRM, the EPA issued a SIP Requirements Rule for implementing the PM2.5 NAAQS (81 FR 58010, August 24, 2016) (PM2.5 SIP Requirements Rule). It provides guidance and establishes additional regulatory requirements for States regarding development of attainment plans for nonattainment areas for the 1997, 2006, and 2012 revisions of the PM2.5 NAAQS. The guidance and regulations in the SIP Requirements Rule also apply to any States for which the EPA promulgates nonattainment area designations for the new revised primary annual PM2.5 NAAQS.
The PM2.5 SIP Requirements Rule provides comprehensive information regarding nonattainment plan requirements including, among other things: nonattainment area emissions inventories; policies regarding PM2.5 precursor pollutants ( i.e., SO2, NOX, VOC, and ammonia); control strategies (such as reasonably available control measures and reasonably available control technology for direct PM2.5 and relevant precursors); air quality modeling; attainment demonstrations; reasonable further progress requirements; quantitative milestones; and contingency measures. Information provided in the PM2.5 SIP Requirements Rule is supplemented by other EPA documents, including guidance on emissions inventory development (80 FR 8787, February 19, 2015; U.S. EPA, 2017), optional PM2.5 precursor demonstrations (U.S. EPA, 2019b),[215] and guidance on air quality modeling for meeting air quality goals for the ozone and PM2.5 NAAQS and regional haze program (U.S. EPA, 2018b).
As stated in the NPRM, the PM2.5 SIP Requirements Rule provides recommendations to States regarding consideration of environmental justice in the context of PM2.5 attainment Start Printed Page 16369 planning. Some of the considerations for States include: (1) Identifying areas with overburdened communities where more ambient monitoring may be warranted; (2) targeting emissions reductions that may be needed to attain the PM2.5 NAAQS; and (3) increasing opportunities for meaningful involvement for overburdened populations ( see88 FR 5558, 5684, January 27, 2023; 80 FR 58010, 58136, August 25, 2016). In light of the identification of at-risk populations for this reconsideration, the EPA encourages States to consider these and other factors as part of their attainment plan SIP development process.
The PM2.5 SIP Requirements Rule outlines some examples of how States can elect to implement these recommendations.[216] For instance, States can use modeling and screening tools to better understand where sources of PM2.5 or PM2.5 precursor emissions are located and identify areas that may be candidates for additional ambient monitoring. Furthermore, once these target areas are identified, States can prioritize direct PM2.5 or PM2.5 precursor control measures and enforcement strategies in these areas to reduce ambient PM2.5 and achieve the NAAQS. As articulated in the NPRM and the PM2.5 SIP Requirements Rule, the EPA recognizes that States have flexibility under the CAA to concentrate State resources on controlling sources of PM2.5 emissions in light of environmental justice considerations ( see88 FR 5558, 5684, January 27, 2023; 81 FR 58010, 58137, August 24, 2016). Moreover, States can establish opportunities to bolster meaningful involvement in a number of ways, such as communicating in appropriate languages, ensuring access to draft SIPs and other information, and developing enhanced notice-and-comment opportunities, as appropriate ( see88 FR 5558, 5684, January 27, 2023; 80 FR 58010, 58136, August 25, 2016).
As previously mentioned, the PM2.5 SIP Requirements Rule provides guidance and regulatory requirements for remaining nonattainment areas for the 1997, 2006, and 2012 revisions of the PM2.5 NAAQS, as well as for nonattainment areas designated pursuant to any future revisions of the PM2.5 NAAQS, including the revised annual PM2.5 NAAQS being finalized in this action. The EPA is not making any changes to the current PM2.5 SIP Requirements Rule.
D. Implementing the Primary and Secondary PM10 NAAQS
As summarized in sections III.B.4 and V.B.4 above, the EPA is retaining the current primary and secondary 24-hour PM10 NAAQS to protect against the health effects associated with short-term exposures to thoracic coarse particles and against the welfare effects considered in this reconsideration ( i.e., visibility, climate, and materials effects). The EPA is retaining the existing implementation strategy for meeting the CAA requirements for the PM10 NAAQS. States and emissions sources should continue to follow the existing regulations and guidance for implementing the current standards.[217]
E. Prevention of Significant Deterioration and Nonattainment New Source Review Programs for the Revised Primary Annual PM2.5 NAAQS
The CAA, at parts C and D of title I, contains preconstruction review and permitting programs applicable to new major stationary sources and major modifications of existing major sources. The preconstruction review of each new major stationary source and major modification applies on a pollutant-specific basis, and the requirements that apply for each pollutant depend on whether the area in which the source is situated is designated as attainment (or unclassifiable) or nonattainment for that pollutant. In areas designated attainment or unclassifiable for a pollutant, the Prevention of Significant Deterioration (PSD) requirements under part C apply to construction at major sources. In areas designated nonattainment for a pollutant, the Nonattainment New Source Review (NNSR) requirements under part D apply to construction at major sources. Collectively, those two sets of permit requirements are commonly referred to as the “major New Source Review” or “major NSR” programs.
Until the EPA designates an area with respect to the revised primary annual PM2.5 NAAQS, the NSR provisions applicable under an area's current designation for the 1997, 2006, and 2012 PM2.5 NAAQS would continue to apply. See40 CFR 51.166(i)(2) and 52.21(i)(2). That is, for areas designated as attainment/unclassifiable for the 1997, 2006, and 2012 PM2.5 NAAQS, PSD will apply to new major stationary sources and major modifications that trigger major source permitting requirements for PM2.5. For areas designated nonattainment for the 1997, 2006, or 2012 PM2.5 NAAQS, NNSR requirements will apply for new major stationary sources and major modifications that trigger major source permitting requirements for PM2.5 . When the initial area designations for this revised primary annual PM2.5 NAAQS become effective, those designations will further determine whether PSD or NNSR applies to PM2.5 in a particular area, depending on the designation status. New major sources and major modifications will be subject to the PSD program requirements for PM2.5 if they are located in an area that does not have a current nonattainment designation under CAA section 107 for PM2.5 .[218]
Under the PSD program, the permit applicant must demonstrate that the new or modified source emissions increase does not cause or contribute to a NAAQS violation. In 2017, the EPA revised the Guideline on Air Quality Models (published as appendix W to 40 CFR part 51) to address primary and secondary PM2.5 impacts in making this demonstration. The EPA has since provided associated technical guidance, models and tools, such as the recent “Final Guidance for Ozone and Fine Particulate Matter Permit Modeling” (July 29, 2022).[219] Additionally, in light of this NAAQS revision, the EPA is updating its guidance that provides recommended significant impact levels (SILs) for PM2.5 and expects that an updated SIL for the revised primary annual PM2.5 NAAQS will be available Start Printed Page 16370 on or before the effective date of the final NAAQS.
The statutory requirements for a PSD permit program set forth under part C of title I of the CAA (sections 160 through 169) are addressed by the EPA's PSD regulations found at 40 CFR 51.166 (minimum requirements for an approvable PSD SIP) and 40 CFR 52.21 (PSD permitting program for permits issued under the EPA's Federal permitting authority). These regulations already apply to PM2.5 in areas that are designated attainment or unclassifiable for PM2.5 whenever a proposed new major source or major modification triggers PSD requirements for PM2.5.
For PSD, a “major stationary source” is one with the potential to emit 250 tons per year (tpy) or more of any regulated NSR pollutant, unless the new or modified source is classified under a list of 28 source categories contained in the statutory definition of “major emitting facility” in section 169(1) of the CAA. For those 28 source categories, a “major stationary source” is one with the potential to emit 100 tpy or more of any regulated NSR pollutant. A “major modification” is a physical change or a change in the method of operation of an existing major stationary source that results, first, in a significant emissions increase of a regulated NSR pollutant and, second, in a significant net emissions increase of that pollutant. See 40 CFR 51.166(b)(2)(i), 40 CFR 52.21(b)(2)(i). The EPA PSD regulations define the term “regulated NSR pollutant” to include any pollutant for which a NAAQS has been promulgated and any pollutant identified by the EPA as a constituent or precursor to such pollutant. See 40 CFR 51.166(b)(49), 40 CFR 52.21(b)(50). These regulations identify SO2 and NOX as precursors to PM2.5 in attainment and unclassifiable areas. See 40 CFR 51.166(b)(49)(i)(b), 40 CFR 52.21(b)(50)(i)(b).[220] Thus, for PM2.5, the PSD program currently requires the review and control of emissions of direct PM2.5 emissions and SO2 and NOX (as precursors to PM2.5), absent a demonstration otherwise for NOX . Among other things, for each regulated NSR pollutant emitted or increased in a significant amount, the PSD program requires a new major stationary source or a major modification to apply the “best available control technology” (BACT) to limit emissions and to conduct an air quality impact analysis to demonstrate that the proposed major stationary source or major modification will not cause or contribute to a violation of any NAAQS or PSD increment.[221] See CAA section 165(a)(3) and (4), 40 CFR 51.166(j) and (k), 40 CFR 52.21(j) and (k). The PSD requirements may also include, in appropriate cases, an analysis of potential adverse impacts on Class I areas. See CAA sections 162(a) and 165(d), 40 CFR 51.166(p); 40 CFR 52.21(p)).[222] The EPA developed the Guideline on Air Quality Models and other documents to, among other things, provide methods and guidance for demonstrating that increased emissions from construction will not cause or contribute to exceedances of the PM2.5 NAAQS and PSD increments for PM2.5 .[223]
Upon the effective date of the revised primary annual PM2.5 NAAQS, the demonstration required under CAA Section 165(a)(3), and the associated regulations, must include the revised primary annual PM2.5 NAAQS. In past NAAQS revision rules, including the 2012 PM2.5 NAAQS (78 FR 3086, January 15, 2013) and 2015 Ozone NAAQS (80 FR 65292, October 26, 2015), the EPA included limited provision that exempted certain sources with pending PSD permit applications (those that had reached a particular stage in the permitting process at the time the revised NAAQS was promulgated or became effective) from the requirement to demonstrate that the proposed emissions increases would not cause or contribute to a violation of the revised NAAQS.[224] In August 2019, the U.S. Court of Appeals for the D.C. Circuit vacated the exemption provision in the PSD rules for the 2015 Ozone NAAQS, finding that the provision contradicted “Congress's `express policy choice' not to allow construction which will `cause or contribute to' nonattainment of `any' effective NAAQS, regardless of when they are adopted or when a permit was completed.” Murray Energy Corp. v. EPA, 936 F.3d 597, 627 (D.C. Cir. 2019).[225] Based on that court decision, the EPA is not establishing any PSD permitting exemption provision in this action. Some commenters requested that the EPA provide the same kind of relief for pending PSD permit applications by extending the effective date of this new revised NAAQS beyond the 60 days that the EPA has traditionally used for such rules. Such comments are addressed in the Response to Comments portion of this action. The EPA is making this revised primary annual PM2.5 NAAQS effective in 60 days.
The EPA anticipates that the existing PM2.5 air quality in some areas will not be in attainment with the revised primary annual PM2.5 NAAQS, and the EPA will designate these areas as nonattainment at a later date, consistent with the designation process described in the preceding sections. However, until such nonattainment designation occurs, proposed new major sources and major modifications located in any area currently designated attainment or unclassifiable for all preexisting PM2.5 NAAQS will continue to be subject to the PSD program requirements for PM2.5 . Any proposed major stationary source or major modification triggering PSD requirements for PM2.5 that does not receive its PSD permit by the effective date of a new nonattainment designation for the area where the source would locate would then be required to satisfy applicable NNSR preconstruction permit requirements for PM2.5.
In areas where air pollution exceeds the level of the revised primary annual PM2.5 NAAQS, a PSD permit applicant must demonstrate that the source or modification will not cause or Start Printed Page 16371 contribute to a violation of the NAAQS. Section 165(a)(3)(B) of the CAA states that a proposed source may not construct unless it demonstrates that it will not cause or contribute to a violation of any NAAQS. This statutory requirement is implemented through a provision contained in the PSD regulations at 40 CFR 51.166(k) and 52.21(k).[226] If a source cannot make this demonstration, or if its initial air quality impact analysis shows that the source's impact would cause or contribute to a violation, the reviewing authority may not issue a PSD permit to that source. However, a PSD permit applicant may be able to make this demonstration if it compensates for the adverse impact that would otherwise cause or contribute to a violation of the NAAQS. In contrast to the NSR requirements for nonattainment areas, the PSD regulations do not explicitly specify remedial actions that a prospective source must take to address such a situation, but the EPA has historically recognized that sources applying for PSD permits may utilize offsetting reductions in emissions as part of the required PSD demonstration under CAA section 165(a)(3)(B).[227]
Part D of title I of the CAA includes preconstruction review and permitting requirements applicable to new major stationary sources and major modifications located in areas designated nonattainment for a pollutant for which the EPA has established a NAAQS ( i.e., a criteria pollutant). The relevant part D requirements are typically referred to as the nonattainment NSR (NNSR) program. The EPA's regulations for the NNSR program are contained in 40 CFR 51.165 and 52.24 and part 51, appendix S. Specifically, the EPA has developed minimum program requirements for a NNSR program that is approvable in a SIP, and those requirements, which include requirements for PM2.5, are contained in 40 CFR 51.165. In addition, 40 CFR part 51, appendix S, contains requirements constituting an interim NNSR program. This interim program enables NNSR permitting in nonattainment areas by States that lack a SIP-approved NNSR permitting program during the time between the date of the relevant designation and the date that the EPA approves into the SIP a NNSR program. See40 CFR part 51, appendix S, section I; 40 CFR 52.24(k).
For NNSR, “major stationary source” is generally defined as a source with the potential to emit at least 100 tpy of the regulated NSR pollutant for which the area is designated nonattainment. In some cases, however, the CAA and the NNSR regulations define “major stationary source” for NNSR in terms of a lower rate dependent on the pollutant and degree of nonattainment in the area. For purposes of the PM2.5 NAAQS, in addition to the general threshold level of 100 tpy in Moderate PM2.5 nonattainment areas, a lower major source threshold of 70 tpy applies in Serious PM2.5 nonattainment areas pursuant to subpart 4 of part D, title I of the CAA. See40 CFR 51.165(a)(1)(iv)(A)( 1)( vii) and ( viii); 40 CFR part 51, appendix S, II.A.4(i)(a)(7) and (8).
Under the NNSR program, direct PM2.5 emissions and emissions of each PM2.5 precursor are considered separately in accordance with the applicable major source threshold. For example, the threshold for Serious PM2.5 nonattainment areas is 70 tpy of direct PM2.5, as well as for the PM2.5 precursors SO2, NOX , VOC, and ammonia.[228] See 40 CFR 51.165(a)(1)(iv)(A)( 1)( vii) and ( viii); 40 CFR part 51, appendix S, II.A.4.(i)(a)(7) and (8). A source qualifies as major for nonattainment NSR in a PM2.5 nonattainment area if it emits or has the potential to emit direct PM2.5 or any PM2.5 precursor in an amount equal to or greater than the applicable threshold.
For modifications, NNSR applies to proposed physical changes or changes in the method of operation of an existing stationary source where (1) the source is major for the nonattainment pollutant (or a precursor for that pollutant) and (2) the physical change or change in the method of operation of a major stationary source results, first, in a significant emissions increase of a regulated NSR pollutant and, second, in a significant net emissions increase of that same nonattainment pollutant (or same precursor for that pollutant). See40 CFR 51.165(a)(1)(v)(A); 40 CFR part 51, appendix S, II.A.5.(i). For example, to qualify as a major modification for SO2 (as a PM2.5 precursor) in a Moderate PM2.5 nonattainment area, the existing source would have to have the potential to emit 100 tpy or more of SO2, and the project would have to result in an increase in SO2 emissions of 40 tpy or more. See 40 CFR 51.165(a)(1)(x)(A).
New major stationary sources and major modifications for PM2.5 subject to NNSR must comply with the “lowest achievable emission rate” (LAER), as defined in the CAA and NNSR rules. Such sources must also perform other analyses and obtain emission offsets, as required under section 173 of the CAA and applicable regulations.
Following the promulgation of this revised primary annual PM2.5 NAAQS, some new areas may be designated nonattainment for PM2.5 . Where a State does not have an existing NNSR program or where the current NNSR program does not apply to PM2.5, that State will be required to submit the necessary SIP revisions to ensure that new major stationary sources and major modifications for PM2.5 or a PM2.5 precursor undergo preconstruction review pursuant to the NNSR program. States with designated nonattainment areas for the revised primary annual PM2.5 NAAQS are required to make SIP submissions to meet nonattainment plan requirements within 18 months from the effective date of designations, as required under CAA section 189(a)(2)(B). States that have existing NNSR program requirements that cannot be interpreted to apply at the time of designation to the revised primary annual PM2.5 NAAQS may, in the interim, issue permits in accordance with the applicable nonattainment permitting requirements contained in 40 CFR part 51, appendix S, which would apply to the revised primary annual PM2.5 NAAQS upon its effective date. See73 FR 28321, 28340, May 16, 2008.
Finally, the EPA has released several documents that discuss air permitting Start Printed Page 16372 and environmental justice, including, for example, a memorandum [229] and attached permitting principles.[230] The EPA recommends that PSD and NNSR permitting authorities review this memorandum and the principles and consider applying them in their air permitting actions as appropriate to help identify, analyze, and address environmental justice concerns in those air permitting actions to help ensure that the NAAQS achieve their intended health benefits for at-risk populations.
F. Transportation Conformity Program
Transportation conformity is required under CAA section 176(c) to ensure that transportation plans, transportation improvement programs (TIPs) and federally supported highway and transit projects will not cause or contribute to any new air quality violation, increase the frequency or severity of any existing violation, or delay timely attainment or any required interim emissions reductions or other milestones. Transportation conformity applies to areas that are designated as nonattainment or nonattainment areas that have been redesignated to attainment with an approved CAA section 175A maintenance plan ( i.e., maintenance areas) for transportation-related criteria pollutants: carbon monoxide, ozone, NO2, PM2.5, and PM10 . Transportation conformity for the revised primary annual PM2.5 NAAQS does not apply until one year after the effective date of nonattainment designations for that NAAQS. See CAA section 176(c)(6) and 40 CFR 93.102(d)). The EPA's Transportation Conformity Rule [231] establishes the criteria and procedures for determining whether transportation activities conform to the SIP. No changes are being made to the transportation conformity rule in this final rulemaking. The EPA notes that the transportation conformity rule already addresses the PM2.5 and PM10 NAAQS. However, in the future, the EPA intends to review the need to issue or revise guidance describing how the current conformity rule applies in nonattainment and maintenance areas for the revised primary annual PM2.5 NAAQS, as needed.
G. General Conformity Program
The conformity requirement under CAA section 176(c) ensures that federal activities implemented by federal agencies will not interfere with a State's ability to attain and maintain the NAAQS. Under CAA 176(c)(1), the requirement prohibits Federal agencies from approving, permitting, licensing, or funding activities that do not conform to the purpose of the applicable SIP for the control and prevention of air pollution. See CAA 176(c)(1)(A). Under CAA 176(c)(1)(B), conformity to an implementation plan means that federal activities will not cause or contribute to any new violations of the NAAQS, increase the frequency or severity of any existing NAAQS violation, or delay timely attainment or any required interim emissions reductions or other milestones contained in the applicable SIP.
The general conformity program [232] implements CAA section 176(c)(4)(A), and the criteria and procedures for determining conformity of federal activities to the applicable SIP are established under 40 CFR part 93 subpart B, sections 93.150 through 93.165. General Conformity applies to federal activities that (1) would cause emissions of relevant criteria or precursor pollutants to originate within nonattainment areas or areas that have been redesignated to attainment with an approved CAA section 175A maintenance plan ( i.e., maintenance areas), as set forth under 40 CFR 93.153, and (2) are not Federal Highway Administration (FHWA) or Federal Transit Administration (FTA) transportation projects as defined in 40 CFR 93.101 under the transportation conformity requirements. See40 CFR 93.153. General conformity for the revised primary annual PM2.5 NAAQS does not apply until one year after the effective date of the nonattainment designation for that NAAQS. See40 CFR 93.153(k).
With regard to issues regarding prescribed fires, which were addressed earlier in this action, here is some additional information regarding prescribed fires and General Conformity regulations. Under the General Conformity regulations at 40 CFR 93.153(c)(4), a conformity evaluation is not required to support a decision by a federal agency to conduct or carry out prescribed burning when the burn is consistent with the terms of a land management plan or other plan that includes the prescribed burn at issue, where the overall plan that includes the burn was previously evaluated under 40 CFR part 93 subpart B by the responsible federal agency, and the agency found the plan conforms under CAA paragraphs 176(c)(1)(A) and (1)(B). This assumes the burn at issue will be conducted by meeting any conditions specified as necessary for meeting conformity in the agency's decision to approve the plan. Alternatively, a presumption of conformity applies also under 40 CFR 93.153(i)(2) for prescribed fires conducted in accordance with a Smoke Management Program that meets the requirements of the EPA's 1998 Interim Air Quality Policy on Wildland and Prescribed Fires or an equivalent replacement EPA policy. The preamble to the Exceptional Events Rule explains that the EPA adapted language associated with the six basic components of a certifiable Smoke Management Program for exceptional events purposes from the 1998 Interim Air Quality Policy on Wildland and Prescribed Fires ( see, e.g.,81 FR 68216, 68252 (including footnote 75), 68256, October 2, 2016). The Exceptional Events Rule at 40 CFR 50.14(a)(3)(ii)(A) also indicates that certain requirements within the Exceptional Events Rule can be satisfied if a prescribed fire is conducted under a certified Smoke Management Program or using appropriate basic smoke management practices such as those identified in Table 1 to 40 CFR 50.14 ( see e.g.,81 FR 68216, 68250–68257, 68277–68278, October 3, 2016).
No changes are being made to the general conformity regulations in this final rulemaking and the EPA notes that the courts recognize the regulations constitute control for the established PM2.5 and PM10 NAAQS. However, in the future, the EPA intends to review the need to issue or revise guidance describing how the current General Conformity regulations apply within nonattainment and maintenance areas for the revised primary annual PM2.5 NAAQS, as needed.[233]
IX. Statutory and Executive Order Reviews
Additional information about these statutes and Executive orders can be Start Printed Page 16373 found at https://www.epa.gov/laws-regulations/laws-and-executive-orders.
A. Executive Order 12866: Regulatory Planning and Review and Executive Order 14094: Modernizing Regulatory Review
This action is “significant regulatory action” as defined under section 3(f)(1) of Executive Order 12866, as amended by Executive Order 14094. Accordingly, the EPA submitted this action to the Office of Management and Budget (OMB) for review. Documentation of any changes made in response to the Executive Order 12866 review is available in the docket. The EPA prepared an illustrative analysis of the potential costs and benefits associated with this action. This analysis, “Regulatory Impact Analysis for the Reconsideration of the National Ambient Air Quality Standards for Particulate Matter,” is available in the Regulatory Impact Analysis (RIA) docket (EPA–HQ–OAR–2019–0587) and briefly summarized below. However, the CAA and judicial decisions make clear that the economic and technical feasibility of attaining ambient standards are not to be considered in setting or revising NAAQS, although such factors may be considered in the development of State plans to implement the standards. Accordingly, although an RIA has been prepared, the results of the RIA have not been considered in issuing this final rule.
The RIA estimates the costs and monetized human health benefits in 2032, after implementing existing and expected regulations and assessing emissions reductions to meet the current primary annual and 24-hour particulate matter NAAQS (12/35 μg/m3 ), associated with applying national control strategies for the revised annual and 24-hour standard levels of 9/35 μg/m3 , as well as the following less and more stringent alternative standard levels: (1) A less stringent alternative annual standard level of 10 μg/m3 in combination with the current 24-hour standard ( i.e., 10/35 μg/m3 ), (2) a more stringent alternative annual standard level of 8 μg/m3 in combination with the current 24-hour standard ( i.e., 8/35 μg/m3 ), and (3) a more stringent alternative 24-hour standard level of 30 μg/m3 in combination with an annual standard level of 10 μg/m3 ( i.e., 10/30 μg/m3 ). Table 3 provides a summary of the estimated monetized benefits, costs, and net benefits associated with applying national control strategies toward reaching the revised and alternative standard levels.
Table 3—Estimated Monetized Benefits, Costs, and Net Benefits of the Illustrative Control Strategies Applied Toward the Primary Revised and Alternative Annual and Daily Standard Levels of 10/35 μ g/m3 , 10/30 μ g/m3 , 9/35 μ g/m3 , and 8/35 μ g/m3 in 2032 for the U.S.
[Millions of 2017$]
10/35 10/30 9/35 8/35 Benefits a $8,500 and $17,000 $10,000 and $21,000 $22,000 and $46,000 $48,000 and $99,000. Costs b $200 $340 $590 $1,500. Net Benefits $8,300 and $17,000 $9,900 and $21,000 $22,000 and $46,000 $46,000 and $97,000. Notes: Rows may not appear to add correctly due to rounding. We provide a snapshot of costs and benefits in 2032, using the best available information to approximate social costs and social benefits recognizing uncertainties and limitations in those estimates. The estimated costs and monetized human health benefits associated with applying national control strategies do not fully account for all the emissions reductions needed to reach the final and more stringent alternative standard levels for some standard levels analyzed. a We assume that there is a cessation lag between the change in PM exposures and the total realization of changes in mortality effects. Specifically, we assume that some of the incidences of premature mortality related to PM 2.5 exposures occur in a distributed fashion over the 20 years following exposure, which affects the valuation of mortality benefits at different discount rates. Similarly, we assume there is a cessation lag between the change in PM exposures and both the development and diagnosis of lung cancer. The benefits are associated with two point estimates from two different epidemiologic studies, and we present the benefits calculated at a real discount rate of 3 percent. The monetized benefits exclude additional health and welfare benefits that could not be quantified. b The costs are annualized using a 7 percent interest rate. B. Paperwork Reduction Act (PRA)
This action does not impose any new information collection burden under the PRA. OMB has previously approved the information collection activities contained in the existing regulations and has assigned OMB control number 2060–0084. The data collected through this information collection consist of ambient air concentration measurements for the seven air pollutants with national ambient air quality standards ( i.e., ozone, sulfur dioxide, nitrogen dioxide, lead, carbon monoxide, PM2.5 and PM10), ozone precursors, air toxics, meteorological variables at a select number of sites, and other supporting measurements. Accompanying the pollutant concentration data are quality assurance/quality control data and air monitoring network design information. The EPA and others ( e.g., State and local air quality management agencies, tribal entities, environmental organizations, academic institutions, industrial groups) use the ambient air quality data for many purposes including informing the public and other interested parties of an area's air quality, judging an area's air quality in comparison with the established health or welfare standards, evaluating an air quality management agency's progress in achieving or maintaining air pollutant levels below the national and local standards, developing and revising State Implementation Plans (SIPs), evaluating air pollutant control strategies, developing or revising national control policies, providing data for air quality model development and validation, supporting enforcement actions, documenting episodes and initiating episode controls, assessing air quality trends, and conducting air pollution research.
C. Regulatory Flexibility Act (RFA)
I certify that this action will not have a significant economic impact on a substantial number of small entities under the RFA. This action will not impose any requirements on small entities. Rather, this final rule establishes national standards for allowable concentrations of PM in ambient air as required by section 109 of the CAA. See also American Trucking Associations v. EPA, 175 F.3d 1027, 1044–45 (D.C. Cir. 1999) (NAAQS do not have significant impacts upon small entities because NAAQS themselves impose no regulations upon small entities), rev'd in part on other grounds, Whitman v. American Trucking Associations, 531 U.S. 457 (2001). Start Printed Page 16374
D. Unfunded Mandates Reform Act (UMRA)
This action does not contain an unfunded mandate of $100 million or more as described in the Unfunded Mandates Reform Act (UMRA), 2 U.S.C. 1531–1538, and does not significantly or uniquely affect small governments. Furthermore, as indicated previously, in setting a NAAQS the EPA cannot consider the economic or technological feasibility of attaining ambient air quality standards, although such factors may be considered to a degree in the development of State plans to implement the standards. See also American Trucking Associations v. EPA, 175 F. 3d at 1043 (noting that because the EPA is precluded from considering costs of implementation in establishing NAAQS, preparation of the RIA pursuant to the Unfunded Mandates Reform Act would not furnish any information that the court could consider in reviewing the NAAQS).
E. Executive Order 13132: Federalism
This action will not have substantial direct effects on the States, on the relationship between the National Government and the States, or on the distribution of power and responsibilities among the various levels of government. However, the EPA recognizes that States will have a substantial interest in this action and any future revisions to associated requirements.
F. Executive Order 13175: Consultation and Coordination With Indian Tribal Governments
This action does not have Tribal implications, as specified in Executive Order 13175. It does not have a substantial direct effect on one or more Indian Tribes as Tribes are not obligated to adopt or implement any NAAQS. In addition, Tribes are not obligated to conduct ambient monitoring for PM or to adopt the ambient monitoring requirements of 40 CFR part 58. Thus, Executive Order 13175 does not apply to this action. However, consistent with the EPA Policy on Consultation and Coordination with Indian Tribes, the EPA offered consultation to all 574 Federally Recognized Tribes during the development of this action. Although no Tribes requested consultation, the EPA provided informational meetings including an informational meeting with the Pueblo de San Ildefonso and provided information on the monthly National Tribal Air Association calls.
G. Executive Order 13045: Protection of Children From Environmental Health Risks and Safety Risks
Executive Order 13045 directs federal agencies to include an evaluation of the health and safety effects of the planned regulation on children in federal health and safety standards and explain why the regulation is preferable to potentially effective and reasonably feasible alternatives. This action is subject to Executive Order 13045 because it is a significant regulatory action under section 3(f)(1) of Executive Order 12866, and the EPA believes that the environmental health or safety risk addressed by this action may have a disproportionate effect on children. Accordingly, we have evaluated the environmental health or safety effects of PM exposures on children. The protection offered by these standards may be especially important for children because childhood represents a lifestage associated with increased susceptibility to PM-related health effects. Because children have been identified as a susceptible population, we have carefully evaluated the environmental health effects of exposure to PM pollution among children. Children make up a substantial fraction of the U.S. population, and often have unique factors that contribute to their increased risk of experiencing a health effect due to exposures to ambient air pollutants because of their continuous growth and development. As described in the 2019 Integrated Science Assessment, children may be particularly at risk for health effects related to ambient air PM2.5 exposures compared with adults because they have (1) a developing respiratory system, (2) increased ventilation rates relative to body mass compared with adults, and (3) an increased proportion of oral breathing, particularly in boys, relative to adults. More detailed information on the evaluation of the scientific evidence and policy considerations pertaining to children, including an explanation for why the Administrator judges the revised standards to be requisite to protect public health, including the health of children, with an adequate margin of safety, are contained in section II.A.2. “Overview of the Health Effects Evidence”, section II.A.2.b “Public Health Implications and At-Risk Populations” and II.B “Conclusions on the Primary PM2.5 Standards” of this preamble. Copies of all documents have been placed in the public docket for this action. The Administrator judges that revising the primary annual PM2.5 standard to a level of 9.0 µg/m3 and retaining the primary 24-hour PM2.5 standard provides requisite public health protection with an adequate margin of safety, including for children. Furthermore, the Policy on Children's Health also applies to this action. Information on how the Policy was applied is described in section II.A.2 “Overview of the Health Effects Evidence”, section II.A.2.b “Public Health Implications and At-Risk Populations” and II.B “Conclusions on the Primary PM2.5 Standards” of this preamble.
H. Executive Order 13211: Actions Concerning Regulations That Significantly Affect Energy Supply, Distribution or Use
This action is not a “significant energy action” because it is not likely to have a significant adverse effect on the supply, distribution, or use of energy. The purpose of this action is to revise level of the primary annual PM2.5 NAAQS. The action does not prescribe specific pollution control strategies by which these ambient standards and monitoring revisions will be met. Such strategies will be developed by States on a case-by-case basis, and the EPA cannot predict whether the control options selected by States will include regulations on energy suppliers, distributors, or users. Thus, the EPA concludes that this action does not constitute a significant energy action as defined in Executive Order 13211.
I. National Technology Transfer and Advancement Act (NTTAA)
This rulemaking involved environmental monitoring or measurement. The EPA has decided it will continue to use the existing indicators for fine (PM2.5) and coarse (PM10) particles. The indicator for fine particles is measured using the Reference Method for the Determination of Fine Particulate Matter as PM2.5 in the Atmosphere (appendix L to 40 CFR part 50), which is known as the PM2.5 FRM, and the indicator for coarse particles is measured using the Reference Method for the Determination of Particulate Matter as PM10 in the Atmosphere (appendix J to 40 CFR part 50), which is known as the PM10 FRM.
To the extent feasible, the EPA employs a Performance-Based Measurement System (PBMS), which does not require the use of specific, prescribed analytic methods. The PBMS is defined as a set of processes wherein the data quality needs, mandates or limitations of a program or project are specified and serve as criteria for selecting appropriate methods to meet those needs in a cost-effective manner. Start Printed Page 16375 It is intended to be more flexible and cost effective for the regulated community; it is also intended to encourage innovation in analytical technology and improved data quality. Though the FRM defines the particular specifications for ambient monitors, there is some variability with regard to how monitors measure PM, depending on the type and size of PM and environmental conditions. Therefore, it is not practically possible to fully define the FRM in performance terms to account for this variability. Nevertheless, our approach in the past has resulted in multiple brands of monitors being approved as FRM for PM, and we expect this to continue. Also, the FRMs described in 40 CFR part 50 and the equivalency criteria described in 40 CFR part 53, constitute a performance-based measurement system for PM, since methods that meet the field testing and performance criteria can be approved as FEMs. Since finalized in 2006 (71 FR 61236, October 17, 2006) the new field and performance criteria for approval of PM2.5 continuous FEMs has resulted in the approval of 13 approved FEMs. In summary, for measurement of PM2.5 and PM10, the EPA relies on both FRMs and FEMs, with FEMs relying on a PBMS approach for their approval. The EPA is not precluding the use of any other method, whether it constitutes a voluntary consensus standard or not, as long as it meets the specified performance criteria.
J. Executive Order 12898: Federal Actions To Address Environmental Justice in Minority Populations and Low-Income Populations and Executive Order 14096: Revitalizing Our Nation's Commitment to Environmental Justice for All
The EPA believes that the human health or environmental conditions associated with the primary PM2.5 NAAQS that exist prior to this action result in or have the potential to result in disproportionate and adverse human health or environmental effects on communities with environmental justice concerns. There is strong evidence for racial and ethnic disparities in PM2.5 exposures and PM2.5 -related health risk, as assessed in the 2019 Integrated Science Assessment and with even more evidence available since the literature cutoff date for the 2019 Integrated Science Assessment and evaluated in the Supplement to the 2019 Integrated Science Assessment. There is strong evidence demonstrating that Black and Hispanic populations, in particular, have higher PM2.5 exposures than non-Hispanic White populations. Black populations or individuals that live in predominantly Black neighborhoods experience higher PM2.5 exposures, in comparison to non-Hispanic White populations. There is also consistent evidence across multiple studies that demonstrate increased risk of PM2.5 -related health effects, with the strongest evidence for health risk disparities for mortality. There is also evidence of health risk disparities for both Hispanic and non-Hispanic Black populations compared to non-Hispanic White populations for cause-specific mortality and incident hypertension.
Socioeconomic status (SES) is a composite measure that includes metrics such as income, occupation, or education, and can play a role in access to healthy environments as well as access to healthcare. SES may be a factor that contributes to differential risk from PM2.5 -related health effects. Studies assessed in the 2019 Integrated Science Assessment and Supplement to the 2019 Integrated Science Assessment provide evidence that lower SES communities are exposed to higher concentrations of PM2.5 compared to higher SES communities. Studies using composite measures of neighborhood SES consistently demonstrated a disparity in both PM2.5 exposure and the risk of PM2.5 -related health outcomes. There is some evidence that supports associations larger in magnitude between mortality and long-term PM2.5 exposures for those with low income or living in lower income areas compared to those with higher income or living in higher income neighborhoods. Additionally, evidence supports conclusions that lower SES is associated with cause-specific mortality and certain health endpoints ( i.e., HI and CHF), but less so for all-cause or total (non-accidental) mortality.
The EPA believes that this action is likely to reduce existing disproportionate and adverse effects on communities with environmental justice concerns.
The EPA additionally identified and addressed environmental justice concerns by providing opportunities for public input on the proposed decisions. The EPA held a multi-day virtual public hearing for the public to provide oral testimony and there was a 60-day public comment period for the proposed action. As described in section II.A.3 above, the EPA conducted a risk assessment to support this action that included an at-risk analysis that evaluates exposure and PM2.5 mortality risk for older adults ( e.g., 65 years and older), stratified for White, Black, Asian, Native American, Non-Hispanic, and Hispanic individuals. This at-risk analysis found that compared to a primary annual PM2.5 standard with a level of 12.0 µg/m3 , meeting a revised annual standard with a level of 9.0 µg/m3 is estimated to reduce PM2.5 -associated health risks in the 30 study areas controlled by the annual standard by about 22–28% and is expected to reduce disparities in exposure and risk among these populations.
The information supporting this Executive Order review is is contained in sections II.A.2, II.B.3.a, II.B.3.c, II.B.2, and II.B.4. of this preamble and also in the 2019 Integrated Science Assessment, Supplement to the 2019 Integrated Science Assessment, and 2022 Policy Assessment. The EPA has carefully evaluated the potential impacts on minority populations and low SES populations as discussed in sections II.A.2, II.A.3, II.B.2, and II.B.4 of this preamble. The 2019 Integrated Science Assessment, Supplement to the Integrated Science Assessment, and 2022 Policy Assessment contain the evaluation of the scientific evidence, quantitative risk analyses and policy considerations that pertain to these populations. These documents are available in the public docket for this action.
K. Congressional Review Act (CRA)
This action is subject to the CRA, and the EPA will submit a rule report to each House of the Congress and to the Comptroller General of the United States. This action meets the criteria set forth in 5 U.S.C. 804(2).
References
Abt Associates, Inc. (2001). Assessing public opinions on visibility impairment due to air pollution: Summary report. U.S. Environmental Protection Agency. Research Triangle Park, NC. Available at: https://www3.epa.gov/ttn/naaqs/standards/pm/data/vis_rpt_final.pdf.
Abt Associates, Inc. (2005). Particulate matter health risk assessment for selected urban areas: Draft report. EPA Contract No. 68–D–03–002. U.S. Environmental Protection Agency. Research Triangle Park, NC. Available at: http://www3.epa.gov/ttn/naaqs/standards/pm/data/PMrisk20051220.pdf.
ATS (2000). What Constitutes an Adverse Health Effect of Air Pollution? American Journal of Respiratory and Critical Care Medicine 161(2): 665–673.
BBC Research & Consulting (2003). Phoenix area visibility survey. Denver, CO. Available at: https://www.regulations.gov/document/EPA-HQ-OAR-2015-0072-0089.
Behbod, B, Urch, B, Speck, M, Scott, JA, Liu, L, Poon, R, Coull, B, Schwartz, J, Koutrakis, P, Silverman, F and Gold, DR (2013). Endotoxin in concentrated coarse and fine ambient particles induces acute systemic inflammation in controlled Start Printed Page 16376 human exposures. Occupational and Environmental Medicine 70(11): 761–767.
Bell, ML, Ebisu, K, Peng, RD, Walker, J, Samet, JM, Zeger, SL and Dominic, F (2008). Seasonal and regional short-term effects of fine particles on hospital admissions in 202 U.S. counties, 1999–2005. American Journal of Epidemiology 168(11): 1301–1310.
Bellavia, A, Urch, B, Speck, M, Brook, RD, Scott, JA, Albetti, B, Behbod, B, North, M, Valeri, L, Bertazzi, PA, Silverman, F, Gold, D and Baccarelli, AA (2013). DNA hypomethylation, ambient particulate matter, and increased blood pressure: Findings from controlled human exposure experiments. Journal of the American Heart Association 2(3): e000212.
Bennett, JE, Tamura-Wicks, H, Parks, RM, Burnett, RT, Pope, CA, Bechle, MJ, Marshall, JD, Danaei, G and Ezzati, M (2019). Particulate matter air pollution and national and county life expectancy loss in the USA: A spatiotemporal analysis. PLoS Medicine 16(7): e1002856.
Besson, P, Muñoz, C, Ramírez-Sagner, G, Salgado, M, Escobar, R and Platzer, W (2017). Long-Term Soiling Analysis for Three Photovoltaic Technologies in Santiago Region. IEEE Journal of Photovoltaics 7(6): 1755–1760.
Bourdrel, T, Annesi-Maesano, I, Alahmad, B, Maesano, CN and Bind, MA (2021). The impact of outdoor air pollution on COVID–19: a review of evidence from in vitro, animal, and human studies. 30(159).
Bräuner, EV, Møller, P, Barregard, L, Dragsted, LO, Glasius, M, Wåhlin, P, Vinzents, P, Raaschou-Nielsen, O and Loft, S (2008). Exposure to ambient concentrations of particulate air pollution does not influence vascular function or inflammatory pathways in young healthy individuals. Particle and Fibre Toxicology 5: 13.
Brook, RD, Urch, B, Dvonch, JT, Bard, RL, Speck, M, Keeler, G, Morishita, M, Marsik, FJ, Kamal, AS, Kaciroti, N, Harkema, J, Corey, P, Silverman, F, Gold, DR, Wellenius, G, Mittleman, MA, Rajagopalan, S and Brook, JR (2009). Insights into the mechanisms and mediators of the effects of air pollution exposure on blood pressure and vascular function in healthy humans. Hypertension 54(3): 659–667.
Burns, J, Boogaard, H, Polus, S, Pfadenhauer, LM, Rohwer, AC, van Erp, AM, Turley, R and Rehfuess, E (2019). Interventions to reduce ambient particulate matter air pollution and their effect on health. Cochrane Database of Systematic Reviews (5).
Cangerana Pereira, FA, Lemos, M, Mauad, T, de Assuncao, JV and Nascimento Saldiva, PH (2011). Urban, traffic-related particles and lung tumors in urethane treated mice. Clinics 66(6): 1051–1054.
Chan, EAW, Gantt, B and McDow, S (2018). The reduction of summer sulfate and switch from summertime to wintertime PM2.5 concentration maxima in the United States. Atmospheric Environment 175: 25–32.
Chen, H, Burnett, RT, Copes, R, Kwong, JC, Villeneuve, PJ, Goldberg, MS, Brook, RD, van Donkelaar, A, Jerrett, M, Martin, RV, Brook, JR, Kopp, A and Tu, JV (2016). Ambient fine particulate matter and mortality among survivors of myocardial infarction: population-based cohort study. Environmental Health Perspectives 124(9): 1421–1428.
Correia, AW, Pope, CA, III, Dockery, DW, Wang, Y, un, Ezzati, M and Dominici, F (2013). Effect of air pollution control on life expectancy in the United States: an analysis of 545 U.S. counties for the period from 2000 to 2007. Epidemiology 24(1): 23–31.
Corrigan, AE, Becker, MM, Neas, LM, Cascio, WE and Rappold, AG (2018). Fine particulate matters: The impact of air quality standards on cardiovascular mortality. Environmental research 161: 364–369.
Cox, LA. (2019a). Letter from Louis Anthony Cox, Jr., Chair, Clean Air Scientific Advisory Committee, to Administrator Andrew R. Wheeler. Re: CASAC Review of the EPA's Integrated Science Assessment for Particulate Matter (External Review Draft—October 2018). April 11, 2019. EPA–CASAC–19–002. Office of the Administrator, Science Advisory Board U.S. EPA HQ, Washington DC. Available at: https://casac.epa.gov/ords/sab/r/sab_apex/casac/0?report_id=1069&request=APPLICATION_PROCESS%3DREPORT_DOC&session=7184955370570.
Cox, LA. (2019b). Letter from Louis Anthony Cox, Jr., Chair, Clean Air Scientific Advisory Committee, to Administrator Andrew R. Wheeler. Re: CASAC Review of the EPA's Policy Assessment for the Review of the National Ambient Air Quality Standards for Particulate Matter (External Review Draft—September 2019). December 16, 2019. EPA–CASAC–20–001. Office of the Administrator, Science Advisory Board U.S. EPA HQ, Washington DC. Available at: https://casac.epa.gov/ords/sab/r/sab_apex/casac/0?report_id=1073&request=APPLICATION_PROCESS%3DREPORT_DOC&session=6224161457429.
DeFlorio-Barker, S, Crooks, J, Reyes, J and Rappold, AG (2019). Cardiopulmonary effects of fine particulate matter exposure among older adults, during wildfire and non-wildfire periods, in the United States 2008–2010. Environmental health perspectives 127(3): 037006.
DHEW (1969). Air Quality Criteria for Particulate Matter. National Air Pollution Control Administration. Washington, DC U.S. Department of Health. January 1969.
Di, Q, Amini, H, Shi, L, Kloog, I, Silvern, R, Kelly, J, Sabath, MB, Choirat, C, Koutrakis, P and Lyapustin, A (2019). An ensemble-based model of PM2.5 concentration across the contiguous United States with high spatiotemporal resolution. Environment International 130: 104909.
Di, Q, Dai, L, Wang, Y, Zanobetti, A, Choirat, C, Schwartz, JD and Dominici, F (2017a). Association of short-term exposure to air pollution with mortality in older adults. JAMA: Journal of the American Medical Association 318(24): 2446–2456.
Di, Q, Kloog, I, Koutrakis, P, Lyapustin, A, Wang, Y and Schwartz, J (2016). Assessing PM2.5 exposures with high spatiotemporal resolution across the Continental United States. Environmental Science and Technology 50(9): 4712–4721.
Di, Q, Wang, Y, Zanobetti, A, Wang, Y, Koutrakis, P, Choirat, C, Dominici, F and Schwartz, JD (2017b). Air pollution and mortality in the Medicare population. New England Journal of Medicine 376(26): 2513–2522.
Dominici, F, Schwartz, J, Di, Q, Braun, D, Choirat, C and Zanobetti, A (2019). Assessing adverse health effects of long-term exposure to low levels of ambient air pollution: Phase 1. Health Effects Institute. Boston, MA. Available at: https://www.healtheffects.org/system/files/dominici-rr-200-report.pdf.
Ely, DW, Leary, JT, Stewart, TR and Ross, DM (1991). The establishment of the Denver Visibility Standard. Colorado Department of Health. Denver, Colorado.
Erickson, AC, Christidis, T, Pappin, A, Brook, JR, Crouse, DL, Hystad, P, Li, C, Martin, RV, Meng, J, Pinault, L, von Donkelaar, A, Weichenthal, S, Tjepkema, M, Burnett, RT and Brauer, M (2020). Disease assimilation: The mortality impacts of fine particulate matter on immigrants to Canada. Health Reports 31(3): 14–26.
Eum, K, Suh, HH, Pun, V and Manjourides, J (2018). Impact of long-term temporal trends in fine particulate matter (PM2.5) on association of annual PM2.5 exposure and mortality: an analysis of over 20 million Medicare beneficiaries. Environmental Epidemiology 2(2): e009.
Fiore, AM, Naik, V and Leibensperger, EM (2015). Air quality and climate connections. Journal of the Air and Waste Management Association 65(6): 645–685.
Frank, N. (2012). Memorandum to PM NAAQS Review Docket (EPA–HQ–OAR–2007–0492) regarding the Differences between maximum and composite monitor annual PM2.5 design values by CBSA. Dec 14, 2012. Docket ID No. EPA–HQ–OAR–2007–0492. Office of Air Quality Planning and Standards Research Triangle Park, NC. Available at: https://www.regulations.gov/document/EPA-HQ-OAR-2007-0492-10099.
Franklin, M, Zeka, A and Schwartz, J (2007). Association between PM2.5 and all-cause and specific-cause mortality in 27 US communities. Journal of Exposure Science and Environmental Epidemiology 17(3): 279–287.
Gantt, B, Owen, RC and Watkins, N (2021). Characterizing Nitrogen Oxides and Fine Particulate Matter near Major Highways in the United States Using the National Near-Road Monitoring Network. Environmental science & technology 55(5): 2831–2838. Start Printed Page 16377
Ghio, AJ, Hall, A, Bassett, MA, Cascio, WE and Devlin, RB (2003). Exposure to concentrated ambient air particles alters hematologic indices in humans. Inhalation Toxicology 15(14): 1465–1478.
Ghio, AJ, Kim, C and Devlin, RB (2000). Concentrated ambient air particles induce mild pulmonary inflammation in healthy human volunteers. American Journal of Respiratory and Critical Care Medicine 162(3): 981–988.
Greven, S, Dominici, F and Zeger, S (2011). An Approach to the Estimation of Chronic Air Pollution Effects Using Spatio-Temporal Information. Journal of the American Statistical Association 106(494): 396–406.
Grøntoft, T, Verney-Carron, A and Tidblad, J (2019). Cleaning Costs for European Sheltered White Painted Steel and Modern Glass Surfaces Due to Air Pollution Since the Year 2000. Atmosphere 10(4): 167.
Hammer, MS, van Donkelaar, A, Li, C, Lyapustin, A, Sayer, AM, Hsu, NC, Levy, RC, Garay, MJ, Kalashnikova, OV and Kahn, RA (2020). Global estimates and long-term trends of fine particulate matter concentrations (1998–2018). Environmental Science & Technology 54(13): 7879–7890.
Hart, JE, Liao, X, Hong, B, Puett, RC, Yanosky, JD, Suh, H, Kioumourtzoglou, MA, Spiegelman, D and Laden, F (2015). The association of long-term exposure to PM2.5 on all-cause mortality in the Nurses' Health Study and the impact of measurement-error correction. Environmental Health: A Global Access Science Source 14: 38.
Hassett-Sipple, B, Schmidt, M and Rajan, P. (2010). Memorandum to PM NAAQS Review Docket (EPA–HQ–OAR–2007–0492). Analysis of PM2.5 (Particulate Matter Smaller than 2.5 Micrometers in Diameter). Mar 30, 2010. Docket ID No. EPA–HQ–OAR–2007–0492. Office of Air Quality Planning and Standards Research Triangle Park, NC. Available at: https://www.regulations.gov/document/EPA-HQ-OAR-2007-0492-0077.
Hemmingsen, JG, Jantzen, K, Møller, P and Loft, S (2015a). No oxidative stress or DNA damage in peripheral blood mononuclear cells after exposure to particles from urban street air in overweight elderly. Mutagenesis 30(5): 635–642.Hemmingsen, JG, Rissler, J, Lykkesfeldt, J, Sallsten, G, Kristiansen, J, Møller, P and Loft, S (2015). Controlled exposure to particulate matter from urban street air is associated with decreased vasodilation and heart rate variability in overweight and older adults. Particle and Fibre Toxicology 12(1): 6.
Henneman, LR, Liu, C, Mulholland, JA and Russell, AG (2017). Evaluating the effectiveness of air quality regulations: A review of accountability studies and frameworks. Journal of the Air Waste Management Association 67(2): 144–172.
Henneman, LRF, Choirat, C and Zigler, ACM (2019). Accountability assessment of health improvements in the United States associated with reduced coal emissions between 2005 and 2012. Epidemiology 30(4): 477–485.
Hutchinson, JA, Vargo, J, Milet, M, French, NH, Billmire, M, Johnson, J and Hoshiko, S (2018). The San Diego 2007 wildfires and Medi-Cal emergency department presentations, inpatient hospitalizations, and outpatient visits: An observational study of smoke exposure periods and a bidirectional case-crossover analysis. PLoS medicine 15(7): e1002601.
IPCC (2013). Climate change 2013: The physical science basis. Contribution of working group I to the fifth assessment report of the Intergovernmental Panel on Climate Change. T. F. Stocker, D. Qin, G. K. Plattner et al. Cambridge University Press. Cambridge, UK.
Kloog, I, Ridgway, B, Koutrakis, P, Coull, BA and Schwartz, JD (2013). Long- and short-term exposure to PM2.5 and mortality: Using novel exposure models. Epidemiology 24(4): 555–561.
Krewski, D, Jerrett, M, Burnett, RT, Ma, R, Hughes, E, Shi, Y, Turner, MC, Pope, CA, III, Thurston, G, Calle, EE, Thun, MJ, Beckerman, B, Deluca, P, Finkelstein, N, Ito, K, Moore, DK, Newbold, KB, Ramsay, T, Ross, Z, Shin, H and Tempalski, B (2009). Extended follow-up and spatial analysis of the American Cancer Society study linking particulate air pollution and mortality. ISSN 1041–5505, HEI Research Report 140. Health Effects Institute. Boston, MA. Available at: https://www.healtheffects.org/system/files/Krewski140Statement.pdf.
Laden, F, Schwartz, J, Speizer, FE and Dockery, DW (2006). Reduction in fine particulate air pollution and mortality: extended follow-up of the Harvard Six Cities study. American Journal of Respiratory and Critical Care Medicine 173(6): 667–672.
Lavigne, E, Burnett, RT and Weichenthal, S (2018). Association of short-term exposure to fine particulate air pollution and mortality: effect modification by oxidant gases. Scientific Reports 8(1): 16097.
Lee, M, Koutrakis, P, Coull, B, Kloog, I and Schwartz, J (2015). Acute effect of fine particulate matter on mortality in three Southeastern states from 2007–2011. Journal of Exposure Science and Environmental Epidemiology 26(2): 173–179.
Lepeule, J, Laden, F, Dockery, D and Schwartz, J (2012). Chronic exposure to fine particles and mortality: an extended follow-up of the Harvard Six Cities study from 1974 to 2009. Environmental Health Perspectives 120(7): 965–970.
Lippmann, M, Chen, LC, Gordon, T, Ito, K and Thurston, GD (2013). National Particle Component Toxicity (NPACT) Initiative: Integrated epidemiologic and toxicologic studies of the health effects of particulate matter components: Investigators' Report. 177. Health Effects Institute. Boston, MA.
Liu, C, Chen, R, Sera, F, Vicedo-Cabrera, AM, Guo, Y, Tong, S, Coelho, M, Saldiva, PHN, Lavigne, E, Matus, P, Valdes Ortega, N, Osorio Garcia, S, Pascal, M, Stafoggia, M, Scortichini, M, Hashizume, M, Honda, Y, Hurtado-Díaz, M, Cruz, J, Nunes, B, Teixeira, JP, Kim, H, Tobias, A, Íñiguez, C, Forsberg, B, Åström, C, Ragettli, MS, Guo, YL, Chen, BY, Bell, ML, Wright, CY, Scovronick, N, Garland, RM, Milojevic, A, Kyselý, J, Urban, A, Orru, H, Indermitte, E, Jaakkola, JJK, Ryti, NRI, Katsouyanni, K, Analitis, A, Zanobetti, A, Schwartz, J, Chen, J, Wu, T, Cohen, A, Gasparrini, A and Kan, H (2019). Ambient Particulate Air Pollution and Daily Mortality in 652 Cities. New England Journal of Medicine 381(8): 705–715.
Lowenthal, DH and Kumar, N (2004). Variation of mass scattering efficiencies in IMPROVE. Journal of the Air and Waste Management Association (1990–1992) 54(8): 926–934.
Lowenthal, DH and Kumar, N (2016). Evaluation of the IMPROVE Equation for estimating aerosol light extinction. Journal of the Air and Waste Management Association 66(7): 726–737.
Lucking, AJ, Lundbäck, M, Barath, SL, Mills, NL, Sidhu, MK, Langrish, JP, Boon, NA, Pourazar, J, Badimon, JJ, Gerlofs-Nijland, ME, Cassee, FR, Boman, C, Donaldson, K, Sandstrom, T, Newby, DE and Blomberg, A (2011). Particle traps prevent adverse vascular and prothrombotic effects of diesel engine exhaust inhalation in men. Circulation 123(16): 1721–1728.
Malm, WC and Hand, JL (2007). An examination of the physical and optical properties of aerosols collected in the IMPROVE program. Atmospheric Environment 41(16): 3407–3427.
Malm, WC, Schichtel, B, Molenar, J, Prenni, A and Peters, M (2019). Which visibility indicators best represent a population's preference for a level of visual air quality? Journal of the Air & Waste Management Association 69(2): 145–161.
Malm, WC, Sisler, JF, Huffman, D, Eldred, RA and Cahill, TA (1994). Spatial and seasonal trends in particle concentration and optical extinction in the United States. Journal of Geophysical Research 99(D1): 1347–1370.
Mauad, T, Rivero, DH, de Oliveira, RC, Lichtenfels, AJ, Guimaraes, ET, de Andre, PA, Kasahara, DI, Bueno, HM and Saldiva, PH (2008). Chronic exposure to ambient levels of urban particles affects mouse lung development. American Journal of Respiratory and Critical Care Medicine 178(7): 721–728.
Mie, G (1908). Beitrage zur Optik truber Medien, speziell kolloidaler Metallosungen [Optics of cloudy media, especially colloidal metal solutions]. Annalen der Physik 25(3): 377–445.
Miller, KA, Siscovick, DS, Sheppard, L, Shepherd, K, Sullivan, JH, Anderson, GL and Kaufman, JD (2007). Long-term exposure to air pollution and incidence of cardiovascular events in women. New England Journal of Medicine 356(5): 447–458.
Myhre, G, Shindell, D, Bréon, FM, Collins, W, Fuglestvedt, J, Huang, J, Koch, D, Lamarque, JF, Lee, D, Mendoza, B, Nakajima, T, Robock, A, Stephens, G, Start Printed Page 16378 Takemura, T and Zhang, H, Eds. (2013). Anthropogenic and natural radiative forcing. Cambridge University Press Cambridge, UK.
NHLBI (2017). “NHLBI fact book, fiscal year 2012: Disease statistics.” Retrieved August 23, 2017, from https://web.archive.org/web/20170711012213/http://www.nhlbi.nih.gov/about/documents/factbook/2012/chapter4.
Orr, A, AL Migliaccio, C, Buford, M, Ballou, S and Migliaccio, CT (2020). Sustained effects on lung function in community members following exposure to hazardous pm2. 5 levels from wildfire smoke. Toxics 8(3): 53.
Pitchford, M, Maim, W, Schichtel, B, Kumar, N, Lowenthal, D and Hand, J (2007). Revised algorithm for estimating light extinction from IMPROVE particle speciation data. Journal of the Air and Waste Management Association 57(11): 1326–1336.
Pope, CA, III, Burnett, RT, Thurston, GD, Thun, MJ, Calle, EE, Krewski, D and Godleski, JJ (2004). Cardiovascular mortality and long-term exposure to particulate air pollution: epidemiological evidence of general pathophysiological pathways of disease. Circulation 109(1): 71–77.
Pope, CA, III, Ezzati, M and Dockery, DW (2009). Fine-particulate air pollution and life expectancy in the United States. New England Journal of Medicine 360(4): 376–386.
Pruitt, E. (2018). Memorandum from E. Scott Pruitt, Administrator, U.S. EPA to Assistant Administrators. Back-to-Basics Process for Reviewing National Ambient Air Quality Standards. May 9, 2018. Office of the Administrator U.S. EPA HQ, Washington DC. Available at: https://www.epa.gov/criteria-air-pollutants/back-basics-process-reviewing-national-ambient-air-quality-standards.
Pryor, SC (1996). Assessing public perception of visibility for standard setting exercises. Atmospheric Environment 30(15): 2705–2716.
Puett, RC, Hart, JE, Yanosky, JD, Spiegelman, D, Wang, M, Fisher, JA, Hong, B and Laden, F (2014). Particulate matter air pollution exposure, distance to road, and incident lung cancer in the Nurses' Health Study cohort. Environmental Health Perspectives 122(9): 926–932.
Pun, VC, Kazemiparkouhi, F, Manjourides, J and Suh, HH (2017). Long-term PM2.5 exposures and respiratory, cancer and cardiovascular mortality in American older adults. American Journal of Epidemiology 186(8): 961–969.
Raaschou-Nielsen, O, Andersen, ZJ, Beelen, R, Samoli, E, Stafoggia, M, Weinmayr, G, Hoffmann, B, Fischer, P, Nieuwenhuijsen, MJ, Brunekreef, B, Xun, WW, Katsouyanni, K, Dimakopoulou, K, Sommar, J, Forsberg, B, Modig, L, Oudin, A, Oftedal, B, Schwarze, PE, Nafstad, P, De Faire, U, Pedersen, NL, Östenson, CG, Fratiglioni, L, Penell, J, Korek, M, Pershagen, G, Eriksen, KT, Sørensen, M, Tjønneland, A, Ellermann, T, Eeftens, M, Peeters, PH, Meliefste, K, Wang, M, Bueno-De-mesquita, B, Key, TJ, De Hoogh, K, Concin, H, Nagel, G, Vilier, A, Grioni, S, Krogh, V, Tsai, MY, Ricceri, F, Sacerdote, C, Galassi, C, Migliore, E, Ranzi, A, Cesaroni, G, Badaloni, C, Forastiere, F, Tamayo, I, Amiano, P, Dorronsoro, M, Trichopoulou, A, Bamia, C, Vineis, P and Hoek, G (2013). Air pollution and lung cancer incidence in 17 European cohorts: Prospective analyses from the European Study of Cohorts for Air Pollution Effects (ESCAPE). The Lancet Oncology 14(9): 813–822.
Ramanathan, G, Yin, F, Speck, M, Tseng, CH, Brook, JR, Silverman, F, Urch, B, Brook, RD and Araujo, JA (2016). Effects of urban fine particulate matter and ozone on HDL functionality. Particle and Fibre Toxicology 13(1): 26.
Ryan, PA, Lowenthal, D and Kumar, N (2005). Improved light extinction reconstruction in interagency monitoring of protected visual environments. Journal of the Air and Waste Management Association 55(11): 1751–1759.
Sacks, JD, Ito, K, Wilson, WE and Neas, LM (2012). Impact of covariate models on the assessment of the air pollution-mortality association in a single- and multipollutant context. American Journal of Epidemiology 176(7): 622–634.
Sanders, NJ, Barreca, AI and Neidell, MJ (2020a). Estimating causal effects of particulate matter regulation on mortality. Epidemiology (Cambridge, Mass.) 31(2): 160.
Sanders, NJ, Barreca, AI and Neidell, MJ (2020b). Estimating Causal Effects of Particulate Matter Regulation on Mortality. Epidemiology 31(2): 160–167.
Schwartz, J, Austin, E, Bind, MA, Zanobetti, A and Koutrakis, P (2015). Estimating causal associations of fine particles with daily deaths in Boston. American Journal of Epidemiology 182(7): 644–650.
Schwartz, J, Bind, MA and Koutrakis, P (2017). Estimating causal effects of local air pollution on daily deaths: Effect of low levels. Environmental Health Perspectives 125(1): 23–29.
Schwartz, J, Wei, Y, Di, Q, Dominici, F and Zanobetti, A (2021). A national difference in differences analysis of the effect of PM2. 5 on annual death rates. Environmental Research 194: 110649.
Schwartz, JD, Wang, Y, Kloog, I, Yitshak-Sade, M, Dominici, F and Zanobetti, A (2018). Estimating the Effects of PM2.5 on Life Expectancy Using Causal Modeling Methods. Environmental Health Perspectives 126(12): 127002.
Sheppard, EA. (2022a). Letter from Elizabeth A. (Lianne) Sheppard, Chair, Clean Air Scientific Advisory Committee, to Administrator Michael S. Regan. Re: CASAC Review of the EPA's Policy Assessment for the Review of the National Ambient Air Quality Standards for Particulate Matter (External Review Draft—October 2021). March 18, 2022. EPA–CASAC–22–002. Office of the Administrator, Science Advisory Board U.S. EPA HQ, Washington DC. Available at: https://casac.epa.gov/ords/sab/r/sab_apex/casac/0?report_id=1094&request=APPLICATION_PROCESS%3DREPORT_DOC&session=7184955370570.
Sheppard, EA. (2022b). Letter from Elizabeth A. (Lianne) Sheppard, Chair, Clean Air Scientific Advisory Committee, to Administrator Michael S. Regan. Re: CASAC Review of the EPA's Supplement to the 2019 Integrated Science Assessment for Particulate Matter (External Review Draft—October 2021). EPA–CASAC–22–001. Office of the Administrator, Science Advisory Board U.S. EPA HQ, Washington DC. Available at: https://casac.epa.gov/ords/sab/r/sab_apex/casac/0?report_id=1093&request=APPLICATION_PROCESS%3DREPORT_DOC&session=10813926997922.
Shi, L, Zanobetti, A, Kloog, I, Coull, BA, Koutrakis, P, Melly, SJ and Schwartz, JD (2016). Low-concentration PM2.5 and mortality: estimating acute and chronic effects in a population-based study. Environmental Health Perspectives 124(1): 46–52.
Shin, HH, Gogna, P, Maquiling, A, Parajuli, RP, Haque, L and Burr, B (2021). Comparison of hospitalization and mortality associated with short-term exposure to ambient ozone and PM2.5 in Canada. Chemosphere 265: 128683.
Sivagangabalan, G, Spears, D, Masse, S, Urch, B, Brook, RD, Silverman, F, Gold, DR, Lukic, KZ, Speck, M, Kusha, M, Farid, T, Poku, K, Shi, E, Floras, J and Nanthakumar, K (2011). The effect of air pollution on spatial dispersion of myocardial repolarization in healthy human volunteers. Journal of the American College of Cardiology 57(2): 198–206.
Smith, AE and Howell, S (2009). An assessment of the robustness of visual air quality preference study results. CRA International. Washington, DC. Available at: https://www.regulations.gov/document/EPA-HQ-ORD-2007-0517-0085.
Statistics Canada (2023). Census Profile. 2021 Census of Population. Statistics Canada Catalogue no. 98–316–X2021001. Ottawa. Released March 29, 2023. Available at: https://www12.statcan.gc.ca/census-recensement/2021/dp-pd/prof/index.cfm?Lang=E.
Thurston, GD, Kipen, H, Annesi-Maesano, I, Balmes, J, Brook, RD, Cromar, K, De Matteis, S, Forastiere, F, Forsberg, B, Frampton, MW, Grigg, J, Heederik, D, Kelly, FJ, Kuenzli, N, Laumbach, R, Peters, A, Rajagopalan, ST, Rich, D, Ritz, B, Samet, JM, Sandstrom, T, Sigsgaard, T, Sunyer, J and Brunekreef, B (2017). A joint ERS/ATS policy statement: what constitutes an adverse health effect of air pollution? An analytical framework. European Respiratory Journal 49(1): 1600419.
Tong, H, Rappold, AG, Caughey, M, Hinderliter, AL, Bassett, M, Montilla, T, Case, MW, Berntsen, J, Bromberg, PA, Cascio, WE, Diaz-Sanchez, D, Devlin, RB and Samet, JM (2015). Dietary Start Printed Page 16379 supplementation with olive oil or fish oil and vascular effects of concentrated ambient particulate matter exposure in human volunteers. Environmental Health Perspectives 123(11): 1173–1179.
U.S. EPA (2004a). Air Quality Criteria for Particulate Matter. (Vol I of II). Office of Research and Development. Research Triangle Park, NC. U.S. EPA. EPA–600/P–99–002aF. October 2004. Available at: https://nepis.epa.gov/Exe/ZyPURL.cgi?Dockey=P100LFIQ.txt.
U.S. EPA (2004b). Air Quality Criteria for Particulate Matter. (Vol II of II). Office of Research and Development. Research Triangle Park, NC. U.S. EPA. EPA–600/P–99–002bF. October 2004. Available at: https://nepis.epa.gov/Exe/ZyPURL.cgi?Dockey=P100LG7Q.txt.
U.S. EPA (2005). Review of the National Ambient Air Quality Standards for Particulate Matter: Policy Assessment of Scientific and Technical Information, OAQPS Staff Paper. Office of Air Quality Planning and Standards. Research Triangle Park, NC. U.S. EPA. EPA–452/R–05–005a. December 2005. Available at: https://nepis.epa.gov/Exe/ZyPURL.cgi?Dockey=P1009MZM.txt.
U.S. EPA (2008). Integrated Review Plan for the National Ambient Air Quality Standards for Particulate Matter. Office of Research and Development, National Center for Environmental Assessment; Office of Air Quality Planning and Standards, Health and Environmental Impacts Division. Research Triangle Park, NC. U.S. EPA. EPA 452/R–08–004. March 2008. Available at: https://nepis.epa.gov/Exe/ZyPURL.cgi?Dockey=P1001FB9.txt.
U.S. EPA (2009a). Particulate Matter National Ambient Air Quality Standards: Scope and Methods Plan for Health Risk and Exposure Assessment. Office of Air Quality Planning and Standards, Health and Environmental Impacts Division. Research Triangle Park, NC. U.S. EPA. EPA–452/P–09–002. February 2009. Available at: https://nepis.epa.gov/Exe/ZyPURL.cgi?Dockey=P100FLWP.txt.
U.S. EPA (2009b). Particulate Matter National Ambient Air Quality Standards: Scope and Methods Plan for Urban Visibility Impact Assessment. Office of Air Quality Planning and Standards, Health and Environmental Impacts Division. Research Triangle Park, NC. U.S. EPA. EPA–452/P–09–001. February 2009. Available at: https://nepis.epa.gov/Exe/ZyPURL.cgi?Dockey=P100FLUX.txt.
U.S. EPA (2009c). Integrated Science Assessment for Particulate Matter (Final Report). Office of Research and Development, National Center for Environmental Assessment. Research Triangle Park, NC. U.S. EPA. EPA–600/R–08–139F. December 2009. Available at: https://cfpub.epa.gov/ncea/risk/recordisplay.cfm?deid=216546.
U.S. EPA (2010a). Quantitative Health Risk Assessment for Particulate Matter (Final Report). Office of Air Quality Planning and Standards, Health and Environmental Impacts Division. Research Triangle Park, NC. U.S. EPA. EPA–452/R–10–005. June 2010. Available at: https://nepis.epa.gov/Exe/ZyPURL.cgi?Dockey=P1007RFC.txt.
U.S. EPA (2010b). Particulate Matter Urban-Focused Visibility Assessment (Final Document). Office of Air Quality Planning and Standards, Health and Environmental Impacts Division. Research Triangle Park, NC. U.S. EPA. EPA–452/R–10–004. July 2010. Available at: https://nepis.epa.gov/Exe/ZyPURL.cgi?Dockey=P100FO5D.txt.
U.S. EPA (2011). Policy Assessment for the Review of the Particulate Matter National Ambient Air Quality Standards. Office of Air Quality Planning and Standards, Health and Environmental Impacts Division. Research Triangle Park, NC. U.S. EPA. EPA–452/R–11–003. April 2011. Available at: https://nepis.epa.gov/Exe/ZyPURL.cgi?Dockey=P100AUMY.txt.
U.S. EPA (2012). Responses to Significant Comments on the 2012 Proposed Rule on the National Ambient Air Quality Standards for Particulate Matter (June 29, 2012; 77 FR 38890). Research Triangle Park, NC. U.S. EPA. Docket ID No. EPA–HQ–OAR–2007–0492. Available at: https://www3.epa.gov/ttn/naaqs/standards/pm/data/20121214rtc.pdf.
U.S. EPA (2015). Preamble to the integrated science assessments. U.S. Environmental Protection Agency, Office of Research and Development, National Center for Environmental Assessment, RTP Division. Research Triangle Park, NC. U.S. EPA. EPA/600/R–15/067. November 2015. Available at: https://cfpub.epa.gov/ncea/isa/recordisplay.cfm?deid=310244.
U.S. EPA (2016). Integrated review plan for the national ambient air quality standards for particulate matter. Office of Air Quality Planning and Standards. Research Triangle Park, NC. U.S. EPA. EPA–452/R–16–005. December 2016. Available at: https://www3.epa.gov/ttn/naaqs/standards/pm/data/201612-final-integrated-review-plan.pdf.
U.S. EPA (2017). Emissions Inventory Guidance for Implementation of Ozone and Particulate Matter National Ambient Air Quality Standards (NAAQS) and Regional Haze Regulations. Office of Air Quality Planning and Standards, Office of Air and Radiation. Research Triangle Park, NC. U.S. EPA. U.S. EPA–454/B–17–002. Available at: https://www.epa.gov/sites/default/files/2017-07/documents/ei_guidance_may_2017_final_rev.pdf.
U.S. EPA (2018a). Technical Assistance Document (TAD) for the Reporting of Daily Air Quality—the Air Quality Index (AQI). U.S. Environmental Protection Agency, Office of Air Quality Planning and Standards. Research Triangle Park, NC. U.S. EPA. EPA 454/B–18–007. September 2018. Available at: https://www.airnow.gov/sites/default/files/2020-05/aqi-technical-assistance-document-sept2018.pdf.
U.S. EPA (2018b). Modeling Guidance for Demonstrating Air Quality Goals for Ozone, PM2.5, and Regional Haze. Office of Air Quality Planning and Standards, Air Quality Policy Division. Research Triangle Park, NC. U.S. EPA. EPA 454/R–18–009. November 2018. Available at: https://www.epa.gov/sites/default/files/2020-10/documents/o3-pm-rh-modeling_guidance-2018.pdf.
U.S. EPA (2019a). Integrated Science Assessment (ISA) for Particulate Matter (Final Report). U.S. Environmental Protection Agency, Office of Research and Development, National Center for Environmental Assessment. Washington, DC. U.S. EPA. EPA/600/R–19/188. December 2019. Available at: https://www.epa.gov/naaqs/particulate-matter-pm-standards-integrated-science-assessments-current-review.
U.S. EPA (2019b). PM2.5 Precursor Demonstration Guidance. Office of Air Quality Planning and Standards, Air Quality Policy Division. Research Triangle Park, NC. U.S. EPA. EPA–454/R–19–004. May 2019. Available at: https://nepis.epa.gov/Exe/ZyPDF.cgi/P100YD1Q.PDF?Dockey=P100YD1Q.PDF.
U.S. EPA (2020a). Responses to significant comments on the 2020 proposed rule on the National Ambient Air Quality Standards for particulate matter (April 30, 2020; 85 FR 24094). EPA–HQ–OAR–2015–0072. Available at: https://www.epa.gov/sites/production/files/2020-12/documents/pm_naaqs_response_to_comments_final.pdf.
U.S. EPA (2020b). Policy Assessment for the Review of the National Ambient Air Quality Standards for Particulate Matter. Office of Air Quality Planning and Standards, Health and Environmental Impacts Division. Research Triangle Park, NC. U.S. EPA. EPA–452/R–20–002. January 2020. Available at: https://www.epa.gov/system/files/documents/2021-10/final-policy-assessment-for-the-review-of-the-pm-naaqs-01-2020.pdf.
U.S. EPA (2021a). Supplement to the 2019 Integrated Science Assessment for Particulate Matter (External Review Draft). U.S. Environmental Protection Agency, Office of Research and Development, Center for Public Health and Environmental Assessment. Research Triangle Park, NC. U.S. EPA. EPA/600/R–21/198. December 2019. Available at: https://www.epa.gov/naaqs/particulate-matter-pm-standards-integrated-science-assessments-current-review.
U.S. EPA (2021b). Comparative Assessment of the Impacts of Prescribed Fire Versus Wildfire (CAIF): A Case Study in the Western U.S. U.S. Environmental Protection Agency. Washington, DC. U.S. EPA. EPA/600/R–21/197.
U.S. EPA (2021c). Policy Assessment for the Review of the National Ambient Air Quality Standards for Particulate Matter (External Review Draft). Office of Air Quality Planning and Standards, Health and Environmental Impacts Division. Research Triangle Park, NC. U.S. EPA. EPA–452/P–21–001. October 2021. Available at: https://www.epa.gov/system/files/documents/2022-05/ Start Printed Page 16380 Final%20Policy%20Assessment%20for%20the%20Reconsideration%20of%20the%20PM%20NAAQS_May2022_0.pdf.
U.S. EPA (2021d). Guidance for Ozone and Fine Particulate Matter Permit Modeling. U.S. Environmental Protection Agency, Office of Air Quality Planning and Standards, Air Quality Assessment Division. Research Triangle Park, NC. U.S. EPA. EPA–454/P–21–001. September 2021.
U.S. EPA (2022a). Policy Assessment for the Reconsideration of the National Ambient Air Quality Standards for Particulate Matter. Office of Air Quality Planning and Standards, Health and Environmental Impacts Division. Research Triangle Park, NC. U.S. EPA. EPA–452/R–22–004. May 2022. Available at: https://www.epa.gov/system/files/documents/2022-05/Final%20Policy%20Assessment%20for%20the%20Reconsideration%20of%20the%20PM%20NAAQS_May2022_0.pdf.
U.S. EPA (2022b). Supplement to the 2019 Integrated Science Assessment for Particulate Matter (Final Report). U.S. Environmental Protection Agency, Office of Research and Development, Center for Public Health and Environmental Assessment. Research Triangle Park, NC. U.S. EPA. EPA/600/R 22/028. May 2022. Available at: https://www.epa.gov/naaqs/particulate-matter-pm-standards-integrated-science-assessments-current-review.
Urch, B, Speck, M, Corey, P, Wasserstein, D, Manno, M, Lukic, KZ, Brook, JR, Liu, L, Coull, B, Schwartz, J, Gold, DR and Silverman, F (2010). Concentrated ambient fine particles and not ozone induce a systemic interleukin-6 response in humans. Inhalation Toxicology 22(3): 210–218.
Van de Hulst, H (1981). Light scattering by small particles. Dover Publications, Inc. New York.
van Donkelaar, A, Martin, RV, Li, C and Burnett, RT (2019). Regional estimates of chemical composition of fine particulate matter using a combined geoscience-statistical method with information from satellites, models, and monitors. Environmental Science & Technology 53(5).
Vieira, JL, Guimaraes, GV, de Andre, PA, Cruz, FD, Nascimento Saldiva, PH and Bocchi, EA (2016a). Respiratory filter reduces the cardiovascular effects associated with diesel exhaust exposure a randomized, prospective, double-blind, controlled study of heart failure: the FILTER–HF trial. JACC: Heart Failure 4(1): 55–64.
Vieira, JL, Guimaraes, GV, de Andre, PA, Nascimento Saldiva, PH and Bocchi, EA (2016b). Effects of reducing exposure to air pollution on submaximal cardiopulmonary test in patients with heart failure: Analysis of the randomized, double-blind and controlled FILTER–HF trial. International Journal of Cardiology 215: 92–97.
Wang, Y, Shi, L, Lee, M, Liu, P, Di, Q, Zanobetti, A and Schwartz, JD (2017). Long-term exposure to PM2.5 and mortality among older adults in the Southeastern US. Epidemiology 28(2): 207–214.
Ward-Caviness, CK, Weaver, AM, Buranosky, M, Pfaff, ER, Neas, LM, Devlin, RB, Schwartz, J, Di, Q, Cascio, WE and Diaz-Sanchez, D (2020). Associations between long-term fine particulate matter exposure and mortality in heart failure patients. Journal of the American Heart Association 9(6): e012517.
Wei, Y, Yazdi, MD, Di, Q, Requia, WJ, Dominici, F, Zanobetti, A and Schwartz, J (2021). Emulating causal dose-response relations between air pollutants and mortality in the Medicare population. Environmental Health: A Global Access Science Source 20(1): 53.
Wu, X, Braun, D, Schwartz, J, Kioumourtzoglou, MA and Dominici, F (2020). Evaluating the impact of long-term exposure to fine particulate matter on mortality among the elderly. Science Advances 6(29): eaba5692.
Wyatt, LH, Devlin, RB, Rappold, AG, Case, MW and Diaz-Sanchez, D (2020). Low levels of fine particulate matter increase vascular damage and reduce pulmonary function in young healthy adults. Particle and fibre toxicology 17(1): 1–12.
Yorifuji, T, Kashima, S and Doi, H (2016). Fine-particulate air pollution from diesel emission control and mortality rates in Tokyo: a quasi-experimental study. Epidemiology 27(6): 769–778.
Zanobetti, A and Schwartz, J (2009). The effect of fine and coarse particulate air pollution on mortality: A national analysis. Environmental Health Perspectives 117(6): 1–40.
Zhang, Z, Wang, J, Kwong, JC, Burnett, RT, van Donkelaar, A, Hystad, P, Martin, RV, Bai, L, McLaughlin, J and Chen, H (2021). Long-term exposure to air pollution and mortality in a prospective cohort: The Ontario Health Study. Environment International 154: 106570.
Start List of SubjectsList of Subjects
40 CFR Part 50
- Environmental protection
- Air pollution control
- Carbon monoxide
- Lead
- Nitrogen dioxide
- Ozone
- Particulate matter
- Sulfur oxides
40 CFR Part 53
- Environmental protection
- Administrative practice and procedure
- Air pollution control
- Reporting and recordkeeping requirements
40 CFR Part 58
- Environmental protection
- Administrative practice and procedure
- Air pollution control
- Intergovernmental relations
- Reporting and recordkeeping requirements
End SignatureMichael S. Regan,
Administrator.
For the reasons set forth in the preamble, chapter I of title 40 of the Code of Federal Regulations is amended as follows:
Start PartPART 50—NATIONAL PRIMARY AND SECONDARY AMBIENT AIR QUALITY STANDARDS
End Part Start Amendment Part1. The authority citation for part 50 continues to read as follows:
End Amendment Part Start Amendment Part2. Add § 50.20 to read as follows:
End Amendment PartStart Amendment PartNational primary ambient air quality standards for PM 2.5 .(a) The national primary ambient air quality standards for PM2.5 are 9.0 micrograms per cubic meter (µg/m3 ) annual arithmetic mean concentration and 35 µg/m3 24-hour average concentration measured in the ambient air as PM2.5 (particles with an aerodynamic diameter less than or equal to a nominal 2.5 micrometers) by either:
(1) A reference method based on appendix L to this part and designated in accordance with part 53 of this chapter; or
(2) An equivalent method designated in accordance with part 53 of this chapter.
(b) The primary annual PM2.5 standard is met when the annual arithmetic mean concentration, as determined in accordance with appendix N to this part, is less than or equal to 9.0 µg/m3 .
(c) The primary 24-hour PM2.5 standard is met when the 98th percentile 24-hour concentration, as determined in accordance with appendix N to this part, is less than or equal to 35 µg/m3 .
3. Amend appendix K to part 50 by:
End Amendment Part Start Amendment Parta. In section 1.0 revising paragraph (b);
End Amendment Part Start Amendment Partb. In section 2.3 adding paragraph (d); and
End Amendment Part Start Amendment Partc. In section 3.0 adding paragraphs (a) and (b).
End Amendment PartThe revision and additions read as follows:
Appendix K to Part 50—Interpretation of the National Ambient Air Quality Standards for Particulate Matter
1.0 General
* * * * *(b) The terms used in this appendix are defined as follows:
Average refers to the arithmetic mean of the estimated number of exceedances per year, as per section 3.1 of this appendix.
Collocated monitors refer to two or more air measurement instruments for the same parameter ( e.g., PM10 mass) operated at the same site location, and whose placement is consistent with part 53 of this chapter. For purposes of considering a combined site record in this appendix, when two or more monitors are operated at the same site, one Start Printed Page 16381 monitor is designated as the “primary” monitor with any additional monitors designated as “collocated.” It is implicit in these appendix procedures that the primary monitor and collocated monitor(s) are all reference or equivalent methods; however, it is not a requirement that the primary and collocated monitors utilize the same specific sampling and analysis method.
Combined site data record is the data set used for performing computations in this appendix and represents data for the primary monitors augmented with data from collocated monitors according to the procedure specified in section 3.0(a) of this appendix.
Daily value for PM10 refers to the 24-hour average concentration of PM10 calculated or measured from midnight to midnight (local time).
Exceedance means a daily value that is above the level of the 24-hour standard after rounding to the nearest 10 µg/m3 ( i.e., values ending in 5 or greater are to be rounded up).
Expected annual value is the number approached when the annual values from an increasing number of years are averaged, in the absence of long-term trends in emissions or meteorological conditions.
Primary monitors are suitable monitors designated by a State or local agency in their annual network plan as the default data source for creating a combined site data record. If there is only one suitable monitor at a particular site location, then it is presumed to be a primary monitor.
Year refers to a calendar year.
* * * * *2.3 Data Requirements
* * * * *(d) 24-hour average concentrations will be computed from submitted hourly PM10 concentration data for each corresponding day of the year and the result will be stored in the first, or start, hour ( i.e., midnight, hour `0') of the 24-hour period. A 24-hour average concentration shall be considered valid if at least 75 percent of the hourly averages ( i.e., 18 hourly values) for the 24-hour period are available. In the event that fewer than all 24 hourly average concentrations are available ( i.e., fewer than 24 but at least 18), the 24-hour average concentration shall be computed on the basis of the hours available using the number of available hours within the 24-hour period as the divisor ( e.g., the divisor is 19 if 19 hourly values are available). 24-hour periods with 7 or more missing hours shall also be considered for computations in this appendix if, after substituting zero for all missing hourly concentrations, the resulting 24-hour average daily value exceeds the level of the 24-hour standard specified in § 50.6 after rounding to the nearest 10 µg/m3 .
* * * * *3.0 Computational Equations for the 24-Hour Standards
(a) All computations shown in this appendix shall be implemented on a site-level basis. Site level concentration data shall be processed as follows:
(1) The default dataset for PM10 mass concentrations for a site shall consist of the measured concentrations recorded from the designated primary monitor(s). All daily values produced by the primary monitor are considered part of the site record.
(2) If a daily value is not produced by the primary monitor for a particular day, but a value is available from a single collocated monitor, then that collocated monitor value shall be considered part of the combined site data record. If daily value data is available from two or more collocated monitors, the average of those collocated values shall be used as the daily value. The data record resulting from this procedure is referred to as the “combined site data record.”
(b) In certain circumstances, including but not limited to site closures or relocations, data from two nearby sites may be combined into a single site data record for the purpose of calculating a valid design value. The appropriate Regional Administrator may approve such combinations if the Regional Administrator determines that the measured concentrations do not differ substantially between the two sites, taking into consideration factors such as distance between sites, spatial and temporal patterns in air quality, local emissions and meteorology, jurisdictional boundaries, and terrain features.
* * * * *Start Amendment Part4. Amend appendix L to part 50 by revising section 7.3.4 and adding section 7.3.4.5 to read as follows:
End Amendment PartAppendix L to Part 50—Reference Method for the Determination of Fine Particulate Matter as PM2. 5 in the Atmosphere
* * * * *7.3.4 Particle size separator. The sampler shall be configured with one of the three alternative particle size separators described in this section. One separator is an impactor-type separator (WINS impactor) described in sections 7.3.4.1, 7.3.4.2, and 7.3.4.3 of this appendix. One alternative separator is a cyclone-type separator (VSCCTM ) described in section 7.3.4.4 of this appendix. The other alternative separator is also a cyclone-type separator (TE–PM2.5 C) described in section 7.3.4.5 of this appendix.
* * * * *7.3.4.5 A second cyclone-type separator is identified as a Tisch TE–PM2.5 C Cyclone particle size separator specified as part of EPA-designated reference method RFPS–1014–219 and as manufactured by Tisch Environmental Incorporated, 145 S. Miami Avenue, Village of Cleves, Ohio 45002.
* * * * *Start Amendment Part5. Amend appendix N to part 50 by:
End Amendment Part Start Amendment Parta. In section 1.0 revising paragraph (a);
End Amendment Part Start Amendment Partb. In section 3.0 adding paragraph (d)(3);
End Amendment Part Start Amendment Partc. In section 4.1 revising paragraph (a); and
End Amendment Part Start Amendment Partd. In section 4.2 revising paragraph (a).
End Amendment PartThe addition and revisions read as follows.
Appendix N to Part 50—Interpretation of the National Ambient Air Quality Standards for PM2. 5
1.0 General
(a) This appendix explains the data handling conventions and computations necessary for determining when the national ambient air quality standards (NAAQS) for PM2.5 are met, specifically the primary and secondary annual and 24-hour PM2.5 NAAQS specified in §§ 50.7, 50.13, 50.18, and 50.20. PM2.5 is defined, in general terms, as particles with an aerodynamic diameter less than or equal to a nominal 2.5 micrometers. PM2.5 mass concentrations are measured in the ambient air by a Federal Reference Method (FRM) based on appendix L to this part, as applicable, and designated in accordance with part 53 of this chapter or by a Federal Equivalent Method (FEM) designated in accordance with part 53 of this chapter. Only those FRM and FEM measurements that are derived in accordance with part 58 of this chapter ( i.e., that are deemed “suitable”) shall be used in comparisons with the PM2.5 NAAQS. The data handling and computation procedures to be used to construct annual and 24-hour NAAQS metrics from reported PM2.5 mass concentrations, and the associated instructions for comparing these calculated metrics to the levels of the PM2.5 NAAQS, are specified in sections 2.0, 3.0, and 4.0 of this appendix.
* * * * *3.0 Requirements for Data Use and Data Reporting for Comparisons With the NAAQS for PM2. 5
* * * * *(d) * * *
(3) In certain circumstances, including but not limited to site closures or relocations, data from two nearby sites may be combined into a single site data record for the purpose of calculating a valid design value. The appropriate Regional Administrator may approve such site combinations if the Regional Administrator determines that the measured concentrations do not differ substantially between the two sites, taking into consideration factors such as distance between sites, spatial and temporal patterns in air quality, local emissions and meteorology, jurisdictional boundaries, and terrain features.
* * * * *4.1 Annual PM2. 5 NAAQS
(a) Levels of the primary and secondary annual PM2.5 NAAQS are specified in §§ 50.7, 50.13, 50.18, and 50.20 as applicable.
* * * * *4.2 Twenty-Four-Hour PM2. 5 NAAQS
(a) Levels of the primary and secondary 24-hour PM2.5 NAAQS are specified in §§ 50.7, 50.13, 50.18, and 50.20 as applicable.
* * * * *Start Part Start Printed Page 16382PART 53—AMBIENT AIR MONITORING REFERENCE AND EQUIVALENT METHODS
End Part Start Amendment Part6. The authority citation for part 53 continues to read as follows:
End Amendment PartSubpart A—General Provisions
Start Amendment Part7. Amend § 53.4 by:
End Amendment Part Start Amendment Parta. Revising paragraph (a);
End Amendment Part Start Amendment Partb. Adding paragraph (b)(7); and
End Amendment Part Start Amendment Partc. Revising paragraph (d).
End Amendment PartThe revisions and addition read as follows:
Start Amendment PartApplications for reference or equivalent method determinations.(a) Applications for FRM or FEM determinations and modification requests of existing designated instruments shall be submitted to: U.S. Environmental Protection Agency, Director, Center for Environmental Measurement and Modeling, Reference and Equivalent Methods Designation Program (MD–D205–03), 109 T.W. Alexander Drive, P.O. Box 12055, Research Triangle Park, North Carolina 27711 (commercial delivery address: 4930 Old Page Road, Durham, North Carolina 27703).
* * * * *(b) * * *
(7) All written materials for new FRM and FEM applications and modification requests must be submitted in English in MS Word format. For any calibration certificates originally written in a non-English language, the original non-English version of the certificate must be submitted to EPA along with a version of the certificate translated to English. All laboratory and field data associated with new FRM and FEM applications and modification requests must be submitted in MS Excel format. All worksheets in MS Excel must be unprotected to enable full inspection as part of the application review process.
* * * * *(d) For candidate reference or equivalent methods or for designated instruments that are the subject of a modification request, the applicant, if requested by EPA, shall provide to EPA a representative sampler or analyzer for test purposes. The sampler or analyzer shall be shipped free on board (FOB) destination to Director, Center for Environmental Measurements and Modeling, Reference and Equivalent Methods Designation Program (MD D205–03), U.S. Environmental Protection Agency, 4930 Old Page Road, Durham, North Carolina 27703, scheduled to arrive concurrently with or within 30 days of the arrival of the other application materials. This sampler or analyzer may be subjected to various tests that EPA determines to be necessary or appropriate under § 53.5(f), and such tests may include special tests not described in this part. If the instrument submitted under this paragraph (d) malfunctions, becomes inoperative, or fails to perform as represented in the application before the necessary EPA testing is completed, the applicant shall be afforded the opportunity to repair or replace the device at no cost to the EPA. Upon completion of EPA testing, the sampler or analyzer submitted under this paragraph (d) shall be repacked by EPA for return shipment to the applicant, using the same packing materials used for shipping the instrument to EPA unless alternative packing is provided by the applicant. Arrangements for, and the cost of, return shipment shall be the responsibility of the applicant. The EPA does not warrant or assume any liability for the condition of the sampler or analyzer upon return to the applicant.
8. Amend § 53.8 by revising paragraph (a) to read as follows:
End Amendment PartStart Amendment PartDesignation of reference and equivalent methods.(a) A candidate method determined by the Administrator to satisfy the applicable requirements of this part shall be designated as an FRM or FEM (as applicable) by and upon publication of the designation in the Federal Register . Applicants shall not publicly announce, market, or sell the candidate sampler and analyzer as an approved FRM or FEM (as applicable) until the designation is published in the Federal Register .
* * * * *9. Amend § 53.14 by revising paragraphs (c)(4), (5), and (6) to read as follows:
End Amendment PartStart Amendment PartModification of a reference or equivalent method.* * * * *(c) * * *
(4) Send notice to the applicant that additional information must be submitted before a determination can be made and specify the additional information that is needed (in such cases, the 90-day period shall commence upon receipt of the additional information).
(5) Send notice to the applicant that additional tests are necessary and specify which tests are necessary and how they shall be interpreted (in such cases, the 90-day period shall commence upon receipt of the additional test data).
(6) Send notice to the applicant that additional tests will be conducted by the Administrator and specify the reasons for and the nature of the additional tests (in such cases, the 90-day period shall commence 1 calendar day after the additional tests are completed).
* * * * *10. Revise table A–1 to subpart A of part 53 to read as follows:
End Amendment PartTable A–1 to Subpart A of Part 53—Summary of Applicable Requirements for Reference and Equivalent Methods for Air Monitoring of Criteria Pollutants
Pollutant Reference or equivalent Manual or automated Applicable appendix of part 50 of this chapter Applicable subparts of this part A B C D E F SO 2 Reference Manual A–2 Automated A–1 ✓ ✓ Equivalent Manual A–1 ✓ ✓ Automated A–1 ✓ ✓ ✓ CO Reference Automated C ✓ ✓ Equivalent Manual C ✓ ✓ Automated C ✓ ✓ ✓ O 3 Reference Automated D ✓ ✓ Equivalent Manual D ✓ ✓ Automated D ✓ ✓ ✓ NO 2 Reference Automated F ✓ ✓ Equivalent Manual F ✓ ✓ Automated F ✓ ✓ ✓ Start Printed Page 16383 Pb Reference Manual G Equivalent Manual G ✓ ✓ Automated G ✓ ✓ PM 10 -Pb Reference Manual Q Equivalent Manual Q ✓ ✓ Automated Q ✓ ✓ PM 10 Reference Manual J ✓ ✓ Equivalent Manual J ✓ ✓ ✓ Automated J ✓ ✓ ✓ PM 2.5 Reference Manual L ✓ ✓ Equivalent Class I Manual L ✓ ✓ ✓ Equivalent Class II Manual L 1 ✓ 2 ✓ ✓ 1 2 ✓ Equivalent Class III Automated L 1 ✓ ✓ ✓ 1 ✓ PM 10–2.5 Reference Manual L,2 O ✓ ✓ Equivalent Class I Manual L,2 O ✓ ✓ ✓ Equivalent Class II Manual L,2 O ✓ 2 ✓ ✓ 1,2 ✓ Equivalent Class III Automated 1 L, 1 2 O ✓ ✓ ✓ 1 ✓ 1 Some requirements may apply, based on the nature of each particular candidate method, as determined by the Administrator. 2 Alternative Class III requirements may be substituted. Subpart B—Procedures for Testing Performance Characteristics of Automated Methods for SO 2 , CO, O 3 , and NO 2
Start Amendment Part11. Amend table B–1 to subpart B of part 53 by revising footnote 4 to read as follows:
End Amendment PartTable B–1 to Subpart B of Part 53—Performance Limit Specifications for Automated Methods
* * * * *4 For nitric oxide interference for the SO2 ultraviolet fluorescence (UVF) method, interference equivalent is ±0.003 ppm for the lower range.
* * * * *Start Amendment Part12. Revise table B–3 to subpart B of part 53 to read as follows: Start Printed Page 16384
End Amendment PartStart Printed Page 16385 Start Amendment PartTable B–3 to Subpart B of Part 53—Interferent Test Concentration 1
[Parts per million]
Pollutant Analyzer type 2 Hydro-chloric acid Ammonia Hydrogen sulfide Sulfur dioxide Nitrogen dioxide Nitric oxide Carbon dioxide Ethylene Ozone M-xylene Water vapor Carbon monoxide Methane Ethane Naphthalene SO 2 Ultraviolet fluorescence 5 0.1 4 0.14 0.5 0.5 0.5 0.2 20,000 6 0.05 SO 2 Flame photometric 0.01 4 0.14 750 3 20,000 50 SO 2 Gas chromatography 0.1 4 0.14 750 3 20,000 50 SO 2 Spectrophotometric-wet chemical (pararosanaline) 0.2 0.1 0.1 4 0.14 0.5 750 0.5 SO 2 Electrochemical 0.2 0.1 0.1 4 0.14 0.5 0.5 0.2 0.5 3 20,000 SO 2 Conductivity 0.2 0.1 4 0.14 0.5 750 SO 2 Spectrophotometric-gas phase, including DOAS 4 0.14 0.5 0.5 0.5 0.2 O 3 Ethylene Chemiluminescence 3 0.1 750 4 0.08 3 20,000 O 3 NO-chemiluminescence 3 0.1 0.5 750 4 0.08 3 20,000 O 3 Electrochemical 3 0.1 0.5 0.5 4 0.08 3 20,000 O 3 Spectrophotometric-wet chemical (potassium iodide) 3 0.1 0.5 0.5 3 0.5 4 0.08 O 3 Spectrophotometric-gas phase, including ultraviolet absorption and DOAS 0.5 0.5 3 0.5 4 0.08 0.02 20,000 CO Non-dispersive Infrared 750 20,000 4 10 CO Gas chromatography with flame ionization detector 20,000 4 10 0.5 CO Electrochemical 0.5 0.2 20,000 4 10 CO Catalytic combustion-thermal detection 0.1 750 0.2 20,000 4 10 5.0 0.5 CO IR fluorescence 750 20,000 4 10 0.5 CO Mercury replacement-UV photometric 0.2 4 10 0.5 NO 2 Chemiluminescent 3 0.1 0.5 4 0.1 0.5 20,000 NO 2 Spectrophotometric-wet chemical (azo-dye reaction) 0.5 4 0.1 0.5 750 0.5 NO 2 Electrochemical 0.2 3 0.1 0.5 4 0.1 0.5 750 0.5 20,000 50 NO 2 Spectrophotometric-gas phase 3 0.1 0.5 4 0.1 0.5 0.5 20,000 50 1 Concentrations of interferent listed must be prepared and controlled to ±10 percent of the stated value. 2 Analyzer types not listed will be considered by the Administrator as special cases. 3 Do not mix interferent with the pollutant. 4 Concentration of pollutant used for test. These pollutant concentrations must be prepared to ±10 percent of the stated value. 5 If candidate method utilizes an elevated-temperature scrubber for removal of aromatic hydrocarbons, perform this interference test. 6 If naphthalene test concentration cannot be accurately quantified, remove the scrubber, use a test concentration that causes a full-scale response, reattach the scrubber, and evaluate response for interference. 13. Amend appendix A to subpart B of part 53 by revising figures B–3 and B–5 to read as follows:
End Amendment PartAppendix A to Subpart B of Part 53—Optional Forms for Reporting Test Results
* * * * *Figure B–3 to Appendix A to Subpart B of Part 53—Form for Test Data and Calculations for Lower Detectable Limit (LDL) and Interference Equivalent (IE) (see § 53.23(c) and (d))
LDL Interference Test Data
Applicant
Analyzer
Date
Pollutant
 * * * * *
* * * * *Figure B–5 to Appendix A to Subpart B of Part 53—Form for Calculating Zero Drift, Span Drift and Precision (see § 53.23(e))
Calculation of Zero Drift, Span Drift, and Precision
Applicant
Analyzer
Date
Pollutant
Start Printed Page 16386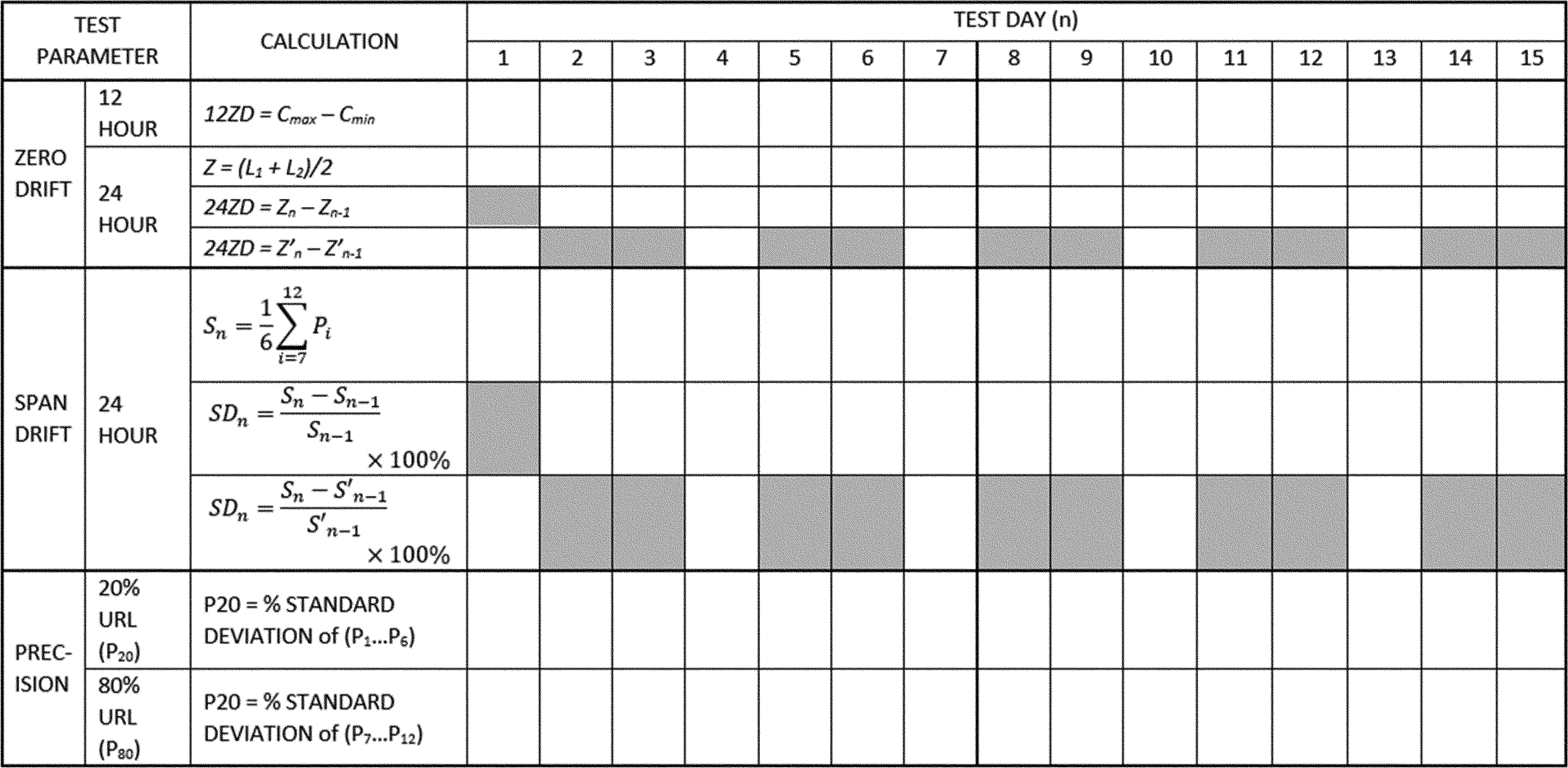 * * * * *
* * * * *Subpart C—Procedures for Determining Comparability Between Candidate Methods and Reference Methods
Start Amendment Part14. Amend § 53.35 by revising paragraph (b)(1)(ii)(D) to read as follows:
End Amendment PartStart Amendment PartTest procedure for Class II and Class III methods for PM 2.5 and PM 10−2.5 .* * * * *(b) * * *
(1) * * *
(ii) * * *
(D) Site D shall be in a large city east of the Mississippi River, having characteristically high humidity levels.
* * * * *15. Revise table C–4 to subpart C of part 53 to read as follows:
End Amendment PartStart Printed Page 16387Table C–4 to Subpart C of Part 53—Test Specifications for PM 10 , PM 2.5 , and PM 10–2.5 Candidate Equivalent Methods
Specification PM 10 PM 2.5 PM 10–2.5 Class I Class II Class III Class II Class III Acceptable concentration range (R j ), µg/m3 5–300 3–200 3–200 3–200 3–200 3–200. Minimum number of test sites 2 1 2 4 2 4. Minimum number of candidate method samplers or analyzers per site 3 3 31 31 31 3.1 Number of reference method samplers per site 3 3 31 31 31 3.1 Minimum number of acceptable sample sets per site for PM 10 methods: R j < 20 µg/m3 3 R j > 20 µg/m3 3 Total 10 Minimum number of acceptable sample sets per site for PM 2.5 and PM 10–2.5 candidate equivalent methods: R j < 15 µg/m3 for 24-hr or R j < 8 µg/m3 for 48-hr samples. 3 3 3 3 3. Rj > 15 µg/m3 for 24-hr or R j > 8 µg/m3 for 48-hr samples 3 3 3 3 3. Each season 10 23 23 23 23. Total, each site 10 23 23 (46 for two-season sites) 23 23 (46 for two-season sites). Precision of replicate reference method measurements, P Rj or RP Rj , respectively; RP for Class II or III PM 2.5 or PM 10–2.5 , maximum 5 μg/m3 or 7%. 2 μg/m3 or 5%. 10%2 10%2 10%2 10%.2 Precision of PM 2.5 or PM 10–2.5 candidate method, CP, each site 10%2 15%2 15%2 15%.2 Slope of regression relationship 1 ±0.10 1 ±0.05 1 ±0.10 1 ±0.10 1 ±0.10 1 ±0.12. Intercept of regression relationship, µg/m3 0 ±5 0 ±1 Between: 13.55—(15.05 × slope), but not less than—1.5; and 16.56—(15.05 × slope), but not more than +1.5 Between: 15.05—(17.32 × slope), but not less than—2.0; and 15.05—(13.20 × slope), but not more than +2.0 Between: 62.05—(70.5 × slope), but not less than—3.5; and 78.95—(70.5 × slope), but not more than +3.5 Between: 70.50—(82.93 × slope), but not less than—7.0; and 70.50—(61.16 × slope), but not more than +7.0. Correlation of reference method and candidate method measurements ≥ 0.97 ≥ 0.97 ≥ 0.93—for CCV ≤ 0.4; ≥ 0.85 + 0.2 × CCV—for 0.4 ≤ CCV ≤ 0.5; ≥ 0.95—for CCV ≥ 0.5 1 Some missing daily measurement values may be permitted; see test procedure. 2 Calculated as the root mean square over all measurement sets. Subpart D—Procedures for Testing Performance Characteristics of Methods for PM 10
Start Amendment Part16. Amend § 53.43 by revising the formula in paragraph (a)(2)(xvi) and the formula in paragraph (c)(2)(iv) to read as follows:
End Amendment PartTest procedures.(a) * * *
(2) * * *
(xvi) * * *
 * * * * *
* * * * *(c) * * *
(2) * * *
(iv) * * *

if C ̄j is below 80 µg/m3 , or

if C ̄j is above 80 µg/m3 .
Subpart E—Procedures for Testing Physical (Design) and Performance Characteristics of Reference Methods and Class I and Class II Equivalent Methods for PM 2.5 or PM 10 –2.5
Start Amendment Part17. Amend § 53.51 by revising paragraph (d)(2) to read as follows:
End Amendment PartDemonstration of compliance with design specifications and manufacturing and test requirements.* * * * *(d) * * *
(2) VSCC and TE–PM2.5C separators. For samplers and monitors utilizing the BGI VSCC or Tisch TE–PM2.5 C particle size separators specified in sections 7.3.4.4 and 7.3.4.5 of appendix L to part 50 of this chapter, respectively, the respective manufacturers shall identify the critical dimensions and manufacturing tolerances for the separator, devise appropriate test procedures to verify that the critical dimensions and tolerances are maintained during the manufacturing process, and carry out those procedures on each separator manufactured to verify conformance of the manufactured products. The manufacturer shall also maintain records of these tests and their test results and submit evidence that this procedure is incorporated into the manufacturing procedure, that the test is or will be routinely implemented, and that an appropriate procedure is in place for the disposition of units that fail this tolerance tests.
* * * * *Subpart F—Procedures for Testing Performance Characteristics of Class II Equivalent Methods for PM 2.5
Start Amendment Part18. Amend § 53.61 by revising paragraph (g) introductory text, the first sentence of paragraph (g)(1), the first sentence of (g)(1)(i), (g)(2)(i) and adding paragraph (g)(2)(iii) to read as follows:
End Amendment PartStart PartTest conditions.* * * * *(g) Vibrating Orifice Aerosol Generator (VOAG) and Flow-Focusing Monodisperse Aerosol Generator (FMAG) conventions. This section prescribes conventions regarding the use of the vibrating orifice aerosol generator (VOAG) and the flow-focusing monodisperse aerosol generator (FMAG) for the size-selective performance tests outlined in §§ 53.62, 53.63, 53.64, and 53.65.
(1) Particle aerodynamic diameter. The VOAG and FMAG produce near-monodisperse droplets through the controlled breakup of a liquid jet. * * *
(i) The physical diameter of a generated spherical particle can be calculated from the operational parameters of the VOAG and FMAG as:
* * * * *(2) * * *
(i) Solid particle tests performed in this subpart shall be conducted using particles composed of ammonium fluorescein. For use in the VOAG or FMAG, liquid solutions of known volumetric concentration can be prepared by diluting fluorescein powder (C2 OH12 O5, FW = 332.31, CAS 2321–07–5) with aqueous ammonia. Guidelines for preparation of fluorescein solutions of the desired volume concentration (Cvol ) are presented in Vanderpool and Rubow (1988) (Reference 2 in appendix A to this subpart). For purposes of converting particle physical diameter to aerodynamic diameter, an ammonium fluorescein particle density of 1.35 g/cm3 shall be used.
* * * * *(iii) Calculation of the physical diameter of the particles produced by the VOAG and FMAG requires Start Printed Page 16388 knowledge of the liquid solution's volume concentration (Cvol). Because uranine is essentially insoluble in oleic acid, the total particle volume is the sum of the oleic acid volume and the uranine volume. The volume concentration of the liquid solution shall be calculated as:

Where:
Vu = uranine volume, ml;
Voleic = oleic acid volume, ml;
Vsol = total solution volume, ml;
Mu = uranine mass, g;
Pu = uranine density, g/cm3 ;
Moleic = oleic acid mass, g; and
Poleic = oleic acid density, g/cm3 .
* * * * *PART 58—AMBIENT AIR QUALITY SURVEILLANCE
End Part Start Amendment Part19. The authority citation for part 58 continues to read as follows:
End Amendment PartSubpart A—General Provisions
Start Amendment Part20. Amend § 58.1 by:
End Amendment Part Start Amendment Parta. Removing the definition for “Approved regional method (ARM)”; and
End Amendment Part Start Amendment Partb. Revising the definition for “Traceable.”
End Amendment PartThe revision reads as follows:
Definitions.* * * * *Traceable means a measurement result from a local standard whereby the result can be related to the International System of Units (SI) through a documented unbroken chain of calibrations, each contributing to the measurement uncertainty. Traceable measurement results must be compared and certified, either directly or via not more than one intermediate standard, to a National Institute of Standards and Technology (NIST)-certified reference standard. Examples include but are not limited to NIST Standard Reference Material (SRM), NIST-traceable Reference Material (NTRM), or a NIST-certified Research Gas Mixture (RGM). Traceability to the SI through other National Metrology Institutes (NMIs) in addition to NIST is allowed if a Declaration of Equivalence (DoE) exists between NIST and that NMI.
* * * * *Subpart B—Monitoring Network
Start Amendment Part21. Amend § 58.10 by:
End Amendment Part Start Amendment Parta. Revising paragraphs (a)(1) and (b)(10) and (13);
End Amendment Part Start Amendment Partb. Adding paragraph (b)(14); and
End Amendment Part Start Amendment Partc. Revising paragraph (d).
End Amendment PartThe revisions and addition read as follows:
Start Amendment PartAnnual monitoring network plan and periodic network assessment.(a)(1) Beginning July 1, 2007, the State, or where applicable local, agency shall submit to the Regional Administrator an annual monitoring network plan which shall provide for the documentation of the establishment and maintenance of an air quality surveillance system that consists of a network of SLAMS monitoring stations that can include FRM and FEM monitors that are part of SLAMS, NCore, CSN, PAMS, and SPM stations. The plan shall include a statement of whether the operation of each monitor meets the requirements of appendices A, B, C, D, and E to this part, where applicable. The Regional Administrator may require additional information in support of this statement. The annual monitoring network plan must be made available for public inspection and comment for at least 30 days prior to submission to the EPA and the submitted plan shall include and address, as appropriate, any received comments.
* * * * *(b) * * *
(10) Any monitors for which a waiver has been requested or granted by the EPA Regional Administrator as allowed for under appendix D or appendix E to this part. For those monitors where a waiver has been approved, the annual monitoring network plan shall include the date the waiver was approved.
* * * * *(13) The identification of any PM2.5 FEMs used in the monitoring agency's network where the data are not of sufficient quality such that data are not to be compared to the national ambient air quality standards (NAAQS). For required SLAMS where the agency identifies that the PM2.5 Class III FEM does not produce data of sufficient quality for comparison to the NAAQS, the monitoring agency must ensure that an operating FRM or filter-based FEM meeting the sample frequency requirements described in § 58.12 or other Class III PM2.5 FEM with data of sufficient quality is operating and reporting data to meet the network design criteria described in appendix D to this part.
(14) The identification of any site(s) intended to address being sited in an at-risk community where there are anticipated effects from sources in the area as required in section 4.7.1(b)(3) of appendix D to this part. An initial approach to the question of whether any new or moved sites are needed and to identify the communities in which they intend to add monitoring for meeting the requirement in this paragraph (b)(14), if applicable, shall be submitted in accordance with the requirements of section 4.7.1(b)(3) of appendix D to this part, which includes submission to the EPA Regional Administrator no later than July 1, 2024. Specifics on the resulting proposed new or moved sites for PM2.5 network design to address at-risk communities, if applicable, would need to be detailed in annual monitoring network plans due to each applicable EPA Regional office no later than July 1, 2025. The plan shall provide for any required sites to be operational no later than 24 months from date of approval of a plan or January 1, 2027, whichever comes first.
* * * * *(d) The State, or where applicable local, agency shall perform and submit to the EPA Regional Administrator an assessment of the air quality surveillance system every 5 years to determine, at a minimum, if the network meets the monitoring objectives defined in appendix D to this part, whether new sites are needed, whether existing sites are no longer needed and can be terminated, and whether new technologies are appropriate for incorporation into the ambient air monitoring network. The network assessment must consider the ability of existing and proposed sites to support air quality characterization for areas with relatively high populations of Start Printed Page 16389 susceptible individuals ( e.g., children with asthma) and other at-risk populations, and, for any sites that are being proposed for discontinuance, the effect on data users other than the agency itself, such as nearby States and Tribes or health effects studies. The State, or where applicable local, agency must submit a copy of this 5-year assessment, along with a revised annual network plan, to the Regional Administrator. The assessments are due every 5 years beginning July 1, 2010.
* * * * *22. Amend § 58.11 by revising paragraphs (a)(2) and (e) to read as follows:
End Amendment PartStart Amendment PartNetwork technical requirements.(a) * * *
(2) Beginning January 1, 2009, State and local governments shall follow the quality assurance criteria contained in appendix A to this part that apply to SPM sites when operating any SPM site which uses an FRM or an FEM and meets the requirements of appendix E to this part, unless the Regional Administrator approves an alternative to the requirements of appendix A with respect to such SPM sites because meeting those requirements would be physically and/or financially impractical due to physical conditions at the monitoring site and the requirements are not essential to achieving the intended data objectives of the SPM site. Alternatives to the requirements of appendix A may be approved for an SPM site as part of the approval of the annual monitoring plan, or separately.
* * * * *(e) State and local governments must assess data from Class III PM2.5 FEM monitors operated within their network using the performance criteria described in table C–4 to subpart C of part 53 of this chapter, for cases where the data are identified as not of sufficient comparability to a collocated FRM, and the monitoring agency requests that the FEM data should not be used in comparison to the NAAQS. These assessments are required in the monitoring agency's annual monitoring network plan described in § 58.10(b) for cases where the FEM is identified as not of sufficient comparability to a collocated FRM. For these collocated PM2.5 monitors, the performance criteria apply with the following additional provisions:
(1) The acceptable concentration range (Rj), µg/m3 may include values down to 0 µg/m3 .
(2) The minimum number of test sites shall be at least one; however, the number of test sites will generally include all locations within an agency's network with collocated FRMs and FEMs.
(3) The minimum number of methods shall include at least one FRM and at least one FEM.
(4) Since multiple FRMs and FEMs may not be present at each site, the precision statistic requirement does not apply, even if precision data are available.
(5) All seasons must be covered with no more than 36 consecutive months of data in total aggregated together.
(6) The key statistical metric to include in an assessment is the bias (both additive and multiplicative) of the PM2.5 continuous FEM(s) compared to a collocated FRM(s). Correlation is required to be reported in the assessment, but failure to meet the correlation criteria, by itself, is not cause to exclude data from a continuous FEM monitor.
23. Amend § 58.12 by revising paragraph (d)(1):
End Amendment PartStart Amendment PartOperating schedules.* * * * *(d) * * *
(1)(i) Manual PM2.5 samplers at required SLAMS stations without a collocated continuously operating PM2.5 monitor must operate on at least a 1-in-3 day schedule unless a waiver for an alternative schedule has been approved per paragraph (d)(1)(ii) of this section.
(ii) For SLAMS PM2.5 sites with both manual and continuous PM2.5 monitors operating, the monitoring agency may request approval for a reduction to 1-in-6 day PM2.5 sampling or for seasonal sampling from the EPA Regional Administrator. Other requests for a reduction to 1-in-6 day PM2.5 sampling or for seasonal sampling may be approved on a case-by-case basis. The EPA Regional Administrator may grant sampling frequency reductions after consideration of factors (including but not limited to the historical PM2.5 data quality assessments, the location of current PM2.5 design value sites, and their regulatory data needs) if the Regional Administrator determines that the reduction in sampling frequency will not compromise data needed for implementation of the NAAQS. Required SLAMS stations whose measurements determine the design value for their area and that are within plus or minus 10 percent of the annual NAAQS, and all required sites where one or more 24-hour values have exceeded the 24-hour NAAQS each year for a consecutive period of at least 3 years are required to maintain at least a 1-in-3 day sampling frequency until the design value no longer meets the criteria in this paragraph (d)(1)(ii) for 3 consecutive years. A continuously operating FEM PM2.5 monitor satisfies the requirement in this paragraph (d)(1)(ii) unless it is identified in the monitoring agency's annual monitoring network plan as not appropriate for comparison to the NAAQS and the EPA Regional Administrator has approved that the data from that monitor may be excluded from comparison to the NAAQS.
(iii) Required SLAMS stations whose measurements determine the 24-hour design value for their area and whose data are within plus or minus 5 percent of the level of the 24-hour PM2.5 NAAQS must have an FRM or FEM operate on a daily schedule if that area's design value for the annual NAAQS is less than the level of the annual PM2.5 standard. A continuously operating FEM or PM2.5 monitor satisfies the requirement in this paragraph (d)(1)(iii) unless it is identified in the monitoring agency's annual monitoring network plan as not appropriate for comparison to the NAAQS and the EPA Regional Administrator has approved that the data from that monitor may be excluded from comparison to the NAAQS. The daily schedule must be maintained until the referenced design values no longer meets the criteria in this paragraph (d)(1)(iii) for 3 consecutive years.
(iv) Changes in sampling frequency attributable to changes in design values shall be implemented no later than January 1 of the calendar year following the certification of such data as described in § 58.15.
* * * * *24. Revise § 58.15 to read as follows:
End Amendment PartAnnual air monitoring data certification.(a) The State, or where appropriate local, agency shall submit to the EPA Regional Administrator an annual air monitoring data certification letter to certify data collected by FRM and FEM monitors at SLAMS and SPM sites that meet criteria in appendix A to this part from January 1 to December 31 of the previous year. The head official in each monitoring agency, or his or her designee, shall certify that the previous year of ambient concentration and quality assurance data are completely submitted to AQS and that the ambient concentration data are accurate to the best of her or his knowledge, taking into consideration the quality assurance findings. The annual data certification letter is due by May 1 of each year.
(b) Along with each certification letter, the State shall submit to the Regional Administrator an annual Start Printed Page 16390 summary report of all the ambient air quality data collected by FRM and FEM monitors at SLAMS and SPM sites. The annual report(s) shall be submitted for data collected from January 1 to December 31 of the previous year. The annual summary serves as the record of the specific data that is the object of the certification letter.
(c) Along with each certification letter, the State shall submit to the Regional Administrator a summary of the precision and accuracy data for all ambient air quality data collected by FRM and FEM monitors at SLAMS and SPM sites. The summary of precision and accuracy shall be submitted for data collected from January 1 to December 31 of the previous year.
Subpart C—Special Purpose Monitors
Start Amendment Part25. Amend § 58.20 by revising paragraphs (b) through (e) to read as follows:
End Amendment PartStart Amendment PartSpecial purpose monitors (SPM).* * * * *(b) Any SPM data collected by an air monitoring agency using a Federal reference method (FRM) or Federal equivalent method (FEM) must meet the requirements of §§ 58.11 and 58.12 and appendix A to this part or an approved alternative to appendix A. Compliance with appendix E to this part is optional but encouraged except when the monitoring agency's data objectives are inconsistent with the requirements in appendix E. Data collected at an SPM using a FRM or FEM meeting the requirements of appendix A must be submitted to AQS according to the requirements of § 58.16. Data collected by other SPMs may be submitted. The monitoring agency must also submit to AQS an indication of whether each SPM reporting data to AQS monitor meets the requirements of appendices A and E.
(c) All data from an SPM using an FRM or FEM which has operated for more than 24 months are eligible for comparison to the relevant NAAQS, subject to the conditions of §§ 58.11(e) and 58.30, unless the air monitoring agency demonstrates that the data came from a particular period during which the requirements of appendix A, appendix C, or appendix E to this part were not met, subject to review and EPA Regional Office approval as part of the annual monitoring network plan described in § 58.10.
(d) If an SPM using an FRM or FEM is discontinued within 24 months of start-up, the Administrator will not base a NAAQS violation determination for the PM2.5 or ozone NAAQS solely on data from the SPM.
(e) If an SPM using an FRM or FEM is discontinued within 24 months of start-up, the Administrator will not designate an area as nonattainment for the CO, SO2, NO2, or 24-hour PM10 NAAQS solely on the basis of data from the SPM. Such data are eligible for use in determinations of whether a nonattainment area has attained one of these NAAQS.
* * * * *26. Amend appendix A to part 58 by:
End Amendment Part Start Amendment Parta. Revising section 2.6.1 and adding sections 2.6.1.1 and 2.6.1.2;
End Amendment Part Start Amendment Partb. Removing section 3.1.2.2 and redesignating sections 3.1.2.3, 3.1.2.4, 3.1.2.5, and 3.1.2.6 as sections 3.1.2.2, 3.1.2.3, 3.1.2.4, and 3.1.2.5, respectively;
End Amendment Part Start Amendment Partc. Revising sections 3.1.3.3, 3.2.4, 4.2.1, and 4.2.5; and
End Amendment Part Start Amendment Partd. In section 6 revising References (1), (4), (6), (7), (9), (10), and (11) and table A–1.
End Amendment PartThe revisions and additions read as follows:
Appendix A to Part 58—Quality Assurance Requirements for Monitors used in Evaluations of National Ambient Air Quality Standards
* * * * *2.6.1 Gaseous pollutant concentration standards (permeation devices or cylinders of compressed gas) used to obtain test concentrations for CO, SO2, NO, and NO2 must be EPA Protocol Gases certified in accordance with one of the procedures given in Reference 4 of this appendix.
2.6.1.1 The concentrations of EPA Protocol Gas standards used for ambient air monitoring must be certified with a 95-percent confidence interval to have an analytical uncertainty of no more than ±2.0 percent (inclusive) of the certified concentration (tag value) of the gas mixture. The uncertainty must be calculated in accordance with the statistical procedures defined in Reference 4 of this appendix.
2.6.1.2 Specialty gas producers advertising certification with the procedures provided in Reference 4 of this appendix and distributing gases as “EPA Protocol Gas” for ambient air monitoring purposes must adhere to the regulatory requirements specified in 40 CFR 75.21(g) or not use “EPA” in any form of advertising. Monitoring organizations must provide information to the EPA on the specialty gas producers they use on an annual basis. PQAOs, when requested by the EPA, must participate in the EPA Ambient Air Protocol Gas Verification Program at least once every 5 years by sending a new unused standard to a designated verification laboratory.
* * * * *3.1.3.3 Using audit gases that are verified against the NIST standard reference methods or special review procedures and validated per the certification periods specified in Reference 4 of this appendix (EPA Traceability Protocol for Assay and Certification of Gaseous Calibration Standards) for CO, SO2, and NO2 and using O3 analyzers that are verified quarterly against a standard reference photometer.
* * * * *3.2.4 PM2.5 Performance Evaluation Program (PEP) Procedures. The PEP is an independent assessment used to estimate total measurement system bias. These evaluations will be performed under the national performance evaluation program (NPEP) as described in section 2.4 of this appendix or a comparable program. A prescribed number of Performance evaluation sampling events will be performed annually within each PQAO. For PQAOs with less than or equal to five monitoring sites, five valid performance evaluation audits must be collected and reported each year. For PQAOs with greater than five monitoring sites, eight valid performance evaluation audits must be collected and reported each year. A valid performance evaluation audit means that both the primary monitor and PEP audit concentrations are valid and equal to or greater than 2 µg/m3. Siting of the PEP monitor must be consistent with section 3.2.3.4(c) of this appendix. However, any horizontal distance greater than 4 meters and any vertical distance greater than one meter must be reported to the EPA regional PEP coordinator. Additionally for every monitor designated as a primary monitor, a primary quality assurance organization must:
* * * * *4.2.1 Collocated Quality Control Sampler Precision Estimate for PM10, PM2.5, and Pb. Precision is estimated via duplicate measurements from collocated samplers. It is recommended that the precision be aggregated at the PQAO level quarterly, annually, and at the 3-year level. The data pair would only be considered valid if both concentrations are greater than or equal to the minimum values specified in section 4(c) of this appendix. For each collocated data pair, calculate ti, using equation 6 to this appendix:
Start Printed Page 16391
Where Xi is the concentration from the primary sampler and Yi is the concentration value from the audit sampler. The coefficient of variation upper bound is calculated using equation 7 to this appendix:

Where k is the number of valid data pairs being aggregated, and X20.1,k-1 is the 10th percentile of a chi-squared distribution with k-1 degrees of freedom. The factor of 2 in the denominator adjusts for the fact that each ti is calculated from two values with error.
* * * * *4.2.5 Performance Evaluation Programs Bias Estimate for PM2.5 . The bias estimate is calculated using the PEP audits described in section 3.2.4. of this appendix. The bias estimator is based on, si, the absolute difference in concentrations divided by the square root of the PEP concentration.
 * * * * *
* * * * *6. References
(1) American National Standard Institute—Quality Management Systems For Environmental Information And Technology Programs—Requirements With Guidance For Use. ASQ/ANSI E4–2014. February 2014. Available from ANSI Webstore https://webstore.ansi.org/.
* * * * *(4) EPA Traceability Protocol for Assay and Certification of Gaseous Calibration Standards. EPA–600/R–12/531. May, 2012. Available from U.S. Environmental Protection Agency, National Risk Management Research Laboratory, Research Triangle Park NC 27711. https://www.epa.gov/nscep.
* * * * *(6) List of Designated Reference and Equivalent Methods. Available from U.S. Environmental Protection Agency, Center for Environmental Measurements and Modeling, Air Methods and Characterization Division, MD–D205–03, Research Triangle Park, NC 27711. https://www.epa.gov/amtic/air-monitoring-methods-criteria-pollutants.
(7) Transfer Standards for the Calibration of Ambient Air Monitoring Analyzers for Ozone. EPA–454/B–13–004 U.S. Environmental Protection Agency, Research Triangle Park, NC 27711, October, 2013. https://www.epa.gov/sites/default/files/2020-09/documents/ozonetransferstandardguidance.pdf.
* * * * *(9) Quality Assurance Handbook for Air Pollution Measurement Systems, Volume 1—A Field Guide to Environmental Quality Assurance. EPA–600/R–94/038a. April 1994. Available from U.S. Environmental Protection Agency, ORD Publications Office, Center for Environmental Research Information (CERI), 26 W. Martin Luther King Drive, Cincinnati, OH 45268. https://www.epa.gov/amtic/ambient-air-monitoring-quality-assurance#documents.
(10) Quality Assurance Handbook for Air Pollution Measurement Systems, Volume II: Ambient Air Quality Monitoring Program Quality System Development. EPA–454/B–13–003. https://www.epa.gov/amtic/ambient-air-monitoring-quality-assurance#documents.
(11) National Performance Evaluation Program Standard Operating Procedures. https://www.epa.gov/amtic/ambient-air-monitoring-quality-assurance#npep.
Table A–1 to Section 6 of Appendix A—Minimum Data Assessment Requirements for NAAQS Related Criteria Pollutant Monitors
Method Assessment method Coverage Minimum frequency Parameters reported AQS assessment type Gaseous Methods (CO, NO 2 , SO 2 , O 3 ): Start Printed Page 16392 One-Point QC for SO 2 , NO 2 , O 3 , CO Response check at concentration 0.005–0.08 ppm SO 2 , NO 2 , O 3 , and 0.5 and 5 ppm CO Each analyzer Once per 2 weeks 5 Audit concentration 1 and measured concentration.2 One-Point QC. Annual performance evaluation for SO 2 , NO 2 , O 3 , CO See section 3.1.2 of this appendix Each analyzer Once per year Audit concentration 1 and measured concentration 2 for each level Annual PE. NPAP for SO 2 , NO 2 , O 3 , CO Independent Audit 20% of sites each year Once per year Audit concentration1 and measured concentration 2 for each level NPAP. Particulate Methods: Continuous 4 method—collocated quality control sampling PM 2.5 Collocated samplers 15% 1-in-12 days Primary sampler concentration and duplicate sampler concentration.3 No Transaction reported as raw data. Manual method—collocated quality control sampling PM 10 , PM 2.5 , Pb-TSP, Pb-PM 10 Collocated samplers 15% 1-in-12 days Primary sampler concentration and duplicate sampler concentration.3 No Transaction reported as raw data. Flow rate verification PM 10 (low Vol) PM 2.5 , Pb-PM 10 Check of sampler flow rate Each sampler Once every month 5 Audit flow rate and measured flow rate indicated by the sampler Flow Rate Verification. Flow rate verification PM 10 (High-Vol), Pb-TSP Check of sampler flow rate Each sampler Once every quarter 5 Audit flow rate and measured flow rate indicated by the sampler Flow Rate Verification. Semi-annual flow rate audit PM 10 , TSP, PM 10 –2.5, PM 2.5 , Pb-TSP, Pb-PM 10 Check of sampler flow rate using independent standard Each sampler Once every 6 months 5 Audit flow rate and measured flow rate indicated by the sampler Semi Annual Flow Rate Audit. Pb analysis audits Pb-TSP, Pb-PM 10 Check of analytical system with Pb audit strips/filters Analytical Once each quarter 5 Measured value and audit value (ug Pb/filter) using AQS unit code 077 Pb Analysis Audits. Performance Evaluation Program PM 2.5 Collocated samplers (1) 5 valid audits for primary QA orgs, with ≤5 sites (2) 8 valid audits for primary QA orgs, with >5 sites (3) All samplers in 6 years Distributed over all 4 quarters 5 Primary sampler concentration and performance evaluation sampler concentration PEP. Performance Evaluation Program Pb-TSP, Pb-PM 10 Collocated samplers (1) 1 valid audit and 4 collocated samples for primary QA orgs, with ≤5 sites (2) 2 valid audits and 6 collocated samples for primary QA orgs with >5 sites Distributed over all 4 quarters 5 Primary sampler concentration and performance evaluation sampler concentration. Primary sampler concentration and duplicate sampler concentration PEP. 1 Effective concentration for open path analyzers. 2 Corrected concentration, if applicable for open path analyzers. 3 Both primary and collocated sampler values are reported as raw data. 4 PM 2.5 is the only particulate criteria pollutant requiring collocation of continuous and manual primary monitors. 5 EPA's recommended maximum number of days that should exist between checks to ensure that the checks are routinely conducted over time and to limit data impacts resulting from a failed check. * * * * *Start Amendment Part27. Amend appendix B to part 58 by:
End Amendment Part Start Amendment Parta. Revising section 2.6.1 and adding sections 2.6.1.1 and 2.6.1.2;
End Amendment Part Start Amendment Partb. Removing and reserving section 3.1.2.2; Start Printed Page 16393
End Amendment Part Start Amendment Partc. Revising sections 3.1.3.3 and 3.2.4;
End Amendment Part Start Amendment Partd. Adding sections 3.2.4.1 through 3.2.4.3;
End Amendment Part Start Amendment Parte. Revising sections 4.2.1, and 4.2.5; and
End Amendment Part Start Amendment Partf. In section 6 revising References (1), (4), (6), (7), (9), (10), and (11) and table B–1.
End Amendment PartThe revisions and additions read as follows:
Appendix B to Part 58—Quality Assurance Requirements for Prevention of Significant Deterioration (PSD) Air Monitoring
* * * * *2.6.1 Gaseous pollutant concentration standards (permeation devices or cylinders of compressed gas) used to obtain test concentrations for CO, SO2, NO, and NO2 must be EPA Protocol Gases certified in accordance with one of the procedures given in Reference 4 of this appendix.
2.6.1.1 The concentrations of EPA Protocol Gas standards used for ambient air monitoring must be certified with a 95-percent confidence interval to have an analytical uncertainty of no more than ±2.0 percent (inclusive) of the certified concentration (tag value) of the gas mixture. The uncertainty must be calculated in accordance with the statistical procedures defined in Reference 4 of this appendix.
2.6.1.2 Specialty gas producers advertising certification with the procedures provided in Reference 4 of this appendix and distributing gases as “EPA Protocol Gas” for ambient air monitoring purposes must adhere to the regulatory requirements specified in 40 CFR 75.21(g) or not use “EPA” in any form of advertising. The PSD PQAOs must provide information to the PSD reviewing authority on the specialty gas producers they use (or will use) for the duration of the PSD monitoring project. This information can be provided in the QAPP or monitoring plan but must be updated if there is a change in the specialty gas producers used.
* * * * *3.1.3.3 Using audit gases that are verified against the NIST standard reference methods or special review procedures and validated per the certification periods specified in Reference 4 of this appendix (EPA Traceability Protocol for Assay and Certification of Gaseous Calibration Standards) for CO, SO2, and NO2 and using O3 analyzers that are verified quarterly against a standard reference photometer.
* * * * *3.2.4 PM2.5 Performance Evaluation Program (PEP) Procedures. The PEP is an independent assessment used to estimate total measurement system bias. These evaluations will be performed under the NPEP as described in section 2.4 of this appendix or a comparable program. Performance evaluations will be performed annually within each PQAO. For PQAOs with less than or equal to five monitoring sites, five valid performance evaluation audits must be collected and reported each year. For PQAOs with greater than five monitoring sites, eight valid performance evaluation audits must be collected and reported each year. A valid performance evaluation audit means that both the primary monitor and PEP audit concentrations are valid and equal to or greater than 2 µg/m3. Siting of the PEP monitor must be consistent with section 3.2.3.4(c) of this appendix. However, any horizontal distance greater than 4 meters and any vertical distance greater than one meter must be reported to the EPA regional PEP coordinator. Additionally for every monitor designated as a primary monitor, a primary quality assurance organization must:
3.2.4.1 Have each method designation evaluated each year; and,
3.2.4.2 Have all FRM and FEM samplers subject to a PEP audit at least once every 6 years, which equates to approximately 15 percent of the monitoring sites audited each year.
3.2.4.3 Additional information concerning the PEP is contained in Reference 10 of this appendix. The calculations for evaluating bias between the primary monitor and the performance evaluation monitor for PM2.5 are described in section 4.2.5 of this appendix.
* * * * *4.2.1 Collocated Quality Control Sampler Precision Estimate for PM10, PM2.5, and Pb. Precision is estimated via duplicate measurements from collocated samplers. It is recommended that the precision be aggregated at the PQAO level quarterly, annually, and at the 3-year level. The data pair would only be considered valid if both concentrations are greater than or equal to the minimum values specified in section 4(c) of this appendix. For each collocated data pair, calculate ti, using equation 6 to this appendix:
Where Xi is the concentration from the primary sampler and Yi is the concentration value from the audit sampler. The coefficient of variation upper bound is calculated using equation 7 to this appendix:

Where k is the number of valid data pairs being aggregated, and X20.1,k-1 is the 10th percentile of a chi-squared distribution with k-1 degrees of freedom. The factor of 2 in the denominator adjusts for the fact that Start Printed Page 16394 each ti is calculated from two values with error.
* * * * *4.2.5 Performance Evaluation Programs Bias Estimate for PM2.5 . The bias estimate is calculated using the PEP audits described in section 3.2.4. of this appendix. The bias estimator is based on, si, the absolute difference in concentrations divided by the square root of the PEP concentration.
 * * * * *
* * * * *6. References
(1) American National Standard Institute—Quality Management Systems For Environmental Information And Technology Programs—Requirements With Guidance For Use. ASQ/ANSI E4–2014. February 2014. Available from ANSI Webstore https://webstore.ansi.org/.
* * * * *(4) EPA Traceability Protocol for Assay and Certification of Gaseous Calibration Standards. EPA–600/R–12/531. May, 2012. Available from U.S. Environmental Protection Agency, National Risk Management Research Laboratory, Research Triangle Park NC 27711. https://www.epa.gov/nscep.
* * * * *(6) List of Designated Reference and Equivalent Methods. Available from U.S. Environmental Protection Agency, Center for Environmental Measurements and Modeling, Air Methods and Characterization Division, MD–D205–03, Research Triangle Park, NC 27711. https://www.epa.gov/amtic/air-monitoring-methods-criteria-pollutants.
(7) Transfer Standards for the Calibration of Ambient Air Monitoring Analyzers for Ozone. EPA–454/B–13–004 U.S. Environmental Protection Agency, Research Triangle Park, NC 27711, October, 2013. https://www.epa.gov/sites/default/files/2020-09/documents/ozonetransferstandardguidance.pdf.
* * * * *(9) Quality Assurance Handbook for Air Pollution Measurement Systems, Volume 1—A Field Guide to Environmental Quality Assurance. EPA–600/R–94/038a. April 1994. Available from U.S. Environmental Protection Agency, ORD Publications Office, Center for Environmental Research Information (CERI), 26 W. Martin Luther King Drive, Cincinnati, OH 45268. https://www.epa.gov/amtic/ambient-air-monitoring-quality-assurance#documents.
(10) Quality Assurance Handbook for Air Pollution Measurement Systems, Volume II: Ambient Air Quality Monitoring Program Quality System Development. EPA–454/B–13–003. https://www.epa.gov/amtic/ambient-air-monitoring-quality-assurance#documents.
(11) National Performance Evaluation Program Standard Operating Procedures. https://www.epa.gov/amtic/ambient-air-monitoring-quality-assurance#npep.
Start Amendment PartTable B–1 to Section 6 of Appendix B- Minimum Data Assessment Requirements for NAAQS Related Criteria Pollutant PSD Monitors
Method Assessment method Coverage Minimum frequency Parameters reported AQS Assessment type Gaseous Methods (CO, NO 2 , SO 2 , O 3 ): One-Point QC for SO 2 , NO 2 , O 3 , CO Response check at concentration 0.005–0.08 ppm SO 2 , NO 2 , O 3 , & 0.5 and 5 ppm CO Each analyzer Once per 2 weeks5 Audit concentration1 and measured concentration2 One-Point QC. Quarterly performance evaluation for SO 2 , NO 2 , O 3 , CO See section 3.1.2 of this appendix Each analyzer Once per quarter5 Audit concentration1 and measured concentration2 for each level Annual PE. NPAP for SO 2 , NO 2 , O 3 , CO3 Independent Audit Each primary monitor Once per year Audit concentration1 and measured concentration2 for each level NPAP. Particulate Methods: Collocated sampling PM 10 , PM 2.5 , Pb Collocated samplers 1 per PSD Network per pollutant Every 6 days or every 3 days if daily monitoring required Primary sampler concentration and duplicate sampler concentration4 No Transaction reported as raw data. Flow rate verification PM 10 , PM 2.5 , Pb Check of sampler flow rate Each sampler Once every month5 Audit flow rate and measured flow rate indicated by the sampler Flow Rate Verification. Semi-annual flow rate audit PM 10 , PM 2.5 , Pb Check of sampler flow rate using independent standard Each sampler Once every 6 months or beginning, middle and end of monitoring5 Audit flow rate and measured flow rate indicated by the sampler Semi Annual Flow Rate Audit. Start Printed Page 16395 Pb analysis audits Pb-TSP, Pb-PM 10 Check of analytical system with Pb audit strips/filters Analytical Each quarter5 Measured value and audit value (ug Pb/filter) using AQS unit code 077 for parameters: 14129—Pb (TSP) LC FRM/FEM 85129—Pb (TSP) LC Non-FRM/FEM. Pb Analysis Audits. Performance Evaluation Program PM 2.53 Collocated samplers (1) 5 valid audits for PQAOs with <= 5 sites. (2) 8 valid audits for PQAOs with > 5 sites. (3) All samplers in 6 years Over all 4 quarters5 Primary sampler concentration and performance evaluation sampler concentration PEP. Performance Evaluation Program Pb 3 Collocated samplers (1) 1 valid audit and 4 collocated samples for PQAOs, with <=5 sites. (2) 2 valid audits and 6 collocated samples for PQAOs with >5 sites. Over all 4 quarters5 Primary sampler concentration and performance evaluation sampler concentration. Primary sampler concentration and duplicate sampler concentration PEP. 1 Effective concentration for open path analyzers. 2 Corrected concentration, if applicable for open path analyzers. 3 NPAP, PM 2.5 , PEP, and Pb-PEP must be implemented if data is used for NAAQS decisions otherwise implementation is at PSD reviewing authority discretion. 4 Both primary and collocated sampler values are reported as raw data 5 A maximum number of days should be between these checks to ensure the checks are routinely conducted over time and to limit data impacts resulting from a failed check. 28. Amend appendix C to part 58 by:
End Amendment Part Start Amendment Parta. Adding sections 2.2 and 2.2.1 through 2.2.19;
End Amendment Part Start Amendment Partb. Removing and reserving sections 2.4, 2.4.1;
End Amendment Part Start Amendment Partc. Removing sections 2.4.1.1 through 2.4.1.7; and
End Amendment Part Start Amendment Partd. Revising section 2.7.1.
End Amendment PartThe additions and revision reads as follows:
Appendix C to Part 58—Ambient Air Quality Monitoring Methodology
* * * * *2.2 PM10, PM2.5, or PM10–2.5 continuous FEMs with existing valid designations may be calibrated using network data from collocated FRM and continuous FEM data under the following provisions:
2.2.1 Data to demonstrate a calibration may include valid data from State, local, or Tribal air agencies or data collected by instrument manufacturers in accordance with 40 CFR 53.35 or other data approved by the Administrator.
2.2.2 A request to update a designated methods calibration may be initiated by the instrument manufacturer of record or the EPA Administrator. State, local, Tribal, and multijusistincional organizations of these entities may work with an instrument manufacture to update a designated method calibration.
2.2.3 Requests for approval of an updated PM10, PM2.5, or PM10–2.5 continuous FEM calibration must meet the general submittal requirements of section 2.7 of this appendix.
2.2.4 Data included in the request should represent a subset of representative locations where the method is operational. For cases with a small number of collocated FRMs and continuous FEMs sites, an updated candidate calibration may be limited to the sites where both methods are in use.
2.2.5 Data included in a candidate method updated calibration may include a subset of sites where there is a large grouping of sites in one part of the country such that the updated calibration would be representative of the country as a whole.
2.2.6 Improvements should be national in scope and ideally implemented through a firmware change.
2.2.7 The goal of a change to a methods calibration is to increase the number of sites meeting measurements quality objectives of the method as identified in section 2.3.1.1 of appendix A to this part.
2.2.8 For meeting measurement quality objectives (MQOs), the primary objective is to meet the bias goal as this statistic will likely have the most influence on improving the resultant data collected.
2.2.9 Precision data are to be included, but so long as precision data are at least as good as existing network data or meet the MQO referenced in section 2.2.8 of this appendix, no further work is necessary with precision.
2.2.10 Data available to use may include routine primary and collocated data.
2.2.11 Audit data may be useful to confirm the performance of a candidate updated calibration but should not be used as the basis of the calibration to keep the independence of the audit data.
2.2.12 Data utilized as the basis of the updated calibration may be obtained by accessing EPA's AQS database or future analogous EPA database.
2.2.13 Years of data to use in a candidate method calibration should include two recent years where we are past the certification period for the previous year's data, which is May 1 of each year.
2.2.14 Data from additional years is to be used to test an updated calibration such that the calibration is independent of the test years of interest. Data from these additional years need to minimally demonstrate that a larger number of sites are expected to meet bias MQO especially at sites near the level of the NAAQS for the PM indicator of interest.
2.2.15 Outliers may be excluded using routine outlier tests.
2.2.16 The range of data used in a calibration may include all data available or alternatively use data in the range from the lowest measured data available up to 125% of the 24-hour NAAQS for the PM indicator of interest. Start Printed Page 16396
2.2.17 Other improvements to a PM continuous method may be included as part of a recommended update so long as appropriate testing is conducted with input from EPA's Office of Research and Development (ORD) Reference and Equivalent (R&E) Methods Designation program.
2.2.18 EPA encourages early communication by instrument manufacturers considering an update to a PM method. Instrument companies should initiate such dialogue by contacting EPA's ORD R&E Methods Designation program. The contact information for this can be found at 40 CFR 53.4.
2.2.19 Manufacturers interested in improving instrument's performance through an updated factory calibration must submit a written modification request to EPA with supporting rationale. Because the testing requirements and acceptance criteria of any field and/or lab tests can depend upon the nature and extent of the intended modification, applicants should contact EPA's R&E Methods Designation program for guidance prior to development of the modification request.
* * * * *2.7.1 Requests for approval under sections 2.2, 2.4, 2.6.2, or 2.8 of this appendix must be submitted to: Director, Center for Environmental Measurement and Modeling, Reference and Equivalent Methods Designation Program (MD–D205–03), U.S. Environmental Protection Agency, P.O. Box 12055, Research Triangle Park, North Carolina 27711.
Start Amendment Part29. Amend appendix D to part 58 by revising sections 1 and 1.1(b), the introductory text before the table in section 4.7.1(a), and sections 4.7.1(b)(3) and 4.7.2 to read as follows:
End Amendment PartAppendix D to Part 58—Network Design Criteria for Ambient Air Quality Monitoring
* * * * *1. Monitoring Objectives and Spatial Scales
The purpose of this appendix is to describe monitoring objectives and general criteria to be applied in establishing the required SLAMS ambient air quality monitoring stations and for choosing general locations for additional monitoring sites. This appendix also describes specific requirements for the number and location of FRM and FEM sites for specific pollutants, NCore multipollutant sites, PM10 mass sites, PM2.5 mass sites, chemically-speciated PM2.5 sites, and O3 precursor measurements sites (PAMS). These criteria will be used by EPA in evaluating the adequacy of the air pollutant monitoring networks.
1.1 * * *
(b) Support compliance with ambient air quality standards and emissions strategy development. Data from FRM and FEM monitors for NAAQS pollutants will be used for comparing an area's air pollution levels against the NAAQS. Data from monitors of various types can be used in the development of attainment and maintenance plans. SLAMS, and especially NCore station data, will be used to evaluate the regional air quality models used in developing emission strategies, and to track trends in air pollution abatement control measures' impact on improving air quality. In monitoring locations near major air pollution sources, source-oriented monitoring data can provide insight into how well industrial sources are controlling their pollutant emissions.
* * * * *4.7.1 * * *
(a) State and where applicable, local, agencies must operate the minimum number of required PM2.5 SLAMS sites listed in table D–5 to this appendix. The NCore sites are expected to complement the PM2.5 data collection that takes place at non-NCore SLAMS sites, and both types of sites can be used to meet the minimum PM2.5 network requirements. For many State and local networks, the total number of PM2.5 sites needed to support the basic monitoring objectives of providing air pollution data to the general public in a timely manner, support compliance with ambient air quality standards and emission strategy development, and support for air pollution research studies will include more sites than the minimum numbers required in table D–5 to this appendix. Deviations from these PM2.5 monitoring requirements must be approved by the EPA Regional Administrator.
* * * * *(b) * * *
(3) For areas with additional required SLAMS, a monitoring station is to be sited in an at-risk community with poor air quality, particularly where there are anticipated effects from sources in the area ( e.g., a major industrial area, point source(s), port, rail yard, airport, or other transportation facility or corridor).
* * * * *4.7.2 Requirement for Continuous PM2.5 Monitoring. The State, or where appropriate, local agencies must operate continuous PM2.5 analyzers equal to at least one-half (round up) the minimum required sites listed in table D–5 to this appendix. At least one required continuous analyzer in each MSA must be collocated with one of the required FRM/FEM monitors, unless at least one of the required FRM/FEM monitors is itself a continuous FEM monitor in which case no collocation requirement applies. State and local air monitoring agencies must use methodologies and quality assurance/quality control (QA/QC) procedures approved by the EPA Regional Administrator for these required continuous analyzers.
* * * * *Start Amendment Part30. Revise appendix E to part 58 to read as follows:
End Amendment PartAppendix E to Part 58—Probe and Monitoring Path Siting Criteria for Ambient Air Quality Monitoring
1. Introduction
2. Monitors and Samplers with Probe Inlets
3. Open Path Analyzers
4. Waiver Provisions
5. References
1. Introduction
1.1 Applicability
(a) This appendix contains specific location criteria applicable to ambient air quality monitoring probes, inlets, and optical paths of SLAMS, NCore, PAMS, and other monitor types whose data are intended to be used to determine compliance with the NAAQS. These specific location criteria are relevant after the general location has been selected based on the monitoring objectives and spatial scale of representation discussed in appendix D to this part. Monitor probe material and sample residence time requirements are also included in this appendix. Adherence to these siting criteria is necessary to ensure the uniform collection of compatible and comparable air quality data.
(b) The probe and monitoring path siting criteria discussed in this appendix must be followed to the maximum extent possible. It is recognized that there may be situations where some deviation from the siting criteria may be necessary. In any such case, the reasons must be thoroughly documented in a written request for a waiver that describes whether the resulting monitoring data will be representative of the monitoring area and how and why the proposed or existing siting must deviate from the criteria. This documentation should help to avoid later questions about the validity of the resulting monitoring data. Conditions under which the EPA would consider an application for waiver from these siting criteria are discussed in section 4 of this appendix.
(c) The pollutant-specific probe and monitoring path siting criteria generally apply to all spatial scales except where noted otherwise. Specific siting criteria that are phrased with “shall” or “must” are defined as requirements and exceptions must be granted through the waiver provisions. However, siting criteria that are phrased with “should” are defined as goals to meet for consistency but are not requirements.
2. Monitors and Samplers with Probe Inlets
2.1 Horizontal and Vertical Placement
(a) For O3 and SO2 monitoring, and for neighborhood or larger spatial scale Pb, PM10, PM10–2.5, PM2.5, NO2, and CO sites, the probe must be located greater than or equal to 2.0 meters and less than or equal to 15 meters above ground level.
(b) Middle scale CO and NO2 monitors must have sampler inlets greater than or equal to 2.0 meters and less than or equal to 15 meters above ground level.
(c) Middle scale PM10–2.5 sites are required to have sampler inlets greater than or equal to 2.0 meters and less than or equal to 7.0 meters above ground level.
(d) Microscale Pb, PM10, PM10–2.5, and PM2.5 sites are required to have sampler inlets greater than or equal to 2.0 meters and less than or equal to 7.0 meters above ground level.
(e) Microscale near-road NO2 monitoring sites are required to have sampler inlets greater than or equal to 2.0 meters and less than or equal to 7.0 meters above ground level.
(f) The probe inlets for microscale carbon monoxide monitors that are being used to Start Printed Page 16397 measure concentrations near roadways must be greater than or equal to 2.0 meters and less than or equal to 7.0 meters above ground level. Those probe inlets for microscale carbon monoxide monitors measuring concentrations near roadways in downtown areas or urban street canyons must be greater than or equal to 2.5 meters and less than or equal to 3.5 meters above ground level. The probe must be at least 1.0 meter vertically or horizontally away from any supporting structure, walls, parapets, penthouses, etc ., and away from dusty or dirty areas. If the probe is located near the side of a building or wall, then it should be located on the windward side of the building relative to the prevailing wind direction during the season of highest concentration potential for the pollutant being measured.
2.2 Spacing From Minor Sources
(a) It is important to understand the monitoring objective for a particular site in order to interpret this requirement. Local minor sources of a primary pollutant, such as SO2, lead, or particles, can cause high concentrations of that particular pollutant at a monitoring site. If the objective for that monitoring site is to investigate these local primary pollutant emissions, then the site will likely be properly located nearby. This type of monitoring site would, in all likelihood, be a microscale-type of monitoring site. If a monitoring site is to be used to determine air quality over a much larger area, such as a neighborhood or city, a monitoring agency should avoid placing a monitor probe inlet near local, minor sources, because a plume from a local minor source should not be allowed to inappropriately impact the air quality data collected at a site. Particulate matter sites should not be located in an unpaved area unless there is vegetative ground cover year-round, so that the impact of windblown dusts will be kept to a minimum.
(b) Similarly, local sources of nitric oxide (NO) and ozone-reactive hydrocarbons can have a scavenging effect causing unrepresentatively low concentrations of O3 in the vicinity of probes for O3 . To minimize these potential interferences from nearby minor sources, the probe inlet should be placed at a distance from furnace or incineration flues or other minor sources of SO2 or NO. The separation distance should take into account the heights of the flues, type of waste or fuel burned, and the sulfur content of the fuel.
2.3 Spacing From Obstructions
(a) Obstacles may scavenge SO2, O3, or NO2, and can act to restrict airflow for any pollutant. To avoid this interference, the probe inlet must have unrestricted airflow pursuant to paragraph (b) of this section and should be located at a distance from obstacles. The horizontal distance from the obstacle to the probe inlet must be at least twice the height that the obstacle protrudes above the probe inlet. An obstacle that does not meet the minimum distance requirement is considered an obstruction that restricts airflow to the probe inlet. The EPA does not generally consider objects or obstacles such as flag poles or site towers used for NOy convertors and meteorological sensors, etc. to be deemed obstructions.
(b) A probe inlet located near or along a vertical wall is undesirable because air moving along the wall may be subject to removal mechanisms. A probe inlet must have unrestricted airflow with no obstructions (as defined in paragraph (a) of this section) in a continuous arc of at least 270 degrees. An unobstructed continuous arc of 180 degrees is allowable when the applicable network design criteria specified in appendix D of this part require monitoring in street canyons and the probe is located on the side of a building. This arc must include the predominant wind direction for the season of greatest pollutant concentration potential. For particle sampling, there must be a minimum of 2.0 meters of horizontal separation from walls, parapets, and structures for rooftop site placement.
(c) A sampling station with a probe inlet located closer to an obstacle than required by the criteria in this section should be classified as middle scale or microscale, rather than neighborhood or urban scale, since the measurements from such a station would more closely represent these smaller scales.
(d) For near-road monitoring stations, the monitor probe shall have an unobstructed air flow, where no obstacles exist at or above the height of the monitor probe, between the monitor probe and the outside nearest edge of the traffic lanes of the target road segment.
2.4 Spacing From Trees
(a) Trees can provide surfaces for SO2, O3, or NO2 adsorption or reactions and surfaces for particle deposition. Trees can also act as obstructions in locations where the trees are between the air pollutant sources or source areas and the monitoring site and where the trees are of a sufficient height and leaf canopy density to interfere with the normal airflow around the probe inlet. To reduce this possible interference/obstruction, the probe inlet should be 20 meters or more from the drip line of trees and must be at least 10 meters from the drip line of trees. If a tree or group of trees is an obstacle, the probe inlet must meet the distance requirements of section 2.3 of this appendix.
(b) The scavenging effect of trees is greater for O3 than for other criteria pollutants. Monitoring agencies must take steps to consider the impact of trees on ozone monitoring sites and take steps to avoid this problem.
(c) Beginning January 1, 2024, microscale sites of any air pollutant shall have no trees or shrubs located at or above the line-of-sight fetch between the probe and the source under investigation, e.g., a roadway or a stationary source.
2.5 Spacing From Roadways
Table E–1 to Section 2.5 of Appendix E—Minimum Separation Distance Between Roadways and Probes for Monitoring Neighborhood and Urban Scale Ozone (O 3 ) and Oxides of Nitrogen (NO, NO 2 , NO X , NO y )
Roadway average daily traffic, vehicles per day Minimum distance1 3 (meters) Minimum distance1 2 3 (meters) ≤1,000 10 10 10,000 10 20 15,000 20 30 20,000 30 40 40,000 50 60 70,000 100 100 ≥110,000 250 250 1 Distance from the edge of the nearest traffic lane. The distance for intermediate traffic counts should be interpolated from the table values based on the actual traffic count./TNOTE> 2 Applicable for ozone monitors whose placement was not approved as of December 18, 2006. 3 All distances listed are expressed as having 2 significant figures. When rounding is performed to assess compliance with these siting requirements, the distance measurements will be rounded such as to retain at least two significant figures. 2.5.1 Spacing for Ozone Probes
In siting an O3 monitor, it is important to minimize destructive interferences from sources of NO, since NO readily reacts with O3. Table E–1 of this appendix provides the required minimum separation distances between a roadway and a probe inlet for various ranges of daily roadway traffic. A sampling site with a monitor probe located closer to a roadway than allowed by the Table E–1 requirements should be classified as middle scale or microscale, rather than neighborhood or urban scale, since the measurements from such a site would more closely represent these smaller scales.
2.5.2 Spacing for Carbon Monoxide Probes
(a) Near-road microscale CO monitoring sites, including those located in downtown areas, urban street canyons, and other near-road locations such as those adjacent to highly trafficked roads, are intended to provide a measurement of the influence of the immediate source on the pollution exposure on the adjacent area.
(b) Microscale CO monitor probe inlets in downtown areas or urban street canyon locations shall be located a minimum distance of 2.0 meters and a maximum distance of 10 meters from the edge of the nearest traffic lane.
(c) Microscale CO monitor probe inlets in downtown areas or urban street canyon locations shall be located at least 10 meters from an intersection, preferably at a midblock location. Midblock locations are preferable to intersection locations because intersections represent a much smaller portion of downtown space than do the streets between Start Printed Page 16398 them. Pedestrian exposure is probably also greater in street canyon/corridors than at intersections.
(d) Neighborhood scale CO monitor probe inlets in downtown areas or urban street canyon locations shall be located according to the requirements in Table E–2 of this appendix.
Table E–2 to Section 2.5.2 of Appendix E—Minimum Separation Distance Between Roadways and Probes for Monitoring Neighborhood Scale Carbon Monoxide
Roadway average daily traffic, vehicles per day Minimum distance 1 2 (meters) ≤10,000 10 15,000 25 20,000 45 30,000 80 40,000 115 50,000 135 ≥60,000 150 1 Distance from the edge of the nearest traffic lane. The distance for intermediate traffic counts should be interpolated from the table values based on the actual traffic count. 2 All distances listed are expressed as having 2 significant figures. When rounding is performed to assess compliance with these siting requirements, the distance measurements will be rounded such as to retain at least two significant figures. 2.5.3 Spacing for Particulate Matter (PM2.5, PM2.5–10, PM10, Pb) Inlets
(a) Since emissions associated with the operation of motor vehicles contribute to urban area particulate matter ambient levels, spacing from roadway criteria are necessary for ensuring national consistency in PM sampler siting.
(b) The intent is to locate localized hot-spot sites in areas of highest concentrations, whether it be caused by mobile or multiple stationary sources. If the area is primarily affected by mobile sources and the maximum concentration area(s) is judged to be a traffic corridor or street canyon location, then the monitors should be located near roadways with the highest traffic volume and at separation distances most likely to produce the highest concentrations. For microscale traffic corridor sites, the location must be greater than or equal 5.0 meters and less than or equal to 15 meters from the major roadway. For the microscale street canyon site, the location must be greater than or equal 2.0 meters and less than or equal to 10 meters from the roadway. For the middle scale site, a range of acceptable distances from the roadway is shown in Figure E–1 of this appendix. This figure also includes separation distances between a roadway and neighborhood or larger scale sites by default. Any PM probe inlet at a site, 2.0 to 15 meters high, and further back than the middle scale requirements will generally be neighborhood, urban or regional scale. For example, according to Figure E–1 of this appendix, if a PM sampler is primarily influenced by roadway emissions and that sampler is set back 10 meters from a 30,000 ADT (average daily traffic) road, the site should be classified as microscale, if the sampler's inlet height is between 2.0 and 7.0 meters. If the sampler's inlet height is between 7.0 and 15 meters, the site should be classified as middle scale. If the sampler is 20 meters from the same road, it will be classified as middle scale; if 40 meters, neighborhood scale; and if 110 meters, an urban scale.

2.5.4 Spacing for Nitrogen Dioxide (NO2) Probes
(a) In siting near-road NO2 monitors as required in section 4.3.2 of appendix D of this part, the monitor probe shall be as near as practicable to the outside nearest edge of the traffic lanes of the target road segment but shall not be located at a distance greater than 50 meters, in the horizontal, from the outside nearest edge of the traffic lanes of the target road segment. Where possible, the near-road NO2 monitor probe should be within 20 meters of the target road segment.
(b) In siting NO2 monitors for neighborhood and larger scale monitoring, it is important to minimize near-road influences. Table E–1 of this appendix provides the required minimum separation distances between a roadway and a probe inlet for various ranges of daily roadway traffic. A site with a monitor probe located closer to a roadway than allowed by the Table E–1 requirements should be classified Start Printed Page 16399 as microscale or middle scale rather than neighborhood or urban scale.
2.6 Probe Material and Pollutant Sampler Residence Time
(a) For the reactive gases (SO2, NO2, and O3), approved probe materials must be used for monitors. Studies25 34 have been conducted to determine the suitability of materials such as polypropylene, polyethylene, polyvinyl chloride, Tygon®, aluminum, brass, stainless steel, copper, borosilicate glass, polyvinylidene fluoride (PVDF), polytetrafluoroethylene (PTFE), perfluoroalkoxy (PFA), and fluorinated ethylene propylene (FEP) for use as intake sampling lines. Of the above materials, only borosilicate glass, PVDF, PTFE, PFA, and FEP have been found to be acceptable for use as intake sampling lines for all the reactive gaseous pollutants. Furthermore, the EPA 25 has specified borosilicate glass, FEP Teflon®, or their equivalents as the only acceptable probe materials for delivering test atmospheres in the determination of reference or equivalent methods. Therefore, borosilicate glass, PVDF, PTFE, PFA, FEP, or their equivalents must be the only material in the sampling train (from probe inlet to the back of the monitor) that can be in contact with the ambient air sample for reactive gas monitors. NafionTM , which is composed primarily of PTFE, can be considered equivalent to PTFE; it has been shown in tests to exhibit virtually no loss of ozone at 20-second residence times.35
(b) For volatile organic compound (VOC) monitoring at PAMS, FEP Teflon® is unacceptable as the probe material because of VOC adsorption and desorption reactions on the FEP Teflon®. Borosilicate glass, stainless steel, or their equivalents are the acceptable probe materials for VOC and carbonyl sampling. Care must be taken to ensure that the sample residence time is kept to 20 seconds or less.
(c) No matter how nonreactive the sampling probe material is initially, after a period of use, reactive particulate matter is deposited on the probe walls. Therefore, the time it takes the gas to transfer from the probe inlet to the sampling device is critical. Ozone in the presence of nitrogen oxide (NO) will show significant losses, even in the most inert probe material, when the residence time exceeds 20 seconds.26 Other studies 27 28 indicate that a 10-second or less residence time is easily achievable. Therefore, sampling probes for all reactive gas monitors for SO2, NO2, and O3 must have a sample residence time less than 20 seconds.
2.7 Summary
Table E–3 of this appendix presents a summary of the general requirements for probe siting criteria with respect to distances and heights. Table E–3 requires different elevation distances above the ground for the various pollutants. The discussion in this appendix for each of the pollutants describes reasons for elevating the monitor or probe inlet. The differences in the specified range of heights are based on the vertical concentration gradients. For source oriented and near-road monitors, the gradients in the vertical direction are very large for the microscale, so a small range of heights are used. The upper limit of 15 meters is specified for the consistency between pollutants and to allow the use of a single manifold for monitoring more than one pollutant.
Table E–3 to Section 2.7 of Appendix E—Summary of Probe Siting Criteria
Pollutant Scale 9 Height from ground to probe 8 (meters) Horizontal or vertical distance from supporting structures 18 to probe inlet (meters) Distance from drip line of trees to probe 8 (meters) Distance from roadways to probe 8 (meters) SO 22 3 4 5 Middle, Neighborhood, Urban, and Regional 2.0–15 ≥1.0 ≥10 N/A. CO 3 4 6 Micro [downtown or street canyon sites] 2.5–3.5 2.0–10 for downtown areas or street canyon microscale. Micro [Near-Road sites] 2.0–7.0 ≥1.0 ≥10 ≤50 for near-road microscale. Middle and Neighborhood 2.0–15 See Table E–2 of this appendix for middle and neighborhood scales. O 3 2 3 4 Middle, Neighborhood, Urban, and Regional 2.0–15 ≥1.0 ≥10 See Table E–1. Micro 2.0–7.0 ≤50 for near-road micro-scale. NO 2 2 3 4 Middle, Neighborhood, Urban, and Regional 2.0–15 ≥1.0 ≥10 See Table E–1. PAMS 2 3 4 Ozone precursors Neighborhood and Urban 2.0–15 ≥1.0 ≥10 See Table E–1. PM, Pb 2 3 4 7 Micro 2.0–7.0 Middle, Neighborhood, Urban and Regional 2.0–15 ≥2.0 (horizontal distance only) ≥10 See Figure E–1. N/A—Not applicable. 1 When a probe is located on a rooftop, this separation distance is in reference to walls, parapets, or penthouses located on the roof. 2 Should be greater than 20 meters from the dripline of tree(s) and must be 10 meters from the dripline. 3 Distance from sampler or probe inlet to obstacle, such as a building, must be at least twice the height the obstacle protrudes above the sampler or probe inlet. Sites not meeting this criterion may be classified as microscale or middle scale ( see paragraphs 2.3(a) and 2.3(c)). 4 Must have unrestricted airflow in a continuous arc of at least 270 degrees around the probe or sampler; 180 degrees if the probe is on the side of a building or a wall for street canyon monitoring. 5 The probe or sampler should be away from minor sources, such as furnace or incineration flues. The separation distance is dependent on the height of the minor source emission point(s), the type of fuel or waste burned, and the quality of the fuel (sulfur, ash, or lead content). This criterion is designed to avoid undue influences from minor sources. 6 For microscale CO monitoring sites, the probe must be ≥10 meters from a street intersection and preferably at a midblock location. 7 Collocated monitor inlets must be within 4.0 meters of each other and at least 2.0 meters apart for flow rates greater than 200 liters/min or at least 1.0 meter apart for samplers having flow rates less than 200 liters/min to preclude airflow interference, unless a waiver has been granted by the Regional Administrator pursuant to paragraph 3.3.4.2(c) of appendix A of part 58. For PM 2.5 , collocated monitor inlet heights should be within 1.0 meter of each other vertically. 8 All distances listed are expressed as having 2 significant figures. When rounding is performed to assess compliance with these siting requirements, the distance measurements will be rounded such as to retain at least two significant figures. 9 See section 1.2 of appendix D for definitions of monitoring scales. 3. Open Path Analyzers
3.1 Horizontal and Vertical Placement
(a) For all O3 and SO2 monitoring sites and for neighborhood or larger spatial scale NO2, and CO sites, at least 80 percent of the monitoring path must be located greater than or equal 2.0 meters and less than or equal to 15 meters above ground level.
(b) Middle scale CO and NO2 sites must have monitoring paths greater than or equal 2.0 meters and less than or equal to 15 meters above ground level.
(c) Microscale near-road monitoring sites are required to have monitoring paths greater than or equal 2.0 meters and less than or equal to 7.0 meters above ground level.
(d) For microscale carbon monoxide monitors that are being used to measure concentrations near roadways, the monitoring path must be greater than or equal 2.0 meters and less than or equal to 7.0 meters above ground level. If the microscale carbon monoxide monitors measuring concentrations near roadways are in downtown areas or urban street canyons, the monitoring path must be greater than or equal 2.5 meters and less than or equal to 3.5 meters above ground level and at least 90 Start Printed Page 16400 percent of the monitoring path must be at least 1.0 meter vertically or horizontally away from any supporting structure, walls, parapets, penthouses, etc., and away from dusty or dirty areas. If a significant portion of the monitoring path is located near the side of a building or wall, then it should be located on the windward side of the building relative to the prevailing wind direction during the season of highest concentration potential for the pollutant being measured.
3.2 Spacing From Minor Sources
(a) It is important to understand the monitoring objective for a particular site in order to interpret this requirement. Local minor sources of a primary pollutant, such as SO2 can cause high concentrations of that particular pollutant at a monitoring site. If the objective for that monitoring site is to investigate these local primary pollutant emissions, then the site will likely be properly located nearby. This type of monitoring site would, in all likelihood, be a microscale type of monitoring site. If a monitoring site is to be used to determine air quality over a much larger area, such as a neighborhood or city, a monitoring agency should avoid placing a monitoring path near local, minor sources, because a plume from a local minor source should not be allowed to inappropriately impact the air quality data collected at a site.
(b) Similarly, local sources of nitric oxide (NO) and ozone-reactive hydrocarbons can have a scavenging effect causing unrepresentatively low concentrations of O3 in the vicinity of monitoring paths for O3 . To minimize these potential interferences from nearby minor sources, at least 90 percent of the monitoring path should be at a distance from furnace or incineration flues or other minor sources of SO2 or NO. The separation distance should take into account the heights of the flues, type of waste or fuel burned, and the sulfur content of the fuel.
3.3 Spacing From Obstructions
(a) Obstacles may scavenge SO2, O3, or NO2, and can act to restrict airflow for any pollutant. To avoid this interference, at least 90 percent of the monitoring path must have unrestricted airflow and should be located at a distance from obstacles. The horizontal distance from the obstacle to the monitoring path must be at least twice the height that the obstacle protrudes above the monitoring path. An obstacle that does not meet the minimum distance requirement is considered an obstruction that restricts airflow to the monitoring path. The EPA does not generally consider objects or obstacles such as flag poles or site towers used for NOy convertors and meteorological sensors, etc. to be deemed obstructions.
(b) A monitoring path located near or along a vertical wall is undesirable because air moving along the wall may be subject to removal mechanisms. At least 90 percent of the monitoring path for open path analyzers must have unrestricted airflow with no obstructions (as defined in paragraph (a) of this section) in a continuous arc of at least 270 degrees. An unobstructed continuous arc of 180 degrees is allowable when the applicable network design criteria specified in appendix D of this part require monitoring in street canyons and the monitoring path is located on the side of a building. This arc must include the predominant wind direction for the season of greatest pollutant concentration potential.
(c) Special consideration must be given to the use of open path analyzers given their inherent potential sensitivity to certain types of interferences and optical obstructions. A monitoring path must be clear of all trees, brush, buildings, plumes, dust, or other optical obstructions, including potential obstructions that may move due to wind, human activity, growth of vegetation, etc. Temporary optical obstructions, such as rain, particles, fog, or snow, should be considered when siting an open path analyzer. Any of these temporary obstructions that are of sufficient density to obscure the light beam will negatively affect the ability of the open path analyzer to continuously measure pollutant concentrations. Transient, but significant obscuration of especially longer measurement paths, could occur as a result of certain meteorological conditions ( e.g., heavy fog, rain, snow) and/or aerosol levels that are of a sufficient density to prevent the open path analyzer's light transmission. If certain compensating measures are not otherwise implemented at the onset of monitoring ( e.g., shorter path lengths, higher light source intensity), data recovery during periods of greatest primary pollutant potential could be compromised. For instance, if heavy fog or high particulate levels are coincident with periods of projected NAAQS-threatening pollutant potential, the representativeness of the resulting data record in reflecting maximum pollution concentrations may be substantially impaired despite the fact that the site may otherwise exhibit an acceptable, even exceedingly high, overall valid data capture rate.
(d) A sampling station with a monitoring path located closer to an obstacle than required by the criteria in this section should be classified as middle scale or microscale, rather than neighborhood or urban scale, since the measurements from such a station would more closely represent these smaller scales.
(e) For near-road monitoring stations, the monitoring path shall have an unobstructed air flow, where no obstacles exist at or above the height of the monitoring path, between the monitoring path and the outside nearest edge of the traffic lanes of the target road segment.
3.4 Spacing From Trees
(a) Trees can provide surfaces for SO2, O3, or NO2 adsorption or reactions. Trees can also act as obstructions in locations where the trees are located between the air pollutant sources or source areas and the monitoring site, and where the trees are of a sufficient height and leaf canopy density to interfere with the normal airflow around the monitoring path. To reduce this possible interference/obstruction, at least 90 percent of the monitoring path should be 20 meters or more from the drip line of trees and must be at least 10 meters from the drip line of trees. If a tree or group of trees could be considered an obstacle, the monitoring path must meet the distance requirements of section 3.3 of this appendix.
(b) The scavenging effect of trees is greater for O3 than for other criteria pollutants. Monitoring agencies must take steps to consider the impact of trees on ozone monitoring sites and take steps to avoid this problem.
(c) Beginning January 1, 2024, microscale sites of any air pollutant shall have no trees or shrubs located at or above the line-of-sight fetch between the monitoring path and the source under investigation, e.g., a roadway or a stationary source.
3.5 Spacing from Roadways
Table E–4 of Section 3.5 of Appendix E—Minimum Separation Distance Between Roadways and Monitoring Paths for Monitoring Neighborhood and Urban Scale Ozone (O 3 ) and Oxides of Nitrogen (NO, NO 2 , NO X , NO y )
Roadway average daily traffic, vehicles per day Minimum distance 1 3 (meters) Minimum distance 1 2 3 (meters) ≤1,000 10 10 10,000 10 20 15,000 20 30 20,000 30 40 40,000 50 60 70,000 100 100 ≥110,000 250 250 1 Distance from the edge of the nearest traffic lane. The distance for intermediate traffic counts should be interpolated from the table values based on the actual traffic count. 2 Applicable for ozone open path monitors whose placement was not approved as of December 18, 2006. 3 All distances listed are expressed as having 2 significant figures. When rounding is performed to assess compliance with these siting requirements, the distance measurements will be rounded such as to retain at least two significant figures. 3.5.1 Spacing for Ozone Monitoring Paths
In siting an O3 open path analyzer, it is important to minimize destructive interferences form sources of NO, since NO readily reacts with O3. Table E–4 of this appendix provides the required minimum separation distances between a roadway and at least 90 percent of a monitoring path for various ranges of daily roadway traffic. A monitoring site with a monitoring path located closer to a roadway than allowed by the Table E–4 requirements should be classified as microscale or middle scale, rather than neighborhood or urban scale, since the measurements from such a site would more closely represent these smaller scales. The monitoring path(s) must not cross over a roadway with an average daily traffic count of 10,000 vehicles per day or more. For locations where a monitoring path crosses a roadway with fewer than 10,000 vehicles per day, monitoring agencies must consider the entire segment of the monitoring path in the area of potential atmospheric interference from automobile emissions. Therefore, this Start Printed Page 16401 calculation must include the length of the monitoring path over the roadway plus any segments of the monitoring path that lie in the area between the roadway and minimum separation distance, as determined from Table E–4 of this appendix. The sum of these distances must not be greater than 10 percent of the total monitoring path length.
3.5.2 Spacing for Carbon Monoxide Monitoring Paths
(a) Near-road microscale CO monitoring sites, including those located in downtown areas, urban street canyons, and other near-road locations such as those adjacent to highly trafficked roads, are intended to provide a measurement of the influence of the immediate source on the pollution exposure on the adjacent area.
(b) Microscale CO monitoring paths in downtown areas or urban street canyon locations shall be located a minimum distance of 2.0 meters and a maximum distance of 10 meters from the edge of the nearest traffic lane.
(c) Microscale CO monitoring paths in downtown areas or urban street canyon locations shall be located at least 10 meters from an intersection, preferably at a midblock location. Midblock locations are preferable to intersection locations because intersections represent a much smaller portion of downtown space than do the streets between them. Pedestrian exposure is probably also greater in street canyon/corridors than at intersections.
(d) Neighborhood scale CO monitoring paths in downtown areas or urban street canyon locations shall be located according to the requirements in Table E–5 of this appendix.
Table E–5 Section 3.5.2 of Appendix E—Minimum Separation Distance Between Roadways and Monitoring Paths for Monitoring Neighborhood Scale Carbon Monoxide
Roadway average daily traffic, vehicles per day Minimum distance 1 2 (meters) ≤10,000 10 15,000 25 20,000 45 30,000 80 40,000 115 50,000 135 ≥60,000 150 1 Distance from the edge of the nearest traffic lane. The distance for intermediate traffic counts should be interpolated from the table values based on the actual traffic count. 2 All distances listed are expressed as having 2 significant figures. When rounding is performed to assess compliance with these siting requirements, the distance measurements will be rounded such as to retain at least two significant figures. 3.5.3 Spacing for Nitrogen Dioxide (NO2) Monitoring Paths
(a) In siting near-road NO2 monitors as required in section 4.3.2 of appendix D of this part, the monitoring path shall be as near as practicable to the outside nearest edge of the traffic lanes of the target road segment but shall not be located at a distance greater than 50 meters, in the horizontal, from the outside nearest edge of the traffic lanes of the target road segment.
(b) In siting NO2 open path monitors for neighborhood and larger scale monitoring, it is important to minimize near-road influences. Table E–5 of this appendix provides the required minimum separation distances between a roadway and at least 90 percent of a monitoring path for various ranges of daily roadway traffic. A site with a monitoring path located closer to a roadway than allowed by the Table E–4 requirements should be classified as microscale or middle scale rather than neighborhood or urban scale. The monitoring path(s) must not cross over a roadway with an average daily traffic count of 10,000 vehicles per day or more. For locations where a monitoring path crosses a roadway with fewer than 10,000 vehicles per day, monitoring agencies must consider the entire segment of the monitoring path in the area of potential atmospheric interference form automobile emissions. Therefore, this calculation must include the length of the monitoring path over the roadway plus any segments of the monitoring path that lie in the area between the roadway and minimum separation distance, as determined from Table E–5 of this appendix. The sum of these distances must not be greater than 10 percent of the total monitoring path length.
3.6 Cumulative Interferences on a Monitoring Path
The cumulative length or portion of a monitoring path that is affected by minor sources, trees, or roadways must not exceed 10 percent of the total monitoring path length.
3.7 Maximum Monitoring Path Length
The monitoring path length must not exceed 1.0 kilometer for open path analyzers in neighborhood, urban, or regional scale. For middle scale monitoring sites, the monitoring path length must not exceed 300 meters. In areas subject to frequent periods of dust, fog, rain, or snow, consideration should be given to a shortened monitoring path length to minimize loss of monitoring data due to these temporary optical obstructions. For certain ambient air monitoring scenarios using open path analyzers, shorter path lengths may be needed in order to ensure that the monitoring site meets the objectives and spatial scales defined in appendix D to this part. The Regional Administrator may require shorter path lengths, as needed on an individual basis, to ensure that the SLAMS sites meet the appendix D requirements. Likewise, the Administrator may specify the maximum path length used at NCore monitoring sites.
3.8 Summary
Table E–6 of this appendix presents a summary of the general requirements for monitoring path siting criteria with respect to distances and heights. Table E–6 requires different elevation distances above the ground for the various pollutants. The discussion in this appendix for each of the pollutants describes reasons for elevating the monitoring path. The differences in the specified range of heights are based on the vertical concentration gradients. For source oriented and near-road monitors, the gradients in the vertical direction are very large for the microscale, so a small range of heights are used. The upper limit of 15 meters is specified for the consistency between pollutants and to allow the use of a monitoring path for monitoring more than one pollutant.
Table E–6 Section 3.8 of Appendix E—Summary of Monitoring Path Siting Criteria
Pollutant Maximum monitoring path length 9 10 Height from ground to 80% of monitoring path 1 8 (meters) Horizontal or vertical distance from supporting structures 2 to 90% of monitoring path 1 8 (meters) Distance from trees to 90% of monitoring path 1 8 (meters) Distance from roadways to monitoring path 1 8 (meters) SO 2 3 4 5 6 <= 300 m for Middle <= 1.0 km for Neighborhood, Urban, and Regional 2.0–15 ≥1.0 ≥10 N/A. CO 4 5 7 <= 300 m for Micro [downtown or street canyon sites] 2.5–3.5 ≥1.0 ≥10 2.0–10 for downtown areas or street canyon microscale. <= 300 m for Micro [Near-Road sites] 2.0–7.0 ≤50 for near-road microscale. Start Printed Page 16402 <= 300 m for Middle 2.0–15 See Table E–5 of this appendix for middle and neighborhood scales. <= 1.0 km for Neighborhood O 3 3 4 5 <= 300 m for Middle <= 1.0 km for Neighborhood, Urban, and Regional 2.0–15 ≥1.0 ≥10 See Table E–4. NO 2 3 4 5 Between 50 m–300 m for Micro (Near-Road) 2.0–7.0 ≤50 for near-road micro-scale. <= 300 m for Middle ≥1.0 ≥10 <= 1.0 km for Neighborhood, Urban, and Regional 2.0–15 See Table E–4. PAMS 3 4 5 Ozone precursors <= 1.0 km for Neighborhood and Urban 2.0–15 ≥1.0 ≥10 See Table E–4. N/A—Not applicable. 1 Monitoring path for open path analyzers is applicable only to middle or neighborhood scale CO monitoring, middle, neighborhood, urban, and regional scale NO 2 monitoring, and all applicable scales for monitoring SO 2 , O 3 , and O 3 precursors. 2 When the monitoring path is located on a rooftop, this separation distance is in reference to walls, parapets, or penthouses located on roof. 3 At least 90 percent of the monitoring path should be greater than 20 meters from the dripline of tree(s) and must be 10-meters from the dripline. 4 Distance from 90 percent of monitoring path to obstacle, such as a building, must be at least twice the height the obstacle protrudes above the monitoring path. Sites not meeting this criterion may be classified as microscale or middle scale ( see text). 5 Must have unrestricted airflow 270 degrees around at least 90 percent of the monitoring path; 180 degrees if the monitoring path is adjacent to the side of a building or a wall for street canyon monitoring. 6 The monitoring path should be away from minor sources, such as furnace or incineration flues. The separation distance is dependent on the height of the minor source's emission point (such as a flue), the type of fuel or waste burned, and the quality of the fuel (sulfur, ash, or lead content). This criterion is designed to avoid undue influences from minor sources. 7 For microscale CO monitoring sites, the monitoring path must be ≥10. meters from a street intersection and preferably at a midblock location. 8 All distances listed are expressed as having 2 significant figures. When rounding is performed to assess compliance with these siting requirements, the distance measurements will be rounded such as to retain at least two significant figures. 9 See section 1.2 of appendix D for definitions of monitoring scales. 10 See section 3.7 of this appendix. 4. Waiver Provisions
Most sampling probes or monitors can be located so that they meet the requirements of this appendix. New sites, with rare exceptions, can be located within the limits of this appendix. However, some existing sites may not meet these requirements and may still produce useful data for some purposes. The EPA will consider a written request from the State, or where applicable local, agency to waive one or more siting criteria for some monitoring sites providing that the State or their designee can adequately demonstrate the need (purpose) for monitoring or establishing a monitoring site at that location.
4.1 For a proposed new site, a waiver may be granted only if both the following criteria are met:
4.1.1 The proposed new site can be demonstrated to be as representative of the monitoring area as it would be if the siting criteria were being met.
4.1.2 The monitor or probe cannot reasonably be located so as to meet the siting criteria because of physical constraints ( e.g., inability to locate the required type of site the necessary distance from roadways or obstructions).
4.2 For an existing site, a waiver may be granted if either the criterion in section 4.1.1 or the criterion in 4.1.2 of this appendix is met.
4.3 Cost benefits, historical trends, and other factors may be used to add support to the criteria in sections 4.1.1 and 4.1.2 of this appendix; however, by themselves, they will not be acceptable reasons for the EPA to grant a waiver. Written requests for waivers must be submitted to the Regional Administrator. Granted waivers must be renewed minimally every 5 years and ideally as part of the network assessment as defined in § 58.10(d). The approval date of the waiver must be documented in the annual monitoring network plan to support the requirements of § 58.10(a)(1) and 58.10(b)(10).
5. References
1. Bryan, R.J., R.J. Gordon, and H. Menck. Comparison of High Volume Air Filter Samples at Varying Distances from Los Angeles Freeway. University of Southern California, School of Medicine, Los Angeles, CA. (Presented at 66th Annual Meeting of Air Pollution Control Association. Chicago, IL. June 24–28, 1973. APCA 73–158.)
2. Teer, E.H. Atmospheric Lead Concentration Above an Urban Street. Master of Science Thesis, Washington University, St. Louis, MO. January 1971.
3. Bradway, R.M., F.A. Record, and W.E. Belanger. Monitoring and Modeling of Resuspended Roadway Dust Near Urban Arterials. GCA Technology Division, Bedford, MA. (Presented at 1978 Annual Meeting of Transportation Research Board, Washington, DC. January 1978.)
4. Pace, T.G., W.P. Freas, and E.M. Afify. Quantification of Relationship Between Monitor Height and Measured Particulate Levels in Seven U.S. Urban Areas. U.S. Environmental Protection Agency, Research Triangle Park, NC. (Presented at 70th Annual Meeting of Air Pollution Control Association, Toronto, Canada. June 20–24, 1977. APCA 77–13.4.)
5. Harrison, P.R. Considerations for Siting Air Quality Monitors in Urban Areas. City of Chicago, Department of Environmental Control, Chicago, IL. (Presented at 66th Annual Meeting of Air Pollution Control Association, Chicago, IL. June 24–28, 1973. APCA 73–161.)
6. Study of Suspended Particulate Measurements at Varying Heights Above Ground. Texas State Department of Health, Air Control Section, Austin, TX. 1970. p.7.
7. Rodes, C.E. and G.F. Evans. Summary of LACS Integrated Pollutant Data. In: Los Angeles Catalyst Study Symposium. U.S. Environmental Protection Agency, Research Triangle Park, NC. EPA Publication No. EPA–600/4–77–034. June 1977.
8. Lynn, D.A. et al. National Assessment of the Urban Particulate Problem: Volume 1, National Assessment. GCA Technology Division, Bedford, MA. U.S. Environmental Protection Agency, Research Triangle Park, NC. EPA Publication No. EPA–450/3–75–024. June 1976.
9. Pace, T.G. Impact of Vehicle-Related Particulates on TSP Concentrations and Rationale for Siting Hi-Vols in the Vicinity of Roadways. OAQPS, U.S. Environmental Protection Agency, Research Triangle Park, NC. April 1978.
10. Ludwig, F.L., J.H. Kealoha, and E. Shelar. Selecting Sites for Monitoring Total Suspended Particulates. Stanford Research Institute, Menlo Park, CA. Prepared for U.S. Environmental Protection Agency, Research Triangle Park, NC. EPA Publication No. EPA–450/3–77–018. June 1977, revised December 1977.
11. Ball, R.J. and G.E. Anderson. Optimum Site Exposure Criteria for SO2 Monitoring. The Center for the Environment and Man, Start Printed Page 16403 Inc., Hartford, CT. Prepared for U.S. Environmental Protection Agency, Research Triangle Park, NC. EPA Publication No. EPA–450/3–77–013. April 1977.
12. Ludwig, F.L. and J.H.S. Kealoha. Selecting Sites for Carbon Monoxide Monitoring. Stanford Research Institute, Menlo Park, CA. Prepared for U.S. Environmental Protection Agency, Research Triangle Park, NC. EPA Publication No. EPA–450/3–75–077. September 1975.
13. Ludwig, F.L. and E. Shelar. Site Selection for the Monitoring of Photochemical Air Pollutants. Stanford Research Institute, Menlo Park, CA. Prepared for U.S. Environmental Protection Agency, Research Triangle Park, NC. EPA Publication No. EPA–450/3–78–013. April 1978.
14. Lead Analysis for Kansas City and Cincinnati, PEDCo Environmental, Inc., Cincinnati, OH. Prepared for U.S. Environmental Protection Agency, Research Triangle Park, NC. EPA Contract No. 66–02–2515, June 1977.
15. Barltrap, D. and C.D. Strelow. Westway Nursery Testing Project. Report to the Greater London Council. August 1976.
16. Daines, R. H., H. Moto, and D. M. Chilko. Atmospheric Lead: Its Relationship to Traffic Volume and Proximity to Highways. Environ. Sci. and Technol., 4:318, 1970.
17. Johnson, D. E., et al. Epidemiologic Study of the Effects of Automobile Traffic on Blood Lead Levels, Southwest Research Institute, Houston, TX. Prepared for U.S. Environmental Protection Agency, Research Triangle Park, NC. EPA–600/1–78–055, August 1978.
18. Air Quality Criteria for Lead. Office of Research and Development, U.S. Environmental Protection Agency, Washington, DC EPA–600/8–83–028 aF–dF, 1986, and supplements EPA–600/8–89/049F, August 1990. (NTIS document numbers PB87–142378 and PB91–138420.)
19. Lyman, D. R. The Atmospheric Diffusion of Carbon Monoxide and Lead from an Expressway, Ph.D. Dissertation, University of Cincinnati, Cincinnati, OH. 1972.
20. Wechter, S.G. Preparation of Stable Pollutant Gas Standards Using Treated Aluminum Cylinders. ASTM STP. 598:40–54, 1976.
21. Wohlers, H.C., H. Newstein and D. Daunis. Carbon Monoxide and Sulfur Dioxide Adsorption On and Description From Glass, Plastic and Metal Tubings. J. Air Poll. Con. Assoc. 17:753, 1976.
22. Elfers, L.A. Field Operating Guide for Automated Air Monitoring Equipment. U.S. NTIS. p. 202, 249, 1971.
23. Hughes, E.E. Development of Standard Reference Material for Air Quality Measurement. ISA Transactions, 14:281–291, 1975.
24. Altshuller, A.D. and A.G. Wartburg. The Interaction of Ozone with Plastic and Metallic Materials in a Dynamic Flow System. Intern. Jour. Air and Water Poll., 4:70–78, 1961.
25. Code of Federal Regulations. 40 CFR 53.22, July 1976.
26. Butcher, S.S. and R.E. Ruff. Effect of Inlet Residence Time on Analysis of Atmospheric Nitrogen Oxides and Ozone, Anal. Chem., 43:1890, 1971.
27. Slowik, A.A. and E.B. Sansone. Diffusion Losses of Sulfur Dioxide in Sampling Manifolds. J. Air. Poll. Con. Assoc., 24:245, 1974.
28. Yamada, V.M. and R.J. Charlson. Proper Sizing of the Sampling Inlet Line for a Continuous Air Monitoring Station. Environ. Sci. and Technol., 3:483, 1969.
29. Koch, R.C. and H.E. Rector. Optimum Network Design and Site Exposure Criteria for Particulate Matter, GEOMET Technologies, Inc., Rockville, MD. Prepared for U.S. Environmental Protection Agency, Research Triangle Park, NC. EPA Contract No. 68–02–3584. EPA 450/4–87–009. May 1987.
30. Burton, R.M. and J.C. Suggs. Philadelphia Roadway Study. Environmental Monitoring Systems Laboratory, U.S. Environmental Protection Agency, Research Triangle Park, N.C. EPA–600/4–84–070 September 1984.
31. Technical Assistance Document for Sampling and Analysis of Ozone Precursors. Atmospheric Research and Exposure Assessment Laboratory, U.S. Environmental Protection Agency, Research Triangle Park, NC 27711. EPA 600/8–91–215. October 1991.
32. Quality Assurance Handbook for Air Pollution Measurement Systems: Volume IV. Meteorological Measurements. Atmospheric Research and Exposure Assessment Laboratory, U.S. Environmental Protection Agency, Research Triangle Park, NC 27711. EPA 600/4–90–0003. August 1989.
33. On-Site Meteorological Program Guidance for Regulatory Modeling Applications. Office of Air Quality Planning and Standards, U.S. Environmental Protection Agency, Research Triangle Park, NC 27711. EPA 450/4–87–013. June 1987F.
34. Johnson, C., A. Whitehill, R. Long, and R. Vanderpool. Investigation of Gaseous Criteria Pollutant Transport Efficiency as a Function of Tubing Material. U.S. Environmental Protection Agency, Research Triangle Park, NC 27711. EPA/600/R–22/212. August 2022.
35. Hannah Halliday, Cortina Johnson, Tad Kleindienst, Russell Long, Robert Vanderpool, and Andrew Whitehill. Recommendations for Nationwide Approval of NafionTM Dryers Upstream of UV-Absorption Ozone Analyzers. U.S. Environmental Protection Agency, Research Triangle Park, NC 27711. EPA/600/R–20/390. November 2020.
Start Amendment Part31. Revise appendix G to part 58 to read as follows:
End Amendment PartAppendix G to Part 58—Uniform Air Quality Index (AQI) and Daily Reporting
1. General Information
2. Reporting Requirements
3. Data Handling
1. General Information
1.1 AQI Overview. The AQI is a tool that simplifies reporting air quality to the public in a nationally uniform and easy to understand manner. The AQI converts concentrations of pollutants, for which the EPA has established a national ambient air quality standard (NAAQS), into a uniform scale from 0–500. These pollutants are ozone (O3), particulate matter (PM2.5, PM10), carbon monoxide (CO), sulfur dioxide (SO2), and nitrogen dioxide (NO2). The scale of the index is divided into general categories that are associated with health messages.
2. Reporting Requirements
2.1 Applicability. The AQI must be reported daily for a metropolitan statistical area (MSA) with a population over 350,000. When it is useful and possible, it is recommended, but not required for an area to report a sub-daily AQI as well.
2.2 Contents of AQI Report.
2.2.1 Content of AQI Report Requirements. An AQI report must contain the following:
a. The reporting area(s) (the MSA or subdivision of the MSA).
b. The reporting period (the day for which the AQI is reported).
c. The main pollutant (the pollutant with the highest index value).
d. The AQI (the highest index value).
e. The category descriptor and index value associated with the AQI and, if choosing to report in a color format, the associated color. Use only the following descriptors and colors for the six AQI categories:
Start Printed Page 16404Table 1 to Section 2 of Appendix G—AQI Categories
For this AQI Use this descriptor And this color 1 0 to 50 “Good” Green. 51 to 100 “Moderate” Yellow. 101 to 150 “Unhealthy for Sensitive Groups” Orange. 151 to 200 “Unhealthy” Red. 201 to 300 “Very Unhealthy” Purple. 301 and above “Hazardous” Maroon1 . 1 Specific color definitions can be found in the most recent reporting guidance (Technical Assistance Document for the Reporting of Daily Air Quality), which can be found at https://www.airnow.gov/publications/air-quality-index/technical-assistance-document-for-reporting-the-daily-aqi/. f. The pollutant specific sensitive groups for any reported index value greater than 100. The sensitive groups for each pollutant are identified as part of the periodic review of the air quality criteria and the NAAQS. For convenience, the EPA lists the relevant groups for each pollutant in the most recent reporting guidance (Technical Assistance Document for the Reporting of Daily Air Quality), which can be found at https://www.airnow.gov/publications/air-quality-index/technical-assistance-document-for-reporting-the-daily-aqi/.
2.2.2 Contents of AQI Report When Applicable. When appropriate, the AQI report may also contain the following, but such information is not required:
a. Appropriate health and cautionary statements.
b. The name and index value for other pollutants, particularly those with an index value greater than 100.
c. The index values for sub-areas of your MSA.
d. Causes for unusually high AQI values.
e. Pollutant concentrations.
f. Generally, the AQI report applies to an area's MSA only. However, if a significant air quality problem exists (AQI greater than 100) in areas significantly impacted by the MSA but not in it (for example, O3 concentrations are often highest downwind and outside an urban area), the report should identify these areas and report the AQI for these areas as well.
2.3. Communication, Timing, and Frequency of AQI Report. The daily AQI must be reported 7 days per week and made available via website or other means of public access. The daily AQI report represents the air quality for the previous day. Exceptions to this requirement are in section 2.4 of this appendix.
a. Reporting the AQI sub-daily is recommended, but not required, to provide more timely air quality information to the public for making health-protective decisions.
b. Submitting hourly data in real-time to the EPA's AirNow (or future analogous) system is recommended, but not required, and assists the EPA in providing timely air quality information to the public for making health-protective decisions.
c. Submitting hourly data for appropriate monitors (referenced in section 3.2 of this appendix) satisfies the daily AQI reporting requirement because the AirNow system makes daily and sub-daily AQI reports widely available through its website and other communication tools.
d. Forecasting the daily AQI provides timely air quality information to the public and is recommended but not required. Sub-daily forecasts are also recommended, especially when air quality is expected to vary substantially throughout the day, like during wildfires. Long-term (multi-day) forecasts can also be made available when useful.
2.4. Exceptions to Reporting Requirements.
a. If the index value for a particular pollutant remains below 50 for a season or year, then it may be excluded from the calculation of the AQI in section 3 of this appendix.
b. If all index values remain below 50 for a year, then the AQI may be reported at the discretion of the reporting agency. In subsequent years, if pollutant levels rise to where the AQI would be above 50, then the AQI must be reported as required in section 2 of this appendix.
c. As previously mentioned in section 2.3 of this appendix, submitting hourly data in real-time from appropriate monitors (referenced in section 3.2 of this appendix) to the EPA's AirNow (or future analogous) system satisfies the daily AQI reporting requirement.
3. Data Handling.
3.1 Relationship of AQI and pollutant concentrations. For each pollutant, the AQI transforms ambient concentrations to a scale from 0 to 500. As appropriate, the AQI is associated with the NAAQS for each pollutant. In most cases, the index value of 100 is associated with the numerical level of the short-term standard ( i.e., averaging time of 24-hours or less) for each pollutant. The index value of 50 is associated with the numerical level of the annual standard for a pollutant, if there is one, at one-half the level of the short-term standard for the pollutant or at the level at which it is appropriate to begin to provide guidance on cautionary language. Higher categories of the index are based on the potential for increasingly serious health effects to occur following exposure and increasing proportions of the population that are likely to be affected. The reported AQI corresponds to the pollutant with the highest calculated AQI. For the purposes of reporting the AQI, the sub-indexes for PM10 and PM2.5 are to be considered separately. The pollutant responsible for the highest index value (the reported AQI) is called the “main” pollutant for that day.
3.2 Monitors Used for AQI Reporting. Concentration data from State/Local Air Monitoring Station (SLAMS) or parts of the SLAMS required by 40 CFR 58.10 must be used for each pollutant except PM. For PM, calculate and report the AQI on days for which air quality data has been measured ( e.g., from continuous PM2.5 monitors required in appendix D to this part). PM measurements may be used from monitors that are not reference or equivalent methods (for example, continuous PM10 or PM2.5 monitors). Detailed guidance for relating non-approved measurements to approved methods by statistical linear regression is referenced here:
Reference for relating non-approved PM measurements to approved methods (Eberly, S., T. Fitz-Simons, T. Hanley, L. Weinstock., T. Tamanini, G. Denniston, B. Lambeth, E. Michel, S. Bortnick. Data Quality Objectives (DQOs) For Relating Federal Reference Method (FRM) and Continuous PM2.5 Measurements to Report an Air Quality Index (AQI). U.S. Environmental Protection Agency, Research Triangle Park, NC. EPA–454/B–02–002, November 2002).
3.3 AQI Forecast. The AQI can be forecasted at least 24-hours in advance using the most accurate and reasonable procedures considering meteorology, topography, availability of data, and forecasting expertise. The guidance document, “Guidelines for Developing an Air Quality (Ozone and PM2.5) Forecasting Program,” can be found at https://www.airnow.gov/publications/weathercasters/guidelines-developing-air-quality-forecasting-program/.
3.4 Calculation and Equations.
a. The AQI is the highest value calculated for each pollutant as follows:
i. Identify the highest concentration among all of the monitors within each reporting area and truncate as follows:
(A) Ozone—truncate to 3 decimal places
PM2.5 —truncate to 1 decimal place
PM10 —truncate to integer
CO—truncate to 1 decimal place
SO2 —truncate to integer
NO2 —truncate to integer
(B) [Reserved]
ii. Using table 2 to this appendix, find the two breakpoints that contain the concentration.
iii. Using equation 1 to this appendix, calculate the index.
iv. Round the index to the nearest integer.
Table 2 to Section 3.4 of Appendix G—Breakpoints for the AQI
These breakpoints Equal these AQI's O 3 (ppm) 8-hour O 3 (ppm) 1-hour1 PM 2.5 (µg/m3 ) 24-hour PM 10 (µg/m3 ) 24-hour CO (ppm) 8-hour SO 2 (ppb) 1-hour NO 2 (ppb) 1-hour AQI Category 0.000–0.054 0.0–9.0 0–54 0.0–4.4 0–35 0–53 0–50 Good. 0.055–0.070 9.1–35.4 55–154 4.5–9.4 36–75 54–100 51–100 Moderate. 0.071–0.085 0.125–0.164 35.5–55.4 155–254 9.5–12.4 76–185 101–360 101–150 Unhealthy for Sensitive Groups. 0.086–0.105 0.165–0.204 55.5–125.4 255–354 12.5–15.4 3 186–304 361–649 151–200 Unhealthy. 0.106–0.200 0.205–0.404 125.5—225.4 355–424 15.5–30.4 3 305–604 650–1249 201–300 Very Unhealthy. Start Printed Page 16405 0.201−(2 ) 0.405+ 225.5+ 425+ 30.5+ 3 605+ 1250+ 301+ 4 Hazardous. 1 Areas are generally required to report the AQI based on 8-hour ozone values. However, there are a small number of areas where an AQI based on 1-hour ozone values would be more precautionary. In these cases, in addition to calculating the 8-hour ozone index value, the 1-hour ozone index value may be calculated, and the maximum of the two values reported. 2 8-hour O 3 concentrations do not define higher AQI values (>301). AQI values > 301 are calculated with 1-hour O 3 concentrations. 3 1-hr SO 2 concentrations do not define higher AQI values (≥200). AQI values of 200 or greater are calculated with 24-hour SO 2 concentration. 4 AQI values between breakpoints are calculated using equation 1 to this appendix. For AQI values in the hazardous category, AQI values greater than 500 should be calculated using equation 1 and the concentration specified for the AQI value of 500. The AQI value of 500 are as follows: O 3 1-hour—0.604 ppm; PM 2.5 24-hour—325.4 µg/m3 ; PM 10 24-hour—604 µg/m3 ; CO ppm—50.4 ppm; SO 2 1-hour—1004 ppb; and NO 2 1-hour—2049 ppb. b. If the concentration is equal to a breakpoint, then the index is equal to the corresponding index value in table 2 to this appendix. However, equation 1 to this appendix can still be used. The results will be equal. If the concentration is between two breakpoints, then calculate the index of that pollutant with equation 1. It should also be noted that in some areas, the AQI based on 1-hour O3 will be more precautionary than using 8-hour values ( see footnote 1 to table 2). In these cases, the 1-hour values as well as 8-hour values may be used to calculate index values and then use the maximum index value as the AQI for O3.
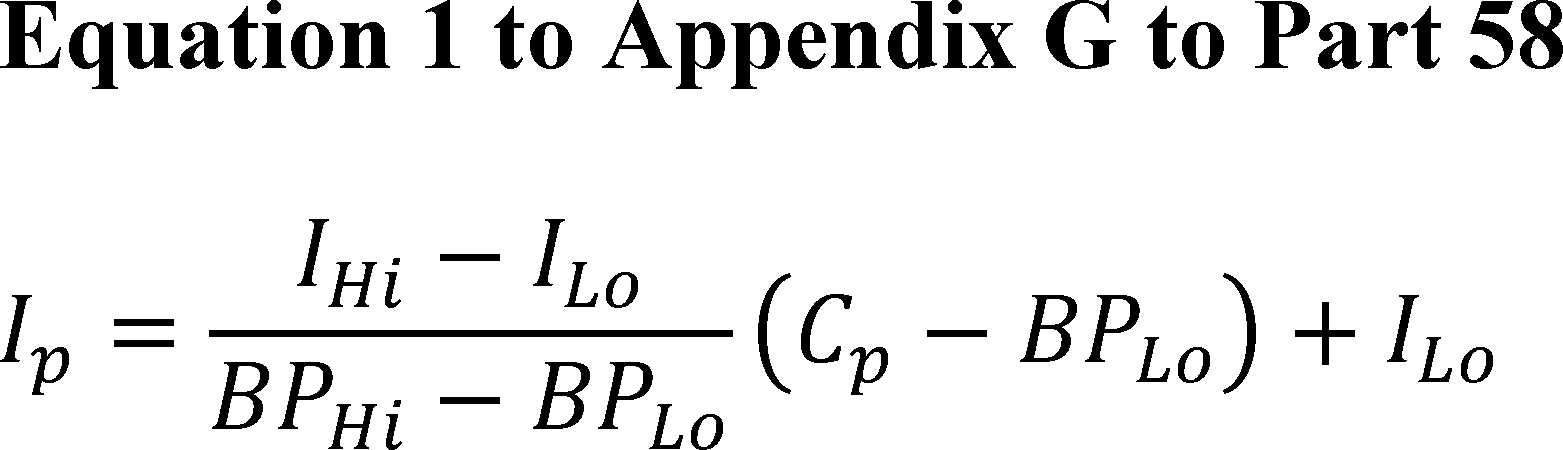
Where:
Ip = the index value for pollutantp.
Cp = the truncated concentration of pollutantp.
BPHi = the breakpoint that is greater than or equal to Cp.
BPLo = the breakpoint that is less than or equal to Cp.
IHi = the AQI value corresponding to BPHi.
Ilo = the AQI value corresponding to BPLo.
c. If the concentration is larger than the highest breakpoint in table 2 to this appendix then the last two breakpoints in table 2 may be used when equation 1 to this appendix is applied.
Example:
d. Using table 2 and equation 1 to this appendix, calculate the index value for each of the pollutants measured and select the one that produces the highest index value for the AQI. For example, if a PM10 value of 210 µg/m3 is observed, a 1-hour O3 value of 0.156 ppm, and an 8-hour O3 value of 0.130 ppm, then do this:
i. Find the breakpoints for PM10 at 210 µg/m3 as 155 µg/m3 and 254 µg/m3 , corresponding to index values 101 and 150;
ii. Find the breakpoints for 1-hour O3 at 0.156 ppm as 0.125 ppm and 0.164 ppm, corresponding to index values 101 and 150;
iii. Find the breakpoints for 8-hour O3 at 0.130 ppm as 0.116 ppm and 0.374 ppm, corresponding to index values 201 and 300;
iv. Apply equation 21 to this appendix for 210 µg/m3 , PM10:
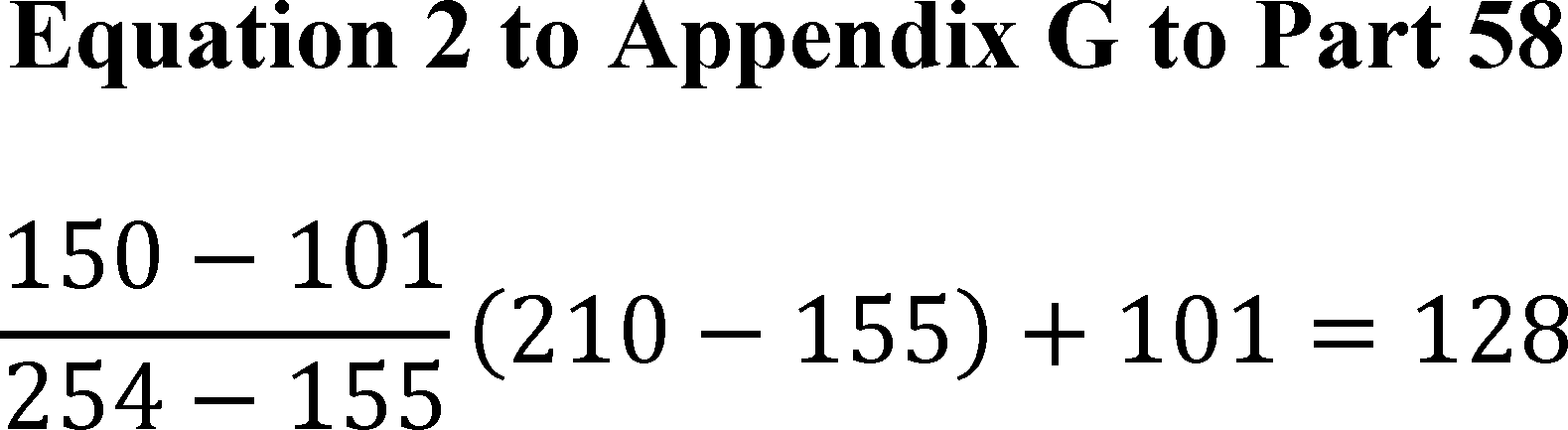
v. Apply equation 3 to this appendix for 0.156 ppm, 1-hour O3:
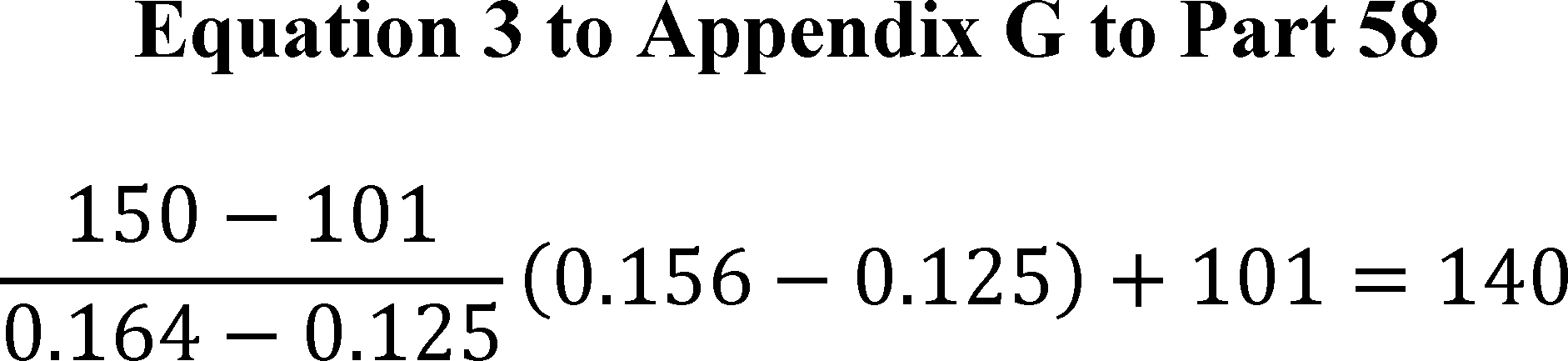
vi. Apply equation 4 to this appendix for 0.130 ppm, 8-hour O3:
Start Printed Page 16406
vii. Find the maximum, 206. This is the AQI. A minimal AQI report could read: “Today, the AQI for my city is 206, which is Very Unhealthy, due to ozone.” It would then reference the associated sensitive groups.
End Supplemental InformationFootnotes
1. The press release for this announcement is available at: https://www.epa.gov/newsreleases/epa-reexamine-health-standards-harmful-soot-previous-administration-left-unchanged.
Back to Citation2. In 2021, the Administrator announced his decision to reestablish the membership of the CASAC. The Administrator selected seven members to serve on the chartered CASAC, and appointed a PM CASAC panel to support the chartered CASAC's review of the draft ISA Supplement and the draft PA as a part of this reconsideration (see section I.C.6.b below for more information).
Back to Citation3. More information regarding the CASAC review of the draft ISA Supplement and the draft PA, including opportunities for public comment, can be found in the following Federal Register notices: 86 FR 54186, September 30, 2021; 86 FR 52673, September 22, 2021; 86 FR 56263, October 8, 2021; 87 FR 958, January 7, 2022.
Back to Citation4. Consistent with the 2016 Integrated Review Plan (U.S. EPA, 2016), other welfare effects of PM, such as ecological effects, are being considered in the separate, on-going review of the secondary NAAQS for oxides of nitrogen, oxides of sulfur and PM. Accordingly, the public welfare protection provided by the secondary PM standards against ecological effects such as those related to deposition of nitrogen- and sulfur-containing compounds in vulnerable ecosystems is being considered in that separate review. Thus, the Administrator's conclusion in this reconsideration of the 2020 final decision is focused only and specifically on the adequacy of public welfare protection provided by the secondary PM standards from effects related to visibility, climate, and materials and hereafter “welfare effects” refers to those welfare effects.
Back to Citation5. The legislative history of section 109 indicates that a primary standard is to be set at “the maximum permissible ambient air level . . . which will protect the health of any [sensitive] group of the population,” and that for this purpose “reference should be made to a representative sample of persons comprising the sensitive group rather than to a single person in such a group.” S. Rep. No. 91–1196, 91st Cong., 2d Sess. 10 (1970).
Back to Citation6. Under CAA section 302(h) (42 U.S.C. 7602(h)), effects on welfare include, but are not limited to, “effects on soils, water, crops, vegetation, manmade materials, animals, wildlife, weather, visibility, and climate, damage to and deterioration of property, and hazards to transportation, as well as effects on economic values and on personal comfort and well-being.”
Back to Citation7. Prior to the review initiated in 2007 (see below), the AQCD provided the scientific foundation ( i.e., the air quality criteria) for the NAAQS. Beginning in that review, the Integrated Science Assessment (ISA) has replaced the AQCD.
Back to Citation8. PM10 refers to particles with a nominal mean aerodynamic diameter less than or equal to 10 µm. More specifically, 10 µm is the aerodynamic diameter for which the efficiency of particle collection is 50 percent.
Back to Citation9. The 1997 annual PM2.5 standard was compared with measurements made at the community-oriented monitoring site recording the highest concentration or, if specific constraints were met, measurements from multiple community-oriented monitoring sites could be averaged ( i.e., “spatial averaging”). In the last review (completed in 2012) the EPA replaced the term “community-oriented” monitor with the term “area-wide” monitor. Area-wide monitors are those sited at the neighborhood scale or larger, as well as those monitors sited at micro- or middle-scales that are representative of many such locations in the same core-based statistical area (CBSA) (78 FR 3236, January 15, 2013).
Back to Citation10. Prior to the review initiated in 2007, the Staff Paper presented the EPA staff's considerations and conclusions regarding the adequacy of existing NAAQS and, when appropriate, the potential alternative standards that could be supported by the evidence and information. More recent reviews present this information in the Policy Assessment.
Back to Citation11. The history of the NAAQS review process, including revisions to the process, is discussed at https://www.epa.gov/naaqs/historical-information-naaqs-review-process.
Back to Citation12. The EPA also eliminated the option for spatial averaging.
Back to Citation13. Consistent with the primary standard, the EPA eliminated the option for spatial averaging with the annual standard.
Back to Citation14. Announcement available at: https://www.regulations.gov/document/EPA-HQ-OAR-2015-0072-0223.
Back to Citation15. See California v. EPA, (D.C. Cir., No. 21–2014 consolidated with Nos. 21–1027, 21–1054).
Back to Citation18. The press release for this announcement is available at: https://www.epa.gov/newsreleases/epa-reexamine-health-standards-harmful-soot-previous-administration-left-unchanged.
Back to Citation19. The list of provisionally considered studies is included in Appendix A to the 2020 Response to Comments document (U.S. EPA, 2020a).
Back to Citation20. The press release for this announcement is available at: https://www.epa.gov/newsreleases/administrator-regan-directs-epa-reset-critical-science-focused-federal-advisory.
Back to Citation21. The press release for this announcement is available at: https://www.epa.gov/newsreleases/epa-announces-selections-charter-members-clean-air-scientific-advisory-committee.
22. The list of members of the chartered CASAC and their biosketches are available at: https://casac.epa.gov/ords/sab/r/sab_apex/casac/mems?p14_committeeon=2021%20CASAC%20PM%20Panel&session=17433386035954.
Back to Citation23. The list of members of the PM CASAC panel and their biosketches are available at: https://casac.epa.gov/ords/sab/f?p=105:14:9979229564047:::14:P14_COMMITTEEON:2021%20CASAC%20PM%20Panel.
Back to Citation24. As described in section 1.2.1 of the ISA Supplement: “In considering the public health protection provided by the current primary PM2.5 standards, and the protection that could be provided by alternatives, [the U.S. EPA, within the 2020 PM PA] emphasized health outcomes for which the ISA determined that the evidence supports either a ` causal ' or a ` likely to be causal ' relationship with PM2.5 exposures” (U.S. EPA, 2020b). Although the 2020 PA initially focused on this broader set of evidence, the basis of the discussion on potential alternative standards primarily focused on health effect categories where the 2019 PM ISA concluded a ` causal relationship ' ( i.e., short- and long-term PM2.5 exposure and cardiovascular effects and mortality) as reflected in Figures 3–7 and 3–8 of the 2020 PA (U.S. EPA, 2020b).”
Back to Citation25. As described in section 1.2.1 of the ISA Supplement: “The 2019 PM ISA concluded a ` causal relationship ' for each of the welfare effects categories evaluated ( i.e., visibility, climate effects and materials effects). While the 2020 PA considered the broader set of evidence for these effects, for climate effects and material effects, it concluded that there remained `substantial uncertainties with regard to the quantitative relationships with PM concentrations and concentration patterns that limit[ed] [the] ability to quantitatively assess the public welfare protection provided by the standards from these effects' (U.S. EPA, 2020b).”
Back to Citation26. These key scientific topics include experimental studies conducted at near-ambient concentrations, epidemiologic studies that employed alternative methods for confounder control or conducted accountability analyses, studies that assess the relationship between PM2.5 exposure and severe acute respiratory syndrome coronavirus 2 (SARS–CoV–2) infection and coronavirus disease 2019 (COVID–19) death; and in accordance with recent EPA goals on addressing environmental justice, studies that examine disparities in PM2.5 exposure and the risk of health effects by race/ethnicity or socioeconomic status (SES) (U.S. EPA, 2022a, section 1.2.1).
Back to Citation27. In addition to the 2020 review's opening “call for information” (79 FR 71764, December 3, 2014), the 2019 ISA identified and evaluated studies and reports that have undergone scientific peer review and were published or accepted for publication between January 1, 2009, through approximately January 2018 (U.S. EPA, 2019a, p. ES–2). References that are cited in the 2019 ISA, the references that were considered for inclusion but not cited, and electronic links to bibliographic information and abstracts can be found at: https://hero.epa.gov/hero/particulate-matter.
Back to Citation28. As described above, the ISA Supplement represents an evaluation of recent studies that are of greatest policy relevance and utility to the reconsideration of the 2020 final decision on the PM NAAQS (U.S. EPA, 2022a).
Back to Citation29. See also: https://www.usda.gov/sites/default/files/documents/usda-epa-doi-cdc-mou.pdf.
Back to Citation31. For PM2.5, neighborhood scale is defined at 40 CFR part 58, appendix D, 4.7.1(c)(3) as follows: Measurements in this category would represent conditions throughout some reasonably homogeneous urban sub-region with dimensions of a few kilometers and of generally more regular shape than the middle scale. Homogeneity refers to the particulate matter concentrations, as well as the land use and land surface characteristics. Much of the PM2.5 exposures are expected to be associated with this scale of measurement. In some cases, a location carefully chosen to provide neighborhood scale data would represent the immediate neighborhood as well as neighborhoods of the same type in other parts of the city. PM2.5 sites of this kind provide good information about trends and compliance with standards because they often represent conditions in areas where people commonly live and work for periods comparable to those specified in the NAAQS. In general, most PM2.5 monitoring in urban areas should have this scale.
Back to Citation32. 40 CFR part 58, app. D, 4.7.1(b)(2).
Back to Citation33. See https://www.epa.gov/air-trends/particulate-matter-pm25-trends for up-to-date PM2.5 trends information.
Back to Citation34. A design value is considered valid if it meets the data handling requirements given in appendix N to 40 CFR part 50.
Back to Citation35. The Elizabeth Lab site in Elizabeth, NJ, is situated approximately 30 meters from travel lanes of the Interchange 13 toll plaza of the New Jersey Turnpike and within 200 meters of travel lanes for Interstate 278 and the New Jersey Turnpike.
Back to Citation36. The form of the current 24-hour PM10 standard is one-expected-exceedance, averaged over three years.
Back to Citation37. For more information, see https://www.epa.gov/air-trends/particulate-matter-pm10-trends#pmnat.
Back to Citation38. PM from dust emissions in the National Emissions Inventory (NEI) remain fairly consistent from year-to-year, except when there are severe weather incursions or there is a dust event that transports or causes major local dust storms to occur (particularly in the western U.S.). These dust events and weather incursions needed to effect dust emissions on a national level are not common and only seldomly occur. In the emissions trends analysis presented in the 2022 PA (U.S. EPA, 2022b, section 2.1.1), dust is included in the NEI sector labeled “miscellaneous.”
Back to Citation39. For the annual PM2.5 standard, design values are calculated as the annual arithmetic mean PM2.5 concentration, averaged over 3 years. For the 24-hour standard, design values are calculated as the 98th percentile of the annual distribution of 24-hour PM2.5 concentrations, averaged over three years (appendix N of 40 CFR part 50).
Back to Citation40. This analysis includes an updated version of the surface used in Di et al. (2016). Predictions in Di et al. (2016) were for 2000 to 2012 using a neural network model. The Di et al. (2019) study improved on that effort in several ways. First, a generalized additive model was used that accounted for geographic variations in performance to combine predictions from three models (neural network, random forest, and gradient boosting) to make the final optimal PM2.5 predictions. Second, the datasets were updated that were used in model training and included additional variables such as 12-km CMAQ modeling as predictors. Finally, more recent years were included in the Di et al. (2019) study.
Back to Citation41. The HA2020 field is based on the V4.NA.03 product available at: https://sites.wustl.edu/acag/datasets/surface-pm2-5/. The name “HA2020” comes from the references for this product (Hammer et al., 2020; van Donkelaar et al., 2019).
Back to Citation42. For the national scale, 3-year averages of the average annual PM2.5 concentrations generally range from about 5.3 µg/m3. to 8.1 µg/m3. , compared to the CBSA scale, which ranges from 5.7 µg/m3. to 8.7 µg/m3. . (U.S. EPA, 2022b, section 2.3.3.2.4, Table 2–6).
Back to Citation43. For this analysis, the 2022 PA includes CBSAs with three or more valid design values for the 3-year period. The regulatory design values for the CBSAs were calculated for each 3-year period for the CBSAs with 3 or more design values in each of the 3-year periods. Using the maximum design value for each CBSA and by each 3-year period, the ratio of maximum design values to modeled average annual PM2.5 concentrations were calculated, for each 3-year period. More details about the analytical methods used for this analysis are described in section A.6 of Appendix A in the 2022 PA (U.S. EPA, 2022b).
Back to Citation44. Sources that contribute to natural background PM include dust from the wind erosion of natural surfaces, sea salt, wildland fires, primary biological aerosol particles such as bacteria and pollen, oxidation of biogenic hydrocarbons such as isoprene and terpenes to produce secondary organic aerosols (SOA), and geogenic sources such as sulfate formed from volcanic production of SO2 and oceanic production of dimethyl-sulfide (U.S. EPA, 2022b, section 2.4). While most of these sources release or contribute predominantly to fine aerosol, some sources including windblown dust, and sea salt also produce particles in the coarse size range (U.S. EPA, 2019a, section 2.3.3).
Back to Citation45. In addition to the 2020 review's opening “call for information” (79 FR 71764, December 3, 2014), the 2019 ISA identified and evaluated studies and reports that have undergone scientific peer review and were published or accepted for publication between January 1, 2009, through approximately January 2018 (U.S. EPA, 2019a, p. ES–2). References that are cited in the 2019 ISA, the references that were considered for inclusion but not cited, and electronic links to bibliographic information and abstracts can be found at: https://hero.epa.gov/hero/particulate-matter.
Back to Citation46. Short-term exposures are defined as those exposures occurring over hours up to 1 month, whereas long-term exposures are defined as those exposures occurring over 1 month to years (U.S. EPA, 2019a, section P.3.1).
Back to Citation47. The ISA Supplement represents an evaluation of recent studies that are of greatest policy relevance to the reconsideration of the 2020 final decision on the PM NAAQS. Specifically, the ISA Supplement focuses on studies of health effects for which the evidence in the 2019 ISA supported a “causal relationship” ( i.e., short- and long-term PM2.5 exposure and mortality and cardiovascular effects) because those were the health effects that were most useful in informing conclusions in the 2020 PA. The ISA Supplement does not include an evaluation of studies for other PM2.5 -related health effects (U.S. EPA, 2022a).
Back to Citation48. As noted in section I.A above, the legislative history describes such protection for the sensitive group of individuals and not for a single person in the sensitive group (see S. Rep. No. 91–1196, 91st Cong, 2d Sess. 10 [1970]); see also Am. Lung Ass'n v. EPA, 134 F.3d 388, 389 (D.C. Cir. 1998).
Back to Citation49. The median of the study-reported mean (or median) PM2.5 concentrations is 13.3 µg/m3. , which was also above the level of the existing standard.
Back to Citation50. As noted in the ISA Supplement (U.S. EPA, 2022a, p. 1–3): “In the peer-reviewed literature, these epidemiologic studies are often referred to as causal inference studies or studies that used causal modeling methods. For the purposes of this Supplement, this terminology is not used to prevent confusion with the main scientific conclusions ( i.e., the causality determinations) presented within an ISA. In addition, as is consistent with the weight-of-evidence framework used within ISAs and discussed in the Preamble to the Integrated Science Assessments, an individual study on its own cannot inform causality, but instead represents a piece of the overall body of evidence.”
Back to Citation51. As with the epidemiologic studies for long- and short-term PM2.5 exposure and mortality and cardiovascular effects, epidemiologic studies of exposure or risk disparities and SARS–CoV–2 infection and/or COVID–19 death were limited to those conducted in the U.S. and Canada.
Back to Citation52. In this reconsideration of the PM NAAQS, the EPA considers the full body of health evidence, placing the greatest emphasis on the health effects for which the evidence has been judged in the 2019 ISA to demonstrate a “causal” or “likely to be causal” relationship with PM2.5 exposures.
Back to Citation53. The majority of these studies examined non-accidental mortality outcomes, though some Medicare studies lack cause-specific death information and, therefore, examine total mortality.
Back to Citation54. In public comments on the 2019 draft PA, the authors of the Pun et al. (2017) study further note that “the presence of unmeasured confounding. . .was expected given that we did not control for several potential confounders that may impact PM2.5 -mortality associations, such as smoking, socio-economic status (SES), gaseous pollutants, PM2.5 components, and long-term time trends in PM2.5 ” and that “spatial confounding may bias mortality risks both towards and away from the null” (Docket ID EPA–HQ–OAR–2015–0072–0065; accessible in https://www.regulations.gov/).
Back to Citation55. As detailed in the Preface to the ISA, risk estimates are for a 10 µg/m3. increase in 24-hour avg PM2.5 concentrations, unless otherwise noted (U.S. EPA, 2019a).
Back to Citation56. Lee et al. (2015) restrict exposures below 35 μg/m3. only in areas with annual average concentrations <12 μg/m3. . Additionally, Lee et al. (2015) also report that positive and statistically significant associations between short-term PM2.5 exposures and mortality persist in analyses restricted to areas with long-term concentrations below 12 μg/m3. .
Back to Citation57. As noted above for mortality, uncertainty in the shape of the C–R relationship increases near the upper and lower ends of the distribution due to limited data.
Back to Citation58. Some animal studies included in the 2009 ISA examined exposures to mixtures, such as motor vehicle exhaust or woodsmoke. In these studies, it was unclear if the resulting cardiovascular effects could be attributed specifically to the fine particle component of the mixture.
Back to Citation59. While there is no exact corollary within the 2019 ISA for these types of studies, the 2019 ISA presented evidence that evaluates the potential relationship between short- and long-term PM2.5 exposure and respiratory infection (U.S. EPA, 2022a, section 5.1.5 and 5.2.6). Studies assessed in the 2019 ISA report some evidence of positive associations between short-term PM2.5 and hospital admissions and ED visits for respiratory infections, however the interpretation of these studies is complicated by the variability in the type of respiratory infection outcome examined (U.S. EPA, 2022a, Figure 5–7). In the 2019 ISA, studies of long-term PM2.5 exposure were limited and while there were some positive associations reported, there was minimal overlap in respiratory infection outcomes examined across studies. Exposure to PM2.5 has been shown to impair host defense, specifically altering macrophage function, providing a biological pathway by which PM2.5 exposure could lead to respiratory infection (U.S. EPA, 2022a, sections 5.1.1 and 5.1.5.) There is some additional evidence that PM2.5 exposure can lead to decreases in an individual's immune response, which can subsequently facilitate replication of respiratory viruses (Bourdrel et al., 2021).
Back to Citation60. As described in the 2019 ISA, other factors that have the potential to contribute to increased risk include obesity, diabetes, genetic factors, smoking status, sex, diet, and residential location (U.S. EPA, 2019, chapter 12).
Back to Citation61. Children, as used throughout this document, generally refers to those younger than 18 years old.
Back to Citation62. As described in more detail in section 5 of the Preamble to the ISAs, judgments regarding causality take into consideration a number of aspects when evaluating the available scientific evidence (U.S. EPA, 2015, Table I). In reaching conclusions regarding causality, “evidence is evaluated for major outcome categories or groups of related endpoints ( e.g., respiratory effects, vegetation growth), integrating evidence from across disciplines, and evaluating the coherence of evidence across a spectrum of related endpoints” (U.S. EPA, 2015, p. 24). Furthermore, “[i]n drawing judgments regarding causality for the criteria air pollutants, the ISA focuses on evidence of effects in the range of relevant pollutant exposures or doses and not on determination of causality at any dose. Emphasis is placed on evidence of effects at doses ( e.g., blood Pb concentration) or exposures ( e.g., air concentrations) that are relevant to, or somewhat above, those currently experienced by the population. The extent to which studies of higher concentrations are considered varies by pollutant and major outcome category, but generally includes those with doses or exposures in the range of one to two orders of magnitude above current or ambient conditions to account for intra-species variability and toxicokinetic or toxicodynamic differences between experimental animals and humans. Studies that use higher doses or exposures may also be considered to the extent that they provide useful information to inform understanding of mode of action, inter-species differences, or factors that may increase risk of effects for a population and if biological mechanisms have not been demonstrated to differ based on exposure concentration. Thus, a causality determination is based on weight-of-evidence evaluation for health or welfare effects, focusing on the evidence from exposures or doses generally ranging from recent ambient concentrations to one or two orders of magnitude above recent ambient concentrations” (U.S. EPA, 2015, p. 24).
Back to Citation63. In contrast, controlled human exposure studies provide little evidence for respiratory effects following short-term PM2.5 exposures (U.S. EPA, 2019a, section 5.1, Table 5–18). Therefore, this section focuses on cardiovascular effects evaluated in controlled human exposure studies of PM2.5 exposure.
Back to Citation64. The ATS/ERS described its 2017 statement as one “intended to provide guidance to policymakers, clinicians and public health professionals, as well as others who interpret the scientific evidence on the health effects of air pollution for risk management purposes” and further notes that “considerations as to what constitutes an adverse health effect, in order to provide guidance to researchers and policymakers when new health effects markers or health outcome associations might be reported in future.” The most recent policy statement by the ATS, which once again broadens its discussion of effects, responses and biomarkers to reflect the expansion of scientific research in these areas, reiterates that concept, conveying that it does not offer “strict rules or numerical criteria, but rather proposes considerations to be weighed in setting boundaries between adverse and nonadverse health effects,” providing a general framework for interpreting evidence that proposes a “set of considerations that can be applied in forming judgments” for this context (Thurston et al., 2017).
Back to Citation65. Similar analyses of 4-hour and 5-hour PM2.5 concentrations are presented in Appendix A, Figure A–2 and Figure A–3, respectively of the 2022 PA (U.S. EPA, 2022b).
Back to Citation66. As detailed in the 2011 PA, we note the interrelatedness of the distributional statistics and a range of one standard deviation around the mean which represents approximately 68% of normally distributed data, and in that one standard deviation below the mean falls between the 25th and 10th percentiles (U.S. EPA, 2011, p. 2–71; U.S. EPA, 2005, p. 5–22).
Back to Citation67. In setting a standard level that would require the design value monitor to meet a level equal to the study-reported mean PM2.5 concentrations would generally result in lower concentrations of PM2.5 across the entire area, such that even those people living near an area design value monitor (where PM concentrations are generally highest) will be exposed to PM2.5 concentrations below the air quality conditions reported in the epidemiologic studies.
Back to Citation68. More detailed information about hybrid model methods and performance is described in section 2.3.3.2 of the 2022 PA (U.S. EPA, 2022b).
Back to Citation69. In those studies that use ground-based monitors alone to estimate long- or short-term PM2.5 concentrations, approaches include: (1) PM2.5 concentrations from a single monitor within a city/county; (2) average of PM2.5 concentrations across all monitors within a city/county or other defined study area ( e.g., CBSA); or (3) population-weighted averages of exposures. Once the study location average PM2.5 concentration is calculated, the study-reported long-term average is derived by averaging daily/annual PM2.5 concentrations across all study locations over the entire study period.
Back to Citation70. Detailed information on the methods by which mean PM2.5 concentrations are calculated in key monitor- and hybrid model-based U.S. and Canadian epidemiologic studies are presented in Tables 3–6 through 3–9 in the 2022 PA (U.S. EPA, 2022b).
Back to Citation71. More details on the evaluation of the two hybrid modeling approaches is provided in section 2.3.3.2.4 of the 2022 PA (U.S. EPA, 2022b).
Back to Citation72. The annual PM2.5 concentrations for the population-weighted averages ranged from 8.2–10.2 μg/m3. , while those that do not apply population weighting ranged from 7.0–8.6 μg/m3. . Average maximum annual design values ranged from 9.5 to 11.7 μg/m3. .
Back to Citation73. As described in the Preamble to the ISAs (U.S. EPA, 2015), “the U.S. EPA emphasizes the importance of examining the pattern of results across various studies and does not focus solely on statistical significance or the magnitude of the direction of the association as criteria of study reliability. Statistical significance is influenced by a variety of factors including, but not limited to, the size of the study, exposure and outcome measurement error, and statistical model specifications. Statistical significance may be informative; however, it is just one of the means of evaluating confidence in the observed relationship and assessing the probability of chance as an explanation. Other indicators of reliability such as the consistency and coherence of a body of studies as well as other confirming data may be used to justify reliance on the results of a body of epidemiologic studies, even if results in individual studies lack statistical significance. Traditionally, statistical significance is used to a larger extent to evaluate the findings of controlled human exposure and animal toxicological studies. Understanding that statistical inferences may result in both false positives and false negatives, consideration is given to both trends in data and reproducibility of results. Thus, in drawing judgments regarding causality, the U.S. EPA emphasizes statistically significant findings from experimental studies, but does not limit its focus or consideration to statistically significant results in epidemiologic studies.”
Back to Citation74. This emphasis on studies conducted in the U.S. or Canada is consistent with the approach in the 2012 and 2020 reviews of the PM NAAQS (U.S. EPA, 2011, section 2.1.3; U.S. EPA, 2020b, section 3.2.3.2.1) and with approaches taken in other NAAQS reviews. However, the importance of studies in the U.S., Canada, and other countries in informing an ISA's considerations of the weight of the evidence that informs causality determinations is recognized.
Back to Citation75. The cohorts examined in the studies included in Figure 3–4 to Figure 3–7 of the 2022 PA include large numbers of individuals in the general population, and often also include those populations identified as at-risk ( i.e., children, older adults, minority populations, and individuals with pre-existing cardiovascular and respiratory disease).
Back to Citation76. For some studies of long-term PM2.5 exposures, exposure is estimated from air quality data corresponding to only part of the study period, often including only the later years of the health data, and are not likely to reflect the full ranges of ambient PM2.5 concentrations that contributed to reported associations. While this approach can be reasonable in the context of an epidemiologic study that is evaluating health effect associations with long-term PM2.5 exposures, under the assumption that spatial patterns in PM2.5 concentrations are not appreciably different during time periods for which air quality information is not available ( e.g., Chen et al., 2016), the 2022 PA focuses on the distribution of ambient PM2.5 concentrations that could have contributed to reported health outcomes. Therefore, the 2022 PA identifies studies as key epidemiologic studies when the years of air quality data and health data overlap in their entirety.
Back to Citation77. Such studies are identified as those that use hybrid modeling approaches for which recent methods and models were used ( e.g., recent versions and configurations of the air quality models); studies that are fused with PM2.5 data from national monitoring networks ( i.e., FRM/FEM data); and studies that reported a thorough model performance evaluation for core years of the study.
Back to Citation78. Canadian studies that use ground-based monitors estimate long- or short-term PM2.5 exposures are found in Figure 3–9 of the 2022 PA, including concentrations corresponding to the 25th and 10th percentiles of estimated exposures or health events, when available (U.S. EPA, 2022b).
Back to Citation79. That is, 25% of the total health events occurred in study locations with mean PM2.5 concentrations ( i.e., averaged over the study period) below the 25th percentiles identified in Figure 3–8 of the 2022 PA and 10% of the total health events occurred in study locations with mean PM2.5 concentrations below the 10th percentiles identified.
Back to Citation80. For most studies in Figure 2 below (Figure 3–14 in the 2022 PA), 25th percentiles of exposure estimates are presented. The exception is Di et al. (2017b), for which Figure 2 (U.S. EPA, 2022b, Figure 3–14) presents the short-term PM2.5 exposure estimates corresponding to the 25th and 10th percentiles of deaths in the study population ( i.e., 25% and 10% of deaths occurred at concentrations below these concentrations). In addition, the authors of Di et al. (2017b) provided population-weighted exposure values. The 10th and 25th percentiles of these population-weighted exposure estimates are 7.9 and 9.5 μg/m3. , respectively.
Back to Citation81. Overall mean (or median) PM2.5 concentrations reported in key Canadian studies that use model-based approaches to estimate long- or short-term PM2.5 concentrations and the concentrations corresponding to the 25th and 10th percentiles of estimated exposures or health events, when available are found in Figure 3–9 of the 2022 PA (U.S. EPA, 2022b).
Back to Citation82. This is generally consistent with, but slightly below, the lowest study-reported mean PM2.5 concentration from monitor-based studies available in the 2020 PA, which was 10.7 μg/m3. (U.S. EPA, 2020a, Figure 3–7).
Back to Citation83. In the one study that reports 25th percentile exposure estimates of 4.6 µg/m3. (Shi et al., 2016), the authors report that most deaths occurred at or above the 75th percentile of annual exposure estimates ( i.e., 10 μg/m3. ). The short-term exposure estimates accounting for most deaths are not presented in the published study.
Back to Citation84. As noted in the ISA Supplement (U.S. EPA, 2022a, p. 1–3): “In the peer-reviewed literature, these epidemiologic studies are often referred to as alternative methods for confounder control. For the purposes of this Supplement, this terminology is not used to prevent confusion with the main scientific conclusions ( i.e., the causality determinations) presented within an ISA. In addition, as is consistent with the weight-of-evidence framework used within ISAs and discussed in the Preamble to the Integrated Science Assessments, an individual study on its own cannot inform causality, but instead represents a piece of the overall body of evidence.”
Back to Citation85. Given the nature of these studies, the majority tend to focus on time periods in the past during which ambient PM2.5 concentrations were substantially higher than those measured more recently ( e.g., see U.S. EPA, 2022b, Figure 2–16).
Back to Citation86. For the annual PM2.5 standard, design values are calculated as the annual arithmetic mean PM2.5 concentration, averaged over 3 years. For the 24-hour standard, design values are calculated as the 98th percentile of the annual distribution of 24-hour PM2.5 concentrations, averaged over three years (Appendix N of 40 CFR part 50).
Back to Citation87. Additional detail regarding the selection of epidemiologic studies and specification of C–R functions is provided in the 2022 PA (U.S. EPA, 2022b, Appendix C, section C.1.1).
Back to Citation88. While the 2019 ISA also found that evidence supports the determination of a “causal relationship” between long- and short-term PM2.5 exposures and cardiovascular effects, cardiovascular mortality was not included as a health outcome as it will be captured in the estimates of all-cause mortality.
Back to Citation89. For these areas, the annual standard is the “controlling standard” because when air quality is adjusted to simulate just meeting the current or potential alternative annual standards, that air quality also would meet the 24-hour standard being evaluated.
Back to Citation90. For these areas, the 24-hour standard is the controlling standard because when air quality is adjusted to simulate just meeting the current or potential alternative 24-hour standards, that air quality also would meet the annual standard being evaluated. Some areas classified as being controlled by the 24-hour standard also violate the annual standard.
Back to Citation91. In these 6 areas, the controlling standard depended on the air quality adjustment method used and/or the standard scenarios evaluated.
Back to Citation92. As noted in the ISA Supplement: “In the peer-reviewed literature, these epidemiologic studies are often referred to as causal inference studies or studies that used causal modeling methods. For the purposes of this Supplement, this terminology is not used to prevent confusion with the main scientific conclusions ( i.e., the causality determinations) presented within an ISA. In addition, as is consistent with the weight-of-evidence framework used within ISAs and discussed in the Preamble to the Integrated Science Assessments, an individual study on its own cannot inform causality, but instead represents a piece of the overall body of evidence” (U.S. EPA, 2022a, p. 1–3).
Back to Citation93. The EPA notes that, in considering the additional scientific evidence available in this reconsideration, one member of the CASAC who reviewed both the 2019 draft PA and the 2021 draft PA found that the available scientific and quantitative information available in this reconsideration supported revising the level of the primary annual PM2.5 standard, whereas he recommended retaining the standard during the review of the 2019 draft PA.
Back to Citation94. In providing advice on the 2019 draft PA, the CASAC did not weigh in specifically on the averaging time of the primary 24-hour PM2.5 standard but did recommend that the standard be retained because the available evidence does not call into question its adequacy (Cox, 2019b, p. 3 of consensus letter).
Back to Citation95. The CASAC did not provide advice or recommendations regarding the forms of the primary PM2.5 standards in their review of the 2019 draft PA (Cox, 2019b).
Back to Citation96. The Administrator notes that, in their review of the 2021 draft PA, a majority of members of the CASAC noted that there are some limitations for this approach “for the purpose of informing the adequacy of the standards” (Sheppard, 2022a, p. 8 of consensus responses) and advised that future reviews should include evaluation of other metrics, including the distribution of concentrations reported in epidemiologic studies and in analyses restricting concentrations to below the current standard level. The Administrator also notes that, in their review of the 2019 draft PA, the CASAC lacked consensus on the inferences to be drawn from the epidemiologic evidence, with a majority of CASAC having concerns about confounding, error and bias and concluding that newer studies did not provide a basis for revising the current standards, while a minority concluded that the evidence, including more recent studies showing associations in areas with average long-term PM2.5 concentrations below the current annual standard, supported their conclusion that the current standards are inadequate (Cox, 2019b, pp. 8–9 of consensus responses).
Back to Citation97. The Wang et al. (2017) study only reports the 25th percentile of the estimated PM2.5 concentrations, not the 10th percentile.
Back to Citation98. All of the key U.S. epidemiologic studies considered in this reconsideration focus on all or subsections of the continental U.S.
Back to Citation99. The legislative history of section 109 indicates that a primary standard is to be set at “the maximum permissible ambient air level . . . which will protect the health of any [sensitive] group of the population,” and that for this purpose “reference should be made to a representative sample of persons comprising the sensitive group rather than to a single person in such a group.” S. Rep. No. 91–1196, 91st Cong., 2d Sess. 10 (1970); see also, e.g., Am. Lung Ass'n v. EPA, 134 F.3d 388, 389 (D.C. Cir. 1998) (“If a pollutant adversely affects the health of these sensitive individuals, EPA must strengthen the entire national standard”).
Back to Citation100. Additional information on all available at-risk epidemiologic studies in this reconsideration are available in section 3.4 and Appendix C of the 2022 PA (U.S. EPA, 2022b, section 3.4, Figure 3–17, and Appendix C, section C.3.2).
Back to Citation101. Similarly, the Administrator recognizes that changes in air quality to meet a 24-hour standard, would result not only in fewer and lower peak 24-hour PM2.5 concentrations, but also in lower annual average PM2.5 concentrations. However, as noted in 2012, an approach that relied on setting the level of the 24-hour standard such that the 24-hour standard was generally controlling would be less effective and result in less uniform protection across the U.S. than an approach that focuses on setting a generally controlling annual standard (78 FR 3163, January 15, 2013).
Back to Citation102. Judgments regarding adversity or health significance of measurable physiological responses to air pollutants have been informed by guidance, criteria or interpretative statements developed within the public health community, including the American Thoracic Society (ATS) and the European Respiratory Society (ERS), which cooperatively updated the ATS 2000 statement What Constitutes an Adverse Health Effect of Air Pollution (ATS, 2000) with new scientific findings, including the evidence related to air pollution and the cardiovascular system (Thurston et al., 2017).
103. The ATS/ERS described its 2017 statement as one “intended to provide guidance to policymakers, clinicians and public health professionals, as well as others who interpret the scientific evidence on the health effects of air pollution for risk management purposes” and further notes that “considerations as to what constitutes an adverse health effect, in order to provide guidance to researchers and policymakers when new health effects markers or health outcome associations might be reported in future.” The most recent policy statement by the ATS, which once again broadens its discussion of effects, responses and biomarkers to reflect the expansion of scientific research in these areas, reiterates that concept, conveying that it does not offer “strict rules or numerical criteria, but rather proposes considerations to be weighed in setting boundaries between adverse and nonadverse health effects,” providing a general framework for interpreting evidence that proposes a “set of considerations that can be applied in forming judgments” for this context (Thurston et al., 2017).
Back to Citation104. In their review of the 2021 draft PA, the majority of the CASAC advised that “evidence of effects from controlled human exposure studies with exposures close to the current standard support epidemiologic evidence for lowering the standard” (Sheppard, 2022a, p. 4 of consensus letter). The minority of the CASAC also advised that it was appropriate to place “more emphasis on the controlled human exposure studies, showing effects at PM2.5 concentrations well above those typically measured in areas meeting the current standards” (Sheppard, 2022a, p. 4 of consensus letter), in evaluating adequacy of the 24-hour standard.
Back to Citation105. Jones et al. (2023). Comparison of Occurrence of Scientifically Relevant Air Quality Observations Between Design Value Groups. Memorandum to the Rulemaking Docket for the Review of the National Ambient Air Quality Standards for Particulate Matter (EPA–HQ–OAR–2015–0072). Available at: https://www.regulations.gov/docket/EPA-HQ-OAR-2015-0072.
Back to Citation106. In the 2022 PA, the EPA has identified a number of key areas for additional research and data collection for PM2.5, based on the uncertainties and limitations that remain in the scientific evidence and technical information. In addition to research and data collection, the EPA specifically highlights additional information that could be reported in the epidemiologic studies that may help inform future reviews of the primary PM2.5 standards, including additional descriptive statistics in the upper percentiles of the air quality distribution ( i.e., from the 95th to the 99th percentile), as well as the number of days of concentrations and/or health events within each of these percentiles (U.S. EPA, 2022a, section 3.7).
Back to Citation107. The EPA notes that, in considering the additional scientific evidence available in this reconsideration, one member of the CASAC who reviewed both the 2019 draft PA and the 2021 draft PA found that the available scientific and quantitative information available in this reconsideration supported revising the level of the primary annual PM2.5 standard to within the range of 10–11 µg/m3. , whereas he recommended retaining the standard during the review of the 2019 draft PA.
Back to Citation108. The CASAC did not provide advice or recommendations regarding the indicator of the primary PM2.5 standards in their review of the 2019 draft PA (Cox, 2019b).
Back to Citation109. The CASAC did not provide advice or recommendations regarding the averaging times of the primary PM2.5 standards in their review of the 2019 draft PA (Cox, 2019b).
Back to Citation110. The CASAC did not provide advice or recommendations regarding the forms of the primary PM2.5 standards in their review of the 2019 draft PA (Cox, 2019b).
Back to Citation111. The CASAC did not provide advice or recommendations regarding the forms of the primary PM2.5 standards in their review of the 2019 draft PA (Cox, 2019b).
Back to Citation112. “Long-term” represents PM2.5 exposures and concentrations that are annual or multi-year.
Back to Citation113. As described in section II.A.2.c above, key epidemiologic studies are those that report overall mean (or median) PM2.5 concentrations and for which the years of PM2.5 air quality data used to estimate exposures overlap entirely with the years during which health events are reported.
Back to Citation114. Reported mean PM2.5 concentrations in monitor-based studies are averaged across monitors in each study area with multiple monitors, referred to as a composite monitor concentration, in contrast to the highest concentration monitored in the study area, referred to as a maximum monitor concentration ( i.e., the “design value” concentration), which is used to determine whether an area meets a given standard.
Back to Citation115. Studies that use hybrid modeling approaches employ methods to estimate ambient PM2.5 concentrations across large geographical areas, including areas without monitors, and thus, when compared to monitor-based studies, require additional information to inform the relationship between the estimated PM2.5 concentrations across an area and the maximum monitor design values used to assess compliance.
Back to Citation116. Analyses in the 2022 PA suggest that the highest monitored value would be expected to be greater than the study-reported mean values by 10–20% for monitor-based studies and 15–18% for hybrid modeling studies that apply aspects of population weighting.
Back to Citation117. The Wang et al. (2017) study only reports the 25th percentile of the estimated PM2.5 concentrations, not the 10th percentile.
Back to Citation118. There is a third hybrid model-based study, as described in the 2022 PA and in section II.B.3 above in responding to public comments, but it is not referenced here because it reports a 25th percentile PM2.5 concentration based on the 25th percentile of health events that occur in the study (Di et al., 2017a) rather than report the 25th percentile based on air quality concentrations.
Back to Citation119. Analyses in the 2022 PA suggest that the highest monitored value would be expected to be greater than the study-reported mean values by 10–20% for monitor-based studies and 15–18% for hybrid modeling studies that apply aspects of population weighting (U.S. EPA, 2022b, section 2.3.3.2.4).
120. The risk assessment in the 2022 PA used air quality adjustments to simulate just meeting the current primary PM2.5 standards, as well as alternative standard levels (U.S. EPA, 2022b, section 3.4.1.4 and Appendix C, section C.1.4).
Back to Citation121. Jones et al. (2023). Comparison of Occurrence of Scientifically Relevant Air Quality Observations Between Design Value Groups. Memorandum to the Rulemaking Docket for the Review of the National Ambient Air Quality Standards for Particulate Matter (EPA–HQ–OAR–2015–0072). Available at: https://www.regulations.gov/docket/EPA-HQ-OAR-2015-0072.
Back to Citation122. Jones et al. (2023). Comparison of Occurrence of Scientifically Relevant Air Quality Observations Between Design Value Groups. Memorandum to the Rulemaking Docket for the Review of the National Ambient Air Quality Standards for Particulate Matter (EPA–HQ–OAR–2015–0072). Available at: https://www.regulations.gov/docket/EPA-HQ-OAR-2015-0072.
Back to Citation123. The annual mean is calculated by averaging daily values in a calendar quarter and then averaging calendar quarters. See 40 CFR part 50 Appendix N, section 4.4.
Back to Citation124. These studies do not report information about the distribution of the health events and PM2.5 concentrations ( e.g., means, medians, other percentiles) in the restricted analyses.
Back to Citation125. Jones et al. (2023). Comparison of Occurrence of Scientifically Relevant Air Quality Observations Between Design Value Groups. Memorandum to the Rulemaking Docket for the Review of the National Ambient Air Quality Standards for Particulate Matter (EPA–HQ–OAR–2015–0072). Available at: https://www.regulations.gov/docket/EPA-HQ-OAR-2015-0072.
Back to Citation126. In addition to the review's opening “call for information” (79 FR 71764, December 3, 2014), the 2019 ISA identified and evaluated studies and reports that have undergone scientific peer review and were published or accepted for publication between January 1, 2009, through approximately January 2018 (U.S. EPA, 2019a, p. ES–2). References cited in the 2019 ISA, the references considered for inclusion but not cited, and electronic links to bibliographic information and abstracts can be found at: https://hero.epa.gov/hero/particulate-matter.
Back to Citation127. As discussed further below, methods employed by the epidemiologic studies to estimate ambient PM10–2.5 concentrations include: (1) Calculating the difference between PM10 and PM2.5 at co-located monitors, (2) calculating the difference between county-wide averages of monitored PM10 and PM2.5 based on monitors that are not necessarily co-located, and (3) direct measurement of PM10–2.5 using a dichotomous sampler (U.S. EPA, 2019a, section 1.4.2).
Back to Citation128. Non-inhalation exposure experiments ( i.e., intratracheal [IT] instillation) are informative for size fractions ( e.g., PM10–2.5) that cannot penetrate the airway of a study animal and may provide information relevant to biological plausibility and dosimetry (U.S. EPA, 2019a, section A–12).
Back to Citation129. As described in section I.C.5.b above, the scope of the ISA Supplement did not include consideration of studies of health effects associated with exposure to PM10–2.5. Therefore, the information and conclusions presented in the 2022 PA are very similar to those in the 2020 PA.
Back to Citation130. As described in section I.C.5.b above, the scope of the ISA Supplement did not include consideration of studies of health effects associated with exposure to PM10–2.5. Therefore, the information and conclusions presented in the 2022 PA are very similar to those in the 2020 PA.
Back to Citation131. PM10 concentrations presented as the annual second maximum 24-hour concentration (in µg/m3. ) at 262 sites in the U.S. For more information, see: https://www.epa.gov/air-trends/particulate-matter-pm10-trends
Back to Citation132. PM2.5 concentrations presented as the seasonally-weighted annual average concentration (in µg/m3. ) at 406 sites in the U.S. For more information, see: https://www.epa.gov/air-trends/particulate-matter-pm25-trends
Back to Citation133. See http://www.airnow.gov/.
Back to Citation134. In 1976, the EPA established a nationally uniform air quality index, then called the Pollutant Standard Index (PSI), for use by State and local agencies on a voluntary basis (41 FR 37660, September 7, 1976; 52 FR 24634, July 1,1987). In August 1999, the EPA adopted revisions to this air quality index (64 FR 42530, August 4, 1999) and renamed the index the AQI.
Back to Citation135. In evaluating the scientific evidence available to inform decisions regarding the AQI breakpoints, the EPA considered studies that were included as a part of the 2019 ISA and ISA Supplement, but also considered other studies that were not included as a part of the review of the air quality criteria. The ISAs have specific criteria for study inclusion and consideration in reaching conclusions regarding causal relationships, and some studies that may not have met those criteria ( e.g., epidemiologic studies that evaluate the health effects of wildfire smoke exposure that would have higher PM2.5 concentrations, which are outside of the scope of the ISA) were identified as studies that could be used to inform decisions on the AQI, particularly for the upper breakpoints.
Back to Citation136. The AQI breakpoint at 150 was originally set in 1999 to be linearly related to the concentrations at the 100 and 500 breakpoints but then revised in 2012 to be proportional to the AQI breakpoint concentration at 100 (78 FR 3181, January 15, 2013).
Back to Citation137. In this reconsideration, the controlled human exposure studies were evaluated in the 2019 ISA, whereas the epidemiologic studies of wildfire smoke exposures were included in the EPA Comparative Assessment of the Impacts of Prescribed Fire Versus Wildfire (CAIF): A Case Study in the Western U.S. (U.S. EPA 2021b).
Back to Citation138. Although participants in Lucking et al. (2011) were exposed to diesel exhaust (DE), the authors also conducted analyses using a particle trap, and as noted in the 2019 ISA, this type of study design allows for the assessment of the role of PM2.5 on the health effects observed by removing PM from the DE mixture.
Back to Citation139. These effects were attenuated when the DE was filtered, to reduce PM2.5 concentrations, indicating the effects were likely associated with PM2.5 exposure.
Back to Citation140. When applying a particle trap, PM2.5 concentrations were reduced, and effects associated with cardiovascular function including impaired vascular function, as measured by vasodilatation and thrombus formation were attenuated indicating associations with PM2.5.
Back to Citation141. U.S. EPA. (2013). Transitioning to a New NowCast Method. Presentation available in the Rulemaking Docket for the Review of the National Ambient Air Quality Standards for Particulate Matter (EPA–HQ–OAR–2015–0072), at: https://www.regulations.gov/docket/EPA-HQ-OAR-2015-0072.
Back to Citation142. Consistent with the 2016 Integrated Review Plan (U.S. EPA, 2016), other welfare effects of PM, including ecological effects, are being considered in the separate, on-going review of the secondary NAAQS for oxides of nitrogen, oxides of sulfur and PM. Accordingly, the public welfare protection provided by the secondary PM standards against ecological effects such as those related to deposition of nitrogen- and sulfur-containing compounds in vulnerable ecosystems is being considered in that separate review. Thus, the Administrator's decision in this reconsideration will be focused only and specifically on the adequacy of public welfare protection provided by the secondary PM standards from effects related to visibility, climate, and materials and hereafter “welfare effects” refers to non-ecological welfare effects ( i.e., visibility, climate, and materials effects).
Back to Citation143. In addition to the 2020 review's opening “call for information” (79 FR 71764, December 3, 2014), the 2019 ISA identified and evaluated studies and reports that have undergone scientific peer review and were published or accepted for publication between January 1, 2009 through approximately January 2018 (U.S. EPA, 2019a, p. ES–2). References that are cited in the 2019 ISA, the references that were considered for inclusion but not cited, and electronic links to bibliographic information and abstracts can be found at: https://hero.epa.gov/hero/particulate-matter.
Back to Citation144. As described in more detail in the ISA Supplement, “the scope of this Supplement provides specific criteria for the types of studies considered for inclusion within the Supplement. Specifically, studies must be peer reviewed and published between approximately January 2018 and March 2021” (U.S. EPA, 2022a, section 1.2.2).
Back to Citation145. As described in section 1.2.1 of the ISA Supplement, “the selection of welfare effects to evaluate within this Supplement is based on the causality determinations reported in the 2019 PM ISA and the subsequent use of scientific evidence in the 2020 PM PA. The 2019 PM ISA concluded a causal relationship for each of the welfare effects categories evaluated ( i.e., visibility, climate effects, and materials effects). While the 2020 PM PA considered the broader set of evidence for these effects, for climate effects and material effects, it concluded that there remained `substantial uncertainties with regard to the quantitative relationships with PM concentrations and concentration patterns that limit[ed] [the] ability to quantitatively assess the public welfare protection provided by the standards from these effects (U.S. EPA, 2020b). Given these uncertainties and limitations, the basis of the discussion on conclusions regarding the secondary standards in the 2020 PM PA primarily focused on visibility effects. Therefore, this Supplement focuses only on visibility effects in evaluating newly available scientific information and is limited to studies conducted in the U.S. and Canada” (U.S. EPA, 2022a, section 1.2.1).
Back to Citation146. Preference studies were available in four urban areas. Three western preference studies were available, including one in Denver, Colorado (Ely et al., 1991), one in the lower Fraser River valley near Vancouver, British Columbia, Canada (Pryor, 1996), and one in Phoenix, Arizona (BBC Research & Consulting, 2003). A pilot focus group study was also conducted for Washington, DC (Abt Associates, 2001), and a replicate study with 26 participants was also conducted for Washington, DC (Smith and Howell, 2009). More details about these studies are available in Appendix D of the 2022 PA (U.S. EPA, 2022b).
Back to Citation147. Deciview (dv) refers to a scale for characterizing visibility that is defined directly in terms of light extinction. The deciview scale is frequently used in the scientific and regulatory literature on visibility.
148. For comparison, 20 dv, 25 dv, and 30 dv are equivalent to 64, 112, and 191 megameters (Mm−1), respectively.
Back to Citation149. All particles scatter light and, although a larger particle scatters more light than a similarly shaped smaller particle of the same composition, the light scattered per unit of mass is greatest for particles with diameters from ~0.3–1.0 µm (U.S. EPA, 2009a, section 2.5.1; U.S. EPA, 2019a, section 13.2.1). Particles with hygroscopic components ( e.g., particulate sulfate and nitrate) contribute more to light extinction at higher relative humidity than at lower relative humidity because they change size in the atmosphere in response to relative humidity.
Back to Citation150. The algorithm is referred to as the IMPROVE algorithm as it was developed specifically to use monitoring data generated at IMPROVE network sites and with equipment specifically designed to support the IMPROVE program and was evaluated using IMPROVE optical measurements at the subset of monitoring sites that make those measurements (Malm et al., 1994).
Back to Citation151. Preference studies were available in four urban areas in the last review: Denver, Colorado (Ely et al., 1991), Vancouver, British Columbia, Canada (Pryor, 1996), Phoenix, Arizona (BBC Research & Consulting, 2003), and Washington, DC (Abt Associates, 2001; Smith and Howell, 2009).
Back to Citation152. The Grand Canyon study used a single scene looking west down the canyon with a small landscape feature of a 100-km-distant mountain (Mount Trumbull), along with other closer landscape features. The scenes presented in the previously available visibility preference studies are presented in more detail in Table D–9 in the 2022 PA (U.S. EPA, 2022b, Appendix D).
Back to Citation153. The Grand Canyon study superimposed light extinction ranging from 3 dv to 20 dv on the image slides shown to participants compared to the previously available preference studies. In those studies, the visibility ranges presented were as low as 9 dv and as high as 45 dv. The visibility ranges presented in the previously available visibility preference studies are described in more detail in Table D–9 in the 2022 PA (U.S. EPA, 2022b, Appendix D).
Back to Citation154. In the Grand Canyon study, the level of impairment that was determined to be “acceptable” by at least 50 percent of study participants was 7 dv (Malm et al., 2019).
Back to Citation155. Radiative forcing (RF) for a given atmospheric constituent is defined as the perturbation in net radiative flux, at the tropopause (or the top of the atmosphere) caused by that constituent, in watts per square meter (Wm-2. ), after allowing for temperatures in the stratosphere to adjust to the perturbation but holding all other climate responses constant, including surface and tropospheric temperatures (Fiore et al., 2015; Myhre et al., 2013). A positive forcing indicates net energy trapped in the Earth system and suggests warming of the Earth's surface, whereas a negative forcing indicates net loss of energy and suggests cooling (U.S. EPA, 2019a, section 13.3.2.2).
Back to Citation156. As discussed in the 2019 ISA (U.S. EPA, 2019a, section 13.4.1), corrosion typically involves reactions of acidic PM ( i.e., acidic sulfate or nitrate) with material surfaces, but gases like SO2 and nitric acid (HNO3) also contribute. Because “the impacts of gaseous and particulate N and S wet deposition cannot be clearly distinguished” (U.S. EPA, 2019a, p. 13–1), the assessment of the evidence in the 2019 ISA considers the combined impacts.
Back to Citation157. As noted above, the available public preference studies include those conducted in Denver, Colorado (Ely et al., 1991), Vancouver, British Columbia, Canada (Pryor, 1996), Phoenix, Arizona (BBC Research & Consulting, 2003), and Washington, DC (Abt Associates, 2001; Smith and Howell, 2009).
Back to Citation158. The other preference studies did not include populations that were necessarily representative of the population in the area for which the images being judged. For example, in the Denver, CO, study, participants were from intact groups ( i.e., those who were meeting for other reasons) and were asked to provide a period of time during a regularly scheduled meeting to participate in the study (Ely et al., 1991). As another example, in the British Columbia, Canada, study, participants were recruited from undergraduate and graduate students enrolled in classes at the University of British Columbia's Department of Geography (Pryor, 1996).
Back to Citation159. The analyses presented in the 2022 PA focus on the visibility index and the current secondary 24-hour PM2.5 standard with a level of 35 µg/m3. . However, we recognize that all three secondary PM standards influence the PM concentrations associated with the air quality distribution. As noted in section V.A.1 above, the current secondary PM standards include the 24-hour PM2.5 standard, with its level of 35 µg/m3. , the annual PM2.5 standard, with its level of 15.0 µg/m3. , and the 24-hour PM10 standard, with its level of 150 µg/m3. . With regard to the annual PM2.5 standard, we note that all 60 areas included in the analyses meet the current secondary annual PM standard (U.S. EPA, 2022b, Table D–7).
Back to Citation160. While the PM2.5 monitoring network has an increasing number of continuous FEM monitors reporting hourly PM2.5 mass concentrations, there continue to be data quality uncertainties associated with providing hourly PM2.5 mass and component measurements that could be input into IMPROVE equation calculations for subdaily visibility impairment estimates. As detailed in the 2022 PA, there are uncertainties associated with the precision and bias of 24-hour PM2.5 measurements (U.S. EPA, 2022b, p. 2–18), as well as to the fractional uncertainty associated with 24-hour PM component measurements (U.S. EPA, 2022b, p. 2–21). Given the uncertainties present when evaluating data quality on a 24-hour basis, the uncertainty associated with subdaily measurements may be even greater. Therefore, the inputs to these light extinction calculations are based on 24-hour average measurements of PM2.5 mass and components, rather than subdaily information.
Back to Citation161. A 3-year visibility metric with a level of 30 dv would be at the upper end of the range of levels identified from the public preference studies.
Back to Citation162. When light extinction is calculated using the original IMPROVE equation, all 60 sites have 3-year visibility metrics below 30 dv, 58 sites are at or below 25 dv, and 26 sites are at or below 20 dv (see U.S. EPA, 2022b, Appendix D, Table D–3).
Back to Citation163. As described in more detail in the 2022 PA, the revised IMPROVE equation divides PM components into smaller and larger sizes of particles in PM2.5, with separate mass scattering efficiencies and hygroscopic growth functions for each size category (U.S. EPA, 2022b, section 5.3.1.1).
Back to Citation164. When light extinction is calculated using the revised IMPROVE equation, all 60 sites have 3-year visibility metrics below 30 dv, 56 sites are at or below 25 dv, and 26 sites are at or below 20 dv (see U.S. EPA, 2022b, Appendix D, Table D–3).
Back to Citation165. When light extinction is calculated using the Lowenthal and Kumar IMPROVE equation, 59 sites have 3-year visibility metrics below 30 dv, 45 sites are at or below 25 dv, and 15 sites are at or below 20 dv. The one site with a 3-year visibility metric of 32 dv exceeds the secondary 24-hour PM2.5 standard, with a design value of 56 µg/m3. (see U.S. EPA, 2022b, Appendix D, Table D–3).
Back to Citation166. The Regional Haze Program was established by Congress specifically to achieve “the prevention of any future, and the remedying of existing, impairment of visibility in mandatory Class I areas, which impairment results from man-made air pollution,” and that Congress established a long-term program to achieve that goal (CAA section 169A).
Back to Citation167. In adopting section 169A, Congress set a goal of eliminating anthropogenic visibility impairment at Class I areas, as well as a framework for achieving that goal which extends well beyond the planning process and timeframe for attaining secondary NAAQS. Thus, the Regional Haze Program will continue to contribute to reductions in visibility impairment in Class I areas.
Back to Citation168. As noted above, the Administrator viewed the Regional Haze Program as a complement to the secondary PM NAAQS, and thus took into consideration its approach to improving visibility in considering how to address visibility outside of Class I areas.
Back to Citation169. As noted earlier, other welfare effects of PM, such as ecological effects, are being considered in the separate, on-going review of the secondary NAAQS for oxides of nitrogen, oxides of sulfur and PM.
Back to Citation170. As noted earlier in section V, the 2019 ISA “identified and evaluated studies and reports that that have undergone scientific peer review and were published or accepted for publication between January 1, 2009, and March 31, 2017. A limited literature update identified some additional studies that were published before December 31, 2017” (U.S. EPA, 2019a, Appendix, p. A–3).
Back to Citation171. As discussed in section I.D, the EPA has provisionally considered studies that were highlighted by commenters and that were published after the 2019 ISA. These studies are generally consistent with the evidence assessed in the 2019 ISA, and they do not materially alter our understanding of the scientific evidence or the Agency's conclusions based on that evidence.
Back to Citation172. Gantt, B., and Hagan, N. (2023). Analysis of Percentile Forms of the Visibility Index. Memorandum to the Rulemaking Docket for the Review of the National Ambient Air Quality Standards for Particulate Matter (EPA–HQ–OAR–2015–0072). Available at: https://www.regulations.gov/docket/EPA-HQ-OAR-2015-0072.
Back to Citation173. Gantt, B., and Hagan, N. (2023). Analysis of Percentile Forms of the Visibility Index. Memorandum to the Rulemaking Docket for the Review of the National Ambient Air Quality Standards for Particulate Matter (EPA–HQ–OAR–2015–0072). Available at: https://www.regulations.gov/docket/EPA-HQ-OAR-2015-0072.
Back to Citation174. Gantt, B., and Hagan, N. (2023). Analysis of Percentile Forms of the Visibility Index. Memorandum to the Rulemaking Docket for the Review of the National Ambient Air Quality Standards for Particulate Matter (EPA–HQ–OAR–2015–0072). Available at: https://www.regulations.gov/docket/EPA-HQ-OAR-2015-0072.
Back to Citation175. When light extinction is calculated using the revised IMPROVE equation, all 60 sites have 3-year visibility metrics below 28 dv, 56 sites are at or below 25 dv, and 26 sites are at or below 20 dv. When light extinction is calculated using the Lowenthal and Kumar IMPROVE equation, 59 sites have 3-year visibility metrics below 28 dv, 45 sites are at or below 25 dv, and 15 sites are at or below 20 dv. The one site with a 3-year visibility metric of 32 dv exceeds the secondary 24-hour PM2.5 standard, with a design value of 56 μg/m3. (see U.S. EPA, 2022b, Appendix D, Table D–3).
Back to Citation176. Gantt, B., and Hagan, N. (2023). Analysis of Percentile Forms of the Visibility Index. Memorandum to the Rulemaking Docket for the Review of the National Ambient Air Quality Standards for Particulate Matter (EPA–HQ–OAR–2015–0072). Available at: https://www.regulations.gov/docket/EPA-HQ-OAR-2015-0072.
Back to Citation177. Gantt, B., and Hagan, N. (2023). Analysis of Percentile Forms of the Visibility Index. Memorandum to the Rulemaking Docket for the Review of the National Ambient Air Quality Standards for Particulate Matter (EPA–HQ–OAR–2015–0072). Available at: https://www.regulations.gov/docket/EPA-HQ-OAR-2015-0072.
Back to Citation178. For reasons stated above and described in the 2022 PA and proposal, the Administrator does not find it appropriate to use the most recent preference study based on the Grand Canyon study area (Malm et al., 2019) for purposes of identifying a target level of protection for the visibility index.
Back to Citation179. As noted earlier, other welfare effects of PM, such as ecological effects, are being considered in the separate, on-going review of the secondary NAAQS for oxides of nitrogen, oxides of sulfur and PM.
Back to Citation180. Mention of commercial names does not constitute EPA endorsement.
Back to Citation181. Noah, G. (2023). Task 16 on PEP/NPAP Task Order: Bias and Precision DQOs for the PM2.5 Ambient Air Monitoring Network. Memorandum to the Rulemaking Docket for the Review of the National Ambient Air Quality Standards for Particulate Matter (EPA–HQ–OAR–2015–0072). Available at: https://www.regulations.gov/docket/EPA-HQ-OAR-2015-0072.
Back to Citation182. See the EPA's PM2.5 Data Quality Dashboard available at https://sti-r-shiny.shinyapps.io/QVA_Dashboard/.
Back to Citation183. Noah, G. (2023). Task 16 on PEP/NPAP Task Order: Bias and Precision DQOs for the PM2.5 Ambient Air Monitoring Network. Memorandum to the Rulemaking Docket for the Review of the National Ambient Air Quality Standards for Particulate Matter (EPA–HQ–OAR–2015–0072). Available at: https://www.regulations.gov/docket/EPA-HQ-OAR-2015-0072.
Back to Citation184. Noah, G. (2023). Task 16 on PEP/NPAP Task Order: Bias and Precision DQOs for the PM2.5 Ambient Air Monitoring Network. Memorandum to the Rulemaking Docket for the Review of the National Ambient Air Quality Standards for Particulate Matter (EPA–HQ–OAR–2015–0072). Available at: https://www.regulations.gov/docket/EPA-HQ-OAR-2015-0072.
Back to Citation185. In the proposal, in section VII.C.2 Quality Assurance Requirements for Prevention of Significant Deterioration (PSD) Air Monitoring (88 FR 5667–69), the EPA inadvertently referred to “appendix A” in the section rather than the correct “appendix B.” The EPA's intent to have proposed changes to appendix B on these pages is made clear by the section header, the Table of Contents on page 5559, and the proposed regulatory text for appendix B on pages 5707–08. See, e.g., id. at p.5668 (preamble erroneously states that the EPA proposed to change appendix A, section 2.6.1); id. at p.5668 (preamble erroneously states that the EPA proposed to adjust the minimum value required by appendix A, section 3.2.4).
Back to Citation186. Noah, G. (2023). Task 16 on PEP/NPAP Task Order: Bias and Precision DQOs for the PM2.5 Ambient Air Monitoring Network. Memorandum to the Rulemaking Docket for the Review of the National Ambient Air Quality Standards for Particulate Matter (EPA–HQ–OAR–2015–0072). Available at: https://www.regulations.gov/docket/EPA-HQ-OAR-2015-0072.
Back to Citation187. Noah, G. (2023). Task 16 on PEP/NPAP Task Order: Bias and Precision DQOs for the PM2.5 Ambient Air Monitoring Network. Memorandum to the Rulemaking Docket for the Review of the National Ambient Air Quality Standards for Particulate Matter (EPA–HQ–OAR–2015–0072). Available at: https://www.regulations.gov/docket/EPA-HQ-OAR-2015-0072.
Back to Citation188. SES is a composite measure that includes metrics such as income, occupation, and education, and can play a role in populations' access to healthy environments and healthcare.
Back to Citation189. Metropolitan and Micropolitan Statistical Areas are collectively referred to as “Core-Based Statistical Areas.” Metropolitan statistical areas have at least one urbanized area of 50,000 or more population, plus adjacent territory that has a high degree of social and economic integration with the core as measured by commuting ties. Micropolitan statistical areas are a set of statistical areas that have at least one urban cluster of at least 10,000 but less than 50,000 population, plus adjacent territory that has a high degree of social and economic integration with the core as measured by commuting ties.
Back to Citation190. MSA means a CBSA associated with at least one urbanized area of 50,000 population or greater. The central-county, plus adjacent counties with a high degree of integration, comprise the area.
Back to Citation191. Gantt, B. (2022). Analyses of Minimally Required PM2.5 Sites Under Alternative NAAQS. Memorandum to the Rulemaking Docket for the Review of the National Ambient Air Quality Standards for Particulate Matter (EPA–HQ–OAR–2015–0072). Available at: https://www.regulations.gov/docket/EPA-HQ-OAR-2015-0072.
Back to Citation192. See: https://www.epa.gov/ejscreen.
Back to Citation194. See: https://inmap.run/#home.
Back to Citation195. Mention of commercial names does not constitute EPA endorsement.
Back to Citation196. Mention of commercial names does not constitute EPA endorsement.
Back to Citation197. See: https://fire.airnow.gov/.
Back to Citation198. Gantt, B. (2022). Analyses of Minimally Required PM2.5 Sites Under Alternative NAAQS. Memorandum to the Rulemaking Docket for the Review of the National Ambient Air Quality Standards for Particulate Matter (EPA–HQ–OAR–2015–0072). Available at: https://www.regulations.gov/docket/EPA-HQ-OAR-2015-0072.
Back to Citation199. Available at https://fire.airnow.gov/.
Back to Citation200. While the CAA says “designating” with respect to the Governor's letter, in the full context of the CAA section it is clear that the Governor actually makes a recommendation to which the EPA must respond via a specified process if the EPA does not accept it.
Back to Citation201. In certain circumstances in which the Administrator has insufficient information to promulgate area designations within two years from the promulgation of the NAAQS, CAA section 107(d)(1)(B)(i) provides that the EPA may extend the designations schedule by up to one year.
Back to Citation202. API v. Costle, 609 F.2d 20 (D.C. Cir. 1979).
Back to Citation203. “Guidance to Regions for Working with Tribes during the National Ambient Air Quality Standards (NAAQS) Designations Process,” December 20, 2011, Memorandum from Stephen D. Page to Regional Air Directors, Regions 1–X available at https://www.epa.gov/sites/default/files/2017-02/documents/12-20-11_guidance_to_regions_for_working_with_tribes_naaqs_designations.pdf.
Back to Citation204. In certain circumstances in which the Administrator has insufficient information to promulgate area designations within two years from the promulgation of a new or revised NAAQS, CAA section 107(d)(1)(B)(i) provides the EPA may extend the designations schedule by up to one year.
Back to Citation206. See the EPA's Exceptional Events homepage at https://www.epa.gov/air-quality-analysis/treatment-air-quality-data-influenced-exceptional-events-homepage-exceptional.
Back to Citation207. See EPA's “Final Guidance on the Preparation of Exceptional Events Demonstrations for Wildfire Events that May Influence Ozone Concentrations and EPA's Exceptional Events Guidance: Prescribed Fire on Wildland that May Influence Ozone and Particulate Matter Concentrations,” found on EPA's Exceptional Events homepage at https://www.epa.gov/air-quality-analysis/treatment-air-quality-data-influenced-exceptional-events-homepage-exceptional.
Back to Citation208. See “Guidance on Infrastructure State Implementation Plan (SIP) Elements under Clean Air Act Sections 110(a)(1) and 110(a)(2)” September 2013, Memorandum from Stephen D. Page to Regional Air Directors, Regions 1–10.
Back to Citation209. CAA section 110(a)(2)(D)(i)(I).
Back to Citation210. CAA section 110(a)(2)(D)(i)(II) also addresses certain interstate effects that states must address and thus is also sometimes referred to as relating to “interstate transport.”
Back to Citation211. See North Carolina v. EPA, 531 F.3d 896, 909–11 (D.C. Cir. 2008).
Back to Citation212. See id. 911–13. See also Wisconsin v. EPA, 938 F.3d 303, 313–20 (D.C. Cir. 2019); Maryland v. EPA, 958 F.3d 1185, 1203–04 (D.C. Cir. 2020).
Back to Citation213. A “certification” approach would not be appropriate for the interstate pollution control requirements of CAA section 110(a)(2)(D)(i).
Back to Citation215. Provides guidance on developing demonstrations under section 189(e) intended to show that a certain PM2.5 precursor in a particular nonattainment area does not significantly contribute to PM2.5 concentrations that exceed the standard.
Back to Citation216. For more information on the EPA's recommendations and examples, see81 FR 58010, 58137, August 24, 2016.
Back to Citation217. CAA Sections 110(a) and 172 contain general nonattainment planning provisions, regarding the public review, adoption, submittal, and content of implementation plans. CAA Section 189 specifies additional plan provisions for particulate matter nonattainment areas. General Preamble for the Implementation of Title I of the Clean Air Act Amendments of 1990 provides a detailed discussion of the EPA's interpretation of the Title I requirements (57 FR 13498, April 16, 1992; 59 FR 41998, August 16, 1994).
Back to Citation218. 40 CFR 51.166(i)(2) and 52.21(i)(2).
Back to Citation219. On July 29, 2022, the EPA issued “Final Guidance for Ozone and Fine Particulate Matter Permit Modeling,” available at https://www.epa.gov/system/files/documents/2022-07/Guidance_for_O3_PM25_Permit_Modeling.pdf. This guidance provides the EPA's recommendations for how a stationary source seeking a PSD permit may demonstrate that it will not cause or contribute to a violation of the National Ambient Air Quality Standards for Ozone and PM2.5 and PSD increments for PM2.5, as required under section 165(a)(3) of the Clean Air Act and 40 CFR 51.166(k) and 52.21(k). The EPA has also previously issued two technical guidance documents for use in conducting these demonstrations: “Guidance on the Development of Modeled Emission Rates for Precursors (MERPs) as a Tier 1 Demonstration Tool for Ozone and PM2.5 under the PSD Permitting Program,” available at https://www.epa.gov/sites/default/files/2020-09/documents/epa-454_r-19-003.pdf, and “Guidance on the Use of Models for Assessing the Impacts of Emissions from Single Sources on the Secondarily Formed Pollutants: Ozone and PM2.5, ” available at https://www.epa.gov/sites/default/files/2020-09/documents/epa-454_r-16-005.pdf.
Back to Citation220. Sulfur dioxide is a precursor to PM2.5 in all attainment and unclassifiable areas. NOX is presumed to be a precursor to PM2.5 in all attainment and unclassifiable areas, unless a state or the EPA demonstrates that emissions of NOX from sources in a specific area are not a significant contributor to that area's ambient PM2.5 concentrations. VOC is presumed not to be a precursor to PM2.5 in any attainment or unclassifiable area, unless a state or the EPA demonstrates that emissions of VOC from sources in a specific area are a significant contributor to that area's ambient PM2.5 concentrations.
Back to Citation221. By establishing the maximum allowable level of ambient pollutant concentration increase in a particular area, an increment defines “significant deterioration” of air quality in that area. Increments are defined by the CAA as maximum allowable increases in ambient air concentrations above a baseline concentration and are specified in the PSD regulations by pollutant and area classification (Class I, II and III). 40 CFR 51.166(c), 40 CFR 52.21(c); 75 FR 64864 (October 20, 2010).
Back to Citation222. Congress established certain Class I areas in section 162(a) of the CAA, including international parks, national wilderness areas, and national parks that meet certain criteria. Such Class I areas, known as mandatory Federal Class I areas, are afforded special protection under the CAA. In addition, States and Tribal governments may establish Class I areas within their own political jurisdictions to provide similar special air quality protection.
Back to Citation223. See40 CFR part 51, appendix W; 82 FR 5182 (January 17, 2017); See also U.S. EPA, 2021d. The EPA provided an initial version of the 2021 guidance for public comment on February 10, 2020. Upon consideration of the comments received, and consistent with Executive Order 13990, the EPA revised the initial draft guidance and posted the revised version for additional public comment.
Back to Citation224. This exemption was referred to as “grandfathering” in the 2015 Ozone NAAQS and the D.C. Circuit's Murray Energy Corp. decision on that exemption. See80 FR 65292, 65431 (October 26, 2015); Murray Energy Corp. v. EPA, 936 F.3d 597, 627 (D.C. Cir. 2019). The EPA refers to this “grandfathering” provision in this action as an exemption provision.
Back to Citation225. While the specifics of this case involved the 2015 ozone NAAQS, the case was based upon an interpretation of CAA section 165(a) and therefore applies equally to any PSD permitting exemption provision for a new or revised NAAQS.
Back to Citation226. 40 CFR 51.166(k) states that SIPs must require that the owner or operator of the proposed source or modification demonstrate that allowable emission increases from the proposed source or modification, in conjunction with all other applicable emissions increases or reductions (including secondary emissions), would not cause or contribute to air pollution in violation of: (i) Any national ambient air quality standard in any air quality control region; or (ii) any applicable maximum allowable increase over the baseline concentration in any area.
Back to Citation227. See, e.g., Memorandum from Stephen D. Page, Director, Office of Air Quality Planning and Standards to Regional Air Division Directors, Guidance Concerning Implementation of the 1-hour SO2 NAAQS for the Prevention of Significant Deterioration Program. August 23, 2010. Office of Air Quality Planning and Standards U.S. EPA, Research Triangle Park. Available at: https://www.epa.gov/sites/default/files/2015-07/documents/appwso2.pdf;44 FR 3274, 3278, January 16, 1979; See also In re Interpower of New York, Inc., 5 E.A.D. 130, 141 (EAB 1994) (describing an EPA Region 2 PSD permit that relied in part on offsets to demonstrate the source would not cause or contribute to a violation of the NAAQS). 52 FR 24634, 24684, July 1, 1987; 78 FR 3085, 3261–62, January 15, 2013. The EPA has recognized the ability of sources to obtain offsets in the context of PSD though the PSD provisions of the Act do not expressly reference offsets as the NNSR provisions of the Act do. See80 FR 65292, 65441, October 26, 2015.
Back to Citation228. All of these pollutants are identified as precursors to PM2.5 in NNSR regulations. See40 CFR 51.165(a)(1)(xxxvii)(C)( 2). No significant emission rate is established by the EPA for ammonia, and states are required to define “significant” for ammonia for their respective areas unless the state pursues the optional precursor demonstration to exclude ammonia from planning requirements. See40 CFR 51.165(a)(1)(x)(F); 40 CFR 51.165(a)(13).
Back to Citation229. Memorandum from Joseph Goffman, Principal Deputy Assistant Administrator, Office of Air and Radiation, to Air and Radiation Division Directors, “Principles for Addressing Environmental Justice in Air Permitting” (December 22, 2022), available at https://www.epa.gov/caa-permitting/ej-air-permitting-principles-addressing-environmental-justice-concerns-air.
Back to Citation230. Id., Attachment, “EJ in Air Permitting: Principles for Addressing Environmental Justice Concerns in Air Permitting” (December 2022), available at https://www.epa.gov/caa-permitting/ej-air-permitting-principles-addressing-environmental-justice-concerns-air.
Back to Citation233. Further, the EPA's current Unified Agenda and Regulatory Plan includes its intention to issue a proposed rule to amend the General Conformity Regulations. The EPA intends to address in that regulatory action topics regarding prescribed fire, including consideration of smoke management approaches such as those discussed in the Exceptional Events Rule, among other topics. See, e.g., https://www.reginfo.gov/public/do/eAgendaViewRule?pubId=202310&RIN=2060-AV28.
Back to CitationBILLING CODE 6560–50–P
BILLING CODE 6560–50–C
[FR Doc. 2024–02637 Filed 3–5–24; 8:45 am]
BILLING CODE 6560–50–P
























Document Information
- Effective Date:
- 5/6/2024
- Published:
- 03/06/2024
- Department:
- Environmental Protection Agency
- Entry Type:
- Rule
- Action:
- Final rule.
- Document Number:
- 2024-02637
- Dates:
- This final rule is effective May 6, 2024.
- Pages:
- 16202-16406 (205 pages)
- Docket Numbers:
- EPA-HQ-OAR-2015-0072, FRL-8635-02-OAR
- RINs:
- 2060-AV52: Reconsideration of the National Ambient Air Quality Standards for Particulate Matter
- RIN Links:
- https://www.federalregister.gov/regulations/2060-AV52/reconsideration-of-the-national-ambient-air-quality-standards-for-particulate-matter
- Topics:
- Administrative practice and procedure, Air pollution control, Carbon monoxide, Environmental protection, Intergovernmental relations, Lead, Nitrogen dioxide, Ozone, Particulate matter, Reporting and recordkeeping requirements, Sulfur oxides
- PDF File:
- 2024-02637.pdf
- Supporting Documents:
- » Schwartz, J, Wei, Y, Yitshak-Sade, M, Di, Q, Dominici, F and Zanobetti, A (2021). A national difference in differences analysis of the effect of PM2.5 on annual death rates. Environmental Research 194: 110649
- » Thurston, GD, Ahn, J, Cromar, KR, Shao, Y, Reynolds, HR, Jerrett, M, Lim, CC, Shanley, R, Park, Y and Hayes, RB (2016). Ambient Particulate Matter Air Pollution Exposure and Mortality in the NIH-AARP Diet and Health Cohort. Environmental Health Perspectives 124(4): 484-490
- » Shin, S, Burnett, RT, Kwong, JC, Hystad, P, van Donkelaar, A, Brook, JR, Goldberg, MS, Tu, K, Copes, R, Martin, R, Lia, Y, Kopp, A and Chen, H (2019). Ambient Air Pollution and the Risk of Atrial Fibrillation and Stroke: A Population-Based Cohort Study. Environmental Health Perspectives 127(8): 87009
- » Lipfert, FW and Wyzga, RE (2020). Environmental predictors of survival in a cohort of U.S. military veterans: A multi-level spatio-temporal analysis stratified by race. Environmental Research 183(Elsevier): 108842
- » Vieira, JL, Guimaraes, GV, de Andre, PA, Nascimento Saldiva, PH and Bocchi, EA (2016b). Effects of Reducing Exposure to Air Pollution on Submaximal Cardiopulmonary Test in Patients with Heart Failure: Analysis of the Randomized, Double-blind and Controlled FILTER-HF trial. International Journal of Cardiology 215: 92-97
- » Ghio, AJ, Kim, C and Devlin, RB (2000). Concentrated ambient air particles induce mild pulmonary inflammation in healthy human volunteers. American Journal of Respiratory and Critical Care Medicine 162(3): 981-988.
- » Peng, RD, Dominici, F and Welty, LJ (2009b). A Bayesian Hierarchical Distributed Lag Model for Estimating the Time Course of Risk of Hospitalization Associated with Particulate Matter Air Pollution. J Roy Stat Soc Ser C (Appl Stat) 58: 3-24
- » Pappin, AJ, et al. (2019). Examining the Shape of the Association between Low Levels of Fine Particulate Matter and Mortality across Three Cycles of the Canadian Census Health and Environment Cohort. Environmental Health Perspectives 127(10): 107008
- » RE ppt for today's PM NAAQS review meeting re: RTC TOC mtg w OMB
- » a 11 9 2020 OMB mtg on draft RTC TOC
- CFR: (14)
- 40 CFR 50.20
- 40 CFR 53.4
- 40 CFR 53.8
- 40 CFR 53.14
- 40 CFR 53.35
- More ...