2021-14250. Medicare Program; End-Stage Renal Disease Prospective Payment System, Payment for Renal Dialysis Services Furnished to Individuals With Acute Kidney Injury, End-Stage Renal Disease Quality Incentive Program, and End-Stage Renal Disease ...
-
Start Preamble
Start Printed Page 36322
AGENCY:
Centers for Medicare & Medicaid Services (CMS), HHS.
ACTION:
Proposed rule.
SUMMARY:
This proposed rule would update the End-Stage Renal Disease (ESRD) Prospective Payment System (PPS) for calendar year (CY) 2022. This rulemaking also proposes to update the payment rate for renal dialysis services furnished by an ESRD facility to individuals with acute kidney injury (AKI). In addition, this rulemaking proposes to update requirements for the ESRD Quality Incentive Program (QIP), including a proposed measure suppression policy for the duration of the coronavirus disease 2019 (COVID-19) public health emergency (PHE) and as well as proposals to suppress individual ESRD QIP measures under that proposed measure suppression policy. This proposed rule also announces an extension of time for facilities to report September through December 2020 ESRD QIP data under our Extraordinary Circumstances Exception (ECE) policy due to CMS operational issues, and proposes to not score facilities or reduce payment to any facility in PY 2022. In addition, this proposed rule includes requests for information on topics that are relevant to the ESRD QIP. Further, this rule also proposes changes to the ESRD Treatment Choices (ETC) Model, which is a mandatory payment model that is focused on encouraging greater use of home dialysis and kidney transplants, to reduce Medicare expenditures while preserving or enhancing the quality of care furnished to Medicare beneficiaries. Finally, this proposed rule includes several requests for information to inform payment reform under the ESRD PPS.
DATES:
To be assured consideration, comments must be submitted at one of the addresses provided below, by August 31, 2021.
ADDRESSES:
In commenting, please refer to file code CMS-1749-P. Because of staff and resource limitations, we cannot accept comments by facsimile (FAX) transmission. Comments, including mass comment submissions, must be submitted in one of the following three ways (please choose only one of the ways listed):
1. Electronically. You may submit electronic comments on this regulation to http://www.regulations.gov. Follow the “Submit a comment” instructions.
2. By regular mail. You may mail written comments to the following address ONLY: Centers for Medicare & Medicaid Services, Department of Health and Human Services, Attention: CMS-1749-P, P.O. Box 8010, Baltimore, MD 21244-8010.
Please allow sufficient time for mailed comments to be received before the close of the comment period.
3. By express or overnight mail. You may send written comments to the following address ONLY: Centers for Medicare & Medicaid Services, Department of Health and Human Services, Attention: CMS-1749-P, Mail Stop C4-26-05, 7500 Security Boulevard, Baltimore, MD 21244-1850.
For information on viewing public comments, see the beginning of the SUPPLEMENTARY INFORMATION section.
Start Further InfoFOR FURTHER INFORMATION CONTACT:
ESRDPayment@cms.hhs.gov, for issues related to the ESRD PPS and coverage and payment for renal dialysis services furnished to individuals with AKI.
ESRDApplications@cms.hhs.gov, for issues related to the Transitional Add-On Payment Adjustment for New and Innovative Equipment and Supplies (TPNIES).
Delia Houseal, (410) 786-2724, for issues related to the ESRD QIP.
ETC-CMMI@cms.hhs.gov, for issues related to the ESRD Treatment Choices (ETC) Model.
End Further Info End Preamble Start Supplemental InformationSUPPLEMENTARY INFORMATION:
Inspection of Public Comments: All comments received before the close of the comment period are available for viewing by the public, including any personally identifiable or confidential business information that is included in a comment. We post all comments received before the close of the comment period on the following website as soon as possible after they have been received: http://www.regulations.gov. Follow the search instructions on that website to view public comments. CMS will not post on Regulations.gov public comments that make threats to individuals or institutions or suggest that the individual will take actions to harm the individual. CMS continues to encourage individuals not to submit duplicative comments. We will post acceptable comments from multiple unique commenters even if the content is identical or nearly identical to other comments.
Current Procedural Terminology (CPT) Copyright Notice: Throughout this proposed rule, we use CPT® codes and descriptions to refer to a variety of services. We note that CPT® codes and descriptions are copyright 2020 American Medical Association (AMA). All Rights Reserved. CPT® is a registered trademark of the AMA. Applicable Federal Acquisition Regulations (FAR) and Defense Federal Acquisition Regulations (DFAR) apply.
Table of Contents
To assist readers in referencing sections contained in this preamble, we are providing a Table of Contents.
I. Executive Summary
A. Purpose
B. Summary of the Major Provisions
C. Summary of Cost and Benefits
II. Calendar Year (CY) 2022 End-Stage Renal Disease (ESRD) Prospective Payment System (PPS)
A. Background
B. Provisions of the Proposed Rule
C. Proposed Transitional Add-On Payment Adjustment for New and Innovative Equipment and Supplies (TPNIES) for CY 2022 Payment
III. Calendar Year (CY) 2022 Payment for Renal Dialysis Services Furnished to Individuals With Acute Kidney Injury (AKI)
A. Background
B. Proposed Annual Payment Rate Update for CY 2022
IV. End-Stage Renal Disease Quality Incentive Program (ESRD QIP)
A. Background
B. Extraordinary Circumstances Exception (ECE) Previously Granted for the ESRD QIP and Notification of ECE Due to ESRD Quality Reporting System Issues
C. Proposed Flexibilities for the ESRD QIP in Response to the COVID-19 PHE
D. Proposed Special Scoring Methodology and Payment Policy for the PY 2022 ESRD QIP
E. Proposed Updates to Requirements Beginning With the PY 2024 ESRD QIP
F. Updates for the PY 2025 ESRD QIP
G. Requests for Information (RFIs) on Topics Relevant to ESRD QIP
V. End-Stage Renal Disease Treatment Choices (ETC) Model
A. Background
B. Provisions of the Proposed Rule
C. Requests for Information (RFIs) on Topics Relevant to ETC Model
VI. Requests for Information
A. Informing Payment Reform Under the ESRD PPSStart Printed Page 36323
B. Technical Expert Panels (TEPs)
C. Calculation of the Low-Volume Payment Adjustment (LVPA)
D. Calculation of the Case-Mix Adjustments
E. Calculation of the Outlier Payment Adjustment
F. Calculation of the Pediatric Dialysis Payment Adjustment
G. Modifying the ESRD PPS and Hospital Cost Reports
H. Modifying the Pediatric Cost Report
I. Modifying Site of Services Provided to Medicare Beneficiaries with Acute Kidney Injury (AKI)
VII. Collection of Information Requirements
A. Legislative Requirement for Solicitation of Comments
B. Requirements in Regulation Text
C. Additional Information Collection Requirements
VIII. Response to Comments
IX. Economic Analyses
A. Regulatory Impact Analysis
B. Detailed Economic Analysis
C. Accounting Statement
D. Regulatory Flexibility Act Analysis (RFA)
E. Unfunded Mandates Reform Act Analysis (UMRA)
F. Federalism
G. Congressional Review Act
X. Files Available to the Public via the Internet
Regulations Text
I. Executive Summary
A. Purpose
1. End-Stage Renal Disease (ESRD) Prospective Payment System (PPS)
On January 1, 2011, we implemented the End-Stage Renal Disease (ESRD) Prospective Payment System (PPS), a case-mix adjusted, bundled PPS for renal dialysis services furnished by ESRD facilities as required by section 1881(b)(14) of the Social Security Act (the Act), as added by section 153(b) of the Medicare Improvements for Patients and Providers Act of 2008 (MIPPA) (Pub. L. 110-275). Section 1881(b)(14)(F) of the Act, as added by section 153(b) of MIPPA, and amended by section 3401(h) of the Patient Protection and Affordable Care Act (the Affordable Care Act) (Pub. L. 111-148), established that beginning calendar year (CY) 2012, and each subsequent year, the Secretary of the Department of Health and Human Services (the Secretary) shall annually increase payment amounts by an ESRD market basket increase factor, reduced by the productivity adjustment described in section 1886(b)(3)(B)(xi)(II) of the Act. This rule proposes updates to the ESRD PPS for CY 2022.
2. Coverage and Payment for Renal Dialysis Services Furnished to Individuals With Acute Kidney Injury (AKI)
On June 29, 2015, the President signed the Trade Preferences Extension Act of 2015 (TPEA) (Pub. L. 114-27). Section 808(a) of the TPEA amended section 1861(s)(2)(F) of the Act to provide coverage for renal dialysis services furnished on or after January 1, 2017, by a renal dialysis facility or a provider of services paid under section 1881(b)(14) of the Act to an individual with acute kidney injury (AKI). Section 808(b) of the TPEA amended section 1834 of the Act by adding a new subsection (r) that provides for payment for renal dialysis services furnished by renal dialysis facilities or providers of services paid under section 1881(b)(14) of the Act to individuals with AKI at the ESRD PPS base rate beginning January 1, 2017. This rule proposes to update the AKI payment rate for CY 2022.
3. End-Stage Renal Disease Quality Incentive Program (ESRD QIP)
The End-Stage Renal Disease Quality Incentive Program (ESRD QIP) is authorized by section 1881(h) of the Act. The Program fosters improved patient outcomes by establishing incentives for dialysis facilities to meet or exceed performance standards established by the Centers for Medicare & Medicaid Services (CMS). This rule proposes to suppress the use of certain ESRD QIP measure data for scoring and payment adjustment purposes in the PY 2022 ESRD QIP because we have determined that circumstances caused by the Public Health Emergency (PHE) for the coronavirus disease 2019 (COVID-19) pandemic have significantly affected the validity and reliability of the measures and resulting performance scores, as well as special scoring and payment policies for PY 2022. We are also announcing an extension of time for facilities to report September-December 2020 ESRD QIP data under our Extraordinary Circumstances Exception (ECE) policy due to CMS operational issues. Beginning with the PY 2024 ESRD QIP, we are proposing to update the specifications for the SHR clinical measure. We are also proposing for the PY 2024 ESRD QIP to adopt CY 2019 as the baseline period for purposes of calculating the achievement thresholds, benchmarks, and performance standard values. Although no new requirements are proposed for the PY 2025 ESRD QIP, this proposed rule includes policies that would apply in PY 2025. This proposed rule also includes requests for information on several important topics, including strategies that CMS can use to address the gap in existing health inequities, the addition of COVID-19 vaccination measures in future rulemaking, and the use of digital quality measurement.
4. End-Stage Renal Disease Treatment Choices (ETC) Model
This rulemaking proposes to implement changes to the End-Stage Renal Disease (ESRD) Treatment Choices Model (ETC) Model, a mandatory Medicare payment model tested under the authority of section 1115A of the Act. The ETC Model is operated by the Center for Medicare and Medicaid Innovation (Innovation Center), and tests the use of payment adjustments to encourage greater utilization of home dialysis and kidney transplants, in order to preserve or enhance the quality of care furnished to Medicare beneficiaries while reducing Medicare expenditures. The ETC Model includes ESRD facilities and certain clinicians caring for beneficiaries with ESRD—or Managing Clinicians—located in Selected Geographic Areas as participants.
The ETC Model was finalized as part of a final rule published in the Federal Register on September 29, 2020, titled, “Medicare Program; Specialty Care Models to Improve Quality of Care and Reduce Expenditures” (85 FR 61114), referred to herein as the “Specialty Care Models final rule.” The ETC Model is designed to test the effectiveness of adjusting certain Medicare payments to ETC Participants (ESRD facilities and Managing Clinicians—clinicians who furnish and bill the Monthly Capitation Payment (MCP) for managing ESRD Beneficiaries—who have been selected to participate in the ETC Model) to encourage greater utilization of home dialysis and kidney transplantation, support beneficiary modality choice, reduce Medicare expenditures, and preserve or enhance the quality of care. In the Specialty Care Models final rule, we established that the ETC Model adjusts payments for home dialysis and home dialysis-related claims with claim service dates from January 1, 2021 through December 31, 2023 through the Home Dialysis Payment Adjustment (HDPA). We are assessing the rates of home dialysis and of kidney transplant waitlisting and living donor transplantation, among beneficiaries attributed to ETC Participants during the period beginning January 1, 2021, and ending June 30, 2026. Based on those rates, we are applying the Performance Payment Adjustment (PPA) to claims for dialysis and dialysis-Start Printed Page 36324related services with claim service dates beginning July 1, 2022, and ending June 30, 2027. We codified these provisions in a new subpart of the Code of Federal Regulations (CFR) 42 CFR part 512, subpart C.
This rulemaking proposes modifications to the ETC Model, including changes to the home dialysis rate and transplant rate, the PPA achievement benchmarking methodology, and the PPA improvement benchmarking and scoring methodology. We are also proposing to add processes and requirements for ETC Participants to receive certain data from CMS and to include certain additional waivers and flexibilities as part of the ETC Model test. This proposed rule also includes requests for information regarding the placement of peritoneal dialysis catheters and the development of a home dialysis beneficiary experience measure.
B. Summary of the Major Provisions
1. ESRD PPS
- Update to the ESRD PPS base rate for CY 2022: The proposed CY 2022 ESRD PPS base rate is $255.55. This proposed amount reflects the application of the wage index budget-neutrality adjustment factor (.999546) and a productivity-adjusted market basket increase of 1.0 percent as required by section 1881(b)(14)(F)(i)(I) of the Act, equaling $255.55 (($253.13 × .999546) × 1.010 = $255.55).
- Annual update to the wage index: We adjust wage indices on an annual basis using the most current hospital wage data and the latest core-based statistical area (CBSA) delineations to account for differing wage levels in areas in which ESRD facilities are located. For CY 2022, we are proposing to update the wage index values based on the latest available data and continuing the 2-year transition to the Office of Management and Budget (OMB) delineations as described in the September 14, 2018 OMB Bulletin No. 18-04.
- Update to the outlier policy: We are proposing to update the outlier policy using the most current data, as well as update the outlier services fixed-dollar loss (FDL) amounts for adult and pediatric patients and Medicare allowable payment (MAP) amounts for adult and pediatric patients for CY 2022 using CY 2020 claims data. Based on the use of the latest available data, the proposed FDL amount for pediatric beneficiaries would decrease from $44.78 to $30.38, and the MAP amount would decrease from $30.88 to $28.73, as compared to CY 2021 values. For adult beneficiaries, the proposed FDL amount would decrease from $122.49 to $111.18, and the MAP amount would decrease from $50.92 to $47.87. The 1.0 percent target for outlier payments was not achieved in CY 2020. Outlier payments represented approximately 0.6 percent of total payments rather than 1.0 percent.
- Update to the offset amount for the transitional add-on payment adjustment for new and innovative equipment and supplies (TPNIES) for CY 2022: The proposed CY 2022 average per treatment offset amount for the transitional add-on payment adjustment for new and innovative equipment and supplies (TPNIES) for capital-related assets that are home dialysis machines is $9.41. This proposed offset amount reflects the application of the productivity-adjusted market basket increase of 1.0 percent ($9.32 × 1.010 = $9.41).
- TPNIES applications received for CY 2022: This proposed rule presents a summary of the two CY 2022 TPNIES applications that we received by the February 1, 2021 deadline and our analysis of the applicants' claims related to substantial clinical improvement (SCI) and other eligibility criteria for the TPNIES.
2. Payment for Renal Dialysis Services Furnished to Individuals With AKI
We are proposing to update the AKI payment rate for CY 2022 to $255.55, which is the same as the base rate proposed under the ESRD PPS for CY 2022.
3. ESRD QIP
We are announcing an extension of time for facilities to report September through December 2020 ESRD QIP data under our Extraordinary Circumstances Exception (ECE) policy due to CMS operational issues. We are proposing to adopt a measure suppression policy for the duration of the COVID-19 PHE that would enable us to suppress the use of one or more measures in the ESRD QIP for scoring and payment adjustment purposes if we determine that circumstances caused by the COVID-19 PHE have significantly affected the measures and resulting performance scores. We are also proposing to suppress the Standardized Hospitalization Ratio (SHR) clinical measure, the Standardized Readmission Ratio (SRR) clinical measure, the In-Center Hemodialysis Consumer Assessment of Healthcare Providers and Systems (ICH CAHPS) clinical measure, and the Long-Term Catheter Rate clinical measure for PY 2022 under the proposed measure suppression policy. Finally, we are proposing to not score or reduce payment to any facility in PY 2022. Beginning with the PY 2024 ESRD QIP, we are proposing to update the specifications for the SHR clinical measure. We are also proposing for the PY 2024 ESRD QIP to adopt CY 2019 as the baseline period for purposes of calculating the achievement thresholds, benchmarks, and performance standard values. This proposed rule also announces the performance standards and payment reductions that would apply for PY 2024. This proposed rule describes several policies continuing for PY 2025, but does not propose any new requirements beginning with the PY 2025 ESRD QIP.
This proposed rule includes requests for public comment on several important topics, including closing the gap in health equity, adding a COVID-19 vaccination measure for health care personnel (HCP) and a COVID-19 vaccination measure for ESRD patients to the ESRD QIP measure set in future rulemaking, and potential actions and priority areas that would enable the continued transformation of our quality measurement enterprise toward greater digital capture of data and use of the Fast Healthcare Interoperability Resources (FHIR®) standard.
4. ETC Model
We are proposing to implement the following changes to the ETC Model beginning for the third Measurement Year (MY3) of the Model, which begins January 1, 2022.
- Beneficiary Attribution for Living Kidney Donor Transplants: To better reflect the care relationship between beneficiaries who receive pre-emptive living donor transplants (LDT) and the Managing Clinicians who provide their care, we propose to modify the methodology for attributing Pre-emptive LDT Beneficiaries to Managing Clinicians, such that a Pre-emptive LDT Beneficiary would be attributed to the Managing Clinician who submitted the most claims for services furnished to the beneficiary during the 365 days prior to the transplant date.
- Home Dialysis Rate Calculation: To incentivize additional alternative renal replacement modalities under the ETC Model, we propose adding nocturnal in-center dialysis to the calculation of the home dialysis rate for ESRD facilities not owned in whole or in part by a large dialysis organization (LDO) as well as Managing Clinicians.
- Transplant Rate Beneficiary Exclusion: To better align with common reasons transplant centers do not place patients on the transplant waitlist, we propose to exclude beneficiaries with a diagnosis of, and who are receiving Start Printed Page 36325treatment with chemotherapy or radiation for, vital solid organ cancers from the calculation of the transplant rate.
- Performance Payment Adjustment Achievement Benchmarking Methodology: When we originally finalized the ETC Model, we stated our intent to increase achievement benchmarks above rates observed in Comparison Geographic Areas for future model years. As such, we propose to increase achievement benchmarks by 10 percent over rates observed in Comparison Geographic Areas every two MYs, beginning in MY3 (2022). We also propose to stratify achievement benchmarks based on the proportion of attributed beneficiaries who are dually-eligible for Medicare and Medicaid or receive the Low Income Subsidy (LIS) during the MY, in recognition that beneficiaries with lower socioeconomic status have lower rates of home dialysis and transplant than those with higher socioeconomic status.
- Performance Payment Adjustment Improvement Benchmarking and Scoring: In conjunction with our proposal to stratify achievement benchmarks based on the proportion of beneficiaries who are dual-eligible or LIS recipients, we propose to introduce the Health Equity Incentive to the improvement scoring methodology used in calculating the PPA. CMS expects that the Health Equity Incentive would encourage ETC Participants to decrease disparities in renal replacement modality choice among beneficiaries with lower socioeconomic status by rewarding ETC Participants that demonstrate significant improvement in the home dialysis rate or transplant rate among their attributed beneficiaries who are dual-eligible or LIS recipients. We also propose to adjust the improvement scoring calculation to avoid the scenario where an ETC Participant cannot receive an improvement score because its home dialysis rate or transplant rate was zero during the Benchmark Year.
- Performance Payment Adjustment Reports and Related Data Sharing: To ensure that ETC Participants have timely access to ETC Model reports, we are proposing a process by which CMS would share certain model data with ETC Participants.
- Medicare Waivers: We are proposing an additional programmatic waiver to provide Managing Clinicians who are ETC Participants additional flexibility in furnishing the kidney disease patient education services described in § 410.48: A waiver of certain telehealth requirements as necessary solely for purposes of allowing ETC Participants to furnish kidney disease patient education services via telehealth under the ETC Model.
- Kidney Disease Patient Education Services Coinsurance Waivers: We are proposing to permit Managing Clinicians who are ETC Participants to reduce or waive the beneficiary coinsurance for kidney disease patient education services, subject to certain requirements. We anticipate making the determination that the anti-kickback statute safe harbor for CMS-sponsored model patient incentives (42 CFR 1001.952(ii)), would be available to protect the reduction or elimination of coinsurance performed in accordance with our proposed policy, if finalized.
C. Summary of Costs and Benefits
In section IX.B of this proposed rule, we set forth a detailed analysis of the impacts that the proposed changes would have on affected entities and beneficiaries. The impacts include the following:
1. Impacts of the Proposed ESRD PPS
The impact table in section IX.B.1.a of this proposed rule displays the estimated change in payments to ESRD facilities in CY 2022 compared to estimated payments in CY 2021. The overall impact of the proposed CY 2022 changes is projected to be a 1.2 percent increase in payments. Hospital-based ESRD facilities have an estimated 1.3 percent increase in payments compared with freestanding facilities with an estimated 1.2 percent increase. We estimate that the aggregate ESRD PPS expenditures would increase by approximately $140 million in CY 2022 compared to CY 2021. This reflects a $120 million increase from the payment rate update and a $20 million increase due to the updates to the outlier threshold amounts. Because of the projected 1.2 percent overall payment increase, we estimate there would be an increase in beneficiary coinsurance payments of 1.2 percent in CY 2022, which translates to approximately $30 million.
2. Impacts of the Proposed Payment for Renal Dialysis Services Furnished to Individuals With AKI
The impact table in section IX.B.2.a of this proposed rule displays the estimated change in payments to ESRD facilities in CY 2022 compared to estimated payments in CY 2021. The overall impact of the proposed CY 2022 changes is projected to be a 1.0 percent increase in payments for individuals with AKI. Hospital-based ESRD facilities have an estimated 1.1 percent increase in payments compared with freestanding ESRD facilities with an estimated 1.0 percent increase. The overall impact reflects the effects of the updated wage index and the proposed payment rate update. We estimate that the aggregate payments made to ESRD facilities for renal dialysis services furnished to patients with AKI, at the proposed CY 2022 ESRD PPS base rate, would increase by $1 million in CY 2022 compared to CY 2021.
3. Impacts of the Proposed ESRD QIP
Our proposals to suppress measures for the PY 2022 ESRD QIP and to revise the scoring and payment methodology such that no facility will receive a payment reduction necessitates a modification to our previous estimated overall economic impact of the PY 2022 ESRD QIP (84 FR 60651). In the CY 2020 ESRD PPS final rule, we estimated that the overall economic impact of the PY 2022 ESRD QIP would be approximately $229 million as a result of the policies we had finalized at that time. The $229 million figure for PY 2022 included costs associated with the collection of information requirements, which we estimated would be approximately $211 million, and $18 million in estimated payment reductions across all facilities. However, as a result of the proposals impacting the PY 2022 ESRD QIP we are making in this proposed rule, we are modifying our previous estimate. We now estimate that the overall economic impact of the PY 2022 ESRD QIP would be approximately $215 million. The $215 million figure for PY 2022 includes costs associated with the collection of information requirements. If our proposals are finalized as proposed, there would be no payment reductions in PY 2022. We estimate that the overall economic impact of the PY 2024 ESRD QIP would be approximately $232 million as a result of the policies we have previously finalized and the proposals in this proposed rule. The $232 million figure for PY 2024 includes costs associated with the collection of information requirements, which we estimate would be approximately $215 million, and $17 million in estimated payment reductions across all facilities. We also estimate that the overall economic impact of the PY 2025 ESRD QIP would be approximately $232 million as a result of the policies we have previously finalized.
4. Impacts of Proposed Changes to the ETC Model
The impact estimate in section IX.B.4 of this proposed rule describes the estimated change in anticipated Medicare program savings arising from Start Printed Page 36326the ETC Model over the duration of the ETC Model as a result of the changes proposed in this proposed rule. We estimate that the ETC Model would result in $38 million in net savings over the 6.5-year duration of the ETC Model. We also estimate that $7 million of the estimated $38 million in net savings would be attributable to changes proposed in this proposed rule.
II. Calendar Year (CY) 2022 End-Stage Renal Disease (ESRD) Prospective Payment System (PPS)
A. Background
1. Statutory Background
On January 1, 2011, the Centers for Medicare & Medicaid Services (CMS) implemented the End-Stage Renal Disease (ESRD) Prospective Payment System (PPS), a case-mix adjusted bundled PPS for renal dialysis services furnished by ESRD facilities, as required by section 1881(b)(14) of the Social Security Act (the Act), as added by section 153(b) of the Medicare Improvements for Patients and Providers Act of 2008 (MIPPA). Section 1881(b)(14)(F) of the Act, as added by section 153(b) of MIPPA and amended by section 3401(h) of the Patient Protection and Affordable Care Act (the Affordable Care Act), established that beginning with CY 2012, and each subsequent year, the Secretary of the Department of Health and Human Services (the Secretary) shall annually increase payment amounts by an ESRD market basket increase factor reduced by the productivity adjustment described in section 1886(b)(3)(B)(xi)(II) of the Act.
Section 632 of the American Taxpayer Relief Act of 2012 (ATRA) (Pub. L. 112-240) included several provisions that apply to the ESRD PPS. Section 632(a) of ATRA added section 1881(b)(14)(I) to the Act, which required the Secretary, by comparing per patient utilization data from 2007 with such data from 2012, to reduce the single payment for renal dialysis services furnished on or after January 1, 2014 to reflect the Secretary's estimate of the change in the utilization of ESRD-related drugs and biologicals (excluding oral-only ESRD-related drugs). Consistent with this requirement, in the CY 2014 ESRD PPS final rule we finalized $29.93 as the total drug utilization reduction and finalized a policy to implement the amount over a 3- to 4-year transition period (78 FR 72161 through 72170).
Section 632(b) of ATRA prohibited the Secretary from paying for oral-only ESRD-related drugs and biologicals under the ESRD PPS prior to January 1, 2016. Section 632(c) of ATRA required the Secretary, by no later than January 1, 2016, to analyze the case-mix payment adjustments under section 1881(b)(14)(D)(i) of the Act and make appropriate revisions to those adjustments.
On April 1, 2014, the Protecting Access to Medicare Act of 2014 (PAMA) (Pub. L. 113-93) was enacted. Section 217 of PAMA included several provisions that apply to the ESRD PPS. Specifically, sections 217(b)(1) and (2) of PAMA amended sections 1881(b)(14)(F) and (I) of the Act and replaced the drug utilization adjustment that was finalized in the CY 2014 ESRD PPS final rule (78 FR 72161 through 72170) with specific provisions that dictated the market basket update for CY 2015 (0.0 percent) and how the market basket should be reduced in CY 2016 through CY 2018.
Section 217(a)(1) of PAMA amended section 632(b)(1) of ATRA to provide that the Secretary may not pay for oral-only ESRD-related drugs under the ESRD PPS prior to January 1, 2024. Section 217(a)(2) of PAMA further amended section 632(b)(1) of ATRA by requiring that in establishing payment for oral-only drugs under the ESRD PPS, the Secretary must use data from the most recent year available. Section 217(c) of PAMA provided that as part of the CY 2016 ESRD PPS rulemaking, the Secretary shall establish a process for (1) determining when a product is no longer an oral-only drug; and (2) including new injectable and intravenous products into the ESRD PPS bundled payment.
Finally, on December 19, 2014, the President signed the Stephen Beck, Jr., Achieving a Better Life Experience Act of 2014 (ABLE) (Pub. L. 113-295). Section 204 of ABLE amended section 632(b)(1) of ATRA, as amended by section 217(a)(1) of PAMA, to provide that payment for oral-only renal dialysis services cannot be made under the ESRD PPS bundled payment prior to January 1, 2025.
2. System for Payment of Renal Dialysis Services
Under the ESRD PPS, a single per-treatment payment is made to an ESRD facility for all of the renal dialysis services defined in section 1881(b)(14)(B) of the Act and furnished to individuals for the treatment of ESRD in the ESRD facility or in a patient's home. We have codified our definitions of renal dialysis services at § 413.171, which is in 42 CFR part 413, subpart H, along with other ESRD PPS payment policies. The ESRD PPS base rate is adjusted for characteristics of both adult and pediatric patients and accounts for patient case-mix variability. The adult case-mix adjusters include five categories of age, body surface area, low body mass index, onset of dialysis, and four comorbidity categories (that is, pericarditis, gastrointestinal tract bleeding, hereditary hemolytic or sickle cell anemia, myelodysplastic syndrome). A different set of case-mix adjusters are applied for the pediatric population. Pediatric patient-level adjusters include two age categories (under age 22, or age 22-26) and two dialysis modalities (that is, peritoneal or hemodialysis) (§ 413.235(a) and (b)).
The ESRD PPS provides for three facility-level adjustments. The first payment adjustment accounts for ESRD facilities furnishing a low volume of dialysis treatments (§ 413.232). The second adjustment reflects differences in area wage levels developed from core-based statistical areas (CBSAs) (§ 413.231). The third payment adjustment accounts for ESRD facilities furnishing renal dialysis services in a rural area (§ 413.233).
There are four additional payment adjustments under the ESRD PPS. The ESRD PPS provides adjustments, when applicable, for: (1) A training add-on for home and self-dialysis modalities (§ 413.235(c)); (2) an additional payment for high cost outliers due to unusual variations in the type or amount of medically necessary care (§ 413.237); (3) a transitional drug add-on payment adjustment (TDAPA) for certain new renal dialysis drugs and biological products (§ 413.234(c)); and (4) a transitional add-on payment adjustment for new and innovative equipment and supplies (TPNIES) for certain qualifying, new and innovative renal dialysis equipment and supplies (§ 413.236(d)).
3. Updates to the ESRD PPS
Policy changes to the ESRD PPS are proposed and finalized annually in the Federal Register. The CY 2011 ESRD PPS final rule was published on August 12, 2010 in the Federal Register (75 FR 49030 through 49214). That rule implemented the ESRD PPS beginning on January 1, 2011 in accordance with section 1881(b)(14) of the Act, as added by section 153(b) of MIPPA, over a 4-year transition period. Since the implementation of the ESRD PPS, we have published annual rules to make routine updates, policy changes, and clarifications.
On November 9, 2020, we published a final rule in the Federal Register titled, “Medicare Program; End-Stage Renal Disease Prospective Payment System, Payment for Renal Dialysis Services Furnished to Individuals With Acute Kidney Injury, and End-Stage Start Printed Page 36327Renal Disease Quality Incentive Program,” referred to herein as the “CY 2021 ESRD PPS final rule”. In that rule, we updated the ESRD PPS base rate, wage index, and outlier policy, for CY 2021. We also finalized an update to the ESRD PPS wage index to adopt the 2018 OMB delineations with a transition period, changes to the eligibility criteria and determination process for the TPNIES, an expansion of the TPNIES to include certain new and innovative capital-related assets that are home dialysis machines, an addition to the ESRD PPS base rate to include calcimimetics in the ESRD PPS bundled payment, and a change to the low-volume payment adjustment eligibility criteria and attestation requirement to account for the coronavirus disease 2019 (COVID-19) Public Health Emergency (PHE). For further detailed information regarding these updates, see 85 FR 71398.
B. Provisions of the Proposed Rule
1. Proposed CY 2022 ESRD PPS Update
a. Proposed CY 2022 ESRD Bundled (ESRDB) Market Basket Update, Productivity Adjustment, and Labor-Related Share
In accordance with section 1881(b)(14)(F)(i) of the Act, as added by section 153(b) of MIPPA and amended by section 3401(h) of the Affordable Care Act, beginning in 2012, the ESRD PPS payment amounts are required to be annually increased by an ESRD market basket increase factor and reduced by the productivity adjustment described in section 1886(b)(3)(B)(xi)(II) of the Act. The application of the productivity adjustment may result in the increase factor being less than 0.0 percent for a year and may result in payment rates for a year being less than the payment rates for the preceding year. The statute also provides that the market basket increase factor should reflect the changes over time in the prices of an appropriate mix of goods and services used to furnish renal dialysis services.
As required under section 1881(b)(14)(F)(i) of the Act, CMS developed an all-inclusive ESRD Bundled (ESRDB) input price index (75 FR 49151 through 49162). In the CY 2015 ESRD PPS final rule we rebased and revised the ESRDB input price index to reflect a 2012 base year (79 FR 66129 through 66136). Subsequently, in the CY 2019 ESRD PPS final rule, we finalized a rebased ESRDB input price index to reflect a 2016 base year (83 FR 56951 through 56962).
Although “market basket” technically describes the mix of goods and services used for ESRD treatment, this term is also commonly used to denote the input price index (that is, cost categories, their respective weights, and price proxies combined) derived from a market basket. Accordingly, the term “ESRDB market basket,” as used in this document, refers to the ESRDB input price index.
We propose to use the CY 2016-based ESRDB market basket as finalized and described in the CY 2019 ESRD PPS final rule (83 FR 56951 through 56962) to compute the CY 2022 ESRDB market basket increase factor based on the best available data. Consistent with historical practice, we propose to estimate the ESRDB market basket update based on IHS Global Inc.'s (IGI's) forecast using the most recently available data. IGI is a nationally recognized economic and financial forecasting firm with which we contract to forecast the components of the market baskets. Using this methodology and the IGI first quarter 2021 forecast of the CY 2016-based ESRDB market basket (with historical data through the fourth quarter of 2020), the proposed CY 2022 ESRDB market basket increase factor is 1.6 percent.
Under section 1881(b)(14)(F)(i) of the Act, for CY 2012 and each subsequent year, the ESRD market basket percentage increase factor shall be reduced by the productivity adjustment described in section 1886(b)(3)(B)(xi)(II) of the Act. The productivity adjustment is calculated using a projection of multifactor productivity (MFP), which is derived by subtracting the contribution of labor and capital input growth from output growth. We finalized the detailed methodology for deriving the projection of MFP in the CY 2012 ESRD PPS final rule (76 FR 40503 through 40504). The most up-to-date MFP projection methodology is available on the CMS website at https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/MedicareProgramRatesStats/Downloads/MFPMethodology.pdf. We note that for CY 2022 and beyond, CMS is changing the name of this adjustment to refer to it as the productivity adjustment, which is the term used in sections 1881(b)(14)(F)(i) and 1886(b)(3)(B)(xi)(II) of the Act, rather than the multifactor productivity or MFP adjustment. This is not a change in policy, as we will continue to use the same methodology for deriving the adjustment and rely on the same underlying data. Using this methodology and the IGI first quarter 2021 forecast, the proposed productivity adjustment for CY 2022 (the 10-year moving average of MFP for the period ending CY 2022) is projected to be 0.6 percent.
As a result of these provisions, the proposed CY 2022 ESRD market basket increase factor reduced by the productivity adjustment is 1.0 percent. The proposed market basket increase factor is calculated by starting with the proposed CY 2022 ESRDB market basket percentage increase factor of 1.6 percent and reducing it by the proposed productivity adjustment (the 10-year moving average of MFP for the period ending CY 2022) of 0.6 percent.
As is our general practice, we are proposing that if more recent data become available after the publication of this proposed rule and before the publication of the final rule (for example, a more recent estimate of the CY 2016-based ESRD market basket increase factor or productivity adjustment), we would use such data, if appropriate, to determine the final CY 2022 market basket update and productivity adjustment.
For the CY 2022 ESRD payment update, we propose to continue using a labor-related share of 52.3 percent for the ESRD PPS payment, which was finalized in the CY 2019 ESRD PPS final rule (83 FR 56963).
b. The Proposed CY 2022 ESRD PPS Wage Indices
(1) Background
Section 1881(b)(14)(D)(iv)(II) of the Act provides that the ESRD PPS may include a geographic wage index payment adjustment, such as the index referred to in section 1881(b)(12)(D) of the Act, as the Secretary determines to be appropriate. In the CY 2011 ESRD PPS final rule (75 FR 49200), we finalized an adjustment for wages at § 413.231. Specifically, CMS adjusts the labor-related portion of the base rate to account for geographic differences in the area wage levels using an appropriate wage index, which reflects the relative level of hospital wages and wage-related costs in the geographic area in which the ESRD facility is located. We use OMB's CBSA-based geographic area designations to define urban and rural areas and their corresponding wage index values (75 FR 49117). OMB publishes bulletins regarding CBSA changes, including changes to CBSA numbers and titles. The bulletins are available online at https://www.whitehouse.gov/omb/information-for-agencies/bulletins/.
For CY 2022, we would update the wage indices to account for updated wage levels in areas in which ESRD facilities are located using our existing methodology. We use the most recent Start Printed Page 36328pre-floor, pre-reclassified hospital wage data collected annually under the inpatient PPS. The ESRD PPS wage index values are calculated without regard to geographic reclassifications authorized under sections 1886(d)(8) and (d)(10) of the Act and utilize prefloor hospital data that are unadjusted for occupational mix. For CY 2022, the updated wage data are for hospital cost reporting periods beginning on or after October 1, 2017, and before October 1, 2018 (fiscal year [FY] 2018 cost report data).
We have also adopted methodologies for calculating wage index values for ESRD facilities that are located in urban and rural areas where there is no hospital data. For a full discussion, see CY 2011 and CY 2012 ESRD PPS final rules at 75 FR 49116 through 49117 and 76 FR 70239 through 70241, respectively. For urban areas with no hospital data, we compute the average wage index value of all urban areas within the state to serve as a reasonable proxy for the wage index of that urban CBSA, that is, we use that value as the wage index. For rural areas with no hospital data, we compute the wage index using the average wage index values from all contiguous CBSAs to represent a reasonable proxy for that rural area. We apply the statewide urban average based on the average of all urban areas within the state to Hinesville-Fort Stewart, Georgia (78 FR 72173), and we apply the wage index for Guam to American Samoa and the Northern Mariana Islands (78 FR 72172).[1]
A wage index floor value (0.5000) is applied under the ESRD PPS as a substitute wage index for areas with very low wage index values. Currently, all areas with wage index values that fall below the floor are located in Puerto Rico. However, the wage index floor value is applicable for any area that may fall below the floor. A description of the history of the wage index floor under the ESRD PPS can be found in the CY 2019 ESRD PPS final rule (83 FR 56964 through 56967).
An ESRD facility's wage index is applied to the labor-related share of the ESRD PPS base rate. In the CY 2019 ESRD PPS final rule (83 FR 56963), we finalized a labor-related share of 52.3 percent, which is based on the 2016-based ESRDB market basket. In the CY 2021 ESRD PPS final rule (85 FR 71436), we updated the OMB delineations as described in the September 14, 2018 OMB Bulletin No. 18-04, beginning with the CY 2021 ESRD PPS wage index. In addition, we finalized the application of a 5 percent cap on any decrease in an ESRD facility's wage index from the ESRD facility's wage index from the prior CY. We finalized that the transition would be phased in over 2 years, such that the reduction in an ESRD facility's wage index would be capped at 5 percent in CY 2021, and no cap would be applied to the reduction in the wage index for the second year, CY 2022. Thus, for CY 2022, the labor-related share to which a facility's wage index would be applied is 52.3 percent.
For CY 2022, we are proposing to update the ESRD PPS wage index to use the most recent hospital wage data. The proposed CY 2022 ESRD PPS wage index is set forth in Addendum A and is available on the CMS website at https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ESRDpayment/End-Stage-Renal-Disease-ESRD-Payment-Regulations-and-Notices. Addendum A provides a crosswalk between the CY 2021 wage index and the proposed CY 2022 wage index. Addendum B provides an ESRD facility level impact analysis. Addendum B is available on the CMS website at https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ESRDpayment/End-Stage-Renal-Disease-ESRD-Payment-Regulations-and-Notices.
c. Proposed CY 2022 Update to the Outlier Policy
Section 1881(b)(14)(D)(ii) of the Act requires that the ESRD PPS include a payment adjustment for high cost outliers due to unusual variations in the type or amount of medically necessary care, including variability in the amount of erythropoiesis-stimulating agents (ESAs) necessary for anemia management. Some examples of the patient conditions that may be reflective of higher facility costs when furnishing dialysis care would be frailty, obesity, and comorbidities, such as secondary hyperparathyroidism. The ESRD PPS recognizes high cost patients, and we have codified the outlier policy and our methodology for calculating outlier payments at § 413.237.
The policy provides that the following ESRD outlier items and services are included in the ESRD PPS bundle: (1) Renal dialysis drugs and biological products that were or would have been, prior to January 1, 2011, separately billable under Medicare Part B; (2) renal dialysis laboratory tests that were or would have been, prior to January 1, 2011, separately billable under Medicare Part B ; (3) renal dialysis medical/surgical supplies, including syringes, used to administer renal dialysis drugs and biological products that were or would have been, prior to January 1, 2011, separately billable under Medicare Part B; (4) renal dialysis drugs and biological products that were or would have been, prior to January 1, 2011, covered under Medicare Part D, including renal dialysis oral-only drugs effective January 1, 2025; and (5) renal dialysis equipment and supplies, except for capital-related assets that are home dialysis machines(as defined in § 413.236(a)(2)), that receive the transitional add-on payment adjustment as specified in § 413.236 after the payment period has ended.
In the CY 2011 ESRD PPS final rule (75 FR 49142), CMS stated that for purposes of determining whether an ESRD facility would be eligible for an outlier payment, it would be necessary for the facility to identify the actual ESRD outlier services furnished to the patient by line item (that is, date of service) on the monthly claim. Renal dialysis drugs, laboratory tests, and medical/surgical supplies that are recognized as outlier services were specified in Transmittal 2134, dated January 14, 2011.[2] https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/downloads/R2134CP.pdf. Furthermore, CMS uses administrative issuances to update the renal dialysis service items available for outlier payment via our quarterly update CMS Change Requests, when applicable. For example, we use these updates to identify renal dialysis service drugs that were or would have been covered under Medicare Part D for outlier eligibility purposes and items and services that have been incorrectly identified as eligible outlier services.
Under § 413.237, an ESRD facility is eligible for an outlier payment if its actual or imputed Medicare Allowable Payment (MAP) amount per treatment for ESRD outlier services exceeds a threshold. The MAP amount represents the average incurred amount per treatment for services that were or would have been considered separately billable services prior to January 1, 2011. The threshold is equal to the ESRD facility's predicted ESRD outlier services MAP amount per treatment (which is case-mix adjusted and described in the following paragraphs) Start Printed Page 36329plus the fixed-dollar loss (FDL) amount. In accordance with § 413.237(c), facilities are paid 80 percent of the per treatment amount by which the imputed MAP amount for outlier services (that is, the actual incurred amount) exceeds this threshold. ESRD facilities are eligible to receive outlier payments for treating both adult and pediatric dialysis patients.
In the CY 2011 ESRD PPS final rule and codified in § 413.220(b)(4), using 2007 data, we established the outlier percentage, which is used to reduce the per treatment base rate to account for the proportion of the estimated total payments under the ESRD PPS that are outlier payments, at 1.0 percent of total payments (75 FR 49142 through 49143). We also established the FDL amounts that are added to the predicted outlier services MAP amounts. The outlier services MAP amounts and FDL amounts are different for adult and pediatric patients due to differences in the utilization of separately billable services among adult and pediatric patients (75 FR 49140). As we explained in the CY 2011 ESRD PPS final rule (75 FR 49138 through 49139), the predicted outlier services MAP amounts for a patient are determined by multiplying the adjusted average outlier services MAP amount by the product of the patient-specific case-mix adjusters applicable using the outlier services payment multipliers developed from the regression analysis used to compute the payment adjustments.
For CY 2022, we propose that the outlier services MAP amounts and FDL amounts would be derived from claims data from CY 2020. Because we believe that any adjustments made to the MAP amounts under the ESRD PPS should be based upon the most recent data year available in order to best predict any future outlier payments, we propose the outlier thresholds for CY 2022 would be based on utilization of renal dialysis items and services furnished under the ESRD PPS in CY 2020.
We recognize that the utilization of ESAs and other outlier services have continued to decline under the ESRD PPS, and that we have lowered the MAP amounts and FDL amounts every year under the ESRD PPS. As discussed in the CY 2021 ESRD PPS final rule (85 FR 71438), CY 2019 claims data show outlier payments represented approximately 0.5 percent of total payments. As discussed in section II.B.1.c.(1) of this proposed rule, CY 2020 claims data show outlier payments represent approximately 0.6 percent of total payments.
(1) CY 2022 Update to the Outlier Services MAP Amounts and FDL Amounts
For CY 2022, we propose to update the outlier services MAP amounts and FDL amounts to reflect the utilization of outlier services reported on 2020 claims. For this proposed rule, the outlier services MAP amounts and FDL amounts were updated using 2020 claims data. The impact of this update is shown in Table 1, which compares the outlier services MAP amounts and FDL amounts used for the outlier policy in CY 2021 with the updated proposed estimates for this rule. The estimates for the proposed CY 2022 outlier policy, which are included in Column II of Table 1, were inflation adjusted to reflect projected 2022 prices for outlier services.

The estimated FDL amount per treatment that determines the CY 2022 outlier threshold amount for adults (Column II; $111.18) is lower than that used for the CY 2021 outlier policy (Column I; $122.49). The lower threshold is accompanied by a decrease in the adjusted average MAP for outlier services from $50.92 to $47.87. For Start Printed Page 36330pediatric patients, there is a decrease in the FDL amount from $44.78 to $30.38. There is a corresponding decrease in the adjusted average MAP for outlier services among pediatric patients, from $30.08 to $28.73.
We estimate that the percentage of patient months qualifying for outlier payments in CY 2022 would be 5.45 percent for adult patients and 11.37 percent for pediatric patients, based on the 2020 claims data. The outlier MAP and FDL amounts continue to be lower for pediatric patients than adults due to the continued lower use of outlier services (primarily reflecting lower use of ESAs and other injectable drugs).
(2) Outlier Percentage
In the CY 2011 ESRD PPS final rule (75 FR 49081) and under § 413.220(b)(4), we reduced the per treatment base rate by 1 percent to account for the proportion of the estimated total payments under the ESRD PPS that are outlier payments as described in § 413.237. Based on the 2020 claims, outlier payments represented approximately 0.6 percent of total payments, which is below the 1 percent target due to declines in the use of outlier services. As noted in past rulemaking, recalibration of the thresholds using 2020 data is expected to result in aggregate outlier payments close to the 1 percent target in CY 2022. We believe the update to the outlier MAP and FDL amounts for CY 2022 would increase payments for ESRD beneficiaries requiring higher resource utilization. This would move us closer to meeting our 1 percent outlier policy goal, because we are using more current data for computing the MAP and FDL, which is more in line with current outlier services utilization rates. We note that recalibration of the FDL amounts in this proposed rule would result in no change in payments to ESRD facilities for beneficiaries with renal dialysis items and services that are not eligible for outlier payments.
d. Proposed Impacts to the CY 2022 ESRD PPS Base Rate
(1) ESRD PPS Base Rate
In the CY 2011 ESRD PPS final rule (75 FR 49071 through 49083), CMS established the methodology for calculating the ESRD PPS per-treatment base rate, that is, ESRD PPS base rate, and calculating the per treatment payment amount, which are codified at §§ 413.220 and 413.230. The CY 2011 ESRD PPS final rule also provides a detailed discussion of the methodology used to calculate the ESRD PPS base rate and the computation of factors used to adjust the ESRD PPS base rate for projected outlier payments and budget neutrality in accordance with sections 1881(b)(14)(D)(ii) and 1881(b)(14)(A)(ii) of the Act, respectively. Specifically, the ESRD PPS base rate was developed from CY 2007 claims (that is, the lowest per patient utilization year as required by section 1881(b)(14)(A)(ii) of the Act), updated to CY 2011, and represented the average per treatment MAP for composite rate and separately billable services. In accordance with section 1881(b)(14)(D) of the Act and our regulation at § 413.230, the per-treatment payment amount is the sum of the ESRD PPS base rate, adjusted for the patient specific case-mix adjustments, applicable facility adjustments, geographic differences in area wage levels using an area wage index, and any applicable outlier payment, training adjustment add-on, TDAPA, and TPNIES.
(2) Annual Payment Rate Update for CY 2022
We are proposing an ESRD PPS base rate for CY 2022 of $255.55. This update reflects several factors, described in more detail as follows:
Wage Index Budget-Neutrality Adjustment Factor: We compute a wage index budget-neutrality adjustment factor that is applied to the ESRD PPS base rate. For CY 2022, we are not proposing any changes to the methodology used to calculate this factor, which is described in detail in the CY 2014 ESRD PPS final rule (78 FR 72174). We computed the proposed CY 2022 wage index budget-neutrality adjustment factor using treatment counts from the 2020 claims and facility-specific CY 2021 payment rates to estimate the total dollar amount that each ESRD facility would have received in CY 2021. The total of these payments became the target amount of expenditures for all ESRD facilities for CY 2022. Next, we computed the estimated dollar amount that would have been paid for the same ESRD facilities using the ESRD PPS wage index for CY 2022. As discussed in section II.B.1.b of this proposed rule, the proposed ESRD PPS wage index for CY 2022 includes an update to the most recent hospital wage data, use of the 2018 OMB delineations, and no cap on wage index decreases applied for CY 2022. The total of these payments becomes the new CY 2022 amount of wage-adjusted expenditures for all ESRD facilities. The wage index budget-neutrality factor is calculated as the target amount divided by the new CY 2022 amount. When we multiplied the wage index budget neutrality factor by the applicable CY 2022 estimated payments, aggregate payments to ESRD facilities would remain budget neutral when compared to the target amount of expenditures. That is, the wage index budget neutrality adjustment factor ensures that wage index adjustments do not increase or decrease aggregate Medicare payments with respect to changes in wage index updates. The CY 2022 proposed wage index budget-neutrality adjustment factor is .999546. This application would yield a CY 2022 ESRD PPS proposed base rate of $253.02 prior to the application of the proposed market basket increase ($253.13 × .999546 = $253.02).
Market Basket Increase: Section 1881(b)(14)(F)(i)(I) of the Act provides that, beginning in 2012, the ESRD PPS payment amounts are required to be annually increased by the ESRD market basket percentage increase factor. The latest CY 2022 projection of the proposed ESRDB market basket percentage increase factor is 1.6 percent. In CY 2022, this amount must be reduced by the productivity adjustment described in section 1886(b)(3)(B)(xi)(II) of the Act, as required by section 1881(b)(14)(F)(i)(II) of the Act. As discussed previously, the proposed productivity adjustment for CY 2021 is 0.6 percent, thus yielding a proposed update to the base rate of 1.0 percent for CY 2022. Therefore, the CY 2022 ESRD PPS proposed base rate is $255.55 ($253.02 × 1.010 = $255.55).
In summary, we are proposing a CY 2022 ESRD PPS base rate of $255.55. This amount reflects a proposed CY 2022 wage index budget-neutrality adjustment factor of .999546, and the CY 2022 ESRD PPS productivity-adjusted market basket update of 1.0 percent.
e. Update to the Offset Amount for TPNIES
In the CY 2021 ESRD PPS final rule (85 FR 71427), we expanded eligibility for the TPNIES under § 413.236 to include certain capital-related assets that are home dialysis machines when used in the home for a single patient. We finalized the additional steps that the Medicare Administrative Contractors (MACs) must follow to establish the basis of payment of the TPNIES for these capital-related assets that are home dialysis machines when used in the home, including an offset to the pre-adjusted per treatment amount to account for the cost of the home dialysis machine that is already in the ESRD PPS base rate. We will pay 65 percent of the MAC-determined preadjusted per treatment amount reduced by an offset for 2-calendar Start Printed Page 36331years. Section § 413.236(f)(3)(v) states that effective January 1, 2022, CMS will annually update the amount determined in paragraph (f)(3)(iv) of § 413.236 by the ESRD bundled market basket percentage increase factor minus the productivity adjustment factor.
The CY 2021 offset amount for TPNIES for capital-related equipment that are home dialysis machines used in the home is $9.32. As discussed previously in section II.B.1.a of this proposed rule, the proposed CY 2022 ESRD bundled market basket increase factor minus the productivity adjustment is 1.0 percent (1.6 percent minus 0.6 percent). Applying the proposed update factor of 1.010 to the CY 2021 offset amount results in a proposed CY 2022 offset amount of $9.41($9.32 × 1.010). We will update this calculation to use the most recent data available in the CY 2022 ESRD PPS final rule.
C. Proposed Transitional Add-On Payment Adjustment for New and Innovative Equipment and Supplies (TPNIES) for CY 2022 Payment
1. Background
In the CY 2020 ESRD PPS final rule (84 FR 60681 through 60698), CMS established the transitional add-on payment adjustment for new and innovative equipment and supplies (TPNIES) under the ESRD PPS, under the authority of section 1881(b)(14)(D)(iv) of the Act, in order to support ESRD facility use and beneficiary access to these new technologies. We established this add-on payment adjustment to help address the unique circumstances experienced by ESRD facilities when incorporating new and innovative equipment and supplies into their businesses and to support ESRD facilities transitioning or testing these products during the period when they are new to market. We added § 413.236 to establish the eligibility criteria and payment policies for the TPNIES.
In the CY 2020 ESRD PPS final rule (84 FR 60650), we established in § 413.236(b) that for dates of service occurring on or after January 1, 2020, we will provide the TPNIES to an ESRD facility for furnishing a covered equipment or supply only if the item: (1) Has been designated by CMS as a renal dialysis service under § 413.171; (2) is new, meaning granted marketing authorization by the Food and Drug Administration (FDA) on or after January 1, 2020; (3) is commercially available by January 1 of the particular calendar year, meaning the year in which the payment adjustment would take effect; (4) has a Healthcare Common Procedure Coding System (HCPCS) application submitted in accordance with the official Level II HCPCS coding procedures by September 1 of the particular calendar year; (5) is innovative, meaning it meets the SCI criteria specified in the Inpatient Prospective Payment System (IPPS) regulations at 42 CFR 412.87(b)(1) and related guidance, and (6) is not a capital related asset that an ESRD facility has an economic interest in through ownership (regardless of the manner in which it was acquired).
Regarding the innovation requirement in § 413.236(b)(5), in the CY 2020 ESRD PPS final rule (84 FR 60690), we stated that we will use the following criteria to evaluate SCI for purposes of the TPNIES under the ESRD PPS based on the IPPS SCI criteria in § 412.87(b)(1) and related guidance:
A new technology represents an advance that substantially improves, relative to renal dialysis services previously available, the diagnosis or treatment of Medicare beneficiaries. First, CMS considers the totality of the circumstances when making a determination that a new renal dialysis equipment or supply represents an advance that substantially improves, relative to renal dialysis services previously available, the diagnosis or treatment of Medicare beneficiaries. Second, a determination that a new renal dialysis equipment or supply represents an advance that substantially improves, relative to renal dialysis services previously available, the diagnosis or treatment of Medicare beneficiaries means one of the following:
- The new renal dialysis equipment or supply offers a treatment option for a patient population unresponsive to, or ineligible for, currently available treatments; or
- The new renal dialysis equipment or supply offers the ability to diagnose a medical condition in a patient population where that medical condition is currently undetectable, or offers the ability to diagnose a medical condition earlier in a patient population than allowed by currently available methods, and there must also be evidence that use of the new renal dialysis service to make a diagnosis affects the management of the patient; or
- The use of the new renal dialysis equipment or supply significantly improves clinical outcomes relative to renal dialysis services previously available as demonstrated by one or more of the following: A reduction in at least one clinically significant adverse event, including a reduction in mortality or a clinically significant complication; a decreased rate of at least one subsequent diagnostic or therapeutic intervention; a decreased number of future hospitalizations or physician visits; a more rapid beneficial resolution of the disease process treatment including, but not limited to, a reduced length of stay or recovery time; an improvement in one or more activities of daily living; an improved quality of life; or, a demonstrated greater medication adherence or compliance; or,
- The totality of the circumstances otherwise demonstrates that the new renal dialysis equipment or supply substantially improves, relative to renal dialysis services previously available, the diagnosis or treatment of Medicare beneficiaries.
Third, evidence from the following published or unpublished information sources from within the U.S. or elsewhere may be sufficient to establish that a new renal dialysis equipment or supply represents an advance that substantially improves, relative to renal dialysis services previously available, the diagnosis or treatment of Medicare beneficiaries: Clinical trials, peer reviewed journal articles; study results; meta-analyses; consensus statements; white papers; patient surveys; case studies; reports; systematic literature reviews; letters from major healthcare associations; editorials and letters to the editor; and public comments. Other appropriate information sources may be considered.
Fourth, the medical condition diagnosed or treated by the new renal dialysis equipment or supply may have a low prevalence among Medicare beneficiaries. Fifth, the new renal dialysis equipment or supply may represent an advance that substantially improves, relative to services or technologies previously available, the diagnosis or treatment of a subpopulation of patients with the medical condition diagnosed or treated by the new renal dialysis equipment or supply.
In the CY 2020 ESRD PPS final rule (84 FR 60681 through 60698), we also established a process modeled after IPPS's process of determining if a new medical service or technology meets the SCI criteria specified in § 412.87(b)(1). Specifically, similar to the IPPS New Technology Add-On Payment, we wanted to align our goals with the agency's efforts to transform the healthcare delivery system for the ESRD beneficiary through competition and innovation to provide patients with better value and results. As we discuss in the CY 2020 ESRD PPS final rule (84 Start Printed Page 36332FR 60682), we believe it is appropriate to facilitate access to new and innovative equipment and supplies through add-on payments similar to the IPPS New Technology Add-On Payment and to provide stakeholders with standard criteria for both inpatient and outpatient settings. In § 413.236(c), we established a process for our announcement of TPNIES determinations and a deadline for consideration of new renal dialysis equipment or supply applications under the ESRD PPS. CMS will consider whether a new renal dialysis equipment or supply meets the eligibility criteria specified in § 413.236(b) and summarize the applications received in the annual ESRD PPS proposed rules. Then, after consideration of public comments, we will announce the results in the Federal Register as part of our annual updates and changes to the ESRD PPS in the ESRD PPS final rule. In the CY 2020 ESRD PPS final rule, we also specified certain deadlines for the application requirements. We noted that we would only consider a complete application received by February 1 prior to the particular calendar year. In addition, we required that FDA marketing authorization for the equipment or supply must occur by September 1 prior to the particular calendar year. We also stated in the CY 2020 ESRD PPS final rule (84 FR 60690 through 60691) that we would establish a workgroup of CMS medical and other staff to review the materials submitted as part of the TPNIES application, public comments, FDA marketing authorization, and HCPCS application information and assess the extent to which the product provides SCI over current technologies.
In the CY 2020 ESRD PPS final rule, we established § 413.236(d) to provide a payment adjustment for a new and innovative renal dialysis equipment or supply. We stated that the TPNIES is paid for 2-calendar years. Following payment of the TPNIES, the ESRD PPS base rate will not be modified and the new and innovative renal dialysis equipment or supply will become an eligible outlier service as provided in § 413.237.
Regarding the basis of payment for the TPNIES, in the CY 2020 ESRD PPS final rule, we finalized at § 413.236(e) that the TPNIES is based on 65 percent of the price established by the MACs, using the information from the invoice and other specified sources of information. In the CY 2021 ESRD PPS final rule (85 FR 71410 through 71464), we made several changes to the TPNIES eligibility criteria at § 413.236. First, we revised the definition of new at § 413.236(b)(2) as within 3 years beginning on the date of the FDA marketing authorization. Second, we changed the deadline for TPNIES applicants' HCPCS Level II code application submission from September 1 of the particular calendar year to the HCPCS Level II code application deadline for biannual Coding Cycle 2 for durable medical equipment, orthotics, prosthetics, and supplies (DMEPOS) items and services as specified in the HCPCS Level II coding guidance on the CMS website prior to the calendar year. In addition, a copy of the applicable FDA marketing authorization must be submitted to CMS by the HCPCS Level II code application deadline for biannual Coding Cycle 2 for DMEPOS items and services as specified in the HCPCS Level II coding guidance on the CMS website in order for the equipment or supply to be eligible for the TPNIES the following year. Third, we revised § 413.236(b)(5) to remove a reference to related guidance on the SCI criterion, as the guidance has already been codified.
Finally, in the CY 2021 ESRD PPS final rule, we expanded the TPNIES policy to include certain capital-related assets that are home dialysis machines when used in the home for a single patient. We explained that capital-related assets are defined in the Provider Reimbursement Manual (chapter 1, section 104.1) as assets that a provider has an economic interest in through ownership (regardless of the manner in which they were acquired). We noted that examples of capital-related assets for ESRD facilities are dialysis machines and water purification systems. We explained that while in the CY 2020 ESRD PPS proposed rule (84 FR 38354), we stated that we did not believe capital-related assets should be eligible for additional payment through the TPNIES because the cost of these items is captured in cost reports, they depreciate over time, and are generally used for multiple patients, there were a number of other factors we considered that led us to consider expanding eligibility for these technologies in the CY 2021 ESRD PPS rulemaking. We explained that, following publication of the CY 2020 ESRD PPS final rule, we continued to study the issue of payment for capital-related assets under the ESRD PPS, taking into account information from a wide variety of stakeholders and recent developments and initiatives regarding kidney care. For example, we considered various HHS home dialysis initiatives, Executive Orders to transform kidney care, and how the risk of COVID-19 for particularly vulnerable ESRD beneficiaries could be mitigated by encouraging home dialysis. After closely considering these issues, we proposed a revision to § 413.236(b)(6) in the CY 2021 ESRD PPS proposed rule to provide an exception to the general exclusion for capital-related assets from eligibility for the TPNIES for capital-related assets that are home dialysis machines when used in the home for a single patient and that meet the other eligibility criteria in § 413.235(b), and finalized the exception as proposed. We finalized the same determination process for TPNIES applications for capital-related assets that are home dialysis machines as for all other TPNIES applications; that we will provide a description of the new home dialysis machine and pertinent facts in the ESRD PPS proposed rule so the public may comment and then publish the results in the ESRD PPS final rule. We will consider whether the new home dialysis machine meets the eligibility criteria specified in the proposed revisions to § 413.236(b) and announce the results in the Federal Register as part of our annual updates and changes to the ESRD PPS. Per § 413.236(c), we will only consider, for additional payment using the TPNIES for a particular calendar year, an application for a capital-related asset that is a home dialysis machine received by February 1 prior to the particular calendar year. If the application is not received by February 1, the application will be denied and the applicant will need to reapply within 3 years beginning on the date of FDA marketing authorization in order to be considered for the TPNIES, in accordance with the proposed revisions to § 413.236(b)(2).
In the CY 2021 ESRD PPS final rule, at § 413.236(f), we finalized a pricing methodology for capital-related assets that are home dialysis machines when used in the home for a single patient by requiring MACs to calculate the annual allowance and the preadjusted per treatment amount. The pre-adjusted per treatment amount is reduced by an estimated average per treatment offset amount to account for the costs already paid through the ESRD PPS base rate. The CY 2021 TPNIES offset amount was $9.32, and we finalized that this amount will be updated on an annual basis so that it is consistent with how the ESRD PPS base rate is updated.
We revised § 413.236(d) to reflect that we would pay 65 percent of the pre-adjusted per treatment amount minus the offset for capital-related assets that are home dialysis machines when used in the home for a single patient.
We revised § 413.236(d)(2) to reflect that following payment of the TPNIES, the ESRD PPS base rate will not be Start Printed Page 36333modified and the new and innovative renal dialysis equipment or supply will be an eligible outlier service as provided in § 413.237, except a capital-related asset that is a home dialysis machine will not be an eligible outlier service as provided in § 413.237. In summary, under the current eligibility requirements in § 413.236(b), CMS provides for a TPNIES to an ESRD facility for furnishing a covered equipment or supply only if the item: (1) Has been designated by CMS as a renal dialysis service under § 413.171; (2) Is new, meaning within 3 years beginning on the date of the FDA marketing authorization; (3) Is commercially available by January 1 of the particular calendar year, meaning the year in which the payment adjustment would take effect; (4) Has a complete HCPCS Level II code application submitted in accordance with the HCPCS Level II coding procedures on the CMS website, by the HCPCS Level II code application deadline for biannual Coding Cycle 2 for DMEPOS items and services as specified in the HCPCS Level II coding guidance on the CMS website prior to the calendar year; (5) Is innovative, meaning it meets the criteria specified in § 412.87(b)(1) of this chapter; and (6) Is not a capital-related asset, except for capital-related assets that are home dialysis machines.
We received two applications for the TPNIES for CY 2022. A discussion of these applications is presented below. The applications received are for technologies commonly used for the treatment of ESRD: Hemodialysis (HD) and peritoneal dialysis (PD). Detailed definitions for HD and PD are found in Chapter 11, Section 10 of the Medicare Benefits Policy Manual (Pub. L. 100-02).[3] In brief, HD is a process that involves blood passing through an artificial kidney machine and the waste products diffusing across a manmade membrane into a bath solution known as dialysate after which the cleansed blood is returned to the patient's body. HD is accomplished usually in 3 to 5 hour sessions, 3 times a week. PD is a process that involves waste products passing from the patient's body through the peritoneal membrane into the peritoneal (abdominal) cavity where the bath solution (dialysate) is introduced and removed periodically.
a. Tablo® System
Outset Medical, Inc. submitted an application for the TPNIES for the Tablo® System (Tablo®) for CY 2022. According to the applicant, the technology is an HD machine that has been designed for patient-driven self-care and to minimize system training time. The applicant also stated that the system is intended to substantially improve the treatment of people with ESRD by removing barriers to home dialysis. The applicant explained that the Tablo® System is comprised of (1) the Tablo® Console with integrated water purification, on-demand dialysate production, and a simple-to-use touchscreen interface; (2) a proprietary, disposable, single-use pre-strung cartridge that easily clicks into place, minimizing steps, touch points, and connections; and (3) the Tablo® Connectivity and Data Ecosystem. Per the applicant, the system is built to function in a connected setting with cloud-based system monitoring, patient analytics and clinical recordkeeping.
The applicant stated that the Tablo® System's unique features combine to provide a significantly differentiated HD solution with many benefits. First, the applicant stated that the Tablo® System's intuitive touchscreen interface makes it easy to learn and use, guiding users through treatment from start to finish using step-by-step instructions with simple words and animation. The applicant also stated that instructions include non-technical language and color-coded parts to enable easier training, faster set-up, and simpler management including clear alarm explanations and resolution instructions.
Second, the applicant stated that the Tablo® System can accommodate treatments at home allowing for flexibility in treatment frequencies, durations, and flow rates. Per the applicant, the Tablo® System does not have a pre-configured dialyzer, which allows clinicians to use a broad range of dialyzer types and manufactures, allowing for greater customization of treatment for the patient. The applicant stated that this is an improvement over the incumbent home device, which requires a separate device component and complex process to switch to another dialyzer.
Third, the applicant stated that the Tablo® System is an all-in-one system with integrated water purification and on-demand dialysate production, eliminating the need for industrial water treatment rooms that are required to operate traditional HD machines. The applicant also stated that electronic data capture and automatic wireless transmission eliminate the need for manual record keeping by the patient, care partner, or nurse. Per the applicant, a single-use Tablo® Cartridge with user-friendly pre-strung blood, saline, and infusion tubing and a series of sensor-receptors mounted to a user-friendly organizer snaps easily into the system minimizing difficult connections that require additional training. The applicant stated that automated features, including an integrated blood pressure monitor, air removal, priming, and blood return, minimize user errors, save time, and streamline the user experience.
Fourth, the applicant stated that the Tablo® System's two-way wireless connectivity and data analytics provide the ability to continuously activate new capabilities and enhancements through wireless software updates, while also enabling predictive preventative maintenance to maximize machine uptime.
The applicant stated that currently 88 percent of patients receive HD in a clinic 3 times per week, for 3.0 to 4.5 hours a day and fewer than 2 percent perform HD treatment at home.[4] The applicant stated that 25 to 36 percent of home HD patients return to in-center care within 1 year of initiating HD at home.[5 6] Per the applicant, barriers to home dialysis adoption and retention have been well studied and include treatment burden for patients and care partner fatigue; technical challenges with operating a HD machine; space, home modifications, and supplies management; patients not wanting medical equipment in the home; and safety concerns.[7 8]
Start Printed Page 36334The applicant stated that innovation in making home dialysis more accessible to patients has been lacking due to a lack of investment funding, limited incremental reimbursement for new technology, and a consolidated, price-sensitive dialysis provider market where the lack of market competition is costly and has been associated with increased hospitalizations in dialysis patients.[9] The applicant stated that the Tablo® System was designed to address many system-related barriers that result in patients resigning themselves to in-center care and/or stopping home modalities due to the burden of self-managed therapy.
The applicant stated that while PD, like HD, removes excess fluid and waste from the body, it has a different mechanism of action and relies on the body's own membrane, the peritoneum, to act as the “dialyzer”. Per the applicant, PD requires surgical placement of a catheter in the abdomen and utilizes a cleansing fluid, dialysate, that must be infused and dwell in the abdomen to remove waste products from the blood. The applicant stated that PD must be conducted daily to achieve adequate dialysis and can be conducted manually or via a cycler; while in contrast, HD directly cleanses the blood with the use of a HD machine, dialysate and a dialyzer, which acts as an artificial kidney in removing excess fluid and toxins. The applicant stated that HD also requires surgical placement of a dialysis access, which is usually in the form of a catheter or a more permanent arteriovenous fistula.[10]
The applicant asserted that PD is the dominant home therapy used around the world, but should not be solely relied upon to increase growth in home dialysis, as there are physiological contraindications.[11] The applicant also stated that there is recent evidence that post 90-day mortality is higher in PD patients than in HD patients. Per the applicant, multivariable risk-adjusted analyses demonstrate that the mortality hazard ratio of HD versus PD is 0.74 (95 percent confidence interval (CI), 0.68-0.80) in the 270 to 360-day period after starting dialysis.[12] The applicant stated that patients and clinicians should weigh the risks and benefits of both options and select the one that meets the individual patient's preferences, goals, values and physiology. Per the applicant, because PD relies on the patient's own membrane, physiologic changes can occur and result in patients who are unable to continue PD due to loss of the ability to achieve adequacy. The applicant stated that these home patients could consider home HD rather than a return to in-center and noted that the practice of transitioning from one home modality to another is acknowledged by experts to be underutilized and is particularly pronounced in the U.S., where the ratio of PD use to home HD is 6:1,[13] as compared to 4:1 in Canada.[14]
The applicant asserted that that the Tablo® System presents a significant clinical improvement over NxStage® System One (NxStage®), the current standard of home HD care, with the goal of getting patients access to easier to use technology and increasing the number of patients who can do dialysis at home. Per the applicant, NxStage® is the only other mobile HD machine that is approved for home use.
(1) Renal Dialysis Service Criterion (§ 413.236(b)(1))
With respect to the first TPNIES eligibility criterion under § 413.236(b)(1), whether the item has been designated by CMS as a renal dialysis service under § 413.171, maintenance dialysis treatments and all associated services, including historically defined dialysis-related drugs, laboratory tests, equipment, supplies, and staff time, were included in the composite rate for renal dialysis services as of December 31, 2010 (75 FR 49036). An in-home HD machine would be considered equipment necessary for the provision of maintenance dialysis and, therefore, we would consider this a renal dialysis service under § 413.171.
(2) Newness Criterion (§ 413.236(b)(2))
With respect to the second TPNIES eligibility criterion under § 413.236(b)(2), whether the item is new, meaning within 3 years beginning on the date of the FDA marketing authorization, the applicant stated that the Tablo® System received FDA marketing authorization for home use on March 31, 2020. Therefore, the Tablo® System is considered new. We note that, in reviewing the enclosure to which the March 31, 2020 FDA authorization letter refers, the applicant's Section 510(k) submission indicates that the Tablo® Cartridge was reviewed separately from the Tablo® System and has its own separate 510(k) clearance. As discussed in the CY 2021 ESRD PPS final rule, CMS determined that the cartridge did not meet the newness criterion for the TPNIES (85 FR 71464) and as such, the cartridge is not new.
(3) Commercial Availability Criterion (§ 413.236(b)(3))
With respect to the third TPNIES eligibility criterion under § 413.236(b)(3), whether the item is commercial available by January 1 of the particular calendar year, meaning the year in which the payment adjustment would take effect, the applicant stated that the Tablo® System became available for home use on April 1, 2020. Therefore, the Tablo® System is commercially available.
(4) HCPCS Level II Application Criterion (§ 413.236(b)(4))
With respect to the fourth TPNIES eligibility criterion under § 413.236(b)(4), whether the applicant submitted a HCPCS Level II code application by the July 6, 2021 deadline, the applicant stated that it intends to submit a HCPCS Level II code application by the deadline.
(5) Innovation Criterion (§§ 413.236(b)(5) and 412.87(b)(1))
With respect to the fifth TPNIES eligibility criterion under § 413.236(b)(5), that the item is innovative, meaning it meets the SCI criteria specified in § 412.87(b)(1), the applicant claimed that the Tablo® System significantly improves clinical outcomes relative to the current standard of care for home HD services, which it identified as the incumbent NxStage® home dialysis machine. The applicant presented the following SCI claims: (1) Decreased treatment frequency with adequate dialysis clearance; (2) increased adherence to dialysis treatment and retention to home therapy; and (3) improved patient Start Printed Page 36335quality of life. The applicant supported these claims with the Tablo® Investigational Device Exemption (IDE) Study [15] and secondary support from four papers [16 17 18 19] and two posters.[20 21] The applicant also provided comparison data from three studies directly related to the incumbent [22 23 24] and an additional study that, based on the timeframe of the study, likely involved participants undergoing treatment with NxStage® although the article does not directly reference the incumbent.[25]
We provide an overview of these ten sources below, followed by the applicant's summary of how the data support each claim of SCI. We conclude with a discussion of the way in which we have applied the requirements of § 413.236(b)(5) to our review of the application and a summary of our concerns. We have not included detailed summaries of the remaining supplemental content included with the application. Specifically, the applicant submitted numerous supplemental background materials related to the dialysis industry, reimbursement patterns, modalities, treatment frequencies, patient adherence, hospitalization rates, and quality of life. The applicant also submitted several letters of support for the Tablo® System; three from dialysis patients, three from nephrologists, and one from a dialysis clinic nurse. These letters emphasized benefits of the Tablo® System, including reduced frequency of dialysis treatment, improved home dialysis retention, reduced patient and caregiver burden, reduced patient fatigue, and improved patient quality of life.
(a) Applicant SCI Sources
As stated previously, the applicant's primary support for its three SCI claims comes from a prospective, multicenter, open-label, non-randomized crossover study that compared in-center and in-home HD performance using the Tablo® System. Per the applicant, this study is referred to as the Tablo® Investigational Device Exemption (IDE) Study and the original study protocol and amendments were approved by FDA and registered on http://www.clinicaltrials.gov as ID: NCT02460263. The applicant stated that of the 30 participants enrolled (17 White and 13 Black or African American), 28 (18 men and 10 women) completed the study. Thirteen of the participants had previous home HD experience with NxStage®, and the remainder had previously received conventional in-center HD care. The applicant also noted that the Tablo® IDE study sample was comprised of a representative cohort of dialysis patients and reports that it was similar to the population studied for the IDE study for the incumbent NxStage®. As described in the study protocol, the primary and secondary efficacy endpoints were a standardized weekly Kt/V of greater than or equal to 2.1 and ultrafiltration (fluid removal) value as reported by the device within ten percent of the expected fluid removal based on the ultrafiltration prescription and the Tablo® Console fluid removal algorithm, respectively.[26] We clarify that Kt/V is a value used to quantify dialysis treatment adequacy and “K” = dialyzer clearance, “t” = time, and “V” = Volume of distribution of urea. The applicant stated that each participant served as his or her own control and remained in the trial for approximately 21 weeks, during which time they were prescribed HD with the Tablo® System on a 4 times per week schedule. The applicant explained that the trial consisted of 4 treatment periods: (1) A 1 week, in-center run-in period; (2) an in-center period of 32 treatments (approximately 8 weeks) during which ESRD facility staff managed the dialysis treatments; (3) a transition period of up to 4 weeks to train the patient and care partner in managing the dialysis; and (4) a final in-home period of 32 treatments (approximately 8 weeks).
With respect to the applicant's secondary sources of support, a poster presentation from Alvarez, et al., presented dialysis adequacy data collected from a retrospective review of 29 patients' (18 males, 11 females and 17 percent Black, 10 percent Hispanic) dialysis records. The study compared Kt/V results of patients aged 34-84 receiving dialysis using the Tablo® System to patients receiving dialysis from a conventional HD machine. The majority of patients used a fistula or graft (59 percent fistula, 28 percent graft, 10 percent catheter). One hundred ninety two dialysis treatments were conducted on a thrice-weekly schedule using the Tablo® System with a dialysate flow rate of 300 mL per minute. A single pool Kt/V of greater than 1.2 was achieved in 94 percent of treatments in patients less than 90 kg with an average duration of treatment at 224 +/−29 minutes and in 79 percent of treatments in patients greater than 90 kg with an average duration of treatment at 249 +/−27 minutes. The average achieved Kt/V was 1.4 +/−0.2 among treatments provided with the Tablo® System. Eighty-eight treatments were conducted using a conventional HD machine with a dialysate flow rate of 500 mL per minute. A single pool Kt/V of greater than 1.2 was achieved in 93 percent of treatments in patients less than 90 kg with an average duration of treatment at 227 +/−21 minutes and in 83 percent of treatments in patients greater than 90 kg with an average duration of treatment at 249 +/−14 minutes. The average achieved Kt/V was 1.6 +/−0.4 among the conventional HD treatments.[27]
Next, an article from Chertow, et al., described additional data from the Tablo® IDE study (discussed previously), including health-related quality of life, to further assess the safety of home HD with the Tablo® Start Printed Page 36336System. Demographic information identified the mean age as 49.8 ± 13 years, 62 percent male, 62 percent White, 38 percent Black or African American, 23 percent Hispanic or Latino, 68 percent Not Hispanic or Latino, and 8 percent not reported, among patients established on home HD. Among the patients new to home HD, the mean age was identified as 54.2 ± 10.4 years, 65 percent male, 53 percent White, 47 percent Black or African American, 29 percent Hispanic or Latino, 71 percent Not Hispanic or Latino, and 0 percent not reported. Twenty-eight of 30 patients (93 percent) completed all trial periods. Adherence to the prescribed 4 treatments per week schedule was 96 percent in-center and 99 percent in-home. The median time to recovery was 1.5 hours during the in-center and 2 hours during the at-home phase of the trial. Median index values on the 5-level EuroQol-5 Dimension (EQ-5D-5L) (a self-assessed, health related, quality of life questionnaire) were similar during the in-center as compared to in-home dialysis at 0.832 and 0.826, respectively. Patients new to home HD had lower median values (0.751) for both in-center and in-home periods. Patients who had used home dialysis prior to the trial had higher median values during both in-center (0.903) and in-home (0.906) periods. Patients reported feeling alert or well-rested with little difficulty falling or staying asleep or feeling tired and worn out when using the Tablo® System in either environment. The authors concluded that when using the Tablo® System in-home, patients reported similar time to recovery, general health status, and sleep quality compared to using the Tablo® System in-center.[28]
Next, an article from Leypoldt, et al., described the use of uremic solute kinetic models to assess dialysis adequacy via theoretical single pool Kt/V levels when varying the dialysis blood flow rates and the patient urea volume of distribution. A comparison was made between dialysate flows of 300 and 500 mL/min at blood flows of both 300 and 400 mL/min. The patient urea volume of distribution range modeled by the authors ranged from 25 to 45 L. Under ideal conditions, the authors demonstrate that with a blood flow of 300 mL per minute, a single pool Kt/V of greater than 1.2 could be achieved in patients with a urea volume of distribution of 35 L and 240 minutes of dialysis. Patients with a urea volume of distribution of 40 L would require 255 minutes of dialysis. Patients with a urea volume of distribution of 45 L would require over 270 minutes of dialysis. With a blood flow of 400 mL per minute, patients with a urea volume of distribution of 40 L could achieve the target single pool Kt/V of greater than 1.2 with 240 minutes of dialysis. Patients with a volume of distribution of 45 L could achieve the target with 270 minutes of dialysis. The authors did not model urea kinetics for patients with volumes of distribution greater than 45 L.[29]
Next, an article by Plumb, et al., described the Tablo® IDE study (discussed previously). Demographic information reflected the mean age as 52.3 ± 11.6 years, 19 men and the following racial and ethnic representation: 17 White, 13 Black or African American, 8 Hispanic or Latino, and 21 Not Hispanic or Latino. Comparisons among the 28 patients in this study and subsequent secondary analyses were either made between the 8 weeks of using the Tablo® System for in-center HD and the 8 weeks of the Tablo® System for in-home HD or between using the Tablo® System in-home HD and the treatment provided prior to study enrollment. In both settings, patients dialyzed using the Tablo® System 4 times per week. The primary efficacy endpoint was achievement of a weekly standard Kt/V greater than or equal to 2.1 in both the 8-week in-center phase of the study and the 8-week in-home phase of the study. This endpoint was achieved in 199 of 200 weeks in the in-center dialysis period and in 168 of 171 weeks in the in-home dialysis period. The primary safety endpoint of adverse event rates were similar at 1.9 percent in the in-center dialysis period and 1.8 percent in the in-home dialysis period. The secondary efficacy endpoint was whether the ultrafiltration volume and rate achieved the prescribed levels. In both in-center and in-home dialysis, 94 percent of treatments achieved successful delivery of ultrafiltration, defined as a rate within ten percent of the prescribed value. Of 960 in-center dialysis services and 896 in-home dialysis services, 922 and 884 were completed respectively, yielding adherence rates of 96 percent and 99 percent.[30]
Next, a separate article by Plumb et al., reports additional data from the Tablo® IDE study (previously discussed) regarding participants' assessment of the Tablo® System's ease-of-use, the degree of dependence on health care workers and caregivers after training with the system was complete, and the training time required for a participant to be competent in self-care. Demographic information reflected the mean age as 52.6 years, 18 men, 10 women, 16 White, 7 Hispanic or Latino, 9 Not Hispanic or Latino, and 12 Black or African American. Participants were stratified according to whether they were previously on self-care dialysis at home or conventional in-center HD. Thirteen participants had previous experience performing self-care HD. The remaining 15 participants had previous experience with in-center HD only. All participants rated the Tablo® System's setup, treatment, and takedown on a scale from 1 (very difficult) to 5 (very simple) and indicated whether they had required assistance with treatment over the prior 7 days. Set up times were similar regardless of whether the participants were previously on self-care HD or conventional in-center HD. For the participants previously on in-center HD, the average set up time for the concentrates was 0.93 minutes and for the cartridge, 9.35 minutes. For participants previously on self-care home HD, the average set up time for the concentrates was 1.22 minutes and for the cartridge, 10.28 minutes. The average rating of the Tablo® System's ease of use for setup was 4.5, treatment 4.6, and take down 4.6 among the participants previously on self-care home HD. In comparison, based on recollection (not based on rating during time of use) these participants' average rating of their previous device's ease of use for setup was 3.5, treatment 3.3, and take down 3.8. The average rating of the Tablo® System's ease of use for setup and treatment was 4.6 and 4.7 for take down among participants without prior self-care experience.
Among patients surveyed, caregiver assistance was required in 62 percent of patient-weeks during home self-care. Participants previously on self-care home HD required some caregiver assistance in 42 percent of the in-home dialysis treatment weeks. Participants previously on conventional in-center dialysis required some caregiver assistance in 35 percent of the in-home dialysis treatment weeks. The requirement for some form of assistance Start Printed Page 36337among participants with or without previous self-care experience was not meaningfully different. Finally, the authors noted that a protocol amendment allowed for the recording of the number of training sessions necessary to deem a patient competent to do self-care dialysis. This recording was limited to the last 15 participants enrolled into the study. Five of these participants had previous self-care dialysis at home experience. The average number of training sessions required to be deemed competent was 3.6 for participants with previous self-care dialysis at home experience and 3.9 sessions for participants with only conventional in-center HD experience.[31]
Next, a poster presentation from Chahal et al., reported patient device preference of prior in-home HD patients based on data from the Tablo® IDE study (previously discussed). The authors noted that 13 of the 30 participants in the Tablo® IDE trial were performing in-home HD at the time of enrollment and that prior to the study, dialysis prescriptions averaged 4.5 treatments per week with an average time of 3.1 hours per session. Trial prescriptions were for 4 days per week and an average of 3.4 hours per session. Adherence to the study regimen was 97 percent and 92 percent of surveys were completed. The authors concluded that participants with prior home HD experience preferred the Tablo® System compared to their prior device and 85.6 percent found that the Tablo® System was easier to use.[32]
As stated previously in this section of the proposed rule, the applicant submitted several sources pertaining to the incumbent, NxStage.® First, an article from Kraus et al., describes a feasibility study to demonstrate the safety of center-based versus home-based daily HD with the NxStage® portable HD device. This retrospective analysis examined the extent to which clinical effects previously associated with short-daily dialysis were also seen using the NxStage® device. The authors conducted a prospective, two-treatment, two-period, open-label, crossover study of in-center HD vs. home HD in 32 patients treated at six U.S. centers. Demographic information reflected the mean age as 51 years, 63 percent male, 38 percent female, 24 White, 6 Black or African American, 1 American Indian or Alaskan native, and 1 Asian. The 8-week In-Center Phase (6 days/week) was followed by a 2-week transition period and then followed by the 8-week Home Phase (6 days/week). Data was collected retrospectively on HD treatment parameters immediately preceding the study in a subset of patients. Twenty-six out of 32 patients (81 percent) successfully completed the study. Treatment compliance (defined as completing 43 to 48 treatments in a given phase) was comparable between the 2 treatment environments (88 percent In-Center vs. 89 percent Home). Successful delivery of at least 90 percent of prescribed fluid volume (primary endpoint) was achieved in 98.5 percent of treatments in-center and 97.3 percent at home. Total effluent volume as a percentage of prescribed volume was between 94 percent and 100 percent for all study weeks. The composite rate of intradialytic and interdialytic adverse events per 100 treatments was significantly higher for the In-Center Phase (5.30) compared with the Home Phase (2.10; p=0.007). Compared with the period immediately preceding the study, there were reductions in blood pressure, antihypertensive medications, and interdialytic weight gain. The study concluded that daily home HD with a small, easy-to-use HD device is a viable dialysis option for ESRD patients capable of self/partner administered dialysis.[33]
Second, an article from Finkelstein et al., reports on interim results of the Following Rehabilitation, Economics and Everyday-Dialysis Outcome Measurements (FREEDOM) study, a multi-center, prospective, cohort study of at-home short daily HD with a planned 12-month follow-up (ClinicalTrials.gov identifier, NCT00288613). Eligible patients were adults with ESRD requiring dialysis who were being initiated on short daily HD (prescribed 6 times per week) at home using the NxStage® cycler and who had Medicare as their primary insurance payer. The authors examined the long-term effect of short daily HD on health-related quality of life, as measured by the Short Form-36 (SF-36) health survey. The survey was administered at baseline, 4 and 12 months after initiation of short daily HD to 291 (total cohort) participants. Demographic information reflected the mean age as 53 years, 66 percent male and 70 percent White. Of the 291 participants, 154 completed the 12-month follow-up (as-treated cohort).
In the total cohort analysis, both the physical- and mental-component summary scores improved over the 12-month period, as did all 8 individual domains of the SF-36. The as-treated cohort analysis showed similar improvements with the exception of the role-emotional domain. Significantly, in the as-treated cohort, the percentage of patients achieving a physical component summary score at least equivalent to the general population more than doubled. The authors concluded by noting that at-home short daily HD is associated with long-term improvements in various physical and mental health-related quality of life measures.[34]
Third, in Weinhandl et al., authors described a cohort study in which 4,201 new home HD patients in 2007 were matched with 4,201 new PD patients in 2010 from the United States Renal Data System (USRDS) database to assess relative mortality, hospitalization, and technique failure. Demographic information reflected the mean age as 53.8 ± 14.9 years, 67 percent male, 33 percent female, 24.4 percent Black, and 75.6 percent Nonblack. Daily home HD patients initiated use of NxStage® from 2007 through 2010. Authors reported home HD was associated with 20 percent lower risk for all-cause mortality, 8 percent lower risk for all-cause hospitalization, and 37 percent lower risk for technique failure, all relative to PD. Regarding hospitalization, risk comparisons favored home HD for cardiovascular disease and dialysis access infection and PD for bloodstream infection. Authors noted that matching was unlikely to reduce confounding attributable to unmeasured factors, including residual kidney function; lack of data regarding dialysis frequency, duration, and dose in daily home HD patients and frequency and solution in PD patients; and diagnosis codes used to classify admissions. The authors concluded that these data suggest that relative to peritoneal dialysis, daily home HD is associated with decreased mortality, hospitalization, and technique failure but that risks for mortality and hospitalization were similar with these modalities in new dialysis patients.[35]
Start Printed Page 36338Fourth, in Suri et al., 1116, daily home HD patients were matched by propensity scores to 2784, contemporaneous USRDS patients receiving home peritoneal dialysis. The authors compared hospitalization rates from cardiovascular, infectious, access-related or bleeding causes, and modality failure risk. Similar analyses were performed for 1187, daily home HD patients matched to 3173, USRDS patients receiving in-center conventional HD. Demographic information identified the mean age as 50.5 years, 67.3 percent male, 70.9 percent White, 26.6 percent Black, and 2.5 percent Other, among the daily home HD patients. Among the home PD patients, the mean age was identified as 50.9 years, 66.9 percent male, 73.1 percent White, 25.1 percent Black and 1.2 percent Other. The composite hospitalization rate was significantly lower with daily home HD than with PD (0.93 vs. 1.35/patient-year). Daily home HD patients spent significantly fewer days in the hospital than PD patients (5.2 vs. 9.2 days/patient-year), and significantly more daily home HD patients remained admission-free (52 percent daily home dialysis vs. 32 percent peritoneal dialysis). In contrast, there was no significant difference in hospitalizations between daily home HD and conventional HD (0.93 vs. 1.10/patient-year). Cardiovascular hospitalizations were lower with daily home HD than with conventional HD (0.68) while infectious and access hospitalizations were higher (1.15) and 1.25 respectively). Significantly more PD than daily home HD patients switched back to in-center HD (44 percent vs. 15 percent). In this prevalent cohort, daily home HD was associated with fewer admissions and hospital days than PD, and a substantially lower risk of modality failure.[36]
(b) Applicant SCI Claims
Regarding the applicant's first claim that the Tablo® System decreases treatment frequency with adequate dialysis clearance, the applicant stated that the Tablo® System is the only mobile HD device approved for use in the home that can achieve adequate dialysis in as little as 3 treatments per week, while also providing flexibility for more frequent dialysis and thus greater personalization of care. The applicant stated that adequate dialysis for a standard, thrice weekly treatment schedule is a single treatment clearance of urea, expressed as a single-pool Kt/V (spKt/V) of greater than 1.2 where “K” = dialyzer clearance, “t” = time, and “V” = Volume of distribution of urea. The applicant also stated that dialyzer clearance, or “K”, is dependent on the mass transfer coefficient (KoA) characteristics of the prescribed dialyzer and prescribed blood and dialysate flow rates. The applicant further noted that limitations in “K” or “t” affect the ability of a patient to achieve adequate clearance during a dialysis treatment. Per the applicant, across a broad range of weights, patients using the Tablo® System can achieve the target of dialysis adequacy, a single pool Kt/V of 1.2, with 3 treatments per week in less than 4 hours.[37] The applicant also stated that when used 4 times per week, patients using the Tablo® System had a higher mean weekly standard Kt/V with equivalent or better dialysis-related hospitalization rates,[38] as compared to NxStage® IDE patients prescribed therapy at 6 days per week.[39]
The applicant stated that the Tablo® System's on-demand dialysate production has no limitation to the volume of dialysate that can be produced and used during a single treatment. The applicant further stated that this facilitates the delivery of adequate dialysis clearance (Kt/V) in a standard duration and target frequency of 3 times per week, as well as alternate frequencies and durations as preferred by a patient or recommended by a health care provider.
The applicant asserted that NxStage,® when attached to its Pureflow device, requires users to batch a set amount of dialysate (maximum of 60 liters) in advance of a treatment or use sterile dialysate bags (maximum of 30 liters). The applicant also stated that at its maximum dialysate flow rate (Qd) of 300ml/min, NxStage® greatly limits time by restricting treatment to a maximum of 200 minutes before exhausting its dialysate capacity (200 min = 60L/300ml/min).
The applicant stated that Dialysis Outcomes and Practice Patterns Study (DOPPS) data demonstrate that the current U.S. practice for thrice weekly dialysis occurs at an average treatment time of greater than 220 minutes, and has increased in the last 25 years.[40] Per the applicant, with the limited “t”, a single-pooled Kt/V of >1.2 cannot be expected to be achieved for the majority of U.S. patients with ESRD on a thrice weekly schedule, requiring increased treatment frequency [41] at home for these patients to meet the desired clearance level.
In citing Leypoldt et al., the applicant stated that data from the Hemodialysis (HEMO) trial combined with modeling results from Leypoldt et al.,[42] allow for an estimation of the patients with ESRD, based on weight, that cannot be expected to achieve target clearance with standard thrice weekly dialysis at this treatment duration. The applicant explained that because urea is evenly distributed throughout a body's water, the volume of distribution of urea is equal to a patient's total volume of water. The applicant also stated that total body water and volume of distribution of urea can be expressed as a volume or as a percentage of total weight and can vary based on numerous factors including disease state. The applicant stated that it is possible to estimate the percent of water for the ESRD population from the HEMO trial as summarized in Leypoldt et al.[43] The applicant stated that in the trial, the mean patient weight was 69.8kg and the mean patient volume of body water (V) was 30.9L. The applicant further explained that from this, total body water (and volume of distribution of urea) are calculated as 44.3 percent of the mean weight of patients with ESRD (44.3 = 30.9L/69.8kg × 100). Per the applicant, applying this 44.3 percent of total body weight to the volumes of distribution in Leypoldt et al.[44] allows the conversion of the kinetic model described into anticipated patient weights. The applicant further stated Start Printed Page 36339that in calculating with standard blood flow and a higher dialyzer mass transfer area coefficient for urea (KoA) diayzer, a 200 minute treatment at a dialysate flow rate (Qd) of 300ml/min would not achieve what the applicant refers to as the CMS target spKt/V target 1.2 for patients with a volume of distribution of urea (V) of 35L or greater. The applicant stated that these assumptions were drawn from NxStage® technical specifications.[45 46] The applicant stated that at 44.3 percent of total weight, this volume of distribution of urea correlates to patients with ESRD with a mean weight above 79 kg (79 = 35L/.443) or approximately 174 pounds. Per the applicant, patients at or above this weight cannot be expected to achieve a spKt/V urea of 1.2 on a thrice weekly schedule using the NxStage® system at its maximal dialysate flow rate.
The applicant stated that for the majority of the U.S. prevalent ESRD population between the ages of 22-74, whose mean weight is between 84.3-89.1 kg by age group,[47] thrice weekly therapy at home on NxStage® would not achieve the Medicare coverage standard. Specifically, per the applicant, Medicare's national coverage policy is to reimburse for dialysis care 3 times per week, regardless of the modality that is used and health care providers are expected to ensure that patients receive adequate clearance with the 3 times per week cadence. The applicant also stated that Medicare Administrative Contractors (MACs) have discretion in reimbursing additional treatments with medical justification.[48] Per the applicant, an analysis of Medicare claims data from 2018 finds that despite the limitations of the reimbursement policy, Medicare is paying for 5 or more treatments per week in 50 percent of home HD patients nationwide, amounting to an estimated annual cost to Medicare of $122 to $126 million.[49] However, based on CMS review of dialysis facility claims data, among all beneficiaries who had home dialysis treatments in 2018, 39.1 percent had 5 or more dialysis sessions at least once during any week. The overall percentage of beneficiary-weeks that had 5 or more home HD sessions in 2018 was 20.9 percent. Medicare payment for these additional sessions totaled $17 million. We note that, as indicated in Local Coverage Determination ID L35014, “Frequency of Dialysis” (revised effective September 26, 2019),[50] CMS established payment for HD based on conventional treatment which is defined as 3 times per week. Sessions in excess of 3 times per week must be both reasonable and necessary in order to receive payment. Covered indications include metabolic conditions (acidosis, hyperkalemia, hyperphosphatemia), fluid positive status not controlled with routine dialysis, pregnancy, heart failure, pericarditis, and incomplete dialysis secondary to hypotension or access issues. The applicant asserted that the use of the Tablo® System would decrease the number of necessary dialysis treatments, without affecting patient outcomes such as clearance or hospitalizations.
The applicant stated that there is clinical evidence and expert consensus that as treatment frequency increases, native residual kidney function drops, patient and care partner burden increases, and vascular access complications increase.[51 52] Per the applicant, home use of the Tablo® System can reduce the need for a fifth or sixth weekly treatment without increasing patients' symptom burden.[53] The applicant stated that by achieving adequacy targets with fewer treatments, Tablo® System patients can be expected to have fewer vascular access interventions and health care providers will have increased flexibility in personalizing the frequency and duration of patient treatments.[54 55] The applicant stated that reducing treatment frequency while maintaining adequate patient clearance levels may also reduce complications that lead to hospitalizations. The applicant stated that during the Tablo® IDE study, patients using the Tablo® System 4 times per week, for an average duration of less than 4 hours per treatment, had an all-cause hospital admission rate of 426 per 1,000 patient-years whereas in the general dialysis population, the all-cause admission rate is 1,688 per 1,000 patient-years, and for patients who utilize peritoneal dialysis, the hospitalization rate is 1,460 per 1,000 patient years.[56]
The applicant stated that while NxStage® has not specifically reported the hospitalization rates per patient-year from its IDE study, published data from Weinhandl et al.,[57] and Suri et al.,[58] report hospital admission rates amongst patients on daily home HD ranging from 930 to 1,663 per 1,000 patient-years, using a national sample of dialysis patients matched for comparison to similar peritoneal and in-center dialysis patients. We clarify that this would represent 930 to 1,663 cases observed Start Printed Page 36340among 1,000 persons during 1 year. The applicant also noted that all data on home patients in Weinhandl et al. came from a matched cohort of NxStage® patients. Per the applicant, in Suri et al., data were collected prior to 2015 and that during this timeframe, it can be reasonably assumed that home HD patients were using NxStage® for treatment. The applicant stated that the results from these studies suggest that patients receiving treatment at home with NxStage® 5 to 6 times per week do not have a lower all-cause hospitalization rate, relative to matched in-center HD patients. The applicant concluded by stating that because of the clinical and demographic diversity of the Tablo® System's patient population, the applicant's results show incremental improvement over the hospitalization rate of the current home HD population.
Regarding the applicant's second claim that the Tablo® System increases adherence to dialysis treatment and retention to home therapy, the applicant stated that patients using the Tablo® System have improved adherence to prescribed treatments and a higher rate of retention to home therapy. The applicant further stated that this increased adherence and retention is likely to improve patient outcomes by reducing the rate of dialysis-related hospitalizations and other adverse events associated with missing treatment in this patient population.[59]
The applicant stated that adherence to prescribed dialysis treatments is crucial for dialysis patients because missed treatments increases the risk of dialysis dropout, hospitalization, and death.[60] Per the applicant, the Tablo® IDE study demonstrated a 99 percent treatment adherence rate to all prescribed home treatments [61] among both prior in-center participants and prior self-care home HD participants who used NxStage®. The applicant also stated that the Tablo® System's adherence rates were similar among both the prior in-center and prior self-care participants. The applicant stated that these results represent a significant improvement over the treatment adherence rate reported in the NxStage® IDE, where the treatment compliance rate was defined less stringently as missing 5 or fewer treatments of the 48 possible treatments and was only 89 percent among patients at home and during the study period.[62] Per the applicant, using a comparable metric of missing 5 or fewer of all possible treatments at home, Tablo® IDE patients at home had a 100 percent treatment compliance rate.
The applicant stated that technique failure in home HD, defined as reduced retention at home and a return to in-center care, has been high with NxStage®. Per the applicant, real world data show that technique failure occurs in 36 percent of home HD patients using NxStage® within 1 year of initiating treatment.[63] The applicant stated that this is challenging for the patient and taxing on the healthcare system that has invested in providing patients with home dialysis training and in paying for more frequent therapy.
The applicant stated that by directly comparing the Tablo® System's retention to that of NxStage®, the applicant assessed rates in the analogous IDE populations while excluding those who exited either study for reasons unrelated to the device such as receipt of a transplant or death. The applicant stated that the Tablo® System demonstrated a 97 percent (28 of 29) patient retention rate for the entire IDE study and a 100 percent retention rate in the in-home phase of the trial among both prior NxStage® users and prior in-center patients.[64] The applicant stated that in comparison, 81 percent of participants completed the NxStage® IDE study.[65]
The applicant stated that the Tablo® System's ease of use contributed to the improved adherence and retention rates and that the Tablo® System is designed to enable patients to become proficient and independent in using the Tablo® System after an average of 3.9 days.[66] Per the applicant, published NxStage® IDE data [67] reported an average of 14.5 days “to complete device training on NxStage®.” The applicant stated that, in comparison, device-related training time is reduced by at least 50 percent on the Tablo® System. Per the applicant, the reduced training time and ease of use will likely improve retention and potentially reduce the number of reimbursable training sessions. The applicant stated that because of the significant role that caregivers play in supporting home dialysis treatments,[68] care partner burnout and a patient's perception of being a burden is associated with discontinuation of home therapy.[69 70] Per the applicant, the 28 patients who entered the home phase of the Tablo® IDE study were asked weekly if they needed help with their dialysis treatments during the prior 7 days. The applicant stated that a 96 percent response rate (216 of 224 possible) was achieved at the end of the study and that for both prior-in-center and NxStage® study participants, in 79 percent of the treatment weeks, patients reported needing no assistance from their care partner in performing dialysis set-up, treatment, or breakdown. The applicant explained that among the 13 prior in-home patients, all of whom were formerly NxStage® users, participants reported needing help from a trained individual with dialysis treatment in 69 percent of treatment weeks, with 46 percent of instances involving a need for device-related help. We clarify that per Plumb, et al.,[71] this Start Printed Page 36341is the baseline percentage and reflects 9 of the 13 patients with previous self-care experience. The applicant stated that patients reported needing help with treatment in only 42 percent of treatment weeks while using the Tablo® System, which is a 39 percent reduction from baseline NxStage® use; and only 18 percent of these instances related to use of the Tablo® System, which is a 61 percent reduction in rate from baseline NxStage® use.[72]
The applicant stated that it collected weekly data from patients by asking them to rate the extent to which they believed that they were a burden on a scale of 1 to 5, with 1 representing never and 5 representing always. The applicant stated that this measure was adapted from an instrument used in assessing terminally ill patients.[73] The applicant stated that the subpopulation of study participants who had previously used NxStage® reported an average score of 3.1 for self-perceived burden on their care partner when using their prior device, which subsequently reduced to 2.4 when using the Tablo® System (a 23 percent reduction in score from baseline NxStage® use).[74] Per the applicant, these data underscore that a significant increase in patients' confidence, ability to achieve treatment independence at home, and subsequent reduction in the sense of self burden can positively contribute to success in the home setting. The applicant further noted that the ease of use, reduced training time, and substantial reduction in care partner assistance required for the Tablo® System correlated to the improved retention and adherence rates in the Tablo® IDE study. The applicant stated that on a population level, this likely translates to reduced barriers to continuing home HD once initiated, and ultimately, a reduced risk of adverse outcomes due to missed treatments. The applicant also stated that the Tablo® System's electronic data capture and automatic wireless transmission eliminates the need for manual record keeping, which represents an improvement with respect to burden and monitoring as compared to NxStage®.
Regarding the applicant's third claim that the Tablo® System improves patient quality of life, the applicant stated that patients on the Tablo® System experience reduced disease burden, dialysis related symptoms, and an improved quality of life at home as compared to in-center and existing home care options. Per the applicant, patients with ESRD experience significant dialysis-related symptoms including difficulty sleeping, dizziness, and pain associated with recovery time that affect mental and physical health and lead to decreased overall quality of life.[75] Per the applicant, the Tablo® IDE study assessed several validated Patient-Reported Outcome Measures (PROMs) to better understand overall health-related quality of life (HR-QoL). The applicant explained that the overall measure was the EQ-5D-5L, a validated, preference-based PROM in which patients self-assess mobility, self-care, usual activities, pain/discomfort, and anxiety/depression.[76] The applicant stated that from these domains, an index value is calculated to report a summary score that ranges from 0 (death) to 1 (full health).
Per the applicant, while the NxStage® IDE study did not report results for a quality-of-life instrument, HR-QoL was assessed in NxStage® patients in a prospective multicenter observational study referred to as the FREEDOM trial, which examined the effects of at-home dialysis 6 times per week with the NxStage® System on costs and HR-QoL using the SF-36 instrument. The applicant further stated that the reported results at 4-month follow-up among these patients [77] translates to a mean EQ-5D score of 0.70. The applicant included an appendix describing the Methodology to Derive EQ-5D Scores from the FREEDOM Study Results in its application and derived a predicted mean EQ-5D score of 0.695-0.70 at follow up for the FREEDOM study. The applicant further noted that because this estimate is based on the average aggregate change for an adjusted measure that was then translated to the EQ-5D scale, and the applicant did not have access to standard error estimates for the Mental Component Score (MCS) and Physical Component Score (PCS), its interpretation of this estimate and its variance is limited. Per the applicant, nonetheless, it provides a sense of the comparable HR-QoL of this sample of NxStage® patients at follow-up. The applicant further noted that mean EQ-5D index values for traditional HD and PD patients reported from a meta-analysis of existing studies in the literature are 0.56 (95 percent CI: 0.49-0.62) and 0.58 (95 percent CI: 0.5-0.67), respectively.[78]
Per the applicant, patients in the Tablo® IDE study reported mean EQ-5D index values of 0.821 (SD: ±0.163) [79] in the home phase of the study with final measures taken at approximately 5 months from trial start. The applicant stated that this is a significant improvement when using traditional HD patients as a comparator, and higher overall HR-QoL as compared to NxStage® patients. The applicant emphasized that participants in the Tablo® IDE trial underwent a reduced treatment frequency as compared to participants in the FREEDOM study who were prescribed 6 treatments per week on NxStage®. The applicant stated that among patients in the Tablo® IDE study who had previously been using NxStage®, the mean EQ-5D score during the in-home phase of the study was 0.906 (SD: ±0.119) and asserted that this is significantly greater than index population values for HD and peritoneal dialysis.
The applicant stated that sleep problems are present in 60 percent of patients with chronic kidney disease (CKD) and ESRD [80] and that patients rank fatigue and lack of energy as the most important contributor to their decreased quality of life.[81] Per the Start Printed Page 36342applicant, the frequency of sleep-related symptoms among the Tablo® System's patients was assessed by a survey that was administered weekly during the Tablo® IDE study. The applicant stated that, in the absence of a well-validated sleep survey specific to the ESRD population, study investigators selected survey questions from previously validated sleep questionnaires in the non-ESRD population, based on their relevance to the study population.[82 83] The applicant explained that questions were designed to focus on quality of sleep and restfulness and noted that these measures are validated for use among chronically ill populations and measure the frequency of 4 key sleep-related symptoms. The applicant stated that, while at home, patients on the Tablo® System reported improved quality of sleep, with a measurable reduction in rate of patient-reported sleep symptoms ranging from a 10-60 percent reduction, depending on symptom.[84] The applicant stated that this reduction was observed among study participants who were previously receiving dialysis in-center (average magnitude of reduction in rate across symptoms: 42 percent) and among study participants who were previously receiving in-home dialysis on NxStage® (average magnitude of reduction in rate across symptoms: 27 percent). Per the applicant, on average, sleep-related difficulties reduced from being reported in 33 percent of treatment weeks while on NxStage® to 23 percent of treatment weeks while on the Tablo® System.
The applicant stated that hypotensive symptoms such as feelings of dizziness and lightheadedness are associated with the drops in blood pressure that can occur during dialysis and are also among the top ten symptoms dialysis patients report that impact their quality of life.[85] Per the applicant, participants in the Tablo® IDE study were asked at the time of enrollment regarding symptoms previously experienced during dialysis. The applicant also stated that at the end of each study treatment, participants were surveyed regarding the presence of any symptoms during that treatment on the Tablo® System. Per the applicant, a total of 8 (26.7 percent) subjects reported hypotensive symptoms during the Tablo® System treatments during the in-home treatment period, compared to 27 (90 percent) subjects reporting hypotensive symptoms at baseline (prior to initiating care on the Tablo® System). The applicant reported a 70 percent reduction in the rate of patient-reported hypotensive symptoms while on the Tablo® System, though we were unable to validate the source of this statement.
The applicant stated that currently, ESRD patients on dialysis report meaningfully lower quality of life compared to those with other chronic illnesses.[86] The applicant further noted that decreased quality of life is associated with a meaningful decline in continuation of home therapy, dialysis frequency, and worse clinical and health care utilization outcomes.[87]
The applicant concluded by asserting that the totality of evidence submitted in support of the Tablo® System demonstrates SCI over the current standard of home dialysis care. The applicant also stated that patient preference for devices is currently used by FDA to guide marketing authorization decisions and provides important information on the benefit and risks that some patients are willing to trade when choosing a device.[88] Per the applicant, patients may be more likely to choose home dialysis to the extent that the device is both accessible and easy to use. The applicant also stated that 86 percent of prior NxStage® patients in the Tablo® IDE study found the Tablo® System easier to use than their incumbent device and preferred to remain on the Tablo® System at the end of the study.[89]
In summary, the applicant claimed that the Tablo® System improves the treatment of Medicare beneficiaries relative to the incumbent by focusing on outcomes set forth in § 412.87(b)(1)(ii)(C), including a decreased number of treatments to achieve dialysis adequacy, which the applicant stated leads to greater adherence to prescribed therapy, and improved quality of life.
(c) CMS Preliminary Assessment of SCI Claims and Sources
After a review of the information provided by the applicant, we have identified the following concerns regarding the SCI eligibility criterion for the TPNIES. We note that, consistent with § 413.236(c), CMS will announce its final determination regarding whether Tablo® meets the SCI criterion and other eligibility criteria for the TPNIES in the CY 2022 ESRD PPS final rule.
With respect to the applicant's claim that patients can achieve dialysis adequacy in as little as 3 treatments per week, we note that the Tablo® IDE study did not test whether patients receive adequate dialysis on a thrice-weekly schedule. Instead, data published from the Tablo® IDE study address a weekly measure of dialysis adequacy among patients treated on a 4 times per week schedule. The applicant relied on modeling and unpublished data on patients receiving thrice-weekly dialysis in making the conclusion that dialysis adequacy can be reached on a thrice-weekly schedule. Specifically, the applicant referred to a theoretical modeling study based on historical data from the USRDS, Medicare claims, and historical outcomes from NxStage® observational studies. The applicant also stated that findings from a retrospective review of 29 patients receiving treatment with the Tablo® System on a thrice-weekly schedule affirm the results from the modeling study. We also note that the authors in Alvarez et al.[90] stated that conclusions about fluid removal could not be made from their study. We would be interested in whether additional studies are available that address issues related to effective fluid removal using home Start Printed Page 36343self-care dialysis thrice-weekly with the Tablo® System. We invite comments on whether less frequent dialysis sessions would represent SCI over shorter, more frequent sessions that, according to the applicant, are common among users of the incumbent technology.
The applicant's second claim was that the Tablo® System increases adherence to dialysis treatment and retention to home therapy, which may reduce dialysis-related hospitalizations and other adverse events associated with missing treatment. This claim was supported by the Tablo® IDE study (28 participants completed the study) and the use of historical comparisons to prior studies involving the NxStage® System. The applicant noted that hospitalization rates from the Tablo® IDE trial were lower than rates in the general dialysis population and rates reported in two observational studies of patients using the NxStage® device. While the applicant cited an all-cause hospitalization rate of 426 per 1000 patient years in the Tablo® IDE study, it does not appear that the sources [91 92] published these hospitalization rates. We further note that the applicant relied on historical comparisons in asserting that that patients treated with the Tablo® System experience reduced disease burden and improved quality of life.
We note that in the Tablo® IDE study, the before-after comparisons in patients with NxStage® regarding improved sleep compared to prior to the Tablo® System may be prone to recall bias in that participants' experiences with NxStage® were not recorded at the time they were receiving NxStage® treatments, but rather, were based on recall at the time of the Tablo® IDE study.
We understand that greater flexibility for patients in the way that they receive their dialysis treatments may represent a benefit to Medicare beneficiaries who are candidates to receive this treatment in the home setting. We invite comments on whether this potential benefit represents SCI, including whether the Tablo® System represents an advance that substantially improves, relative to renal dialysis services previously available, the treatment of Medicare beneficiaries.
(6) Capital Related Assets Criterion (§ 413.236(b)(6))
With respect to the sixth TPNIES eligibility criterion under § 413.236(b)(6), whether the item is a capital-related asset and home dialysis machine, § 413.236(a)(2) defines these terms. First, a capital-related asset is an asset that an ESRD facility has an economic interest in through ownership (regardless of the manner in which it was acquired) and is subject to depreciation. Equipment obtained by the ESRD facility through operating leases are not considered capital-related assets. Second, home dialysis machines are HD machines and PD cyclers in their entirety (meaning that one new part of a machine does not make the entire capital-related asset new) that receive FDA marketing authorization for home use and when used in the home for a single patient. The applicant identified the Tablo® System as an asset that an ESRD facility has an economic interest in through ownership, is subject to depreciation, and is an HD machine that received FDA marketing authorization for home use. Therefore, the Tablo® System is a capital-related asset that is a home dialysis machine. We welcome comments on the Tablo® System's status as a capital related asset that is a home dialysis machine.
b. CloudCath Peritoneal Dialysis Drain Set Monitoring System (CloudCath System)
CloudCath submitted an application for the TPNIES for the CloudCath Peritoneal Dialysis Drain Set Monitoring System (CloudCath System) for CY 2022. According to the application, the CloudCath System is a tabletop passive drainage system that detects and monitors solid particles in dialysate effluent during PD treatments. Solid particles in dialysate effluent, manifesting itself as cloudy dialysate, may indicate that the patient has peritonitis, the inflammation of the peritoneum in the abdominal wall usually due to a bacterial or fungal infection.[93] PD therapy is a common cause of peritonitis.[94] If left untreated, the condition can be life threatening.[95]
PD-related peritonitis is a major complication and challenge to the long-term success and adherence of patients on PD therapy.[96] The applicant stated that only about 12 percent of eligible patients are on PD therapy.[97] The applicant claimed that the risk of PD-related peritonitis, and the challenges to detect it, are the main reasons for these figures. The guidelines for diagnosis of PD-related peritonitis, as outlined by the International Society for Peritoneal Dialysis (ISPD), recommend that peritonitis be diagnosed when at least 2 of the following criteria are present: (1) The patient experiences clinical features consistent with peritonitis (abdominal pain and/or cloudy dialysate effluent); (2) the patient's dialysate effluent has a whole blood count (WBC) >100 cells/μL or >0.1 × 10/L with polymorphonuclear (PMN) cells >50 percent; and (3) positive dialysis effluent culture is identified.[98] Additionally, the guidelines recommend that PD patients presenting with cloudy effluent be presumed to have peritonitis and treated as such until the diagnosis can be confirmed or excluded.[99] Per the guidelines, this means that for patients undergoing PD treatments at home, it is recommended that they self-monitor for symptoms of peritonitis, cloudy dialysate and/or abdominal pain, and seek medical attention for additional testing and treatment upon experiencing any or both of these symptoms. According to the applicant, despite the fact that peritonitis is highly prevalent, symptom monitoring is insensitive and non-specific, which can contribute to late presentation for medical attention and treatment. The applicant asserted that under the current standard of care, PD patients face the following challenges in detecting peritonitis. First, the applicant stated that patients' fluid observation has low compliance rates as it relies on patients' close examination of their own dialysate effluent during PD treatments, which often occur while patients are asleep. Second, the applicant noted that it can be difficult for patients to visually detect peritonitis in dialysate effluent using a “newspaper test” for cloudiness, and can be even more difficult to see when the fluid is drained into a toilet, where it is diluted by water. The applicant stated that, as a result of these challenges, patients with ESRD suffer unsatisfactorily high mortality and morbidity from Start Printed Page 36344peritonitis, as well as high rates of PD modality loss, meaning they must discontinue PD and begin a different type of dialysis treatment. Per the applicant, the CloudCath System addresses these challenges by detecting changes in dialysate effluent at much lower levels of particle concentrations than the amount needed to accumulate for visual detection by patients.
Per the applicant, the CloudCath System consists of three components: (1) Drain set, (2) sensor, and (3) patient monitoring software. As explained in the application, the CloudCath System's drain set connects to a compatible PD cycler's drain line to enable draining and monitoring of dialysate effluent before routing the fluid to the drainage receptacle. Per the CloudCath System User Guide, included in the application, the CloudCath System is compatible with the following PD cyclers: Baxter Healthcare Home Choice PROTM, Baxter Healthcare AMIATM Automated PD System, and Fresenius Liberty® Select Cycler. Per the applicant, once the CloudCath System is attached to a compatible cycler, the dialysate effluent runs through the drain set, through the CloudCath System's optical sensor. The applicant explained that the CloudCath System's optical sensor detects and monitors changing concentrations of solid particles in the dialysate effluent during each dialysis cycle and reports the concentrations in a turbidity score. Per the applicant, the CloudCath System will indicate whether dialysate effluent has normal turbidity and will notify the patient and/or health care professional if the dialysate effluent turbidity has exceeded the notification threshold set by the patient's dialysis provider. The applicant stated that the optical sensor's hardware and software components allow for data trending over time and remote monitoring by a healthcare professional.
(1) Renal Dialysis Service Criterion (§ 413.236(b)(1))
Regarding the first TPNIES eligibility criterion in § 413.236(b)(1), that the item has been designated by CMS as a renal dialysis service under § 413.171, monitoring for peritonitis is a service that is essential for dialysis, and therefore would be considered a renal dialysis service under § 413.171.
(2) Newness Criterion (§ 413.236(b)(2))
With respect to the second TPNIES eligibility criterion in § 413.236(b)(2), that the item is new, meaning within 3 years beginning on the date of the FDA marketing authorization, the applicant stated that it is seeking 510(k) marketing authorization from the FDA. To be eligible for the TPNIES, the applicant must apply within three years of the FDA marketing authorization date and receive FDA marketing authorization by the HCPCS Level II deadline of July 6, 2021. The applicant stated that it anticipates the CloudCath System will receive FDA marketing authorization by the HCPCS Level II deadline.
(3) Commercial Availability Criterion (§ 413.236(b)(3))
Regarding the third TPNIES eligibility criterion in § 413.236(b)(3), that the item is commercially available by January 1 of the particular calendar year, meaning the year in which the payment adjustment would take effect, the applicant stated that the CloudCath System is not currently commercially available because it has not received FDA marketing authorization. The applicant noted that it expects the CloudCath System will be commercially available immediately after receiving FDA marketing authorization.
(4) HCPCS Level II Application Criterion (§ 413.236(b)(4))
Regarding the fourth TPNIES eligibility criterion in § 413.236(b)(4) requiring that the applicant submit a complete HCPCS Level II code application by the HCPCS Level II application deadline of July 6, 2021, the applicant stated that it has not submitted an application yet, but intends to apply by the deadline.
(5) Innovation Criteria (§§ 413.236(b)(5) and 412.87(b)(1))
(a) SCI Claims and Sources
With regard to the fifth TPNIES eligibility criterion under § 413.236(b)(5), that the item is innovative, meaning it meets the SCI criteria specified in § 412.87(b)(1), the applicant asserted that the CloudCath System offers SCI over technologies currently available for the Medicare patient population by offering the ability to monitor changes in turbidity of peritoneal dialysate effluent through continuous remote monitoring in patients with ESRD receiving PD therapy, earlier than the current standard of care. By allowing the clinical standard of care to be initiated earlier, per the applicant, the use of the CloudCath System changes the management of peritonitis patients by enabling clinicians to both diagnose peritonitis and initiate antibiotic treatment earlier.
The applicant submitted two studies on the technology in support of the SCI claims. The applicant included a preliminary, unpublished report by Briggs, et al. on a clinical study that tested the ability of the CloudCath System and its dialysate effluent monitoring algorithm to detect indicators of peritonitis.[100] The proof of principle observational study consisted of 70 PD patients outside of the U.S. who had been on PD for a long interval of time (>10 days), and thus were at an increased risk of developing peritonitis. Out of the 64 PD patients whose data were included in the study, over 40 PD patients were receiving intermittent PD, which is not commonly used in the U.S. The remainder of the participants were receiving Continuous Ambulatory Peritoneal Dialysis. The report states that in the U.S., PD is generally performed in a modality called Continuous Cycling Peritoneal Dialysis (CCPD), in which a cycler automatically administers multiple dialysis exchange cycles, typically while patients sleep. Samples were collected from patients' PD effluent drainage bags and measured in the CloudCath System against a proprietary Turbidity Score threshold value and also tested for reference laboratory measurements according to ISPD guidelines for WBC count and differential (>100 cells/μL, >50 percent PMN).[101] Regarding the Turbidity Score threshold value, the study set a score to determine if the effluent sample in the CloudCath System was infected or not; samples greater than or equal to the Turbidity Score threshold value would be classified as infected, and samples less than the Turbidity Score threshold value would be classified as non-infected. The crude sensitivity and specificity of the CloudCath System was 96.2 percent and 91.2 percent, respectively. A majority of false positives (44 of 77 samples) occurred among patients already receiving antibiotic treatment for peritonitis, and another 20 false positive reports occurred because the patient had elevated turbidity due to a cause other than peritonitis. The investigators subsequently removed samples from patients already receiving treatment for peritonitis, setting the sensitivity for detecting peritonitis using the CloudCath System at 99 percent and the specificity at 97.6 percent.
The second study the applicant submitted is the Prospective Clinical Study to Evaluate the Ability of the CloudCath System to Detect Peritonitis Start Printed Page 36345Compared to Standard of Care during In-Home Peritoneal Dialysis (CATCH).[102] CloudCath initiated this ongoing single-arm, open-label, multi-center study to demonstrate that the CloudCath System is able to detect changes in turbidity associated with peritonitis in PD patients prior to laboratory diagnosis of peritonitis with a high degree of specificity and sensitivity. The target enrollment is 186 participants over 18 years of age using CCPD as their PD modality, with at least 2 exchanges per night.[103] Patients with active infection and/or cancer are excluded from the trial.[104] The primary endpoint is time of peritonitis detection by the CloudCath System (defined as two consecutive Turbidity Scores >7.0) as compared to laboratory evidence of peritonitis (defined as WBC count >100 cells/μL or >0.1 × 109/L with percentage of PMN >50 percent).[105] While the study is ongoing, the applicant included the study protocol and preliminary results with its application.[106] The preliminary results demonstrate that as of December 29, 2020, 132 participants have been enrolled in the CATCH Study at 13 sites.[107] Of the 132 enrolled participants, 59.1 percent of participants were male, 65.9 percent of participants were White and 29.6 percent of participants were Black or African American.[108] Enrolled participants underwent an average of 4.5 exchanges per night.[109] The preliminary results indicate that, as of December 29, 2020, there have been 7 peritonitis events that met the ISPD peritoneal fluid cell counts and differentials standard.[110] All 7 of the peritonitis events were also detected by the CloudCath System.[111] In 5 out of the 7 peritonitis events, the CloudCath System detected peritonitis 44 to 368 hours prior to the time of detection from a clinical laboratory.[112] The CloudCath System also detected peritonitis 27 to 344 hours prior to participants presenting to the hospital or clinic with signs or symptoms of peritonitis.[113] The applicant stated that these results support the claim that the CloudCath System would enable diagnosis of peritonitis earlier than the current standard of care through turbidity monitoring.
In addition to the studies on the technology, the applicant submitted an article by Muthucumarana, et al. on the impact of time-to-treatment on clinical outcomes of PD-related peritonitis.[114] The article includes data from the Presentation and the Time of Initial Administration of Antibiotics With Outcomes of Peritonitis (PROMPT) Study, a prospective multicenter from 2012 to 2014 that observed symptom-to-contact time, contact-to-treatment time, defined as the time from health care presentation to initial antibiotic, and symptom-to-treatment time in Australian PD patients. 116 patients participated in the survey, 83 of which were caucasian and 14 were aboriginal.[115] Out of the sample size of 116 survey participants, there were 159 episodes of PD-related peritonitis. Of these, 38 patient episodes met the primary outcome of PD failure (defined as catheter removal or death) at 30 days.[116] The median symptom-to-treatment time was 9.0 hours in all patients, 13.6 hours in the PD-fail group, and 8.0 hours in the PD-cure group.[117] The study found that the risk of PD-failure increased by 5.5 percent for each hour of delay of administration of antibiotics once patients presented to a health care provider.[118] However, neither symptom-to-contact nor symptom-to-treatment was associated with PD-failure in non-adjusted analyses, and the time from presentation to a health care provider to treatment was only associated with PD-failure outcomes in multivariable-adjusted analyses in a subset of patients who presented to hospital-based facilities. In addition to the Muthucumarana et al. article, the applicant cited to other studies that have found that antibiotic treatment should begin as soon as possible in order to effectively treat infections other than peritonitis.[119 120 121] Per the applicant, these articles on time-to-treatment demonstrate that the CloudCath System's ability to detect effluent changes substantially earlier improves the standard of care, enabling PD-related peritonitis diagnosis and antibiotic treatment earlier while decreasing the likelihood of PD-failure due to PD-related peritonitis.
The applicant also submitted letters of support from a nephrologist at an academic institution and the following ESRD patient advocacy groups: The American Kidney Fund, the American Association of Kidney Patients, and the International Society of Nephrology. The letter of support from Dr. Thomas A. Golper, president-elect of the International Society of Nephrology, endorsed the CloudCath System's ability to detect peritonitis and enable clinicians to begin to treat the infection earlier, preventing hospitalizations and related complications such as the abandonment of home dialysis. The letter also stated that the CloudCath System helps address the challenge of peritonitis as the main reason for abandonment of PD for HD, and will encourage a greater number of patients to select PD as their dialysis modality of choice. The letters from the American Association of Kidney Patients and the International Society of Nephrology encouraged CMS to consider the CloudCath System's application, explaining that the technology would have several benefits to patients, for example, by reducing peritonitis-related hospitalizations, increasing adherence to PD, and encouraging higher utilization of PD as a viable alternative to in-center HD. The American Kidney Fund's letter emphasized that peritonitis is a significant concern for PD patients [122] and requested CMS support of all efforts that ensure patients Start Printed Page 36346with ESRD undergoing PD treatments can quickly detect and treat infections.
(b) CMS Preliminary Assessment of SCI Claims and Sources
After a review of the information provided by the applicant, we note the following concerns with regard to the SCI criterion under § 413.236(b)(5) and § 412.87(b)(1). We note that, consistent with § 413.236(c), CMS will announce its final determination regarding whether the CloudCath System meets the SCI criterion and other eligibility criteria for the TPNIES in the CY 2022 ESRD PPS final rule.
Because the applicant claims to offer the ability to diagnose a medical condition, PD-related peritonitis, earlier in a patient population than allowed by currently available methods, the applicant must also include evidence that use of the new technology to make a diagnosis affects the management of the patient, as required under the SCI criterion at § 412.87(b)(1)(ii)(B). Specifically, § 412.87(b)(1)(ii)(B) states that a determination that a technology represents SCI over existing technology means: The new medical service or technology offers the ability to diagnose a medical condition in a patient population where that medical condition is currently undetectable, or offers the ability to diagnose a medical condition earlier in a patient population than allowed by currently available methods and there must also be evidence that use of the new medical service or technology to make a diagnosis affects the management of the patient.
It is not clear to us whether the studies submitted demonstrate or examine the impacts of using the technology on patients with ESRD such that we can determine whether it represents an advance that substantially improves the treatment of Medicare beneficiaries compared to renal dialysis services previously available. We note that the studies submitted serve as “proof of concept,” as they provide evidence that the CloudCath System detects solid particles in dialysate effluent that may indicate PD-related peritonitis, and, may do so earlier than patient observation and a cell count test. However, the studies are limited in that they do not observe how the CloudCath System, in detecting the solid particles in dialysate effluent and doing so earlier than a cell count test, affects the management of the patient, as required under the SCI criterion at § 412.87(b)(1)(ii)(B). For example, as part of the CATCH Study, investigators deactivated the notification capability of the CloudCath System for the duration of the study, so that neither the participants nor the investigators would be aware of the device measurements.[123] Therefore, the CATCH study did not examine patient and clinician behavior, including the medical management of the patient, after the CloudCath System detected the solid particles in the dialysate effluent. The Briggs et al. study also did not examine how use of the CloudCath System impacted management of the patient. The investigators in that study stated, “none of the data from our device was used for clinical decision making,” meaning that the study did not test how or if the CloudCath System offered the ability to diagnose a medical condition and how use of the CloudCath System to make a diagnosis affected the management of the patient.[124] Because the studies submitted did not observe how patients and clinicians use the CloudCath System's monitoring to make decisions regarding patient management, we are concerned that we will not be able to make a determination on whether early detection of PD-related peritonitis by the CloudCath System meets the SCI criterion at § 412.87(b)(1)(ii)(B). Similarly, while the applicant submitted evidence to show that time-to-treatment plays a role in preventing PD failure in patients with ESRD with PD-related peritonitis,[125] CMS has not received any information regarding how the CloudCath System would affect management of the patient by reducing time-to-treatment for patients with ESRD receiving PD therapy. CMS also notes that the applicant referenced studies that support beginning antibacterial therapy for infections other than PD-related peritonitis, like pneumonia, and, therefore do not directly demonstrate the importance of time-to-treatment for PD-related peritonitis.
Additionally, it is not clear to us whether the CloudCath System would affect medical management of the patient because use of the technology may potentially detect solid particles in dialysate effluent so early, that, in some cases, healthcare providers may decide to wait for confirmation via patient symptoms, cell count, or positive culture as stated in the ISPD guidelines on diagnosis.[126] The preliminary results of the CATCH study demonstrate that in 5 out of 7 PD-related peritonitis events, the CloudCath System detected PD-related peritonitis 33 to 367 hours prior to the time of detection from a clinical laboratory.[127] The CloudCath System also detected PD-related peritonitis 27 to 344 hours prior to participants presenting to a healthcare facility with symptoms of PD-related peritonitis.[128] We note that no evidence was submitted to show that clinicians would begin to treat suspected peritonitis if the CloudCath System alerted the patient and clinician of possible PD-related peritonitis that was too early to detect via any of the ISPD guidelines.[129] In other words, we have not received evidence to demonstrate that the CloudCath System would affect medical management of the patient by replacing one of the ISPD guidelines for diagnosis.[130]
Additionally, CMS notes that the applicant has not submitted evidence to show that beginning treatment for presumed PD-related peritonitis in patients with ESRD prior to the occurrence of any of the ISPD guidelines would not be harmful to patients. In the Briggs et al. study, the CloudCath System identified 20 false positives that occurred because the patient had elevated turbidity due to some cause other than PD-related peritonitis.[131] However, the applicant did not explain or provide evidence on whether beginning treatment for PD-related peritonitis for a group of patients with ESRD who tested positive, but were in fact negative for the condition, was clinically advisable. CMS is concerned that the CloudCath System's potential for false positive results may lead to Start Printed Page 36347clinicians beginning treatment for PD-related peritonitis when not necessary in an already vulnerable group of Medicare beneficiaries. We welcome public comment on these issues.
(6) Capital Related Assets Criterion (§ 413.236(b)(6))
Regarding the sixth TPNIES eligibility criterion in § 413.236(b)(6), limiting capital-related assets from being eligible for the TPNIES, except those that are home dialysis machines, the applicant stated that the CloudCath System is not a capital-related asset. The applicant explained that the CloudCath System does not meet the definition of a capital-related asset, as defined in the Provider Reimbursement Manual (chapter 1, section 104.1), because the device is not subject to depreciation, nor is used by a provider as part of a regular lease agreement.[132]
III. Calendar Year (CY) 2022 Payment for Renal Dialysis Services Furnished to Individuals With Acute Kidney Injury (AKI)
A. Background
The Trade Preferences Extension Act of 2015 (TPEA) (Pub. L. 114-27) was enacted on June 29, 2015, and amended the Act to provide coverage and payment for dialysis furnished by an ESRD facility to an individual with acute kidney injury (AKI). Specifically, section 808(a) of the TPEA amended section 1861(s)(2)(F) of the Act to provide coverage for renal dialysis services furnished on or after January 1, 2017, by a renal dialysis facility or a provider of services paid under section 1881(b)(14) of the Act to an individual with AKI. Section 808(b) of the TPEA amended section 1834 of the Act by adding a subsection (r) to provide payment, beginning January 1, 2017, for renal dialysis services furnished by renal dialysis facilities or providers of services paid under section 1881(b)(14) of the Act to individuals with AKI at the ESRD PPS base rate, as adjusted by any applicable geographic adjustment applied under section 1881(b)(14)(D)(iv)(II) of the Act and adjusted (on a budget neutral basis for payments under section 1834(r) of the Act) by any other adjustment factor under section 1881(b)(14)(D) of the Act that the Secretary elects.
In the CY 2017 ESRD PPS final rule, we finalized several coverage and payment policies in order to implement subsection (r) of section 1834 of the Act and the amendments to section 1881(s)(2)(F) of the Act, including the payment rate for AKI dialysis (81 FR 77866 through 77872, and 77965). We interpret section 1834(r)(1) of the Act as requiring the amount of payment for AKI dialysis services to be the base rate for renal dialysis services determined for a year under the ESRD PPS base rate as set forth in § 413.220, updated by the ESRD bundled market basket percentage increase factor minus a productivity adjustment as set forth in § 413.196(d)(1), adjusted for wages as set forth in § 413.231, and adjusted by any other amounts deemed appropriate by the Secretary under § 413.373. We codified this policy in § 413.372 (81 FR 77965).
B. Proposed Annual Payment Rate Update for CY 2022
1. CY 2022 AKI Dialysis Payment Rate
The payment rate for AKI dialysis is the ESRD PPS base rate determined for a year under section 1881(b)(14) of the Act, which is the finalized ESRD PPS base rate, including the applicable annual productivity-adjusted market basket payment update, geographic wage adjustments, and any other discretionary adjustments, for such year. We note that ESRD facilities have the ability to bill Medicare for non-renal dialysis items and services and receive separate payment in addition to the payment rate for AKI dialysis.
As discussed in section II.B.1.d of this proposed rule, the CY 2022 proposed ESRD PPS base rate is $255.55, which reflects the application of the proposed CY 2022 wage index budget-neutrality adjustment factor of .999546 and the CY 2022 proposed ESRDB market basket increase of 1.6 percent reduced by the productivity adjustment of 0.6 percentage point, that is, 1.0 percent. Accordingly, we are proposing a CY 2022 per treatment payment rate of $255.55 for renal dialysis services furnished by ESRD facilities to individuals with AKI. This payment rate is further adjusted by the wage index, as discussed in the next section of this proposed rule.
2. Geographic Adjustment Factor
Under section 1834(r)(1) of the Act and § 413.372, the amount of payment for AKI dialysis services is the base rate for renal dialysis services determined for a year under section 1881(b)(14) of the Act (updated by the ESRD bundled market basket and reduced by the productivity adjustment), as adjusted by any applicable geographic adjustment factor applied under section 1881(b)(14)(D)(iv)(II) of the Act.[133] Accordingly, we apply the same wage index under § 413.231 that is used under the ESRD PPS and discussed in section II.B.1.b of this proposed rule. The AKI dialysis payment rate is adjusted by the wage index for a particular ESRD facility in the same way that the ESRD PPS base rate is adjusted by the wage index for that facility (81 FR 77868). Specifically, we apply the wage index to the labor-related share of the ESRD PPS base rate that we utilize for AKI dialysis to compute the wage adjusted per-treatment AKI dialysis payment rate. As stated previously, we are proposing a CY 2022 AKI dialysis payment rate of $255.55, adjusted by the ESRD facility's wage index.
IV. End-Stage Renal Disease Quality Incentive Program (ESRD QIP)
A. Background
For a detailed discussion of the End-Stage Renal Disease Quality Incentive Program's (ESRD QIP's) background and history, including a description of the Program's authorizing statute and the policies that we have adopted in previous final rules, we refer readers to the following final rules:
- CY 2011 ESRD PPS final rule (75 FR 49030),
- CY 2012 ESRD PPS final rule (76 FR 628),
- CY 2012 ESRD PPS final rule (76 FR 70228),
- CY 2013 ESRD PPS final rule (77 FR 67450),
- CY 2014 ESRD PPS final rule (78 FR 72156),
- CY 2015 ESRD PPS final rule (79 FR 66120),
- CY 2016 ESRD PPS final rule (80 FR 68968),
- CY 2017 ESRD PPS final rule (81 FR 77834),
- CY 2018 ESRD PPS final rule (82 FR 50738),
- CY 2019 ESRD PPS final rule (83 FR 56922),
- CY 2020 ESRD PPS final rule (84 FR 60648), and
- CY 2021 ESRD PPS final rule (85 FR 71398).
We have also codified many of our policies for the ESRD QIP at 42 CFR 413.177 and 413.178.Start Printed Page 36348
B. Extraordinary Circumstances Exception (ECE) Previously Granted for the ESRD QIP and Notification of ECE Due to ESRD Quality Reporting System Issues
1. Extraordinary Circumstance Exception (ECE) Previously Granted in Response to the COVID-19 PHE
On March 22, 2020, in response to the COVID-19 PHE, we announced relief for clinicians, providers, hospitals, and facilities participating in Medicare quality reporting and value-based purchasing programs.[134] On March 27, 2020, we published a supplemental guidance memorandum that described the scope and duration of the ECEs we were granting under each Medicare quality reporting and VBP program.[135] Each of these ECEs relieved these providers and facilities of their obligation to report data for Q4 CY 2019, Q1 and Q2 CY 2020, but we stated that we would score such data if optionally reported.
The September 2020 IFC updated the ECE we granted in response to the COVID-19 PHE for the ESRD QIP and several other quality reporting programs (85 FR 54827 through 54838).
In the IFC, we updated the ECE policy for the ESRD QIP (85 FR 54828 through 54830). First, we updated our regulations at § 413.178(d)(7) to state that a facility has opted out of the ECE for COVID-19 with respect to the reporting of Q4 CY 2019 NHSN data if the facility actually reported the data by the March 31, 2020 deadline but did not notify CMS that it would do so. Additionally, we finalized that facilities would not have the option to opt-out of the ECE we granted with respect to Q1 and Q2 2020 ESRD QIP data. We stated that measures calculated using excepted data could affect the national comparability of these data due to the geographic differences of COVID-19 incidence rates and hospitalizations along with different impacts resulting from different state and local law and policy changes implemented in response to COVID-19, and therefore may not provide a nationally comparable assessment of performance in keeping with the program goal of national comparison.
In the September 2020 IFC, we welcomed public comments on our policy to update our regulations at § 413.178(d)(7) to consider a facility as having opted out of the ECE with respect to NHSN data reported for Q4 2019 if the facility actually reported the data by the submission deadline, without notifying CMS, and on the exception we finalized to the ECE opt out policy for the ESRD QIP to exclude any ESRD QIP data that facilities optionally reported during Q1 and Q2 2020 from our calculation of PY 2022 TPSs and from the baseline for PY 2023. We will respond to the public comments we received in the CY 2022 ESRD PPS final rule.
2. Notification of ECE Due to ESRD Quality Reporting System (EQRS) Issues
On November 9, 2020,[136] we launched the ESRD Quality Reporting System (EQRS). The EQRS contains the functionalities of the following three legacy ESRD Systems in one global application: (1) A quality measure and VBP performance score review system (ESRD QIP System); (2) an ESRD patient registry and quality measure reporting system through CROWNWeb; and (3) Medicare coverage determination support through the Renal Management Information System (REMIS). The transition to EQRS supports our efforts to consolidate the functionalities of the CROWNWeb, ESRD QIP System, and REMIS applications into a single system, and aims to provide ongoing support to the ESRD user community to foster accurate and timely monthly data submission. This migration eliminates the need for multiple user accounts, and will in the long-term also improve the overall user experience and reduce burden due to enhanced navigation features.
In order to access EQRS, all authorized users must create an account with the Health Care Quality Information Systems (HCQIS) Access Roles and Profile, known as HARP, which is a secure identity management portal provided by CMS. Previously, users created separate accounts for each ESRD application through CMS' Enterprise Identity Data Management (EIDM) system. Creating an account via HARP provides users with a user ID and password that can be used to access many CMS applications. It also provides a single location for users to modify their profile, change their password, update their challenge question, and add or remove two-factor authentication devices. Users can register for a HARP account by going to the QualityNet HARP Registration page, available at https://harp.cms.gov/register/profile-info.
Since the launch of EQRS, several critical data submission issues have been identified that impact the overall quality and accuracy of data available to support the implementation of the ESRD QIP, and we suspended all clinical data submissions into EQRS to allow time to resolve the issue.[137] Based on our assessment, the data submission issues only impact ESRD QIP, Dialysis Star Ratings, Dialysis Facility Compare and data submitted for ESRD Network quality improvement activities. We have analyzed the data submission issues and believe that the data systems issues will be resolved on or about July 12, 2021.
We recognize that these operational systems issues will prevent facilities from submitting ESRD QIP clinical data until the data systems issues are resolved. Therefore, we are announcing a blanket extension of remaining CY 2020 clinical reporting deadlines. Under this extension, facilities will have until September 1, 2021 to submit September through December 2020 ESRD QIP clinical data. We believe this reporting extension aligns with the time estimated for resolution of our operational systems issues and will give dialysis facilities nearly seven weeks to submit their data to EQRS. We will provide further details to facilities when the EQRS issues are resolved, as well as when facilities can begin submitting their data for CY 2020 and CY 2021, through routine communication channels to facilities, vendors, Quality Improvement Organizations (QIOs) and ESRD Networks. The communications could include memos, emails, and notices on the public QualityNet website (https://www.qualitynet.org/). We discuss the treatment of impacted CY 2020 data in this proposed rule. As this situation is ongoing, we will announce any relevant extension deadlines and data submission requirements for impacted CY 2021 data through the routine communication channels discussed above.
Because the current data submissions issue will not be resolved until on or about July 12, 2021 and has impacted all facilities that participate in ESRD QIP, we believe that granting a blanket ECE Start Printed Page 36349to all facilities without a request under 42 CFR 413.178(d)(6)(ii) is the appropriate remedy under these circumstances. We also believe that requiring facilities to report the CY 2020 data impacted by this ECE by September 1, 2021 is reasonable. In our data suspension announcements, we noted that facilities are expected to continue to use EQRS to collect clinical data to complete tasks such as admit and discharge patients, complete CMS forms (such as the CMS-2728: End Stage Renal Disease Medical Evidence Report Medicare Entitlement and/or Patient Registration, CMS-2744: End Stage Renal Disease Annual Facillity Survey Form, and CMS-2746: ESRD Death Notification), add or update treatment summaries, resolve notifications within a timely manner, and should also continue to keep facilities' information up-to-date. In other words, although facilities were unable to submit clinical data through EQRS, facilities were advised that they must continue to collect the clinical data.
While we are working to resolve all known systems issues by on or about July 12, 2021 and reopen submissions so that facilities may submit their September through December 2020 ESRD QIP data no later than September 1, 2021, we will only be able to ensure the validity of the impacted data after they are submitted. Given that the system issues experienced during the initial implementation of the EQRS, if not fully resolved, could potentially impact the accuracy and reliability of the data reported, we are concerned that facilities may be unfairly penalized because the current systems issues may impact the quality of the data. The EQRS system issues have resulted in multiple or incorrect dates of patient admissions and/or discharges, as well as showing duplicate patient records. Facilities have also expressed concerns about their experience with EQRS issues, noting that there is no way for a facility to verify accuracy or completeness. They have reported issues including missing record status in response files, which means that facilities do not know if the records were accepted or received an error response, and issues with determining whether clinical data are accepted because the information does not show in the user interface or the reports that facilities are receiving from EQRS.
We recognize stakeholders' concerns about the potential impact to the quality of data for CY 2020. We believe the observed system issues, and any unresolved issues that may be identified only after data submissions are resumed, could impact the quality and accuracy of the data needed to calculate accurate ESRD QIP scores used for PY 2022 ESRD QIP calculations because patient admittance dates, discharge dates, record status in response files, clinical data, and the number of active patient cases are data points that are included in measure calculations for all of the PY 2022 ESRD QIP measures. If these data points are incorrect, then this would impact our ability to accurately calculate measures and would distort a facility's measure performance.
Therefore, because of the EQRS system issues described above, and additionally, due to the impact of the COVID-19 PHE on some of the PY 2022 ESRD QIP measures, as described more fully in section IV.C. of this proposed rule, we are proposing to not score or award a TPS to any facility, or reduce payment to any facility, in PY 2022, as discussed more fully in section IV.D.
Although we considered if there may be any alternative data sources for the measures impacted by these EQRS system issues, we concluded that this was not feasible for several reasons. First, all 14 ESRD QIP measures for PY 2022 are impacted by these system issues. Although certain measures do not require that facilities submit clinical data into EQRS, we use EQRS data to determine whether a facility has treated a sufficient number of patients in order to meet the measure's minimum patient case threshold necessary to calculate the measure for ESRD QIP. For example, the National Healthcare Safety Network (NHSN) Bloodstream Infection (BSI) clinical measure requires that facilities report data to NHSN. However, the measure also has a requirement to exclude facilities that do not treat at least 11 eligible in-center hemodialysis patients during the 12 month performance period. In order to determine whether a facility has treated at least 11 eligible patients, we use EQRS admission data and Medicare claims data in order to determine whether the facility is eligible to receive a score on the measure.[138]
We ultimately decided to propose the special rule for PY 2022, as described further, because not only do these system issues impact all ESRD QIP measures, which could lead to distorted performance scores and unfair penalties, but we also want to provide facilities with the business certainty they need regarding their PY 2022 payments. In order to determine whether all data quality issues have been resolved when EQRS reopens for data submissions, we will need time to validate the impacted data after facilities are able to resume data submission. Due to the timing of this reporting extension, we believe that there are no feasible alternative data sources for PY 2022. Therefore, we believe that the scoring and payment modifications for PY 2022 as proposed in section IV.D in this proposed rule are appropriate in this situation.
C. Proposed Flexibilities for the ESRD QIP in Response to the COVID-19 PHE
1. Proposal To Adopt a Measure Suppression Policy for the Duration of the COVID-19 PHE
In previous rules, we have identified the need for flexibility in our quality measurement programs to account for changing conditions that are beyond participating facilities' or practitioners' control. We identified this need because we would like to ensure that participants in our programs are not affected negatively when their quality performance suffers for reasons not due to the care provided, but instead due to external factors.
A significant example of the type of external factor that may affect quality measurement is the COVID-19 PHE, which has had, and continues to have, significant and ongoing effects on the provision of medical care in the country and around the world. The COVID-19 pandemic and associated PHE have impeded effective quality measurement in many ways. Changes to clinical practices to accommodate safety protocols for medical personnel and patients, as well as unpredicted changes in the number of stays and facility-level case mixes, have affected the data used in quality measurement and the resulting quality scores. Measures used in the ESRD QIP need to be evaluated to determine whether their specifications need to be updated to account for new clinical guidelines, diagnosis or procedure codes, and medication changes that we have observed during the PHE. Additionally, because COVID-19 prevalence is not consistent across the country, dialysis facilities located in different areas have been affected differently at different times throughout the pandemic. Under those circumstances, we remain significantly concerned that the ESRD QIP's quality measure scores that are calculated using data submitted during the PHE for COVID-19 will be distorted and will result in skewed payment incentives and inequitable payments, particularly for dialysis facilities that have treated more COVID-19 patients than others.
It is not our intention to penalize dialysis facilities based on measure Start Printed Page 36350scores that we believe are distorted by the COVID-19 pandemic and, thus, not reflective of the quality of care that the measures in the ESRD QIP were designed to assess. As discussed above, the COVID-19 pandemic has had, and continues to have, significant and enduring effects on health care systems around the world, and affects care decisions, including those made on clinical topics covered by the ESRD QIP's measures. As a result of the COVID-19 PHE, dialysis facilities could provide care to their patients that meets the underlying clinical standard but results in worse measured performance, and by extension, payment penalties in the ESRD QIP. We are also concerned that regional differences in COVID-19 prevalence during the performance period for PY 2022 have directly affected dialysis facilities' measure scores on the ESRD QIP for PY 2022. Although these regional differences in COVID-19 prevalence rates do not reflect differences in the quality of care furnished by dialysis facilities, they could directly affect the payment penalties that these facilities could receive and could result in an unfair and inequitable distribution of those penalties. These inequities could be especially pronounced for dialysis facilities that have treated a large number of COVID-19 patients.
We are therefore proposing to adopt a policy for the duration of the COVID-19 PHE that would enable us to suppress the use of ESRD QIP measure data for all facilities if we determine that circumstances caused by the COVID-19 PHE have affected those measures and the resulting total performance scores (TPSs) significantly. We are also proposing, as described in more detail in section IV.C.2. of this proposed rule, to suppress certain measures for the PY 2022 program year because we have determined that circumstances caused by the COVID-19 PHE have affected those measures significantly. In addition, due to both the impacts of the COVID-19 PHE on certain measures and the EQRS system issues described in section IV.B.2. we are proposing to adopt a special scoring and payment rule for PY 2022, as described more fully in section IV.D.
In developing this proposed policy, we considered what circumstances caused by the COVID-19 PHE would affect a quality measure significantly enough to warrant its suppression in a value-based purchasing (VBP) program. We believe that a significant deviation in measured performance that can be reasonably attributed to the COVID-19 PHE is a significant indicator of changes in clinical conditions that affect quality measurement. Similarly, we believe that a measure may be focused on a clinical topic or subject that is proximal to the disease, pathogen, or other health impacts of the PHE. As has been the case during the COVID-19 pandemic, we believe that rapid or unprecedented changes in clinical guidelines and care delivery, potentially including appropriate treatments, drugs, or other protocols may affect quality measurement significantly and should not be attributed to the participating facility positively or negatively. We also note that scientific understanding of a particular disease or pathogen may evolve quickly during an emergency, especially in cases of new disease or conditions. Finally, we believe that, as evidenced during the COVID-19 pandemic, national or regional shortages or changes in health care personnel, medical supplies, equipment, diagnostic tools, and patient case volumes or case mix may result in significant distortions to quality measurement.
Based on these considerations, we developed a number of Measure Suppression Factors that we believe should guide our determination of whether to propose to suppress ESRD QIP measures for one or more payment years that overlap with the COVID-19 PHE. We are proposing to adopt these Measure Suppression Factors for use in the ESRD QIP and, for consistency, the following other VBP programs: Hospital VBP, Hospital Readmissions Reduction Program, Hospital-Acquired Condition (HAC) Reduction Program, and Skilled Nursing Facility VBP Program (see, for example, 86 FR 25460 through 25462, 25470 through 25472, and 25497 through 25499). We believe that these Measure Suppression Factors will help us evaluate measures in the ESRD QIP and that their adoption in the other VBP programs noted above will help ensure consistency in our measure evaluations across programs. The proposed Measure Suppression Factors are:
- Factor 1: Significant deviation in national performance on the measure during the COVID-19 PHE, which could be significantly better or significantly worse compared to historical performance during the immediately preceding program years.
- Factor 2: Clinical proximity of the measure's focus to the relevant disease, pathogen, or health impacts of the COVID-19 PHE.
- Factor 3: Rapid or unprecedented changes in:
++ Clinical guidelines, care delivery or practice, treatments, drugs, or related protocols, or equipment or diagnostic tools or materials; or
++ the generally accepted scientific understanding of the nature or biological pathway of the disease or pathogen, particularly for a novel disease or pathogen of unknown origin.
- Factor 4: Significant national shortages or rapid or unprecedented changes in:
++ Healthcare personnel;
++ medical supplies, equipment, or diagnostic tools or materials; or
++ patient case volumes or facility-level case mix.
We also considered alternatives to this proposed policy that could fulfill our objective to not penalize dialysis facilities for measure results that are distorted due to the COVID-19 PHE. As noted above, the country continues to grapple with the effects of the COVID-19 pandemic, and in March 2020, CMS issued a nationwide, blanket Extraordinary Circumstances Exception (ECE) for all hospitals and other facilities participating in our quality reporting and VBP programs in response to the COVID-19 PHE. This blanket ECE excepted all data reporting requirements for Q1 and Q2 2020 data, including claims data and data collected through the CDC's web-based surveillance system for this data period, and quality data collection resumed on July 1, 2020. For claims-based measures, we also stated that we would exclude all qualifying Q1 and Q2 2020 claims from our measure calculations. We considered extending this blanket ECE that we issued for Q1 and Q2 2020 to also include Q3 and Q4 2020. This alternative would protect providers and suppliers from having their quality data used for quality scoring purposes while those data are likely to have been affected significantly by the COVID-19 PHE. However, this option would make quality data collection and reporting to CMS no longer mandatory and would leave no comprehensive data available for us to provide confidential performance feedback to providers nor for monitoring and to inform decision-making for potential future programmatic changes, particularly as the PHE is extended.
As an alternative to the proposed quality measure suppression policy, we also considered not suppressing any measures under the ESRD QIP. However, this alternative would mean assessing dialysis facilities using quality measure data that has been significantly affected by the COVID-19 pandemic. Additionally, given the geographic disparities in the COVID-19 pandemic's effects, implementation of the PY 2022 ESRD QIP as previously finalized would place dialysis facilities in regions that were more heavily impacted by the Start Printed Page 36351pandemic in Q3 and Q4 of 2020 at a disadvantage compared to facilities in regions that were more heavily impacted during the first two quarters for CY 2020.
We view this measure suppression proposal as a necessity to ensure that the ESRD QIP does not penalize facilities based on external factors that were beyond the control of facilities. We intend for this proposed policy to provide short-term relief to dialysis facilities when we have determined that one or more of the Measure Suppression Factors warrants the suppression of an ESRD QIP measure.
We welcome public comments on this proposal for the adoption of a measure suppression policy for the duration of the COVID-19 PHE, and also on the proposed Measure Suppression Factors that we developed for purposes of this proposed policy.
2. Proposals To Suppress Four ESRD QIP Measures for PY 2022
a. Background
In response to the PHE for the COVID-19 pandemic, we have conducted analyses of the fourteen current ESRD QIP measures to determine whether and how COVID-19 may have impacted the validity of these measures. For the reasons discussed below, we have concluded that COVID-19 has so severely impacted the validity of four measures that we cannot fairly and equitably score these measures for the PY 2022 program year, and we are proposing to suppress these measures for the PY 2022 program year for all ESRD QIP participants. Specifically, the measures we are proposing to suppress for the PY 2022 ESRD QIP are as follows:
- SHR clinical measure (under proposed Measure Suppression Factor 1, Significant deviation in national performance on the measure during the COVID-19 PHE, which could be significantly better or significantly worse compared to historical performance during the immediately preceding program years; and proposed Measure Suppression Factor 4, Significant national shortages or rapid or unprecedented changes in:
++ Healthcare personnel;
++ medical supplies, equipment, or diagnostic tools or materials; or (iii) patient case volumes or facility-level case mix);
- Standardized Readmission Ratio (SRR) clinical measure (under proposed Measure Suppression Factor 1, Significant deviation in national performance on the measure during the COVID-19 PHE, which could be significantly better or significantly worse compared to historical performance during the immediately preceding program years; and proposed Measure Suppression Factor 4, Significant national shortages or rapid or unprecedented changes in:
++ Healthcare personnel;
++ medical supplies, equipment, or diagnostic tools or materials; or
++ patient case volumes or facility-level case mix);
- In-Center Hemodialysis Consumer Assessment of Healthcare Providers and Systems (ICH CAHPS) Survey Administration clinical measure (under proposed Measure Suppression Factor 1, Significant deviation in national performance on the measure during the COVID-19 PHE, which could be significantly better or significantly worse compared to historical performance during the immediately preceding program years); and
- Long-Term Catheter Rate clinical measure (under proposed Measure Suppression Factor 1, Significant deviation in national performance on the measure during the COVID-19 PHE, which could be significantly better or significantly worse compared to historical performance during the immediately preceding program years).
b. Proposal To Suppress the SHR Clinical Measure for PY 2022
We are proposing to suppress the SHR clinical measure for the PY 2022 program year under proposed Measure Suppression Factor 1, Significant deviation in national performance on the measure during the COVID-19 PHE, which could be significantly better or significantly worse as compared to historical performance during the immediately preceding program years. The SHR clinical measure is an all-cause, risk-standardized rate of hospitalizations during a 1-year observation window. The standardized hospitalization ratio is defined as the ratio of the number of hospital admissions that occur for Medicare ESRD dialysis patients treated at a particular facility to the number of hospitalizations that would be expected given the characteristics of the dialysis facility's patients and the national norm for dialysis facilities. This measure is calculated as a ratio but can also be expressed as a rate. The intent of the SHR clinical measure is to improve health care delivery and care coordination to help reduce unplanned hospitalization among ESRD patients.
Based on our analysis of Medicare dialysis patient data from January 2020 through August 2020, we found that hospitalizations involving patients diagnosed with COVID-19 resulted in higher mortality rates, higher rates of discharge to hospice or skilled nursing facilities, and lower rates of discharge to home than hospitalizations involving patients who are not diagnosed with COVID-19. Specifically, the hospitalization rate for Medicare dialysis patients diagnosed with COVID-19 was more than 7 times greater than the hospitalization rate during the same period for Medicare dialysis patients who were not diagnosed with COVID-19, which is much greater than the relative risk of hospitalization for any other comorbidity. This indicates that COVID-19 has had a significant impact on the hospitalization rate for dialysis patients. Because COVID-19 Medicare dialysis patients are at significantly greater risk of hospitalization, and the SHR clinical measure was not developed to account for the impact of COVID-19 on this patient population, we are concerned about the effects of the observed COVID-19 hospitalizations on the SHR clinical measure. We also note that COVID-19 affected different regions of the country at different rates depending on factors like time of year, geographic density, state and local policies, and health care system capacity. Because of the increased hospitalization risk associated with COVID-19 and the Medicare dialysis patient population, we are concerned that these regional differences in COVID-19 rates has led to distorted hospitalization rates such that we cannot reliably measure national performance on the SHR clinical measure.
Our analysis of the available Medicare claims data indicates that the COVID-19 PHE has had significant effects on hospital admissions of dialysis patients, and will result in significant deviation in national performance on the measure during the COVID-19 PHE which could be significantly worse as compared to historical performance during the immediately preceding program years. Not only are there effects on patients diagnosed with COVID-19, but the presence of the virus strongly affected hospital admission patterns of dialysis patients from March 2020 to June 2020, and we are concerned that similar effects will be seen in the balance of the calendar year (CY) as the PHE continued. Because the COVID-19 pandemic swept through geographic regions of the country unevenly, we are concerned that dialysis facilities in different regions of the country would have been affected differently throughout the 2020 year, thereby Start Printed Page 36352skewing measure performance and affecting national comparability due to significant and unprecedented changes in patient case volumes or facility-level case mix. Given the limitations of the data available to us for CY 2020, we believe the resulting performance measurement on the SHR clinical measure would not be sufficiently reliable or valid for use in the ESRD QIP.
We are proposing to suppress this measure for the PY 2022 program year, rather than remove it, because we believe that the SHR clinical measure is an important part of the ESRD QIP measure set. However, we are concerned that the COVID-19 PHE affects measure performance on the current SHR clinical measure such that we would not be able to score facilities fairly or equitably on it. Additionally, we would continue to collect the measure's claims data from participating facilities so that we can monitor the effect of the circumstances on quality measurement and determine the appropriate policies in the future. We would also continue to provide confidential feedback reports to facilities as part of program activities to ensure that they are made aware of the changes in performance rates that we observe. We also intend to publicly report PY 2022 data where feasible and appropriately caveated.
We are currently exploring ways to adjust effectively for the systematic effects of the COVID-19 PHE on hospital admissions for the SHR clinical measure. However, we are still working to improve these COVID-19 adjustments and verify the validity of a potential modified version of the SHR clinical measure as additional data become available. As an alternative, we considered whether we could exclude patients with a diagnosis of COVID-19 from the SHR clinical measure cohort, but we determined suppression will provide us with additional time and additional months of data potentially impacted by COVID-19 to more thoroughly evaluate a broader range of alternatives. We want to ensure that the measure reflects care provided to Medicare dialysis patients and we are concerned that excluding otherwise eligible patients may not accurately reflect the care provided, particularly given the unequal distribution of COVID-19 patients across facilities and hospitals over time. As an alternative approach, we also might consider updating the specifications for the SHR clinical measure to eliminate any exposure time and events after infection for patients who contract COVID-19, as COVID-19 symptoms may continue to affect patients after infection. We believe this approach might help distinguish between ESRD-related hospitalizations and COVID-19 related hospitalizations that might otherwise impact SHR clinical measure calculations.
We welcome public comment on our proposal to suppress the SHR clinical measure for PY 2022.
c. Proposal To Suppress the SRR Clinical Measure for PY 2022
We are proposing to suppress the SRR clinical measure for the PY 2022 program year under proposed Measure Suppression Factor 1, Significant deviation in national performance on the measure during the COVID-19 PHE, which could be significantly better or significantly worse compared to historical performance during the immediately preceding program years. The SRR assesses the number of readmission events for the patients at a facility, relative to the number of readmission events that would be expected based on overall national rates and the characteristics of the patients at that facility as well as the number of discharges. The intent of the SRR clinical measure has always been to improve care coordination between dialysis facilities and hospitals to improve communication prior to and post discharge.
Based on our analysis, we found that index discharge hospitalizations involving dialysis patients diagnosed with COVID-19 resulted in lower readmissions and higher mortality rates within the first 7 days. We used index hospitalizations occurring from January 1, 2020 through June 30, 2020 to identify eligible index hospitalizations and unplanned hospital readmissions. In an analysis of unadjusted readmission and death rates by COVID-19 hospitalization status and days since index discharge, during the first 4 to 7 days after discharge there was a readmission rate of 81.3 percent of dialysis patients hospitalized with COVID-19, as compared to 82.6 percent of dialysis patients hospitalized without COVID-19. During that same 4 to 7 day time period, the unadjusted mortality rate for dialysis patients hospitalized with COVID-19 was 16.9 percent, compared with 10.9 percent of patients hospitalized without COVID-19. Based on this discrepancy, we are concerned about the effects of these observations on the calculations for the SRR clinical measure. The denominator of SRR reflects the expected number of index discharges followed by an unplanned readmission within 4 to 30 days in each facility, which is derived from a model that accounts for patient characteristics, the dialysis facility to which the patient is discharged, and the discharging acute care or critical access hospitals involved. Our analysis indicates potential competing risks of higher mortality and lower readmissions due to patient death or discharge to hospice, both of which would remove them from the denominator for the SRR clinical measure. If readmissions rates are lower because patient mortality is higher due to the impact of COVID-19 on dialysis patients, then readmission rates are distorted by appearing significantly better compared to historical performance during the immediately preceding program years. Based on the impact of COVID-19 on SRR results, including the deviance in measurement, we concluded that the SRR clinical measure meets our criteria for Factor 1 where performance data would significantly deviate from historical data performance and would be considered unreliable. Therefore, we believe the resulting performance measurement on the SRR clinical measure would not be sufficiently reliable or valid for use in the ESRD QIP.
We are proposing to suppress this measure for the PY 2022 program year, rather than remove it, because we believe that the SRR clinical measure is an important part of the ESRD QIP Program measure set. However, we are concerned that the PHE for the COVID-19 pandemic affects measure performance on the current SRR clinical measure such that we will not be able to score facilities fairly or equitably on it. Additionally, we would continue to collect the measure's claims data from participating facilities so that we can monitor the effect of the circumstances on quality measurement and determine the appropriate policies in the future. We would also continue to provide confidential feedback reports to facilities as part of program activities to ensure that they are made aware of the changes in performance rates that we observe. We also intend to publicly report PY 2022 data where feasible and appropriately caveated.
We are currently exploring ways to adjust effectively for the systematic effects of the COVID-19 PHE on hospital admissions for the SRR clinical measure. However, we are still working to improve these COVID-19 adjustments and verify the validity of a potential modified version of the SRR clinical measure as additional data becomes available. As an alternative approach, we might also consider eliminating from the calculation of the SRR clinical measure any cases of patients who had a COVID-19 event prior to or at the time of index hospitalization. We believe this Start Printed Page 36353approach might help distinguish between ESRD-related readmissions and COVID-19 related readmissions that might otherwise impact SRR clinical measure calculations.
We welcome public comment on our proposal to suppress the SRR clinical measure for PY 2022.
d. Proposal To Suppress the ICH CAHPS Clinical Measure for PY 2022
We are proposing to suppress the ICH CAHPS clinical measure for the PY 2022 program year under proposed Measure Suppression Factor 1, Significant deviation in national performance on the measure during the COVID-19 PHE, which could be significantly better or significantly worse compared to historical performance during the immediately preceding program years. Based on our analysis of CY 2020 ICH CAHPS data, we have found a significant decrease in response scores as compared to previous years.
The ICH CAHPS clinical measure is scored based on three composite measures and three global ratings.[139] Global ratings questions employ a scale of 0 to 10, worst to best; each of the questions within a composite measure use either “Yes” or “No” responses, or response categories ranging from “Never” to “Always” to assess the patient's experience of care at a facility. Facility performance on each composite measure is determined by the percent of patients who choose “top-box” responses (that is, most positive or “Always”) to the ICH CAHPS survey questions in each domain. The ICH CAHPS survey is administered twice yearly, once in the spring and once in the fall.
Because of the ECE we granted in response to the COVID-19 PHE, facilities were not required to submit CY 2020 spring ICH CAHPS data for purposes of the ESRD QIP. On September 2, 2020, we published an interim final rule with comment (IFC) in the Federal Register titled, “Medicare and Medicaid Programs, Clinical Laboratory Improvement Amendments (CLIA), and Patient Protection and Affordable Care Act; Additional Policy and Regulatory Revisions in Response to the COVID-19 Public Health Emergency” (85 FR 54820) referred to herein as the “September 2020 IFC”. In the September 2020 IFC, we noted that we would not use any first or second quarter CY 2020 data to calculate TPSs for the applicable performance period (85 FR 54829 through 54830). Because the PY 2022 performance period for the ICH CAHPS measure is January 1, 2020 through December 31, 2020, and the ICH CAHPS survey is administered twice a year (once in the spring and once in the fall), we only have data available from the fall CY 2020 survey to calculate facility performance on this measure. Therefore, facilities would only be scored on data based on one ICH CAHPS survey administration for CY 2020, rather than two. Even if we were to score facilities based on the one ICH CAHPS survey administered in the fall, our preliminary data indicates that 95 percent of facilities would not be eligible for scoring on ICH CAHPS for CY 2020. By contrast, 58.9 percent of facilities were not eligible for ICH CAHPS during CY 2018. If we were to score the 5 percent of eligible facilities on ICH CAHPS, we believe there would be a significant deviation in national performance on this measure compared to the national performance based on 41.1 percent of facilities eligible for scoring on ICH CAHPS during 2018. This is a significant deviation in national performance on this measure compared to historical performance during the immediately preceding program years. Given this significant deviation in national performance during the PHE, we believe the ICH CAHPS clinical measure meets the criteria for Measure Suppression Factor 1.
We also believe that this significant change in performance may unfairly penalize facilities and that suppressing this measure for the PY 2022 program year will address concerns about the potential unintended consequences of penalizing facilities that treat COVID-19 diagnosed patients in the ESRD QIP. As alternative approaches, we considered changing the performance period or scoring facilities on one survey administration, but otherwise meeting the 30 completed surveys requirement. However, we found that neither of these approaches were feasible; extending the performance period would not accurately reflect ICH CAHPS performance during CY 2020, and as discussed above, an estimated 95 percent of facilities would not be eligible for ICH CAHPS scoring on one survey. Therefore, to avoid unfairly penalizing facilities due to their performance on the ICH CAHPS survey for the PY 2022 ESRD QIP, we believe it is appropriate to suppress the ICH CAHPS measure for CY 2020, which is the performance period for the PY 2022 ESRD QIP program year (83 FR 57010).
We are proposing to suppress this measure for the PY 2022 program year, rather than remove it, because we believe that the ICH CAHPS measure is an important part of the ESRD QIP measure set. However, we are concerned that the COVID-19 PHE affects measure performance on the current ICH CAHPS measure such that we will not be able to score facilities fairly or equitably on it. Additionally, participating facilities would continue to report the measure's data to CMS so that we can monitor the effect of the circumstances on quality measurement and determine the appropriate policies in the future. We would also continue to provide confidential feedback reports to facilities as part of program activities to ensure that they are made aware of the changes in performance rates that we observe. We also intend to publicly report PY 2022 data where feasible and appropriately caveated.
We welcome public comment on our proposal to suppress the ICH CAHPS measure for the PY 2022 program year.
e. Proposal To Suppress Long-Term Catheter Rate Clinical Measure for PY 2022
Under the measure suppression policy discussion in section IV.C.1 of this proposed rule, we are proposing to suppress the Long-Term Catheter Rate clinical measure for the PY 2022 program year under proposed Measure Suppression Factor 1, Significant deviation in national performance on the measure during the COVID-19 PHE, which could be significantly better or significantly worse compared to historical performance during the immediately preceding program years. Based on our analysis of Long-Term Catheter Rate clinical measure data during CY 2020, we have found a significant increase in long-term catheter use as compared to previous years, which may be the result of hesitancy to seek medical treatment among dialysis patients concerned about being exposed to COVID-19 during the PHE.
In the CY 2018 ESRD PPS final rule, we finalized the inclusion of the Hemodialysis Vascular Access: Long-Term Catheter Rate clinical measure in the ESRD QIP measure set beginning with the PY 2021 program (82 FR 50778). The Long-Term Catheter Rate clinical measure is defined as the percentage of adult hemodialysis patient-months using a catheter continuously for three months or longer for vascular access. The measure is based on vascular access data reported in the Consolidated Renal Operations in a Web-enabled Network (CROWNWeb) and excludes patient-months where a patient has a catheter in place and has a limited life expectancy.Start Printed Page 36354
Our analysis based on the available data indicates that long-term catheter use rates have increased significantly during the COVID-19 PHE. Average long-term catheter rates were averaging around 12 percent in CY 2017 and CY 2018. In CY 2019, rates increased to average around 12.25 percent. This increase continued into CY 2020, with rates reaching a peak of 14.7 percent in June 2020 and declining slightly to 14.3 percent in July and August 2020. After remaining around 12 percent for 3 consecutive years, we view a sudden 2 percent increase in average long-term catheter rates as a significant deviation compared to historical performance during immediately preceding years. We are concerned that the COVID-PHE impacted the ability of ESRD patients to seek treatment from medical providers regarding their catheter use, either due to difficulty accessing treatment due to COVID-19 precautions at healthcare facilities, or due to increased patient reluctance to seek medical treatment because of risk of COVID-19 exposure and increased health risks resulting therefrom, and that these contributed to the significant increase in long-term catheter use rates.
We are proposing to suppress this measure for the PY 2022 program year, rather than remove it, because we believe that the Long-Term Catheter Rate clinical measure is an important part of the ESRD QIP measure set. However, we are concerned that the PHE for COVID-19 affects measure performance on the current Long-Term Catheter Rate clinical measure such that we will not be able to score facilities fairly or equitably on it. Additionally, participating facilities would continue to report the measure's data to CMS so that we can monitor the effect of the circumstances on quality measurement and determine the appropriate policies in the future. We would also continue to provide confidential feedback reports to facilities as part of program activities to ensure that they are made aware of the changes in performance rates that we observe. We also intend to publicly report PY 2022 data where feasible and appropriately caveated.
We welcome public comment on our proposal to suppress the Long-Term Catheter Rate clinical measure for the PY 2022 program year.
D. Proposed Special Scoring Methodology and Payment Policy for the PY 2022 ESRD QIP
As described in section IV.B.2 of this proposed rule, we have considered the impact of operational systems issues preventing facilities from submitting September through December 2020 patient and clinical data into the EQRS from November 1, 2020 through on or about July 12, 2021. Even when facilities are able to submit the September through December 2020 patient and clinical data by September 1, 2021, we will need time to validate the quality and reliability of the impacted data in order to determine whether all data quality issues have been resolved. In addition, as described in section IV.C. we believe four of the ESRD QIP measures have been impacted by the COVID-19 PHE that could result in distorted measure performance for PY 2022.
It is not our intention to penalize dialysis facilities based on the performance on data that are not reliable, thus, not reflective of the quality of care that the measures in the program are designed to assess. Therefore, we are proposing a special rule for PY 2022 scoring for the ESRD QIP under which we would calculate measure rates for all measures, but would not calculate achievement and improvement points for any of them because they have all been impacted by the operational systems issues and, as proposed above, we believe that four of them have additionally been significantly impacted by COVID. Because we would not calculate achievement and improvement scores for any measures, we are also proposing under this special rule that we would not score any of the measures in the four domains or calculate or award Total Performance Scores for any facility. We are also proposing to not apply any payment reductions to ESRD facilities for PY 2022.
In order to ensure that a facility is aware of any changes to its measure rates that we have observed, we are proposing to provide confidential feedback reports that contain the measure rates we calculated for PY 2022. Performance scores for facilities would be released on Dialysis Facility Compare and footnoted to indicate potential accuracy concerns with the scores. Performance score certificates would be generated with the TPS showing as “Not Applicable.”
We propose to codify these policies for PY 2022 at 42 CFR 413.177(a) and § 413.178(h).
However if the policies in sections IV.C and IV.D of this proposed rule are not finalized, the PY 2022 ESRD QIP payment would be as implemented in accordance with our current policy, as well as the payment reduction ranges finalized in the CY 2020 ESRD PPS final rule (84 FR 60725 through 60727).
We invite public comment on this proposed special scoring and payment policy for the PY 2022 ESRD QIP.
E. Proposed Updates to Requirements Beginning With the PY 2024 ESRD QIP
1. PY 2024 ESRD QIP Measure Set
Under our current policy, we retain all ESRD QIP measures from year to year unless we propose through rulemaking to remove them or otherwise provide notification of immediate removal if a measure raises potential safety issues (77 FR 67475). Accordingly, the PY 2024 ESRD QIP measure set will include the same 14 measures as the PY 2023 ESRD QIP measure set (85 FR 71465 through 71466). These measures are described in Table 2. For the most recent information on each measure's technical specifications for PY 2024, we refer readers to the CMS ESRD Measures Manual for the 2021 Performance Period.[140]
Start Printed Page 36355
We discuss our proposal to update the SHR clinical measure in the following section.
a. Proposal To Update the Standardized Hospitalization Ratio (SHR) Clinical Measure Beginning With the PY 2024 ESRD QIP
In the CY 2017 ESRD PPS final rule, we adopted the SHR clinical measure under the authority of section 1881(h)(2)(B)(ii) of the Act (81 FR 77906 through 77911). The SHR clinical measure is a National Quality Forum (NQF)-endorsed all-cause, risk-standardized rate of hospitalizations during a 1-year observation window. The standardized hospitalization ratio is defined as the ratio of the number of hospital admissions that occur for Medicare ESRD dialysis patients treated at a particular facility to the number of hospitalizations that would be expected Start Printed Page 36356given the characteristics of the dialysis facility's patients and the national norm for dialysis facilities. This measure is calculated as a ratio but can also be expressed as a rate.
Hospitalizations are an important indicator of patient morbidity and quality of life. On average, dialysis patients are admitted to the hospital nearly twice a year and spend an average of 11.2 days in the hospital per year.[141] Hospitalizations account for approximately 33 percent of total Medicare expenditures for ESRD patients.[142] Studies have shown that improved health care delivery and care coordination may help reduce unplanned acute care including hospitalization.[143] Hospitalization rates vary across dialysis facilities even after adjustment for patient characteristics, suggesting that hospitalizations might be influenced by dialysis facility practices. An adjusted facility-level standardized hospitalization ratio, accounting for differences in patients' characteristics, plays an important role in identifying potential problems, and helps facilities provide cost-effective quality health care to help limit escalating medical costs.
In the CY 2017 ESRD PPS final rule, we finalized our proposal to adopt the SHR clinical measure, which was a modified version of the NQF-endorsed SHR clinical measure (NQF #1463), as part of the ESRD QIP measure set (81 FR 77911). In that final rule, we stated that our modified SHR clinical measure would incorporate 210 prevalent comorbidities into our risk adjustment calculation, as our analyses suggested that incorporating prevalent comorbidities would result in a more robust and reliable measure of hospitalization (81 FR 77906 through 77907). In that final rule, we explained that data used to calculate the SHR clinical measure are derived from an extensive national ESRD patient database (81 FR 77908). We noted that the database is comprehensive for Medicare Parts A and B patients, and that non-Medicare patients are included in all sources except for the Medicare payment records. In that final rule, we also stated that the Standard Information Management System/CROWNWeb provides tracking by dialysis provider and treatment modality for non-Medicare patients, and information on hospitalizations and patient comorbidities are obtained from Medicare Inpatient Claims Standard Analysis Files. In the CY 2019 ESRD PPS final rule, we increased the weight of the SHR clinical measure from 8.25 percent to 14 percent of the TPS (83 FR 56992 through 56997).
On November 20, 2020, NQF completed its most recent review of the SHR clinical measure, a measure maintenance review, and renewed the measure's endorsement. As part of this review, the NQF endorsed updating the prevalent comorbidity adjustment, which would group 210 individual ICD-9-CM prevalent comorbidities into 90 condition groups, derived from the Agency for Healthcare Research and Quality (AHRQ) Clinical Classifications Software (CCS) groups. The updated prevalent comorbidity adjustment would also limit the source of prevalent comorbidities to inpatient claims. The switch to using only Medicare inpatient claims to identify prevalent comorbidities is due to the lack of Medicare outpatient claims data for the growing Medicare Advantage (MA) patient population. By using the original set of Medicare claims datasets (inpatient, outpatient, hospice, skilled nursing, and home health), the NQF stated its concern that MA patient prevalent comorbidities would be systematically biased. These MA patient prevalent comorbidities would only be populated by Medicare inpatient claims, as compared to non-MA patient prevalent comorbidities that would be populated by the aforementioned set of Medicare claim sources. The updated NQF-endorsed SHR clinical measure would also include all time at risk for MA patients, and added a MA indicator for adjustment in the model. The NQF-endorsed specifications also included updates to parameterization of existing adjustment factors and re-evaluation of interactions, and also created three distinct groups of patients to use in the SHR model based on time spent in a skilled nursing facility, noting that nursing home residence is a marker of higher morbidity.
The updated SHR clinical measure was included on the publicly available “List of Measures under Consideration for December 21, 2020” (MUC List), a list of measures under consideration for use in various Medicare programs.[144] When the Measure Applications Partnership Hospital Workgroup convened on January 11, 2021, it reviewed the MUC List, including the SHR clinical measure. The Measure Applications Partnership Hospital Workgroup recognized that hospitalization rates vary across dialysis facilities, even after adjusting for patient characteristics, which suggests that hospitalizations might be influenced by dialysis facility practices. The Measure Applications Partnership Hospital Workgroup also noted that the SHR clinical measure seeks to improve patient outcomes by measuring hospitalization ratios among dialysis facilities, and that the measure seeks to promote communication between the dialysis facilities and other care settings to improve care transitions.[145] In its final report, the Measure Applications Partnership supported this measure for rulemaking.[146]
In this proposed rule, we are proposing to update the SHR clinical measure specifications to align with the NQF-endorsed updates. These include updates to the risk adjustment method of the measure, which include a prevalent comorbidity adjustment, the addition of MA patients and a MA indicator in the model, updates to parameterization of existing adjustment factors and re-evaluation of interactions, and an indicator for a patient's time spent in a skilled nursing facility.
We believe that adopting these updates would be consistent with our stated goal of evaluating opportunities to more closely align ESRD QIP measures with NQF measure specifications (84 FR 60724). The SHR clinical measure seeks to improve patient outcomes by measuring hospitalization ratios among dialysis facilities, and we believe that these updates would result in a more reliable and robust SHR clinical measure.
We seek comment on this proposal to update the SHR clinical measure specifications for use in the ESRD QIP beginning with PY 2024.Start Printed Page 36357
2. Performance Standards for the PY 2024 ESRD QIP
Section 1881(h)(4)(A) of the Act requires the Secretary to establish performance standards with respect to the measures selected for the ESRD QIP for a performance period with respect to a year. The performance standards must include levels of achievement and improvement, as required by section 1881(h)(4)(B) of the Act, and must be established prior to the beginning of the performance period for the year involved, as required by section 1881(h)(4)(C) of the Act. We refer readers to the CY 2013 ESRD PPS final rule (76 FR 70277) for a discussion of the achievement and improvement standards that we have established for clinical measures used in the ESRD QIP. We define the terms “achievement threshold,” “benchmark,” “improvement threshold,” and “performance standard” in our regulations at § 413.178(a)(1), (3), (7), and (12), respectively.
a. Proposal To Update the Performance Standards Applicable to the PY 2024 Clinical Measures
Our current policy is to automatically adopt a performance and baseline period for each year that is 1 year advanced from those specified for the previous payment year (84 FR 60728). Under this policy, CY 2022 is currently the performance period and CY 2020 is the baseline period for the PY 2024 ESRD QIP. However, under the nationwide ECE that we granted in response to the COVID-19 PHE, first and second quarter data for CY 2020 are excluded from scoring for purposes of the ESRD QIP. We are concerned that it will be difficult to assess levels of achievement and improvement if the performance standards are based on partial year data.[147] Our preliminary analysis indicates that the effect of the excluded data would create higher performance standards for certain measures and lower performance standards for other measures, which may skew achievement and improvement thresholds for facilities and therefore may result in performance standards that do not accurately reflect levels of achievement and improvement.
Our current policy substitutes the performance standard, achievement threshold, and/or benchmark for a measure for a performance year if final numerical values for the performance standard, achievement threshold, and/or benchmark are worse than the numerical values for that measure in the previous year of the ESRD QIP (82 FR 50764). We adopted this policy because we believe that the ESRD QIP should not have lower performance standards than in previous years. However, our general policy provides flexibility to substitute the performance standard, achievement threshold and benchmark in appropriate cases (82 FR 50764).
Although the lower performance standards would be substituted with those from the prior year, the higher performance standards would be used to set performance standards for certain measures, even though they would be based on partial year data. We are concerned that this may create performance standards for certain measures that would be difficult for facilities to attain with a full 12 months of data.
Therefore, in this proposed rule, we are proposing to calculate the performance standards for PY 2024 using CY 2019 data, which is the most recently available full calendar year of data we can use to calculate those standards. Due to the impact of CY 2020 data that is excluded from the ESRD QIP for scoring purposes, we believe that using CY 2019 data for performance standard setting purposes is appropriate. Consistent with our established policy, we would continue to use the prior year's numerical values for performance standard, achievement threshold, and benchmark if the most recent full CY's final numerical values are worse.
We welcome public comments on this proposal.
b. Performance Standards for the PY 2024 ESRD QIP if Proposal to Use CY 2019 as the Baseline Period is Finalized
Table 3 displays the achievement thresholds, 50th percentiles of the national performance, and benchmarks for the PY 2024 clinical measures, and we would use these standards if our proposal to use CY 2019 as the baseline period is finalized.
Start Printed Page 36358
In addition, we have summarized in Table 4 existing requirements for successful reporting on reporting measures in the PY 2024 ESRD QIP. We are not making any proposals to change these standards as a result of the COVID-19 PHE.
Start Printed Page 36359
3. Eligibility Requirements for the PY 2024 ESRD QIP
Our current minimum eligibility requirements for scoring the ESRD QIP measures are described in Table 5.
Start Printed Page 36360
4. Payment Reduction Scale for the PY 2024 ESRD QIP
Under our current policy, a facility will not receive a payment reduction for a payment year in connection with its performance for the ESRD QIP if it achieves a TPS that is at or above the minimum TPS (mTPS) that we establish for the payment year. We have defined the mTPS in our regulations at § 413.178(a)(8) as, with respect to a payment year, the TPS that an ESRD facility would receive if, during the baseline period it performed at the 50th percentile of national performance on all clinical measures and the median of national ESRD facility performance on all reporting measures.
Our current policy, which is codified at § 413.177 of our regulations, also implements the payment reductions on a sliding scale using ranges that reflect payment reduction differentials of 0.5 percent for each 10 points that the facility's TPS falls below the mTPS (76 FR 634 through 635).
For PY 2024, based on available data, a facility must meet or exceed a mTPS of 57 in order to avoid a payment reduction. We note that the mTPS in this proposed rule is based on data from CY 2019 instead of the PY 2024 baseline period (CY 2020) because we have proposed to use CY 2019 as the baseline period for that payment year.
We refer readers to Table 3 for the estimated values of the 50th percentile of national performance for each clinical measure. Under our current policy, a facility that achieves a TPS of 56 or below would receive a payment reduction based on the TPS ranges indicated in Table 6.
Start Printed Page 36361
If we do not finalize the proposed update to our performance standards policy as described in section IV.E.2.a of this proposed rule, then we would update the mTPS for PY 2024, as well as the payment reduction ranges for that payment year, in the CY 2022 ESRD PPS final rule using data from CY 2020.
F. Updates for the PY 2025 ESRD QIP
1. Continuing Measures for the PY 2025 ESRD QIP
Under our previously adopted policy, the PY 2024 ESRD QIP measure set will also be used for PY 2025. At this time, we are not proposing to adopt any new measures beginning with the PY 2025 ESRD QIP.
2. Performance Period for the PY 2025 ESRD QIP
We continue to believe that 12-month performance and baseline periods provide us sufficiently reliable quality measure data for the ESRD QIP. Under this policy, we would adopt CY 2023 as the performance period and CY 2021 as the baseline period for the PY 2025 ESRD QIP.
In this proposed rule, we are not proposing any changes to this policy.
3. Performance Standards for the PY 2025 ESRD QIP
Section 1881(h)(4)(A) of the Act requires the Secretary to establish performance standards with respect to the measures selected for the ESRD QIP for a performance period with respect to a year. The performance standards must include levels of achievement and improvement, as required by section 1881(h)(4)(B) of the Act, and must be established prior to the beginning of the performance period for the year involved, as required by section 1881(h)(4)(C) of the Act. We refer readers to the CY 2012 ESRD PPS final rule (76 FR 70277) for a discussion of the achievement and improvement standards that we have established for clinical measures used in the ESRD QIP. We define the terms “achievement threshold,” “benchmark,” “improvement threshold,” and “performance standard” in our regulations at § 413.178(a)(1), (3), (7), and (12), respectively. In section IV.E.2.a of this proposed rule, we note that we are proposing to use CY 2019 data for purposes of calculating the performance standards for PY 2024 because, due to the anticipated impact of CY 2020 data that is excluded from the ESRD QIP for scoring purposes during CY 2020, we believe that using CY 2019 data for performance standard setting purposes would be appropriate.
a. Performance Standards for Clinical Measures in the PY 2025 ESRD QIP
At this time, we do not have the necessary data to assign numerical values to the achievement thresholds, benchmarks, and 50th percentiles of national performance for the clinical measures for the PY 2025 ESRD QIP because we do not have CY 2021 data. We intend to publish these numerical values, using CY 2021 data, in the CY 2023 ESRD PPS final rule.
b. Performance Standards for the Reporting Measures in the PY 2025 ESRD QIP
In the CY 2019 ESRD PPS final rule, we finalized the continued use of existing performance standards for the Screening for Clinical Depression and Follow-Up reporting measure, the Ultrafiltration Rate reporting measure, the NHSN Dialysis Event reporting measure, and the MedRec reporting measure (83 FR 57010 through 57011). We will continue use of these performance standards in PY 2025.
4. Scoring the PY 2025 ESRD QIP
a. Scoring Facility Performance on Clinical Measures
In the CY 2014 ESRD PPS final rule, we finalized policies for scoring performance on clinical measures based on achievement and improvement (78 FR 72215 through 72216). In the CY 2019 ESRD PPS final rule, we finalized a policy to continue use of this methodology for future payment years (83 FR 57011) and we codified these scoring policies at § 413.178(e).
In this proposed rule, we are not proposing any changes to this policy for PY 2025.
b. Scoring Facility Performance on Reporting Measures
Our policy for scoring performance on reporting measures is codified at § 413.178(e), and more information on our scoring policy for reporting measures can be found in the CY 2020 ESRD PPS final rule (84 FR 60728). We previously finalized policies for scoring performance on the NHSN Dialysis Event reporting measure in the CY 2018 ESRD PPS final rule (82 FR 50780 through 50781), as well as policies for scoring the MedRec reporting measure and Clinical Depression Screening and Follow-up reporting measure in the CY 2019 ESRD PPS final rule (83 FR 57011). We also previously finalized the scoring policy for the STrR reporting measure in the CY 2020 ESRD PPS final rule (84 FR 60721 through 60723). In the CY 2021 ESRD PPS final rule, we finalized our updated scoring methodology for the Ultrafiltration Rate reporting measure (85 FR 71468 through 71470).
In this proposed rule, we are not proposing any changes to this policy for PY 2025.
5. Weighting the Measure Domains and the TPS for PY 2025
Under our current policy, we assign the Patient & Family Engagement Start Printed Page 36362Measure Domain a weight of 15 percent of the TPS, the Care Coordination Measure Domain a weight of 30 percent of the TPS, the Clinical Care Measure Domain a weight of 40 percent of the TPS, and the Safety Measure domain a weight of 15 percent of the TPS.
In the CY 2019 ESRD PPS final rule, we finalized a policy to assign weights to individual measures and a policy to redistribute the weight of unscored measures (83 FR 57011 through 57012). In the CY 2020 ESRD PPS final rule, we finalized a policy to use the measure weights we finalized for PY 2022 for the PY 2023 ESRD QIP and subsequent payment years, and also to use the PY 2022 measure weight redistribution policy for the PY 2023 ESRD QIP and subsequent payment years (84 FR 60728 through 60729). We are not proposing any updates to these policies for PY 2025.
G. Requests for Information (RFIs) on Topics Relevant to ESRD QIP
1. Closing the Health Equity Gap in CMS Quality Programs Request for Information
Persistent inequities in health care outcomes exist in the United States (U.S.), including among Medicare patients. In recognition of persistent health disparities and the importance of closing the health equity gap, we request information on expanding several related CMS programs to make reporting of health disparities based on social risk factors and race and ethnicity, and disability more comprehensive and actionable for dialysis facilities, providers, and patients. The following is part of an ongoing effort across CMS to evaluate appropriate initiatives to reduce health disparities. Feedback will be used to inform the creation of a future, comprehensive, request for information (RFI) focused on closing the health equity gap in CMS programs and policies. This RFI contains four parts:
- Background. This section provides information on existing statements describing our commitment to health equity, and existing initiatives with an emphasis on reducing disparity.
- Current CMS Disparity Methods. This section describes the methods, measures, and indicators of social risk currently used with the CMS Disparity Methods.
- Future potential stratification of quality measure results. This section describes four potential future expansions of the CMS Disparity Methods, including (a) Future potential stratification of quality measure results by dual eligibility; (b) Future potential stratification of quality measure results by race and ethnicity; (c) Improving Demographic Data Collection; and (d) Potential Creation of an ESRD Facility Equity Score to Synthesize Results Across Multiple Social Risk Factors.
- Solicitation of public comment. This section specifies 11 requests for feedback on the topics specified in this RFI.
a. Background
Significant and persistent inequities in health care outcomes exist in the U.S.[148] Belonging to a racial or ethnic minority group, living with a disability, being a member of the lesbian, gay, bisexual, transgender, and queer (LGBTQ+) community, living in a rural area, or being near or below the poverty level, is often associated with worse health outcomes.[149 150 151 152 153 154 155 156] Such disparities in health outcomes are the result of number of factors, but importantly for CMS programs, although not the sole determinant, poor access and provision of lower quality health care contribute to health disparities. For instance, numerous studies have shown that among Medicare beneficiaries, racial and ethnic minority individuals often receive lower quality of care, report lower experiences of care, and experience more frequent hospital readmissions and operative complications.[157 158 159 160 161 162] Readmission rates for common conditions in the Hospital Readmissions Reduction Program are higher for Black Medicare beneficiaries and higher for Hispanic Medicare beneficiaries with Congestive Heart Failure and Acute Myocardial Infarction.[163 164 165 166 167] Although Black Americans represent 7.5 percent of all older adult Medicare beneficiaries, they represent 28 percent of those with ESRD.[168] Among individuals with ESRD the odds of 30-day hospital readmission are 19 percent higher for Black beneficiaries as compared with white beneficiaries.[169] Studies have also shown that African Americans are significantly more likely than white Americans to die prematurely from heart disease and stroke.[170] The COVID-19 pandemic has further illustrated many of these longstanding health inequities with higher rates of infection, hospitalization, and mortality among Black, Latino, and Indigenous and Native American Start Printed Page 36363persons relative to white persons.[171 172 ] In the ESRD patient population, one study found that the rate of COVID-19 hospitalizations among dialysis patients peaked at 40 times higher than the rate in the general population during the pandemic, with Black, Latino, and Asian persons hospitalized at a higher rate than white persons.[173] As noted by the Centers for Disease Control “long-standing systemic health and social inequities have put many people from racial and ethnic minority groups at increased risk of getting sick and dying from COVID-19.” [174] One important strategy for addressing these important inequities is by improving data collection to allow for better measurement and reporting on equity across our programs and policies.
We are committed to achieving equity in health care outcomes for our beneficiaries by supporting providers in quality improvement activities to reduce health inequities, enabling them to make more informed decisions, and promoting provider accountability for health care disparities.[175] For the purposes of this rule, we are using a definition of equity established in Executive Order 13985, as “the consistent and systematic fair, just, and impartial treatment of all individuals, including individuals who belong to underserved communities that have been denied such treatment, such as Black, Latino, and Indigenous and Native American persons, Asian Americans and Pacific Islanders and other persons of color; members of religious minorities; lesbian, gay, bisexual, transgender, and queer (LGBTQ+) persons; persons with disabilities; persons who live in rural areas; and persons otherwise adversely affected by persistent poverty or inequality.” [176] We note that this definition was recently established by the Biden administration, and provides a useful, common definition for equity across different areas of government, although numerous other definitions of equity exist.
Our ongoing commitment to closing the equity gap in CMS quality programs is demonstrated by a portfolio of programs aimed at making information on the quality of health care providers and services, including disparities, more transparent to consumers and providers. The CMS Equity Plan for Improving Quality in Medicare outlines a path to equity which aims to support Quality Improvement Networks and Quality Improvement Organizations (QIN-QIOs); federal, state, local, and tribal organizations; providers; researchers; policymakers; beneficiaries and their families; and other stakeholders in activities to achieve health equity.[177] The CMS Equity Plan for Improving Quality in Medicare focuses on three core priority areas which inform our policies and programs: (1) Increasing understanding and awareness of disparities; (2) developing and disseminating solutions to achieve health equity; and (3) implementing sustainable actions to achieve health equity.[178] The CMS Quality Strategy [179] and Meaningful Measures Framework [180] include elimination of racial and ethnic disparities as a central principle. Our efforts aimed at closing the health equity gap to date have included both providing transparency of health disparities, supporting providers with evidence-informed solutions to achieve health equity, and reporting to providers on gaps in quality in the following:
- The CMS Mapping Medicare Disparities Tool which is an interactive map that identifies areas of disparities and is a starting point to understand and investigate geographic, racial and ethnic differences in health outcomes for Medicare patients.[181]
- The Racial, Ethnic, and Gender Disparities in Health Care in Medicare Advantage Stratified Report, which highlights racial and ethnic differences in health care experiences and clinical care, compares quality of care for women and men, and looks at racial and ethnic differences in quality of care among women and men separately for Medicare Advantage plans.[182]
- The Rural-Urban Disparities in Health Care in Medicare Report which details rural-urban differences in health care experiences and clinical care.[183]
- The Standardized Patient Assessment Data Elements for certain post-acute care Quality Reporting Programs, which now includes data reporting for race and ethnicity and preferred language, in addition to screening questions for social needs (84 FR 42536 through 42588).
- The CMS Innovation Center's Accountable Health Communities Model which includes standardized collection of health-related social needs data.
- The Guide to Reducing Disparities which provides an overview of key issues related to disparities in readmissions and reviews set of activities that can help hospital leaders reduce readmissions in diverse populations.[184]
- The Chronic Kidney Disease Disparities: Educational Guide for Primary Care, which is intended to foster the development of primary care practice teams in order to enhance care for vulnerable patients with chronic kidney disease (CKD) and are at risk of progression of disease or complications. The guide provides information about disparities in the care of patients with CKD, presents potential actions that may improve care and suggests other available resources that may be used by primary care practice teams in caring for vulnerable patients.[185]
- The CMS Disparity Methods which provide hospital-level confidential results stratified by dual eligibility for condition-specific readmission Start Printed Page 36364measures currently included in the Hospital Readmissions Reduction Program (see 84 FR 42496 through 42500 for a discussion of using stratified data in additional measures).
These programs are informed by reports by the National Academies of Science, Engineering and Medicine (NASEM) [186] and the Office of the Assistant Secretary for Planning and Evaluation (ASPE) [187] which have examined the influence of social risk factors on several of our quality programs. In this request for public comment, we address only the eighth initiative listed above, the CMS Disparity Methods, which we have implemented for measures in the Hospital Readmissions Reduction Program and are considering in other programs, including the ESRD QIP. We discuss the implementation of these methods to date and present considerations for continuing to improve and expand these methods.
b. Current CMS Disparity Methods
We first sought public comment on potential confidential and public reporting of ESRD QIP measure data stratified by social risk factors in the CY 2018 ESRD PPS proposed rule (82 FR 31202). We initially focused on stratification by dual eligibility, which is consistent with recommendations from ASPE's First Report to Congress which was required by the Improving Medicare Post-Acute Care Transformation (IMPACT) Act of 2014 (Pub. L. 113-185).[188] This report found that in the context of value-based purchasing (VBP) programs, dual eligibility was among the most powerful predictors of poor health outcomes among those social risk factors that ASPE examined and tested. In the FY 2018 IPPS/LTCH PPS final rule we also solicited feedback on two potential methods for illuminating differences in outcomes rates among patient groups within a provider's patient population that would also allow for a comparison of those differences, or disparities, across providers for the Hospital IQR program (82 FR 38403 through 38409). The first method (the Within-Hospital disparity method) promotes quality improvement by calculating differences in outcome rates among patient groups within a hospital while accounting for their clinical risk factors. This method also allows for a comparison of the magnitude of disparity across hospitals, so hospitals could assess how well they are closing disparity gaps compared to other hospitals. The second methodological approach (the Across-Hospital method) is complementary and assesses hospitals' outcome rates for dual-eligible patients only, across hospitals, allowing for a comparison among hospitals on their performance caring for their patients with social risk factors. In the CY 2018 ESRD PPS proposed rule (82 FR 31202 through 31203), we also specifically solicited feedback on which social risk factors provide the most valuable information to stakeholders. In addition, feedback was solicited on the methodology for illuminating differences in outcomes rates among patient groups within a provider's patient population that would also allow for a comparison of those differences, or disparities, across providers. Overall, comments supported the use of dual eligibility as a proxy for social risk, although commenters also suggested investigation of additional social risk factors, and we continue to consider commenter suggestions for which risk factors provide the most valuable information to stakeholders.
c. Future Potential Expansion of the CMS Disparity Methods to the ESRD QIP
We are committed to advancing health equity by improving data collection to better measure and analyze disparities across programs and policies.[189] As we previously noted, we have been considering, among other things, expanding our efforts to provide stratified data for additional social risk factors and measures, optimizing the ease-of-use of the results, enhancing public transparency of equity results, and building towards provider accountability for health equity. We are seeking public comment on the potential stratification of quality measures in the ESRD QIP across two social risk factors: Dual eligibility and race/ethnicity.
(1) Stratification of Quality Measure Results—Dual Eligibility
As described above, landmark reports by NASEM [190] and ASPE,[191] which have examined the influence of social risk factors on several of our quality programs, have shown that in the context of VBP programs, dual eligibility, as an indicator of social risk, is a powerful predictor of poor health outcomes. We are considering stratification of quality measure results in the ESRD QIP and are considering which measures would be most appropriate for stratification and if dual eligibility would be a meaningful social risk factor for stratification.
For the ESRD QIP, we would consider disparity reporting using two disparity methods the Within-Facility and Across-Facility methods. The first method (based on the Within-Hospital disparity method, described above) would aim to promote quality improvement by calculating differences in outcome rates between dual and non-dual eligible patient groups within a facility while accounting for their clinical risk factors. This method would allow for a comparison of those differences, or disparities, across facilities, so facilities could assess how well they are closing disparity gaps compared to other facilities. The second approach (based on the Across-Hospital method) would be complementary and assesses facilities' outcome rates for subgroups of patients, such as dual eligible patients, across facilities, allowing for a comparison among facilities on their performance caring for their patients with social risk factors.
(2) Stratification of Quality Measure Results—Race and Ethnicity
The Administration's Executive Order on Advancing Racial Equity and Support for Underserved Communities Through the Federal Government directs agencies to assess potential barriers that underserved communities and individuals may face to enrollment in and access to benefits and services in federal programs. As summarized earlier in the preamble, studies have shown that among Medicare beneficiaries, racial and ethnic minority persons often experience worse health outcomes, including more frequent hospital readmissions and procedural Start Printed Page 36365complications.[192] We also note that the prevalence of ESRD is higher among racial minorities.[193] For example, in 2016 ESRD prevalence was approximately 9.5 times greater in Native Hawaiians and Pacific Islanders, 3.7 times greater in African Americans, 1.5 times greater in American Indians and Alaska Natives, and 1.3 times greater in Asians.[194] An important part of identifying and addressing inequities in health care is improving data collection to allow us to better measure and report on equity across our programs and policies. We are considering stratification of quality measure results in the ESRD QIP by race and ethnicity, and are identifying which measures would be most appropriate for stratification.
As outlined in the 1997 Office of Management and Budget (OMB) Revisions to the Standards for the Collection of Federal Data on Race and Ethnicity, the racial and ethnic categories which may be used for reporting the disparity methods are considered to be social and cultural, not biological or genetic.[195] The 1997 OMB Standard lists five minimum categories of race: (1) American Indian or Alaska Native; (2) Asian; (3) Black or African American; (4) Native Hawaiian or Other Pacific Islander; (5) and White. In the OMB standards, Hispanic or Latino is the only ethnicity category included, and since race and ethnicity are two separate and distinct concepts, persons who report themselves as Hispanic or Latino can be of any race.[196] Another example, the “Race & Ethnicity—CDC” code system in Public Health Information Network (PHIN) Vocabulary Access and Distribution Systems (VADS) [197] permits a much more granular structured recording of a patient's race and ethnicity with its inclusion of over 900 concepts for race and ethnicity. The recording and exchange of patient race and ethnicity at such a granular level can facilitate the accurate identification and analysis of health disparities based on race and ethnicity. Further, the “Race & Ethnicity—CDC” code system has a hierarchy that rolls up to the OMB minimum categories for race and ethnicity and, thus, supports aggregation and reporting using the OMB standard. ONC includes both the CDC and OMB standards in its criterion for certified health IT products.[198] For race and ethnicity, a certified health IT product must be able to express both detailed races and ethnicities using any of the 900 plus concepts in the “Race & Ethnicity—CDC” code system in PHIN VADS, as well as aggregate each one of a patient's races and ethnicities to the categories in the OMB standard for race and ethnicity. This approach can reduce burden on providers recording demographics using certified products.
Self-reported race and ethnicity data remain the gold standard for classifying an individual according to race or ethnicity. However, historical inaccuracies in federal data systems and limited collection classifications have contributed to the limited quality of race and ethnicity information in our administrative data systems.[199] In recent decades, to address these data quality issues, CMS has undertaken numerous initiatives, including updating data taxonomies and conducting direct mailings to some beneficiaries to enable more comprehensive race and ethnic identification.[200 201] Despite those efforts, studies reveal varying data accuracy in identification of racial and ethnic groups in Medicare administrative data, with higher sensitivity for correctly identifying white and Black individuals, and lower sensitivity for correctly identifying individuals of Hispanic ethnicity or of Asian/Pacific Islander and American Indian/Alaskan Native race.[202] Incorrectly classified race or ethnicity may result in overestimation or underestimation in the quality of care received by certain groups of beneficiaries.
We continue to work with public and private partners to better collect and leverage data on social risk to improve our understanding of how these factors can be better measured in order to close the health equity gap. Among other things, we have developed an Inventory of Resources for Standardized Demographic and Language Data Collection [203] and supported collection of specialized International Classification of Disease, 10th Edition, Clinical Modification (ICD-10-CM) codes for describing the socioeconomic, cultural, and environmental determinants of health, and sponsored several initiatives to statistically estimate race and ethnicity information when it is absent.[204]
The Office of the National Coordinator for Health Information Technology (ONC) included social, psychological, and behavioral standards in the 2015 Edition health information technology certification criteria (2015 Edition), providing interoperability standards LOINC (Logical Observation Identifiers Names and Codes) and SNOMED CT (Systematized Nomenclature of Medicine—Clinical Terms) for financial strain, education, social connection and isolation, and others. Additional stakeholder efforts underway to expand capabilities to capture additional social determinants of health data elements include the Gravity Project to identify and harmonize social risk factor data for interoperable electronic health information exchange for EHR fields, as well as proposals to expand the ICD-10 (International Classification of Diseases, Tenth Revision) Z-codes, the alphanumeric codes used worldwide to represent diagnoses.[205]
While development of sustainable and consistent programs to collect data on social determinants of health can be considerable undertakings, we recognize Start Printed Page 36366that another method to identify better race and ethnicity data is needed in the short term to address the need for reporting on health equity. In working with our contractors, two algorithms have been developed to indirectly estimate the race and ethnicity of Medicare beneficiaries (as described further in the next section). We believe that using indirect estimation can help to overcome the current limitations of demographic information and enable timelier reporting of equity results until longer term collaborations to improve demographic data quality across the health care sector materialize. The use of indirectly estimated race and ethnicity for conducting stratified reporting does not place any additional collection or reporting burdens on facilities as these data are derived using existing administrative and Census-linked data.
Indirect estimation relies on a statistical imputation method for inferring a missing variable or improving an imperfect administrative variable using a related set of information that is more readily available.[206] Indirectly estimated data are most commonly used at the population level (such as the facility or health plan-level), where aggregated results form a more accurate description of the population than existing, imperfect data sets. These methods often estimate race and ethnicity using a combination of other data sources which are predictive of self-identified race and ethnicity, such as language preference, information about race and ethnicity in our administrative records, first and last names matched to validated lists of names correlated to specific national origin groups, and the racial and ethnic composition of the surrounding neighborhood. Indirect estimation has been used in other settings to support population-based equity measurement when self-identified data are not available.[207]
As discussed earlier in the preamble, we have previously supported the development of two such methods of indirect estimation of race and ethnicity of Medicare beneficiaries. One indirect estimation approach, developed by our contractor, uses Medicare administrative data, first name and surname matching, derived from the U.S. Census and other sources, with beneficiary language preference, state of residence, and the source of the race and ethnicity code in Medicare administrative data to reclassify some beneficiaries as Hispanic or Asian Pacific Islander (API).[208] In recent years, we have also worked with another contractor to develop a new approach, the Medicare Bayesian Improved Surname Geocoding (MBISG), which combines Medicare administrative data, first and surname matching, geocoded residential address linked to the 2010 U.S. Census, and uses both Bayesian updating and multinomial logistic regression to estimate the probability of belonging to each of six racial/ethnic groups.[209]
The MBISG model is currently used to conduct the national, contract-level, stratified reporting of Medicare Part C & D performance data for Medicare Advantage Plans by race and ethnicity.[210] Validation testing reveals concordances of 0.88-0.95 between indirectly estimated and self-report among individuals who identify as White, Black, Hispanic, and Asian Pacific Islander for the MBISG version 2.0 and concordances with self-reported race and ethnicity of 0.96-0.99 for these same groups for MBISG version 2.1.[211 212] The algorithms under consideration are considerably less accurate for individuals who self-identify as American Indian or Alaskan Native as well as for those who self-identify as multiracial.[213]
Indirect estimation can be a statistically reliable approach for calculating population-level equity results for groups of individuals (such as the facility-level) and is not intended, nor being considered, as an approach for inferring the race and ethnicity of an individual. However, despite the high degree of statistical accuracy of the indirect estimation algorithms under consideration there remains the small risk of unintentionally introducing bias. For example, if the indirect estimation is not as accurate in correctly estimating race and ethnicity in certain geographies or populations it could lead to some bias in the method results. Such bias might result in slight overestimation or underestimation of the quality of care received by a given group. We feel this amount of bias is considerably less than would be expected if stratified reporting was conducted using the race and ethnicity currently contained in our administrative data. Indirect estimation of race and ethnicity is envisioned as an intermediate step, filling the pressing need for more accurate demographic information for the purposes of exploring inequities in service delivery, while allowing newer approaches, as described in the next section, for enhancing demographic data collection. We are interested in learning more about, and soliciting comments, about the potential benefits and challenges associated with measuring facility equity using an imputation algorithm to enhance existing administrative data quality for race and ethnicity until self-reported information is sufficiently available.
(3) Improving Demographic Data Collection
Stratified facility-level reporting using indirectly estimated race and ethnicity and dual eligibility would represent an important advance in our ability to provide equity reports to facilities. However, self-reported disability status, race and ethnicity data remain the gold standard for classifying an individual according to disability status, race or ethnicity. The CMS Quality Strategy outlines our commitment to strengthening infrastructure and data systems by ensuring that standardized demographic information is collected to identify disparities in health care delivery outcomes.[214] Collection and sharing of a standardized set of social, psychological, and behavioral data by facilities, including disability status and race and ethnicity, using electronic data definitions which permit nationwide, interoperable health information Start Printed Page 36367exchange, can significantly enhance the accuracy and robustness of our equity reporting.[215] This could potentially include expansion to additional social risk factors, such as language preference and disability status, where accuracy of administrative data is currently limited. We are mindful that additional resources, including data collection and staff training may be necessary to ensure that conditions are created whereby all patients are comfortable answering all demographic questions, and that individual preferences for non-response are maintained.
We are also interested in learning about and are soliciting comments on current data collection practices by facilities to capture demographic data elements (such as race, ethnicity, sex, sexual orientation and gender identity (SOGI), language preference, and disability status). Further, we are interested in potential challenges facing facility collection of a minimum set of demographic data elements in alignment with national data collection standards (such as the standards finalized by the Affordable Care Act) [216] and standards for interoperable exchange (such as the U.S. Core Data for Interoperability put forth by the Office of the National Coordinator for Health Information Technology for incorporation in certified health IT products as part of the 2015 Edition of health IT certification criteria.) [217] Advancing data interoperability through collection of a minimum set of demographic data collection has the potential for improving the robustness of the disparity methods results, potentially permitting reporting using more accurate, self-reported, information, such as race and ethnicity, and expanding reporting to additional dimensions of equity, including stratified reporting by disability status.
(4) Potential Creation of an ESRD Facility Equity Score to Synthesize Results Across Multiple Social Risk Factors
As we describe above, we are considering expanding the disparity methods to include two social risk factors (dual eligibility and race/ethnicity). This approach would improve the comprehensiveness of health equity information provided to facilities. Aggregated results from multiple measures and multiple social risk factors, from the CMS Disparity Methods, in the format of a summary score, can improve the usefulness of the equity results. In working with our contractors, we recently developed an equity summary score for Medicare Advantage contract/plans, the Health Equity Summary Score (HESS), with application to stratified reporting using two social risk factors: Dual eligibility and race and as described in Incentivizing Excellent Care to At-Risk Groups with a Health Equity Summary Score.[218]
The HESS calculates standardized and combined performance scores blended across the two social risk factors. The HESS also combines results of the within-plan (similar to the Within-Facility method) and across-plan method (similar to the Across-Facility method) across multiple performance measures.
We are considering building an ESRD Facility Equity Score, not yet developed, which would be modeled off the HESS but adapted to the context of risk-adjusted facility outcome measures and potentially other ESRD QIP quality measures. We envision that the ESRD Facility Equity Score would synthesize results for a range of measures and using multiple social risk factors, using measures and social risk factors which would be reported to facilities as part of the CMS Disparity Methods. We believe that creation of the ESRD Facility Equity Score has the potential to supplement the overall measure data already reporting on the Care Compare or successor website, by providing easy to interpret information regarding disparities measured within individual facilities and across facilities nationally. A summary score would decrease burden by minimizing the number of measure results provided and providing an overall indicator of equity.
The ESRD Facility Equity Score under consideration would potentially:
- Summarize facility performance across multiple social risk factors (initially dual eligibility and indirectly estimated race and ethnicity, as described above).
- Summarize facility performance across the two disparity methods (that is, the Within-Facility Disparity Method and the Across-Facility Disparity Method) and potentially multiple measures.
Prior to any future public reporting of stratified measure data using indirectly estimated race and ethnicity information, if we determine that an ESRD Facility Equity Score can be feasibly and accurately calculated, we would provide results of the ESRD Facility Equity Score, in confidential facility specific reports which facilities and their QIN-QIOs would be able to download. Any potential future proposal to display the ESRD Facility Equity Score on the Care Compare or successor website would be made through future RFI or rulemaking.
d. Solicitation of Public Comment
We are seeking comment on the possibility of stratifying ESRD QIP measures by dual eligibility and race and ethnicity. We are soliciting public comments on the application of the within-facility or across-facility disparities methods if we were to stratify ESRD QIP measures. We are also seeking comment on the possibility of facility collection of standardized demographic information for the purposes of potential future quality reporting and measure stratification. In addition, we are seeking comment on the potential design of a facility equity score for calculating results across multiple social risk factors and measures, including race and disability. Any data pertaining to these areas that are recommended for collection for measure reporting for a CMS program and any potential public disclosure on Care Compare or successor website would be addressed through a separate and future notice- and-comment rulemaking. We plan to continue working with ASPE, facilities, the public, and other key stakeholders on this important issue to identify policy solutions that achieve the goals of attaining health equity for all patients and minimizing unintended consequences. We look forward to receiving feedback on these topics and note for readers that responses to the RFI will not directly impact payment decisions. We also note our intention for additional RFI or rulemaking on this topic in the future.
Specifically, we are inviting public comment on the following:
Future Potential Stratification of Quality Measure Results
- The possible stratification of facility-specific reports for ESRD QIP measure data by dual-eligibility status, including which measures would be most appropriate for stratification;
- The potential future application of indirect estimation of race and ethnicity information to permit stratification of Start Printed Page 36368measure data for reporting ESRD facility-level disparity results;
- Appropriate privacy safeguards with respect to data produced from the indirect estimation of race and ethnicity to ensure that such data is properly identified if/when it is shared with facilities.
- Ways to address the challenges of defining and collecting, accurate and standardized self-identified demographic information, including information on race and ethnicity, disability, and language preference for the purposes of reporting, measure stratification and other data collection efforts relating to quality.
- Recommendations for other types of readily available data elements for measuring disadvantage and discrimination for the purposes of reporting, measure stratification and other data collection efforts relating to quality, in addition, or in combination with race and ethnicity.
- Recommendations for types of quality measures or measurement domains to prioritize for stratified reporting by dual eligibility, race and ethnicity, and disability.
- Examples of approaches, methods, research, and/or considerations for use of data-driven technologies that do not facilitate exacerbation of health inequities, recognizing that biases may occur in methodology or be encoded in datasets.
Improving Demographic Data Collection
- Experiences of users of certified health IT regarding local adoption of practices for collection of social, psychological, and behavioral data elements, the perceived value of using these data for improving decision-making and care delivery, and the potential challenges and benefits of collecting more granular, structured demographic information, such as the “Race & Ethnicity—CDC” code system.
- The possible collection of a minimum set of social, psychological, and behavioral data elements by ESRD facilities at the time of admission using structured, interoperable electronic data standards, for the purposes of reporting, measure stratification and other data collection efforts relating to quality.
Potential Creation of an ESRD Facility Equity Score To Synthesize Results Across Multiple Social Risk Factors
- The possible creation and confidential reporting of an ESRD Facility Equity Score to synthesize results across multiple social risk factors and disparity measures.
- Interventions ESRD facilities could institute to improve a low facility equity score and how improved demographic data could assist with these efforts.
2. COVID-19 Vaccination Measures Request for Information
a. Background
On January 31, 2020, the Secretary declared a PHE for the U.S. in response to the global outbreak of SARS-CoV-2, a novel (new) coronavirus that causes a disease named “coronavirus disease 2019” (COVID-19).[219] COVID-19 is a contagious respiratory infection [220] that can cause serious illness and death. Older individuals and those with underlying medical conditions are considered to be at higher risk for more serious complications from COVID-19.[221]
As of April 2, 2021, the U.S. reported over 30 million cases of COVID-19 and over 550,000 COVID-19 deaths.[222] Hospitals and health systems saw significant surges of COVID-19 patients as community infection levels increased.[223] From December 2, 2020 through January 30, 2021, more than 100,000 Americans were in the hospital with COVID-19 at the same time.[224]
Evidence indicates that COVID-19 primarily spreads when individuals are in close contact with one another.[225] The virus is typically transmitted through respiratory droplets or small particles created when someone who is infected with the virus coughs, sneezes, sings, talks or breathes.[226] Thus, the CDC advises that infections mainly occur through exposure to respiratory droplets when a person is in close contact with someone who has COVID-19.[227] Although less common, COVID-19 can also spread when individuals are not in close contact if small droplets or particles containing the virus linger in the air after the person who is infected has left the space.[228] Another means of less common transmission is contact with a contaminated surface.[229] According to the CDC, those at greatest risk of infection are persons who have had prolonged, unprotected close contact (that is, within 6 feet for 15 minutes or longer) with an individual with confirmed SARS-CoV-2 infection, regardless of whether the individual has symptoms.[230] Although personal protective equipment (PPE) and other infection-control precautions can reduce the likelihood of transmission in health care settings, COVID-19 can spread between healthcare personnel (HCP) and patients, or from patient to patient given the close contact that may occur during the provision of care.[231] The CDC has emphasized that health care settings can be high-risk places for COVID-19 exposure and transmission.[232]
As part of its national strategy to address COVID-19, the Biden Administration stated that it would work with states and the private sector to execute an aggressive vaccination strategy and outlined a goal of administering 200 million shots in 100 days.[233] After achieving this goal,[234] the Biden Administration announced a new goal to administer at least one COVID-Start Printed Page 3636919 vaccine shot to 70 percent of the U.S. adult population by July 4th, 2021.[235] Although the goal of the U.S. government is to ensure that every American who wants to receive a COVID-19 vaccine can receive one, federal agencies recommended that early vaccination efforts focus on those critical to the PHE response, including HCP providing direct care to patients with COVID-19, and individuals at highest risk for developing severe illness from COVID-19.[236] For example, the CDC's Advisory Committee on Immunization Practices (ACIP) recommended that HCP should be among those individuals prioritized to receive the initial, limited supply of the COVID-19 vaccination, given the potential for transmission in health care settings and the need to preserve health care system capacity.[237] Research suggests most states followed this recommendation,[238] and HCP began receiving the vaccine in mid-December of 2020.[239] Although the vaccination strategy for individuals at highest risk for developing severe illness from COVID-19, including ESRD patients, has varied from state to state,[240] ACIP recommendations indicated that ESRD patients would be offered the COVID-19 vaccine based on their high-risk status as part of phase 1c.[241]
As of June 22, 2021 the CDC reported that over 319 million doses of COVID-19 vaccine had been administered, and approximately 150.4 million people had received a complete vaccination course.[242] President Biden indicated on April 6, 2021 that the U.S. has sufficient vaccine supply to make every adult eligible to receive a vaccine beginning April 19, 2021.[243] Furthermore, on March 25, 2021, the Biden Administration announced a new partnership with dialysis facilities to provide COVID-19 vaccinations directly to people receiving dialysis and HCP in dialysis facilities.[244]
b. COVID-19 Vaccination Coverage Among Healthcare Personnel (HCP) Measure
We believe it is important to incentivize and track HCP vaccination in dialysis facilities through quality measurement in order to protect health care workers, patients, and caregivers, and to help sustain the ability of these facilities to continue serving their communities throughout the PHE and beyond. We recognize the importance of COVID-19 vaccination, and have proposed to include a COVID-19 HCP vaccination measure quality measure in various pay for reporting programs, such as the Inpatient Psychiatric Facility Quality Reporting Program (86 FR 19501 through 19504), the Hospital Inpatient Quality Reporting Program (86 FR 25571 through 25575), and the Skilled Nursing Facility Quality Reporting Program (86 FR 19994 through 19998). We note that there is not a pay for reporting program under the ESRD PPS, however, we believe that the public reporting of vaccination data on Dialysis Facility Compare is important and would help to inform patients of a facility's COVID-19 vaccination rates of HCP. Currently, there is a measure for HCP [245] and another for patient COVID-19 vaccination [246] rates and such measures are currently reported to CDC's National Healthcare Safety Network via ESRD Networks. The two measures track the proportions of a facility's HCP and patient population, respectively, that have been fully vaccinated against COVID-19. Facilities were able to begin weekly COVID-19 vaccination reporting for HCP in December 2020,[247] and were able to begin weekly COVID-19 vaccination reporting for patients in March 2021.[248] Currently, 89 percent of ESRD facilities are reporting HCP vaccination rates and almost 95 percent of ESRD facilities are reporting patient vaccination rates on these measures. We are evaluating options for publicly reporting the data on official CMS datasets that compare the quality of care provided in Medicare-certified dialysis facilities nationwide. We are also exploring the potential future inclusion of a COVID-19 vaccination measure to the ESRD QIP. Therefore, we are seeking public comment on adding a new measure, COVID-19 Vaccination Coverage Among HCP, to the ESRD QIP measure set in the next rulemaking cycle. The measure would assess the proportion of a facility's health care workforce that has been vaccinated against COVID-19.
HCP are at risk of carrying COVID-19 infection to patients, experiencing illness or death as a result of COVID-19 themselves, and transmitting it to their families, friends, and the general public. We believe facilities should track the level of vaccination among their HCP as part of their efforts to assess and reduce the risk of transmission of COVID-19 within their facilities. HCP vaccination can potentially reduce illness that leads to work absence and limit disruptions to care.[249] Data from influenza vaccination Start Printed Page 36370demonstrates that provider uptake of the vaccine is associated with that provider recommending vaccination to patients,[250] and we believe HCP COVID-19 vaccination in dialysis facilities could similarly increase uptake among that patient population. We also believe that publishing the HCP vaccination rates will be helpful to many patients, including those who are at high-risk for developing serious complications from COVID-19, as they choose facilities from which to seek treatment. Under CMS' Meaningful Measures Framework, the COVID-19 measure would address the quality priority of “Promoting Effective Prevention and Treatment of Chronic Disease” through the Meaningful Measures Area of “Preventive Care.”
c. COVID-19 Vaccination Coverage for Patients in End-Stage Renal Disease (ESRD) Facilities Measure
We believe it is important to encourage patient vaccination in dialysis facilities in order to protect health care workers, patients, and caregivers, and to help sustain the ability of these facilities to continue serving their communities throughout the PHE and beyond. COVID-19 can cause outbreaks in ESRD facilities, and may disproportionately affect ESRD patients due to the nature of the treatment and sharing of common spaces.[251] Many patients treated in ESRD facilities have other underlying chronic conditions, and therefore are highly susceptible to illness and disease.[252] Sufficient vaccination coverage among patients in ESRD facilities may reduce transmission of SARS-CoV-2, thereby protecting them from COVID-19 mortality. Therefore, we are seeking public comment on adding new measure, COVID-19 Vaccination Coverage Among Patients, to the ESRD QIP measure set in future rulemaking. The measure would assess the proportion of a facility's patient population that has been vaccinated against COVID-19.
We believe facilities should track the level of vaccination among their patients as part of their efforts to assess and reduce the risk of transmission of COVID-19 within their facilities. We also believe that publishing the vaccination rates will be helpful to many ESRD patients, including those who are at high-risk for developing serious complications from COVID-19, as they choose facilities from which to seek treatment. Under CMS' Meaningful Measures Framework, the COVID-19 measure addresses the quality priority of “Promoting Effective Prevention and Treatment of Chronic Disease” through the Meaningful Measures Area of “Preventive Care.”
d. Review by the Measures Application Partnership and NQF
The COVID-19 HCP vaccination measure and the COVID-19 patient vaccination measure were included on the publicly available “List of Measures under Consideration for December 21, 2020” (MUC List), a list of measures under consideration for use in various Medicare programs.[253] When the Measure Applications Partnership Hospital Workgroup convened on January 11, 2021, it reviewed measures on the MUC List including the two COVID-19 vaccination measures. The Measure Applications Partnership Hospital Workgroup recognized that the proposed measures represent a promising effort to advance measurement for an evolving national pandemic and that it would bring value to the ESRD QIP measure set by providing transparency about an important COVID-19 intervention to help prevent infections in HCP and patients.[254] The Measure Applications Partnership Hospital Workgroup also stated that collecting information on COVID-19 vaccination coverage among HCP and ESRD patients, and providing feedback to facilities, will allow facilities to benchmark coverage rates and improve coverage in their facility. The Measure Applications Partnership Hospital Workgroup further noted that reducing rates of COVID-19 in HCP and ESRD patients may reduce transmission among a patient population that is highly susceptible to illness and disease, and also reduce instances of staff shortages due to illness.[255]
In its preliminary recommendations, the Measure Applications Partnership Hospital Workgroup did not support these two measures for rulemaking, subject to potential for mitigation.[256] To mitigate its concerns, the Measure Applications Partnership Hospital Workgroup believed that both measures needed well-documented evidence, finalized specifications, testing, and NQF endorsement prior to implementation.[257] Subsequently, the Measure Applications Partnership Coordinating Committee met on January 25, 2021, and reviewed the COVID-19 Vaccination Coverage Among HCP measure and the COVID-19 Vaccination Coverage for Patients in ESRD Facilities Measure. In the 2020-2021 Measure Applications Partnership Final Recommendations, Measure Applications Partnership offered conditional support for rulemaking contingent on CMS bringing the measures back to Measure Applications Partnership once the specifications are further refined.[258] The Measure Applications Partnership specifically stated, “the incomplete specifications require immediate mitigation and further development should continue.” [259] The Measure Applications Partnership further noted that the measures would add value to the ESRD QIP measure set by providing visibility into an important intervention to limit COVID-19 infections in HCP and the ESRD patients for whom they provide care.[260] CMS brought both measures back to the Measure Applications Partnership on March 15, 2021 to provide additional information and continue discussing mitigation.
e. Request for Public Comment
In this proposed rule, we would like to seek public comment on potentially adding the two new COVID-19 vaccination measures discussed above, the COVID-19 vaccination measure for HCP and the COVID-19 vaccination measure for patients, to the ESRD QIP measure set.[261]
We are also interested in public comment on data collection, Start Printed Page 36371submission, and reporting for the COVID-19 vaccination measure for HCP and the COVID-19 vaccination measure for patients. For example, we are considering requiring reporting for these measures on an annual basis for the performance period for each calendar year corresponding to the associated payment year, and the reporting period would be January 1 through December 31 annually. Based on the measures currently being developed by the CDC that were submitted to the Measure Applications Partnership, facilities would report the measures through the National Healthcare Safety Network (NHSN) web-based surveillance system. We also seek public comment from stakeholders on other ways to collect data on COVID-19 vaccination rates at dialysis facilities for ESRD QIP purposes and their associated costs and burdens. Given the immediacy of the PHE for COVID-19, as well as the importance of continuing to monitor and make publicly available COVID-19 vaccination rates as the PHE ends, we anticipate rulemaking on this requirement in the CY 2023 rulemaking cycle.
3. Advancing to Digital Quality Measurement and the Use of Fast Healthcare Interoperability Resources (FHIR)
We aim to move fully to digital quality measurement in CMS quality reporting and value-based purchasing programs by 2025. As part of this modernization of our quality measurement enterprise, we are issuing this request for information (RFI). The purpose of this RFI is to gather broad public input solely for planning purposes for our transition to digital quality measurement. Any updates to specific program requirements related to providing data for quality measurement and reporting provisions would be addressed through future rulemaking, as necessary. This RFI contains four parts:
- Background. This part provides information on our quality measurement programs and our goal to move fully to digital quality measurement by 2025. This part also provides a summary of other recent HHS policy developments that are advancing interoperability and could support our move towards full digital quality measurement.
- Definition of Digital Quality Measures (dQMs). This part provides a potential definition for dQMs. Specific requests for input are included in the section.
- Changes Under Consideration to Advance Digital Quality Measurement: Actions in Four Areas to Transition to Digital Quality Measures by 2025. This part introduces four possible steps that would enable transformation of CMS' quality measurement enterprise to be fully digital by 2025. Specific requests for input are included in the section.
- Solicitation of Comments. This part lists all requests for input included in the above sections of this RFI.
a. Background
As required by law, we implemented quality measurement programs and value-based purchasing programs across a broad range of inpatient, outpatient, and post-acute care (PAC) settings, consistent with our mission to improve the quality of health care for Americans through measurement, transparency, and increasingly, value-based purchasing. These quality programs are foundational for incentivizing value-based care, contributing to improvements in health care, enhancing patient outcomes, and informing consumer choice. We aim to move fully to digital quality measurement by 2025. We acknowledge providers within the various care and practice settings covered by our quality programs may be at different stages of readiness, and therefore, the timeline for achieving full digital quality measurement across our quality reporting programs may vary.
We also continue to evolve the Medicare Promoting Interoperability Program that advances the use of certified electronic health record (EHR) technology, from an initial focus on electronic data capture to enhancing information exchange and expanding quality measurement (83 FR 41634). However, reporting quality data via EHRs remains burdensome, and our current approach to quality measurement does not readily incorporate emerging data sources such as patient-reported outcomes (PRO) and patient-generated health data (PGHD).[262] There is a need to streamline our approach to data collection, calculation, and reporting to fully leverage clinical and patient-centered information for measurement, improvement, and learning.
Additionally, advancements in technical standards and regulatory initiatives to improve interoperability of healthcare data are creating an opportunity to significantly improve our quality measurement systems. In May 2020, we finalized interoperability requirements in the CMS Interoperability and Patient Access final rule (85 FR 25510) to support beneficiary access to data held by certain payers. At the same time, the Office of the National Coordinator for Health Information Technology (ONC) finalized policies in the ONC 21st Century Cures Act final rule (85 FR 25642) to advance the interoperability of health IT as defined in section 4003 of the Cures Act, including the “complete access, exchange, and use of all electronically accessible health information.” Closely working with ONC, we collaboratively identified HL7 Fast Healthcare Interoperability Resources (FHIR®) Release 4.0.1 as the standard to support Application Programming Interface (API) policies in both rules. ONC, on behalf of HHS, adopted the HL7 FHIR Release 4.0.1 for APIs and related implementation specifications at 45 CFR 170.215. We believe the FHIR standard has the potential to be a more efficient and modular standard to enable APIs. We also believe this standard enables collaboration and information sharing, which is essential for delivering high-quality care and better outcomes at a lower cost. By aligning technology requirements for payers, health care providers, and health IT developers, HHS can advance-an interoperable health IT infrastructure that ensures providers and patients have access to health data when and where it is needed.
In the ONC 21st Century Cures Act final rule ONC adopted a “Standardized API for Patient and Population Services” certification criterion for health IT that requires the use of the FHIR Release 4 and several implementation specifications. Health IT certified to this criterion will offer single patient and multiple patient services that can be accessed by third party applications (85 FR 25742).[263] The ONC 21st Century Cures Act final rule also requires health IT developers update their certified health IT to support the U.S. Core Data for Interoperability (USCDI) standard.[264] The scope of patient data identified in the USCDI and the data standards that support this data set are expected to evolve over time, starting with data specified in Version 1 of the USCDI. In November 2020, ONC issued an interim final rule with comment period extending the date when health IT developers must make technology meeting updated certification criteria available under the ONC Health IT Start Printed Page 36372Certification Program until December 31, 2022 (85 FR 70064).[265]
The CMS Interoperability and Patient Access final rule (85 FR 25510) and program policies build on the ONC 21st Century Cures Act final rule (85 FR 25642). The CMS Interoperability and Patient Access final rule and policies require certain payers (for example, Medicare Advantage organizations, Medicaid, and CHIP fee for service programs, Medicaid managed care plans, CHIP managed care entities, and Qualified Health Plan [QHP] issuers on the Federally-facilitated Exchanges [FFEs]) to implement and maintain a standards-based Patient Access API using HL7 FHIR Release 4.0.1 to make available certain data to their enrollees and beneficiaries (called “patients” in the CMS interoperability rule). These certain data include data concerning claims and encounters, with the intent to ensure access to their own health care information through third-party software applications. The rule also established new Conditions of Participation for Medicare and Medicaid participating hospitals, psychiatric hospitals, and critical access hospitals (CAHs), requiring them to send electronic notifications to another healthcare facility or community provider or practitioner when a patient is admitted, discharged, or transferred (85 FR 25603). In the CY 2021 Physician Fee Schedule (PFS) final rule (85 FR 84472), we finalized a policy to align the certified EHR technology required for use in the Promoting Interoperability programs and the MIPS Promoting Interoperability performance category with the updates to health IT certification criteria finalized in the ONC 21st Century Cures Act. Under this policy, eligible clinicians, MIPS eligible clinicians, and eligible hospitals and CAHs participating in the Promoting Interoperability Programs, must use technology meeting the updated certification criteria for performance and reporting periods beginning in 2023 (85 FR 84825).
The use of APIs can also reduce long-standing barriers to quality measurement. Currently, health IT developers are required to implement individual measure specifications within their health IT product. The health IT developer must also accommodate how that product connects with the unique variety of systems within a specific care setting.[266] This may be further complicated by systems which integrate a wide range of data schemas. This process is burdensome and costly, and it is difficult to reliably obtain high quality data across systems. As health IT developers map their health IT data to the FHIR standard and related implementation specifications, APIs can enable these data to be easily accessible for measurement or other use cases, such as care coordination, clinical decision support, and supporting patient access.
We believe the emerging data standardization and interoperability enabled by APIs will support the transition to full digital quality measurement by 2025, and are committed to exploring and seeking input on potential solutions for the transition to digital quality measurement as described in this RFI.
b. Definition of Digital Quality Measures
In this section we seek to refine the definition of digital quality measures (dQMs) to further operationalize our objective of fully transitioning to dQMs by 2025. We previously noted dQMs use “sources of health information that are captured and can be transmitted electronically and via interoperable systems.” (85 FR 84845). In this RFI, we seek input on future elaboration that would define a dQM as a software that processes digital data to produce a measure score or measure scores. Data sources for dQMs may include administrative systems, electronically submitted clinical assessment data, case management systems, EHRs, instruments (for example, medical devices and wearable devices), patient portals or applications (for example, for collection of patient-generated health data), health information exchanges (HIEs) or registries, and other sources. We also note that dQMs are intended to improve the patient experience including quality of care, improve the health of populations, and/or reduce costs.
We discuss one potential approach to developing dQM software in section IV.G.3.c of this proposed rule. In this section, we are seeking comment on the potential definition of dQMs in this RFI.
We also seek feedback on how leveraging advances in technology (for example, FHIR APIs) to access and electronically transmit interoperable data for dQMs could reinforce other activities to support quality measurement and improvement (for example, the aggregation of data across multiple data sources, rapid-cycle feedback, and alignment of programmatic requirements).
The transition to dQMs relies on advances in data standardization and interoperability. As providers and payers work to implement the required advances in interoperability over the next several years, we will continue to support reporting of eCQMs through CMS quality reporting programs and through the Promoting Interoperability programs.[267] These fully digital measures continue to be important drivers of interoperability advancement and learning. CMS is currently re-specifying and testing these measures to use FHIR rather than the currently adopted Quality Data Model (QDM) in anticipation of the wider use of FHIR standards. CMS intends to apply significant components of the output of this work, such as the re-specified measure logic and the learning done through measure testing with FHIR APIs, to define and build future dQMs that take advantage of the expansion of standardized, interoperable data.
c. Changes Under Consideration To Advance Digital Quality Measurement: Potential Actions in Four Areas To Transition to Digital Quality Measures by 2025
Building on the advances in interoperability and learning from testing of FHIR-converted eCQMs, we aim to move fully to dQMs, originating from sources of health information that are captured and can be transmitted electronically via interoperable systems, by 2025.
To enable this transformation, we are considering further modernizing the quality measurement enterprise in four major ways: (1) Leverage and advance standards for digital data and obtain all EHR data required for quality measures via provider FHIR-based APIs; (2) redesign our quality measures to be self-contained tools; (3) better support data aggregation; and (4) work to align measure requirements across our reporting programs, other federal programs and agencies, and the private sector where appropriate.
These changes would enable us to collect and utilize more timely, actionable, and standardized data from diverse sources and care settings to improve the scope and quality of data Start Printed Page 36373used in quality reporting and payment programs, reduce quality reporting burden, and make results available to stakeholders in a rapid-cycle fashion. Data collection and reporting efforts would become more efficient, supported by advances in interoperability and data standardization. Aggregation of data from multiple sources would allow assessments of costs and outcomes to be measured across multiple care settings for an individual patient or clinical conditions. We believe that aggregating data for measurement can incorporate a more holistic assessment of an individual's health and healthcare and produce the rich set of data needed to enable patients and caregivers to make informed decisions by combining data from multiple sources (for example, patient reported data, EHR data, and claims data) for measurement.
Perhaps most importantly, these steps would help us deliver on the full promise of quality measurement and drive us toward a learning health system that transforms healthcare quality, safety, and coordination and effectively measures and achieves value-based care. The shift from a static to a learning health system hinges on the interoperability of healthcare data, and the use of standardized data. dQMs would leverage this interoperability to deliver on the promise of a learning health system wherein standards-based data sharing and analysis, rapid-cycle feedback, and quality measurement and incentives are aligned for continuous improvement in patient-centered care. Similarly, standardized, interoperable data used for measurement can also be used for other use cases, such as clinical decision support and care coordination and care decision support, which impacts health care and care quality.
We are requesting comments on four potential future actions that would enable transformation to a fully digital quality measurement enterprise by 2025.
(1) Leveraging and Advancing Standards for Digital Data and Obtaining All EHR Data Required for Quality Measures via Provider FHIR-Based APIs
We are considering targeting the data required for our quality measures that utilize EHR data to be data retrieved via FHIR-based APIs based on standardized, interoperable data. Utilizing standardized data for EHR-based measurement (based on FHIR and associated implementation guides) and aligning where possible with interoperability requirements can eliminate the data collection burden providers currently experience with required chart-abstracted quality measures and reduce the burden of reporting digital quality measure results. We can fully leverage this advance to adapt eCQMs and expand to other dQMs through the adoption of interoperable standards across other digital data sources. We are considering methods and approaches to leverage the interoperability data requirements for APIs set by the ONC 21st Century Cures Act final rule for certified health technology to support modernization of CMS quality measure reporting. As discussed previously, these requirements will be included in certified technology in future years (85 FR 84825), including availability of data included in the USCDI via standards-based APIs, and CMS will require clinicians and hospitals participating in MIPS and the Promoting Interoperability Programs, respectively, to transition to use of certified technology updated consistent with the 2015 Cures Edition Update (85 FR 84825).
Digital data used for measurement could expand beyond data captured in traditional clinical settings, administrative claims data, and EHRs. Many important data sources are not currently captured digitally, such as survey and PGHD. We intend to work to innovate and broaden the digital data used across the quality measurement enterprise beyond the clinical EHR and administrative claims. Agreed upon standards for these data, and associated implementation guides will be important for interoperability and quality measurement. We will consider developing clear guidelines and requirements for these digital data that align with interoperability requirements, for example, expressing in standards, exposing via APIs, and incentivizing technologies that innovate data capture and interoperability.
High quality data are also essential for reliable and valid measurement. Hence, in implementing the shift to capture all clinical EHR data via FHIR-based APIs, we would support efforts to strengthen and test the quality of the data obtained through FHIR-based APIs for quality measurement. We currently conduct audits of electronic data with functions including checks for data completeness and data accuracy, confirmation of proper data formatting, alignment with standards, and appropriate data cleaning. These functions would continue and be applied to dQMs and further expanded to automate the manual validation of the data compared to the original data source (for example, the medical record) where possible. Analytic advancements such as natural language processing, big data analytics, and artificial intelligence, can support this evolution. These techniques can be applied to validating observed patterns in data and inferences or conclusions drawn from associations, as data are received, to ensure high quality data are used for measurement.
We are seeking feedback on the goal of aligning data needed for quality measurement with interoperability requirements and the strengths and limitations of this approach. We are also seeking feedback on the importance of and approaches to supporting inclusion of PGHD and other currently non-standardized data. We also welcome comment on approaches for testing data quality and validity.
(2) Redesigning Quality Measures To Be Self-Contained Tools
We are considering approaches for deploying quality measures to take advantage of standardized data and interoperability requirements that have expanded flexibility and functionality compared to CMS' current eCQMs. We are considering defining and developing dQM software as end-to-end measure calculation solutions that retrieve data from primarily FHIR resources maintained by providers, payers, CMS, and others; calculate measure score(s); and produce reports. In general, we believe to optimize the use of standardized and interoperable data, the software solution for dQMs should do the following:
- Have the flexibility to support calculation of single or multiple quality measure(s).
- Perform three functions: (i) Obtain data via automated queries from a broad set of digital data sources (initially from EHRs, and in the future from claims, PRO, and PGHD); (ii) calculate the measure score according to measure logic; and (iii) generate measure score report(s).
- Be compatible with any data source systems that implement standard interoperability requirements.
- Exist separately from digital data source(s) and respect the limitations of the functionality of those data sources.
- Be tested and updated independently of the data source systems.
- Operate in accordance with health information protection requirements under applicable laws and comply with governance functions for health information exchange.
- Have the flexibility to be deployed by individual health systems, health IT vendors, data aggregators, and health plans; and/or run by CMS depending on the program and measure needs and specifications.Start Printed Page 36374
- Be designed to enable easy installation for supplemental uses by medical professionals and other non-technical end-users, such as local calculation of quality measure scores or quality improvement.
- Have the flexibility to employ current and evolving advanced analytic approaches such as natural language processing.
- Be designed to support pro-competitive practices for development, maintenance, and implementation and diffusion of quality measurement and related quality improvement and clinical tools through for example the use of open-source core architecture.
We seek comment on these suggested functionalities and other additional functionalities that quality measure tools should ideally have particularly in the context of the pending availability of standardized and interoperable data (for example, standardized EHR data available via FHIR-based APIs).
We are also interested whether and how this more open, agile strategy may facilitate broader engagement in quality measure development, the use of tools developed for measurement for local quality improvement, and/or the application of quality tools for related purposes such as public health or research.
(3) Building a Pathway to Data Aggregation in Support of Quality Measurement
Using multiple sources of collected data to inform measurement would reduce data fragmentation (or, different pieces of data regarding a single patient stored in many different places). Additionally, we are also considering expanding and establishing policies and processes for data aggregation and measure calculation by third-party aggregators that include, but are not limited to, HIEs and clinical registries. Qualified Clinical Data Registries and Qualified Registries that report quality measures for eligible clinicians in the Merit-based Incentive Payment System (MIPS) program are potential examples [268] at 42 CFR 414.1440(b)(2)(iv) and (v) and § 414.1440(c)(2)(iii) and (iv) and can also support measure reporting. We are considering establishing similar policies for third-party aggregators to maintain the integrity of our measure reporting process and to encourage market innovation.
We seek feedback on aggregation of data from multiple sources being used to inform measurement. We also seek feedback on the role data aggregators can and should play in CMS quality measure reporting in collaboration with providers, and how we can best facilitate and enable aggregation.
(4) Potential Future Alignment of Measures Across Reporting Programs, Federal and State Agencies, and the Private Sector
We are committed to using policy levers and working with stakeholders to solve the issue of interoperable data exchange and to transition to full digital quality measurement. We are considering the future potential development and multi-staged implementation of a common portfolio of dQMs across our regulated programs, agencies, and private payers. This common portfolio would require alignment of: (1) Measure concepts and specifications including narrative statements, measure logic, and value sets, and (2) the individual data elements used to build these measure specifications and calculate the measure logic. Further, the required data elements would be limited to standardized, interoperable data elements to the fullest extent possible; hence, part of the alignment strategy will be the consideration and advancement of data standards and implementation guides for key data elements. We would coordinate closely with quality measure developers, federal and state agencies, and private payers to develop and to maintain a cohesive dQM portfolio that meets our programmatic requirements and that fully aligns across federal and state agencies and payers to the extent possible.
We intend for this coordination to be ongoing and allow for continuous refinement to ensure quality measures remain aligned with evolving healthcare practices and priorities (for example, PROs, disparities, care coordination), and track with the transformation of data collection, alignment with health IT module updates including capabilities and standards adopted by ONC (for example, standards to enable APIs). This coordination would build on the principles outlined in HHS' National Health Quality Roadmap.[269] It would focus on the quality domains of safety, timeliness, efficiency, effectiveness, equitability, and patient-centeredness. It would leverage several existing federal and public-private efforts including our Meaningful Measures 2.0 Framework; the Federal Electronic Health Record Modernization (DoD/VA); the Agency for Healthcare Research and Quality's Clinical Decision Support Initiative; the Centers for Disease Control and Prevention's Adapting Clinical Guidelines for the Digital Age initiative; the Core Quality Measure Collaborative, which convenes stakeholders from America's Health Insurance Plans (AHIP), CMS, NQF, provider organizations, private payers, and consumers and develops consensus on quality measures for provider specialties; and the NQF-convened Measure Applications Partnership, which recommends measures for use in public payment and reporting programs. We would coordinate with HL7's ongoing work to advance FHIR resources in critical areas to support patient care and measurement such as social determinants of health. Through this coordination, we would identify which existing measures could be used or evolved to be used as dQMs, in recognition of current healthcare practice and priorities.
This multi-stakeholder, joint federal and industry, made possible and enabled by the pending advances towards true interoperability, would yield a significantly improved quality measurement enterprise. The success of the dQM portfolio would be enhanced by the degree to which the measures achieve our programmatic requirements for measures as well as the requirements of other agencies and payers.
We seek feedback on initial priority areas for the dQM portfolio given evolving interoperability requirements (for example, measurement areas, measure requirements, tools, and data standards). We also seek to identify opportunities to collaborate with other federal agencies, states, and the private sector to adopt standards and technology-driven solutions to address our quality measurement priorities across sectors.
d. Solicitation of Comments
As noted previously, we seek input on the future development of the following:
Definition of Digital Quality Measures: We are seeking feedback on the following as described in section IV.G.3.c.(2):
++ Do you have feedback on the dQM definition?
++ Does this approach to defining and deploying dQMs to interface with FHIR-based APIs seem promising? We Start Printed Page 36375also welcome more specific comments on the attributes or functions to support such an approach of deploying dQMs.
- Changes Under Consideration to Advance Digital Quality Measurement: Actions in Four Areas to Transition to Digital Quality Measures by 2025
++ We are seeking feedback on the following as described in section IV.G.3.c.(1) of this proposed rule:
—Do you agree with the goal of aligning data needed for quality measurement with that required for interoperability? What are the strengths and limitations of this approach?
—How important is a data standardization approach that also supports inclusion of PGHD and other currently non-standardized data?
—What are possible approaches for testing data quality and validity?
++ We are seeking feedback on the following as described in section IV.G.3.c.(2) of this proposed rule:
—What functionalities, described in section IV.G.3.c.(2) of this proposed rule or others, should quality measure tools ideally have in the context of the pending availability of standardized and interoperable data (for example, standardized EHR data available via FHIR-based APIs)?
—How would this more open, agile strategy for end-to-end measure calculation facilitate broader engagement in quality measure development, the use of tools developed for measurement for local quality improvement, and/or the application of quality tools for related purposes such as public health or research?
++ We seek feedback on the following as described in section IV.G.3.c.(3) of this proposed rule:
—Do you have feedback on policy considerations for aggregation of data from multiple sources being used to inform measurement?
—Do you have feedback on the role data aggregators can and should play in CMS quality measure reporting in collaboration with providers? How can CMS best facilitate and enable aggregation?
++ We seek feedback on the following as described in section IV.G.3.c.(4) of this proposed rule:
—What are initial priority areas for the dQM portfolio (for example, measurement areas, measure requirements, tools)?
—We also seek to identify opportunities to collaborate with other federal agencies, states, and the private sector to adopt standards and technology-driven solutions to address our quality measurement priorities and across sectors.
We plan to continue working with other agencies and stakeholders to coordinate and to inform any potential transition to dQMs by 2025. While we will not be responding to specific comments submitted in response to this RFI in the CY 2022 ESRD PPS final rule, we will actively consider all input as we develop future regulatory proposals or future subregulatory policy guidance. Any updates to specific program requirements related to quality measurement and reporting provisions would be addressed through separate and future notice-and-comment rulemaking, as necessary.
V. End-Stage Renal Disease Treatment Choices (ETC) Model
A. Background
1. Overview of the ETC Model
As described in the Specialty Care Models final rule (85 FR 61114), beneficiaries with ESRD are among the most medically fragile and high-cost populations served by the Medicare program. ESRD Beneficiaries require dialysis or kidney transplantation to survive, and the majority of ESRD Beneficiaries receiving dialysis receive hemodialysis in an ESRD facility. However, as described in the Specialty Care Models final rule, alternative renal replacement modalities to in-center hemodialysis, including home dialysis and kidney transplantation, are associated with improved clinical outcomes, better quality of life, and lower costs than in-center hemodialysis (85 FR 61264).
Section 1115A of the Act authorizes the Innovation Center to test innovative payment and service delivery models expected to reduce Medicare, Medicaid, and CHIP expenditures while preserving or enhancing the quality of care furnished to such programs' beneficiaries. The purpose of the ETC Model is to test the effectiveness of adjusting certain Medicare payments to ESRD facilities and Managing Clinicians to encourage greater utilization of home dialysis and kidney transplantation, support beneficiary modality choice, reduce Medicare expenditures, and preserve or enhance the quality of care.
The ETC Model is a mandatory payment model, as we seek to test the effect of payment incentives on availability and choice of treatment modality among a diverse group of providers and suppliers. ESRD facilities and Managing Clinicians are selected as ETC Participants based on their location in Selected Geographic Areas—a set of 30 percent of Hospital Referral Regions (HRRs) that have been randomly selected to be included in the ETC Model, as well as HRRs with at least 20 percent of component ZIP codes [270] located in Maryland. CMS excludes all U.S. Territories from the Selected Geographic Areas.
Under the ETC Model, ETC Participants are subject to two payment adjustments. The first is the Home Dialysis Payment Adjustment (HDPA), which is an upward adjustment on certain payments made to participating ESRD facilities under the ESRD PPS on home dialysis claims, and an upward adjustment to the MCP paid to participating Managing Clinicians on home dialysis-related claims. The HDPA applies to claims with claim service dates beginning in January 1, 2021, and ending on December 31, 2023.
The second payment adjustment under the ETC Model is the Performance Payment Adjustment (PPA). For the PPA, we assess ETC Participants' home dialysis rate and transplant rate during a Measurement Year (MY), which includes 12 months of performance data. Each MY overlaps with the previous MY, if any, and the subsequent MY, if any, for a period of 6 months. Each MY has a corresponding PPA Period—a 6-month period which begins 6 months after the conclusion of the MY. We adjust certain payments for ETC Participants during the PPA Period based on the ETC Participant's home dialysis rate and transplant rate, calculated as the sum of the transplant waitlist rate and the living donor transplant rate, during the corresponding MY. Based on an ETC Participant's achievement in relation to benchmarks based on the home dialysis rate and transplant rate observed in Comparison Geographic Areas during the Benchmark Year, and the ETC Participant's improvement in relation to its own home dialysis rate and transplant rate during the Benchmark Year, we make an upward or downward adjustment to certain payments to the ETC Participant. The magnitude of the positive and negative PPAs for ETC Participants increases over the course of the ETC Model. These PPAs apply to claims with claim service dates beginning July 1, 2022, and ending June 30, 2027.
2. Summary of Proposed Changes to the ETC Model
In this proposed rule, we are proposing a number of policy changes to the ETC Model beginning for the third Measurement Year (MY3) of the Model, which begins January 1, 2022. We are proposing changes to the methodology Start Printed Page 36376for attributing Pre-emptive LDT Beneficiaries to Managing Clinicians to better reflect the care relationship between beneficiaries who receive pre-emptive LDT transplants and the Managing Clinicians who provide their care. We are also proposing to include nocturnal in-center dialysis in the numerator of the home dialysis rate calculation for ESRD facilities not owned in whole or in part by an LDO as well as Managing Clinicians, to incentivize additional alternative renal replacement modalities. In addition, we are proposing to exclude beneficiaries who are diagnosed with and receiving treatment with chemotherapy or radiation for vital solid organ cancers from the transplant rate to align with common transplant center requirements.
We are proposing to modify the PPA achievement benchmarking methodology to increase achievement benchmarks by 10 percent above rates observed in Comparison Geographic Areas every two MYs, beginning for MY3 (2022). We are proposing to stratify PPA achievement benchmarks based on the proportion of attributed beneficiaries who are dually-eligible for Medicare and Medicaid or receive the Low-Income Subsidy during the MY, and to introduce the Health Equity Incentive to the PPA improvement scoring methodology, both in an effort to encourage ETC Participants to address disparities in renal replacement modality choice among beneficiaries with lower socioeconomic status. We are proposing to modify the PPA improvement benchmarking and scoring methodology to ensure an ETC Participant can receive an improvement score even if its home dialysis rate or transplant rate was zero during the relevant Benchmark Year.
We are proposing to add processes and requirements for CMS to share certain model data with ETC Participants. We are also proposing additional programmatic waivers as necessary solely for purposes of allowing Managing Clinicians who are ETC participants to furnish kidney disease patient education services via telehealth under the ETC Model. In addition, we propose to permit Managing Clinicians who are ETC Participants to reduce or waive beneficiary coinsurance for kidney disease patient education services, subject to certain requirements. CMS expects that the proposed changes would continue to promote the larger goals of increased renal replacement modality choice and are based on many of the issues we laid out in the Specialty Care Models final rule as issues for which CMS was considering further rulemaking, including updating benchmarks for ETC Participants and adjusting model parameters based on our implementation experience.
3. Impact of Proposed Changes on the ETC Model Evaluation
As we described in the Specialty Care Models final rule, an evaluation of the ETC Model will be conducted in accordance with section 1115A(b)(4) of the Act, which requires the Secretary to evaluate each model tested by the Innovation Center. We noted that we believe an independent evaluation of the Model is necessary to understand the impacts of the Model on quality of care and Medicare program expenditures (85 FR 61345).
We propose to update the evaluation plan presented in the Specialty Care Models final rule to account for all the policies proposed in this rule, if finalized. However, changes in the construction of the PPA, if finalized, would have no impact on the evaluation approach to analyzing the final PPA values. This is because the evaluation plan already includes a consideration of the final PPA values, rather than an evaluation of each step in the PPA calculation. However, we expect to conduct subgroup analyses in the evaluation to determine the effect of the proposed Health Equity Incentive, if finalized, in reducing health disparities among beneficiaries with lower socioeconomic status.
As part of the detailed economic analysis included in section IX.B.4 of this proposed rule, the transplant waitlist benchmarks were annually inflated by approximately 3-percentage points growth. This was a change from the Specialty Care Models final rule (85 FR 61352), where the waitlist benchmarks were annually inflated by approximately 2-percentage points growth observed during years 2017 through 2019 to project rates of growth. By increasing the expected effect to a 3-percentage point change, we improve our ability to detect such an effect at the ETC Model's current size. In the Specialty Care Models final rule, we stated that to detect a 2-percentage point increase in the transplant waitlist rate, we would need 30 percent of the 306 HRRs in order to detect an effect of this size with 80 percent power and an alpha of 0.05. Further, we stated that a model of this size would be large enough to detect a one and one-half percentage point change in the home dialysis rate (85 FR 61280). We clarify that our unadjusted power calculations show that the model requires 30 percent of the 306 HRRs to detect the one and one-half percentage point change in the home dialysis rate with 80 percent power and an alpha of 0.05. Given the updated expectation that the transplant waitlist rate is likely to increase by 3-percentage points as a result of the ETC Model, the power analysis shows the evaluation would also have sufficient sample size to detect, as statistically significant, a 3-percentage point change in the transplant waitlist rate with 80 percent power and an alpha of 0.05.
B. Provisions of the Proposed Rule
1. Technical Clarifications
For ESRD facilities that are ETC Participants, the ETC Model makes certain upward and downward adjustments to the Adjusted ESRD PPS per Treatment Base Rate for certain dialysis claims via the Home Dialysis Payment Adjustment (HDPA) and the Performance Payment Adjustment (PPA). The term “Adjusted ESRD PPS per Treatment Base Rate” is defined at 42 CFR 512.310 as the per-treatment payment amount as defined in § 413.230 of this chapter, including patient-level adjustments and facility-level adjustments, and excluding any applicable training adjustment, add-on payment amount, outlier payment amount, TDAPA amount, and TPNIES amount. In this proposed rule, we are clarifying the claims subject to adjustment under the ETC Model. Specifically, as § 413.230 is specific to the calculation of payment amounts under the ESRD PPS, we clarify that the HDPA and PPA do not apply to claims from ESRD facilities that are not paid under ESRD PPS and are instead paid through other Medicare payment systems.
We are also updating the name of one of the sources of data used throughout the ETC Model. In the Specialty Care Models final rule, we specify that one source of data for the ETC Model is CROWNWeb, a data management system that CMS uses to collect data from ESRD facilities (85 FR 61317). Since publication, CMS has replaced CROWNWeb with the End Stage Renal Disease Quality Reporting System (EQRS). As such, we will refer to CROWNWeb for data that was generated before the change to EQRS, which CMS began using in 2020, and EQRS for data that was generated after the change to EQRS.
2. Performance Payment Adjustment (PPA) Beneficiary Attribution for Living Kidney Donor Transplants
In the Specialty Care Models final rule, we established that beneficiaries are attributed to Managing Clinicians for the purposes of calculating the home Start Printed Page 36377dialysis rate and transplant rate (85 FR 61297). For the home dialysis rate and the transplant waitlist and living donor kidney transplant portions of the transplant rate, as described in 42 CFR 512.360(c)(2)(i), an ESRD Beneficiary is generally attributed to the Managing Clinician with the earliest monthly capitation payment (MCP) claim billed during the month. If more than one Managing Clinician submits a claim for the MCP furnished to a single ESRD Beneficiary with the same earliest claim service date at the claim line through date for the month, the ESRD Beneficiary is randomly attributed to one of these Managing Clinicians.
However, a beneficiary who receives a pre-emptive living donor transplant (Pre-emptive LDT Beneficiary) is not on dialysis and therefore cannot be attributed to a Managing Clinician using an MCP claim. As a result, under § 512.360(c)(2)(ii), a Pre-emptive LDT Beneficiary is generally attributed to the Managing Clinician with whom the Pre-emptive LDT Beneficiary had the most claims between the start of the MY and the month of the transplant. If no Managing Clinician has had the plurality of claims for a given Pre-emptive LDT Beneficiary such that multiple Managing Clinicians each had the same number of claims for that beneficiary during the MY, the Pre-emptive LDT Beneficiary is attributed to the Managing Clinician associated with the latest claim service date during the MY up to and including the month of the transplant, as described in § 512.360(c)(2)(ii)(A). If no Managing Clinician had the plurality of claims for a given Pre-emptive LDT Beneficiary such that multiple Managing Clinicians each had the same number of services for that beneficiary during the MY, and more than one of those Managing Clinicians had the latest claim service date during the MY up to and including the month of the transplant, the Pre-emptive LDT Beneficiary is randomly attributed to one of these Managing Clinicians, as described in § 512.360(c)(2)(ii)(B).
Upon further review of the beneficiary attribution methodology for living donor kidney transplants, we realized that an unintended consequence of the current attribution methodology is that Pre-emptive LDT Beneficiaries may be attributed to the nephrologist who manages their transplant, not the Managing Clinician who has seen them through the living donor transplant process. To avoid this effect, CMS believes it is necessary to update the attribution methodology for Pre-emptive LDT Beneficiaries. Living donor transplants are relatively rare events that require nephrologist support over time in order to inform beneficiaries of their transplant options and to assist them in finding a living donor. However, the current Pre-emptive LDT Beneficiary attribution methodology is based on visits from the beginning of a MY. As a result, if a Pre-emptive LDT Beneficiary has a transplant early in a MY, the beneficiary may be attributed to a transplant nephrologist who may have had only a single visit with the beneficiary, rather than the Managing Clinician who oversaw the largest share of the care that led to the beneficiary receiving the living donor transplant.
As a result, we propose to update the attribution methodology for Pre-emptive LDT Beneficiaries to Managing Clinicians, beginning for MY3, in new provisions at § 512.360(c)(2)(iii). Rather than attributing a Pre-emptive LDT Beneficiary to the Managing Clinician with the plurality of claims from the start of the MY and the month of the transplant, beginning for MY3, we propose to attribute Pre-emptive LDT Beneficiaries to the Managing Clinician with whom the beneficiary has had the most claims during the 365 days prior to the transplant date. Further, we propose that if no Managing Clinician has had the most claims for the Pre-emptive LDT Beneficiary such that multiple Managing Clinicians each had the same number of claims for that beneficiary in the 365 days preceding the date of the transplant, the Pre-emptive LDT Beneficiary would be attributed to the Managing Clinician associated with the latest claim service date at the claim line through date during the 365 days preceding the date of the transplant. We propose that if more than one of those Managing Clinicians had the latest claim service date at the claim line through date during the 365 days preceding the date of the transplant, the Pre-emptive LDT Beneficiary would be randomly attributed to one of these Managing Clinicians. We propose that the Pre-emptive LDT Beneficiary would be considered eligible for attribution to a Managing Clinician under this proposed new § 512.360(c)(2)(iii) if the Pre-emptive LDT Beneficiary has at least 1 eligible-month during the 12-month period that includes the month of the transplant and the 11 months prior to the transplant month. We propose that an eligible month would refer to a month during which the Pre-emptive LDT Beneficiary not does not meet exclusion criteria in § 512.360(b). CMS is proposing changes for Pre-emptive LDT Beneficiary attribution to Managing Clinicians in order to identify and attribute Pre-emptive LDT Beneficiaries to the Managing Clinician who assisted the Beneficiary through the living donor transplant process. We seek comment on these proposed changes for Pre-emptive LDT Beneficiary attribution to Managing Clinicians beginning for MY3 in proposed new § 512.360(c)(2)(iii).
3. PPA Home Dialysis Rate
a. Background on Home Dialysis Rate Calculation
A primary goal of the ETC Model is to support beneficiary modality choice by encouraging ETC Participants to support beneficiaries in selecting alternatives to in-center dialysis. Under 42 CFR 512.365(b), CMS includes in-center self-dialysis treatment beneficiary years in the numerator of the home dialysis rate. Specifically, the home dialysis rate for both Managing Clinicians and ESRD facilities is calculated as the number of dialysis treatment beneficiary years during the MY in which attributed beneficiaries received dialysis at home, plus one half of the total number of dialysis treatment beneficiary years during the MY in which the attributed beneficiaries received self-dialysis in center. As described in the Specialty Care Models final rule, we included self-dialysis in the home dialysis rate calculation because we believe in-center self-dialysis may provide a gradual transition from in-center to home dialysis, and provide beneficiaries with the time needed to get comfortable conducting dialysis by themselves, under medical supervision (85 FR 61306).
The denominator for the home dialysis rate is the total dialysis treatment beneficiary years for attributed ESRD beneficiaries during the MY, as described in §§ 512.365(b)(1)(i) and 512.365(b)(2)(i). This includes the months during which attributed beneficiaries received maintenance dialysis at home or in an ESRD facility.
b. Nocturnal Dialysis
Nocturnal in-center dialysis is a form of in-center dialysis conducted overnight for extended hours while the beneficiary is asleep. This dialysis is longer and slower than traditional in-center dialysis, can take more than 5 hours per treatment, and can be performed 3 to 7 days a week. As this type of in-center dialysis is conducted overnight, it allows the beneficiary more time and flexibility to have a continuous job, as well as a social and family life.[271]
Start Printed Page 36378Dialysis conducted at a slower rate over a longer period of time is also associated with positive health impacts in comparison to traditional dialysis, including improved blood pressure control, better phosphate control, better management of anemia and bone and mineral metabolism, improved cardiovascular disease, increases in urea reduction ratio, and better beneficiary quality of life measures.[272 273 274 275 276]
In addition to the clinical benefits, nocturnal in-center dialysis also provides an alternative to traditional in-center dialysis for those beneficiaries for whom home dialysis is not an option due to limited financial resources, housing insecurity, lack of social support, or personal preference. For example, a beneficiary experiencing housing insecurity may be unable to dialyze at home due to inability to receive and store home dialysis materials. However, that beneficiary could receive nocturnal in-center dialysis, thereby receiving the clinical benefits of a longer, slower dialysis process and the flexibility associated with not having to receive traditional in-center dialysis during the day.[277 278]
While nocturnal in-center dialysis offers some of the same clinical and quality of life benefits as home dialysis in comparison to traditional in-center dialysis, use of nocturnal in-center dialysis is rare. Based on analyses described in section IX.B.4.a.(4) of this proposed rule, less than 1 percent of beneficiaries eligible for attribution to ETC Participants were receiving self-dialysis or nocturnal in-center dialysis in 2019. Potential limitations to nocturnal in-center dialysis utilization include supply factors. At present, few ESRD facilities offer nocturnal dialysis; in 2019, approximately 1 percent of ESRD facilities furnished nocturnal in-center dialysis based on our analysis of claims data. ESRD facilities may face staffing challenges to initiating a nocturnal dialysis program. Potential limitations to nocturnal in-center dialysis also include demand factors: beneficiaries may be unaware of nocturnal in-center dialysis, or may be averse to sleeping at an ESRD facility or experience difficulty sleeping while receiving dialysis.[279]
c. Proposed Inclusion of Nocturnal In-Center Dialysis in Home Dialysis Rate
We propose to modify the home dialysis rate calculation, for ETC Participants that are either ESRD facilities not owned in whole or in part by an LDO or Managing Clinicians, to include nocturnal in-center dialysis in the numerator beginning for MY3. As described previously in this section of the proposed rule, we believe this modality allows beneficiaries to continue to receive maintenance dialysis in an ESRD facility under medical supervision, but at a time of day that is more convenient for them, and in a manner that is associated with improved health outcomes. In particular, we believe that including nocturnal in-center dialysis in the home dialysis rate may improve access to alternative renal replacement modalities for beneficiaries who are unable to dialyze at home.
In addition to promoting access to the benefits of additional alternative renal replacement modalities for ESRD Beneficiaries who may not be able to dialyze at home, we believe that including nocturnal in-center dialysis in the calculation of the home dialysis rate offers an additional pathway to success for ETC Participants with more limited resources. As described in the Specialty Care Models final rule, we received comments that some ESRD facilities, particularly independent ESRD facilities or ESRD facilities owned by small dialysis organizations, may be unable to develop and maintain a home dialysis program (85 FR 61322 through 61324). Operating a home dialysis program requires specialized staff, as well as upfront investment in additional equipment and certification. Establishing a nocturnal in-center dialysis program does not require additional equipment or certification, and may be more feasible for independent ESRD facilities or ESRD facilities owned by small dialysis organizations, and by extension, the Managing Clinicians who serve their patients.
We considered including nocturnal in-center dialysis in the numerator of the home dialysis rate for ESRD facilities owned in whole or in part by LDOs as well. However, we do not believe that ESRD facilities owned in whole or in part by LDOs face the same resource constraints in establishing a home dialysis program as independent ESRD facilities or ESRD facilities owned by small dialysis organizations. ESRD facilities owned in whole or in part by LDOs may be more likely to have access to a home dialysis program, either in the ESRD facility itself or within the network of facilities owned by the same parent company in that facility's aggregation group. ESRD facilities owned in whole or in part by LDOs may also have greater access to the upfront capital necessary to establish a home dialysis program if they do not already have, or have access to, a home dialysis program.
At present, there is not a single definition of what qualifies a legal entity that owns ESRD facilities as an LDO. In general, definitions of LDO focus on the number of ESRD facilities owned by the legal entity. Other Innovation Center models have used such definitions: The Comprehensive ESRD Care (CEC) Model defined an LDO as a legal entity owning 200 or more ESRD facilities; the Kidney Care Choices (KCC) Model defines an LDO as a legal entity owning 35 or more ESRD facilities. Outside of Innovation Center models, definitions used by academic researchers vary significantly. For example, in 2015 the United States Renal Data System (USRDS), a national data registry funded by the National Institutes of Health (NIH), defined an LDO as a dialysis organization one that owns and operates 200 or more ESRD facilities.[280] Other academic research Start Printed Page 36379has employed thresholds as low as owning 20 or more ESRD facilities and as high as owning 1,000 or more ESRD facilities to consider a legal entity an LDO.[281 282] Other definitions do not focus on the number of ESRD facilities owned, but on the relative size of dialysis organizations in the market, or rather, the individual dialysis organizations themselves. For example, in its March 2021 report to Congress, the Medicare Payment Advisory Commission (MedPAC) refers to the two largest dialysis organizations in the country as LDOs based on their relative share of ESRD facilities and Medicare treatments.[283] Based on our review of definitions commonly used, for the purposes of the ETC Model we propose to define the term “ETC Large Dialysis Organization,” abbreviated “ETC LDO,” as a legal entity that owns, in whole or in part, 500 or more ESRD facilities. Based on the current distribution of numbers of ESRD facilities owned by dialysis organizations operating in the market, we believe this threshold is appropriate, as it differentiates the largest dialysis organizations, which at present own over 2,500 ESRD facilities, from smaller dialysis organizations, the next largest of which owns approximately 350 ESRD facilities. We believe the difference in size represents a meaningful difference in access to resources necessary to establish a home dialysis program, as well as the likelihood that an ESRD facility's aggregation group would have at least one ESRD facility with a home dialysis program in the aggregation group. We seek comment on our proposal to include nocturnal in-center dialysis beneficiary years in the numerator of the home dialysis rate calculation only for ESRD facilities not owned in whole or in part by an ETC LDO, as well as our proposal to define an ETC LDO as a legal entity owning 500 or more ESRD facilities.
While nocturnal in-center dialysis can potentially result in better patient health outcomes and savings to Medicare compared to traditional in-center dialysis, we acknowledge that its inclusion in the home dialysis rate may reduce the incentive for ESRD facilities not owned in whole or in part by an LDO to invest in a home dialysis infrastructure. We therefore propose to include nocturnal in-center dialysis as one half of the total number of dialysis treatment beneficiary years during the MY in which the attributed beneficiaries received nocturnal in-center dialysis in the numerator of the home dialysis rate calculation for ESRD facilities not owned in whole or in part by an ETC LDO as well as Managing Clinicians. We believe this policy would effectively balance the benefits of nocturnal in-center dialysis and its ability to help beneficiaries transition to home dialysis with the recognition that in-center nocturnal dialysis is not home dialysis and does not have all of the same benefits. As described in the Specialty Care Models final rule, we included one half of the total number of dialysis treatment beneficiary years during the MY in which the attributed beneficiaries received self-dialysis in center in the home dialysis rate calculation for a similar reason (85 FR 61306).
As such, we propose to amend § 512.365(b) such that, beginning for MY3, the numerator for the home dialysis rate for ESRD facilities not owned in whole or in part by an ETC LDO and Managing Clinicians would be the total number of dialysis treatment beneficiary years during the MY in which attributed ESRD Beneficiaries received maintenance dialysis at home, plus one half of the total number of dialysis treatment beneficiary years during the MY in which attributed ESRD Beneficiaries received maintenance dialysis via self-dialysis, plus one half of the total number of dialysis treatment beneficiary years during the MY in which attributed ESRD Beneficiaries received maintenance dialysis via in-center nocturnal dialysis. We further propose to add paragraph (C) to both §§ 512.365(b)(1)(ii) and 512.365(b)(2)(ii) to specify that nocturnal in-center dialysis beneficiary years included in the numerator of the home dialysis rate calculation would be composed of those months during which attributed ESRD Beneficiaries received nocturnal in-center dialysis, such that 1-beneficiary year is comprised of 12-beneficiary months. The months in which an attributed ESRD Beneficiary received nocturnal in-center dialysis would be identified by claims with Type of Bill 072X, where the type of facility code is 7 and the type of care code is 2, and with the modifier UJ, which specifies that a claim with Type of Bill 072X is for nocturnal in-center dialysis. We seek comment on these proposed changes to § 512.365(b).
4. Performance Payment Adjustment Transplant Rate
a. Status of Organ Availability
The ETC Model is designed to encourage greater rates of transplantation. In the proposed rule published on July 18, 2019 in the Federal Register titled, “Medicare Program; Specialty Care Models to Improve Quality of Care and Reduce Expenditures” (84 FR 34478), referred to herein as the “Specialty Care Models proposed rule,” CMS proposed to include the rate of transplants, both living and deceased donor transplants, in the numerator for the ETC Model's transplant rate. However, in the Specialty Care Models final rule, we recognized the limitations of supply of deceased donor organs and updated the transplant rate to be calculated as the sum of the transplant waitlist rate and the living donor transplant rate (85 FR 61310). We stated that though a transplant is often the best treatment for a beneficiary with ESRD, in light of the current shortage of deceased donor organs for transplant, the transplant waitlist rate and living donor transplant rate are currently more within the control of an ETC Participant (85 FR 61309).
However, in the Specialty Care Models final rule, we indicated our intent to observe the supply of deceased donor organs available for transplantation, with the goal of potentially modifying the transplant rate calculation for the future (85 FR 61309). Since the Specialty Care Models final rule was published on September 29, 2020, there have been several initiatives pursued by the federal government that could potentially have the effect of increasing the supply of both living donor organs and deceased donor organs.
On September 22, 2020, the Health Resources and Services Administration (HRSA) published a final rule in the Federal Register titled “Removing Financial Disincentives to Living Organ Donation” (85 FR 59438). This rule removes financial barriers to organ donation by expanding the scope of reimbursable expenses incurred by living organ donors to include lost wages, and child-care and elder-care expenses incurred by a caregiver. The rule went into effect on October 22, 2020.Start Printed Page 36380
Additionally, on December 2, 2020, CMS published in the Federal Register a final rule titled, “Medicare and Medicaid Programs; Organ Procurement Organizations Conditions for Coverage: Revisions to the Outcome Measure Requirements for Organ Procurement Organizations” (85 FR 77898), revising Conditions for Coverage (CfCs) for Organ Procurement Organizations (OPOs). The final rule revised the CfCs for OPOs in order to increase donation rates and organ transplantation rates and replaced the old outcome measures with new transparent, reliable, and objective measures. The final rule went into effect on March 30, 2021. The new outcome measures will be implemented for the recertification cycle beginning in 2022 and ending in 2026. The goals of this rule are complementary to the goals of the ETC Model, as the revised CfCs are intended to increase the supply of organs, and the ETC Model is designed to incentivize higher rates of transplantation.
Finally, as described in the Specialty Care Models final rule, CMS is in the process of implementing the ETC Learning Collaborative (85 FR 61346). The ETC Learning Collaborative is a voluntary learning system focused on increasing the availability of deceased donor kidneys for transplantation. The ETC Learning Collaborative works with and supports ETC Participants and other stakeholders required for successful kidney transplantation, such as transplant centers, OPOs, and large donor hospitals. CMS is currently in the process of jointly implementing the ETC Learning Collaborative with HRSA.
We are pleased that these efforts have progressed since the publication of the Specialty Care Models final rule. However, given that these efforts are still in the implementation process, we do not believe that it would be appropriate to update the transplant rate to include accountability for deceased donor transplants, rather than transplant waitlisting, at this time. We still intend to update the transplant rate through future rulemaking to include accountability for deceased donor transplants, but we are not proposing to do so at this time.
Beneficiary Exclusions From the Transplant Rate
As we discussed in the Specialty Care Models final rule (85 FR 61300), CMS received comments about excluding ESRD Beneficiaries with cancer from attribution to ETC Participants, as there was concern about treatment appropriateness. However, at that time, CMS did not have any evidence to suggest that this is a concern. Accordingly, we did not exclude beneficiaries with cancer from attribution to ETC Participants for purposes of calculating the home dialysis rate or the transplant rate in the Specialty Care Models final rule.
Nevertheless, after we published the Specialty Care Models final rule, we conducted further analysis, to determine if a difference existed in either the home dialysis rate or transplant rate in beneficiaries with cancer and beneficiaries without cancer. Using the Medicare claims data and input from clinical specialists in the field of nephrology, we found that the majority of ESRD Beneficiaries with cancer, specifically ESRD Beneficiaries with cancer in vital solid organs (heart, lung, liver, and kidney), are not considered to be eligible candidates for transplant. Many transplant centers do not consider these beneficiaries for transplant and require them to be cancer-free for a specific period of time prior to assessing their eligibility for transplant. This is true for getting on a transplant waitlist and for receiving living donor transplants, as a beneficiary either needs to be cancer-free or be in an initial stage of cancer diagnosis to be considered for transplant.
In addition, we found that ESRD Beneficiaries who have a diagnosis of solid organ cancer for which they were receiving treatment, specifically radiation or chemotherapy, are less likely to be in the numerator of the transplant rate—so, being placed on the transplant waitlist or receive a living donor transplant—than ESRD Beneficiaries without a diagnosis of vital solid organ cancer. By contrast, we did not find any evidence to suggest that ESRD Beneficiaries with cancer had a significant difference in the home dialysis rate compared to the ESRD Beneficiaries without cancer.
As noted previously, under §§ 512.310 and 512.365(c), the transplant rate has two components: The transplant waitlist rate and the living donor transplant rate. Upon further review and analysis, beginning for MY3, we propose to exclude ESRD Beneficiaries and, if applicable, Pre-emptive LDT Beneficiaries who have been diagnosed with vital solid organ cancers (heart, lung, liver and kidney) and who are receiving treatment, in the form of radiation or chemotherapy, for such cancers from both components of the denominator of the transplant rate for both ESRD facilities and Managing Clinicians for the duration of the MY.
Furthermore, we propose to include a lookback period, a period of time prior to the MY, to appropriately identify the ESRD Beneficiaries and, if applicable, Pre-emptive LDT Beneficiaries with a diagnosis of vital solid organ cancer for which they are receiving chemotherapy or radiation therapy. Both a diagnosis code and a treatment code are necessary to appropriately identify an ESRD Beneficiary or Pre-emptive LDT Beneficiary with a vital solid organ cancer who is receiving treatment with either radiation or chemotherapy. However, through our analysis we have identified beneficiaries who have only a treatment code available during the MY and do not have a diagnosis code during that period. Hence, we are proposing to include a lookback period of 6-months prior to the MY, so that the appropriate diagnosis code can be identified for ESRD Beneficiaries and Pre-emptive LDT Beneficiaries who have only treatment codes available in the current MY. In the alternative, we considered a 12-month lookback period, but did not find any significant difference in the number of ESRD Beneficiaries and Pre-emptive LDT Beneficiaries that had a diagnosis code for a vital organ solid cancer during a 12-month lookback period as compared to a 6-month lookback period.
We propose to identify ESRD Beneficiaries and, if applicable, Pre-emptive LDT Beneficiaries with a diagnosis of vital solid organ cancer and receiving treatment with radiation or chemotherapy by using Medicare claims. For purposes of the transplant rate calculations, an ESRD Beneficiary or Pre-emptive LDT Beneficiary would be considered to have a diagnosis of vital solid cancer during the MY, if the ESRD Beneficiary has a claim with one of the following ICD-10 diagnosis codes:
- C22.0-C22.9 (malignant neoplasm of liver and intrahepatic bile ducts),
- C34.10-C34.12 (malignant neoplasm of upper lobe, bronchus or lung),
- C34.2 (malignant neoplasm of middle lobe, bronchus or lung),
- C34.30-C34.32 (malignant neoplasm of lower lobe, bronchus or lung),
- C34.80-C34.82 (malignant neoplasm of overlapping sites of bronchus and lung),
- C34.90-C34.92 (malignant neoplasm of unspecified part of bronchus or lung),
- C38.0 (malignant neoplasm of heart),
- C38.8 (malignant neoplasm of overlapping sites of heart, mediastinum and pleura),
- C46.50-C46.52 (Kaposi's sarcoma of lung),Start Printed Page 36381
- C64.1, C64.2, C64.9 (malignant neoplasm of kidney, except renal pelvis),
- C78.00-C78.02 (secondary malignant neoplasm of lung),
- C78.7 (secondary malignant neoplasm of liver and intrahepatic bile duct),
- C79.00-C79.02 (secondary malignant neoplasm of kidney and renal pelvis),
- C7A.090 (malignant carcinoid tumor of the bronchus and lung),
- C7A.093 (malignant carcinoid tumor of the kidney), or
- C7B.02 (secondary carcinoid tumors of liver).
We propose that for the purposes of the transplant rate calculations, an ESRD Beneficiary or Pre-emptive LDT Beneficiary would be considered to be receiving treatment for vital solid organ cancer with either chemotherapy or radiation in the MY if the ESRD Beneficiary or Pre-emptive LDT Beneficiary has a claim with one of the following codes:
- CPT® 96401-96402, 96405-96406, 96409, 96411, 96413, 96415-96417, 96420, 96422-26423, 96425, 96440, 96446 (chemotherapy administration);
- CPT® 96549 (unlisted chemotherapy procedure);
- CPT® 77373 (stereotactic body radiation therapy);
- CPT® 77401-77402, 77407, 77412 (radiation treatment delivery);
- CPT® 77423 (high energy neutron radiation treatment delivery);
- CPT® 77424-77425 (intraoperative radiation treatment delivery);
- CPT® 77520, 77522-77523, 77525 (proton treatment delivery);
- CPT® 77761-77763 (intracavitary radiation source application);
- CPT® 77770-77772, 77778, 77789, 77799 (clinical brachytherapy radiation treatment);
- CPT® 79005, 79101, 79200, 79300, 79403, 79440, 79445, 79999 (radiopharmaceutical therapy);
- ICD-10-PCS DB020ZZ, DB021ZZ, DB022ZZ, DB023Z0, DB023ZZ, DB024ZZ, DB025ZZ, DB026ZZ, DB1297Z, DB1298Z, DB1299Z, DB129BZ, DB129CZ, DB129YZ, DB12B6Z, DB12B7Z, DB12B8Z, DB12B9Z, DB12BB1, DB12BBZ, DB12BCZ, DB12BYZ, DB22DZZ, DB22HZZ, DB22JZZ, DBY27ZZ, DBY28ZZ, DBY2FZZ, DBY2KZZ (radiation of lung);
- ICD-10-PCS DB070ZZ, DB071ZZ, DB072ZZ, DB073Z0, DB073ZZ, DB074ZZ, DB075ZZ, DB076ZZ, DB1797Z, DB1798Z, DB1799Z, DB179BZ, DB179CZ, DB179YZ, DB17B6Z, DB17B7Z, DB17B8Z, DB17B9Z, DB17BB1, DB17BBZ, DB17BCZ, DB17BYZ, DB27DZZ, DB27HZZ, DB27JZZ, DBY77ZZ, DBY78ZZ, DBY7FZZ, DBY7KZZ (radiation of chest wall);
- ICD-10-PCS DF000ZZ, DF001ZZ, DF002ZZ, DF003Z0, DF003ZZ, DF004ZZ, DF005ZZ, DF006ZZ, DF1097Z, DF1098Z, DF1099Z, DF109BZ, DF109CZ, DF109YZ, DF10B6Z, DF10B7Z, DF10B8Z, DF10B9Z, DF10BB1, DF10BBZ, DF10BCZ, DF10BYZ, DF0DZZ, DF20HZZ, DF20JZZ, DFY07ZZ, DFY08ZZ, DFY0CZZ, DFY0FZZ, DFY0KZZ (radiation of liver);
- ICD-10-PCS DT000ZZ, DT001ZZ, DT002ZZ, DT003Z0, DT003ZZ, DT004ZZ, DT005ZZ, DT006ZZ, DT1097Z, DT1098Z, DT1099Z, DT109BZ, DT109CZ, DT109YZ, DT10B6Z, DT10B7Z, DT10B8Z, DT10B9Z, DT10BB1, DT10BBZ, DT10BCZ, DT10BYZ, DT20DZZ, DT20HZZ, DT20JZZ, DTY07ZZ, DTY08ZZ, DTY0CZZ, DTY0FZZ (radiation of kidney);
- ICD-10-PCS DW020ZZ, DW021ZZ, DW022ZZ, DW023Z0, DW023ZZ, DW024ZZ, DW025ZZ, DW026ZZ, DW1297Z, DW1298Z, DW1299Z, DW129BZ, DW129CZ, DW129YZ, DW12B6Z, DW12B7Z, DW12B8Z, DW12B9Z, DW12BB1, DW12BBZ, DW12BCZ, DW12BYZ, DW22DZZ, DW22HZZ, DW22JZZ, DWY27ZZ, DWY28ZZ, DWY2FZZ (radiation of chest); or
- ICD-10-PCS DW030ZZ, DW031ZZ, DW032ZZ, DW033Z0, DW033ZZ, DW034ZZ, DW035ZZ, DW036ZZ, DW1397Z, DW1398Z, DW1399Z, DW139BZ, DW139CZ, DW139YZ, DW13B6Z, DW13B7Z, DW13B8Z, DW13B9Z, DW13BB1, DW13BBZ, DW13BCZ, DB13BYZ, DW23DZZ, DW23HZZ, DW23JZZ, DWY37ZZ, DWY38ZZ, DWY3FZZ (radiation of abdomen);
We seek comment on the proposal to amend § 512.365(c) to exclude ESRD Beneficiaries and, if applicable, Pre-emptive LDT Beneficiaries with a diagnosis of vital solid organ cancer and receiving treatment with chemotherapy or radiation from the denominator of the transplant rate as a whole, including both the transplant waitlist rate component and the living donor transplant rate component, for the duration of the MY for both ESRD facilities and Managing Clinicians.
5. PPA Achievement Benchmarking
a. Background on Achievement Benchmarking
Under the ETC Model, the PPA is a positive or negative adjustment on dialysis and dialysis-related Medicare payments, for both home dialysis and in-center dialysis. To calculate an ETC Participant's PPA, we assess ETC Participant achievement on the home dialysis rate and transplant rate in relation to achievement and improvement benchmarks, as described in 42 CFR 512.370(b) and § 512.370(c), respectively. The Model more heavily weights achievement of results, allowing participating Managing Clinicians or ESRD facilities to earn up to 2 points in the scoring methodology, as opposed to only 1.5 points for maximum level of improvement, as described in §§ 512.370(b) and 512.370(c).
The achievement benchmarks are constructed based on the home dialysis rate and transplant rate observed in Comparison Geographic Areas during corresponding Benchmark Years. Achievement benchmarks are percentile based, and an ETC Participant receives the achievement points that correspond with its performance, at the aggregation group level, on the home dialysis rate and transplant rate in relation to the achievement benchmarks, as described in § 512.370(b). Table 7 details the achievement score scale described in § 512.370(b).
Start Printed Page 36382
In the Specialty Care Models proposed rule, we proposed to apply this achievement benchmark policy only for MY1 and MY2, and stated our intent to increase achievement benchmarks for ETC Participants above the rates observed in Comparison Geographic Areas. We stated our belief that increasing the achievement benchmarks for future MYs, which we would do through subsequent rulemaking, was necessary in order to provide sufficient incentive for ETC Participants to increase rates of home dialysis and transplantation at a rate faster than would occur absent the ETC Model (84 FR 34556 through 34557). In the Specialty Care Models final rule, in response to comments, we finalized the applicability of the achievement benchmarks for MY1-MY2 and for subsequent MYs (85 FR 61323), but reiterated our intent to establish a different method for establishing achievement benchmarks for future years of the Model through subsequent rulemaking (85 FR 61320). We stated our belief that future modifications to the achievement benchmark methodology finalized in the Specialty Care Models final rule would be necessary to provide sufficient incentive for ETC Participants to raise home dialysis and transplant rates at a rate faster than would occur absent the ETC Model (85 FR 61321). However, we clarified that while we had stated a goal of 80 percent of an ETC Participant's receiving home dialysis or a transplant in order to receive the maximum upward payment adjustment by the final MYs, we were not finalizing that goal in the Specialty Care Models final rule (85 FR 61321).
b. Addressing Socioeconomic Factors That Impact ETC Participant Achievement
In the Specialty Care Models final rule, we acknowledged commenters' concerns that non-clinical factors, such as socioeconomic status, may impact a beneficiary's likelihood to receive home dialysis or transplant. We discussed commenters' suggestions to incorporate consideration of socioeconomic status in two elements of the ETC Model: (1) Beneficiary attribution; and (2) risk adjustment. However, we declined to exclude beneficiaries from attribution based on socioeconomic status. Noting the importance of not excluding these beneficiaries, CMS stated its intent to assess the use of various codes for purposes of adding any additional beneficiary exclusions from attribution to ETC Participants based on socioeconomic status, homelessness, or other social determinants of health through future rulemaking (85 FR 61299). We also noted that commenters' suggestions for ways to risk adjust the home dialysis rate based on socioeconomic status were a significant departure from the policy originally proposed (85 FR 61315).
We continue to acknowledge the impact that non-clinical factors, such as socioeconomic status, have on a beneficiary's likelihood to receive home dialysis or a transplant. Based on our additional analysis of Medicare claims data show that beneficiaries who are dual-eligible for Medicare and Medicaid or receive the Medicare Low-Income Subsidy (LIS) are less likely than beneficiaries who are not dual-eligible and are not LIS recipients to dialyze at home or to receive a kidney transplant. As such, ETC Participants who have a higher proportion of attributed beneficiaries who are dual-eligible or LIS recipients may be less likely to achieve high home dialysis and transplant rates than ETC Participants who have a lower proportion of attributed beneficiaries who are dual-eligible or LIS recipients.
c. Proposed Achievement Benchmarking and Scoring
(1) Achievement Benchmarking and Scoring for MY3 Through MY10
We propose to modify the percentile-based achievement benchmarking methodology based on the home dialysis rate and transplant rate observed in Comparison Geographic Areas during the Benchmark Year as the basis for achievement benchmarks in MY3 through MY10. Rather than using rates observed in Comparison Geographic Areas, we propose to modify § 512.370(b)(1) to use rates observed in Comparison Geographic Areas as the base for the achievement benchmarks, and to increase the achievement benchmarks above the Comparison Geographic Area rates during the Benchmark Year by 10 percent every two MYs, beginning for MY3. As such, we propose that achievement benchmarks would be calculated by multiplying the percentile rate observed in Comparison Geographic Areas during the Benchmark Year by 1.1 for MY3 and MY4, by 1.2 for MY5 and MY6, by 1.3 for MY7 and MY8, and by 1.4 for MY9 and MY10.
Based on CMS analyses detailed in section IX.B.4 of this proposed rule, this proposed methodology for increasing benchmarks by 10 percent every two MYs would produce results in keeping with the initial impact estimates for the ETC Model, as described in the Specialty Care Models final rule (85 FR 61353 through 61354). In the Specialty Care Models final rule, we estimated impacts based on projected growth rates for the home dialysis and transplant rates based on historical observation, projected a 1.5 percentage point growth rate (85 FR 61354). In section IX.B.4 of this proposed rule, updated projections assume the same projected growth rate, but note that observed rates of increase have accelerated in more recent data. As such, we believe that this proposed rate Start Printed Page 36383of increase would be attainable for ETC Participants, as initial impact estimates were based on rates of increase observed on the home dialysis rate and transplant rate before the ETC Model began (85 FR 61353). We also note that, unlike in the Specialty Care Models proposed rule (84 FR 34556), we are not proposing to increase achievement benchmarks such that of 80 percent of an ETC Participant's attributed beneficiaries would need to be receiving home dialysis or a transplant in order for the ETC Participant to receive the maximum upward payment adjustment by the final MYs.
Table 8 details the proposed scoring methodology for assessment of MY3 through MY10 achievement scores.

We considered increasing achievement benchmarks by a percentage point amount, rather than by a percent amount, every two MYs (for example, increasing achievement benchmarks by 10-percentage points for MY3 and MY4, by 20-percentage points for MY5 and MY6, etc.). However, we believe that this percentage point-based approach would be less flexible to and accommodating of variation in the underlying distributions of home dialysis and transplant rates than the percent-based approach we are proposing. We also believe this percentage point-based approach would add additional complexity, as we would likely need to develop separate percentage point amounts by which to increase benchmarks as the home dialysis rate and transplant rate observed in Comparison Geographic Areas are not sufficiently similar to expect the same percentage point growth rate for the two rates.
We also considered proposing to modify the Benchmark Year, such that the Benchmark Year would be a fixed duration (for example, July 1, 2018 through June 30, 2019), rather than a period of time defined in relation to the relevant MY. However, we determined that this approach would not account for aggregate changes in the home dialysis rate and transplant rate over time.
We believe that the proposed approach for increasing achievement benchmarks over the course of the ETC Model balances the intent of the model design to increase rates of home dialysis and transplantation above what would have occurred in the absence of the Model with what is achievable for ETC Participants, based on rates of home dialysis and transplantation observed at the high ends of the distributions (for additional discussion, see section IX.B.4.a.(3) of this proposed rule). We also believe the proposed approach would provide clarity to ETC Participants about the benchmarking methodology for the duration of the ETC Model while maintaining flexibility in Start Printed Page 36384that methodology to address long term trends in the home dialysis rate and transplant rate.
We seek public comment on our proposal to modify the achievement benchmarking methodology under § 512.370(b) beginning for MY3 to increase achievement benchmarks, and the proposal to increase achievement benchmarks by 10 percent every two MYs above percentile-based rates of observed in Comparison Geographic Areas.
(2) Achievement Benchmark Stratification by Dual-Eligible and Low Income Subsidy (LIS) Status
We also propose to modify § 512.370(b) to stratify achievement benchmarks based on the proportion of beneficiary years attributed to the ETC Participant's aggregation group for which attributed beneficiaries were dually-eligible for Medicare and Medicaid or received the LIS, based on rates in Comparison Geographic Areas. Under our proposal, we would create two strata with the cutpoint set at 50 percent of attributed beneficiary years being for attributed beneficiaries who were dual-eligible or received the LIS. As such, there would be one stratum for ETC Participants whose aggregation groups had 50 percent or more of their attributed beneficiary years during the MY for beneficiaries who were dual-eligible or received the LIS, based on rates in Comparison Geographic Areas for aggregation groups with 50 percent or more attributed beneficiary years during the Benchmark Year being for dual-eligible or LIS beneficiaries. There would be a second stratum for ETC Participants whose aggregation groups had less than 50 percent of their attributed beneficiary years during the MY for beneficiaries who were dual-eligible or received the LIS, based on rates in Comparison Geographic Areas for aggregation groups with less than 50 percent attributed beneficiary years during the Benchmark Year being for dual-eligible or LIS beneficiaries. We propose to determine whether an attributed beneficiary was dual-eligible or received the LIS for a given month using Medicare administrative data. We believe this proposal would address concerns that socioeconomic factors may impact a beneficiary's likelihood to receive alternative renal replacement modalities, lowering the transplant rate and home dialysis rates for ETC Participants who provide services to low income beneficiaries. We expect that stratifying the achievement benchmarks as proposed would increase home dialysis rate and transplant rates for such ETC Participants.
We considered using more than two strata, in order to increase the precision of the achievement benchmarks and the degree of similarity between ETC Participants within a given stratum. However, increasing the number of strata would decrease the number of observations within each stratum, in turn decreasing statistical reliability. Additionally, analysis of the distribution of the home dialysis rate and transplant rate demonstrates that the underlying distribution does not lend itself to more than two strata, as the distribution is not multi-modal. For this reason, we are proposing only two strata.
We seek public comment on our proposal to amend § 512.370(b) to stratify achievement benchmarks based on the proportion of attributed beneficiary years for which attributed beneficiaries were dual-eligible or received the LIS, and on our proposal to create two strata for this purpose.
6. PPA Improvement Benchmarking and Scoring
a. Background on Improvement Benchmarking and Scoring
Another part of the scoring methodology for the PPA is improvement scoring. We calculate an ETC Participant's improvement score under § 512.370(c) by comparing MY performance on the home dialysis rate and transplant rate against past ETC Participant performance. As described in the Specialty Care Models final rule, the purpose of the improvement score is to acknowledge efforts made in practice transformation to improve rates of home dialysis and transplants (85 FR 61318). The percentage improvement in the ETC Participant's MY performance on the home dialysis rate and the transplant rate relative to the Benchmark Year rate is scored as follows:
- Greater than 10 percent improvement relative to the Benchmark Year rate: 1.5 points
- Greater than 5 percent improvement relative to the Benchmark Year rate: 1 point
- Greater than 0 percent improvement relative to the Benchmark Year rate: 0.5 points
- Less than or equal to the Benchmark Year rate: 0 points
However, when the Benchmark Year rate is zero, an improvement score for the MY cannot be calculated. This is because, when calculating percent change, as used in improvement scoring, the Benchmark Year rate is the denominator. As such, we cannot calculate percent improvement for an aggregation group with a rate of zero during the Benchmark Year because the denominator of the improvement score calculation is zero, and division by zero is undefined. Thus, an aggregation group in this situation will not receive an improvement score if the Benchmark Year rate is zero, even if the aggregation group has made improvements in the home dialysis rate and/or the transplant rate between the Benchmark Year and MY.
b. Incentivizing Improvement for Socioeconomically Disadvantaged Beneficiaries
As described in section V.B.5.b of this proposed rule, beneficiaries who are dual-eligible or receive the LIS are less likely than beneficiaries who are not dual-eligible and do not receive the LIS to dialyze at home or receive a kidney transplant. As described previously in this section of the proposed rule, we are proposing to stratify achievement benchmarks by the proportion of attributed beneficiary years for beneficiaries who are dual-eligible or LIS recipients to avoid disadvantaging ETC Participants who provide care for a high proportion of these beneficiaries. However, this proposed stratification would not provide a direct financial incentive for ETC Participants to focus on reducing disparities by improving the home dialysis rate and transplant rate for beneficiaries who are dual-eligible or receive the LIS. We are interested in creating that incentive as part of the ETC Model, as these beneficiaries may require additional support from ETC Participants to pursue home dialysis and transplant as alternative renal replacement modalities.
c. Proposed Changes to Improvement Benchmarking and Scoring
(1) Revised Improvement Calculation
As described above, when the Benchmark Year rate for an aggregation group is zero, the aggregation group cannot receive an improvement score, even if the aggregation group has made improvements in the home dialysis rate and transplant rate between the Benchmark Year and MY. To address this issue, we propose to amend § 512.370(c)(1) to change the improvement calculation such that the aggregation group's Benchmark Year rate cannot be zero. Specifically, for MY3 through MY10, we propose to add one beneficiary month to the numerator of the home dialysis rate and the transplant rate for the Benchmark Year rate for an ETC Participant's aggregation group Benchmark Year when that rate is zero. CMS does not propose to change Start Printed Page 36385the denominator of the Benchmark Year rate calculations because doing so would negate the purpose of mathematically correcting ETC Participants' improvement scoring. CMS does not expect that adding a beneficiary month to the numerator of the Benchmark Year rate calculations, as proposed, would affect the improvement scoring enough to change the number of points awarded to the ETC Participant, and has the advantage that it would enable an improvement score to be calculated, even when the Benchmark Year rate is zero.
(2) Health Equity Incentive
To incentivize ETC Participants to decrease disparities in the home dialysis rate and transplant rate between beneficiaries who are dual-eligible or LIS recipients and those who are not, we propose to add a Health Equity Incentive to the improvement scoring methodology. We propose to define the Health Equity Incentive at § 512.310 as the amount added to the ETC Participant's improvement score calculated as described in § 512.370(c)(1) if the ETC Participant's aggregation group demonstrated sufficient improvement on the home dialysis rate or transplant rate for attributed beneficiaries who are dual-eligible or LIS recipients between the Benchmark Year and the MY. We propose that this improvement on the home dialysis rate or transplant rate would be based on the performance of the ETC Participant's aggregation group.
As noted previously in this section of the proposed rule, socioeconomic factors impact a beneficiary's receipt of alternative renal replacement modalities. Beneficiaries with limited resources may require more assistance from ESRD facilities and Managing Clinicians to use alternative renal replacement modalities. We believe our proposal to add a Health Equity Incentive would benefit these beneficiaries and improve scoring for home dialysis rate and transplant rate for ETC Participants that serve disproportionately high numbers of beneficiaries with lower socioeconomic status. To earn the Health Equity Incentive, ETC Participants would have to demonstrate sufficiently significant improvement on the home dialysis rate or transplant rate among their attributed beneficiaries who are dual eligible or receive the LIS between the Benchmark Year and the MY. ETC Participants who earn the Health Equity Incentive would receive a 0.5 point increase on their improvement score, thus increasing the maximum improvement score to 2 points. We believe the proposed Health Equity Incentive would benefit attributed beneficiaries who are dual eligible or receive the LIS, by encouraging ETC Participants to address disparities in access to alternative renal replacement modalities among these beneficiaries. We believe that providing this incentive for ETC Participants to increase their home dialysis and transplant rate among their dual eligible or LIS beneficiary population would ultimately reduce this disparity in access for the beneficiaries in question. Therefore, we believe this incentive to reduce socioeconomic disparities in access to alternative renal replacement modalities would be an improvement to the PPA scoring methodology.
We propose to amend § 512.370(c) to add the Health Equity Incentive to the improvement scoring methodology, beginning for MY3. We propose that the Health Equity Incentive would be equal to 0.5 points, which would be added to the ETC Participant's improvement score for the home dialysis rate or for the transplant rate, calculated as described in § 512.370(c)(1), such that the maximum improvement score would increase from 1.5 points to 2 points for ETC Participants that earn the Health Equity Incentive. Therefore, for those ETC Participants that earn the Home Equity Incentive, we propose that the ETC Participant's improvement score for the home dialysis rate and for the transplant rate would be the sum of the improvement score calculated as described in § 512.370(c)(1) and the Health Equity Incentive. The Health Equity Incentive would allow ETC Participants to increase their improvement score, and thereby increase their payment adjustment.
We propose to award the Health Equity Incentive to an ETC Participant if the ETC Participant's aggregation group's home dialysis rate and/or transplant rate among attributed beneficiaries who are dual-eligible or LIS recipients increases by 5 or more percentage points from the Benchmark Year to the MY. We believe that 5-percentage points is the correct threshold for awarding the Health Equity Incentive based on our analysis of Medicare claims. Five percentage points is one standard deviation above the average difference between the home dialysis rate and the transplant rate for attributed beneficiaries who are dual-eligible or LIS recipients and those beneficiaries who are not dual-eligible or LIS recipients, rounded to the nearest integer. We anticipate improvement in home dialysis and transplant rates among dual-eligible or LIS recipients between the MY and the Benchmark Year, but we expect that attaining the proposed threshold for earning the Health Equity Incentive would generally require significant effort on the part of the ETC Participant.
We propose that an ESRD Beneficiary or Pre-emptive LDT Beneficiary would be considered to be dual eligible or an LIS recipient for a given month if at any point during the month the beneficiary was dually eligible for Medicare and Medicaid or an LIS recipient. We propose to determine whether an attributed beneficiary was dual-eligible or received the LIS using Medicare administrative data.
We propose to modify § 512.370(c) such that the improvement benchmarking and scoring methodology for MY1 and MY2 would be specified at § 512.370(c)(1), and the improvement benchmarking and scoring methodology for MY3 through MY10, described above, would be specified at § 512.370(c)(2). We seek comment on the proposal to modify § 512.370(c) accordingly.
We considered using a rolling approach to setting the threshold for earning the Health Equity Incentive, such that the threshold would be recalculated every other MY, to reflect changes in underlying disparities. Under this approach, we would calculate the threshold as one standard deviation above the average difference between the home dialysis rate and the transplant rate for attributed beneficiaries who are dual-eligible or LIS recipients and those beneficiaries who are not dual-eligible or LIS recipients, rounded to the nearest integer. We would calculate this threshold either using data from the Benchmark Year, such that ETC Participants would know the threshold for earning the Health Equity Incentive in advance of the MY, or using data from the MY, such that the threshold for earning the Health Equity Incentive would accurately reflect the magnitude of the disparity observed during the MY. However, we believe that setting a threshold for earning the Health Equity Incentive applicable for all MYs, beginning for MY3, is more appropriate. This approach would be in keeping with the intent of the proposed Health Equity Incentive, which is to provide ETC Participants a financial incentive to focus on decreasing the disparity in the home dialysis and transplant rates between beneficiaries who are dual-eligible or LIS recipients, and those who are not. We believe providing ETC Participants clear information about what they need to achieve to earn the Health Equity Incentive in advance would best enable them to work towards the goal.Start Printed Page 36386
We propose that ETC Participants in aggregation groups that fall below a low-volume threshold would be ineligible to earn the Health Equity Incentive. Specifically, we propose that an ETC Participant in an aggregation group with fewer than 11 attributed beneficiary years comprised of months in which ESRD Beneficiaries and, if applicable, Pre-emptive LDT Beneficiaries are dual eligible or LIS recipients during either the Benchmark Year or the MY would be ineligible to earn the Health Equity Incentive. We selected this particular low-volume threshold for consistency with the low-volume threshold for the applicability of the PPA generally, as specified at § 512.385. We believe it is necessary to apply a low volume threshold in determining whether an ETC Participant has earned the Home Equity Incentive to ensure statistical reliability of the home dialysis rate and transplant rate calculations. This statistical reliability provides consistency in the home dialysis rate and transplant rate calculations. Therefore, similar results are produced under consistent conditions when applying a low volume threshold to ETC Participants. We are proposing a low-volume threshold specific to attributed beneficiaries who are dual-eligible or receive the LIS because whether an ETC Participant has earned the Health Equity Incentive is being assessed on this subset of attributed beneficiaries.
We propose to amend the Modality Performance Score (MPS) methodology to incorporate the Health Equity Incentive. To that end, we propose to modify § 512.370(d) such that the calculation of the MPS for MY1 and MY2 is specified at § 512.370(d)(1), and the calculation of the MPS for MY3 through MY10 is specified at § 512.370(d)(2). We propose that the formula for the MPS for MY3 through MY10 would be the following:
Modality Performance Score
= 2
× (Higher of the home dialysis achievement or (home dialysis improvement score + Health Equity Bonus †))
+ (Higher of the transplant achievement or (transplant improvement score + Health Equity Bonus †))
† The Health Equity Incentive is applied to the home dialysis improvement score or transplant improvement score only if earned by the ETC Participant and provided that the ETC Participant is not ineligible to receive the Home Equity Incentive as described in proposed § 512.370(c)(2)(iii).
We seek comment on our proposed definition for the Health Equity Incentive at § 512.310 and our proposal to amend § 512.370(c) to add the Health Equity Incentive to the improvement scoring methodology for the home dialysis rate and the transplant rate. We also seek comment on our proposal to set the threshold for earning the Health Equity Incentive at 5-percentage points improvement from the Benchmark Year to the MY.
7. PPA Reports and Data Sharing
a. Background on Beneficiary Attribution and Performance Reporting
Under the ETC Model, as described in 42 CFR 512.360, CMS attributes ESRD Beneficiaries and, if applicable, Pre-emptive LDT Beneficiaries to an ETC Participant for each month during a MY based on the beneficiary's receipt of services during that month. CMS performs this attribution for a MY retrospectively, after the end of the MY. As described in § 512.365, each ETC Participant's performance is assessed based on the transplant rate and home dialysis rate among the population of beneficiaries attributed to the ETC Participant. As described in 42 CFR 512.370 and 42 CFR 512.380, these rates are used to calculate the ETC Participant's MPS and, in turn, the ETC Participant's PPA. The PPA is then used to adjust certain Medicare payments of the ETC Participant during 6-month PPA periods, with the first PPA Period taking place from July 1, 2022, through December 31, 2022. As described in 42 CFR 512.390(a), CMS will notify each ETC Participant, in a form and manner determined by CMS, of the ETC Participant's attributed beneficiaries, MPS, and PPA for a PPA Period no later than one month before the start of the applicable PPA Period.
In order to ensure ETC Participant have timely access to these ETC Model reports, we are proposing to add a new paragraph (b) to § 512.390 to establish a process for CMS to share certain beneficiary-identifiable and aggregate data with ETC Participants pertaining to their participation in the ETC Model. CMS believes that ETC Participants need this data to successfully coordinate the care of their ESRD Beneficiaries and, if applicable, Pre-emptive LDT Beneficiaries; to succeed under the ETC Model; and to assess CMS's calculations of the individual ETC Participant's PPA for a given PPA Period. Specifically, CMS believes that ETC Participants must have a clear understanding of the beneficiaries CMS has attributed to them under the ETC Model and how each attributed beneficiary has factored into the ETC Participant's home dialysis rate, transplant waitlist rate, and living donor transplant rate, to better identify care coordination and care management opportunities, and to have the opportunity to seek targeted review of CMS's calculation of the MPS. The purpose of the targeted review process, established under current § 512.390(b), which we would redesignate as paragraph (c), is to determine whether an incorrect PPA has been applied during the PPA Period. CMS additionally believes that timely access to this data is important and proposes to require CMS to make this data available twice a year, prior to each PPA Period in an MY.
In the following sections of this proposed rule, we describe our proposed process for CMS to share and for ETC Participants to retrieve certain beneficiary-identifiable attribution data and performance data, as well as the protections that would apply to this data under a data sharing agreement with CMS. We also describe our proposed process for sharing certain aggregate, de-identified performance data with ETC Participants.
b. CMS Sharing of Beneficiary-Identifiable Data
We propose to establish a process in new § 512.390(b)(1) under which CMS would share certain beneficiary-identifiable data with ETC Participants regarding their attributed beneficiaries and performance under the ETC Model. We are proposing that, in accordance with the timing of the notification requirement described in § 512.390(a), CMS would be required to make the beneficiary-identifiable data pertaining to a given PPA Period available for retrieval by ETC Participants no later than 1 month before the start of that PPA Period. The ETC Participant would be able to retrieve this data at any point during the relevant PPA Period, but, in accordance with current § 512.390(b)(1), which would be redesignated as paragraph (c)(1), the ETC Participant would have 90 days from the date that CMS shares the MPS, including the data CMS used in calculating the MPS, to request a targeted review. We propose that CMS would notify ETC Participants of the availability of the beneficiary-identifiable data for a relevant PPA Period and the process for retrieving that data, through the ETC listserv and through the ETC Model website, available at https://innovation.cms.gov/innovation-models/esrd-treatment-choices-model.
Regarding the specific beneficiary-identifiable data that CMS would be required to share with ETC Participants, Start Printed Page 36387we are proposing in § 512.390(b)(1)(ii)(A) to include, when available, the following data for each PPA Period: The ETC Participant's attributed beneficiaries' names, Medicare Beneficiary Identifiers (MBIs), dates of birth, dual-eligible status, and LIS recipient status. We believe that the patient's name, MBI, and date of birth constitute the minimum elements to enable an ETC Participant to properly identify an attributed beneficiary, and to confirm the identity of an attributed during any communications with a beneficiary or a beneficiary's caregiver, as appropriate and allowable. In addition, the ETC Participant needs to be aware of each attributed beneficiary's dual-eligible status and LIS recipient status to understand how each attributed beneficiary contributed to how CMS calculated the ETC Participant's Health Equity Incentive, if finalized. We propose in § 512.390(b)(1)(ii)(B) that this beneficiary-identifiable data also would include, when available, data regarding the ETC Participant's performance under the ETC Model, including, for each attributed beneficiary, as applicable, the number of months the beneficiary was attributed to the ETC Participant, received home dialysis, self-dialysis, or nocturnal in-center dialysis, or was on a transplant waitlist; and the number of months that have passed since the beneficiary has received a living donor transplant, as applicable. We believe that sharing these data elements would help the ETC Participant understand and, as appropriate, seek targeted review of CMS's calculation of the ETC Participant's MPS, and otherwise understand how CMS adjusted the ETC Participant's Medicare payments by the PPA.
We recognize there are sensitivities surrounding the disclosure of individually-identifiable (beneficiary-specific) health information, and we note that a number of laws place constraints on the sharing of individually identifiable health information. For example, section 1106 of the Act generally bars the disclosure of information collected under the Act without consent unless a law (statute or regulation) permits for the disclosure. In this instance, the HIPAA Privacy Rule provides that legal authority and authorizes this proposed disclosure of individually identifiable health information by us to ETC Participants. Under the HIPAA Privacy Rule, covered entities (defined as health care plans, health care providers that submit certain transactions electronically, and health care clearinghouses) are barred from using or disclosing individually identifiable health information (called “protected health information” or PHI) in a manner that is not explicitly permitted or required under the HIPAA Privacy Rule, without the individual's authorization. The Medicare FFS program, a “health plan” function of the Department, is subject to the HIPAA Privacy Rule limitations on the disclosure of PHI, without an individual's authorization. ETC Participants are also covered entities, provided they are health care providers as defined by 45 CFR 160.103 and they or their agents electronically engage in one or more HIPAA standard transactions, such as for claims, eligibility or enrollment transactions.
The proposed disclosure of ETC Model beneficiary-identifiable data would be permitted by the HIPAA Privacy Rule under the provisions that permit disclosures of PHI as “required by law.” Under 45 CFR 164.512(a)(1), a covered entity may use or disclose PHI to the extent that such use or disclosure is required by law and the use or disclosure complies with and is limited to the relevant requirements of such law.[284] We are proposing to establish a requirement under § 512.390(b)(1) for CMS to share this data with ETC Participants.
The Privacy Act of 1974 also places limits on agency data disclosures. The Privacy Act applies when federal agencies maintain systems of records by which information about an individual is retrieved by use of one of the individual's personal identifiers (names, Social Security numbers, or any other codes or identifiers that are assigned to the individual). The Privacy Act generally prohibits disclosure of information from a system of records to any third party without the prior written consent of the individual to whom the records apply, 5 U.S.C. 552a(b). “Routine uses” are an exception to this general principle. A routine use is a disclosure outside of the agency that is compatible with the purpose for which the data was collected. Routine uses are established by means of a publication in the Federal Register about the applicable system of records describing to whom the disclosure will be made and the purpose for the disclosure. We believe that the proposed data disclosures are consistent with the purposes for which the data discussed in this rule was collected, and thus, should not run afoul of the Privacy Act, provided we ensure that an appropriate Privacy Act system of records “routine use” is in place prior to making any disclosures. The systems of records from which CMS would share data are the Medicare Integrated Data Repository (“IDR”), system of records number 09-70-0571, and the Health Resources and Services Administration (“HRSA”) Organ Procurement and Transplantation Network (“OPTN”)/Scientific Registry of Transplant Recipients (“SRTR”) Data System, system of records number 09-15-0055.
We believe that establishing a regulatory requirement for CMS to share the beneficiary-identifiable data described above would be appropriate for the ETC Model for several reasons. First, we believe that all ETC Participants not only desire but need this data to know which beneficiaries CMS has attributed to them (and thus is holding them financially accountable for such beneficiaries' individual contributions to the ETC Participant's performance measures described in 42 CFR part 512, subpart C, with the proposed modifications described in this proposed rule, if finalized), and for each ETC Participant to understand the basis by which CMS computed their MPS. Second, CMS believes that all ETC Participants, regardless of size, would have the capability of managing and meaningfully using the shared data. We would provide the data in a form and manner that CMS believes is user-friendly. In addition, the ETC Participant would be able to review the beneficiary-identifiable data along with the aggregated data, which should help the ETC Participant understand the data CMS would share with the ETC Participant. Finally, CMS believes that any other approach to making beneficiary-identifiable data available, including the alternative proposal considered by CMS and described below, would impose additional operational burdens on CMS and administrative burdens on both CMS and the ETC Participants without producing any meaningful privacy or security benefit.
We considered an alternative proposal for making beneficiary-identifiable data available to ETC Participants based on the data sharing policies currently used in many models tested under section 1115A of the Act, which would involve ETC Participants formally requesting the data from CMS before CMS could share the data. In particular, ETC Participants Start Printed Page 36388would have the opportunity to request the data for their own “health care operations” and CMS would be permitted to disclose the requested data based on the HIPAA Privacy Rule provisions that permit disclosures of PHI for the recipient's health care operations purposes as described in 45 CFR 164.506(c)(4) and § 164.501. Under this alternative approach, ETC Participants that request this information would have to attest to compliance with specific HIPAA requirements in addition to, or as part of, the data sharing agreement described in the next section of this proposed rule.
After considering this option, we believe that having the ETC Participant request the data from CMS would add steps in the process that would cause administrative burden for both CMS and ETC Participants, and operational cost and burden for CMS. We further believe that adding these steps would not produce a meaningful privacy or security benefit based on the specific circumstances of this ETC Model. Both this option and the approach proposed above would require that the ETC Participant complete and sign a data sharing agreement, and both would allow an ETC Participant to decline receiving beneficiary-identifiable data by declining to complete or sign a data sharing agreement. As such, there are no meaningful privacy or security benefits that this option would create that are not already realized by the proposed approach to data sharing in the ETC Model. We also anticipate that all ETC Participants would want and need, and overwhelmingly would request, the data described previously in this section, would be capable of handling such data, and would take the steps necessary to obtain the data. In addition, under an alternative approach based on the HIPAA provisions for the ETC Participant's “health care operations,” CMS would only be able to disclose the beneficiary-identifiable data for a purpose listed in paragraph (1) or (2) of the definition of “health care operations” in 45 CFR 164.501. However, we also believe it is crucial that an ETC Participant has the opportunity to understand how CMS calculated the ETC Participant's PPA for a PPA Period, and have the information needed to request a targeted review of CMS's MPS calculation if the ETC Participant believes CMS made an error.
Given the policies proposed in this section and the following sections related to data sharing, we propose to modify the title of § 512.390 from “Notification and targeted review” to “Notification, data sharing, and targeted review.” We propose this change so that the section title will more accurately reflect the contents of the section.
We solicit public comment on our proposal to require, under proposed § 512.390(b)(1), that CMS make available certain beneficiary-identifiable attribution and performance data for retrieval by ETC Participants no later than one month prior to the start of each PPA Period, and on our considered alternative to this proposal.
(1) Conditions for Retrieving Beneficiary-Identifiable Data
Given the sensitive nature of the beneficiary-identifiable data that CMS would be required to share under our proposal, we are proposing certain conditions for ETC Participants to be able to retrieve this data and certain protections that would govern use of the data following retrieval. First, we propose that CMS would only share the beneficiary-identifiable data on the condition that the ETC Participant observes all relevant statutory and regulatory provisions regarding the appropriate use of data and the confidentiality and privacy of individually identifiable health information as would apply to a covered entity under the Health Insurance Portability and Accountability Act of 1996 (HIPAA) regulations and agrees to comply with the terms of a separate data sharing agreement. Although we expect ETC Participants are covered entities and must comply with the HIPAA regulations directly, we are including this provision to ensure an ETC Participant would abide by those rules with respect to the data, even if, for example, the ETC Participant is a hybrid entity under HIPAA and the component requesting the data has not been designated as a health care component under 45 CFR 164.105. The HIPAA provisions that the ETC Participant would have to observe would include, but would not be necessarily limited to, standards regarding the use and disclosure of PHI; administrative, physical, and technical safeguards and other security provisions; and breach notification.
We propose that, if an ETC Participant wishes to retrieve the beneficiary-identifiable data, the ETC Participant would be required to first complete, sign, and submit—and thereby agree to the terms of—a data sharing agreement with CMS, which we would call the ETC Data Sharing Agreement. This agreement would include certain protections and limitations on the ETC Participant's use and further disclosure of the beneficiary-identifiable data, and would be provided in a form and manner specified by CMS, which we discuss in more detail in later sections of this proposed rule. This agreement also potentially would require the ETC Participant to make certain attestations, for example, if required under the applicable Privacy Act system of records notice. An ETC Participant that wishes to retrieve the beneficiary-identifiable data would be required to complete and submit a signed ETC Data Sharing Agreement at least annually. CMS believes that it is important for the ETC Participant to complete and submit a signed ETC Data Sharing Agreement at least annually so that CMS has up-to-date information that the ETC Participant wishes to retrieve the beneficiary-identifiable data attestations (if required), and information on the designated data custodian(s). As described in greater detail below, we propose that a designated data custodian would be the individual(s) that an ETC Participant would identify as responsible for ensuring compliance with all privacy and security requirements and for notifying CMS of any incidents relating to unauthorized disclosures of beneficiary-identifiable data.
CMS believes it is important for the ETC Participant to first complete and submit a signed ETC Data Sharing Agreement before it retrieves any beneficiary-identifiable data to help protect the privacy and security of any beneficiary-identifiable data shared by CMS with the ETC Participant. As described previously in this section of the proposed rule, there are important sensitivities surrounding the sharing of this type of individually identifiable health information, and CMS must ensure to the best of its ability that any beneficiary-identifiable data that it shares with ETC Participants would be further protected in an appropriate fashion.
We considered an alternative proposal under which ETC Participants would not need to complete and submit a signed ETC Data Sharing Agreement, but we concluded that, if we proceeded with this option, we would not have adequate assurances that the ETC Participants would appropriately protect the privacy and security of the beneficiary-identifiable data that we are proposing to share with them. We also considered an alternative proposal under which the ETC Participant would need to complete and submit a signed ETC Data Sharing Agreement only once for the duration of the ETC Model. However, we concluded that this similarly would not give CMS adequate assurances that the ETC Participant would protect the privacy and security of the beneficiary-identifiable data from Start Printed Page 36389CMS. We concluded that it is critical that we have up-to-date information and designated data custodians, and that requiring the ETC Participant to submit an ETC Data Sharing Agreement at least annually would represent the best means of achieving this goal.
We solicit public comment on our proposal to require, in § 512.390(b)(1)(iii), that the ETC Participant agree to comply with all applicable laws and the terms of the ETC Data Sharing Agreement as a condition of retrieving the beneficiary-identifiable data, and on our proposal in § 512.390(b)(1)(iv) that the ETC Participant would need to submit the signed ETC Data Sharing Agreement at least annually if the ETC Participant wishes to retrieve the beneficiary-identifiable data.
(2) Content of ETC Data Sharing Agreement Provisions for Beneficiary-Identifiable Data
We are proposing in new § 512.390(b)(iv) that, under the ETC Data Sharing Agreement, ETC Participants would agree to certain terms, namely: (1) To comply with the requirements for use and disclosure of this beneficiary-identifiable data that are imposed on covered entities by the HIPAA regulations and the requirements of the ETC Model set forth in 42 CFR part 512; (2) to comply with additional privacy, security, and breach notification requirements to be specified by CMS in the ETC Data Sharing Agreement; (3) to contractually bind each downstream recipient of the beneficiary-identifiable data that is a business associate of the ETC Participant or performs a similar function for the ETC Participant, to the same terms and conditions to which the ETC Participant is itself bound in its data sharing agreement with CMS as a condition of the downstream recipient's receipt of the beneficiary-identifiable data retrieved by the ETC Participant under the ETC Model; and (4) that if the ETC Participant misuses or discloses the beneficiary-identifiable data in a manner that violates any applicable statutory or regulatory requirements or that is otherwise non-compliant with the provisions of the ETC Data Sharing Agreement, the ETC Participant would no longer be eligible to retrieve the beneficiary-identifiable data and may be subject to additional sanctions and penalties available under the law. CMS believes that these terms for sharing beneficiary-identifiable data with ETC Participants are appropriate and important, as CMS must ensure to the best of its ability that any beneficiary-identifiable data that it shares with ETC Participants would be further protected by the ETC Participant, and any business associates of the ETC Participant, in an appropriate fashion. CMS believes that these proposals would allow CMS to accomplish that.
CMS seeks public comment on the additional privacy, security, breach notification, and other requirements that we would include in the ETC Data Sharing Agreement. CMS has these types of agreements in place as part of the governing documents of other models tested under section 1115A of the Act and in the Medicare Shared Savings Program. In these agreements, CMS typically requires the identification of data custodian(s) and imposes certain requirements related to administrative, physical, and technical safeguards relating to data storage and transmission; limitations on further use and disclosure of the data; procedures for responding to data incidents and breaches; and data destruction and retention. These provisions would be imposed in addition to any restrictions required by law, such as those provided in the HIPAA privacy, security and breach notification regulations. These provisions would not prohibit the ETC Participant from making any disclosure of the data otherwise required by law.
CMS is considering limiting the use of beneficiary-identifiable data for specific purposes, either alone or in combination. For example, in the ETC Data Sharing Agreement, CMS is considering imposing limits on how the ETC Participant may use the beneficiary-identifiable data without prior written authorization from CMS to specific purposes, such as assessing CMS's calculation of the MPS for a given PPA Period, the ETC Participant's clinical care or “treatment” (as that term is defined at 45 CFR 164.501) of an attributed beneficiary, and certain “health care operations” (as that term is defined at 45 CFR 164.501) of the ETC Participant. As noted previously in this section of the proposed rule, CMS believes that ETC Participants would require this data to be able to request a targeted review of CMS's calculation of the MPS as it relates to a given PPA Period, as understanding and being able to seek review of CMS's calculation of the MPS, and thus the reason CMS adjusted the ETC Participant's Medicare payments in the manner it did, is critical for the ETC Model. Importantly, there is no other source of this information outside of CMS. In addition to limiting use to reviewing how CMS calculated the ETC Participant's MPS, CMS is also considering limiting, in the ETC Data Sharing Agreement, use of the beneficiary-identifiable data without prior written authorization from CMS to use for clinical treatment purposes. CMS believes that this beneficiary-identifiable data would be important in helping the ETC Participant determine which of its ESRD Beneficiaries are not on the transplant waitlist or have not received a living donor transplant, to inform how the ETC Participant engages in clinical care of the subject ESRD Beneficiary.
In addition to the previous two uses, CMS is also considering limiting, in the ETC Data Sharing Agreement, the ETC Participant's use of the beneficiary-identifiable data without prior written authorization from CMS to care management and coordination, quality improvement activities, and provider incentive design and implementation, to the extent these activities would constitute “health care operations” that fall within the first and second paragraphs of the definition of that phrase under the HIPAA Privacy Rule (45 CFR 164.501). As it relates to case management and coordination and quality improvement activates, CMS believes that this beneficiary-identifiable data would help the ETC Participant to conduct the important task of identifying which ESRD Beneficiaries are not currently on the transplant waitlist and thus better enable the ETC Participant to engage those beneficiaries, as clinically appropriate, about the process of signing up for the transplant waitlist, thereby improving the ETC Participant's performance on the transplant waitlist rate, and increasing the likelihood that the subject ESRD Beneficiaries would receive a transplant. In addition, CMS believes that sharing this data with the ETC Participant would help the ETC Participant to conduct the important task of identifying which ESRD Beneficiaries are receiving dialysis in-center, and to consider whether furnishing kidney disease patient education services or otherwise making such beneficiaries aware of the possibility of receiving home dialysis, self-dialysis, or nocturnal in-center dialysis, as clinically appropriate in the ESRD Beneficiary's individual situation.
We seek public comment on how an ETC Participant might need to, and want to, use the beneficiary-identifiable data retrieved from CMS under the ETC Model to accomplish the goals of the ETC Model in accordance with applicable law.
CMS also seeks public comment on what further disclosures of the beneficiary-identifiable data might be appropriate to permit or prohibit under the ETC Data Sharing Agreement. For example, CMS is considering Start Printed Page 36390prohibiting, in the ETC Data Sharing Agreement, any further disclosure, not otherwise required by law, of the beneficiary-identifiable data described previously in this section of the proposed rule to anyone who is not a HIPAA covered entity or business associate, as defined in 45 CFR 160.103, or to an individual practitioner in a treatment relationship with the subject ESRD Beneficiary or Pre-emptive LDT Beneficiary, or that practitioner's business associates. Such a prohibition would be similar to that imposed by CMS in other models tested under section 1115A of the Act in which CMS shares beneficiary-identifiable data with model participants. In the alternative, CMS is also considering including more restrictive prohibitions in the ETC Data Sharing Agreement, which would limit further discloses to only some, one, or none of the categories of individuals or entities described above.
CMS is considering all of these possibilities because there exist important legal and policy limitations on the sharing of the beneficiary-identifiable data discussed previously in this section of the proposed rule, and CMS must consider carefully the ways in which and reasons for which we would provide access to this data for purposes of the ETC Model. CMS believes that some ETC Participants may require the assistance of business associates, such as contractors, to perform data analytics or other functions using this beneficiary-identifiable data to support the ETC Participant's review of CMS's MPS calculations, care management and coordination, quality improvement activities, or clinical treatment of attributed beneficiaries. CMS also believes that this beneficiary-identifiable data may be helpful for any HIPAA covered entities who are in a treatment relationship with the subject ESRD Beneficiary or Pre-emptive LDT Beneficiary.
We seek public comment on how an ETC Participant might need to, and want to, disclose the beneficiary-identifiable data to other individuals and entities to accomplish the goals of the ETC Model, in accordance with applicable law.
Under our proposal, the ETC Data Sharing Agreement would include other provisions, including requirements regarding data security, retention, destruction, and breach notification. For example, we are considering including, in the ETC Data Sharing Agreement, a requirement that the ETC Participant designate one or more data custodians who would be responsible for ensuring compliance with the privacy, security and breach notification requirements for the data set forth in the ETC Data Sharing Agreement; various security requirements like those found in other models tested under section 1115A of the Act, but no less restrictive than those provided in the relevant Privacy Act system of records notices; how and when beneficiary-identifiable data could be retained by the ETC Participant or its downstream recipients of the beneficiary-identifiable data; procedures for notifying CMS of any breach or other incident relating to the unauthorized disclosure of beneficiary-identifiable data; and provisions relating to destruction of the data. These are only examples, and are not the only terms CMS would potentially include in the ETC Data Sharing Agreement.
We solicit public comment on this proposal that CMS, by adding § 512.390(b)(1)(iv)(B), would impose certain requirements in the ETC Data Sharing Agreement related to privacy, security, data retention, breach notification, and data destruction.
Finally, as described above, CMS proposes, at § 512.390(b)(1)(iv)(D), that the ETC Data Sharing Agreement would include a term providing that if the ETC Participant misuses or discloses the beneficiary-identifiable data in a manner that violates any applicable statutory or regulatory requirements or that is otherwise non-compliant with the provisions of the ETC Data Sharing Agreement, the ETC Participant would no longer be eligible to retrieve beneficiary-identifiable data under proposed § 512.390(b)(1)(i) and may be subject to additional sanctions and penalties available under law. We also propose to make conforming amendments to 42 CFR 512.160. Section 512.160(b) outlines the remedial actions available under the RO Model and ETC Model, and paragraph (b)(8), in particular provides that, if CMS determines that one or more grounds for remedial action specified in § 512.160(a) has taken place, CMS may discontinue the provision of data sharing and reports to the model participant. We propose to add a new § 512.160(a)(9) to specify that, for the ETC Model only, CMS may take remedial action if the model participant misuses or discloses the beneficiary-identifiable data in a manner that violates any applicable statutory or regulatory requirements or that is otherwise non-compliant with the provisions of the applicable data sharing agreement. This proposed change, if finalized, would align the regulatory provision on remedial action with the proposed remedial action we propose to include in the ETC Data Sharing Agreement.
We solicit public comment on this proposal, to prohibit the ETC Participant from obtaining beneficiary-identifiable data pertaining to the ETC Model if the ETC Participant fails to comply with applicable laws and regulations, the terms of the ETC Model, or the ETC Data Sharing Agreement.
(3) Process for Retrieving the ETC Data Sharing Agreement and Beneficiary-Identifiable Data
We propose that we would make the ETC Data Sharing Agreement and beneficiary-identifiable data available in a form and manner specified by CMS. We expect to provide a web-based platform for ETC Participants to use to retrieve the beneficiary-identifiable data. CMS would provide ETC Participants further information about this web-based platform through the ETC listserv and the ETC Model website at a date to be determined by CMS, but at least 1 month before the first PPA Period begins on June 1, 2022. We expect that CMS would notify ETC Participants of each opportunity to retrieve a new set of beneficiary-identifiable data and the process for accessing the web-based platform to receive the data through the ETC listserv and on the ETC Model website. Under this proposal, the ETC Participant would be required to use the form and manner specified by CMS (which we expect will be a web-based platform) to retrieve the data. If the ETC Participant did not use the form and manner specified by CMS or did not agree to the ETC Data Sharing Agreement, the ETC Participant would be unable to retrieve the beneficiary-identifiable data described previously in this section of the proposed rule. We propose that ETC Participants would be permitted to retrieve this data at any point during the relevant PPA Period. We considered establishing certain periods of time within a PPA Period during which the ETC Participant would be able to retrieve the data, but we concluded that permitting the ETC Participant to obtain the data at any point during the relevant PPA Period would be relatively operationally low-burden for CMS while providing additional flexibility to the ETC Participant.
CMS believes that it is important that the ETC Participant complete and submit its signed ETC Data Sharing Agreement, and retrieve the beneficiary-identifiable data, in the same form and manner (which we expect to be a web-based platform).
In the alternative, we considered providing the beneficiary-identifiable data to ETC Participants via paper mail rather than through a web-based Start Printed Page 36391platform, but we concluded that making the data available through a web-based platform would reduce administrative burden on both CMS and the ETC Participants. We also concluded that making this beneficiary-identifiable data available through a web-based platform would allow CMS to provide the data in a manner that is more secure than if CMS were to make the data available through paper mail. By using a web-based platform, to be further described by CMS through the ETC listserv and the ETC Model website, CMS would help ensure that only authorized users would be able to obtain the data, and would be able to implement a two-factor authentication to help ensure that no one other than an ETC Participant would have access to the data. In addition, we concluded that it would be more efficient to provide the ETC Data Sharing Agreement and the beneficiary-identifiable data itself through the same form and manner (which we expect to be a web-based platform), rather than using two different processes and that using a web-based platform would be more efficient than paper mail. For these reasons, we believe the best option would be for us to use only the web-based platform both for providing the ETC Data Sharing Agreement and for sharing data pertaining to the ETC Model.
We solicit public comment on our proposal to require the ETC Participant to complete and submit a signed ETC Data Sharing Agreement before the ETC Participant could retrieve the beneficiary-identifiable data, and on our proposal that the ETC Participant would be required to retrieve the beneficiary-identifiable data in the same form and manner as the ETC Participant receives and submits the ETC Data Sharing Agreement. We also solicit comment regarding our expectation that we will use a web based platform, rather than paper mail, for these purposes.
e. CMS Sharing of Aggregate Data
In addition to the proposed process for sharing beneficiary-identifiable data described previously in this section, we are proposing in § 512.390(b)(2) that CMS would make available certain aggregate data for retrieval by the ETC Participant, in a form and manner to be specified by CMS, no later than one month before each PPA Period. This aggregate performance data, would include, when available, the following information for each PPA Period, de-identified in accordance with 45 CFR 164.514(b): The ETC Participant's performance scores on the home dialysis rate, transplant waitlist rate, living donor transplant rate, and, if finalized, Health Equity Incentive; the ETC Participant's aggregation group's scores on the home dialysis rate, transplant waitlist rate, living donor transplant rate, and, if finalized, Health Equity Incentive; information on how the ETC Participant's and ETC Participant's aggregation group's scores relate to the achievement benchmark and improvement benchmark (that is, whether the ETC Participant met or exceeded the threshold for each such benchmark); and the ETC Participant's MPS and PPA for the corresponding PPA Period. CMS believes that sharing this aggregate, de-identified data with the ETC Participant would be important to help the ETC Participant better understand its performance in the ETC Model relative to its aggregation group and to the achievement and improvement benchmarks against which CMS is measuring the ETC Participant's performance. Whereas the beneficiary-identifiable data described previously in this section of the proposed rule would indicate which ESRD Beneficiaries and, if applicable, Pre-emptive LDT Beneficiaries the ETC Participant could devote greater resources to, CMS believes this aggregate, de-identified data would better enable the ETC Participant to see which performance rates the ETC Participant might need to improve to more generally improve its performance under the ETC Model.
We are proposing that CMS would make this data available to the ETC Participant for retrieval in a form and manner to be specified by CMS no less than one month prior to each PPA Period. We expect that CMS would make this data available to the ETC Participant on the same web-based platform on which CMS would be providing the beneficiary-identifiable data described previously in this section. The ETC Participant would be required to use the form and manner specified by CMS to retrieve this aggregate data, but would not have to agree to the ETC Data Sharing Agreement to retrieve this aggregated data, as it is not beneficiary-identifiable. We believe that using a web-based platform for sharing this aggregate data would be appropriate for the same reasons it would be appropriate for sharing the beneficiary-identifiable data. By using a web-based platform, CMS would help ensure that only authorized users would be able to obtain the data, and would be able to implement a two-factor authentication to help ensure that no one other than an ETC Participant would have access to the data. In addition, because CMS would be providing the ETC Data Sharing Agreement and beneficiary-identifiable data on the same web-based platform, we believe it would be convenient for the ETC Participant if CMS shared the aggregate data on the same web-based platform.
In the alternative, we considered sending this aggregate data to the ETC Participant via paper mail. However, CMS concluded that it would be more convenient to the ETC Participant to retrieve this data from a web-based platform rather than via paper mail, and that sending this data via paper mail would represent significant administrative and operational burdens for CMS.
We solicit public comment on our proposal to share aggregate data generally, to share aggregated data in the same form and manner we are proposing to use for sharing beneficiary-identifiable data. We also solicit public comment on our expectation to use a web-based platform for this purpose, as well as our considered alternative to share the aggregate data via paper mail.
8. Medicare Waivers and Additional Flexibilities
a. Background on Kidney Disease Patient Education Services Waiver
Pursuant to section 1861(ggg)(1) of the Act and § 410.48 of our regulations, Medicare Part B covers outpatient, face-to-face kidney disease patient education services provided by certain qualified persons to beneficiaries with Stage IV chronic kidney disease. As noted in the Specialty Care Models final rule, kidney disease patient education services play an important role in educating patients about their kidney disease and to help them make informed decisions on the appropriate type of care and/or dialysis needed for them (85 FR 61337). In addition, we noted in the Specialty Care Models final rule that kidney disease patient education services are designed to educate and inform beneficiaries about the effects of kidney disease, their options for transplantation, dialysis modalities, and vascular access (85 FR 61337). Because kidney disease patient education services have been infrequently billed, we found it necessary for purposes of testing the ETC Model to waive select requirements of kidney disease patient education services authorized in section 1861(ggg)(1) of the Act and in the implementing regulation at 42 CFR 410.48. Specifically, to broaden the availability of kidney disease patient education services under the ETC Model, we have used our authority under section 1115A(d) of the Act to waive certain requirements for Start Printed Page 36392individuals and entities that furnish and bill for kidney disease patient education services. We codified these waivers at § 512.397(b). These include waivers to allow more types of beneficiaries to have access to kidney disease patient education services, as well as greater flexibility in how the kidney disease patient education services are performed. For instance, CMS waived the requirement that kidney disease patient education services are covered only for Stage IV chronic kidney disease (CKD) patients to permit beneficiaries to receive kidney disease patient education services if they are diagnosed with CKD Stage V or are in the first 6 months of starting dialysis to receive the benefit. CMS also waived the requirements in section 1861(ggg)(2)(A)(i) of the Act and § 410.48(a) and (c)(2)(i) of the applicable regulations pertaining to the definition of “qualified person” such that registered dieticians/nutrition professionals, licensed clinical social workers, or a clinic/group practice may furnish kidney disease patient education services under the direction of, and incident to the services of a Managing Clinician who is an ETC Participant.
Finally, CMS waived two requirements relating to the content of kidney disease patient education services furnished to a beneficiary. CMS waived the requirement under § 410.48(d)(1) of our regulations that the content of kidney disease patient education services include the management of co-morbidities, including delaying the need for dialysis, when such services are furnished to beneficiaries with CKD Stage V or ESRD, unless such content is relevant for the beneficiary. In addition, CMS waived the requirement under § 410.48(d)(5)(iii) of our regulations that an outcomes assessment designed to measure beneficiary knowledge about chronic kidney disease and its treatment be performed during one of the kidney disease patient education services, requiring instead that such outcomes assessment is performed within 1 month of the final kidney disease patient education services session furnished by qualified staff.
b. Proposed Kidney Disease Patient Education Services Telehealth Waiver and Additional Flexibilities
Many changes took place in 2020 and early 2021 due to the COVID-19 PHE. Legislation enacted to address the PHE for COVID-19 provided the Secretary with new authorities under section 1135(b)(8) of the Act to waive or modify Medicare telehealth payment requirements during the PHE for COVID-19. We established several flexibilities to accommodate these changes in the delivery of care. Through waiver authority under section 1135(b)(8) of the Act, in response to the PHE for COVID-19, we temporarily waived the geographic and site of service originating site restrictions in section 1834(m)(4)(C) of the Act. For example, CMS waived the rural area requirement at section 1834(m) of the Act to allow for telehealth services, including kidney disease patient education services that can be furnished via telehealth, to be furnished to beneficiaries in any geographic area, regardless of location and in their homes, for the duration of the PHE. These waivers are set to terminate at the end of the COVID-19 PHE.
We believe that, once the PHE ends, these waivers removing the geographic and site of service originating site restrictions for kidney disease patient education services furnished via telehealth would be necessary solely for purposes of testing the ETC Model. Except under very limited circumstances, under section 1834(m) of the Act and its implementing regulations, the originating site where the beneficiary is located at the time a telehealth service is furnished is limited to certain, mostly rural, geographic locations and a site of service that is one of certain types of health care facilities. We believe that allowing qualified staff to furnish kidney disease patient education services via telehealth, regardless of the beneficiary's geographic area or the site of the beneficiary, and regardless of the site of service of the practitioner, would increase access to kidney disease patient education services for a few reasons. First, some beneficiaries may not have access to reliable transportation, especially those beneficiaries who suffered economically during the ongoing PHE, but may have access to the technology necessary for practitioners to furnish kidney disease patient education services. Moreover, some beneficiaries, even those with reliable transportation, may be more comfortable receiving kidney disease patient education services via telehealth rather than appearing in person after over a year of social distancing, even when it becomes safe according to Federal guidance for such beneficiaries to enter physical spaces with other individuals. This is especially likely to be the case for instances in which a practitioner would furnish kidney disease patient education services in a group session rather than an individual session. Increasing access to kidney disease patient education services is consistent with one of the main goals of the ETC Model, insofar as we believe that education, as delivered through kidney disease patient education services, helps improve beneficiary choice of dialysis modality.
In addition, we believe that removing beneficiary cost barriers for kidney disease patient education services would be helpful. As we demonstrate below, there is a significant relationship between household income or poverty status and kidney disease, and removing or mitigating cost barriers to access to kidney disease patient education services would likely increase the number of beneficiaries who would be willing to receive kidney disease patient education services.
We therefore propose that, starting in MY3, kidney disease patient education services may be furnished to certain beneficiaries via telehealth in a manner that is more flexible than that required under existing telehealth requirements. In addition, we propose to permit the reduction or waiver of coinsurance for the kidney disease patient education services, starting in MY3.
(1) Kidney Disease Patient Education Services Telehealth Waiver
CMS proposes to amend § 512.397 to add a waiver of certain telehealth requirements to provide qualified staff, as we are proposing to define for purposes of the ETC Model at § 512.310, the flexibility to furnish kidney disease patient education services via telehealth for the reasons described above. Specifically, we propose to waive the geographic and site of service originating site requirements in sections 1834(m)(4)(B) and 1834(m)(4)(C) of the Act, and in our regulations at 42 CFR 410.78(b)(3) and (4), for kidney disease patient education services furnished via telehealth. We believe the kidney disease patient education services telehealth waiver would allow more Medicare beneficiaries to receive kidney disease patient education services via telehealth by removing the originating site restrictions, thus allowing for the beneficiary to be located anywhere, and including at a site not specified in § 410.78(b)(3) of our regulations; and by allowing for the beneficiary to be located outside of a rural area. CMS also proposes to waive the requirement in section 1834(m)(2)(B) of the Act and 42 CFR 414.65(b) such that CMS would not pay an originating site facility fee for kidney disease patient education services furnished via telehealth to a beneficiary at a site not specified in § 410.78(b)(3) of our regulations under this proposed waiver, if finalized. Start Printed Page 36393However, we do not propose to waive the requirement under section 1834(m)(1) of the Act and 42 CFR 410.78(b) that telehealth services be furnished via an “interactive telecommunications system,” as that term is defined in § 410.78(a)(3) to mean multimedia communications equipment that includes, at a minimum, audio and video equipment permitting two-way, real-time interactive communication between the patient and distant site physician or practitioner. Accordingly, we would continue to require that the kidney disease patient education services furnished via telehealth be provided through an interactive telecommunications system; audio-only telehealth services would not be permitted.
We propose that kidney disease patient education services could be furnished via telehealth health only by qualified staff. We used the term “clinical staff” and “qualified staff” in the Specialty Care Models final rule, but did not provide definitions of these terms. For clarity, we now propose to define “clinical staff” and “qualified staff” in 42 CFR 512.310. We propose to define “clinical staff” to mean a licensed social worker or registered dietician/nutrition professional who furnishes services for which payment may be made under the physician fee schedule under the direction of and incident to the services of the Managing Clinician who is an ETC Participant. We are proposing to define the term clinical staff in this manner to describe those clinicians who are authorized to furnish kidney disease patient education services only pursuant to the waiver specified at § 512.390(b)(1)—namely licensed social workers and registered dieticians/nutrition professionals. The remaining clinicians currently specified in § 512.390(b)(1)—doctors, physician assistants, nurse practitioners, and clinical nurse specialists—fall within the existing definition of qualified person at 42 CFR 410.48(a). We therefore propose to define “qualified staff” to mean both clinical staff and any qualified person (as defined at § 410.48(a) of our regulations) who is an ETC Participant.
We seek comment on our proposal to waive the originating site requirements for telehealth services to allow qualified staff to furnish kidney disease patient education services via telehealth to a beneficiary regardless of where the beneficiary is geographically located such that kidney disease patient education services could be furnished via telehealth regardless of the beneficiary's location, including at a site not specified in § 410.78(b)(3) of our regulations. We further seek comment on our proposal to waive the originating site facility fee requirements such that CMS would not pay an originating site facility fee for kidney disease patient education services furnished via telehealth to a beneficiary at a site not specified in § 410.78(b)(3) of our regulations.
(2) Kidney Disease Patient Education Services Beneficiary Coinsurance Waiver
Available data and scholarly research suggest that there is a significant relationship between socioeconomic status and prevalence of CKD. For example, evidence suggests that CKD is more prevalent among individuals with lower income.[285] In addition, at least one study suggests that as an individual's CKD severity increases (for example, from CKD III to CKD IV), the likelihood of the CKD patient falling into poverty increases.[286] In light of this research, CMS believes that cost represents a meaningful barrier for beneficiaries in accessing kidney disease patient education services. While there does not appear to be any research that explicitly investigates to what extent cost barriers preclude access to kidney disease patient education services, the identified relationship between household income or poverty status and prevalence of CKD suggests that cost is an important factor when considering a beneficiary's access to kidney disease patient education services.
Under section 1833 of the Act, the amounts paid by Medicare for kidney disease patient education services are equal to 80 percent of the applicable payment amount; beneficiaries are thus subject to a 20 percent coinsurance for kidney disease patient education services. Kidney disease patient education services can be billed under G0420 for an individual session, or under G0421 for a group session. The current national unadjusted payment for G0420 under the CY2021 Physician Fee Schedule is $114.10; for G0421, it is $27.22. As such, a beneficiary would be required to pay $22.82 for an individual session of kidney disease patient education services or $5.44 for kidney disease patient education services furnished to a group, which may be higher or lower depending on certain factors, such as the geographic location of the beneficiary. Medicare covers up to six kidney disease patient education services for an individual beneficiary during that beneficiary's lifetime, meaning that a beneficiary may be required to pay $136.92 if six individual kidney disease patient education services are clinically appropriate for that beneficiary, or $32.64 if six group kidney disease patient education services are clinically appropriate for that beneficiary.
CMS believes that it is necessary, for purposes of testing the ETC Model, to permit ETC participants the flexibility to reduce or waive the 20 percent coinsurance requirement for kidney disease patient education services. We believe this patient incentive, if finalized, would increase the provision of kidney disease patient education services to beneficiaries, given the relationship between income or poverty and prevalence of CKD, and the relationship between kidney disease patient education services and progression of CKD. CMS has determined that, if this proposal were finalized, this CMS-sponsored patient incentive would advance the ETC Model's goal of increasing access to kidney disease patient education services, and to making beneficiaries more aware of their choices in preparing for kidney treatment, including the choice of receiving home dialysis, self-dialysis, or nocturnal in-center dialysis, rather than traditional in-center dialysis.
Accordingly, beginning January 1, 2022, we propose at § 512.397(c) to permit ETC Participants to reduce or waive the beneficiary coinsurance obligations for kidney disease patient education services furnished to an eligible beneficiary who does not have secondary insurance on the date the kidney disease patient education services are furnished if certain conditions are satisfied. We refer to this patient incentive herein as the “kidney disease patient education services coinsurance patient incentive.” As more fully explained below, we expect to make a determination that the anti-kickback statute safe harbor for CMS-sponsored model patient incentives (42 CFR 1001.952(ii)(2)) would be available to protect cost-sharing support that is furnished in compliance with ETC Start Printed Page 36394Model requirements with respect to kidney disease patient education services. If CMS makes such a determination, the safe harbor for CMS-sponsored model patient incentives would protect an ETC Participant, as that term is defined at § 512.310, who offers a reduction or waiver of coinsurance for kidney disease patient education services to beneficiaries who are eligible to receive kidney disease patient education services, including those eligible pursuant to the waiver described in § 512.397(b)(2), and who do not have secondary insurance on the date that the kidney disease patient education services were furnished.
We are proposing that the kidney disease patient education services coinsurance patient incentive would be available to the ETC Participant for kidney disease patient education services furnished by an individual or entity who is qualified staff. This proposal would align with the individuals who may furnish kidney disease patient education services under § 512.397(b) of this subpart, which are we replacing in its entirety to standardize certain terms and add clarity, as described in greater detail below.
We are proposing to limit the kidney disease patient education services coinsurance patient incentive to beneficiaries who do not have secondary insurance, as secondary insurance typically provides cost-sharing support of the type CMS is proposing in this proposed rule. We also believe that limiting the kidney disease patient education services coinsurance patient incentive to beneficiaries without secondary insurance would better ensure that only beneficiaries who need cost-sharing support would receive it, rather than permitting cost-sharing support for all beneficiaries for whom kidney disease patient education services are clinically appropriate.
We are also proposing that the kidney disease patient education services coinsurance patient incentive would be available only for kidney disease patient education services that were furnished in compliance with the applicable provisions of § 410.48 of our regulations, which includes a requirement that a beneficiary obtain a referral from the physician (as defined in section 1861(r)(1) of the Act) managing the beneficiary's kidney condition in order for the beneficiary to be eligible to receive kidney disease patient education services. We are proposing to include this requirement because we waived some but not all provisions of § 410.48, and we believe that the requirement that the beneficiary receive a referral from their physician is important for ensuring that kidney disease patient education services are furnished only to beneficiaries for whom it is clinically appropriate.
CMS proposes that such coinsurance support would be permitted for the kidney disease patient education services offered either in-person or via telehealth, and that it would be permitted for both individual sessions and group sessions. However, we are considering limiting the kidney disease patient education services coinsurance patient incentive to kidney disease patient education services furnished to an individual beneficiary, rather than allowing the kidney disease patient education services coinsurance patient incentive for kidney disease patient education services furnished either individually or to a group. The cost burden on beneficiaries who receive kidney disease patient education services in a group setting is much lower than it is on beneficiaries who receive kidney disease patient education services individually. However, we are concerned that any cost barrier to kidney disease patient education services, even if low, represents a meaningful barrier to some beneficiaries who would otherwise elect to receive such services. We solicit comments on this issue.
An ETC Participant that offers coinsurance support for kidney disease patient education services would be required to maintain records of certain information. Specifically, an ETC Participant that offers the kidney disease patient education services coinsurance patient incentive would be required to maintain records of the following: The identity of the qualified staff who furnished the kidney disease patient education services for which the coinsurance was reduced or waived; the date the kidney disease patient education services coinsurance patient incentive was provided; the identity of the beneficiary to whom the kidney disease patient education services coinsurance patient incentive was provided; evidence that the beneficiary who received the kidney disease patient education services coinsurance patient incentive was eligible to receive the kidney disease patient education services and did not have secondary insurance; and the amount of the kidney disease patient education services coinsurance patient incentive reduced or waived by the ETC Participant. We propose to require an ETC Participant that offers this kidney disease patient education services coinsurance patient incentive to maintain and provide the government with access to these records in accordance with 42 CFR 512.135(b) and (c) of this part.
We further propose in proposed 42 CFR 512.160(b)(6)(ii) that, for the ETC Model only, CMS could suspend or terminate the ability of an ETC Participant to offer the kidney disease patient education services coinsurance patient incentive if CMS determined that any grounds for remedial action exist pursuant to § 512.160(a).
In lieu of a waiver of certain fraud and abuse provisions in sections 1128A and 1128B of the Act, CMS may determine that the anti-kickback statute safe harbor CMS-sponsored model patient incentives (42 CFR 1001.952(ii)(2)) is available to protect the reduction or waiver of kidney disease patient education services coinsurance permitted under the ETC Model final rule, if issued. Specifically, we expect to determine that the CMS-sponsored model safe harbor will be available to protect the reduction or waiver of coinsurance that satisfies the requirements of such safe harbor and the provisions of proposed § 512.397(c)(1). We propose that, if we make this determination, we would specify in regulation text at § 512.397(c)(4) that the safe harbor is available.
We are also considering prohibiting on an ESRD facility or other entity from providing qualified staff or the ETC Participant with financial support to enable such qualified staff or ETC Participant to provide the kidney disease patient education services coinsurance patient incentive. CMS is concerned that permitting such financial support may encourage unlawful or abusive arrangements designed to induce or reward referrals for Federal health care program business. We solicit comments on whether this prohibition is a necessary to safeguard against fraud and abuse or if other laws effectively provide sufficient protection.
We also considered waiving Medicare payment requirements such that CMS would pay the full amount of the kidney disease patient education services furnished to a beneficiary who does not have secondary insurance, rather than just 80 percent of the amount. Under section 1115A(d)(1) of the Act, the Secretary may waive such requirements of titles XI and XVIII and of sections 1902(a)(1), 1902(a)(13), 1903(m)(2)(A)(iii) of the Act, and certain provisions of section 1934 of the Act as may be necessary solely for purposes of carrying out section 1115A of the Act respect to testing models described in section 1115A(b) of the Act. This is the authority under which we would waive Start Printed Page 36395such Medicare payment requirements. Under such a policy, Medicare would pay 100 percent of the payment amount for kidney disease patient education services furnished by Managing Clinicians who are ETC Participants to beneficiaries who do not have secondary insurance, and such beneficiaries would have no cost-sharing obligation for that benefit. However, we determined that this policy would likely represent too large an impact to the ETC Model's savings estimates, and thus would potentially jeopardize our ability to continue to test the ETC Model, if such a policy were finalized.
Given the policies proposed in this section related to programmatic waivers and additional flexibilities available under the ETC Model, we propose to modify the title of § 512.397 from “ETC Model Medicare program waivers” to “ETC Model Medicare program waivers and additional flexibilities.” We propose this change so that the section title would more accurately reflect the contents of the section if our proposed kidney disease patient education services coinsurance patient incentive is finalized.
We solicit public comments on our proposal to allow qualified staff, as we propose to define the term under § 512.310, to offer coinsurance support for kidney disease patient education services to beneficiaries who are eligible for such services, including those eligible under § 512.397(b)(2), and who do not have secondary insurance on the date the kidney disease patient education services are furnished. We also solicit comment on our proposal to require the ETC Participant to maintain and provide the government with access to records regarding the use of the kidney disease patient education services coinsurance patient incentive.
(3) Revising Language Providing Other ETC Model Medicare Program Waivers
We propose to revise § 512.397(b)(1) through (4) in their entirety to accomplish a few goals. First, we propose to make conforming changes throughout § 512.397(b) to the manner in which CMS discusses kidney disease patient education services. Currently, § 512.397(b) includes references to “KDE services,” “the KDE benefit,” “KDE sessions,” and, simply, “KDE.” CMS would change all of these references to “kidney disease patient education services” for clarity and to conform with the term used elsewhere in our regulations. In addition, we propose to make conforming changes through § 512.397(b) to the manner in which CMS discusses the individuals who are permitted to furnish kidney disease patient education services under the ETC model programmatic waivers. Specifically, as discussed previously, CMS is proposing to add definitions for “clinical staff” and “qualified staff” in this proposed rule, and CMS believes clarifying how CMS discusses these individuals in § 512.397(b) will enhance clarity. Finally, CMS is proposing to remove the “clinic/group practice” from the list of individuals or entities that are permitted to furnished kidney disease patient education services under the ETC Model programmatic waivers, and to remove the waiver of 42 CFR 410.48(c)(2)(i) from § 512.397(b)(1) of this part. CMS believes that its inclusion of clinic/group practices previously was in error; a clinic/group practice is not able to furnish or bill for kidney disease patient education services under existing law and CMS did not intend for the waiver described in § 512.397(b) to permit anyone other than a clinican to furnish kidney disease patient education services. Because the waiver of the requirements under 42 CFR 410.48(c)(2)(i) was implemented only to broaden the “qualified person” that could furnish kidney disease patient education services pursuant to § 512.397(b)(1) to include a clinic/group practice, we are proposing to remove references to 42 CFR 410.48(c)(2)(i) in § 512.397(b)(1) of this part.
We solicit public comments on these proposed changes to § 512.397(b) to make conforming and clarifying changes to the manner in which CMS discusses kidney disease patient education services and the individuals who are permitted to furnish kidney disease patient education services under the ETC Model waivers described in § 512.397(b), and to our proposed removal of “clinic/group practice” from the list of individuals or entities who may, under the ETC Model waivers described in § 512.397(b), furnish kidney disease patient education services.
C. Requests for Information (RFIs) on Topics Relevant to the ETC Model
This section includes several requests for information (RFIs). In responding to the RFIs, the public is encouraged to provide complete, but concise responses. These RFIs are issued solely for information and planning purposes; RFIs do not constitute a Request for Proposal (RFP), application, proposal abstract, or quotation. The RFIs do not commit the U.S. Government to contract for any supplies or services or make a grant award. Further, CMS is not seeking proposals through these RFIs and will not accept unsolicited proposals. Respondents are advised that the U.S. Government will not pay for any information or administrative costs incurred in response to this RFI; all costs associated with responding to these RFIs will be solely at the respondent's expense. Failing to respond to either RFI will not preclude participation in any future procurement, if conducted.
Please note that CMS will not respond to questions about the policy issues raised in these RFIs. CMS may or may not choose to contact individual respondents. Such communications would only serve to further clarify written responses. Contractor support personnel may be used to review RFI responses. Responses to these RFIs are not offers and cannot be accepted by the U.S. Government to form a binding contract or issue a grant. Information obtained because of this RFI may be used by the U.S. Government for program planning on a non-attribution basis. Respondents should not include any information that might be considered proprietary or confidential. All submissions become U.S. Government property and will not be returned. CMS may publicly post the comments received, or a summary thereof.
1. Peritoneal Dialysis Catheter Placement
The most common modality of home dialysis is peritoneal dialysis (PD). In order to perform PD, a beneficiary needs placement of a PD catheter. A PD catheter is a flexible plastic tube that enables dialysate to enter the abdomen for blood filtration purposes. The catheter is generally installed via outpatient surgery, as it is an invasive procedure.
However, CMS has heard concerns from numerous stakeholders about their ability to effectively get PD catheters installed in beneficiaries who may be otherwise interested in home dialysis. These stakeholders reported a variety of issues related to PD catheter placement, including the lack of availability of vascular surgeons to perform PD catheter placements, lack of appropriate operating room time, and a lack of training on PD catheter placement for vascular surgeons.[287] As many stakeholders have pointed out, the lack of timely PD catheter placement is a key barrier preventing many beneficiaries from being able to use PD as a dialysis modality.
Based on these issues, we seek feedback about how CMS can test and Start Printed Page 36396use Medicare payment policy, under the ETC model, to promote placement of PD catheters. Specifically, we are seeking feedback on the following questions:
- What are the key barriers to increased placement of PD catheters?
- How can CMS promote placement of PD catheters in a more timely manner?
- Should the Innovation Center use its authority to test alternative payment structures to address the barriers to PD catheter placement as a part of the ETC Model? If so, why and how?
2. Beneficiary Experience Measure
The ETC Model uses two ESRD facility quality measures; Standardized Mortality Ratio (SMR) (NQF #0369) and Standardized Hospitalization Ratio (NQF #1463). Both measures are currently calculated and displayed on Dialysis Facility Compare, a public reporting tool maintained by CMS. Because data collection and measure reporting are ongoing through claims, there is no additional burden to ETC Participants.
In the Specialty Care Models proposed rule, we considered including the In-Center Hemodialysis (ICH) Consumer Assessment of Healthcare Providers and Systems Survey (CAHPS)® survey to monitor beneficiary perceptions of changes in quality of care as a result of the ETC Model (84 FR 34565). However, the ICH CAHPS survey includes only beneficiaries who receive in-center dialysis, and specifically excludes the two beneficiary populations that the ETC Model focuses on: Beneficiaries who dialyze at home and beneficiaries who receive transplants.
We are considering the inclusion of a measure to capture the beneficiary experience of home dialysis care. The measure could be either an existing measure or one that CMS would develop. The measure could assess any aspect of the patient experience. The domains could include, but are not limited to, patient satisfaction, patient activation, and quality of life. If a new measure is developed, CMS would like to make it useful to other CMS kidney disease programs.
We seek comments on any aspect of a patient experience measure. Questions to consider include:
- What domains of a patient experience of care with home dialysis would be the most useful to assess and why?
- Would you prefer the measure to be newly developed or an update to an existing measure? If an update, which existing measure should be updated?
- How would a patient experience measure be best used to further the purpose of the ETC Model?
- How should CMS use a patient experience measure to assess the quality of care of beneficiaries?
- How should CMS use a patient experience measure to incentivize improved quality of care in the ETC Model and/or for other CMS programs?
While we will not be responding to specific comments submitted in response to this Request for Information, CMS intends to use this input to inform our future quality measure efforts.
CMS is considering publishing the quality outcomes for the ETC Model. While we seek comments on any aspect of reporting quality data, we specifically want input on the following:
- What is the frequency with which CMS should disseminate the results?
- What should be the unit of analysis for the reported data?
VI. Requests for Information
This section addresses several requests for information (RFIs). Upon reviewing the RFIs, respondents are encouraged to provide complete, but concise responses. These RFIs are issued solely for information and planning purposes; RFIs do not constitute a Request for Proposal (RFP), application, proposal abstract, or quotation. The RFIs do not commit the United States (U.S.) Government to contract for any supplies or services or make a grant award. Further, CMS is not seeking proposals through these RFIs and will not accept unsolicited proposals. Responders are advised that the U.S. Government will not pay for any information or administrative costs incurred in response to this RFI; all costs associated with responding to these RFIs will be solely at the interested party's expense. Failing to respond to either RFI will not preclude participation in any future procurement, if conducted.
Please note that CMS will not respond to questions about the policy issues raised in these RFIs. CMS may or may not choose to contact individual responders. Such communications would only serve to further clarify written responses. Contractor support personnel may be used to review RFI responses. Responses to these RFIs are not offers and cannot be accepted by the U.S. Government to form a binding contract or issue a grant. Information obtained because of this RFI may be used by the U.S. Government for program planning on a non-attribution basis. Respondents should not include any information that might be considered proprietary or confidential. All submissions become U.S. Government property and will not be returned. CMS may publically post the comments received, or a summary thereof.
A. Informing Payment Reform Under the ESRD PPS
Over the last several years, CMS, in conjunction with its contractor, has been conducting research, including holding three technical expert panels (TEPs), to explore possible improvements to the ESRD payment model. Additionally, in the CY 2020 ESRD PPS proposed rule (84 FR 38398 through 38400), CMS invited further comment on a number of topics, including expanding the outlier policy to include composite rate drugs, laboratory tests and supplies; reporting the length of each dialysis session directly on the ESRD claim; patient characteristics which contribute significantly to the cost of dialysis care; and improving the quality of facility-level data as reflected in the Medicare cost report. Stakeholders have asked CMS to explore a refined case-mix adjustment model for the ESRD PPS, stating that the existing case mix adjustors may not correlate well with the current cost of dialysis treatment.
Under section 632(b) of ATRA, as amended by section 217(a) of PAMA and section 204 of the ABLE Act, oral-only drugs cannot be incorporated into the ESRD PPS bundled payment until January 1, 2025. In order to provide payment for oral-only renal dialysis service drugs and biologicals under the ESRD PPS beginning January 1, 2025, as provided in 42 CFR 413.174(f)(6), we will need to propose refinements to the payment system through notice-and comment rulemaking. A refinement involves revising the patient and facility-level adjustments by changing the adjustment payment amounts based on updated regression analysis using more recent ESRD claims and cost report data. When refinements occur, due to the nature of regression analysis, all patient-level and facility-level adjustments are affected which can impact budget neutrality requirements and impact ESRD facilities differently than if adopted incrementally. Payment system changes can also require extensive efforts by CMS and health care providers to implement. Consequently, we believe CMS and ESRD facilities would best be served if these major payment methodology changes occur as a unified approach for CY 2025.
In order to obtain additional feedback from as wide of an audience as possible, we are soliciting comments from the Start Printed Page 36397public through this proposed rule. We are seeking comments from all perspectives, including differing beneficiary populations of ESRD facilities and ESRD facilities located in remote locations and their infrastructure issues. Obtaining a variety of perspectives enables CMS to ultimately work toward an improved payment methodology for the ESRD PPS that is both patient-data focused and accounts for the changing landscape in providing renal dialysis services to Medicare beneficiaries.
We encourage the public, and all stakeholders to provide comments and recommend approaches that will assist CMS in making refinements to the ESRD PPS through rulemaking in the future. We are soliciting comments this year so that we have time to consider them for potential proposals in the CY 2023 ESRD PPS proposed rule for a CY 2025 implementation.
B. Technical Expert Panels (TEPs)
CMS' contractor held three TEPs to discuss refinements to the ESRD PPS. The TEPs included panelists representing dialysis providers, independent researchers, patient advocates, and representatives from professional associations and industry groups. The first TEP held in 2018 explored the components of the existing ESRD PPS, and identified limitations of the current model. The TEP discussed topics such as current measures of ESRD PPS costs, costs associated with length of dialysis treatment, variations in cost associated with complex patients, facility level drivers of cost, and additional patient attributes necessary for developing a revised ESRD payment model. One of the main goals of the TEP was to identify items and services potentially appropriate for either itemized data collection on claims or improved reporting on the cost reports. The second TEP held in 2019 elaborated on the previous TEP's themes and focused on alternative approaches to measuring the cost of a dialysis session to better reflect treatment-level variation in cost. Topics included measurement of costs for determining case-mix adjustments, wage index, low volume payment adjustments and rural adjustments, TDAPA, outlier determinations, TPNIES, and home dialysis. The third TEP held in 2020 focused on aspects of the ESRD PPS for which refinements or enhancements were being considered. The topics discussed included adult and pediatric case-mix adjustments, low volume payment adjustments, the acute kidney injury payment system, and cost report revisions.
During each TEP, the data contractor presented to the panelists, and the panelists presented to all the TEP participants, innovative methodological approaches that addressed stakeholder concerns about the current payment model and presented alternative approaches with the goal of soliciting specific input for developing a more refined case-mix adjusted payment system. Panelists discussed potential approaches while weighing the ESRD facility burden those approaches may require. Alternative approaches were presented to solicit feedback from panelists about feasibility and acceptability of the options. The TEPs did not provide formal recommendations, but discussion items and suggestions were captured in three subsequent reports. The materials from the TEPs and summary reports can be found at https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ESRDpayment/Educational_Resources.
The following sections of this RFI provide information and solicit feedback specifically on the following topics: Low-volume payment adjustment (LVPA), calculations for case-mix adjustment, the calculation for the outlier payment adjustment, the current pediatric dialysis payment model, recommendations for ESRD PPS and hospital cost report modifications, recommendations for modifying the pediatric cost report, and home dialysis for Medicare beneficiaries with acute kidney injury. While TEP discussions are noted in each section, CMS encourages the public to reference the TEP reports on CMS' website, noted above, for more details.
C. Calculation of the Low-Volume Payment Adjustment (LVPA)
1. Background on the LVPA
Section 1881(b)(14)(D)(iii) of the Act provides that the ESRD PPS “shall include a payment adjustment that reflects the extent to which costs incurred by low-volume facilities (as defined by the Secretary) in furnishing renal dialysis services exceed the costs incurred by other facilities in furnishing such services, and for payment for renal dialysis services furnished on or after January 1, 2011, and before January 1, 2014, such payment adjustment shall not be less than 10 percent.”
In the CY 2011 ESRD PPS final rule (75 FR 49118 through 49125), we finalized the methodology used to target the appropriate population of ESRD facilities that were low-volume and to determine the treatment threshold for those facilities identified. After consideration of public comments, we established an 18.9 percent adjustment for facilities that furnish less than 4,000 treatments annually with the intention of encouraging small facilities to continue providing access to care.
In the CY 2016 ESRD PPS proposed rule (80 FR 37819), we analyzed ESRD facilities that met the definition of low-volume under § 413.232(b) as part of the updated regression analysis and found that the facilities still had higher costs compared to other facilities. A regression analysis of CYs 2012 and 2013 low-volume facility claims and cost report data indicated a multiplier of 1.239 percent; therefore, we proposed an updated LVPA adjustment factor of 23.9 percent in the CY 2016 ESRD PPS proposed rule (80 FR 37819) and finalized this policy in the CY 2016 ESRD PPS final rule (80 FR 69001). In CY 2019, 332 facilities received the LVPA and using the most recent available data for CY 2020, the number of facilities receiving the LVPA was 344 as of April 2021.
2. Current LVPA Methodology
Under § 413.232(b), a low-volume facility is an ESRD facility that, based on the submitted documentation: (1) Furnished less than 4,000 treatments in each of the 3 cost reporting years (based on as-filed or final settled 12-consecutive month costs reports, whichever is most recent) preceding the payment year; and (2) has not opened, closed, or received a new provider number due to a change in ownership in the three cost reporting years (based on as-filed or final settled 12-consecutive month cost reports, whichever is most recent) preceding the payment year.
In addition, under § 413.232(c), for purposes of determining the number of treatments furnished by the ESRD facility, the number of treatments considered furnished by the ESRD facility equals the aggregate number of treatments furnished by the ESRD facility and the number of treatments furnished by other ESRD facilities that are both under common ownership with, and 5 road miles or less from, the ESRD facility in question. In order to receive the LVPA, an ESRD facility must submit a written attestation statement to its Medicare Administrative Contractor (MAC) confirming that it meets all of the requirements specified in § 413.232 and qualifies as a low-volume ESRD facility. For purposes of determining eligibility for the LVPA, “treatments” mean total hemodialysis equivalent treatments (Medicare and non-Medicare). For peritoneal dialysis patients, one week of peritoneal dialysis is considered Start Printed Page 36398equivalent to two hemodialysis treatments (80 FR 68994). Section 413.232(e) imposes a yearly November 1 deadline for attestation submissions, with a few exceptions where the deadline is December 31. The November 1 timeframe provides 60 days for a MAC to verify that an ESRD facility meets the LVPA eligibility criteria (76 FR 70236). The ESRD facility would then receive the LVPA payment for all the Medicare-eligible treatments in the payment year. Once a facility is determined to be eligible for the LVPA, a 23.9 percent increase is applied to the ESRD PPS base rate for all treatments furnished by the facility (80 FR 69001).
In the CY 2021 ESRD PPS final rule (85 FR 71443), we finalized a policy to allow ESRD facilities flexibility for LVPA eligibility due to the COVID-19 PHE. Under § 413.232(g)(4), for purposes of determining ESRD facilities' eligibility for payment years 2021, 2022, and 2023, we will only consider total dialysis treatments for any 6 months of their cost-reporting period ending in 2020. ESRD facilities will attest that their total dialysis treatments for those 6 months of their cost reporting period ending in 2020 are less than 2,000. The attestation must further include that although the total number of treatments furnished in the entire year otherwise exceeded the LVPA threshold, the excess treatments furnished were due to temporary patient shifting resulting from the COVID-19 PHE. MACs will annualize the total dialysis treatments for the total treatments reported in those 6 months by multiplying by 2.
3. Current Issues and Stakeholder Concerns
ESRD facilities, the Medicare Payment Advisory Commission (MedPAC), and the Government Accountability Office [288] have recommended that we make refinements to the LVPA to better target ESRD facilities that are critical to beneficiary access to dialysis care in remote or isolated areas.[289] These groups have also have expressed concern that the strict treatment count introduces a “cliff-effect” that may incentivize facilities to restrict their patient caseload to remain below the 4,000 treatments per year for the LVPA threshold.[290]
In addition, we have heard from stakeholders that the eligibility criteria for the LVPA are very explicit and leave little room for flexibility in certain circumstances (85 FR 71442). Finally, some view the attestation process as burdensome to facilities and believe it may discourage participation by small facilities with limited resources that would otherwise qualify for the LVPA.[291] Given these concerns, we have been asked to consider alternative approaches to the LVPA that would reduce burden, remove negative incentives that may cause gaming, and better target facilities that are critical for beneficiary access.
4. Suggestions for Calculating the LVPA
a. Census Tract
During the 2020 ESRD PPS TEP, panelists discussed alternatives to the current LVPA. One methodology discussed utilized census tracts to identify geographic areas with low demand, which suggested increased beneficiary access by incentivizing dialysis organizations to continue operating facilities in otherwise non-viable locations.[292] As discussed during the TEP, an advantage to this approach would be a shift in the focus from identifying low volume facilities to identifying geographical areas, specifically census tracts, with low demand for dialysis.
This census tract methodology often results in a single facility being the only dialysis provider for a number of miles. The process would involve dividing the U.S. into geographic areas based on a reasonable assessment of ESRD beneficiaries' ability or willingness to travel. Latent demand is then calculated by counting the number of ESRD beneficiaries near each facility. “Near” is defined by driving time to facilities. Latent demand is calculated by multiplying the number of beneficiaries near an ESRD facility by average number of treatments for ESRD beneficiaries. The LVPA threshold is then applied by determining the threshold of adjusted latent demand. That is, those facilities, which fall below the threshold are LVPA eligible. The panelists noted that this methodology appears administratively simple and could eliminate the burden associated with the LVPA attestation process for facilities and MACs.
b. Low-Volume and Isolated (LVI) Adjustment
In its June 2020 report to Congress, MedPAC recommended that the Secretary replace the LVPA and rural adjustment under the ESRD PPS with a single payment adjustment, a low-volume and isolated (LVI) adjustment, in an effort to better protect isolated, low-volume ESRD facilities that are critical to ensure beneficiary access.[293] A determination that a facility is low volume and isolated would be based on that facility's distance from the nearest facility and its total treatment volume. MedPAC stated that the facilities that would receive the adjustment would be more appropriately targeted. This methodology would be accomplished via a single facility-level regression approach instead of the current two-regression approach utilized by CMS. As an example of how the LVI adjustment would more directly target isolated, low-volume dialysis facilities, the TEP compared the current LVPA and suggested LVI methodologies using 2017 data. In this example, 575 facilities would have been eligible for the LVI verses 1,734 facilities under the current LVPA and rural adjustment methodology.
5. Request for Information on Calculating the LVPA
CMS is considering alternative approaches to the LVPA that directly address stakeholder concerns, and is issuing a request for information to seek feedback on the approaches suggested above, other alternate approaches, and support of the current LVPA methodology. We are soliciting information that will better inform potential future modifications to the methodology. In addition to any other input the public wants to provide regarding the LVPA under the ESRD PPS, we are requesting responses to the following questions.
- Should a distinction other than census tract information be considered?
- What criteria should be used to determine the threshold(s) of adjusted latent demand (in treatment counts) which determine LVPA eligibility (for example, a threshold of high average cost per-treatment)?
- What are the concerns for facilities that would lose the LVPA under the LVI methodology?
- What are the concerns about the potential for gaming within the LVI methodology?Start Printed Page 36399
- To the extent that the LVI methodology captures more isolated (and most often rural) facilities, should a separate rural adjustment be maintained?
D. Calculation of the Case-Mix Adjustments
1. Background on the Case-Mix Adjustments
Section 1881(b)(14)(D)(i) of the Act mandates that the single payment system under the ESRD PPS implemented by the Secretary “shall include a payment adjustment based on case mix that may take into account patient weight, body mass index, comorbidities, length of time on dialysis, age, race, ethnicity, and other appropriate factors.” The ESRD PPS includes facility-level and patient-level adjustments to the base rate associated with resource utilization and the cost of providing dialysis treatment. The goal of case-mix adjustment is to ensure that payment for a dialysis treatment reflects expected resource use. Payment adjustments protect access to care for the most costly beneficiaries by mitigating financial disincentives to providing that care. The ESRD PPS is a case-mix adjusted, bundled payment model intended to reflect total treatment costs, which consist of formerly separately billable costs and composite rate costs (75 FR 49032). As required by section 1881(b)(14) of the Act, formerly separately billable services were included in the ESRD PPS bundled payment, effective January 1, 2011. Refinements to the current case-mix adjusters were implemented in the CY 2016 ESRD PPS final rule, effective January 1, 2016, and are currently in use.
2. Current Case-Mix Methodology
The current model uses two equations, including a patient-level equation for formerly separately billable costs and a facility-level equation for composite rate costs (75 FR 49083 through 49127). Formerly separately billable services are itemized on the ESRD Facility claim, (Type of Bill: 72x) and include injectable drugs and their oral equivalents plus certain laboratory tests and supplies. Composite rate services, which are captured on the cost report, constitute approximately 90 percent of a treatment's cost and include capital, labor, and administrative costs plus certain drugs, laboratory tests, and supplies (75 FR 49036; 84 FR 38396). Final case-mix adjusters for adults are the weighted average of estimated coefficients from these two equations (that is, patient level and facility level equations). Weights are the fraction of costs that are composite rate versus formerly separately billable. The regression equations and weighted averages are calculated using 2012 through 2013 claims and cost report data. Case-mix factors in the current model include age categories, body surface area (BSA), low body mass index (BMI) indicator, onset status, and comorbidities (that is, pericarditis, gastrointestinal tract bleeding, hereditary hemolytic or sickle cell anemia, and myelodysplastic syndrome) (80 FR 68989 through 68992). Facility adjusters include wage index, low volume status, and rural status (80 FR 68972 and 69001).
3. Current Issues and Stakeholder Concerns
Over the last several years, stakeholders have asked CMS to explore a refined case-mix adjustment model for the ESRD PPS, arguing that the existing case-mix adjustors may not correlate well with the current cost of dialysis treatment. They stated that:
- The current adult case-mix adjustors were calculated using old data (that is, 2012-2013 claims and cost report data);
- current adjustors may not align with resource-intensive patient-level services such as isolation rooms, behavioral issues, or neurocognitive issues;
- apportioned composite rate costs (such as labor and capital related costs), from the cost reports, used in the case-mix adjustment are currently only observable at the facility level and do not include patient or treatment level variations; and
- composite rate items are not individually collected on the claim, resulting in the payment not differentiating between the cost of hemodialysis verses peritoneal dialysis, which are affected by different labor and equipment costs.
Other stakeholders raised similar concerns during the TEP meetings. Additionally, panel members questioned the magnitude/significance of age, BMI, and BSA coefficients; the validity of taking weighted average of estimates across the two equations when the joint distribution of composite rate and formerly separately billable costs is not accounted for in the case-mix; and logistical challenges in obtaining the accurate diagnosis and comorbidity data that it is not routinely reported in the 72x claims.
In a comment letter to the Acting CMS Administrator on July 29, 2016,[294] MedPAC noted the current ESRD PPS does not have patient-level variation of composite rate (resource) costs and suggested CMS move to a “one-equation model” (that is, a patient-data focused model). MedPAC specifically stated that CMS should develop payment adjustment factors using a single-equation methodology that accounts for variation in the cost of providing the full PPS payment bundle. CMS is not currently able to implement this recommendation for the ESRD PPS because we do not have data on the charges associated with the components of dialysis treatment costs that vary across patients in the use of the formerly composite rate services.
4. Suggestions for Allocating Composite Rate Costs
CMS has been carefully studying MedPAC's suggestion to base the ESRD PPS on a “one-equation model” (that is, a patient-data focused model). CMS has over the years publicly discussed potential changes with our stakeholders who support a patient-data focused model. For instance, during the 2018 and 2019 TEP meetings discussions included using time on machine to address allocation of composite rate costs, case mix, and patient level adjustments. Time on machine would not be used to directly adjust payment; rather, it would be used to apportion composite rate costs (such as labor and capital-related costs) that are currently only observable at the facility level to the patient or treatment level for use in the case-mix adjustment. Data on the time on machine receiving dialysis would allow for a proportionately higher amount of composite rate costs to be allocated to patients with longer dialysis treatment times. During the December 2019 TEP, a panelist indicated that this option would reduce burden since dialysis treatment time (that is, time on machine) is automatically generated by the dialysis machine and easily entered into the patient's medical record. Under this option, a single aggregate number would be reported on each claim. That number corresponds to the total number of minutes the beneficiary spent on dialysis during that claim period. A panelist noted that reporting a single number would minimize provider burden. Panelists reached consensus that the reporting of actual time on Start Printed Page 36400machine offered the best solution for capturing patient-level differences in the cost of dialysis sessions and would be superior to the current case-mix adjusters.
We included discussions about expanding the data elements, moving to a patient-data focused model, and the use of time on machine to determine patient level variation in dialysis treatment costs in the CY 2019 ESRD PPS final rule (83 FR 56963 through 56970) as well as the CY 2020 ESRD PPS proposed rule (84 FR 38396 through 38400) A comment letter from a large dialysis organization in response to the CY 2019 ESRD PPS proposed rule stated that costs in the remaining category—wages, salaries, and benefits—account for nearly 40 percent of the market basket weight. Additionally, the large dialysis organization noted that these costs represent the majority of expenses associated with dialysis treatment and will vary by patient because they are dependent on dialysis treatment times. The large dialysis organization stated that time on machine was a good proxy for costs in dialysis.
Based on information gathered from our stakeholders and panelists from the first two TEP meetings and comments received based on RFIs in the CY 2020 ESRD PPS proposed rule, CMS took steps towards developing a patient-data focused model. Based on stakeholder input, CMS chose to utilize time on machine to determine patient level variation in dialysis treatment costs. In order to collect this information from ESRD facilities, CMS petitioned the National Uniform Billing Committee (NUBC) for a new value code for time on machine. This value code allows CMS to add time on machine to the ESRD claim. In April 2020, NUBC approved the request. CMS included a requirement to collect time on machine data effective January 1, 2021 in two technical direction letters and two Medicare Learning Network articles. CMS later rescinded the time on machine requirement,[295] but we are discussing this potential requirement in this RFI as a possible future refinement of the ESRD PPS to address allocation of composite rate costs, case mix, and patient level adjustments.
During the 2020 TEP, the data contractor for CMS presented and the panelists discussed potential refinement to concerns regarding the current case-mix adjustment. One of the refinements discussed was collecting time on machine data on the 72x claim using a value code. Specifically, the suggested method includes the costs per beneficiary-facility-month which are the sum of formerly separately billable costs, directly calculated from claims (quantities) and from Part B prices, and composite rate costs for each beneficiary-facility-month, calculated by allocating annual facility costs (less formerly separately billable costs) to the beneficiary-facility-month level using time on machine (duration of all treatments). For some modalities and settings, time on machine is not available and must be imputed. Finally, a regression is run of beneficiary-facility-month costs on case-mix adjusters and facility characteristics. Following a presentation by the data contractor, the panelists agreed that this method would identify a magnitude of factors that best reflect variation in this measure of total cost per treatment. This method would select a set of case-mix adjusters that account for a significant portion of the variance of total costs, subject to intuitive clinical relationship to dialysis treatment costs, reasonable number of risk adjusters, easy to diagnose, identify, or report, and not gameable.
Panelists at the TEPs and stakeholder comments received in response to the CY 2019 ESRD PPS proposed rule believe this one-equation model is more intuitive than current ESRD PPS case-mix adjusters.[296] The suggested case-mix adjusters discussed during the December 2019 and 2020 TEPS are derived relative to variation in total cost of case and that the change in reporting burden is small and would change claims in two ways, including reporting total machine reported treatment minutes and reporting codes for new comorbidities. Finally, stakeholders believe that a magnitude of case-mix adjusters appears to be significantly attenuated relative to the existing ESRD PPS adjusters. As discussed in the TEP Report for the December 2020 TEP,[297] a budget neutral implementation of such a system would result in a 5-10 percent increase in the base rate. Options discussed by the panelists included the one-equation model and keeping the current ESRD PPS case-mix adjustments. CMS is seeking feedback from the public on these options and any additional approaches not yet considered.
5. Request for Information on Calculation of the Case-Mix Adjustments
CMS welcomes the opportunity to inform the public and solicit stakeholder feedback on potential changes to the modeling used to develop the case-mix payment adjustments under the ESRD PPS, in order to inform future model refinements. CMS is considering alternative approaches to calculating the case-mix adjustment that directly address stakeholder concerns, and more appropriately reflects resource use and costs, and is issuing this RFI both to seek feedback on the suggested approach discussed previously, and to solicit information that will better inform future modifications to this methodology. In particular, we are soliciting comments on the methodology to collect data to reflect patient-level differences in composite rate costs, including the use of a value code to collect time on machine on the claim. In addition to any other input the public wants to provide regarding the calculation of the case-mix adjustment, we are requesting responses to the following questions.
- Which of the five composite rate cost components (that is, age, BSA, BMI, onset of dialysis, comorbidities) are most likely to vary with treatment duration?
- Should new information for these cost components be collected on cost reports, for use in better inferring the composite rate costs associated with treatment duration?
- What are the advantages and disadvantages of obtaining treatment duration information from blood urea nitrogen time on dialysis through the End Stage Renal Disease Quality Reporting System (EQRS) (our new system that has replaced the Consolidated Renal Operations in a Web-enabled Network (CROWNWeb)), versus collecting treatment duration through new fields on claims?
- What challenges would be encountered in reporting treatment duration on claims, using one of the options discussed?
- Are there alternative proxies for resource utilization that can be reported at the patient/treatment level?
E. Calculation of the Outlier Payment Adjustment
1. Background on the Outlier Payment Adjustment
Section 1881(b)(14)(D)(ii) of the Act requires that the ESRD PPS include a Start Printed Page 36401payment adjustment for high-cost outliers due to unusual variations in the type or amount of medically necessary care, including variations in the amount of ESAs necessary for anemia management. As discussed in section II.B.1.c of this proposed rule, we recognize that the utilization of ESAs and other outlier services have continued to decline under the ESRD PPS, and that we have lowered the MAP amount and FDL amounts every year under the ESRD PPS. As discussed in the CY 2021 ESRD PPS final rule (85 FR 71439), we acknowledge that, even with annually adjusting the MAP and FDL to reflect the most recent utilization and costs of ESRD PPS eligible outlier services, total outlier payments have not yet reached the 1 percent target.
2. Current Outlier Payment Adjustment Methodology
The current outlier policy was implemented in the CY 2011 ESRD PPS final rule (75 FR 49134 through 49145) and codified at § 413.237. Under § 413.237, an ESRD facility will receive an outlier payment if its actual or imputed Medicare Allowable Payment (MAP) amount per treatment for ESRD outlier services exceeds a threshold. The MAP amount represents the average incurred amount per treatment for services that were or would have been considered separately billable services prior to January 1, 2011. The threshold is equal to the ESRD facility's predicted ESRD outlier services MAP amount per treatment (which is case-mix adjusted) plus the FDL amount, set each year by CMS.[298] The predicted outlier service MAP amount is the outlier MAP amount published by CMS adjusted for the case mix in the payment year; that is, it is calculated by multiplying the separately billable case mix multipliers by the outlier MAP amount. The outlier MAP and FDL amounts are estimated using the most recent, complete data set available, which are data from 2 years prior to the payment year in question.
The predicted outlier MAPamounts and FDLs create thresholds where, if the outlier MAP amount per treatment on the claim is above the threshold, there will be a per-treatment outlier payment equal to 80 percent of the amount exceeding the threshold. The loss-sharing percentage was set at 80 percent in the CY 2011 ESRD PPS final rule (75 FR 49144) to make it consistent with the loss-sharing percentages in other Medicare payment systems.
In the CY 2011 ESRD PPS final rule and codified in § 413.220(b)(4), using 2007 data, we established the outlier percentage, which is used to reduce the per treatment base rate to account for the proportion of the estimated total payments under the ESRD PPS that are outlier payments, at 1.0 percent of total payments (75 FR 49142 through 49143).
The policy provides that the following ESRD outlier items and services are included in the ESRD PPS bundled payment: (1) Renal dialysis drugs and biological products that were or would have been, prior to January 1, 2011, separately billable under Medicare Part B; (2) Renal dialysis laboratory tests that were or would have been, prior to January 1, 2011, separately billable under Medicare Part B; (3) Renal dialysis medical/surgical supplies, including syringes, used to administer renal dialysis drugs and biological products that were or would have been, prior to January 1, 2011, separately billable under Medicare Part B; (4) Renal dialysis drugs and biological products that were or would have been, prior to January 1, 2011, covered under Medicare Part D, including renal dialysis oral-only drugs effective January 1, 2025; and (5) Renal dialysis equipment and supplies that receive the transitional add-on payment adjustment as specified in § 413.236 after the payment period has ended. Beginning January 1, 2021, calcimimetics became outlier services (85 FR 71405).
In the CY 2011 ESRD PPS final rule (75 FR 49064 through 49065), CMS explained that it estimates an ESRD facility's costs based on most recent available data. Since the rulemaking is done in the year prior to the effective date, the most complete available data would be from the year before. This means that for CY 2022 (as discussed in section II.B.1.c of this proposed rule), CMS is proposing to recalibrate the outlier MAP and FDL amounts for each calendar year using data from 2 years prior, which is the most recent and complete claims data. This methodology assumes consistent utilization over time, that is, it assumes that 2020 utilization rates for ESRD PPS outlier items and services are the same as those for 2018. However, the use of ESRD PPS outlier items and services has in fact declined each year since the implementation of the ESRD PPS.
For example, the CY 2020 FDL amount ($48.33 for adult patients) was calculated and added to the predicted MAP to determine the outlier thresholds using 2018 data. However, ESRD PPS outlier spending continued to fall from 2018 to 2020. Consequently, outlier payments for CY 2020 claims comprised only 0.6 percent of total ESRD PPS payments, demonstrating that the use of 2018 data results in thresholds too high to achieve the targeted 1.0 percent outlier payment. Outlier payments for the adult population have constituted less than 1.0 percent of total ESRD PPS payments since such payments began in 2011.[299]
3. Current Issue and Stakeholder Concerns
As the outlier payments have consistently landed below the targeted 1.0 percent of total ESRD PPS payment threshold, stakeholders have noted that the methodology currently used to calculate the outlier results in underpayment to the providers, as money was removed from the base rate to balance the outlier payment (85 FR 71409, 71438 through 71439; 84 FR 60705 through 60706; 83 FR 56969). Therefore, they have urged us to adopt an alternative modeling approach, one that accounts for declining trends in outlier-eligible items and services spending over time. MedPAC echoed these concerns in a comment letter in response to the CY 2021 ESRD PPS proposed rule, where it also suggested that the introduction of calcimimetics as outlier-eligible items could perpetuate the pattern of underpayment. MedPAC stated that if calcimimetic use decreases between 2019 (when the products were paid under the ESRD PPS using the TDAPA) and 2021 (when the products will be paid as part of the ESRD PPS base rate), the outlier threshold will be set too high, and outlier payments will be lower than the 1 percent of total 2021 payments.
4. Suggestions for Outlier Payment Adjustment
During the second and third annual TEP meetings convened by the CMS contractor in 2019 and 2020, panelists discussed concerns regarding the current outlier adjustment policy and alternative methodologies to achieve the 1 percent outlier target. Some TEP panelists and stakeholders have strongly advocated that we establish a new outlier threshold using alternative modeling approaches that account for trends in separately billable spending over time. Overall, panelists expressed support for any change to outlier calculations that result in total outlier payments closer to the target.Start Printed Page 36402
Panelists noted that the underlying basis of an alternative methodology could be to re-examine the assumption of constant utilization over time. Unlike the current outlier methodology that predicts FDL amounts using a single year of claims data, this approach allows for the modeling of the MAP amounts as they change over a longer period of time. CMS has received a number of suggested techniques that could be employed to reach the 1.0 percent target more predictably.
One of these suggestions is a calculation of “after the fact” FDLs that would achieve the 1.0 percent outlier target for each year included in the FDL calculation. This has been referred to as the retrospective FDL, which would be lower than the FDLs published in the final rule for each corresponding year. This calculation would be used for future outlier calculations. For more information, please refer to the TEP reports here: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/ESRDpayment/Educational_Resources.
Data presented during the TEP meeting showed that using the three most recent years to simulate FDLs and outlier payments for 2020 resulted in an FDL amount for adults of $33.83 and a MAP amount of $37.41, respectively. By contrast, the 2020 FDLs and MAPs published in the CY 2020 ESRD PPS final rule (84 FR 60649) were $48.33 and $35.78, respectively. The simulated outlier percentage for 2020 using the alternative methodology was 0.8 percent. The actual outlier payment percentage made for 2020 claims was 0.6 percent. Therefore, the alternative methodology results in an outlier percentage that is closer to the 1.0 percent target in the adult population.
6. Request for Information
CMS is considering potential revisions to the calculation of the outlier threshold to address stakeholder concerns, and is issuing a request for information both to seek feedback on the approach suggested above, and to solicit information that will better inform future modifications to the methodology. In addition to any other input the public wants to provide for calculating the outlier payment adjustment, we are requesting responses to the following questions.
- An alternative approach could be to estimate the retrospective FDL trend by using historical utilization data. The example above was constructed by using 2016-2018 data. There is flexibility in the time used to estimate this trend. The data must contain at least 2 years' worth of claims data and may begin as early 2011. Additionally, it must end with the most recent year with complete data (typically 2 years before the year in which the FDL will take effect).[300]
++ How many years of data should be included in calculation of this trend to best capture changes in treatment patterns?
- The simulation of the FDL can be improved by better anticipating changes in utilization of ESRD outlier services. What are the factors that affect the use of ESRD outlier services over time, and to what extent should CMS try to forecast the effect of these factors?
- ESRD beneficiaries can now choose to enroll in Medicare Advantage.
++ Please describe any anticipated effects of this enrollment change on the use of ESRD outlier services in the ESRD PPS.
- Adoption of the suggested methodology may account for systematic changes in the use of high-cost outlier items. However, inherently unpredictable changes may still push the outlier payment off the 1.0 percent target.
++ Please comment on the acceptability of the below payment adjustment methods.
++ Payment reconciliation—in the form of an add-on payment adjustment or a payment reduction—might be necessary to bring payments in line with the 1 percent target.
++ An add-on payment adjustment would be distributed after sufficient data reveal the magnitude of the deviation (1 year after the end of the payment year). The distribution of these monies could be done via a lump sum or via a per-treatment payment add-on effective for 1 year. This add-on payment adjustment would be paid irrespective of the outlier claim status in that year.
++ A payment reduction could take the form of a reduction in the base rate, also to be applied 1 year after the end of the payment year.
F. Calculation of the Pediatric Dialysis Payment Adjustment
1. Background on the Pediatric Dialysis Payment Adjustment
Section 1881(b)(14)(D)(iv)(I) of the Act provides that the ESRD PPS may include such other payment adjustments as the Secretary determines appropriate, such as a payment adjustment for pediatric providers of services and renal dialysis facilities. Below we discuss the current ESRD PPS with regard to ESRD facilities that furnish renal dialysis services to pediatric patients, and request information on specific approaches as well as other topics related to developing a pediatric payment adjustment under the ESRD PPS.
Prior to implementation of the ESRD PPS, payment for dialysis treatments was made through a composite rate per treatment that was based on cost report data and did not account for differences among patients with ESRD (48 FR 21254). The initial payment rates were established at $127 per treatment for independent facilities and $131 for hospital-based facilities, which reflect the costs incurred by dialysis facilities furnishing outpatient maintenance dialysis, including some routinely provided drugs, laboratory tests, and supplies, whether furnished by hospital-based and independent facilities in a facility or at home.
In addition, we provided a process under which facilities with costs per treatment in excess of their composite rates could seek exceptions to those rates under specified circumstances in §§ 413.182 and 413.184. For example, when a substantial proportion of the facility's outpatient maintenance dialysis treatments involve atypically intense dialysis services, special dialysis procedures, or supplies necessary to meet special medical needs of the facility's patients could qualify for an exception rate. Under § 413.182, CMS could approve exceptions if the facility demonstrates, by convincing objective evidence, that its total per treatment costs are reasonable and allowable under the relevant cost reimbursement principles of part 413 and that its per treatment costs in excess of its payment rate are directly attributable to its patient mix. As a result of these provisions, many pediatric facilities secured an exception rate and were paid the exception rate until the transition to the ESRD PPS ended in CY 2014.
Section 1881(b)(12) of the Act, added by section 623(d) of the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (MMA) required the Secretary to implement a basic case-mix adjustment to an ESRD facility's composite payment rate reflecting a limited number of patient characteristics. On August 5, 2004 and November 15, 2004, we published a proposed rule and final rule with comment period (69 FR 47487 through 47730 and 69 FR 66235 through 66915), respectively, implementing the provisions affecting the composite payment system. The development and Start Printed Page 36403application of the basic case-mix adjustments, using regression-based adjustment factors for the patient variables of age, BSA and BMI are explained in each of those rules (69 FR 47529 through 47531 and 69 FR 66323 through 66324, respectively). The product of the specific adjusters for each patient, multiplied by the otherwise applicable composite payment rate, yielded the basic case-mix adjustment as required by statute. The basic case-mix adjusted composite payment system was effective April 1, 2005 and continued until the ESRD PPS was implemented on January 1, 2011.
As we explained in the CY 2005 ESRD PPS final rule with comment period (69 FR 66326 through 66327), we attempted to develop case-mix adjusters for outpatient patients with ESRD under age 18. However, we found that for the approximately 600 Medicare pediatric patients for whom claims were available from 2000 through 2002, the results were highly variable and statistically unstable, and therefore, inappropriate for the development of case-mix adjusters in accordance with the same methodology otherwise applicable to adult Medicare patients with ESRD.
For this reason, we described an alternative methodology we used to develop a 62 percent pediatric increase (that is, an adjustment factor of 1.62) applied to the composite payment rate per treatment for any facility furnishing outpatient dialysis services to pediatric patients. That factor was based on the average amount of the atypical services exceptions granted for 20 ESRD facilities, each of which sought and received an exception for the atypical costs incurred for the treatment of outpatient pediatric patients, compared to the average unadjusted composite payment rate (that is, the payment without regard to exception amounts) for these same 20 facilities. We explained that application of the pediatric adjustment factor of 1.62 in lieu of an explicit pediatric case-mix adjustment was temporary, and would be eliminated once an appropriate methodology, preferably one applicable to both pediatric and adult Medicare patients, could be developed.
In the CY 2011 ESRD PPS proposed rule (74 FR 49986 through 49987), we proposed a pediatric payment methodology with comorbidity adjusters. However, in the CY 2011 ESRD PPS final rule (75 FR 49130 through 49134), in response to public comments, we explained that instead of using the regression-based composite rate multiplier of 1.199, we established the pediatric payment adjusters using the overall difference in average payments per treatment between pediatric and adult dialysis patients for composite rate services in CY 2007 based on the 872 pediatric dialysis patients reflected in the data. That is, the average CY 2007 MAP for composite rate services for pediatric dialysis patients was $216.46, compared to $156.12 for adult patients. We used CY 2007 data consistent with our determination that 2007 represented the year with the lowest per patient utilization of dialysis services in accordance with section 1881(b)(14)(A)(ii) of the Act. We developed payment adjusters using the variables of age (that is, <13 and 13-17) and modality (peritoneal dialysis or hemodialysis).
In the CY 2016 ESRD PPS final rule (80 FR 68968), we refined the ESRD PPS in accordance with section 632(c) of ATRA, which required CMS to conduct an analysis and make appropriate revisions to the case mix payment adjustments. We analyzed the case-mix payment adjustments under the ESRD PPS and revised the payment adjusters using CYs 2012 and 2013 ESRD claims and cost report data. For pediatric dialysis, we used the same methodology that was used for the CY 2011 ESRD PPS final rule, except for the use of more recent data years (2012 through 2013) and in the method of obtaining payment data. Specifically, we used the projected MAP based on 2013 claims to calculate the ratio of pediatric total MAP per session to adult total MAP per session. The resulting adjustment factors reflected an 8.21 percent increase to account for the overall difference in average payments per treatment for pediatric patients. The pediatric adjusters that were finalized for CY 2016 and are currently in effect are:
<13 peritoneal dialysis = 1.063
<13 hemodialysis = 1.306
13-17 peritoneal dialysis = 1.102
13-17 hemodialysis = 1.327
2. Current Issues and Stakeholder Concerns
Since 2015, we have continued to hear from organizations associated with pediatric dialysis about the undervaluation of pediatric ESRD care, which requires significantly different staffing and supply needs from those required to deliver ESRD care to adults. These organizations support CMS efforts to explore ways to improve collecting pediatric-specific data to better characterize the necessary resources and associated costs of delivering pediatric ESRD care. Commenters have also suggested that we reinstate the exceptions process that would provide individual hospitals and ESRD facilities with their own payment rate based on their costs. We note that this approach would require a statutory change because section 1881(b)(14)(A)(i) of the Act requires the Secretary to implement a payment system under which a single payment is made to all ESRD facilities.
Stakeholders have informed us that costs unique to pediatric dialysis are not adequately captured in current cost reports or claims, and therefore are not accounted for in the pediatric adjustments. In addition, they have explained that pediatric dialysis often requires developmental and behavioral specialists, pediatric dieticians, and social workers, and that pediatric comorbidities require unique specialized care. Further, pediatric nephrologists have told CMS that pediatric patients disproportionately receive treatment in hospital-based facilities, but the hospital cost report (CMS Form 2552-10) does not distinguish pediatric and adult dialysis cost.
One organization suggested that we expand the pediatric age groups and create either pediatric modifiers or a pediatric add-on payment by age group. Alternatively, the organization suggested that we create a pediatric-specific ESRD bundle that would allow for full accounting of costs for pediatric staffing and specialized equipment, and the economic implications of pediatric medical comorbidities that are not addressed in the current PPS. In order to engage dialysis stakeholders in advance of rulemaking, CMS' data contractor conducted TEP discussions for the past three years on various dialysis payment approaches and issues. For the 2020 TEP, one of the discussion topics was pediatric dialysis. Based on discussions and meetings with stakeholders and TEP panelists, the contractor performed several analyses on pediatric dialysis to inform the TEP discussion. The analyses confirmed many of the challenges reflected in stakeholder comments regarding pediatric dialysis.
For example, a small number of facilities provide 95 percent of pediatric dialysis treatments (approximately 100) and those pediatric facilities are hospitals, mostly children's hospitals. Pediatric treatments are split between home peritoneal dialysis (mostly for children younger than 13) and in-center hemodialysis (for older children 13-17). One analysis, using cost report data, found that the median registered nurse/licensed practical nurse hours per-treatment is higher in pediatric facilities and pediatric comorbidities require more (specialized) staffing. Dialysis for Start Printed Page 36404pediatric patients is furnished in hospitals, primarily children's hospitals or in large dialysis organization facilities. For more information, please refer to the TEP reports.
The contractor performed analyses using the expanded age groupings suggested by the commenters and found that finer stratification of the age groups reveals differences in cost per treatment. The contractor found that the median cost per treatment for the pediatric population using the same methodology used in the 2016 refinement but using more recent data (2018 and 2019) resulted in significant differences in cost among the pediatric age categories. The contractor also found that the median cost per treatment for the pediatric population using the national average treatment duration, the relationship between total cost per-treatment and age is consistent with stakeholder comments.
3. Suggestions for the Pediatric Dialysis Payment Adjustment
During the December 2020 TEP, three approaches were discussed among the panelists that could potentially lead to a more accurate estimate of pediatric dialysis costs under a revised payment model: (1) The addition of pediatric-specific case-mix adjustment multipliers; (2) the creation of a separate payment bundle for pediatric ESRD treatment costs; and (3) revisions to current data collection practices.
To illustrate how the refined model would incorporate the pediatric population, the contractor applied the model using each of the two current age groupings, resulting in an increased effect of age on costs, with multipliers of 1.61 and 1.74 for age <13 years and age 13 to 17 years, respectively, compared to the reference adult population. Please refer to the TEP report [301] for more specific information on the analyses and discussion.
Stakeholders suggest that the variables affecting pediatric dialysis costs are sufficiently different from those associated with adult dialysis costs, and that a separate payment system may be warranted. Although the creation of a pediatric bundle or separate pediatric ESRD PPS may improve cost estimates for the pediatric population, if there were a statutory change to authorize this separate payment system, the time required for implementation would be substantial due to the subsequent need for new, pre-implementation data collection, which providers may find burdensome.
The TEP panelists also discussed several modifications to the cost reports that they believe would better capture resources utilized in the pediatric dialysis setting. These include adding lines itemizing pediatric specific labor categories and pediatric specific supplies, clarifying cost report instructions as they pertain to pediatric dialysis, and better aligning the freestanding facility cost report with the hospital cost report. Although these changes have the advantage of being highly feasible to implement, stakeholders have noted that uptake may take additional time, as pediatric facility accounting and billing staff are not generally familiar with Medicare cost reports. Furthermore, stakeholders have noted that changes to the freestanding facility cost report would be of limited value, since pediatric dialysis primarily takes place in hospital-based facilities.
Panelists generally favored the addition of pediatric case-mix adjustment multipliers. One panelist noted that prior to the current case-mix adjustment; the multiplier applied to pediatric facilities was based on actual costs incurred during treatment that were more accurate than the costs being reported currently. The case-mix adjustment multipliers presented during the TEP were similar to the multipliers from the prior payment method, which the panelist found encouraging.
However, there was shared concern among TEP panelists that there will continue to be underpayment for pediatric dialysis patients. One panelist noted that time on dialysis may not accurately reflect all costs, and may be especially misleading for those under 2 years of age. For this patient population, expenditures on some fixed costs (for example, dialysate) will decrease, but staffing costs would be considerably higher, as they require one-on-one nursing and child life specialists and are more difficult to initiate on dialysis. Therefore, panelists expressed the concern that the multipliers based on duration of treatment would not accurately reflect costs. Another panelist noted that certain state laws with personnel requirements for pediatric dialysis could also increase costs.
Panelists supported moving forward with the cost report and case-mix multiplier modifications due to the burden of implementing a new bundle. One panelist noted that a time and motion study attempted by their dialysis organization failed, as there was a high degree of variation among facilities. However, another panelist described their facility's success in securing additional funding for their pediatric dialysis unit as a result of a time and motion study.
Panelists affirmed that accounting and billing departments at children's hospitals are not well equipped to accurately complete Medicare cost reports and suggest that this may be due both to their general lack of familiarity with Medicare (one panelist noted that only 30 percent of pediatric patients are Medicare beneficiaries) and the cost report's current structure.
One panelist cautioned that because most pediatric dialysis is delivered in the hospital setting, if the revised hospital cost report does not include the modifications recommended for the dialysis facility's cost report, pediatric expertise for dieticians, social workers, child life specialists, and behavioral specialists may remain overlooked. Despite this, panelists expressed the desire to move forward with the suggested cost report modifications to improve pediatric payment, which is presented later on in the preamble in section VI.H of this proposed rule.
4. Request for Information for Pediatric Dialysis Payment
CMS is soliciting feedback from the public on pediatric dialysis payment. In addition to any other input the public wants to provide for the pediatric dialysis payment adjustment, we are requesting responses to the following questions.
- Does the magnitude of total costs and pediatric multipliers reflect ESRD facilities' actual incurred costs? If not, what specific costs are not being reported on claims and/or cost reports?
- Is there sufficient variation in composite rate costs among pediatric patients to justify use of a proxy to distribute facility-level composite rate costs to individual treatments?
- If duration of treatment is not a valid proxy for composite rate costs per treatment, what are alternative proxies to consider?
- What, if any, are the specific concerns about incorporating pediatric patients into the estimation of multipliers for both the adult and pediatric populations?
- What are the issues facing pediatric billing and accounting staff with regard to completion of claims and cost reports? How can these problems be remedied?
- Are there additional costs factors for pediatric patients that are not adequately captured on the 72X claim?Start Printed Page 36405
G. Modifying the ESRD PPS and Hospital Cost Reports
1. Special Audit Adjustment Summary
a. Background
Throughout the years, we have received comments about updating the Medicare Renal Cost Reports (CMS-Form-265-11). Data from the Medicare Renal Cost Reports is received by the Hospital Cost Report Information System (HCRIS). Stakeholders have asserted that the cost reports need more granularity to align resource use with payment. In addition, section 217(e) of PAMA mandated an audit of Medicare cost reports beginning during 2012 for a representative sample of providers of services and renal dialysis facilities furnishing renal dialysis services. The following discusses CMS's audit process and findings.
Organizations that consist of multiple ESRD facilities or business entities may have Home Offices that furnish central management and administrative services (for example, centralized accounting, purchasing, personnel services, and management) to other organizations within the chain. To the extent that the Home Office furnishes services related to patient care to a provider, the reasonable costs of such services are included in the ESRD facility's cost report and are reimbursable as part of the ESRD facility's costs. The CMS' Office of the Actuary (OACT) selected a sample of 1,479 freestanding ESRD facilities from five Home Offices of large dialysis organizations for the cost audit. A contractor performed cost audits of these ESRD facilities in September of 2015. All audits were completed by September of 2018.
Upon completion of the audits, adjustments for unallowable costs were made by CMS's Office of Financial Management to the ESRD cost reports and reflected in the HCRIS data. As of March 2020, 1,395 of the 1,479 ESRD facilities had complete HCRIS data (that is, containing both pre-and post-audit information). A summary of the audit adjustments include Home Office costs, drugs, and treatments, which are discussed in this section.
b. Home Office Cost
Of the ESRD facilities sampled, 1,278 of 1,479 received an allocation of Home Office costs from the five Home Offices selected for review. Any adjustments of unallowable Home Office costs would flow down and be reflected in the ESRD facilities' cost reports.
c. Adjustments
Using the HCRIS data, of the 1,395 ESRD freestanding facilities analyzed, a total of $147.5 million of unallowable costs were removed from the total costs reported on Worksheet A. Noteworthy adjustment areas included $136.5 million of the unallowable costs initially reported in the administrative and general cost center on Worksheet A, with $75 million of this $136.5 million pertaining to related-party adjustments recorded on Worksheet A-3. Of the $75 million, $72 million were for Home Office costs, including disallowed related party costs associated with Home Office and management fee adjustments. Some of the major adjustments noted at the Home Office level reviews included the following: Unsupported documentation; related-party management fees; lobbying expense; taxes for items not related to patient care; executive compensation in excess of reasonable guidelines, and related party laboratory costs, which were reduced to cost. Other certain non-allowable items included: Advertising, legal fees interest expense and financing fees, corporate travel/lodging/relocation, various consulting fees, business development expenses; insurance settlement payments; insurance expenses (malpractice, etc.).
d. Drugs
In general, there were minimal adjustments to drugs cost and these were made to both drug expense and drug rebates (<1.0 percent in aggregate). The top five ESRD dialysis organizations were examined based on total reimbursable cost and average cost per treatment for adult hemodialysis (the most common treatment type). No material adjustment was made to total number of treatments. However, there was a significant decrease in the average cost per treatment because of material adjustments made to the total allowable costs. The number of Epoetin Units furnished during the Cost Reporting Period (reported on Worksheet S-1, Line 14) was reduced by approximately 13 percent in aggregate. However, the majority of these adjustments related to two specific facilities, with one of the facilities having the total amount reported reduced to zero. The number of Aranesp Units furnished during the cost reporting period (reported on Worksheet S-1, Line 15) was reduced by approximately 18 percent in aggregate. However, the majority of these adjustments related to two specific facilities, both of which were reduced to zero.
e. Treatments
The total number of treatments not billed to Medicare and furnished directly (Worksheet S-1, Line 1) decreased by an average of 2.6 percent. However, the total number of treatments not billed to Medicare and Furnished under Arrangement (Worksheet S-1, Line 2) had no change. The average cost per treatment among the various types of treatments and categories appears to have decreased by an average of 1.75 percent. However, some of the adult average costs per treatment related to home program continuous ambulatory peritoneal dialysis increased after the audit by an average of 1.5 percent.
Based on this audit, our cost report data was corrected.
2. Suggestions for Modifying the ESRD PPS and Hospital Cost Reports
a. Independent Dialysis Facility Cost Report
During the 2020 ESRD PPS TEP, the data contractor engaged the panelists in a discussion regarding potential revisions to the Independent Dialysis Facility Cost Report (CMS Form 265-11). (See https://www.cms.gov/Research-Statistics-Data-and-Systems/Downloadable-Public-Use-Files/Cost-Reports/Renal-Facility-265-2011-form.) These potential revisions, which would support the efforts to develop a refined case-mix model for the ESRD PPS, are described in this section. CMS seeks input from the public on the feasibility of implementing these suggestions in freestanding ESRD facilities. These potential reporting changes would require facilities to allocate composite rate costs across settings and modalities. Taken together, the resulting cost report data would enable the determination of variation in costs across patient types (by risk groups and dialysis modalities).
In the CY 2020 ESRD PPS proposed rule (84 FR 38396 through 38400) CMS sought input on identifying components of composite rate costs, including specific facility-level costs that, in combination with treatment-level data, could be used to understand variation in dialysis treatment costs across patients. While composite rate costs constitute nearly 90 percent of total treatment costs, they are not itemized on claims, leaving facility cost reports as the only source of information on these costs. Commenters' suggestions included adding detail and stratifying the reporting detail of selected composite rate costs by setting and modality and providing additional data to determine variation in treatment costs across patient risk groups and treatment modalities.Start Printed Page 36406
The facility-level cost components of interest include capital costs related to dialysis machines and other equipment used in dialysis treatment, labor costs, and supply costs. Based on the input received and further analysis conducted by the data contractor, several specific changes to the cost reports were suggested. These include changes in the reporting of composite rate components: (1) Capital costs for dialysis machines and related equipment, (2) direct patient labor costs, (3) administrative and managerial costs, and (4) differentiation of separately billable from composite rate laboratory and supply costs. The suggested changes would also require reporting of these costs by modality. While the “step down” worksheet (Worksheet B-1) in the current cost report separates capital and labor costs by modality, this separation is based on proportionally allocating costs according to a specified statistical basis (for example, treatment counts), rather than the reporting of actual capital and labor resources associated with each modality. The data contractor and panelists agreed that changing the specifications in the instructions to the cost report to indicate that the allocations be made on the basis of actual resource use, would allow for a better estimation of component costs per treatment and analysis of how these costs vary among patient groups and across modalities.
b. Costs for Capital-Related Assets That Are Dialysis Machines
Based on stakeholder feedback, CMS would like to understand difficulties ESRD facilities have in reporting capital costs, particularly as they relate to dialysis machines. Both TEP panelists and dialysis associations have suggested that modifications to reporting of the capital costs of dialysis machines focus on two goals. The first goal is to improve the fidelity and comparability of dialysis machine capital cost reporting across individual facilities. They suggested that this would be achieved with more specific instructions for completing the cost report. The second goal is to ensure CMS's ability to distinguish between dialysis machine capital costs among various modalities and dialysis settings in a way that preserves fidelity and comparability among facilities. This could be achieved with revisions to the cost report itself. As suggested by panelists and some stakeholders, to achieve these ends, revisions to the cost report related to dialysis machine capital costs might include:
- Improve the instructions related to the reporting of dialysis machine capital costs.
++ For purchased equipment: Specify purchase price, depreciation, maintenance, repair, insurance, replacement.
++ For rented equipment: Specify rental rates, maintenance, repair, insurance, rent escalators.
- List and stratify the costs of capital equipment used in dialysis treatment by setting and modality.
++ Differentiate between rented and purchased equipment.
++ Differentiate among machines used in-facility and in the home setting.
++ Differentiate machine costs in the home setting by modality for home hemodialysis and home peritoneal dialysis.
++ Include water treatment machines and indicate location of use: Home versus in-facility.
- Location in Form 265-11
++ Expand Worksheet A, Line 6.
++ Revise instructions for Worksheet A-1, adding specificity corresponding to item definitions discussed earlier in the preamble.
c. Direct Patient Labor Allocation
Currently, the cost report does not stratify full-time equivalent (FTE) hours for direct patient care staff by dialysis modality. It also does not include several job classifications that are commonly found in present-day ESRD facilities.
At present, the statistical basis for allocating direct patient care costs is hours of service (as seen in Worksheet B-1, Column 5). Using this metric and allocating resource (or labor) use proportionally by labor hour (independent of labor type) can result in miscalculation of labor costs by modality. For example, if labor for the provision of home dialysis is on average more expensive than labor for in-facility hemodialysis, then a strict by-hour cost allocation will result in a calculation of home dialysis labor costs that is less costly per-hour than in practice. Suggestions have included that by substituting FTE for hours for each appropriate direct patient care labor category, and using labor categories that more accurately reflect current staffing patterns in ESRD facilities, any potential misrepresentations of relative labor costs across modalities can be remedied.
To this end, CMS has received a suggestion to consider the use of Bureau of Labor Statistics (BLS) occupational categories for outpatient care centers to remedy this situation, as it would provide up-to-date job classifications that the comment believes would better correspond to staffing patterns in ESRD facilities than the currently used Inpatient Prospective Payment System job categories. Selecting BLS occupational categories for outpatient care centers could be added or substituted in Lines 23-31 on Worksheet S-1 of CMS Form 265-11 to reflect current staffing patterns, and columns could be added to separately report home dialysis FTE and in-facility dialysis FTE for each relevant occupational category. Additional labor categories might include registered nurses with varying credentials, dieticians, pharmacists, and nurse practitioners and other intermediate-level providers, as appropriate.
d. Managerial and Administrative Labor Allocation
The data contractor and TEP panelists discussed Medicare cost report's non-direct patient care positions, specifically the current managerial and labor allocation. They made recommendations for differentiating high-cost management from lower-cost administrative and clerical functions, which included a set of potential revisions to bring management and administrative labor categories up to date using occupational categories that reflect current usage in dialysis facilities.
As with the direct patient labor allocation above, suggestions include the use of BLS occupational categories for outpatient care centers that correspond to the roles employed in contemporary dialysis facilities. Suggested additions to these job categories might include business and financial operations personnel, office and administrative workers, facility support workers, and programmers and analysts. With more accurate data, it may be possible to determine how management and administrative costs are differentially allocated across facilities (by region and treatment-type specialization). These suggested changes to managerial and administrative job categories would be made to Worksheet S-1, Lines 31-34.
e. Supplies and Laboratory Services
While composite rate and separately billable drug costs are differentiated on the cost report, supplies and laboratory tests are not differentiated. Supplies comprise approximately 10 percent of composite rate costs. To bring uniformity to the reporting of drugs, laboratory tests, and supplies, we have received suggestions that supplies and laboratory tests be similarly stratified. These costs are currently reported on Worksheet B/B-1. Specifically, Start Printed Page 36407stakeholders have suggested the following changes: (1) Add separate columns differentiating composite rate from separately billable supplies (Worksheet B/B-1, Column 7-8); (2) add separate columns differentiating composite rate from separately billable laboratory services (Worksheet B/B-1, Column 9-10).
3. Request for Information on Independent Facility Cost Report
CMS invites comments on the suggested changes to the Independent Facility Cost Report (CMS Form 265-11), as described earlier in this section of the proposed rule. In addition to any other input the public wants to provide on modifying the Independent Facility Cost Report, we are requesting responses to the following questions.
- What challenges, including operational difficulties, do ESRD facilities currently face in reporting capital costs:
++ In general.
++ Due to inadequate instructions:
—Which instructions should be revised for clarity?
—Of those above, which are most problematic?
++ In responding, please indicate whether you are representing the views of a
—Large dialysis organization.
—Regional organization.
—Independent and/or rural facility or another entity.
++ What level of expertise do personnel typically filling out cost reports have:
—With cost accounting principles and practices?
—With health care cost accounting principles and practices?
—With operational details of how capital equipment is used in their ESRD facility?
++ Are accounting record-keeping systems currently used by ESRD facilities adequate to the task of responding to current and contemplated (in this RFI) cost reporting requirements?
- What challenges, including operational difficulties, would ESRD facilities face:
++ In reporting dialysis-related machine costs by modality and location?
++ In determining the facility level distribution of direct patient labor FTE across modalities for each type of direct patient labor?
++ In reporting separate costs for composite rate supplies and separately billable supplies?
++ In reporting separate costs for composite rate laboratory services and separately billable laboratory services?
- What categories of direct patient care labor, such as registered nurses (North American Classification System (NAICS) 29-1141) and dieticians (NAICS 29-1031), are routinely employed by your dialysis facility and which can be documented in cost reports? Please provide the specific Bureau of Labor Statistics NAICS code associated with each labor category for outpatient care centers found at this website: https://www.bls.gov/oes/current/naics4_621400.htm.
- Please detail the specific categories of administrative and management personnel currently employed by your ESRD facility and which can be reported on CMS Form 265-11. Please provide the specific Bureau of Labor Statistics NAICS code associated with each labor category for management (https://www.bls.gov/oes/current/naics4_541600.htm#11-0000) and administrative (https://www.bls.gov/oes/2018/may/naics3_561000.htm). Please indicate if relevant labor categories are not represented here and how these categories can be documented and reported on CMS Form 265-11.
- Stakeholders have commented on other categorical costs that are not reported on the cost report. These include missed treatments and use of isolation rooms.
++ Specifically, please comment on adding reporting of (1) missed treatments, and (2) maintenance of isolation rooms.
++ Where on CMS Form 265-11 should these items be inserted (if at all)?
- What challenges would hospital-based facilities face were the hospital-based cost report to be revised to harmonize with the changes suggested for the independent facility cost report? How can the two cost reporting forms be brought into congruence as related to: Dialysis related equipment, direct patient care, administrative labor, drugs, laboratory services, and supplies?
- Costing accuracy is difficult to achieve for home dialysis. The suggested revisions described above strive to differentiate costs among the different modalities. Are there other means for facilities to report more accurate cost data for home dialysis modalities? Specifically, how can staff time dedicated to home dialysis treatment be better reported?
- What other changes might be made to the cost report to better differentiate costs across modalities and patient risk groups?
H. Modifying the Pediatric Cost Report
1. Background
Pediatric composite rate costs are not differentiated from adult costs on hospital cost reports, while some pediatric-specific costs are itemized on the existing free-standing cost report. Using CY 2019 cost report data, CMS' data contractor computed total and component specific cost per treatment for hemodialysis-equivalent treatments, stratified by modality, and obtained the ratio of pediatric to adult cost per treatment for each dialysis facility that reported both adult and pediatric treatments. The results indicate that there is variation in costs across composite rate cost components for pediatric and adult treatments. Overall the cost ratio of pediatric to adult treatment costs is 1.58,[302] indicating that pediatric treatments are more expensive to administer than adult treatments. For one cost component in particular, supplies, the ratio is 7.30,[303] indicating much higher costs for pediatric dialysis supplies than for adult supplies. Further analysis, however, revealed that a substantial portion of facilities does not differentiate between adult and pediatric costs in their cost report accounting. Overall, we found that 13 percent of facilities that treat both pediatric and adult dialysis patients do not differentiate costs between the two age groups.
2. Suggestions for the Pediatric Cost Report
In response, CMS is considering that two types of changes be made to the hospital and free-standing ESRD facility cost report that would facilitate the separate reporting of adult and pediatric treatment costs: (1) Changes that differentiate pediatric from adult composite rate component costs, and (2) changes that allow for further differentiation of component costs by modality and age group within the pediatric population. The potential revisions for which stakeholder input is being sought include the addition of select direct patient care labor categories, which correspond to the type of labor typically employed by pediatric dialysis facilities, and the differentiation of pediatric supplies and equipment.
Specifically, CMS is considering adding the following staff categories to CMS Form 265-11, Worksheet S-1, Lines 21-31 (Renal Dialysis Facility—Number of Employees (Full Time Equivalents)): Pediatric dialysis nurses and nurse practitioners, pediatric social workers, pediatric dieticians, child life specialists, teachers, and pediatric Start Printed Page 36408dialysis unit coordinator. We have also received recommendations that additional columns be added to this section of the cost report to differentiate pediatric home dialysis and in-facility dialysis.
With regard to pediatric supplies and equipment, stakeholders have suggested that there be clear differentiation of supplies used in dialysis treatment of pediatric patients, which vary in type and size, from those used with adult dialysis patients. Stakeholders have further indicated that there is added cost involved with the stocking of the range of sizes and types of supplies needed for this population. Categories of supplies for which there is a significantly increased cost for the pediatric population include: Dialyzers, catheter kits, fistula needles, saline flushes, monitors for vitals, blood pressure cuffs and items used to occupy children during their treatment.
Pediatric nephrologists have noted that these suggested revisions would have the greatest impact on the hospital cost report, which currently does not differentiate pediatric from adult dialysis patients. Approximately two-thirds of pediatric dialysis treatments take place in the hospital or medical center setting.
3. Request for Information on the Pediatric Cost Report
CMS invites comments on the potential changes to cost reports, described previously in this section of the proposed rule, as these changes (if proposed and finalized in the future) would apply to ESRD facilities treating pediatric dialysis patients. In addition to any other input the public wants to provide regarding the cost reports, we are requesting responses to the following questions.
- What degree of specificity is needed in the reporting of pediatric dialysis costs?
- Are there dialysis supply costs associated with the treatment of pediatric patients that cannot be reported currently on the cost reports? If so, please specify.
- For ESRD facilities that administer dialysis to both adult and pediatric patients:
++ To what extent can ESRD facilities differentiate dialysis supply costs for adult versus pediatric patients?
—Are there specific high-cost supplies unique to the treatment of pediatric patients that could be used to isolate additional costs related to pediatric dialysis?
—When differentiating pediatric dialysis supply costs on the cost reports, would providers prefer that the cost reports include additional specific items for pediatric supplies or a separate section for supply costs associated with pediatric dialysis?
++ To what extent can providers differentiate dialysis labor costs for adult versus pediatric patients?
- Are there potential revisions that could be made to the cost report, other than those described above, that would help identify costs unique to the pediatric population (for example, revisions to items and services being reported; format revisions to help facilitate reporting on pediatric costs)?
- What obstacles do providers face in reporting pediatric specific costs of dialysis treatment? How can these obstacles be overcome?
- Pediatric dialysis patients comprise a small number of patients in ESRD facilities other than children's hospitals or medical centers. How can pediatric dialysis costs be reported in non-specialized ESRD facilities that predominantly serve adult patients without undue burden on the provider?
I. Modifying Site of Services Provided to Medicare Beneficiaries With Acute Kidney Injury (AKI)
1. Background on Medicare Payment for AKI
On June 29, 2015, the TPEA was enacted. In the TPEA, Congress amended the Act to include coverage and provide for payment for dialysis furnished by an ESRD facility to an individual with AKI. Specifically, section 808(a) of the TPEA amended section 1861(s)(2)(F) of the Act to provide coverage for renal dialysis services furnished on or after January 1, 2017, by a renal dialysis facility or a provider of services paid under section 1881(b)(14) of the Act to individuals with AKI at the ESRD PPS base rate, as adjusted by any applicable geographic adjustment applied under section 1881(b)(14)(D)(iv)(II) of the Act and may be adjusted by the Secretary on a budget neutral basis for payments under section 1834(r) of the Act by any other adjustment factor under section 1881(b)(14)(D) of the Act. In CY 2017 ESRD PPS final rule (81 FR 77870 through 77872), we finalized the AKI dialysis payment rate.
2. Current Issues and Stakeholder Concerns
Over the years, we have received several comments, including concerns from ESRD facilities; national renal groups, nephrologists and patient organizations; patients and care partners; manufacturers; health care systems; and nurses regarding the site of renal dialysis services for Medicare beneficiaries with AKI. A patient advocacy organization supported the proposal in the CY 2017 ESRD PPS proposed rule to adjust the AKI payment rate by only the geographic and wage indices, and stated that some patients with AKI can safely dialyze at home and have their urine and blood tests performed for the assessment of kidney function in a location closer to home. The organization recommended that home training be paid separately, without dollars removed from the base rate. In the CY 2017 ESRD PPS final rule, we finalized several coverage and payment policies in order to implement subsection (r) of section 1834 of the Act and the amendments to section 1881(s)(2)(F) of the Act, including the payment rate for AKI dialysis (81 FR 77866 through 77872). We interpreted section 1834(r)(1) of the Act to mean the amount of payment for AKI dialysis services is the base rate for renal dialysis services determined for such year under the ESRD base rate as set forth in § 413.220, updated by the ESRD bundled market basket percentage increase factor minus a productivity adjustment as set forth in § 413.196(d)(1), adjusted for wages as set forth in § 413.231, and adjusted by any other amounts deemed appropriate by the Secretary under § 413.373. We codified this policy in § 413.372 and finalized a CY 2021 payment rate for renal dialysis services furnished by ESRD facilities to individuals with AKI as $253.13 (85 FR 71399).
In the CY 2017 ESRD PPS final rule, we stated that we do not expect that AKI beneficiaries will dialyze at home (81 FR 77871). We affirmed in the CY 2017 ESRD PPS final rule that payment will only be made for in-center peritoneal dialysis or hemodialysis treatments for AKI beneficiaries. CMS also stated in the CY 2017 ESRD PPS final rule that we would monitor this policy to determine if changes are necessary in the future, understanding that there may be a subset of patients for whom AKI dialysis at home is an appropriate treatment. Currently, CMS continues to believe that this population requires close medical supervision by qualified staff during their dialysis treatment.
Due to the COVID-19 PHE and an increase in the number of hospitalized patients with AKI receiving peritoneal dialysis, stakeholders have raised concerns about patients with AKI having to both travel to, and be present in, an ESRD facility post hospitalization. CMS received comments that patients with AKI require more vigilant monitoring, particularly in infection prevention, blood pressure Start Printed Page 36409management, more frequent laboratory testing, additional medication administration and increased educational needs. Commenters stated that patients with AKI are distinct from regular patients with ESRD in that they need specific critical treatment. CMS continued to receive comments in response to the CY 2021 ESRD PPS proposed rule regarding this concern, including the recommendation that CMS allow patients with AKI to be dialyzed at home. Specifically, the commenters requested that CMS allow patients with AKI to pursue peritoneal dialysis in the home if the patient and nephrologist agree it is safe to do so and the home setting is the patient's choice. We also received comments from organizations requesting that CMS remove barriers that make it difficult for patients who want to select home dialysis. They specifically requested that, for the duration of the COVID-19 PHE, CMS waive the requirement that health care providers are paid for providing care to patients with AKI only when they receive in-center hemodialysis.
The 2020 TEP included a session on AKI and the current Medicare payment system. The panelists discussed cost and utilization of AKI related dialysis services since the policy change in 2017, including the incorporation of payment for dialysis treatment for patients with AKI into the ESRD PPS, assessment of the accuracy of the reported data and the effectiveness of the current AKI payment parameters for accurately capturing the costs of this population.
Panelists agreed that some patients with AKI could benefit from different treatment regimens. In particular, they noted that more frequent, gentler dialysis would be a viable option for some patients, possibly preventing hypotension. During the COVID-19 PHE, many patients received acute peritoneal dialysis treatments in the hospital upon developing AKI, and panelists expressed support for allowing patients with AKI to continue receiving acute peritoneal dialysis once they are discharged from the hospital. One panelist noted that their hospital tries to get patients with AKI accustomed to a more standard treatment regimen such as three treatments per week before discharging them to an ESRD facility. Another panelist expressed support for the implementation of transitional care units, noting they would help patients new to dialysis adjust to dialysis and the lifestyle changes that accompany it. Panelists also advocated for allowing patients with AKI to be treated at home, especially in light of the COVID-19 PHE.
Members of the TEP commented on the similar treatment frequencies observed for patients with AKI and ESRD, stating that the payment system is currently constructed to facilitate the observed treatment patterns for patients with AKI. Panelists stressed that the payment system should continue to be flexible in terms of number of treatments for patients with AKI so that those who need more frequent treatments are not impeded from receiving them.
Panelists expressed support for the CMS guidance temporarily allowing dialysis facilities to send dialysis facility staff to furnish 72x dialysis to their patients in nursing homes, from both a cost and patient health perspective. (See https://www.cms.gov/files/document/covid-19-emergency-declaration-waivers.pdf.) Panelists noted that it was more efficient to send ESRD facility staff to the skilled nursing facilities rather than the costly routine and ambulance-required transportation and physical isolation expenses incurred during the public health emergency. Panelists stated that the full spectrum of care provided in the SNF setting is invaluable, particularly for the patients with multiple comorbidities.
Panelists commented on the costs per treatment observed for patients with AKI, expressing that the higher observed costs compared to ESRD treatments aligns with their expectations. Members of the panel noted that patients with AKI receive more laboratory tests to monitor for recovery, but typically are not prescribed calcimimetics or ESAs. Some panelists also noted that due to the very small population size of Medicare beneficiaries with AKI, reporting AKI costs and statistics on cost reports at a granular level introduces an outsized reporting burden on the part of the providers.
Overall, panelists expressed that the current AKI payment structure is effective and benefits both patients and facilities. One panelist pointed out that the AKI policy change, which we implemented in the CY 2017 ESRD PPS final rule (81 FR 77866 through 77872), helps hospitals, as they can send patients with AKI requiring dialysis to ESRD facilities and consequently free up capacity at the hospital.
4. Request for Information on Modifying the Site of Services Provided to Medicare Beneficiaries With AKI
CMS is soliciting feedback from the public on the differences in care for patients with AKI versus patients with ESRD and whether it has bearing on the ability of patients with AKI to perform home dialysis safely. We request any additional comments regarding potentially modifying site of renal dialysis services and payment for AKI in the home setting.
VII. Collection of Information Requirements
A. Legislative Requirement for Solicitation of Comments
Under the Paperwork Reduction Act of 1995, we are required to provide 60-day notice in the Federal Register and solicit public comment before a collection of information requirement is submitted to the Office of Management and Budget (OMB) for review and approval. In order to fairly evaluate whether an information collection requirement should be approved by OMB, the Paperwork Reduction Act of 1995 (44 U.S.C. 3506(c)(2)(A)) requires that we solicit comment on the following issues:
- The need for the information collection and its usefulness in carrying out the proper functions of our agency.
- The accuracy of our estimate of the information collection burden.
- The quality, utility, and clarity of the information to be collected.
- Recommendations to minimize the information collection burden on the affected public, including automated collection techniques.
We are soliciting public comment on each of these issues for the following sections of this document that contain information collection requirements (ICRs):
B. Requirements in Regulation Text
In sections V through V.B of this proposed rule, we are proposing changes to the regulatory text for the ETC Model. However, the changes that are being proposed do not impose any new information collection requirements.
C. Additional Information Collection Requirements
This proposed rule does not impose any new information collection requirements in the regulation text, as specified above. However, there are changes in some currently approved information collections. The following is a discussion of these information collections.
1. ESRD QIP—Wage Estimates (OMB control numbers 0938-1289 and 0938-1340)
To derive wages estimates, we used data from the U.S. Bureau of Labor Statistics' May 2020 National Occupational Employment and Wage Start Printed Page 36410Estimates. In the CY 2016 ESRD PPS final rule (80 FR 69069), we stated that it was reasonable to assume that Medical Records and Health Information Technicians, who are responsible for organizing and managing health information data, are the individuals tasked with submitting measure data to CROWNWeb (now EQRS) and NHSN, as well as compiling and submitting patient records for purpose of the data validation studies, rather than a Registered Nurse, whose duties are centered on providing and coordinating care for patients. We stated that the median hourly wage of a Medical Records and Health Information Technician is $21.20 per hour.[304] We also stated that fringe benefit and overhead are calculated at 100 percent. Therefore, using these assumptions, we estimated an hourly labor cost of $42.40 as the basis of the wage estimates for all collections of information calculations in the ESRD QIP. We adjusted these employee hourly wage estimates by a factor of 100 percent to reflect current HHS department-wide guidance on estimating the cost of fringe benefits and overhead. We stated that these are necessarily rough adjustments, both because fringe benefits and overhead costs vary significantly from employer to employer and because methods of estimating these costs vary widely from study to study. Nonetheless, we stated that there is no practical alternative and we believe that these are reasonable estimation methods.
We used this updated wage estimate, along with updated facility and patient counts to re-estimate the total information collection burden in the ESRD QIP for PY 2024 that we discussed in the CY 2021 ESRD QIP final rule (85 FR 71473 through 71474) and to estimate the total information collection burden in the ESRD QIP for PY 2025. We provide the re-estimated information collection burden associated with the PY 2024 ESRD QIP and the newly estimated information collection burden associated with the PY 2025 ESRD QIP in section VII.C.3 of this proposed rule.
2. Estimated Burden Associated With the Data Validation Requirements for PY 2024 and PY 2025 (OMB Control Numbers 0938-1289 and 0938-1340)
In the CY 2020 ESRD PPS final rule, we finalized a policy to adopt the CROWNWeb data validation methodology that we previously adopted for the PY 2016 ESRD QIP as the methodology we would use to validate CROWNWeb data for all payment years, beginning with PY 2021 (83 FR 57001 through 57002). Although, as noted in section IV.B.2 of this proposed rule, we are now using EQRS to report data that was previously reported in CROWNWeb, the data validation methodology remains the same. Under this methodology, 300 facilities are selected each year to submit 10 records to CMS, and we reimburse these facilities for the costs associated with copying and mailing the requested records. The burden associated with these validation requirements is the time and effort necessary to submit the requested records to a CMS contractor. In this proposed rule, we are updating these estimates using a newly available wage estimate of a Medical Records and Health Information Technician. In the CY 2020 ESRD PPS final rule, we estimated that it would take each facility approximately 2.5 hours to comply with this requirement. If 300 facilities are asked to submit records, we estimated that the total combined annual burden for these facilities would be 750 hours (300 facilities x 2.5 hours). Since we anticipate that Medical Records and Health Information Technicians or similar administrative staff would submit these data, we estimate that the aggregate cost of the EQRS data validation each year would be approximately $31,800 (750 hours × $42.40), or an annual total of approximately $106.00 ($31,800/300 facilities) per facility in the sample. The burden cost increase associated with these requirements will be revised in information collection request (OMB control number 0938-1289).
In the CY 2021 ESRD PPS final rule, we finalized our policy to reduce the number of records that a facility selected to participate in the NHSN data validation must submit to a CMS contractor, beginning with PY 2023 (85 FR 71471 through 71472). Under this finalized policy, a facility is required to submit records for 20 patients across any two quarters of the year, instead of 20 records for each of the first two quarters of the year. The burden associated with this policy is the time and effort necessary to submit the requested records to a CMS contractor. Applying our policy to reduce the number of records required from each facility participating in the NHSN validation, we estimated that it would take each facility approximately 5 hours to comply with this requirement. If 300 facilities are asked to submit records each year, we estimated that the total combined annual burden hours for these facilities per year would be 1,500 hours (300 facilities × 5 hours). Since we anticipate that Medical Records and Health Information Technicians or similar staff would submit these data, using the newly available wage estimate of a Medical Records and Health Information Technician, we estimate that the aggregate cost of the NHSN data validation each year would be approximately $63,600 (1,500 hours × $42.40), or a total of approximately $212 ($63,600/300 facilities) per facility in the sample. While the burden hours estimate will not change, the burden cost updates associated with these requirements will be revised in the information collection request (OMB control number 0938-1340).
3. EQRS Reporting Requirements for PY 2024 and PY 2025 (OMB Control Number 0938-1289)
To determine the burden associated with the EQRS reporting requirements (previously known as the CROWNWeb reporting requirements), we look at the total number of patients nationally, the number of data elements per patient-year that the facility would be required to submit to EQRS for each measure, the amount of time required for data entry, the estimated wage plus benefits applicable to the individuals within facilities who are most likely to be entering data into EQRS, and the number of facilities submitting data to EQRS. In the CY 2021 ESRD PPS final rule, we estimated that the burden associated with CROWNWeb (now EQRS) reporting requirements for the PY 2024 ESRD QIP was approximately $208 million (85 FR 71400).
As discussed in section IV.C and section IV.D of this proposed rule, we are proposing measure suppressions that would apply for PY 2022 and updates to the scoring methodology and payment reductions for the PY 2022 ESRD QIP. We also announce an extension of EQRS reporting requirements for facilities due to systems issues. However, we believe that none of the policies proposed in this proposed rule would affect our estimates of the annual burden associated with the Program's information collection requirements, as facilities are still expected to continue to collect measure data during this time period. We are not proposing any changes that would affect the burden associated with EQRS reporting requirements for PY 2024 or PY 2025. However, we have re-calculated the burden estimate for PY 2024 using updated estimates of the total number of dialysis facilities, the total number of Start Printed Page 36411patients nationally, and wages for Medical Records and Health Information Technicians or similar staff as well as a refined estimate of the number of hours needed to complete data entry for EQRS reporting. Consistent with our approach in the CY 2021 ESRD PPS final rule (85 FR 71474), in this proposed rule we estimated that the amount of time required to submit measure data to EQRS was 2.5 minutes per element and did not use a rounded estimate of the time needed to complete data entry for EQRS reporting. There are 229 data elements for 532,931 patients across 7,610 facilities. At 2.5 minutes per element, this yields approximately 668.21 hours per facility. Therefore, the PY 2024 burden is 5,085,050 hours (668.21 hours × 7,610 facilities). Using the wage estimate of a Medical Records and Health Information Technician, we estimate that the PY 2024 total burden cost is approximately $215 million (5,085,050 hours × $42.40). There is no net incremental burden change from PY 2024 to PY 2025 because we are not changing the reporting requirements for PY 2025.
VIII. Response to Comments
Because of the large number of public comments we normally receive on Federal Register documents, we are not able to acknowledge or respond to them individually. We will consider all comments we receive by the date and time specified in the “DATES” section of this preamble, and, when we proceed with a subsequent document, we will respond to the comments in the preamble to that document.
IX. Economic Analyses
A. Regulatory Impact Analysis
1. Introduction
We have examined the impacts of this rule as required by Executive Order 12866 on Regulatory Planning and Review (September 30, 1993), Executive Order 13563 on Improving Regulation and Regulatory Review (January 18, 2011), the Regulatory Flexibility Act (RFA) (September 19, 1980; Pub. L. 96-354), section 1102(b) of the Social Security Act, section 202 of the Unfunded Mandates Reform Act of 1995 (March 22, 1995; Pub. L. 104-4), Executive Order 13132 on Federalism (August 4, 1999), and the Congressional Review Act (5 U.S.C. 801(2)).
Executive Orders 12866 and 13563 direct agencies to assess all costs and benefits of available regulatory alternatives and, if regulation is necessary, to select regulatory approaches that maximize net benefits (including potential economic, environmental, public health and safety effects, distributive impacts, and equity). Section 3(f) of Executive Order 12866 defines a “significant regulatory action” as an action that is likely to result in a rule: (1) Having an annual effect on the economy of $100 million or more in any 1 year, or adversely and materially affecting a sector of the economy, productivity, competition, jobs, the environment, public health or safety, or state, local or tribal governments or communities (also referred to as “economically significant”); (2) creating a serious inconsistency or otherwise interfering with an action taken or planned by another agency; (3) materially altering the budgetary impacts of entitlement grants, user fees, or loan programs or the rights and obligations of recipients thereof; or (4) raising novel legal or policy issues arising out of legal mandates, the President's priorities, or the principles set forth in the Executive Order.
A regulatory impact analysis (RIA) must be prepared for major rules with economically significant effects ($100 million or more in any 1 year). We estimate that this rulemaking is “economically significant” as measured by the $100 million threshold, and hence also a major rule under the Congressional Review Act. Accordingly, we have prepared a Regulatory Impact Analysis that to the best of our ability presents the costs and benefits of the rulemaking. We solicit comments on the regulatory impact analysis provided.
2. Statement of Need
a. ESRD PPS
This rule proposes a number of routine updates to the ESRD PPS for CY 2022. The proposed routine updates include the CY 2022 wage index values, the wage index budget-neutrality adjustment factor, and outlier payment threshold amounts. Failure to publish this proposed rule would result in ESRD facilities not receiving appropriate payments in CY 2022 for renal dialysis services furnished to ESRD beneficiaries.
b. AKI
This rule also proposes routine updates to the payment for renal dialysis services furnished by ESRD facilities to individuals with AKI. Failure to publish this proposed rule would result in ESRD facilities not receiving appropriate payments in CY 2022 for renal dialysis services furnished to patients with AKI in accordance with section 1834(r) of the Act.
c. ESRD QIP
This proposed rule proposes to implement requirements for the ESRD QIP, including a proposal to adopt a measure suppression policy and to suppress several ESRD QIP measures under that proposed measure suppression policy, proposals regarding the scoring methodology and payment reductions for the PY 2022 ESRD QIP, a proposed update to the SHR measure, and a proposed update to the PY 2024 performance standards. This proposed rule also includes a request for public comment on closing the gap in health equity, as well as a request for public comment on potential actions and priority areas that would enable the continued transformation of our quality measurement enterprise toward greater digital capture of data and use of the FHIR standard.
d. ETC Model
Beneficiaries with ESRD are among the most medically fragile and high-cost populations served by the Medicare program. One of CMS' goals in designing the ETC Model is to test ways to incentivize home dialysis and kidney transplants, to enhance beneficiary choice of modality for renal replacement therapy, and improve quality of care and quality of life while reducing Medicare program expenditures. The substantially higher expenditures, mortality, and hospitalization rates for dialysis patients in the U.S. compared to those for individuals with ESRD in other countries indicate a population with poor clinical outcomes and potentially avoidable expenditures. This proposed rule would refine the methodology for setting and updating achievement and improvement benchmarks for participating ESRD facilities and Managing Clinicians serving the ESRD population over the remaining years of the ETC Model, among other proposed changes. Notwithstanding the proposed changes, we continue to anticipate improvement in quality of care for beneficiaries and reduced expenditures under the ETC Model inasmuch as the Model is designed to create incentives for beneficiaries, along with their families and caregivers, to choose the optimal kidney replacement modality.
As noted in section IV.B of the Specialty Care Models final rule (85 FR 61264), Medicare payment rules and a deficit in beneficiary education result in a bias toward in-center hemodialysis, which is often not preferred by patients or physicians relative to home dialysis or kidney transplantation. We provided evidence from the published literature Start Printed Page 36412to support the projection that higher rates of home dialysis and kidney transplants would likely reduce Medicare expenditures, and, not only enhance beneficiary choice, independence, and quality of life, but also preserve or enhance the quality of care for ESRD beneficiaries.
As described in detail in section V of this proposed rule, we believe it is necessary to propose certain changes to the ETC Model. Under the proposed changes to the ETC Model, ETC Participants would continue to receive adjusted payments but beginning for MY3, certain aspects of the ETC Model that determine those payment adjustments would change. The proposed change to the achievement benchmarking methodology is necessary to the ETC Model as this change maintains the ETC Model's expectation of savings. The proposed changes to the transplant rate, the achievement benchmarking methodology, and the improvement benchmarking and scoring methodology are necessary to increase accuracy and fairness of performance assessment. The proposed changes to the home dialysis rate, data sharing, and kidney disease patient education services waivers are necessary to support ETC Participants operating in the ETC Model.
3. Overall Impact
a. ESRD PPS
We estimate that the proposed revisions to the ESRD PPS would result in an increase of approximately $140 million in payments to ESRD facilities in CY 2022, which includes the amount associated with updates to the outlier thresholds, and updates to the wage index.
b. AKI
We estimate that the proposed updates to the AKI payment rate would result in an increase of approximately $1 million in payments to ESRD facilities in CY 2022.
c. ESRD QIP
For PY 2024 and PY 2025, we have re-estimated the costs associated with the information collection requirements under the ESRD QIP with updated estimates of the total number of dialysis facilities, the total number of patients nationally, wages for Medical Records and Health Information Technicians or similar staff, and a refined estimate of the number of hours needed to complete data entry for EQRS reporting. We have made no changes to our methodology for calculating the annual burden associated with the information collection requirements for the EQRS validation study (previously known as the CROWNWeb validation study), the NHSN validation study, and EQRS reporting. As discussed in section IV.C and section IV.D of this proposed rule, we are proposing measure suppressions that would apply for PY 2022 and updates to the scoring methodology and payment reductions for the PY 2022 ESRD QIP. We also announce an extension of EQRS reporting requirements for facilities due to systems issues. However, we believe that none of the policies proposed in this proposed rule would affect our estimates of the annual burden associated with the Program's information collection requirements, as facilities are still expected to continue to collect measure data during this time period.
We also updated the payment reduction scale using more recent data for the measures in the ESRD QIP measure set. We estimate approximately $215 million in information collection burden, which includes the cost of complying with this rule, and an additional $17 million in estimated payment reductions across all facilities for PY 2024.
For PY 2025, we estimate that the proposed revisions to the ESRD QIP would result in $215 million in information collection burden, and $17 million in estimated payment reductions across all facilities, for an impact of $232 million as a result of the policies we have previously finalized and the policies we have proposed in this proposed rule.
d. ETC Model
We estimate that the proposed changes to the ETC Model would increase the Model's projected direct savings from payment adjustments alone by $7 million over the duration of the Model. We estimate that the Model would generate $38 million in direct savings related to payment adjustments over 6.5 years with the proposed changes, and would generate $31 million in savings in the absence of the proposed changes.
4. Regulatory Review Cost Estimation
If regulations impose administrative costs on private entities, such as the time needed to read and interpret this proposed rule or final rule, we should estimate the cost associated with regulatory review. Due to the uncertainty involved with accurately quantifying the number of entities that will review the rule, we assume that the total number of unique commenters on last year's proposed rule will be the number of reviewers of this proposed rule. We acknowledge that this assumption may understate or overstate the costs of reviewing this rule. It is possible that not all commenters reviewed last year's rule in detail, and it is possible that some reviewers chose not to comment on the proposed rule. For these reasons, we thought that the number of past commenters would be a fair estimate of the number of reviewers of this rule. We welcome any comments on the approach in estimating the number of entities, which will review this proposed rule. We also recognize that different types of entities are in many cases affected by mutually exclusive sections of this proposed rule, and therefore for the purposes of our estimate we assume that each reviewer reads approximately 50 percent of the rule. We seek comments on this assumption.
Using the wage information from the BLS for medical and health service managers (Code 11-9111), we estimate that the cost of reviewing this rule is $110.74 per hour, including overhead and fringe benefits https://www.bls.gov/oes/current/oes_nat.htm. Assuming an average reading speed, we estimate that it would take approximately 6.25 hours for the staff to review half of this proposed rule. For each entity that reviews the rule, the estimated cost is $692.13 (6.25 hours × $110.74). Therefore, we estimate that the total cost of reviewing this regulation is $ 78,903 ($692.13 × 114).
B. Detailed Economic Analysis
1. CY 2021 End-Stage Renal Disease Prospective Payment System
a. Effects on ESRD Facilities
To understand the impact of the changes affecting payments to different categories of ESRD facilities, it is necessary to compare estimated payments in CY 2021 to estimated payments in CY 2022. To estimate the impact among various types of ESRD facilities, it is imperative that the estimates of payments in CY 2021 and CY 2022 contain similar inputs. Therefore, we simulated payments only for those ESRD facilities for which we are able to calculate both current payments and new payments.
For this proposed rule, we used CY 2020 data from the Part A and Part B Common Working Files as of February 12, 2021, as a basis for Medicare dialysis treatments and payments under the ESRD PPS. We updated the 2020 claims to 2021 and 2022 using various updates. The updates to the ESRD PPS base rate are described in section II.B.1.d of this proposed rule. Table 9 shows the impact of the estimated CY 2022 ESRD PPS Start Printed Page 36413payments compared to estimated payments to ESRD facilities in CY 2021.
Start Printed Page 36414
Column A of the impact table indicates the number of ESRD facilities for each impact category and column B indicates the number of dialysis treatments (in millions). The overall effect of the proposed changes to the outlier payment policy described in section II.B.1.c of this proposed rule is shown in column C. For CY 2022, the impact on all ESRD facilities as a result of the proposed changes to the outlier payment policy would be a 0.2 percent increase in estimated payments. All ESRD facilities are anticipated to experience a positive effect in their estimated CY 2022 payments as a result of the proposed outlier policy changes.
Column D shows the effect of the annual update to the wage index, as described in section II.B.1.b of this proposed rule. That is, this column reflects the update from the CY 2021 ESRD PPS wage index using 2018 OMB delineations as finalized in the CY 2021 ESRD PPS final rule, with a basis of the FY 2022 pre-floor, pre-reclassified IPPS hospital wage index data in a budget neutral manner. The total impact of this change is 0.0 percent; however, there are distributional effects of the change among different categories of ESRD facilities. The categories of types of facilities in the impact table show changes in estimated payments ranging from a 0.7 percent decrease to a 0.5 percent increase due to the annual update to the ESRD PPS wage index.
Column E shows the effect of the proposed CY 2022 ESRD PPS payment rate update as described in section II.B.1.a of this proposed rule. The proposed ESRD PPS payment rate update is 1.0 percent, which reflects the proposed ESRDB market basket percentage increase factor for CY 2022 of 1.6 percent and the proposed productivity adjustment of 0.6 percent.
Column F reflects the overall impact, that is, the effects of the proposed outlier policy changes, the proposed updated wage index, and the payment rate update. We expect that overall ESRD facilities would experience a 1.2 percent increase in estimated payments in CY 2022. The categories of types of facilities in the impact table show impacts ranging from a 0.4 percent increase to a 1.6 percent increase in their CY 2022 estimated payments.
b. Effects on Other Providers
Under the ESRD PPS, Medicare pays ESRD facilities a single bundled payment for renal dialysis services, which may have been separately paid to other providers (for example, laboratories, durable medical equipment suppliers, and pharmacies) by Medicare prior to the implementation of the ESRD PPS. Therefore, in CY 2022, we estimate that the proposed ESRD PPS would have zero impact on these other providers.
c. Effects on the Medicare Program
We estimate that Medicare spending (total Medicare program payments) for ESRD facilities in CY 2022 would be approximately $8.9 billion. This estimate takes into account a projected decrease in fee-for-service Medicare dialysis beneficiary enrollment of 5.9 percent in CY 2022.
d. Effects on Medicare Beneficiaries
Under the ESRD PPS, beneficiaries are responsible for paying 20 percent of the ESRD PPS payment amount. As a result of the projected 1.2 percent overall increase in the proposed CY 2022 ESRD PPS payment amounts, we estimate that there would be an increase in beneficiary co-insurance payments of 1.2 percent in CY 2022, which translates to approximately $30 million.
e. Alternatives Considered
CY 2022 Impacts: 2019 Versus 2020 Claims Data
Each year CMS uses the latest available ESRD claims to update the outlier threshold, budget neutrality factor, and payment rates. Due to the COVID-19 PHE, we compared the impact of using CY 2019 claims against CY 2020 claims to determine if there was any substantial difference in the results that would justify potentially deviating from our longstanding policy to use the latest available data. Analysis suggested that ESRD utilization did not change substantially during the pandemic, likely due to the patients' vulnerability and need for these services. Consequently, we proposed to use the CY 2020 data because it does not negatively impact ESRD facilities and keeps with our longstanding policy to make updates using the latest available ESRD claims data.
2. Proposed Payment for Renal Dialysis Services Furnished to Individuals With AKI
a. Effects on ESRD Facilities
To understand the impact of the changes affecting payments to different categories of ESRD facilities for renal dialysis services furnished to individuals with AKI, it is necessary to compare estimated payments in CY 2021 to estimated payments in CY 2022. To estimate the impact among various types of ESRD facilities for renal dialysis services furnished to individuals with AKI, it is imperative that the estimates of payments in CY 2021 and CY 2022 contain similar inputs. Therefore, we simulated payments only for those ESRD facilities for which we are able to calculate both current payments and new payments.
For this proposed rule, we used CY 2020 data from the Part A and Part B Common Working Files as of February 12, 2021, as a basis for Medicare for renal dialysis services furnished to individuals with AKI. We updated the 2020 claims to 2021 and 2022 using various updates. The proposed updates to the AKI payment amount are described in section III.B of this proposed rule. Table 10 shows the impact of the estimated CY 2022 payments for renal dialysis services furnished to individuals with AKI compared to estimated payments for renal dialysis services furnished to individuals with AKI in CY 2021.
Start Printed Page 36415
Start Printed Page 36416

Column A of the impact table indicates the number of ESRD facilities for each impact category and column B indicates the number of AKI dialysis treatments (in thousands). Column C shows the effect of the proposed CY 2022 wage indices. Column D shows the effect of the proposed CY 2022 ESRD PPS payment rate update. The proposed ESRD PPS payment rate update is 1.0 percent, which reflects the proposed ESRDB market basket percentage increase factor for CY 2022 of 1.6 percent and the proposed productivity adjustment of 0.6 percent.
Column E reflects the overall impact, that is, the effects of the updated wage index and the payment rate update. We expect that overall ESRD facilities would experience a 1.0 percent increase in estimated payments in CY 2022. The categories of types of facilities in the impact table show impacts ranging from an increase of 0.0 percent to 1.6 percent in their CY 2022 estimated payments.
b. Effects on Other Providers
Under section 1834(r) of the Act, as added by section 808(b) of TPEA, we propose to update the payment rate for renal dialysis services furnished by ESRD facilities to beneficiaries with AKI. The only two Medicare providers and suppliers authorized to provide these outpatient renal dialysis services are hospital outpatient departments and ESRD facilities. The patient and his or her physician make the decision about where the renal dialysis services are furnished. Therefore, this proposal will have zero impact on other Medicare providers.
c. Effects on the Medicare Program
We estimate approximately $52 million would be paid to ESRD facilities in CY 2022 as a result of patients with AKI receiving renal dialysis services in the ESRD facility at the lower ESRD PPS base rate versus receiving those services only in the hospital outpatient setting and paid under the outpatient prospective payment system, where services were required to be administered prior to the TPEA.
d. Effects on Medicare Beneficiaries
Currently, beneficiaries have a 20 percent co-insurance obligation when they receive AKI dialysis in the hospital outpatient setting. When these services are furnished in an ESRD facility, the patients would continue to be responsible for a 20 percent coinsurance. Because the AKI dialysis payment rate paid to ESRD facilities is lower than the outpatient hospital PPS's payment amount, we would expect beneficiaries to pay less co-insurance when AKI dialysis is furnished by ESRD facilities.
e. Alternatives Considered
As we discussed in the CY 2017 ESRD PPS proposed rule (81 FR 42870), we considered adjusting the AKI payment rate by including the ESRD PPS case-mix adjustments, and other adjustments at section 1881(b)(14)(D) of the Act, as well as not paying separately for AKI specific drugs and laboratory tests. We ultimately determined that treatment for AKI is substantially different from treatment for ESRD and the case-mix adjustments applied to ESRD patients may not be applicable to AKI patients and as such, including those policies and adjustment would be inappropriate. We continue to monitor utilization and trends of items and services furnished to individuals with AKI for purposes of refining the payment rate in the future. This monitoring would assist us in developing knowledgeable, data-driven proposals.
3. ESRD QIP
a. Effects of the PY 2022 ESRD QIP on ESRD Facilities
The ESRD QIP is intended to prevent reductions in the quality of ESRD dialysis facility services provided to beneficiaries. Although the general methodology that we use to determine a facility's TPS is described in our regulations at 42 CFR 413.178(e), we are proposing to codify special scoring policies for PY 2022 at 42 CFR 413.178(h). Under these proposed regulations, we would calculate measure rates for all measures but would not calculate achievement and improvement points for any measures. We would also not calculate or award a TPS for any facility. Finally, we would not reduce payment to any facility for PY 2022.
If these policies are finalized as proposed, we believe there will be no effects of the PY 2022 ESRD QIP on ESRD Facilities, as no facilities will receive a TPS or payment reductions for PY 2022.Start Printed Page 36417
b. Effects of the PY 2024 ESRD QIP on ESRD Facilities
Any reductions in the ESRD PPS payments as a result of a facility's performance under the PY 2024 ESRD QIP will apply to the ESRD PPS payments made to the facility for services furnished in CY 2024, as codified in our regulations at 42 CFR 413.177.
For the PY 2024 ESRD QIP, we estimate that, of the 7,610 dialysis facilities (including those not receiving a TPS) enrolled in Medicare, approximately 24.4 percent or 1,799 of the facilities that have sufficient data to calculate a TPS would receive a payment reduction for PY 2024. We are presenting an estimate for the PY 2024 ESRD QIP to update the estimated impact that was provided in the CY 2021 ESRD PPS final rule (85 FR 71481 through 71483). If our proposals are finalized as proposed, the total estimated payment reductions for all the 1,799 facilities expected to receive a payment reduction in PY 2024 would decrease from $18,247,083.76 to approximately $17,154,657.12. Facilities that do not receive a TPS do not receive a payment reduction.
Table 11 shows the overall estimated distribution of payment reductions resulting from the PY 2024 ESRD QIP.

To estimate whether a facility would receive a payment reduction for PY 2024, we scored each facility on achievement and improvement on several clinical measures we have previously finalized and for which there were available data from EQRS and Medicare claims. Payment reduction estimates are calculated using the most recent data available (specified in Table 12) in accordance with the policies proposed in this proposed rule. Measures used for the simulation are shown in Table 12.

For all measures except the SHR clinical measure, the Standardized Readmission Ratio (SRR) clinical measure, and the STrR reporting measure, measures with less than 11 patients for a facility were not included in that facility's TPS. For the SHR clinical measure and the SRR clinical measure, facilities were required to have at least 5 patient-years at risk and 11 index discharges, respectively, in order to be included in the facility's TPS. For the STrR reporting measure, facilities were required to have at least 10 patient-years at risk in order to be included in the facility's TPS. Each facility's TPS was compared to an estimated mTPS and an estimated payment reduction table that were consistent with the proposals outlined in sections IV.E and IV.F of this proposed rule. Facility reporting measure scores were estimated using available data from CY 2019. Facilities Start Printed Page 36418were required to have at least one measure in at least two domains to receive a TPS.
To estimate the total payment reductions in PY 2024 for each facility resulting from this final rule, we multiplied the total Medicare payments to the facility during the 1-year period between January 2019 and December 2019 by the facility's estimated payment reduction percentage expected under the ESRD QIP, yielding a total payment reduction amount for each facility.
Table 13 shows the estimated impact of the finalized ESRD QIP payment reductions to all ESRD facilities for PY 2024. The table also details the distribution of ESRD facilities by size (both among facilities considered to be small entities and by number of treatments per facility), geography (both rural and urban and by region), and facility type (hospital based and freestanding facilities). Given that the performance period used for these calculations differs from the performance period we are using for the PY 2024 ESRD QIP, the actual impact of the PY 2024 ESRD QIP may vary significantly from the values provided here.

c. Effects of the PY 2025 ESRD QIP on ESRD Facilities
For the PY 2025 ESRD QIP, we estimate that, of the 7,610 dialysis facilities (including those not receiving a TPS) enrolled in Medicare, approximately 24.4 percent or 1,799 of the facilities that have sufficient data to calculate a TPS would receive a payment reduction for PY 2025. The total payment reductions for all the 1,799 facilities expected to receive a Start Printed Page 36419payment reduction is approximately $17,154,657.121. Facilities that do not receive a TPS do not receive a payment reduction.
Table 14 shows the overall estimated distribution of payment reductions resulting from the PY 2025 ESRD QIP.

To estimate whether a facility would receive a payment reduction in PY 2025, we scored each facility on achievement and improvement on several clinical measures we have previously finalized and for which there were available data from EQRS and Medicare claims. Payment reduction estimates were calculated using the most recent data available (specified in Table 14) in accordance with the policies finalized in this proposed rule. Measures used for the simulation are shown in Table 15.

For all measures except the SHR clinical measure, the SRR clinical measure, and the STrR reporting measure, measures with less than 11 patients for a facility were not included in that facility's TPS. For SHR and SRR, facilities were required to have at least 5 patient-years at risk and 11 index discharges, respectively, in order to be included in the facility's TPS. For the STrR reporting measure, facilities were required to have at least 10 patient-years at risk in order to be included in the facility's TPS. Each facility's TPS was compared to an estimated mTPS and an estimated payment reduction table that incorporates the policies outlined in section IV.E and IV.F of this proposed rule. Facility reporting measure scores were estimated using available data from CY 2019. Facilities were required to have at least one measure in at least two domains to receive a TPS.
To estimate the total payment reductions in PY 2025 for each facility resulting from this proposed rule, we multiplied the total Medicare payments to the facility during the 1-year period between January 2019 and December 2019 by the facility's estimated payment reduction percentage expected under the ESRD QIP, yielding a total payment reduction amount for each facility.
Table 16 shows the estimated impact of the finalized ESRD QIP payment reductions to all ESRD facilities for PY 2025. The table details the distribution of ESRD facilities by size (both among facilities considered to be small entities and by number of treatments per facility), geography (both rural and urban and by region), and facility type (hospital based and freestanding facilities). Given that the performance period used for these calculations differs from the performance period we are proposing to use for the PY 2025 Start Printed Page 36420ESRD QIP, the actual impact of the PY 2025 ESRD QIP may vary significantly from the values provided here.

d. Effects on Other Providers
The ESRD QIP is applicable to dialysis facilities. We are aware that several of our measures impact other providers. For example, with the introduction of the SRR clinical measure in PY 2017 and the SHR clinical measure in PY 2020, we anticipate that hospitals may experience financial savings as dialysis facilities work to reduce the number of unplanned readmissions and hospitalizations. We are exploring various methods to assess the impact these measures have on hospitals and other facilities, such as through the impacts of the Hospital Readmissions Reduction Program and the Hospital-Acquired Condition Reduction Program, and we intend to continue examining the interactions between our quality programs to the greatest extent feasible.
e. Effects on the Medicare Program
For PY 2025, we estimate that the ESRD QIP would contribute approximately $17,154,657.12 in Medicare savings. For comparison, Table 17 shows the payment reductions that we estimate will be applied by the ESRD QIP from PY 2018 through PY 2025. This includes our PY 2022 scoring and payment proposals as described in section IV.D of this proposed rule.
Start Printed Page 36421
f. Effects on Medicare Beneficiaries
The ESRD QIP is applicable to dialysis facilities. Since the Program's inception, there is evidence on improved performance on ESRD QIP measures. As we stated in the CY 2018 ESRD PPS final rule, one objective measure we can examine to demonstrate the improved quality of care over time is the improvement of performance standards (82 FR 50795). As the ESRD QIP has refined its measure set and as facilities have gained experience with the measures included in the Program, performance standards have generally continued to rise. We view this as evidence that facility performance (and therefore the quality of care provided to Medicare beneficiaries) is objectively improving. We are in the process of monitoring and evaluating trends in the quality and cost of care for patients under the ESRD QIP, incorporating both existing measures and new measures as they are implemented in the Program. We will provide additional information about the impact of the ESRD QIP on beneficiaries as we learn more. However, in future years we are interested in examining these impacts through the analysis of available data from our existing measures.
g. Alternatives Considered
In section IV.D. of this proposed rule, we are proposing a special rule to modify the scoring methodology such that no facility would receive a payment reduction for PY 2022. Under this special rule for PY 2022, we would calculate measure rates for all measures for that payment year, but would not use those measure rates to generate an achievement or improvement score, domain scores, or a TPS. We considered retaining our current scoring policy for PY 2022. However, we concluded that this was not feasible because of the EQRS system issues described in section IV.B.2, and additionally, due to the impact of the COVID-19 PHE on some of the PY 2022 ESRD QIP measures, as described more fully in section IV.C. of this proposed rule. This approach would help to ensure that a facility would not be penalized due to extraordinary circumstances beyond the facility's control.
4. ETC Model
(1) Overview
Under the ESRD PPS under Medicare Part B, a single per-treatment payment is made to an ESRD facility for all of the renal dialysis services defined in section 1881(b)(14)(B) of the Act and furnished to individuals for the treatment of ESRD in the ESRD facility or in a patient's home. Under the Physician Fee Schedule, medical management of an ESRD beneficiary receiving dialysis by a physician or other practitioner is paid through the MCP. The ETC Model is a mandatory payment model designed to test payment adjustments to certain dialysis and dialysis-related payments, as discussed in the Specialty Care Models final rule (85 FR 6114), for ESRD facilities and for Managing Clinicians for claims with dates of service from January 1, 2021 to June 30, 2027. The requirements for the ETC Model are set forth in 42 CFR part 512, subpart C. The changes proposed in this proposed rule (discussed in detail in section V.B of this proposed rule) would impact model payment adjustments for PPA Period 3, starting in July 1, 2023.
Under the current ETC Model, there are two payment adjustments designed to increase rates of home dialysis and kidney transplantation through financial incentives. The HDPA is an upward payment adjustment on certain home dialysis claims for ESRD facilities, as described in §§ 512.340 and 512.350, and to certain home dialysis-related claims for Managing Clinicians, as described in §§ 512.345 and 512.350, during the initial 3 years of the ETC Model.
The PPA is an upward or downward payment adjustment on certain dialysis and dialysis-related claims submitted by ETC Participants, as described in §§ 512.375(a) and 512.380 for ESRD facilities and §§ 512.375(b) and 512.380 for Managing Clinicians, which will apply to claims with claim service dates beginning on July 1, 2022 and increase in magnitude over the duration of the ETC Model. We will assess each ETC Participant's home dialysis rate, as described in § 512.365(b), and transplant rate, as described in § 512.365(c), for each MY. The ETC Participant's transplant rate will be aggregated, as described in § 512.365(e), and the ETC Participant's home dialysis rate will be aggregated, as described in § 512.365(e). The ETC Participant will receive a Modality Performance Score (MPS) based on the weighted sum of the higher of the ETC Participant's achievement score or improvement score for the home dialysis rate and the higher of the ETC Participant's achievement score or improvement score for the transplant rate, as described in § 512.370(d).
For MY1 and MY2 (January 1, 2021 through July 6, 2022), the achievement scores will be calculated in relation to a set of benchmarks based on the historical rates of home dialysis and inclusion on the transplant waitlist among ESRD facilities and Managing Clinicians located in Comparison Geographic Areas. The improvement scores will be calculated in relation to a set of benchmarks based on the ETC Participant's own historical performance. The ETC Participant's MPS for a MY will determine the magnitude of its PPA during the corresponding 6-month PPA Period, which will begin 6 months after the end of the MY. An ETC Participant's MPS will be updated on a rolling basis every 6 months.
As mentioned in section IV.C.2.b(1) of the Specialty Care Models final rule (85 FR 61351), the intention was to increase these benchmarks over time through subsequent notice and comment Start Printed Page 36422rulemaking. In this proposed rule, the changes listed with bullets are being proposed for MY3 (beginning January 1, 2022) through the final MY of ETC Model (MY10). More detail on these changes is provided in section V.B of this proposed rule. The proposed changes that are most likely to affect the impact estimate for the ETC Model are:
- Include nocturnal in-center dialysis in the home dialysis rate calculation for Managing Clinicians and ESRD facilities not owned in whole or in part by an ETC LDO.
- Exclude beneficiaries with a diagnosis of and who are receiving chemotherapy or radiation for vital solid organ cancer from the transplant rate calculation.
- Modify the PPA achievement benchmarking methodology:
++ Stratify the home dialysis and transplant rate benchmark by the proportion of beneficiaries who are dual-eligible for Medicare and Medicaid, or, receive the Low-Income Subsidy (LIS), resulting in two strata.
++ Increase the home dialysis and transplant rate benchmarks by 10 percent for each MY couplet (that is, 1.10 for MY3 and MY4, 1.20 for MY5 and MY6, 1.30 for MY7 and MY8, and 1.40 for MY9 and MY10).
- Modify the PPA improvement benchmarking methodology:
++ Health Equity Incentive: Participants can earn 0.5 improvement points in addition to their improvement score for a significant increase in the rate of dual eligible or LIS recipient beneficiaries.
++ Modify improvement calculation to ensure that the Benchmark Year rate cannot be zero, such that improvement is calculable for all participants.
The ETC Model is not a total cost of care model. ETC Participants will still bill FFS Medicare, and items and services not subject to the ETC Model's payment adjustments will continue to be paid as they would in the absence of the Model.
(2) Data and Methods
A stochastic simulation was created to estimate the financial impacts of the proposed changes to the ETC Model relative to baseline expenditures, where baseline expenditures were defined as data from CYs 2018 and 2019 without the proposed changes applied. The simulation relied upon statistical assumptions derived from retrospectively constructed ESRD facilities' and Managing Clinicians' Medicare dialysis claims, transplant claims, and transplant waitlist data reported during 2018 and 2019, the most recent years with complete data available. Both datasets and the risk-adjustment methodologies for the ETC Model were developed by the CMS Office of the Actuary (OACT).
The ESRD facilities and Managing Clinicians datasets were restricted to the following eligibility criteria. Beneficiaries must be residing in the United States, 18 years of age or older, and enrolled in Medicare Part B. Beneficiaries enrolled in Medicare Advantage or other cost or Medicare managed care plans, who have elected hospice, are receiving dialysis for acute kidney injury (AKI) only, with a diagnosis of dementia, who are receiving dialysis in a nursing facility, or reside in a skilled nursing facility were excluded. In addition, beneficiaries who have a diagnosis of and are receiving treatment with chemotherapy or radiation for a vital solid organ cancer were excluded from the transplant rate calculations. Diagnosis of a vital solid organ cancer was defined as a beneficiary that had a claim with any of 39 ICD-10-CM codes ranging from C22.0 through C79.02. Treatment of a vital solid organ cancer was defined as a beneficiary with a claim with any of 2,087 radiation administration ICD-10-PCS codes, 19 chemotherapy administration CPT codes, or 41 radiation administration CPT codes. Last, the HRR was matched to the claim service facility zip code or the rendering physician zip code for ESRD facility and Managing Clinician, respectively.
For the modeling exercise used to estimate changes in payment to providers and suppliers and the resulting savings to Medicare, OACT maintained the previous method to identify ESRD facilities with common ownership, the low-volume exclusion threshold, and the aggregation assumptions as CMS has not proposed changes to these model policies. To clarify OACT's methodology, the ESRD facilities' data were aggregated to the CMS Certification Number (CCN) level for beneficiaries on dialysis identified by outpatient claims with Type of Bill 072X to capture all dialysis services furnished at or through ESRD facilities. Beneficiaries receiving home dialysis services were defined as condition codes 74 and 76 (§ 512.340). Condition code 75 was removed from the home dialysis definition because that billing code is no longer in use. Condition code 80 was removed because we want to exclude beneficiaries who received home dialysis furnished in a SNF or nursing facility. Beneficiaries receiving in-center dialysis services were defined using condition code 71. Two new variables were created: In-center self-dialysis, condition code 72 (§ 512.365) and in-center nocturnal dialysis, based on any of the claims' lines 1-5 HCPCS codes equal to the “UJ” modifier. Self-care in training and ESRD self-care retraining, condition codes 73 and 87, respectively, were only included in the denominator for the home dialysis rate calculation. For consistency with the exclusion in § 512.385(a), after grouping within each HRR, aggregated ESRD facilities with less than 132 total attributed beneficiary months during a given MY were excluded. When constructing benchmarks, for consistency with the methodology for aggregating performance for purposes of the PPA calculation, we aggregated all ESRD facilities owned in whole or in part by the same dialysis organization located in the same HRR.
The Managing Clinicians' performance data were aggregated to the Tax Identification Number (TIN) level (for group practices) and the individual National Provider Identifier (NPI) level (for solo practitioners). For purposes of calculating the home dialysis rate, beneficiaries on home dialysis were identified using outpatient claims with CPT® codes 90965 and 90966 (§ 512.345). Beneficiaries receiving in-center dialysis were identified by outpatient claims with CPT® codes 90957, 90958, 90959, 90960, 90961, and 90962 (§ 512.360). Last, following the low-volume threshold described in § 512.385(b), after grouping within each HRR, Managing Clinicians with less than 132 total attributed beneficiary months during a given MY were excluded.
The Scientific Registry of Transplant Recipients (SRTR) transplant waitlist data were obtained from the Center for Clinical Standards and Quality (CCSQ). To construct the transplant waitlist rate, the numerator was based on per-patient counts and included every addition to the waitlist for a patient in any past year. The waitlist counts for the numerator included waitlists for kidney transplants, alone or with another organ, active and inactive records, multi-organ listings, and patients that have subsequently been removed from the waitlist. The denominator was a unique count of prevalent dialysis patients as of the end of the year. Only patients on dialysis as of December 31st for the selected year were included. Facility attribution was based on the facility the patient was admitted to on the last day of the year.
For MY1 and MY2, the home dialysis score and transplant score for the PPA were calculated using the following methodology for the ESRD facilities and Managing Clinicians. ETC Participant Start Printed Page 36423behavior for each year was simulated by adjusting the ETC Participant's baseline home dialysis (or transplant) rate for a simulated statistical fluctuation and then summing with the assumed increase in home dialysis (or transplant) rate multiplied by a randomly generated improvement scalar. The achievement and improvement scores were assigned by comparing the ETC Participant's simulated home dialysis (or transplant) rate for the MY to the percentile distribution of home dialysis (or transplant) rates in the prior year. Last, the MPS was calculated using the weighted sum of the higher of the achievement or improvement score for the home dialysis rate and the transplant waitlist rate. The home dialysis rate constituted two-thirds of the MPS, and the transplant rate one-third of the MPS.
For MY3 through MY10, the home dialysis rate calculation accounts for modifications proposed in this proposed rule. For Managing Clinicians, the proposed revisions include changing the numerator for the home dialysis rate from the home dialysis beneficiary months to the home dialysis beneficiary months + 0.5(in-center self-dialysis beneficiary months) + 0.5*(nocturnal in-center dialysis beneficiary months), such that 1-beneficiary year is comprised of 12-beneficiary months. The proposed revision for the numerator of the home dialysis rate for ESRD facilities varied if the facility was owned in whole or in part by an ETC LDO, as identified by ownership information for the associated CCN. If the CCN had facilities owned by an ETC LDO, then the proposed numerator for the home dialysis rate was the home dialysis beneficiary months + 0.5*(in-center self-dialysis beneficiary months); therefore, not including nocturnal in-center dialysis months from the numerator. Otherwise, if the CCN did not have facilities owned by an ETC LDO, then the numerator was the same as described above for Managing Clinicians, such that the numerator for the home dialysis rate was home dialysis beneficiary months + 0.5*(in-center self-dialysis beneficiary months) + 0.5*(nocturnal in-center dialysis beneficiary months).
The number of beneficiaries on in-center self-dialysis who met the eligibility criteria for the ETC Model was very small, ranging from 102 to 277 over the period 2012-2019 and decreasing 89.9 percent to 22 beneficiaries in 2020 (based on preliminary 2020 data at CMS). With such a small sample size, the growth rate vacillated significantly. In addition, the in-center nocturnal dialysis UJ modifier code did not become effective until January 1, 2017; therefore, there were insufficient data to generate growth rate assumptions. The in-center nocturnal dialysis beneficiary growth rate decreased by 91.3 percent in 2020. As a solution to these data limitations, to simulate the impact of incorporating in-center self-dialysis and in-center nocturnal dialysis for the purpose of the savings to Medicare estimate, the simulation assumed any given ESRD facility or Managing Clinician would have a one percent chance of receiving an increased achievement score due to this policy proposal.
The overall process for generating achievement and improvement scoring followed modeling from section VI.C.2 of the Specialty Care Models final rule (85 FR 61352), with the exception of the following changes.
Beginning for MY3 and beyond, the achievement benchmarking methodology had two proposed modifications. First, the home dialysis rate and transplant waitlist rate benchmarks were increased by a total of 10 percent relative to ESRD facilities and Managing Clinicians not selected for participation, every two MYs. To clarify, no changes to the achievement benchmarking methodology were made to MYs 1 and 2. The latter MY couplets' achievement benchmarking included the following preset benchmark updates:
- MYs 3 and 4: Comparison Geographic Area percentiles*1.10,
- MYs 5 and 6: Comparison Geographic Area percentiles*1.20,
- MYs 7 and 8: Comparison Geographic Area percentiles*1.30, and
- MYs 9 and 10: Comparison Geographic Area percentiles*1.40.
The percentiles represented the 30th, 50th, 75th, and 90th percentile of the home dialysis rate and transplant rate for ESRD facilities and Managing Clinicians not selected for participation. The preset benchmark updates method provides greater certainty to ETC Participants than the rolling updates in section IV.C.2.b(3) of the Specialty Care Models final rule (85 FR 61353), which would have involved updating benchmarks based on emerging trends over the most recent experience periods for which data were available.
Second, in this proposed rule, we proposed to incorporate two proxies for socioeconomic status, dual eligibility status or receipt of the Low Income Subsidy (LIS), as part of the achievement benchmarking starting for MY3 and beyond. Dual eligibility status was defined as a Medicare beneficiary with any of the following full-time dual type codes: 02=Eligible is entitled to Medicare Qualified Medicare Beneficiary (QMB) and Medicaid coverage including prescription drugs, 04=Eligible is entitled to Medicare Specified Low-Income Medicare Beneficiary (SLMB) and Medicaid coverage including prescription drugs, or 08=Eligible is entitled to Medicare Other dual eligible with Medicaid coverage including prescription drugs. Separately, a yes/no indicator was created for any beneficiary that was either deemed or determined by the Social Security Administration (SSA) to be receiving the LIS. The home dialysis rate and transplant waitlist rate achievement benchmarks were then stratified by the proportion of attributed beneficiaries who are dual-eligible or receive the LIS. Two strata were created with a cutpoint of approximately 50 percent for participants with any dual-eligible or LIS recipient beneficiaries and those who do not have beneficiaries meeting the socioeconomic status proxies.
Third, a Health Equity Incentive was proposed for improvement scoring starting in MY3. For the purpose of the estimates in this Regulatory Impact Analysis, we incorporated a random variable to simulate each ETC Participant's baseline variation and behavioral improvement for each MY. If the participant's simulated improvement behavior in MY3 through MY10 was greater than 5 percent, then the participant received a 0.5 point increase on their improvement score, allowing for a maximum of 2.0 total points.
For all MYs, the transplant waitlist benchmarks were annually inflated by approximately 3-percentage points growth. This was a modification from section VI.C.2 of the Specialty Care Models final rule (85 FR 61352), where the waitlist benchmarks were annually inflated by approximately 2-percentage points growth observed during years 2017 through 2019 in the CCSQ data, to project rates of growth. The additional 1 percentage point growth in this proposed rule was included to account for uncertainty from the COVID-19 PHE disruption and section 17006 of the 21st Century Cures Act (Cures Act) (Pub. L. 114-255), which amended the Act to increase enrollment options for individuals with ESRD into Medicare Advantage. To clarify, applying the 3-percentage point annual growth from the median transplant waitlist rate across HRR condensed facilities grew from 8 percent in 2017 to 11 percent in 2018 to 14 percent in 2019 (that is, not a growth rate of 1.03 percent per year).
To assess the impact of the COVID-19 PHE on the kidney transplant Start Printed Page 36424waitlist, we analyzed data from the United Network for Organ Sharing (UNOS).[305] . The UNOS data suggest that the number of new patients added to the kidney transplant waitlist steadily decreased between the weeks of March 15, 2020 through May 10, 2020, when between 16 to 81 percent of patients listed on the weekly kidney transplant waitlist became inactive due to COVID-19 precautions. During July through December 2020, the number of new patients added to the kidney transplant waitlist increased to near pre-pandemic levels with an average of less than 3 percent of patients listed as inactive due to COVID-19. Anomalous dips in the number of new patients added to the kidney transplant waitlist were observed during the weeks of November 22, 2020 and December 27, 2020, which correspond with federal holidays in addition to a period that Americans were asked to social distance to slow the spread of COVID-19. Continuing into the first quarter of 2021, new additions to the kidney transplant waitlist remained at approximately pre-pandemic rates. Therefore, we assume that the number of new patients added to the waitlist will not decrease as a result of the pandemic and the linear 2-percentage point growth rate for the transplant waitlist calculated using years 2017 through 2019 CCSQ data remains a reasonable assumption for baseline growth going forward. In the proposed rule, we also included a 1 percent increase to the standard error to account for a new variation assumption to address how year-over-year changes could fluctuate at the ESRD facility or Managing Clinician level, which was potentially exacerbated by the exclusion criteria (that is, residents of a nursing facility, receiving dialysis in a skilled nursing facility, dialysis for AKI only) applied to the updated model data source used for estimates in this proposed rule.
No changes were proposed to the payment structure for the HDPA calculation described in the final rule (§ 512.350). As such, the HDPA was calculated using the home dialysis and home dialysis-related payments adjusted by decreasing amounts (3, 2, and 1 percent) during each of the first 3 years of the Model.
The kidney disease patient education services utilization and cost data were identified by codes G0420 and G0421, to capture face-to-face individual and group training sessions for chronic kidney disease beneficiaries on treatment modalities. The home dialysis training costs for incident beneficiaries on home dialysis for Continuous Ambulatory Peritoneal Dialysis (CAPD) or Continuous Cycler-Assisted Peritoneal Dialysis (CCPD) were defined using CPT® codes 90989 and 90993 for complete and incomplete training sessions, respectively.
Data from CY 2019 were used to project baseline expenditures (that is, expenditures before the proposed changes were applied) and the traditional FFS payment system billing patterns were assumed to continue under current law.
(3) Medicare Estimate—Primary Specification, Assume Proposed Benchmark Updates
Start Printed Page 36425
Start Printed Page 36426

Table 18 summarizes the estimated impact of the ETC Model when assuming preset benchmark updates where the achievement benchmarks for each year are set using the average of the home dialysis rates for year t-1 and year t-2 for the HRRs randomly selected for participation in the ETC Model. We estimate the Medicare program will save a net total of $53 million from the PPA and HDPA between January 1, 2021 and June 30, 2027 less $15 million in increased training and education expenditures. Therefore, the net impact to Medicare spending is estimated to be $38 million in savings. In Table 18 and Table 19, negative spending reflects a reduction in Medicare spending, while positive spending reflects an increase. The results for both tables were generated from an average of 400 simulations under the assumption that benchmarks are rolled forward with a 1.5-year lag.
Table 19 is provided to isolate the total impact of the changes proposed in this proposed rule for years 2023 going forward by calculating the difference from our final estimates in Table 18 less totals from our current baseline estimates that used the same years of data, but without the model changes applied. To clarify, the baseline estimates are not the estimates reported in Table 19 of the Specialty Care Models final rule (85 FR 61354); the final rule used data from CYs 2016 and 2017 and this proposed rule used the most recent data available, from CYs 2018 and 2019. There was no impact reported in years 2021 and 2022 since the proposed payment adjustments were not effective until MY3. In addition, the proposed changes did not apply to the HDPA or the Kidney Disease Patient Education Services Costs and HD Training Costs. As expected, Table 19 shows that the proposed changes had a very small effect on Medicare savings; only $7 million in savings for the net impact to Medicare spending over the 4.5-year period can be attributed to the changes proposed in this rule.
As was the case in the Specialty Care Models final rule (85 FR 61353), the projections do not include the Part B premium revenue offset because the payment adjustments under the ETC Model will not affect beneficiary cost-sharing. Any potential effects on Medicare Advantage capitation payments were also excluded from the projections. This approach is consistent with how CMS has previously conveyed the primary FFS effects anticipated for an uncertain model without also assessing the potential impact on Medicare Advantage rates.
Returning to Table 18, as anticipated, the expected Medicare program savings were driven by the net effect of the Facility PPA; a reduction in Medicare spending of $74 million over the period from July 1, 2022 through June 30, 2027. In comparison, the net effect of the Clinician PPA was only $9 million in Medicare savings. This estimate was based on an empirical study of historical home dialysis utilization and transplant waitlist rates for Medicare FFS beneficiaries that CMS virtually attributed to ESRD facilities and to Managing Clinicians based on the plurality of associated spending at the beneficiary level. We analyzed the base variation in those facility/practice level measures and simulated the effect of the payment policy assuming providers and suppliers respond by marginally increasing their share of patients utilizing home dialysis. Random variables were used to vary the effectiveness that individual providers and suppliers might show in such progression over time and to simulate the level of year-to-year variation already noted in the base multi-year data that was analyzed. The uncertainty in the projection was illustrated in sections VII.C.2.b.(3)(a) and VII.C.2.b.(3)(b) of the Specialty Care Models final rule (85 FR 61354), respectively, through alternate scenarios assuming that the benchmarks against which ETC Participants are measured were to not be updated. In those sensitivity analyses, we analyzed a modified version of the model that included a fixed benchmark for the home dialysis and transplant waitlist rates as well as a separate sensitivity analysis that assumed a rolling benchmark for the home dialysis rate and a fixed benchmark for the transplant waitlist rate.
For this proposed rule, we are modeling a preset benchmark growth rate as proposed in this rule but continue to incorporate sensitivity to a range of potential behavioral changes for the home dialysis rate and transplant waitlist rate for ETC facilities and Managing Clinicians assumed to participate in the model. Kidney disease patient education services on treatment modalities and home dialysis (HD) training for incident dialysis beneficiaries are relatively small outlays Start Printed Page 36427and were projected to represent only relatively modest increases in Medicare spending each year.
The key assumptions underlying the impact estimate are that each consolidated ESRD facility or Managing Clinician's share of total maintenance dialysis provided in the home setting was assumed to grow by up to an assumed maximum growth averaging 3-percentage points per year. Factors underlying this assumption about the home dialysis growth rate include: Known limitations that may prevent patients from being able to dialyze at home, such as certain common disease types that make peritoneal dialysis impractical (for example, obesity); current equipment and staffing constraints; and the likelihood that a patient new to maintenance dialysis starts dialysis at home compared to the likelihood that a current dialysis patient who dialyzes in center switches to dialysis at home. In any given trial of the simulation, the maximum growth rate was chosen from a uniform distribution of 0 to 5-percentage points per year. Preliminary data from CMS show that the growth rate for home dialysis was 3.9 percent in CY 2020 for beneficiaries meeting the eligibility criteria for the ETC Model. This growth rate is within range to what was observed prior to the establishment of the Advancing American Kidney Health initiative in 2019 and it also shows that the COVID-19 PHE did not cause the home dialysis growth assumption to become invalid. The 3-percentage point per year average max growth rate will, in effect, move the average market peritoneal dialysis rate (about 10 percent) to the highest market baseline peritoneal dialysis rate (for example, Bend, Oregon HRR at about 25 percent), which we believe is a reasonable upper bound on growth over the duration of the ETC Model for the purposes of this actuarial model.
Consolidated ESRD facilities at the HRR level or Managing Clinicians were assumed to achieve anywhere from zero to 100 percent of such maximum growth in any given year. Thus, the average projected growth for the share of maintenance dialysis provided in the home was 1.5-percentage points per year (expressed as the percentage of total dialysis). In contrast, we do not include an official assumption that the overall number of kidney transplants will increase and provide justification for this assumption in sections VI.C.2.b.(4) and VI.C.2.b.(5) of the Specialty Care Models final rule (85 FR 61355). However, as part of the sensitivity analysis for the savings calculations for the model, we laid out a different savings scenario if the ETC Learning Collaborative described in VI.C.2.b.(6) of the Specialty Care Models final rule (85 FR 61355) were to be successful in decreasing the discard rate of deceased donor kidneys and increasing the utilization rate of deceased donor kidneys that have been retrieved.
(a) Sensitivity Analysis: Medicare Savings Estimate—Results for the 10th and 90th Percentiles
Using the primary specification for the Medicare estimate with preset benchmark updates for home dialysis and transplant waitlist rates, we compare the results for the top 10th and 90th percentiles of the 400 individual simulations to the average of all simulation results reported in Table 18. Since the impact on Medicare spending for the ETC Model using the present benchmark updates is estimated to be in savings rather than losses, the top 10th and 90th percentiles represent the most optimistic and conservative projections, respectively. The overall net PPA and HDPA for the top 10th and 90th percentiles using the present benchmark updates method are $117 million in savings and $3 million in losses (encompassing the mean estimate of $53 million in savings in Table 18). The overall uncertainty of the impact of the model is further illustrated in Table 18, the change from baseline, where the mean $7 million dollars in savings reported for the Overall PPA Net & HDPA has $83 million in savings and $75 million in losses, for the top 10th and 90th percentiles, respectively.
(4) Effects on the Home Dialysis Rate
This proposed rule proposes to modify the home dialysis rate equation by adding 0.5 multiplied by the sum of the self-dialysis beneficiary months and the in-center nocturnal dialysis beneficiary months to the numerator such that 1-beneficiary year is comprised of 12-beneficiary months. The proposed modification was different for ESRD facilities with an aggregation group that had facilities owned by an ETC LDO, for which the nocturnal dialysis months were not included in the numerator.
Less than 1 percent of beneficiaries eligible for attribution into the ETC Model were receiving either self-dialysis or nocturnal in-center dialysis in CY 2019. In addition, in CY 2020, the annual growth rate decreased by 89.9 and 91.3 percent for beneficiaries receiving self-dialysis or nocturnal dialysis, respectively. The sharp decline in these dialysis modalities is potentially in response to the COVID-19 pandemic. The low historical take-up for self-dialysis and shortage of historical years for nocturnal dialysis (that is, a nocturnal dialysis claims line instruction became effective in 2017) result in these proposed modifications having an insignificant impact on the savings to Medicare.
Two of the changes proposed in this proposed rule have the potential to generate higher PPA scores for a limited subset of providers and therefore a small negative impact on estimated savings for the model. First, we proposed two strata for the achievement and improvement benchmarking based on a 50 percent cutpoint for the proportion of attributed beneficiaries with dual eligibility status or receipt of the LIS. This proposed modification would allow participants to be compared to participants who serve ESRD patients with a similar socioeconomic status, essentially making the comparison groups fairer and potentially increasing the cost to Medicare. Second, the proposed Health Equity Incentive rewarded participants with 0.5 points to their improvement score who demonstrated a sufficiently significant improvement on the home dialysis rate among their attributed beneficiaries who are dual eligible or receive the LIS.
Furthermore, we modeled the home dialysis rate achievement and improvement benchmarks by incrementally increasing every two measurement periods the benchmarks by 10 percent relative to ESRD facilities and Managing Clinicians not selected for participation. Applying the preset benchmarks update method balanced out the negative impact to Medicare savings generated from stratification and the Health Equity Incentive, essentially preserving the overall savings level reported in the Specialty Care Models final rule.
(5) Effects on Kidney Transplantation
Kidney transplantation is considered the optimal treatment for most ESRD beneficiaries. The PPA includes a one-third weight on the ESRD facilities' or Managing Clinician's transplant waitlist rate, with the ultimate goal of increasing the rate of kidney transplantation. However, the changes proposed in this proposed rule do not impact our decision in the previous final rule to not include an assumption that the overall number of kidney transplants will increase. The number of ESRD patients on the kidney transplant waitlist has for many years far exceeded the annual number of transplants performed. Transplantation rates have not increased to meet such demand because of the limited supply of deceased donor Start Printed Page 36428kidneys. The U.S. Renal Data System [306] reported 22,393 kidney transplants in 2018 compared to a kidney transplant waiting list [307] of over 98,000. Refer to section VI.C.2.b(4) in the Specialty Care Models final rule (85 FR 61355) for a detailed justification for our assumption that the overall number of kidney transplants will not increase in response to ESRD facilities and Managing Clinicians participating in the ETC Model.
(6) Effects of the Transplant Waitlist Rate
This proposed rule includes the transplant waitlist rate described in the Specialty Care Models final rule (§ 512.365) with the following proposed modifications. First, we are proposing to exclude Medicare beneficiaries with a diagnosis of and treatment with chemotherapy or radiation for vital solid organ cancers. In our analysis of beneficiaries' eligible for the ETC Model, we found that less than 1 percent of the beneficiaries had claims for any vital solid organ cancers. Therefore, the effect of this proposed exclusion criterion is to make the beneficiaries included in the calculation of the transplant rate an improved representation of beneficiaries who are able to join the transplant waitlist and/or receive pre-emptive living donor kidney transplantation. But, due to the very low number of ETC Model potential beneficiaries with these types of cancer, the exclusion criterion is unlikely to have any significant impact on the transplant waitlist rate.
Two of the changes proposed in this proposed rule have the potential to generate higher scores for a limited subset of health care providers and therefore a small negative impact on estimated savings for the model. First, we proposed two strata for the achievement and improvement benchmarking based on a 50 percent cutpoint for the proportion of attributed beneficiaries with dual eligibility status or receipt of the LIS. This proposed modification allowed participants to be compared to participants who serve ESRD patients with a similar socioeconomic status, essentially making the comparison groups fairer and potentially increasing the cost to Medicare. Second, the proposed Health Equity Incentive rewarded participants with 0.5 points to their improvement score who demonstrated a sufficiently significant improvement on the transplant rate among their attributed beneficiaries who are dual eligible or receive the LIS.
Furthermore, we proposed to modify the transplant waitlist rate achievement and improvement benchmarks by incrementally increasing the benchmarks every two measurement periods by 10 percent relative to ESRD facilities and Managing Clinicians not selected for participation. Applying the preset benchmarks update method balanced out the negative impact to Medicare savings generated from the proposed stratification and the Health Equity Incentive, roughly preserving the overall savings level estimated at baseline for the model parameters previously finalized before the changes offered in this proposed rule.
(7) Effects on Kidney Disease Patient Education Services and HD Training Add-Ons
The changes in this proposed rule do not impact the findings reported for the effects of the ETC Model on the Kidney Disease Patient education services and HD training add-ons described in section VI.C.2.b(6) in the Specialty Care Models final rule (85 FR 61355).
b. Effects on Medicare Beneficiaries
The changes in this proposed rule could incentivize ESRD facilities and Managing Clinicians serving dual eligible or LIS recipient Medicare beneficiaries to potentially improve access to care for those beneficiaries. The changes could also marginally improve take-up of the in-center nocturnal dialysis treatment modality compared to how the model was finalized previously since these dialysis methods were not directly incentivized (that is, accounted for in the home dialysis rate and in-center self dialysis rate numerator) in the Specialty Care Models final rule.
As previously noted in section VI.C.3.B of the Specialty Care Models final rule (85 FR 61357), we continue to anticipate that the ETC Model would have a negligible impact on the cost to beneficiaries receiving dialysis. Under current policy, Medicare FFS beneficiaries are generally responsible for 20 percent of the allowed charge for services furnished by providers and suppliers. This policy will remain the same under the ETC Model. However, we will waive certain requirements of title XVIII of the Act as necessary to test the PPA and HDPA under the ETC Model and to hold beneficiaries harmless from any effect of these payment adjustments on cost sharing. In addition, the Medicare beneficiary's quality of life has the potential to improve if the beneficiary elects to have home dialysis as opposed to in-center dialysis. Studies have found that home dialysis patients experienced improved quality of life as a result of their ability to continue regular work schedules or life plans; as well as better overall, physical, and psychological health in comparison to other dialysis options.
c. Alternatives Considered
Throughout this proposed rule, we have identified our policies and alternatives that we have considered, and provided information as to the likely effects of these alternatives and the rationale for each of our policies.
This proposed rule addresses a model specific to ESRD. It provides descriptions of the requirements that we would waive, identifies the performance metrics and payment adjustments proposed to be tested, and presents rationales for our proposals, and where relevant, alternatives that we considered. We carefully considered the alternatives to this proposed rule, including the degree that benchmark targets should be prospectively updated to provide greater transparency to ETC Participants while preserving the expectation for model net savings for the program. For context related to alternatives previously considered when establishing the ETC Model we refer readers to the Specialty Cares Model final rule (85 FR 61114) for more information on policy-related stakeholder comments, our responses to those comments, and statements of final policy preceding the limited modifications proposed here.
C. Accounting Statement
As required by OMB Circular A-4 (available at https://www.whitehouse.gov/sites/whitehouse.gov/files/omb/circulars/A4/a-4.pdf), in Table 20, we have prepared an accounting statement showing the classification of the transfers and costs associated with the various provisions of this proposed rule.
Start Printed Page 36429
In accordance with the provisions of Executive Order 12866, this proposed rule was reviewed by the Office of Management and Budget.
D. Regulatory Flexibility Act Analysis (RFA)
The Regulatory Flexibility Act (RFA) requires agencies to analyze options for regulatory relief of small entities, if a rule has a significant impact on a substantial number of small entities. For purposes of the RFA, small entities include small businesses, nonprofit organizations, and small governmental jurisdictions. Approximately 11 percent of ESRD dialysis facilities are considered small entities according to the Small Business Administration's (SBA) size standards, which classifies small businesses as those dialysis facilities having total revenues of less than $41.5 million in any 1 year. Individuals and states are not included in the definitions of a small entity. For more information on SBA's size standards, see the Small Business Administration's website at http://www.sba.gov/content/small-business-size-standards (Kidney Dialysis Centers are listed as 621492 with a size standard of $41.5 million).
When viewed as individual entities, as opposed to being a part of an LDO, there are approximately 643 (~12 percent of total number of ESRD facilities) ESRD facilities that provide fewer than 4,000 treatments per year. With a low volume payment adjustment, each facility generates revenue from dialysis treatments of ~$1.26 million per year per facility. This is shown in the Table 21.
Start Printed Page 36430
We do not believe ESRD facilities are operated by small government entities such as counties or towns with populations of 50,000 or less, and therefore, they are not enumerated or included in this estimated RFA analysis. Individuals and states are not included in the definition of a small entity.
For purposes of the RFA, we estimate that approximately 11 percent of ESRD facilities are small entities as that term is used in the RFA (which includes small businesses, nonprofit organizations, and small governmental jurisdictions). This amount is based on the number of ESRD facilities shown in the ownership category in Table 9. Using the definitions in this ownership category, we consider 515 facilities that are independent and 378 facilities that are shown as hospital-based to be small entities. The ESRD facilities that are owned and operated by Large Dialysis Organizations (LDOs) and regional chains would have total revenues of more than $41.5 million in any year when the total revenues for all locations are combined for each business (individual LDO or regional chain), and are not, therefore, included as small entities.
For the ESRD PPS updates proposed in this rule, a hospital-based ESRD facility (as defined by type of ownership, not by type of dialysis facility) is estimated to receive a 1.3 percent increase in payments for CY 2022. An independent facility (as defined by ownership type) is estimated to receive a 1.1 percent increase in payments for CY 2022.
For AKI dialysis, we are unable to estimate whether patients would go to ESRD facilities, however, we have estimated there is a potential for $52 million in payment for AKI dialysis treatments that could potentially be furnished in ESRD facilities.
For ETC Model, this proposed rule includes as ETC Participants Managing Clinicians and ESRD facilities required to participate in the Model pursuant to § 512.325(a). We assume for the purposes of the regulatory impact analysis that the great majority of Managing Clinicians are small entities and that the greater majority of ESRD facilities are not small entities. Throughout the proposed rule we describe how the adjustments to certain payments for dialysis services and dialysis-related services furnished to ESRD beneficiaries may affect Managing Clinicians and ESRD facilities participating in the ETC Model. The great majority of Managing Clinicians are small entities by meeting the SBA definition of a small business (having minimum revenues of less than $8 million to $41.5 million in any 1 year, varying by type of provider and highest for hospitals) with a minimum threshold for small business size of $41.5 million (https://www.sba.gov/document/support--table-size-standards http://www.sba.gov/content/small-businesssize-standards). The great majority of ESRD facilities are not small entities, as they are owned, partially or entirely by entities that do not meet the SBA definition of small entities.
The HDPA in the ETC Model is a positive adjustment on payments for specified home dialysis and home dialysis-related services. The PPA in the ETC Model, which includes both positive and negative adjustments on payments for dialysis services and dialysis-related services, excludes aggregation groups with fewer than 132 attributed beneficiary-months during the relevant year.
The aggregation methodology groups ESRD facilities owned in whole or in part by the same dialysis organization within a Selected Geographic Area and Managing Clinicians billing under the same TIN within a Selected Geographic Area. This aggregation policy increases the number of beneficiary months, and thus statistical reliability, of the ETC Participant's home dialysis and transplant rate for ESRD facilities that are owned in whole or in part by the same dialysis organization and for Managing Clinicians that share a TIN with other Managing Clinicians.
Taken together, the low volume threshold exclusions and aggregation policies previously described, coupled with the fact that the ETC Model would affect Medicare payment only for select services furnished to Medicare FFS beneficiaries; we have determined that the provisions of the proposed rule would not have a significant impact on spending for a substantial number of small entities (defined as greater than 5 percent impact).
Therefore, the Secretary has determined that this proposed rule would not have a significant economic impact on a substantial number of small entities. The economic impact assessment is based on estimated Medicare payments (revenues) and HHS's practice in interpreting the RFA is to consider effects economically “significant” only if greater than 5 percent of providers reach a threshold of 3 to 5 percent or more of total revenue or total costs. We solicit comment on the RFA analysis provided.
In addition, section 1102(b) of the Act requires us to prepare a RIA if a rule may have a significant impact on the operations of a substantial number of small rural hospitals. This analysis must conform to the provisions of section 603 Start Printed Page 36431of the RFA. For purposes of section 1102(b) of the Act, we define a small rural hospital as a hospital that is located outside of a metropolitan statistical area and has fewer than 100 beds. We do not believe this proposed rule would have a significant impact on operations of a substantial number of small rural hospitals because most dialysis facilities are freestanding. While there are 122 rural hospital-based dialysis facilities, we do not know how many of them are based at hospitals with fewer than 100 beds. However, overall, the 122 rural hospital-based dialysis facilities would experience an estimated 1.0 percent increase in payments.
Therefore, the Secretary has determined that this proposed rule would not have a significant impact on the operations of a substantial number of small rural hospitals.
E. Unfunded Mandates Reform Act Analysis (UMRA)
Section 202 of the Unfunded Mandates Reform Act of 1995 (UMRA) also requires that agencies assess anticipated costs and benefits before issuing any rule whose mandates require spending in any 1 year of $100 million in 1995 dollars, updated annually for inflation. In 2021, that threshold is approximately $158 million. This proposed rule does not mandate any requirements for state, local, or tribal governments in the aggregate, or by the private sector. Moreover, HHS interprets UMRA as applying only to unfunded mandates. We do not interpret Medicare payment rules as being unfunded mandates, but simply as conditions for the receipt of payments from the federal government for providing services that meet federal standards. This interpretation applies whether the facilities or providers are private, state, local, or tribal.
F. Federalism
Executive Order 13132 establishes certain requirements that an agency must meet when it promulgates a proposed rule (and subsequent final rule) that imposes substantial direct requirement costs on state and local governments, preempts state law, or otherwise has federalism implications. We have reviewed this proposed rule under the threshold criteria of Executive Order 13132, Federalism, and have determined that it would not have substantial direct effects on the rights, roles, and responsibilities of states, local or Tribal governments.
G. Congressional Review Act
These proposed rules are subject to the Congressional Review Act provisions of the Small Business Regulatory Enforcement Fairness Act of 1996 (5 U.S.C. 801 et seq.) and has been transmitted to the Congress and the Comptroller General for review.
X. Files Available to the Public via the Internet
The Addenda for the annual ESRD PPS proposed and final rulemakings will no longer appear in the Federal Register. Instead, the Addenda will be available only through the internet and is posted on the CMS website at http://www.cms.gov/ESRDPayment/PAY/list.asp. In addition to the Addenda, limited data set files are available for purchase at http://www.cms.gov/Research-Statistics-Data-and-Systems/Files-for-Order/LimitedDataSets/EndStageRenalDiseaseSystemFile.html. Readers who experience any problems accessing the Addenda or LDS files, should contact ESRDPayment@cms.hhs.gov.
Chiquita Brooks-LaSure, Administrator of the Centers for Medicare & Medicaid Services, approved this document on June 16, 2021.
Start List of SubjectsList of Subjects
42 CFR Part 413
- Diseases
- Health facilities
- Medicare
- Puerto Rico
- Reporting and recordkeeping requirements
42 CFR Part 512
- Administrative practice and procedure
- Health facilities
- Medicare
- Reporting and recordkeeping requirements
For the reasons set forth in the preamble, the Centers for Medicare & Medicaid Services proposes to amend 42 CFR chapter IV as follows:
Start PartPART 413—PRINCIPLES OF REASONABLE COST REIMBURSEMENT; PAYMENT FOR END-STAGE RENAL DISEASE SERVICES; PROSPECTIVELY DETERMINED PAYMENT RATES FOR SKILLED NURSING FACILITIES; PAYMENT FOR ACUTE KIDNEY INJURY DIALYSIS
End Part Start Amendment Part1. The authority citation for part 413 continues to read as follows:
End Amendment Part Start Amendment Part2. Section 413.177 is amended by revising paragraph (a) introductory text to read as follows:
End Amendment PartStart Amendment PartQuality incentive program payment.(a) With respect to renal dialysis services as defined under § 413.171, except for those renal dialysis services furnished during payment year 2022, in the case of an ESRD facility that does not earn enough points under the program described at § 413.178 to meet or exceed the minimum total performance score (as defined at § 413.178(a)(8)) established by CMS for a payment year (as defined at § 413.178(a)(10)), payments otherwise made to the facility under § 413.230 for renal dialysis services during the payment year, will be reduced by up to 2 percent as follows:
3. Section 413.178 is amended by adding paragraph (h) to read as follows:
End Amendment PartStart PartESRD quality incentive program.* * * * *(h) Special rule for payment year 2022. (1) CMS will calculate a measure rate for all measures specified by CMS under paragraph (c) of this section for the PY 2022 ESRD QIP but will not score facility performance on any of those measures or calculate a TPS for any facility under paragraph (e) of this section.
(2) CMS will not establish a mTPS for PY 2022.
PART 512—RADIATION ONCOLOGY MODEL AND END STAGE RENAL DISEASE TREATMENT CHOICES MODEL
End Part Start Amendment Part4. The authority citation for part 512 continues to read as follows:
End Amendment Part Start Amendment Part5. Section 512.160 is amended by adding paragraph (a)(9), and by revising paragraph (b)(6) as follows:
End Amendment PartStart Amendment PartRemedial action.(a) * * *
(9) For the ETC Model only, has misused or disclosed the beneficiary-identifiable data in a manner that violates any applicable statutory or regulatory requirements or that is otherwise non-compliant with the provisions of the applicable data sharing agreement.
(b) * * *
(6) In the ETC Model only:
(i) Terminate the ETC Participant from the ETC Model.
(ii) Suspend or terminate the ability of the ETC Participant, pursuant to § 512.397(c), to reduce or waive the Start Printed Page 36432coinsurance for kidney disease patient education services.
6. Section 512.310 is amended by adding the definitions of “Clinical staff”, “Health Equity Incentive”, “Kidney disease patient education services coinsurance patient incentive”, and “Qualified staff” in alphabetical order to read as follows:
End Amendment PartStart Amendment PartDefinitions.* * * * *Clinical staff means a licensed social worker or registered dietician/nutrition professional who furnishes services for which payment may be made under the physician fee schedule under the direction of and incident to the services of the Managing Clinician who is an ETC Participant.
* * * * *ETC Large Dialysis Organization (ETC LDO) means a legal entity that owns, in whole or in part, 500 or more ESRD facilities.
* * * * *Health Equity Incentive means the amount added to the ETC Participant's improvement score, calculated as described in § 512.370(c)(1) of this chapter, if the ETC Participant's aggregation group demonstrated sufficient improvement on the home dialysis rate or transplant rate for attributed beneficiaries who are dual eligible or Medicare Low Income Subsidy (LIS) recipients between the Benchmark Year and the MY.
* * * * *Qualified staff means both clinical staff and any qualified person (as defined at § 410.48(a)) who is an ETC Participant.
* * * * *7. Section 512.360 is amended by revising paragraph (c)(2)(ii) introductory text and adding paragraph (c)(2)(iii) to read as follows:
End Amendment PartStart Amendment PartBeneficiary population and attribution.* * * * *(c) * * *
(2) * * *
(ii) For MY1 and MY2, a Pre-emptive LDT Beneficiary who is not excluded based on the criteria in paragraph (b) of this section is attributed to the Managing Clinician with whom the beneficiary has had the most claims between the start of the MY and the month in which the beneficiary received the transplant for all months between the start of the MY and the month of the transplant.
* * * * *(iii) For MY3 through MY10, a Pre-emptive LDT Beneficiary who is not excluded based on the criteria in paragraph (b) of this section is attributed to the Managing Clinician who submitted the most claims for services furnished to the beneficiary in the 365 days preceding the date in which the beneficiary received the transplant.
(A) If no Managing Clinician has had the most claims for a given Pre-emptive LDT Beneficiary such that multiple Managing Clinicians each had the same number of claims for that beneficiary in the 365 days preceding the date of the transplant, the Pre-emptive LDT Beneficiary is attributed to the Managing Clinician associated with the latest claim service date at the claim line through date during the 365 days preceding the date of the transplant.
(B) If no Managing Clinician had the most claims for a given Pre-emptive LDT Beneficiary such that multiple Managing Clinicians each had the same number of claims for that beneficiary in the 365 days preceding the date of the transplant, and more than one of those Managing Clinicians had the latest claim service date at the claim line through date during the 365 days preceding the date of the transplant, the Pre-emptive LDT Beneficiary is randomly attributed to one of these Managing Clinicians.
(C) The Pre-emptive LDT Beneficiary is considered eligible for attribution under this paragraph (c)(2)(iii) if the Pre-emptive LDT Beneficiary has at least 1-eligible month during the 12-month period that includes the month of the transplant and the 11 months prior to the month of the transplant. An eligible month refers to a month during which the Pre-emptive LDT Beneficiary not does not meet exclusion criteria in paragraph (b) of this section.
8. Section 512.365 is amended by—
End Amendment Part Start Amendment Parta. Revising paragraphs (b)(1)(ii) and (b)(2)(ii), and
End Amendment Part Start Amendment Partb. Revising paragraphs (c)(1)(i)(A), (c)(1)(ii)(A), (c)(2)(i)(A), and (c)(2)(ii)(A)( 1) and (2).
End Amendment PartThe revisions read as follows:
Start Amendment PartPerformance assessment.* * * * *(b) * * *
(1) * * *
(ii) For MY1 and MY2, the numerator is the total number of home dialysis treatment beneficiary years plus one half the total number of self dialysis treatment beneficiary years for attributed ESRD Beneficiaries during the MY. For MY3 through MY10, the numerator for ESRD facilities owned in whole or in part by an ETC LDO is the total number of home dialysis treatment beneficiary years plus one half the total number of self dialysis treatment beneficiary years for attributed ESRD Beneficiaries during the MY. For MY3 through MY10, the numerator for ESRD facilities not owned in whole or in part by an ETC LDO is the total number of home dialysis treatment beneficiary years, plus one half the total number of self dialysis treatment beneficiary years, plus one half the total number of nocturnal in center dialysis beneficiary years for attributed ESRD Beneficiaries during the MY.
(A) Home dialysis treatment beneficiary years included in the numerator are composed of those months during which attributed ESRD Beneficiaries received maintenance dialysis at home, such that 1-beneficiary year is comprised of 12-beneficiary months. Months in which an attributed ESRD Beneficiary received maintenance dialysis at home are identified by claims with Type of Bill 072X and condition codes 74 or 76.
(B) Self dialysis treatment beneficiary years included in the numerator are composed of those months during which attributed ESRD Beneficiaries received self dialysis in center, such that 1-beneficiary year is comprised of 12-beneficiary months. Months in which an attributed ESRD Beneficiary received self dialysis are identified by claims with Type of Bill 072X and condition code 72.
(C) Nocturnal in center dialysis beneficiary years included in the numerator are composed of those months during which attributed ESRD Beneficiaries received nocturnal in center dialysis, such that 1-beneficiary year is comprised of 12-beneficiary months. Months in which an attributed ESRD Beneficiary received nocturnal in center dialysis are identified by claims with Type of Bill 072X and modifier UJ.
* * * * *(2) * * *
(ii) For MY1 and MY2, the numerator is the total number of home dialysis treatment beneficiary years for attributed ESRD Beneficiaries during the MY plus one half the total number of self dialysis treatment beneficiary years. For MY3 through MY10, the numerator is the total number of home dialysis treatment beneficiary years, plus one half the total number of self dialysis treatment beneficiary years, plus one half the total number of nocturnal in center dialysis beneficiary years for attributed ESRD Beneficiaries during the MY.
(A) Home dialysis treatment beneficiary years included in the numerator are composed of those months during which attributed ESRD Beneficiaries received maintenance Start Printed Page 36433dialysis at home, such that 1-beneficiary year is comprised of 12-beneficiary months. Months in which an attributed ESRD Beneficiary received maintenance dialysis at home are identified by claims with CPT codes 90965 or 90966.
(B) Self-dialysis treatment beneficiary years included in the numerator are composed of those months during which attributed ESRD Beneficiaries received self dialysis in center, such that 1-beneficiary year is comprised of 12-beneficiary months. Months in which an attributed ESRD Beneficiary received self dialysis are identified by claims with Type of Bill 072X and condition code 72.
(C) Nocturnal in center dialysis beneficiary years included in the numerator are composed of those months during which attributed ESRD Beneficiaries received nocturnal in center dialysis, such that 1-beneficiary year is comprised of 12-beneficiary months. Months in which an attributed ESRD Beneficiary received nocturnal in center dialysis are identified by claims with Type of Bill 072X and modifier UJ.
* * * * *(c) * * *
(1) * * *
(i) * * *
(A) The denominator is the total dialysis treatment beneficiary years for attributed ESRD Beneficiaries during the MY. Dialysis treatment beneficiary years included in the denominator are composed of those months during which an attributed ESRD beneficiary received maintenance dialysis at home or in an ESRD facility, such that 1-beneficiary year is comprised of 12-beneficiary months. For MY1 and MY2, months during which an attributed ESRD Beneficiary received maintenance dialysis are identified by claims with Type of Bill 072X, excluding claims for beneficiaries who were 75 years of age or older at any point during the month. For MY3 through MY10, months during which an attributed ESRD Beneficiary received maintenance dialysis are identified by claims with Type of Bill 072X, excluding claims for beneficiaries who were 75 years of age or older at any point during the month, or had a vital solid organ cancer diagnosis and were receiving treatment with chemotherapy or radiation for vital solid organ cancer during the MY.
(1) An attributed ESRD Beneficiary had a diagnosis of vital solid organ cancer in an MY if the beneficiary had any of the following diagnosis codes on any claim during the MY or the 6 months prior to the start of the MY: C22.0-C22.9, C34.10-C34.12, C34.2, C34.30-C34.32, C34.80-C34.82, C34.90-C34.92, C38.0, C38.8, C46.50-C46.52, C64.1, C64.2, C64.2, C78.00-C78.02, C78.7, C79.00-C79.02, C7A.090, C7A.093, or C7B.02.
(2) Months in which an attributed ESRD Beneficiary received treatment with chemotherapy or radiation for vital solid organ cancer are months during which the beneficiary had a claim with any of the following procedure codes:
(i) CPT® 96401-96402, 96405-96406, 96409, 96411, 96413, 96415-96417, 96420, 96422-26423, 96425, 96440, 96446, 96549, 77373, 77401-77402, 77407, 77412, 77423, 77424-77425, 77520, 77522-77523, 77525, 77761-77763, 77770-77772, 77778, 77789, 77799, 79005, 79101, 79200, 79300, 79403, 79440, 79445, 79999.
(ii) ICD-10-PCS® DB020ZZ, DB021ZZ, DB022ZZ, DB023Z0, DB023ZZ, DB024ZZ, DB025ZZ, DB026ZZ, DB1297Z, DB1298Z, DB1299Z, DB129BZ, DB129CZ, DB129YZ, DB12B6Z, DB12B7Z, DB12B8Z, DB12B9Z, DB12BB1, DB12BBZ, DB12BCZ, DB12BYZ, DB22DZZ, DB22HZZ, DB22JZZ, DBY27ZZ, DBY28ZZ, DBY2FZZ, DBY2KZZ, DB070ZZ, DB071ZZ, DB072ZZ, DB073Z0, DB073ZZ, DB074ZZ, DB075ZZ, DB076ZZ, DB1797Z, DB1798Z, DB1799Z, DB179BZ, DB179CZ, DB179YZ, DB17B6Z, DB17B7Z, DB17B8Z, DB17B9Z, DB17BB1, DB17BBZ, DB17BCZ, DB17BYZ, DB27DZZ, DB27HZZ, DB27JZZ, DBY77ZZ, DBY78ZZ, DBY7FZZ, DBY7KZZ, DF000ZZ, DF001ZZ, DF002ZZ, DF003Z0, DF003ZZ, DF004ZZ, DF005ZZ, DF006ZZ, DF1097Z, DF1098Z, DF1099Z, DF109BZ, DF109CZ, DF109YZ, DF10B6Z, DF10B7Z, DF10B8Z, DF10B9Z, DF10BB1, DF10BBZ, DF10BCZ, DF10BYZ, DF0DZZ, DF20HZZ, DF20JZZ, DFY07ZZ, DFY08ZZ, DFY0CZZ, DFY0FZZ, DFY0KZZ, DT000ZZ, DT001ZZ, DT002ZZ, DT003Z0, DT003ZZ, DT004ZZ, DT005ZZ, DT006ZZ, DT1097Z, DT1098Z, DT1099Z, DT109BZ, DT109CZ, DT109YZ, DT10B6Z, DT10B7Z, DT10B8Z, DT10B9Z, DT10BB1, DT10BBZ, DT10BCZ, DT10BYZ, DT20DZZ, DT20HZZ, DT20JZZ, DTY07ZZ, DTY08ZZ, DTY0CZZ, DTY0FZZ, DW020ZZ, DW021ZZ, DW022ZZ, DW023Z0, DW023ZZ, DW024ZZ, DW025ZZ, DW026ZZ, DW1297Z, DW1298Z, DW1299Z, DW129BZ, DW129CZ, DW129YZ, DW12B6Z, DW12B7Z, DW12B8Z, DW12B9Z, DW12BB1, DW12BBZ, DW12BCZ, DW12BYZ, DW22DZZ, DW22HZZ, DW22JZZ, DWY27ZZ, DWY28ZZ, DWY2FZZ, DW030ZZ, DW031ZZ, DW032ZZ, DW033Z0, DW033ZZ, DW034ZZ, DW035ZZ, DW036ZZ, DW1397Z, DW1398Z, DW1399Z, DW139BZ, DW139CZ, DW139YZ, DW13B6Z, DW13B7Z, DW13B8Z, DW13B9Z, DW13BB1, DW13BBZ, DW13BCZ, DB13BYZ, DW23DZZ, DW23HZZ, DW23JZZ, DWY37ZZ, DWY38ZZ, DWY3FZZ, DW050ZZ, DW051ZZ, DW052ZZ, DW053Z0, DW053ZZ, DW054ZZ, DW055ZZ, DW056ZZ, DWY57ZZ, DWY58ZZ, DWY5FZZ, DWY5GDZ, DWY5GFZ, DWY5GGZ, DWY5GHZ, DWY5GYZ.
* * * * *(ii) * * *
(A) The denominator is the total dialysis treatment beneficiary years for attributed ESRD Beneficiaries during the MY. Dialysis treatment beneficiary years included in the denominator are composed of those months during which an attributed ESRD Beneficiary received maintenance dialysis at home or in an ESRD facility, such that 1-beneficiary year is comprised of 12-beneficiary months. For MY1 and MY2, months during which an attributed ESRD Beneficiary received maintenance dialysis are identified by claims with Type of Bill 072X, excluding claims for beneficiaries who were 75 years of age or older at any point during the month. For MY3 through MY10, months during which an attributed ESRD Beneficiary received maintenance dialysis are identified by claims with Type of Bill 072X, excluding claims for beneficiaries who were 75 years of age or older at any point during the month, or had a vital solid organ cancer diagnosis and were receiving treatment with chemotherapy or radiation for vital solid organ cancer during the MY. Months in which an attributed ESRD Beneficiary had a diagnosis of vital solid organ cancer are identified as described in paragraph (c)(1)(i)(A)(1) of this section. Months in which an attributed ESRD Beneficiary received treatment with chemotherapy or radiation for vital solid organ cancer are identified as described in paragraph (c)(1)(i)(A)(2) of this section.
* * * * *(2) * * *
(i) * * *
(A) The denominator is the total dialysis treatment beneficiary years for attributed ESRD Beneficiaries during the MY. Dialysis treatment beneficiary years included in the denominator are composed of those months during which an attributed ESRD Beneficiary received maintenance dialysis at home or in an ESRD facility, such that 1-beneficiary year is comprised of 12-beneficiary months. For MY1 and MY2, months during which an attributed Start Printed Page 36434ESRD Beneficiary received maintenance dialysis are identified by claims with CPT codes 90957, 90958, 90959, 90960, 90961, 90962, 90965, or 90966, excluding claims for beneficiaries who were 75 years of age or older at any point during the month. For MY3 through MY10, months during which an attributed ESRD Beneficiary received maintenance dialysis are identified by claims with CPT codes 90957, 90958, 90959, 90960, 90961, 90962, 90965, or 90966, excluding claims for beneficiaries who were 75 years of age or older at any point during the month, or had a vital solid organ cancer diagnosis and were receiving treatment with chemotherapy or radiation for vital solid organ cancer during the MY. Months in which an attributed ESRD Beneficiary had a diagnosis of vital solid organ cancer are identified as described in paragraph (c)(1)(i)(A)(1) of this section. Months in which an attributed ESRD Beneficiary received treatment with chemotherapy or radiation for vital solid organ cancer are identified as described in paragraph (c)(1)(i)(A)(2) of this section.
* * * * *(ii) * * *
(A) * * *
(1) Dialysis treatment beneficiary years included in the denominator are composed of those months during which an attributed ESRD Beneficiary received maintenance dialysis at home or in an ESRD facility, such that 1-beneficiary year is comprised of 12-beneficiary months. For MY1 and MY2, months during which an attributed ESRD Beneficiary received maintenance dialysis are identified by claims with CPT codes 90957, 90958, 90959, 90960, 90961, 90962, 90965, or 90966, excluding claims for beneficiaries who were 75 years of age or older at any point during the month. For MY3 through MY10, months during which an attributed ESRD Beneficiary received maintenance dialysis are identified by claims with CPT codes 90957, 90958, 90959, 90960, 90961, 90962, 90965, or 90966, excluding claims for beneficiaries who were 75 years of age or older at any point during the month, or had a vital solid organ cancer diagnosis and were receiving treatment with chemotherapy or radiation for vital solid organ cancer during the MY. Months in which an attributed ESRD Beneficiary had a vital solid organ cancer diagnosis are identified as described in paragraph (c)(1)(i)(A)(1) of this section. Months in which an attributed ESRD Beneficiary received treatment with chemotherapy or radiation for vital solid organ cancer are identified as described in paragraph (c)(1)(i)(A)(2) of this section.
(2) MY1 and MY2, Pre-emptive LDT beneficiary years included in the denominator are composed of those months during which a Pre-emptive LDT Beneficiary is attributed to a Managing Clinician, from the beginning of the MY up to and including the month of the living donor transplant. For MY3 through MY10, Pre-emptive LDT beneficiary years included in the denominator are composed of those months during which a Pre-emptive LDT Beneficiary is attributed to a Managing Clinician, from the beginning of the MY up to and including the month of the living donor transplant, excluding beneficiaries who had a vital solid organ cancer diagnosis and were receiving treatment with chemotherapy or radiation for vital solid organ cancer during the MY. Months in which an attributed ESRD Beneficiary had a vital solid organ cancer diagnosis are identified as described in paragraph (c)(1)(i)(A)(1) of this section. Months in which an attributed ESRD Beneficiary received treatment with chemotherapy or radiation for vital solid organ cancer are identified as described in paragraph (c)(1)(i)(A)(2) of this section. Pre-emptive LDT Beneficiaries are identified using information about living donor transplants from the SRTR Database and Medicare claims data.
* * * * *9. Section 512.370 is amended by revising paragraphs (b), (c), and (d) to read as follows:
End Amendment PartStart Amendment PartBenchmarking and scoring.* * * * *(b) Achievement scoring. CMS assesses ETC Participant performance at the aggregation group level on the home dialysis rate and transplant rate against achievement benchmarks constructed based on the home dialysis rate and transplant rate among aggregation groups of ESRD facilities and Managing Clinicians located in Comparison Geographic Areas during the Benchmark Year. Achievement benchmarks are calculated as described in paragraph (b)(1) of this section and, for MY3 through MY10, are stratified as described in paragraph (b)(2) of this section.
(1) Achievement benchmarks. CMS uses the following scoring methodology to assess an ETC Participant's achievement score.
Table 1 to § 512.370(b)(1)—ETC Model Schedule of PPA Achievment Benchmarks by Measurement Year
MY1 and MY2 MY3 and MY4 MY5 and MY6 MY7 and MY8 MY9 and MY10 Points 90th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year 1.1 * (90th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 1.2 * (90th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 1.3 * (90th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 1.4 * (90th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 2 75th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year 1.1 * (75th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 1.2 * (75th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 1.3 * (75th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 1.4 * (75th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 1.5 50th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year 1.1 * (50th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 1.2 * (50th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 1.3 * (50th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 1.4 * (50th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 1 30th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year 1.1 * (30th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 1.2 * (30th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 1.3 * (30th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 1.4 * (30th+ Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 0.5 Start Printed Page 36435 <30th Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year 1.1 * (<30th Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 1.2 * (<30th Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 1.3 * (<30th Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 1.4 * (<30th Percentile of benchmark rates for Comparison Geographic Areas during the Benchmark Year) 0 (2) Stratifying achievement benchmarks. For MY3 through MY10, CMS stratifies achievement benchmarks based on the proportion of beneficiary years attributed to the aggregation group for which attributed beneficiaries are dual eligible or LIS recipients during the MY. An ESRD Beneficiary or Pre-emptive LDT Beneficiary is considered to be dual eligible or an LIS recipient for a given month if at any point during the month the beneficiary was dual eligible or an LIS recipient based on Medicare administrative data. CMS stratifies the achievement benchmarks into the following two strata:
(i) Stratum 1: 50 percent or more of attributed beneficiary years during the MY are for beneficiaries who are dual eligible or LIS recipients.
(ii) Stratum 2: Less than 50 percent of attributed beneficiary years during the MY are for beneficiaries who are dual eligible or LIS recipients.
(c) Improvement scoring. CMS assesses ETC Participant improvement on the home dialysis rate and transplant rate against benchmarks constructed based on the ETC Participant's aggregation group's historical performance on the home dialysis rate and transplant rate during the Benchmark Year to calculate the ETC Participant's improvement score, as specified in paragraph (c)(1) of this section. For MY3 through MY10, CMS assesses ETC Participant improvement on the home dialysis rate and transplant rate for ESRD Beneficiaries and, if applicable, Pre-emptive LDT Beneficiaries, who are dual eligible or LIS recipients to determine whether to add the Health Equity Incentive to the ETC Participant's improvement score, as specified in paragraph (c)(2) of this section.
(1) Improvement score calculation. CMS uses the following scoring methodology to assess an ETC Participant's improvement score.
(i) Greater than 10 percent improvement relative to the Benchmark Year rate: 1.5 points
(ii) Greater than 5 percent improvement relative to the Benchmark Year rate: 1 point
(iii) Greater than 0 percent improvement relative to the Benchmark Year rate: 0.5 points
(iv) Less than or equal to the Benchmark Year rate: 0 points
(v) For MY3 through MY10, when calculating improvement benchmarks constructed based on the ETC Participant's aggregation group's historical performance on the home dialysis rate and transplant rate during the Benchmark Year, CMS adds one beneficiary month to the numerator of the home dialysis rate and adds one beneficiary month to the numerator of the transplant rate, such that the Benchmark Year rates cannot be equal to zero.
(2) Health Equity Incentive. CMS calculates the ETC Participant's aggregation group's home dialysis rate and transplant rate as specified in §§ 512.365(b) and 512.365(c), respectively, using only attributed beneficiary years comprised of months during the MY in which ESRD Beneficiaries and, if applicable, Pre-emptive LDT Beneficiaries, are dual eligible or LIS recipients. CMS also calculates the threshold for earning the Health Equity Incentive based on the ETC Participant's aggregation group's historical performance on the home dialysis rate and transplant rate during the Benchmark Year, using only attributed beneficiary years comprised of months during the Benchmark Year in which ESRD Beneficiaries and, if applicable, Pre-emptive LDT Beneficiaries, are dual eligible or LIS recipients. An ESRD Beneficiary or Pre-emptive LDT Beneficiary is considered to be dual eligible or an LIS recipient for a given month if at any point during the month the beneficiary was dual eligible or an LIS recipient. CMS determines whether a beneficiary was dual eligible or an LIS recipient based on Medicare administrative data.
(i) The ETC Participant earns the Health Equity Incentive for the home dialysis rate improvement score if the home dialysis rate for the MY, calculated as specified in paragraph (c)(2) of this section, is at least 5-percentage points higher than the home dialysis rate for the Benchmark Year, calculated as specified in paragraph (c)(2) of this section. If the ETC Participant earns the Health Equity Incentive for the home dialysis rate improvement score, CMS adds 0.5 points to the ETC Participant's home dialysis rate improvement score, calculated as specified in paragraph (c)(1) of this section, unless the ETC Participant is ineligible to receive the Home Equity Incentive as specified in paragraph (c)(2)(iii) of this section.
(ii) The ETC Participant earns the Health Equity Incentive for the transplant rate improvement score if the home dialysis rate for the MY, calculated as specified in paragraph (c)(2) of this section, is at least 5-percentage points higher than the transplant rate for the Benchmark Year, calculated as specified in paragraph (c)(2) of this section. If the ETC Participant earns the Health Equity Incentive for the transplant rate improvement score, CMS adds 0.5 points to the ETC Participant's transplant rate improvement score, calculated as specified in paragraph (c)(1) of this section, unless the ETC Participant is ineligible to receive the Home Equity Incentive as specified in paragraph (c)(2)(iii) of this section.
(iii) An ETC Participant in an aggregation group with fewer than 11-attributed beneficiary years comprised of months in which ESRD Beneficiaries and, if applicable, Pre-emptive LDT Beneficiaries, are dual eligible or LIS recipients, during either the Benchmark Year or the MY is ineligible to earn the Health Equity Incentive.
(d) Modality Performance Score. (1) For MY1 and MY2, CMS calculates the ETC Participant's MPS as the higher of ETC Participant's achievement score or improvement score for the home dialysis rate, together with the higher of the ETC Participant's achievement score or improvement score for the transplant rate, weighted such that the ETC Participant's score for the home dialysis rate constitutes 2/3 of the MPS and the ETC Participant's score for the transplant rate constitutes 1/3 of the MPS.
CMS uses the following formula to calculate the ETC Participant's MPS for MY1 and MY2:
Modality Performance Score Start Printed Page 36436
= 2 × (Higher of the home dialysis achievement or improvement score)
+ (Higher of the transplant achievement or improvement score)
(2) For MY3 through MY10, CMS calculates the ETC Participant's MPS as the higher of the ETC Participant's achievement score for the home dialysis rate or the sum of the ETC Participant's improvement score for the home dialysis rate calculated as specified in paragraph (c)(1) of this section and, if applicable, the Health Equity Incentive, calculated as described in paragraph (c)(2)(i) of this section, together with the higher of the ETC Participant's achievement score for the transplant rate or the sum of the ETC Participant's improvement score for the transplant rate calculated as specified in paragraph (c)(1) of this section and, if applicable, the Heath Equity Incentive, calculated as described in paragraph (c)(2)(ii) of this section, weighted such that the ETC Participant's score for the home dialysis rate constitutes 2/3 of the MPS and the ETC Participant's score for the transplant rate constitutes 1/3 of the MPS.
CMS uses the following formula to calculate the ETC Participant's MPS for MY3 through MY10:
Modality Performance Score
= 2
× (Higher of the home dialysis achievement or (home dialysis improvement score + Health Equity Bonus †))
+ (Higher of the transplant achievement or (transplant improvement score
+ Health Equity Bonus †))
† The Health Equity Incentive is applied to the home dialysis improvement score or transplant improvement score only if earned by the ETC Participant.
10. Section 512.390 is amended by revising the section heading, redesignating paragraph (b) as (c) and adding new paragraph (b) to read as follows:
End Amendment PartStart Amendment PartNotification, data sharing, and targeted review.* * * * *(b) Data sharing with ETC Participants. CMS shares certain beneficiary-identifiable data as described in paragraph (b)(1) of this section and certain aggregate data as described in paragraph (b)(2) of this section with ETC Participants regarding their attributed beneficiaries and performance under the ETC Model.
(1) Beneficiary-identifiable data. CMS shares beneficiary-identifiable data with ETC Participants as follows:
(i) CMS will make available certain beneficiary-identifiable data for retrieval by ETC Participants no later than one month before the start of each PPA Period, in a form and manner specified by CMS. ETC Participants may retrieve this data at any point during the relevant PPA Period.
(ii) This beneficiary-identifiable data includes, when available, the following information for each PPA Period:
(A) The ETC Participant's attributed beneficiaries' names, Medicare Beneficiary Identifiers, dates of birth, dual eligible status, and LIS recipient status.
(B) Data regarding the ETC Participant's performance under the ETC Model, including, for each attributed beneficiary, as applicable: The number of months the beneficiary was attributed to the ETC Participant, home dialysis months, self-dialysis months, nocturnal in-center dialysis months, transplant waitlist months, and months following a living donor transplant.
(iii) CMS shares this beneficiary-identifiable data on the condition that the ETC Participants observe all relevant statutory and regulatory provisions regarding the appropriate use of data and the confidentiality and privacy of individually identifiable health information as would apply to a covered entity under the Health Insurance Portability and Accountability Act of 1996 (HIPAA) regulations, and comply with the terms of the data sharing agreement described in paragraph (b)(1)(iv) of this section.
(iv) Data sharing agreement. If an ETC Participant wishes to retrieve the beneficiary-identifiable data specified in paragraph (b)(1)(ii) of this section, the ETC Participant must complete and submit, on at least an annual basis, a signed data sharing agreement, to be provided in a form and manner specified by CMS, under which the ETC Participant agrees:
(A) To comply with the requirements for use and disclosure of this beneficiary-identifiable data that are imposed on covered entities by the HIPAA regulations and the requirements of the ETC Model set forth in this part.
(B) To comply with additional privacy, security, breach notification, and data retention requirements specified by CMS in the data sharing agreement.
(C) To contractually bind each downstream recipient of the beneficiary-identifable data that is a business associate of the ETC Participant or performs a similar function for the ETC Participant, to the same terms and conditions to which the ETC Participant is itself bound in its data sharing agreement with CMS as a condition of the downstream recipient's receipt of the beneficiary-identifiable data retrieved by the ETC Participant under the ETC Model.
(D) That if the ETC Participant misuses or discloses the beneficiary-identifiable data in a manner that violates any applicable statutory or regulatory requirements or that is otherwise non-compliant with the provisions of the data sharing agreement, the ETC Participant will no longer be eligible to retrieve beneficiary-identifiable data under paragraph (b)(1)(i) of this section and may be subject to additional sanctions and penalties available under the law.
(2) Aggregate data. CMS shares aggregate performance data with ETC Participants as follows:
(i) CMS will make available certain aggregate data for retrieval by the ETC Participant, in a form and manner to be specified by CMS, no later than one month before each PPA Period.
(ii) This aggregate data includes, when available, the following information for each PPA Period, de-identified in accordance with 45 CFR 164.514(b):
(A) The ETC Participant's performance scores on the home dialysis rate, transplant waitlist rate, living donor transplant rate, and the Health Equity Incentive.
(B) The ETC Participant's aggregation group's scores on the home dialysis rate, transplant waitlist rate, and living donor transplant rate, and the Health Equity Incentive.
(C) Information on how the ETC Participant's and ETC Participant's aggregation group's scores relate to the achievement benchmark and improvement benchmark.
(D) The ETC Participant's MPS and PPA for the corresponding PPA Period.
* * * * *11. Section 512.397 is amended by revising the section heading and paragraph (b) and adding paragraph (c) to read as follows:
End Amendment PartStart SignatureETC Model Medicare program waivers and additional flexibilities.* * * * *(b) CMS waives the following requirements of title XVIII of the Act solely for purposes of testing the ETC Model:
(1) CMS waives the requirement under section 1861(ggg)(2)(A)(i) of the Act and § 410.48(a) of this chapter that only doctors, physician assistants, nurse practitioners, and clinical nurse specialists can furnish kidney disease patient education services to allow kidney disease patient education Start Printed Page 36437services to be provided by clinical staff (as defined at § 512.310) under the direction of and incident to the services of the Managing Clinician who is an ETC Participant. The kidney disease patient education services may be furnished only by qualified staff (as defined at § 512.310).
(2) CMS waives the requirement that kidney disease patient education services are covered only for Stage IV chronic kidney disease (CKD) patients under section 1861(ggg)(1)(A) of the Act and § 410.48(b)(1) of this chapter to permit beneficiaries diagnosed with CKD Stage V or within the first 6 months of starting dialysis to receive kidney disease patient education services.
(3) CMS waives the requirement that the content of kidney disease patient education services include the management of co-morbidities, including for the purpose of delaying the need for dialysis, under § 410.48(d)(1) of this chapter when such services are furnished to beneficiaries with CKD Stage V or ESRD, unless such content is relevant for the beneficiary.
(4) CMS waives the requirement that an outcomes assessment designed to measure beneficiary knowledge about CKD and its treatment be performed as part of a kidney disease patient education service under § 410.48(d)(5)(iii) of this chapter, provided that such outcomes assessment is performed by qualified staff within one month of the final kidney disease patient education service.
(5) Beginning January 1, 2022, CMS waives the geographic and site of service originating site requirements in sections 1834(m)(4)(B) and 1834(m)(4)(C) of the Act and § 410.78(b)(3) and (4) of this chapter for purposes of kidney disease patient education services furnished by qualified staff via telehealth in accordance with this section, regardless of the location of the beneficiary or qualified staff. Beginning January 1, 2022, CMS also waives the requirement in section 1834(m)(2)(B) of the Act and § 414.65(b) of this chapter that CMS pay a facility fee to the originating site with respect to telehealth services furnished to a beneficiary in accordance with this section at an originating site that is not one of the locations specified in § 410.78(b)(3).
(c)(1) Beginning January 1, 2022, an ETC Participant may reduce or waive the 20 percent coinsurance requirement under section 1833 of the Act if all of the following conditions are satisfied:
(i) The individual or entity that furnished the kidney disease patient education services is qualified staff.
(ii) The kidney disease patient education services were furnished to a beneficiary described in § 410.48(b) or § 512.397(b)(2) who did not have secondary insurance on the date the services were furnished.
(iii) The kidney disease patient education services were furnished in compliance with the applicable provisions of § 410.48 and § 512.397(b).
(2) The ETC Participant must maintain and provide the government with access to records of the following information in accordance with § 512.135(b) and (c) of this part:
(i) The identity of the qualified staff who furnished the kidney disease patient education services for which the coinsurance was reduced or waived and the date such services were furnished.
(ii) The identity of the beneficiary who received the kidney disease patient education services for which the coinsurance was reduced or waived.
(iii) Evidence that the beneficiary who received the kidney disease patient education services coinsurance waiver was eligible to receive the kidney disease patient education services under the ETC Model and did not have secondary insurance.
(iv) The amount of the kidney disease patient education coinsurance reduction or waiver provided by the ETC Participant.
(3) The Federal anti-kickback statute safe harbor for CMS-sponsored model patient incentives (42 CFR 1001.952(ii)(2)) is available to protect the kidney disease patient education coinsurance waivers that satisfy the requirements of such safe harbor and paragraph (c)(1) of this section.
End Signature End Supplemental InformationXavier Becerra,
Secretary, Department of Health and Human Services.
Footnotes
1. We note that for the CY 2020 ESRD PPS final rule, we did not apply the statewide urban average to Carson City, Nevada because hospital data was available to compute the wage index.
Back to Citation2. Transmittal 2033 issued August 20, 2010, was rescinded and replaced by Transmittal 2094, dated November 17, 2010. Transmittal 2094 identified additional drugs and laboratory tests that may also be eligible for ESRD outlier payment. Transmittal 2094 was rescinded and replaced by Transmittal 2134, dated January 14, 2011, which included one technical correction.
Back to Citation3. Medicare Benefits Policy Manual (Pub. L. 100-102), available at: https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/bp102c11.pdf.
Back to Citation4. United States Renal Data System. 2020 USRDS Annual Data Report: Epidemiology of kidney disease in the United States, End-Stage Renal Disease Chapter 2. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2020. Available at: https://adr.usrds.org/2020/end-stage-renaldisease/introduction-to-volume-2. Accessed on Jan. 21, 2021.
Back to Citation5. Seshasai, R.K., et al. (2019). The home hemodialysis patient experience: A qualitative assessment of modality use and discontinuation. Hemodialysis International, 23: 139-150, 2019. doi:10.1111/hdi.12713.
6. Weinhandl, Eric D., Collins Allan, Incidence of Therapy Cessation among Home Hemodialysis Patients in the United States, Abstract presented, American Society of Nephrology Kidney Week 2016.
Back to Citation7. Seshasai, R.K., et al. (2019). The home hemodialysis patient experience: A qualitative assessment of modality use and discontinuation. Hemodialysis International, 23: 139-150, 2019. doi:10.1111/hdi.12713.
8. Chan, Christopher T. et al. (2018). Exploring Barriers and Potential Solutions in Home Dialysis: An NKF-KDOQI Conference Outcomes Report American Journal of Kidney Diseases, Volume 73, Issue 3, 363-371.
Back to Citation9. Erickson, K.F., Zheng, Y., Ho, V., Winkelmayer, W.C., Bhattacharya, J., & Chertow, G.M. (2018). Market Competition and Health Outcomes in Hemodialysis. Health services research, 53(5), 3680-3703. https://doi.org/10.1111/1475-6773.12835.
Back to Citation10. Blake, P.G., Quinn, R.R., & Oliver, M.J. (2013). Peritoneal dialysis and the process of modality selection. Peritoneal dialysis international: journal of the International Society for Peritoneal Dialysis, 33(3), 233-241. https://doi.org/10.3747/pdi.2012.00119.
Back to Citation11. Ibid.
Back to Citation12. Mukhopadhyay, P., Woodside, K.J., Schaubel, D.E., Repeck, K., McCullough, K., Shahinian, V.B., . . . & Saran, R. (2020). Survival among incident peritoneal dialysis versus hemodialysis patients who initiate with an arteriovenous fistula. Kidney Medicine, 2(6), 732-741.
Back to Citation13. United States Renal Data System. 2020 USRDS Annual Data Report: Epidemiology of kidney disease in the United States, End-Stage Renal Disease Chapter 2. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2020. Available at: https://adr.usrds.org/2020/end-stage-renaldisease/introduction-to-volume-2. Accessed on Jan 21, 2021.
Back to Citation14. Canada Institute for Health Information (2020): Annual Statistics. Available at: https://secure.cihi.ca/estore/productSeries.htm?locale=en&pc=PCC24&_ga=2.265337481.729263172.1612199530-510791291.1610562424. Accessed on Jan. 31, 2021.
Back to Citation15. Clinicaltrials.gov website. https://www.clinicaltrials.gov/ct2/show/NCT02460263. Last Updated July 1, 2020. https://www.clinicaltrials.gov/ProvidedDocs/63/NCT02460263/Prot_000.pdf.
Back to Citation16. Chertow, G.M., Alvarez, L., Plumb, T.J., Prichard, S.S., & Aragon, M. (2020). Patient-reported outcomes from the investigational device exemption study of the Tablo hemodialysis system. Hemodialysis International, 24(4), 480-486.
17. Leypoldt, J.K., Prichard, S., Chertow, G.M., & Alvarez, L. (2019). Differential molecular modeling predictions of mid and conventional dialysate flows. Blood purification, 47(4), 369-376.
18. Safety and efficacy of the Tablo hemodialysis system for in-center and home hemodialysis Plumb, T.J., Alvarez, L., Ross, D.L., Lee, J.J., Mulhern, J.G., Bell, J.L., Abra, G., Prichard, S.S., Chertow, G.M. and Aragon, M.A. (2019), Hemodialysis International.
19. Plumb, Troy J., Luis Alvarez, Dennis L. Ross, Joseph J. Lee, Jeffrey G. Mulhern, Jeffrey L. Bell, Graham E. Abra, Sarah S. Prichard, Glenn M. Chertow, and Michael A. Aragon. “Self-care training using the Tablo hemodialysis system.” Hemodialysis International (2020).
Back to Citation20. Alvarez, Luis et al. Urea Clearance Results in Patients Dialyzed Thrice Weekly Using a Dialysate Flow of 300 mL/min, clinical abstract, presented March 2019, Annual Dialysis Conference, Dallas, TX.
21. Chahal, Y., Plumb, T., Aragon M. (2020). Patient Device Preference for Home Hemodialysis: A Subset Analysis of the Tablo Home IDE Trial. Poster Presentation at National Kidney Foundation Spring Clinical Conference, March 2020.
Back to Citation22. Kraus, M., et al., A comparison of center-based vs. home-based daily hemodialysis for patients with end-stage renal disease. Hemodialysis International, 11: 468-477, (2007).
23. Finkelstein, F.O., et al. (2012). At-home short daily hemodialysis improves the long-term health-related quality of life. Kidney international, 82(5), 561-569.
24. Weinhandl, E.D., Gilbertson, D.T., & Collins, A.J. (2016). Mortality, hospitalization, and technique failure in daily home hemodialysis and matched peritoneal dialysis patients: A matched cohort study. American Journal of Kidney Diseases, 67(1), 98-110.
Back to Citation25. Suri, R.S., Li, L., & Nesrallah, G.E. (2015). The risk of hospitalization and modality failure with home dialysis. Kidney international, 88(2), 360-368.
Back to Citation26. Clinicaltrials.gov website. https://www.clinicaltrials.gov/ct2/show/NCT02460263. Last Updated July 1, 2020. https://www.clinicaltrials.gov/ProvidedDocs/63/NCT02460263/Prot_000.pdf.
Back to Citation27. Alvarez, Luis et al. Urea Clearance Results in Patients Dialyzed Thrice Weekly Using a Dialysate Flow of 300 mL/min, clinical abstract, presented March 2019, Annual Dialysis Conference, Dallas, TX.
Back to Citation28. Chertow, G.M., Alvarez, L., Plumb, T.J., Prichard, S.S., & Aragon, M. (2020). Patient-reported outcomes from the investigational device exemption study of the Tablo hemodialysis system. Hemodialysis International, 24(4), 480-486.
Back to Citation29. Leypoldt, J.K., Prichard, S., Chertow, G.M., & Alvarez, L. (2019). Differential molecular modeling predictions of mid and conventional dialysate flows. Blood purification, 47(4), 369-376.
Back to Citation30. Safety and efficacy of the Tablo hemodialysis system for in-center and home hemodialysis Plumb, T.J., Alvarez, L., Ross, D.L., Lee, J.J., Mulhern, J.G., Bell, J.L., Abra, G., Prichard, S.S., Chertow, G.M. and Aragon, M.A. (2019), Hemodialysis International.
Back to Citation31. Plumb, Troy J., Luis Alvarez, Dennis L. Ross, Joseph J. Lee, Jeffrey G. Mulhern, Jeffrey L. Bell, Graham E. Abra, Sarah S. Prichard, Glenn M. Chertow, and Michael A. Aragon. “Self-care training using the Tablo hemodialysis system.” Hemodialysis International (2020).
Back to Citation32. Chahal, Y., Plumb, T., Aragon M. (2020). Patient Device Preference for Home Hemodialysis: A Subset Analysis of the Tablo Home IDE Trial. Poster Presentation at National Kidney Foundation Spring Clinical Conference, March 2020.
Back to Citation33. Kraus, M., et al., A comparison of center-based vs. home-based daily hemodialysis for patients with end-stage renal disease. Hemodialysis International, 11: 468-477, (2007).
Back to Citation34. Finkelstein, F.O., et al. (2012). At-home short daily hemodialysis improves the long-term health-related quality of life. Kidney International, 82(5), 561-569.
Back to Citation35. Weinhandl, E.D., Gilbertson, D.T., & Collins, A.J. (2016). Mortality, hospitalization, and technique failure in daily home hemodialysis and matched peritoneal dialysis patients: A matched cohort study. American Journal of Kidney Diseases, 67(1), 98-110.
Back to Citation36. Suri, R.S., Li, L., & Nesrallah, G.E. (2015). The risk of hospitalization and modality failure with home dialysis. Kidney International, 88(2), 360-368.
Back to Citation37. Alvarez, Luis et al. Urea Clearance Results in Patients Dialyzed Thrice Weekly Using a Dialysate Flow of 300 mL/min, clinical abstract, presented March 2019, Annual Dialysis Conference, Dallas, TX.
Back to Citation38. Plumb, T.J., Alvarez, L., Ross, D.L., Lee, J.J., Mulhern, J.G., Bell, J.L., Abra, G., Prichard, S.S., Chertow, G.M. and Aragon, M.A. (2019). Safety and efficacy of the Tablo hemodialysis system for in-center and home hemodialysis. Hemodialysis International.
Back to Citation39. NxStage Clearance Calculator. Available at: https://dosingcalculator.nxstage.com/DosingCalculator/. Accessed on Jan 21, 2021.
Back to Citation40. Tentori F, Zhang J, Li Y, Karaboyas A, Kerr P, Saran R, Bommer J, Port F, Akiba T, Pisoni R, Robinson B. Longer dialysis session length is associated with better intermediate outcomes and survival among patients on in-center three times per week hemodialysis: results from the Dialysis Outcomes and Practice Patterns Study (DOPPS). Nephrol Dial Transplant. 2012 Nov;27(11):4180-8. doi: 10.1093/ndt/gfs021. Epub 2012 Mar 19. PMID: 22431708; PMCID: PMC3529546.
Back to Citation41. Health Management Associates (HMA) analysis of 2018 100% Medicare Outpatient file.
Back to Citation42. Leypoldt, J.K., Prichard, S., Chertow, G.M., & Alvarez, L. (2019). Differential molecular modeling predictions of mid and conventional dialysate flows. Blood Purification, 47(4), 369-376.
Back to Citation43. Ibid.
Back to Citation44. Ibid.
Back to Citation45. Leypoldt, J.K., Prichard, S., Chertow, G.M., & Alvarez, L. (2019). Differential molecular modeling predictions of mid and conventional dialysate flows. Blood Purification, 47(4), 369-376.
46. Daugirdas JT, Greene T, Depner TA, Chumela C, Rocco, MJ, Chertow, GM for the Hemodialysis (HEMO) Study Group. Anthropometrically Estimated Total Body Water Volumes are Larger than Modeled Urea Volume in Chronic Hemodialysis Patients: Effects of Age, Race and Gender. 2003. Kidney Int. 64:1108-1119.
Back to Citation47. United States Renal Data System. 2020 USRDS Annual Data Report: Epidemiology of kidney disease in the United States, End-Stage Renal Disease Chapter 2. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2020. Available at: https://adr.usrds.org/2020/end-stage-renaldisease/introduction-to-volume-2. Accessed on Jan 21, 2021.
Back to Citation48. Wilk, A.S., Hirth, R.A., Zhang, W., Wheeler, J.R., Turenne, M.N., Nahra, T.A., . . . & Messana, J.M. (2018). Persistent variation in Medicare payment authorization for home hemodialysis treatments. Health services research, 53(2), 649-670.
Back to Citation49. Health Management Associates (HMA) analysis of 2018 100 percent Medicare Outpatient file.
Back to Citation50. Medicare Coverage Database. Retrieved May 24, 2021 from: https://www.cms.gov/medicare-coverage-database/details/lcd-details.aspx?LCDId=35014&ver=39&NCDId=79&ncdver=1&SearchType=Advanced&CoverageSelection=Both&NCSelection=NCA%7CCAL%7CNCD%7CMEDCAC%7CTA%7CMCD&ArticleType=Ed%7CKey%7CSAD%7CFAQ&PolicyType=Final&s=-%7C5%7C6%7C66%7C67%7C9%7C38%7C63%7C41%7C64%7C65%7C44&KeyWord=transplant&KeyWordLookUp=Doc&KeyWordSearchType=Exact&kq=true&bc=IAAAADgAAAAA&.
Back to Citation51. National Kidney Foundation. KDOQI clinical practice guideline for hemodialysis adequacy: 2015 update. Am J Kidney Dis. 2015;66(5):884-930.
52. Shafi T, Wilson RF, Greer R, Zhang A, Sozio S, Tan M, Bass EB. End-stage Renal Disease in the Medicare Population: Frequency and Duration of Hemodialysis and Quality of Life Assessment. Technology Assessment Program Project ID No. JHE51000. (Prepared by the Johns Hopkins University Evidence-based Practice Center under contract number HHSA 290-2015-00006I) Rockville, MD: Agency for Healthcare Research and Quality. July 2020. Available at: http://www.ahrq.gov/research/findings/ta/index.html.
Back to Citation53. Safety and efficacy of the Tablo hemodialysis system for in-center and home hemodialysis Plumb, T.J., Alvarez, L., Ross, D.L., Lee, J.J., Mulhern, J.G., Bell, J.L., Abra, G., Prichard, S.S., Chertow, G.M. and Aragon, M.A. (2019), Hemodialysis International.
Back to Citation54. FHN Trial Group. (2010). In-center hemodialysis six times per week versus three times per week. New England Journal of Medicine, 363(24), 2287-2300.
55. Kuo, T.H., Tseng, C.T., Lin, W.H., Chao, J.Y., Wang, W.M., Li, C.Y., & Wang, M.C. (2015). Association Between Vascular Access Dysfunction and Subsequent Major Adverse Cardiovascular Events in Patients on Hemodialysis: A Population-Based Nested Case-Control Study. Medicine, 94(26).
Back to Citation56. United States Renal Data System. 2020 USRDS Annual Data Report: Epidemiology of kidney disease in the United States, End-Stage Renal Disease Chapter 2. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2020. Available at: https://adr.usrds.org/2020/end-stage-renaldisease/introduction-to-volume-2. Reference Table G2.
Back to Citation57. Weinhandl, E.D., Gilbertson, D.T., & Collins, A.J. (2016). Mortality, hospitalization, and technique failure in daily home hemodialysis and matched peritoneal dialysis patients: A matched cohort study. American Journal of Kidney Diseases, 67(1), 98-110.
Back to Citation58. Suri, R.S., Li, L., & Nesrallah, G.E. (2015). The risk of hospitalization and modality failure with home dialysis. Kidney international, 88(2), 360-368.
Back to Citation59. Chan, K.E., Thadhani, R.I., & Maddux, F.W. (2014). Adherence barriers to chronic dialysis in the United States. Journal of the American Society of Nephrology, 25(11), 2642-2648. Supporting evidence of association between decreased dialysis adherence and poor patient health and utilization outcomes.
Back to Citation60. Weinhandl, Eric D., Collins Allan, Incidence of Therapy Cessation among Home Hemodialysis Patients in the United States, Abstract presented, American Society of Nephrology Kidney Week 2016.
Back to Citation61. Safety and efficacy of the Tablo hemodialysis system for in-center and home hemodialysis Plumb, T.J., Alvarez, L., Ross, D.L., Lee, J.J., Mulhern, J.G., Bell, J.L., Abra, G., Prichard, S.S., Chertow, G.M. and Aragon, M.A. (2019), Hemodialysis International.
Back to Citation62. Kraus, M., et al., A comparison of center-based vs. home-based daily hemodialysis for patients with end-stage renal disease. Hemodialysis International,11: 468-477, (2007). The authors performed a feasibility study to demonstrate the safety of center-based vs. home-based daily hemodialysis with the NxStage System One portable hemodialysis device.
Back to Citation63. Weinhandl, Eric D., Collins Allan, Incidence of Therapy Cessation among Home Hemodialysis Patients in the United States, Abstract presented, American Society of Nephrology Kidney Week 2016.
Back to Citation64. Safety and efficacy of the Tablo hemodialysis system for in-center and home hemodialysis Plumb, T.J., Alvarez, L., Ross, D.L., Lee, J.J., Mulhern, J.G., Bell, J.L., Abra, G., Prichard, S.S., Chertow, G.M. and Aragon, M.A. (2019), Hemodialysis International.
Back to Citation65. Kraus M, Burkart J, Hegeman R, Solomon R, Coplon N, Moran J. A comparison of center-based vs. home-based daily hemodialysis for patients with end-stage renal disease. Hemodial Int. 2007 Oct;11(4):468-77. doi: 10.1111/j.1542-4758.2007.00229.x. PMID: 17922746.
Back to Citation66. Plumb, Troy J., Luis Alvarez, Dennis L. Ross, Joseph J. Lee, Jeffrey G. Mulhern, Jeffrey L. Bell, Graham E. Abra, Sarah S. Prichard, Glenn M. Chertow, and Michael A. Aragon. “Self-care training using the Tablo hemodialysis system.” Hemodialysis International (2020).
Back to Citation67. Kraus, M., et al., A comparison of center-based vs. home-based daily hemodialysis for patients with end-stage renal disease. Hemodialysis International,11: 468-477, (2007).
Back to Citation68. Seshasai, R.K., et al. (2019) The home hemodialysis patient experience: A qualitative assessment of modality use and discontinuation. Hemodialysis International, 23: 139-150 (2019).
Back to Citation69. Suri, R.S., Larive, B., Hall, Y., Kimmel, P.L., Kliger, A.S., Levin, N., . . . & Frequent Hemodialysis Network (FHN) Trial Group. (2014). Effects of frequent hemodialysis on perceived caregiver burden in the Frequent Hemodialysis Network trials. Clinical Journal of the American Society of Nephrology, 9(5), 936-942.
70. Jacquet, S., & Trinh, E. (2019). The potential burden of home dialysis on patients and caregivers: A narrative review. Canadian journal of kidney health and disease, 6, 2054358119893335.
Back to Citation71. Plumb, Troy J., Luis Alvarez, Dennis L. Ross, Joseph J. Lee, Jeffrey G. Mulhern, Jeffrey L. Bell, Graham E. Abra, Sarah S. Prichard, Glenn M. Chertow, and Michael A. Aragon. “Self-care training using the Tablo hemodialysis system.” Hemodialysis International (2020).
Back to Citation72. Ibid.
Back to Citation73. Chochinov, H.M., Kristjanson, L.J., Hack, T.F., Hassard, T., McClement, S., & Harlos, M. (2007). Burden to others and the terminally ill. Journal of pain and symptom management, 34(5), 463-471.
Back to Citation74. Chertow, G.M., Alvarez, L., Plumb, T.J., Prichard, S.S., & Aragon, M. (2020). Patient-reported outcomes from the investigational device exemption study of the Tablo hemodialysis system. Hemodialysis International, 24(4), 480-486.
Back to Citation75. Gabbay, E., Meyer, K.B., Griffith, J.L., Richardson, M.M., & Miskulin, D.C. (2010). Temporal trends in healthrelated quality of life among hemodialysis patients in the United States. Clinical journal of the American Society of Nephrology, 5(2), 261-267.
Back to Citation76. Yang, F., Wong, C.K., Luo, N., Piercy, J., Moon, R., & Jackson, J. (2019). Mapping the kidney disease quality of life 36-item short form survey (KDQOL-36) to the EQ-5D-3L and the EQ-5D-5L in patients undergoing dialysis. The European Journal of Health Economics, 20(8), 1195-1206.
Back to Citation77. Finkelstein, F.O., et al. (2012). At-home short daily hemodialysis improves the long-term health-related quality of life. Kidney international, 82(5), 561-569.
Back to Citation78. Liem, Y.S., Bosch, J.L., & Hunink, M.M. (2008). Preference-based quality of life of patients on renal replacement therapy: A systematic review and meta-analysis. Value in Health, 11(4), 733-741.
Back to Citation79. Chertow, G.M., Alvarez, L., Plumb, T.J., Prichard, S.S., & Aragon, M. (2020). Patient-reported outcomes from the investigational device exemption study of the Tablo hemodialysis system. Hemodialysis International, 24(4), 480-486.
Back to Citation80. Davison SN, Levin A, Moss AH, Jha V, Brown EA, Brennan F, Murtagh FE, Naicker S, Germain MJ, O'Donoghue DJ, Morton RL, Obrador GT; Kidney Disease: Improving Global Outcomes. Executive summary of the KDIGO Controversies Conference on Supportive Care in Chronic Kidney Disease: Developing a roadmap to improving quality care. Kidney Int. 2015 Sep;88(3):447-59.
Back to Citation81. Urquhart-Secord, Rachel et al. (2016). Patient and Caregiver Priorities for Outcomes in Hemodialysis: An International Nominal Group Technique Study American Journal of Kidney Diseases, Volume 68, Issue 3, 444-454.
Back to Citation82. Morin, C.M., Belleville, G., Bélanger, L., & Ivers, H. (2011). The Insomnia Severity Index: Psychometric indicators to detect insomnia cases and evaluate treatment response. Sleep, 34(5), 601-608.
83. Natale, V., Fabbri, M., Tonetti, L., & Martoni, M. (2014). Psychometric goodness of the mini sleep questionnaire. Psychiatry and clinical neurosciences, 68(7), 568-573.
Back to Citation84. Chertow, G.M., Alvarez, L., Plumb, T.J., Prichard, S.S., & Aragon, M. (2020). Patient-reported outcomes from the investigational device exemption study of the Tablo hemodialysis system. Hemodialysis International, 24(4), 480-486.
Back to Citation85. Urquhart-Secord, Rachel et al. (2016). Patient and Caregiver Priorities for Outcomes in Hemodialysis: An International Nominal Group Technique Study American Journal of Kidney Diseases, Volume 68, Issue 3, 444-454.
Back to Citation86. Liem, Y.S., Bosch, J.L., Arends, L.R., Heijenbrok-Kal, M.H., & Hunink, M.M. (2007). Quality of life assessed with the Medical Outcomes Study Short Form 36-Item Health Survey of patients on renal replacement therapy: A systematic review and meta-analysis. Value in Health, 10(5), 390-397.
Back to Citation87. Lowrie, E.G., Curtin, R.B., LePain, N., & Schatell, D. (2003). Medical outcomes study short form-36: A consistent and powerful predictor of morbidity and mortality in dialysis patients. American Journal of Kidney Diseases, 41(6), 1286-1292.
Back to Citation88. Food and Drug Administration Center for Devices and Radiological Health (2020). “Patient Preference-Sensitive Areas: Using Patient Preference Information in Medical Device Evaluation” Available at: https://www.fda.gov/about-fda/cdrh-patient-engagement/patient-preference-sensitive-areas-using-patientpreference-information-medical-device-evaluation. Accessed Jan 21, 2021.
Back to Citation89. Chahal, Y., Plumb, T., Aragon M. (2020). Patient Device Preference for Home Hemodialysis: A Subset Analysis of the Tablo Home IDE Trial. Poster Presentation at National Kidney Foundation Spring Clinical Conference, March 2020.
Back to Citation90. Alvarez, Luis et al. Urea Clearance Results in Patients Dialyzed Thrice Weekly Using a Dialysate Flow of 300 mL/min, clinical abstract, presented March 2019, Annual Dialysis Conference, Dallas, Texas.
Back to Citation91. Safety and efficacy of the Tablo hemodialysis system for in-center and home hemodialysis Plumb, T.J., Alvarez, L., Ross, D.L., Lee, J.J., Mulhern, J.G., Bell, J.L., Abra, G., Prichard, S.S., Chertow, G.M. and Aragon, M.A. (2019), Hemodialysis International.
92. Chertow, G.M., Alvarez, L., Plumb, T.J., Prichard, S. S., & Aragon, M. (2020). Patient-reported outcomes from the investigational device exemption study of the Tablo hemodialysis system. Hemodialysis International, 24(4), 480-486.
Back to Citation93. Mayo Clinic Staff, “Peritonitis,” June 18, 2020, available at: https://www.mayoclinic.org/diseases-conditions/peritonitis/symptoms-causes/syc-20376247.
Back to Citation94. Ibid.
Back to Citation95. Ibid.
Back to Citation96. Kam-Tao Li, Philip, et al., “ISPD Peritonitis recommendations: 2016 Update on Prevention and Treatment,” Peritoneal Dialysis International 2016; 36(5):481-508, June 9, 2016, available at: http://dx.doi.org/10.3747/pdi.2016.00078.
Back to Citation97. Briggs, et al., “Early Detection of Peritonitis in Patients Undergoing Peritoneal Dialysis: A Device and Cloud-Based Algorithmic Solution,” unpublished report.
Back to Citation98. Kam-Tao Li, Philip, et al., “ISPD Peritonitis recommendations: 2016 Update on Prevention and Treatment,” Peritoneal Dialysis International 2016; 36(5):481-508, June 9, 2016, available at: http://dx.doi.org/10.3747/pdi.2016.00078.
Back to Citation99. Ibid.
Back to Citation100. Briggs, et al., “Early Detection of Peritonitis in Patients Undergoing Peritoneal Dialysis: A Device and Cloud-Based Algorithmic Solution,” unpublished report.
Back to Citation101. Kam-Tao Li, Philip, et al., “ISPD Peritonitis recommendations: 2016 Update on Prevention and Treatment,” Peritoneal Dialysis International 2016; 36(5):481-508, June 9, 2016, available at: http://dx.doi.org/10.3747/pdi.2016.00078.
Back to Citation102. CloudCath, “A Prospective Clinical Study to Evaluate the Ability of the CloudCath System to Detect Peritonitis Compared to Standard of Care during In-Home Peritoneal Dialysis (CATCH),” Preliminary Clinical Study Report (NCT04515498), Jan 27, 2020.
Back to Citation103. CloudCath, “A Prospective Clinical Study to Evaluate the Ability of the CloudCath System to Detect Peritonitis Compared to Standard of Care during In-Home Peritoneal Dialysis (CATCH),” Study Protocol (CC-P-001), June 24, 2020.
Back to Citation104. Ibid.
Back to Citation105. Ibid.
Back to Citation106. CloudCath, “A Prospective Clinical Study to Evaluate the Ability of the CloudCath System to Detect Peritonitis Compared to Standard of Care during In-Home Peritoneal Dialysis (CATCH),” Preliminary Clinical Study Report (NCT04515498), Jan 27, 2020.
Back to Citation107. Ibid.
Back to Citation108. Ibid.
Back to Citation109. Ibid.
Back to Citation110. Ibid.
Back to Citation111. Ibid.
Back to Citation112. Ibid.
Back to Citation113. Ibid.
Back to Citation114. Muthucumarana, et al., “The Relationship Between Presentation and the Time of Initial Administration of Antibiotics With Outcomes of Peritonitis in Peritoneal Dialysis Patients: The PROMPT Study.,” Kidney Int Rep. 2016 Jun 11;1(2):65-72. doi: 10.1016/j.ekir.2016.05.003. PMID: 29142915; PMCID: PMC5678844.
Back to Citation115. Ibid.
Back to Citation116. Ibid.
Back to Citation117. Ibid.
Back to Citation118. Ibid.
Back to Citation119. Gacouin, A. et al., “Severe pneumonia due to Legionella pneumophila: prognostic factors, impact of delayed appropriate antimicrobial therapy,” Intensive Care Medicine 28, 686-691 (2002), https://doi.org/10.1007/s00134-002-1304-8.
120. Houck, PM. et al., “Timing of antibiotic administration and outcomes for Medicare patients hospitalized with community-acquired pneumonia,” Arch Intern Med. 2004 Mar 22;164(6):637-44. doi: 10.1001/archinte.164.6.637. PMID: 15037492.
121. Lodise TP, et al., “Outcomes analysis of delayed antibiotic treatment for hospital-acquired Staphylococcus aureus bacteremia,”Clin Infect Dis. 2003 Jun 1;36(11):1418-23. doi: 10.1086/375057. Epub 2003 May 20. PMID: 12766837.
Back to Citation122. Mehrotra, Rajnish et al., “The Current State of Peritoneal Dialysis,” Journal of the American Society of Nephrology 27: 3238-3252, 2016. doi: 10.1681/ASN.2016010112, available at: https://jasn.asnjournals.org/content/jnephrol/27/11/3238.full.pdf?with-ds=yes.
Back to Citation123. CloudCath, “A Prospective Clinical Study to Evaluate the Ability of the CloudCath System to Detect Peritonitis Compared to Standard of Care during In-Home Peritoneal Dialysis (CATCH),” Preliminary Clinical Study Report, NCT04515498, Jan 27, 2020.
Back to Citation124. Briggs, et al., “Early Detection of Peritonitis in Patients Undergoing Peritoneal Dialysis: A Device and Cloud-Based Algorithmic Solution,” unpublished report.
Back to Citation125. Muthucumarana, et al., “The Relationship Between Presentation and the Time of Initial Administration of Antibiotics With Outcomes of Peritonitis in Peritoneal Dialysis Patients: The PROMPT Study.,” Kidney Int Rep. 2016 Jun 11;1(2):65-72. doi: 10.1016/j.ekir.2016.05.003. PMID: 29142915; PMCID: PMC5678844.
Back to Citation126. Kam-Tao Li, Philip, et al., “ISPD Peritonitis recommendations: 2016 Update on Prevention and Treatment,” Peritoneal Dialysis International 2016; 36(5):481-508, June 9, 2016, available at: http://dx.doi.org/10.3747/pdi.2016.00078.
Back to Citation127. CloudCath, “A Prospective Clinical Study to Evaluate the Ability of the CloudCath System to Detect Peritonitis Compared to Standard of Care during In-Home Peritoneal Dialysis (CATCH),” Preliminary Clinical Study Report (NCT04515498), Jan 27, 2020.
Back to Citation128. Ibid.
Back to Citation129. Kam-Tao Li, Philip, et al., “ISPD Peritonitis recommendations: 2016 Update on Prevention and Treatment,” Peritoneal Dialysis International 2016; 36(5):481-508, June 9, 2016, available at: http://dx.doi.org/10.3747/pdi.2016.00078.
Back to Citation130. Ibid.
Back to Citation131. Briggs, et al., “Early Detection of Peritonitis in Patients Undergoing Peritoneal Dialysis: A Device and Cloud-Based Algorithmic Solution,” unpublished report.
Back to Citation132. CMS Provider Reimbursement Manual, Chapter 1, Section 104.1. Available at: https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Paper-Based-Manuals-Items/CMS021929.
Back to Citation133. Section 1881(b)(14)(D)(iv)(II) of the Act.
Back to Citation134. CMS, Press Release, CMS Announces Relief for Clinicians, Providers, Hospitals and Facilities Participating in Quality Reporting Programs in Response to COVID-19 (Mar. 22, 2020), https://www.cms.gov/newsroom/press-releases/cms-announces-relief-clinicians-providers-hospitals-and-facilities-participating-quality-reporting.
Back to Citation135. CMS, Exceptions and Extensions for Quality Reporting Requirements for Acute Care Hospitals, PPS-Exempt Cancer Hospitals, Inpatient Psychiatric Facilities, Skilled Nursing Facilities, Home Health Agencies, Hospices, Inpatient Rehabilitation Facilities, Long-Term Care Hospitals, Ambulatory Surgical Centers, Renal Dialysis Facilities, and MIPS Eligible Clinicians Affected by COVID-19 (Mar. 27, 2020), https://www.cms.gov/files/document/guidance-memo-exceptions-and-extensions-quality-reporting-and-value-based-purchasing-programs.pdf.
Back to Citation138. https://www.cms.gov/files/document/cy-2021-final-technical-specifications-20201130.pdf.
Back to Citation139. Groupings of questions and composite measures can be found at https://ichcahps.org/Portals/0/ICH_Composites_English.pdf.
Back to Citation141. United States Renal Data System. 2018 United States Renal Data System annual data report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD 2018.
Back to Citation142. Ibid.
Back to Citation143. Office of the Assistant Secretary for Planning and Evaluation, U.S. Department of Health & Human Services. Advancing American Kidney Health. 2019. Available at: https://aspe.hhs.gov/system/files/pdf/262046/AdvancingAmericanKidneyHealth.pdf.
Back to Citation144. National Quality Forum. List of Measures Under Consideration for December 21, 2020. Accessed at: https://www.cms.gov/files/document/measures-under-consideration-list-2020-report.pdf on January 29 2021.
Back to Citation145. Measure Applications Partnership. Measure Applications Partnership Preliminary Recommendations 2020-2021. Accessed on January 24, 2021 at: http://www.qualityforum.org/Project_Pages/MAP_Hospital_Workgroup.aspx.
Back to Citation146. Measure Applications Partnership. Measure Applications Partnership 2020-2021: Considerations for Implementing Measures in Federal Programs: Clinician, Hospital & PAC/LTC. Accessed on April 28, 2021 at: https://www.qualityforum.org/WorkArea/linkit.aspx?LinkIdentifier=id&ItemID=94893.
Back to Citation147. We note that for most ESRD QIP measures, this partial year data would be measure data from July and August 2020.
Back to Citation148. United States Department of Health and Human Services. “Healthy People 2020: Disparities. 2014.” Available at: https://www.healthypeople.gov/2020/about/foundation-health-measures/Disparities.
Back to Citation149. Joynt KE, Orav E., Jha AK. Thirty-Day Readmission Rates for Medicare Beneficiaries by Race and Site of Care. JAMA. 2011;305(7):675-681.
150. Lindenauer PK, Lagu T., Rothberg MB, et al. Income Inequality and 30 Day Outcomes After Acute Myocardial Infarction, Heart Failure, and Pneumonia: Retrospective Cohort Study. British Medical Journal. 2013;346.
151. Trivedi AN, Nsa W., Hausmann LRM, et al. Quality and Equity of Care in U.S. Hospitals. New England Journal of Medicine. 2014;371(24):2298-2308.
152. Polyakova, M., et al. Racial Disparities In Excess All-Cause Mortality During The Early COVID-19 Pandemic Varied Substantially Across States. Health Affairs. 2021; 40(2): 307-316.
153. Rural Health Research Gateway. Rural Communities: Age, Income, and Health Status. Rural Health Research Recap. November 2018.
154. Polyakova, M., et al. Racial Disparities In Excess All-Cause Mortality During The Early COVID-19 Pandemic Varied Substantially Across States. Health Affairs. 2021; 40(2): 307-316.
155. www.cdc.gov/mmwr/volumes/70/wr/mm7005a1.htm.
156. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7386532/.
Back to Citation157. Martino, SC, Elliott, MN, Dembosky, JW, Hambarsoomian, K., Burkhart, Q., Klein, DJ, Gildner, J., and Haviland, AM. Racial, Ethnic, and Gender Disparities in Health Care in Medicare Advantage. Baltimore, MD: CMS Office of Minority Health. 2020.
158. Guide to Reducing Disparities in Readmissions. CMS Office of Minority Health. Revised August 2018. Available at: https://www.cms.gov/About-CMS/Agency-Information/OMH/Downloads/OMH_Readmissions_Guide.pdf.
159. Singh JA, Lu X., Rosenthal GE, Ibrahim S., Cram P. Racial disparities in knee and hip total joint arthroplasty: An 18-year analysis of national Medicare data. Ann Rheum Dis. 2014 Dec;73(12):2107-15.
160. Rivera-Hernandez M., Rahman M., Mor V., Trivedi AN. Racial Disparities in Readmission Rates among Patients Discharged to Skilled Nursing Facilities. J Am Geriatr Soc. 2019 Aug;67(8):1672-1679.
161. Joynt KE, Orav E., Jha AK. Thirty-Day Readmission Rates for Medicare Beneficiaries by Race and Site of Care. JAMA. 2011;305(7):675-681.
162. Tsai TC, Orav EJ, Joynt KE. Disparities in surgical 30-day readmission rates for Medicare beneficiaries by race and site of care. Ann Surg. Jun 2014;259(6):1086-1090.
Back to Citation163. Rodriguez F., Joynt KE, Lopez L., Saldana F., Jha AK. Readmission rates for Hispanic Medicare beneficiaries with heart failure and acute myocardial infarction. Am Heart J. Aug 2011;162(2):254-261 e253.
164. Centers for Medicare and Medicaid Services. Medicare Hospital Quality Chartbook: Performance Report on Outcome Measures; 2014.
165. Guide to Reducing Disparities in Readmissions. CMS Office of Minority Health. Revised August 2018. Available at: https://www.cms.gov/About-CMS/Agency-Information/OMH/Downloads/OMH_Readmissions_Guide.pdf.
166. Prieto-Centurion V., Gussin HA, Rolle AJ, Krishnan JA. Chronic obstructive pulmonary disease readmissions at minority-serving institutions. Ann Am Thorac Soc. Dec 2013;10(6):680-684.
167. Joynt KE, Orav E., Jha AK. Thirty-Day Readmission Rates for Medicare Beneficiaries by Race and Site of Care. JAMA. 2011;305(7):675-681.
Back to Citation168. https://www.cms.gov/About-CMS/Agency-Information/OMH/Downloads/ESRD-Infographic.pdf.
Back to Citation169. Ibid.
Back to Citation170. HHS. Heart disease and African Americans. (March 29, 2021). https://www.minorityhealth.hhs.gov/omh/browse.aspx?lvl=4&lvlid=19.
Back to Citation171. https://www.cms.gov/files/document/medicare-covid-19-data-snapshot-fact-sheet.pdf.
172. Ochieng N., Cubanski J., Neuman T., Artiga S., and Damico A. Racial and Ethnic Health Inequities and Medicare. Kaiser Family Foundation. February 2021. Available at: https://www.kff.org/medicare/report/racial-and-ethnic-health-inequities-and-medicare/.
Back to Citation173. Weinhandl ED, Wetmore, JB, Peng Y., et al. Initial effects of COVID-19 on patients with ESKD. J Am Soc Nephrol. Published online April 8, 2021.doi:10.1681/ASN.2021010009.
Back to Citation174. https://www.cdc.gov/coronavirus/2019-ncov/community/health-equity/race-ethnicity.html.
Back to Citation177. Centers for Medicare and Medicaid Services Office of Minority Health. The CMS Equity Plan for Improving Quality in Medicare. 2015. https://www.cms.gov/About-CMS/Agency-Information/OMH/OMH_Dwnld-CMS_EquityPlanforMedicare_090615.pdf.
Back to Citation178. Centers for Medicare and Medicaid Services Office of Minority Health. Paving The Way To Equity: A Progress Report. 2015-2021. https://www.cms.gov/files/document/paving-way-equity-cms-omh-progress-report.pdf.
Back to Citation179. Centers for Medicare Services. CMS Quality Strategy. 2016. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/QualityInitiativesGenInfo/Downloads/CMS-Quality-Strategy.pdf.
Back to Citation181. https://www.cms.gov/About-CMS/Agency-Information/OMH/OMH-Mapping-Medicare-Disparities.
Back to Citation183. Centers for Medicare & Medicaid Services. Rural-Urban Disparities in Health Care in Medicare. 2019. https://www.cms.gov/About-CMS/Agency-Information/OMH/Downloads/Rural-Urban-Disparities-in-Health-Care-in-Medicare-Report.pdf.
Back to Citation184. Guide to Reducing Disparities in Readmissions. CMS Office of Minority Health. Revised August 2018. Available at: https://www.cms.gov/About-CMS/Agency-Information/OMH/Downloads/OMH_Readmissions_Guide.pdf.
Back to Citation185. CMS. Chronic Kidney Disease Disparities: Educational Guide for Primary Care. February 2020. Available at: https://www.cms.gov/files/document/chronic-kidney-disease-disparities-educational-guide-primary-care.pdf.
Back to Citation186. National Academies of Sciences, Engineering, and Medicine. 2016. Accounting for Social Risk Factors in Medicare Payment: Identifying Social Risk Factors. Washington, DC: The National Academies Press. https://doi.org/10.17226/21858.
Back to Citation189. Centers for Medicare Services. CMS Quality Strategy. 2016. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/QualityInitiativesGenInfo/Downloads/CMS-Quality-Strategy.pdf.
Back to Citation190. National Academies of Sciences, Engineering, and Medicine. 2016. Accounting for Social Risk Factors in Medicare Payment: Identifying Social Risk Factors. Washington, DC: The National Academies Press. https://doi.org/10.17226/21858.
Back to Citation192. https://www.kff.org/medicare/report/racial-and-ethnic-health-inequities-and-medicare/.
Back to Citation193. United States Renal Data System. 2018 Annual Data Report: ESRD Incidence, Prevalence, Patient Characteristics, and Treatment Modalities. Available online at https://www.usrds.org/2018/view/Default.aspx.
Back to Citation194. United States Renal Data System. 2018 Annual Data Report, Vol 2, Figure 1.12. Available online at https://www.usrds.org/2018/view/Default.aspx.
Back to Citation195. Executive Office of the President Office of Management and Budget, Office of Information and Regulatory Affairs. Revisions to the standards for the classification of federal data on race and ethnicity. Vol 62. Federal Register. 1997:58782-58790.
Back to Citation197. https://phinvads.cdc.gov/vads/ViewValueSet.action?id=67D34BBC-617F-DD11-B38D-00188B398520.
Back to Citation198. ONC criteria for certified health IT products: https://www.healthit.gov/isa/representing-patient-race-and-ethnicity.
Back to Citation199. Eicheldinger, C., & Bonito, A. (2008). More accurate racial and ethnic codes for Medicare administrative data. Health Care Financing Review, 29(3), 27-42.
Back to Citation200. Filice CE, Joynt KE. Examining Race and Ethnicity Information in Medicare Administrative Data. Med Care. 2017;55(12):e170-e176. doi:10.1097/MLR.0000000000000608.
201. Eicheldinger, C., & Bonito, A. (2008). More accurate racial and ethnic codes for Medicare administrative data. Health Care Financing Review, 29(3), 27-42.
Back to Citation202. Centers for Medicare and Medicaid Services. Building an Organizational Response to Health Disparities Inventory of Resources for Standardized Demographic and Language Data Collection. 2020. https://www.cms.gov/About-CMS/Agency-Information/OMH/Downloads/Data-Collection-Resources.pdf.
Back to Citation203. Centers for Medicare and Medicaid Services. Building an Organizational Response to Health Disparities Inventory of Resources for Standardized Demographic and Language Data Collection. 2020. https://www.cms.gov/About-CMS/Agency-Information/OMH/Downloads/Data-Collection-Resources.pdf.
Back to Citation204. https://pubmed.ncbi.nlm.nih.gov/18567241/, https://pubmed.ncbi.nlm.nih.gov/30506674/, Eicheldinger C., Bonito A. More accurate racial and ethnic codes for Medicare administrative data. Health Care Finance Rev. 2008;29(3):27-42. Haas A., Elliott MN, Dembosky JW, et al. Imputation of race/ethnicity to enable measurement of HEDIS performance by race/ethnicity. Health Serv Res. 2019;54(1):13-23. doi:10.1111/1475-6773.13099.
Back to Citation206. IOM. 2009. Race, Ethnicity, and Language Data: Standardization for Health Care Quality Improvement. Washington, DC: The National Academies Press.
Back to Citation207. IOM. 2009. Race, Ethnicity, and Language Data: Standardization for Health Care Quality Improvement. Washington, DC: The National Academies Press.
Back to Citation208. Eicheldinger, C., & Bonito, A. (2008). More accurate racial and ethnic codes for Medicare administrative data. Health Care Financing Review, 29(3), 27-42.
Back to Citation209. Haas, A., Elliott, M. et al., (2018). Imputation of race/ethnicity to enable measurement of HEDIS performance by race/ethnicity. Health Services Research, 54:13-23.
Back to Citation211. Haas, A., Elliott, M. et al., (2018). Imputation of race/ethnicity to enable measurement of HEDIS performance by race/ethnicity. Health Services Research, 54:13-23.
Back to Citation213. Haas, A., Elliott, M. et al., (2018). Imputation of race/ethnicity to enable measurement of HEDIS performance by race/ethnicity. Health Services Research, 54:13-23 and Bonito AJ, Bann C., Eicheldinger C., Carpenter L. Creation of New Race-Ethnicity Codes and Socioeconomic Status (SES) Indicators for Medicare Beneficiaries. Final Report, Sub-Task 2. (Prepared by RTI International for the Centers for Medicare and Medicaid Services through an interagency agreement with the Agency for Healthcare Research and Policy, under Contract No. 500-00-0024, Task No. 21) AHRQ Publication No. 08-0029-EF. Rockville, MD, Agency for Healthcare Research and Quality. January 2008.
Back to Citation214. The Centers for Medicare & Medicaid Services. CMS Quality Strategy. 2016. https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/QualityInitiativesGenInfo/Downloads/CMS-Quality-Strategy.pdf.
Back to Citation215. The Office of the National Coordinator for Health Information Technology. United State Core Data for Interoperability Draft Version 2. 2021. https://www.healthit.gov/isa/sites/isa/files/2021-01/Draft-USCDI-Version-2-January-2021-Final.pdf.
Back to Citation216. https://minorityhealth.hhs.gov/assets/pdf/checked/1/Fact_Sheet_Section_4302.pdf.
Back to Citation217. https://www.healthit.gov/sites/default/files/2020-08/2015EdCures_Update_CCG_USCDI.pdf.
Back to Citation218. Agniel D., Martino S.C., Burkhart Q., et al. Incentivizing Excellent Care to At-Risk Groups with a Health Equity Summary Score. J Gen Intern Med. Published online November 11, 2019 Nov 11. doi: 10.1007/s11606-019-05473-x.
Back to Citation219. U.S. Dept of Health and Human Services, Office of the Assistant Secretary for Preparedness and Response. (2020). Determination that a Public Health Emergency Exists. Available at: https://www.phe.gov/emergency/news/healthactions/phe/Pages/2019-nCoV.aspx.
Back to Citation220. Centers for Disease Control and Prevention. (2020). Your Health: Symptoms of Coronavirus. Available at: https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html.
Back to Citation221. Ibid.
Back to Citation222. Centers for Disease Control and Prevention. (2020). CDC COVID Data Tracker. Available at: https://covid.cdc.gov/covid-data-tracker/#cases_casesper100klast7days.
Back to Citation223. Associated Press. Tired to the Bone. Hospitals Overwhelmed with Virus Cases. November 18, 2020. Accessed on December 16, 2020, at https://apnews.com/article/hospitals-overwhelmed-coronavirus-cases-74a1f0dc3634917a5dc13408455cd895. Also see: New York Times. Just how full are U.S. intensive care units? New data paints an alarming picture. November 18, 2020. Accessed on December 16, 2020, at: https://www.nytimes.com/2020/12/09/world/just-how-full-are-us-intensive-care-units-new-data-paints-an-alarming-picture.html.
Back to Citation224. U.S. Currently Hospitalized | The COVID Tracking Project . Accessed January 31, 2021 at: https://covidtracking.com/data/charts/us-currently-hospitalized.
Back to Citation225. Centers for Disease Control and Prevention. (2021). How COVID-19 Spreads. Accessed on April 3, 2021 at: https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/how-covid-spreads.html.
Back to Citation226. Ibid.
Back to Citation227. Ibid.
Back to Citation228. Ibid.
Back to Citation229. Ibid.
Back to Citation230. Centers for Disease Control and Prevention. (2021). When to Quarantine. Accessed on April 2, 2021 at: https://www.cdc.gov/coronavirus/2019-ncov/if-you-are-sick/quarantine.html.
Back to Citation231. Centers for Disease Control and Prevention. (2021). Interim U.S. Guidance for Risk Assessment and Work Restrictions for Healthcare Personnel with Potential Exposure to COVID-19. Accessed on April 2 at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/faq.html#Transmission.
Back to Citation232. Dooling, K, McClung, M, et al. “The Advisory Committee on Immunization Practices' Interim Recommendations for Allocating Initial Supplies of COVID-19 Vaccine—United States, 2020.” Morb Mortal Wkly Rep. 2020; 69(49): 1857-1859.
Back to Citation233. The White House. Remarks by President Biden on the COVID-19 Response and the State of Vaccinations. Accessed on April 3, 2021 at: https://www.whitehouse.gov/briefing-room/speeches-remarks/2021/03/29/remarks-by-president-biden-on-the-covid-19-response-and-the-state-of-vaccinations/.
Back to Citation234. The White House. Remarks by President Biden on the COVID-19 Response and the State of Vaccinations. Accessed on June 2, 2021 at: https://www.whitehouse.gov/briefing-room/speeches-remarks/2021/04/21/remarks-by-president-biden-on-the-covid-19-response-and-the-state-of-vaccinations-2/.
Back to Citation235. The White House. Remarks by President Biden on the COVID-19 Response and the State of Vaccinations. Accessed on June 4, 2021, at: https://www.whitehouse.gov/briefing-room/statements-releases/2021/05/04/fact-sheet-president-biden-to-announce-goal-to-administer-at-least-one-vaccine-shot-to-70-of-the-u-s-adult-population-by-july-4th/.
Back to Citation236. Health and Human Services, Department of Defense. (2020) From the Factory to the Frontlines: The Operation Warp Speed Strategy for Distributing a COVID-19 Vaccine. Accessed December 18 at: https://www.hhs.gov/sites/default/files/strategy-for-distributing-covid-19-vaccine.pdf; Centers for Disease Control (2020). COVID-19 Vaccination Program Interim Playbook for Jurisdiction Operations. Accessed December 18 at: https://www.cdc.gov/vaccines/imz-managers/downloads/COVID-19-Vaccination-Program-Interim_Playbook.pdf.
Back to Citation237. Dooling, K, McClung, M, et al. “The Advisory Committee on Immunization Practices' Interim Recommendations for Allocating Initial Supplies of COVID-19 Vaccine—United States, 2020.” Morb. Mortal Wkly Rep. 2020; 69(49): 1857-1859. ACIP also recommended that long-term care residents be prioritized to receive the vaccine, given their age, high levels of underlying medical conditions, and congregate living situations make them high risk for severe illness from COVID-19.
Back to Citation238. Kates, J, Michaud, J, Tolbert, J. “How Are States Prioritizing Who Will Get the COVID-19 Vaccine First?” Kaiser Family Foundation. December 14, 2020. Accessed on December 16 at https://www.kff.org/policy-watch/how-are-states-prioritizing-who-will-get-the-covid-19-vaccine-first/.
Back to Citation239. Associated Press. `Healing is Coming:' U.S. Health Workers Start Getting Vaccine. December 15, 2020. Accessed on December 16 at: https://apnews.com/article/us-health-workers-coronavirus-vaccine-56df745388a9fc12ae93c6f9a0d0e81f.
Back to Citation240. Kates, J, Michaud, J, Tolbert, J. “The COVID-19 Vaccine Priority Line Continues to Change as States Make Further Updates.” Kaiser Family Foundation. January 21, 2021. Accessed on January 29 at https://www.kff.org/policy-watch/the-covid-19-vaccine-priority-line-continues-to-change-as-states-make-further-updates/.
Back to Citation241. Dooling K, Marin M, Wallace M, et al. “The Advisory Committee on Immunization Practices' Updated Interim Recommendation for Allocation of COVID-19 Vaccine—United States, December 2020.” MMWR Morb Mortal Wkly Rep 2021; 69:1657-1660. ACIP recommended that the COVID-19 vaccine should be offered to persons aged ≥75 years and non-health care frontline essential workers in Phase 1b, and to persons aged 16-64 years with high-risk medical conditions in Phase 1c.
Back to Citation242. Centers for Disease Control and Prevention. COVID Data Tracker. COVID-19 Vaccinations in the United States. Accessed June 23, 2021 at: https://covid.cdc.gov/covid-data-tracker/#vaccinations.
Back to Citation243. The White House. Remarks by President Biden Marking the 150 Millionth COVID-19 Vaccine Shot. Accessed April 8, 2021 at: https://www.whitehouse.gov/briefing-room/speeches-remarks/2021/04/06/remarks-by-president-biden-marking-the-150-millionth-covid-19-vaccine-shot/.
Back to Citation244. The White House. FACT SHEET: Biden Administration Announces Historic $10 Billion Investment to Expand Access to COVID-19 Vaccines and Build Vaccine Confidence in Hardest-Hit and Highest-Risk Communities. March 25, 2021. Available at: https://www.whitehouse.gov/briefing-room/statements-releases/2021/03/25/fact-sheet-biden-administration-announces-historic-10-billion-investment-to-expand-access-to-covid-19-vaccines-and-build-vaccine-confidence-in-hardest-hit-and-highest-risk-communities/.
Back to Citation247. https://www.cdc.gov/nhsn/pdfs/hps/covidvax/weekly-covid-guidance-508.pdf.
Back to Citation249. Centers for Disease Control and Prevention. Overview of Influenza Vaccination among Health Care Personnel. October 2020. (2020) Accessed March 16, 2021 at: https://www.cdc.gov/flu/toolkit/long-term-care/why.htm.
Back to Citation250. Measure Application Committee Coordinating Committee Meeting Presentation. March 15, 2021. (2021) Accessed March 16, 2021 at: http://www.qualityforum.org/Project_Pages/MAP_Coordinating_Committee.aspx.
Back to Citation251. Verma, A., Patel, A., Tio, M., Waikar, S., “Caring for Dialysis Patients in a Time of COVID-19”. Kidney Medicine, Volume 2, Issue 6, 2020, Pages 787-792, ISSN 2590-0595. Available at https://doi.org/10.1016/j.xkme.2020.07.006.
Back to Citation252. Ibid.
Back to Citation253. National Quality Forum. List of Measures Under Consideration for December 21, 2020. Accessed at: https://www.cms.gov/files/document/measures-under-consideration-list-2020-report.pdf on January 29 2021.
Back to Citation254. Measure Applications Partnership. MAP Preliminary Recommendations 2020-2021. Accessed on January 24, 2021 at: http://www.qualityforum.org/Project_Pages/MAP_Hospital_Workgroup.aspx.
Back to Citation255. Ibid.
Back to Citation256. Ibid.
Back to Citation257. Ibid.
Back to Citation258. Measure Applications Partnership. 2020-2021 MAP Final Recommendations. Accessed on February 3, 2021 at: http://www.qualityforum.org/Setting_Priorities/Partnership/Measure_Applications_Partnership.aspx.
Back to Citation259. Measure Applications Partnership. 2020-2021 MAP Final Recommendations. Accessed on February 23, 2021 at: http://www.qualityforum.org/Project_Pages/MAP_Hospital_Workgroup.aspx.
Back to Citation260. Measure Applications Partnership. 2020-2021 MAP Final Recommendations. Accessed on February 23, 2021 at: http://www.qualityforum.org/Project_Pages/MAP_Hospital_Workgroup.aspx.
Back to Citation261. Specifications for both measures available at: https://www.qualityforum.org/WorkArea/linkit.aspx?LinkIdentifier=id&ItemID=94650.
Back to Citation262. What are patient generated health data: https://www.healthit.gov/topic/otherhot-topics/what-are-patient-generated-health-data.
Back to Citation263. Application Programming Interfaces (API) Resource Guide, Version 1.0. Available at: https://www.healthit.gov/sites/default/files/page/2020-11/API-Resource-Guide_v1_0.pdf.
Back to Citation264. https://www.healthit.gov/isa/united-states-core-data-interoperability-uscdi.
Back to Citation265. Information Blocking and the ONC Health IT Certification Program: Extension of Compliance Dates and Timeframes in Response to the Covid-19 Public Health Emergency. https://www.govinfo.gov/content/pkg/FR-2020-11-04/pdf/2020-24376.pdf.
Back to Citation266. The Office of the National Coordinator for Health Information Technology, Strategy on Reducing Regulatory and Administrative Burden Relating to the Use of Health IT and EHRs, Final Report (Feb. 2020). Available at: https://www.healthit.gov/sites/default/files/page/2020-02/BurdenReport_0.pdf.
Back to Citation267. eCQI Resource Center, https://ecqi.healthit.gov/.
Back to Citation268. Calendar Year (CY) 2021 Physician Fee Schedule Final Rule: Finalized (New and Updated) Qualified Clinical Data Registry (QCDR) and Qualified Registry Policies, https://qpp-cm-prod-content.s3.amazonaws.com/uploads/1362/QCDR%20and%20QR%20Updates%202021%20Final%20Rule%20Fact%20Sheet.pdf.
Back to Citation269. Department of Health and Human Services, National Health Quality Roadmap (May 2020). Available at: https://www.hhs.gov/sites/default/files/national-health-quality-roadmap.pdf.
Back to Citation270. ZIP code TM. is a trademark of the United States Postal Service.
Back to Citation271. Wilk, Adam S., Lea, Janice P. (2019). How Extended Hemodialysis Treatment Time Can Affect Patient Quality of Life. Clinical Journal of the American Society of Nephrology, 23, 479-485. doi:10.1111/hdi.12782.
Back to Citation272. Burton, J. and Graham-Brown, M., 2018. Nocturnal hemodialysis. Current Opinion in Nephrology and Hypertension, 27(6), pp.472-477.
273. Kalim, S., Wald, R., Yan, A. T., Goldstein, M. B., Kiaii, M., Xu, D., . . . Perl, J. (2018). Extended duration nocturnal hemodialysis and changes in plasma metabolite profiles. Clinical Journal of the American Society of Nephrology, 13(3), 436-444. doi:10.2215/cjn.08790817.
274. Nesrallah, G. E., Lindsay, R. M., Cuerden, M. S., Garg, A. X., Port, F., Austin, P. C., . . . Suri, R. S. (2012). Intensive hemodialysis associates with improved survival compared with conventional hemodialysis. Journal of the American Society of Nephrology, 23(4), 696-705. doi:10.1681/asn.2011070676.
275. Wong, B., Collister, D., Muneer, M., Storie, D., Courtney, M., Lloyd, A., . . . Pauly, R. P. (2017). In-center nocturnal hemodialysis versus conventional hemodialysis: A systematic review of the evidence. American Journal of Kidney Diseases, 70(2), 218-234. doi:10.1053/j.ajkd.2017.01.047.
276 Wilk, Adam S., Lea, Janice P. (2019). How Extended Hemodialysis Treatment Time Can Affect Patient Quality of Life. Clinical Journal of the American Society of Nephrology, 23, 479-485. doi:10.1111/hdi.12782.
276. Lacson E, Diaz-Buxo J. In-center nocturnal hemodialysis performed thrice-weekly—a provider's perspective. Semin Dial. 2011 Nov-Dec;24(6):668-73. doi: 10.1111/j.1525-139X.2011.00998.x. Epub 2011 Nov 22. PMID: 22106828.
Back to Citation277. Bugeja A, Dacouris N, Thomas A, Marticorena R, McFarlane P, Donnelly S, Goldstein M. In-center nocturnal hemodialysis: another option in the management of chronic kidney disease. Clin J Am Soc Nephrol. 2009 Apr;4(4):778-83. doi: 10.2215/CJN.05221008. Epub 2009 Apr 1. PMID: 19339410; PMCID: PMC2666425.
278. Lacson E, Diaz-Buxo J. In-center nocturnal hemodialysis performed thrice-weekly—a provider's perspective. Semin Dial. 2011 Nov-Dec;24(6):668-73. doi: 10.1111/j.1525-139X.2011.00998.x. Epub 2011 Nov 22. PMID: 22106828.
Back to Citation279. Ibid.
Back to Citation280. United States Renal Data System. 2015. “2015 Researcher's Guide to the USRDS Database.” https://usrds.org/media/2219/2015_usrds_researchers_guide_15.pdf.
Back to Citation281. Mehrotra R, Khawar O, Duong U, Fried L, Norris K, Nissenson A, Kalantar-Zadeh K. Ownership patterns of dialysis units and peritoneal dialysis in the United States: utilization and outcomes. Am J Kidney Dis. 2009 Aug;54(2):289-98. doi: 10.1053/j.ajkd.2009.01.262. Epub 2009 Apr 8. PMID: 19359081.
282. Gander JC, Zhang X, Ross K, et al. Association Between Dialysis Facility Ownership and Access to Kidney Transplantation. JAMA. 2019;322(10):957-973. doi:10.1001/jama.2019.12803.
Back to Citation283. Medicare Payment Advisory Commission. 2021. Report to the Congress: Medicare and the health care delivery system. Washington, DC: MedPAC. http://www.medpac.gov/docs/default-source/reports/mar21_medpac_report_to_the_congress_sec.pdf.
Back to Citation284. Under 45 CFR 164.103, “Required by law” means “a mandate contained in law that compels an entity to make a use or disclosure of protected health information and that is enforceable in a court of law.” It includes, among other things, “statutes or regulations that require the production of information, including statutes or regulations that require such information if payment is sought under a government program providing public benefits.”
Back to Citation285. Table 1.2 in United States Renal Data System, 2020 Annual Report, Chronic Kidney Disease: Chapter 1, CKD in the General Population, available at https://adr.usrds.org/2020/chronic-kidney-disease/1-ckd-in-the-general-population (indicating that the prevalence of CKD in those above the poverty line is 14.4 percent while the prevalence of CKD in those below the poverty line is 17.4 percent. See also McClellan, W.M., et al., Poverty and Racial Disparities in Kidney Disease: The REGARDS Study, Am. J Nephrol, 2010, Volume 32, Issue 1, pages 38-46, available at https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2914392/ (providing data suggesting that lower household income is associated with higher prevalence of CKD).
Back to Citation286. Morton, R.L, et al., Impact of CKD on Household Income, Kidney International Reports, Volume 3, Issue 3, 2018, pages 610-618, available at https://www.sciencedirect.com/science/article/pii/S2468024917304795?via%3Dihub.
Back to Citation298. The FDL amount is the amount by which an ESRD facility's per-treatment Medicare allowable payment amount for furnishing ESRD outlier services to an adult/pediatric beneficiary must exceed the adult/pediatric predicted ESRD outlier services Medicare allowable payment amount to be eligible for an outlier payment.
Back to Citation299. Outlier percentages for the pediatric population have high variability from year to year, but have consistently met or exceeded the 1.0 percent target. The methodological modifications in this RFI do not apply to the pediatric population.
Back to Citation300. The example uses CY 2020 to judge the performance of the alternative methodology. The most recent year with complete data when the 2020 FDL was determined was 2018.
Back to Citation302. The fraction would be 158/100, that is $1.58 is spent overall on pediatric dialysis treatments for every $1.00 spent for adult patients.
Back to Citation303. $7.30 is spent, overall, on supplies for a pediatric dialysis treatment for every $1.00 spent on supplies for an adult treatment.
Back to Citation304. https://www.bls.gov/oes/current/oes292098.htm. Accessed on June 7, 2021.
Back to Citation305. UNOS. 2021. COVID-19 and Solid Organ Transplants. Transplant and Waitlist Data Visualizations. https://unos.org/covid/.
Back to Citation306. United States Renal Data System. 2020. “ADR Reference Table E6 Renal Transplants by Donor Type.” https://adr.usrds.org/2020/reference-tables.
Back to Citation307. Organ Procurement and Transplantation Network. 2021. “Current US Waiting List, Overall by Organ.” https://optn.transplant.hrsa.gov/data/view-data-reports/national-data/#.
Back to CitationBILLING CODE 4120-01-P
BILLING CODE 4120-01-C
BILLING CODE 4120-01-P
BILLING CODE 4120-01-C
BILLING CODE 4120-01-C
BILLING CODE 4120-01-P
BILLING CODE 4120-01-C
BILLING CODE 4120-01-P
BILLING CODE 4120-01-C
BILLING CODE 4120-01-P
BILLING CODE 4120-01-C
[FR Doc. 2021-14250 Filed 7-1-21; 4:15 pm]
BILLING CODE 4120-01-P



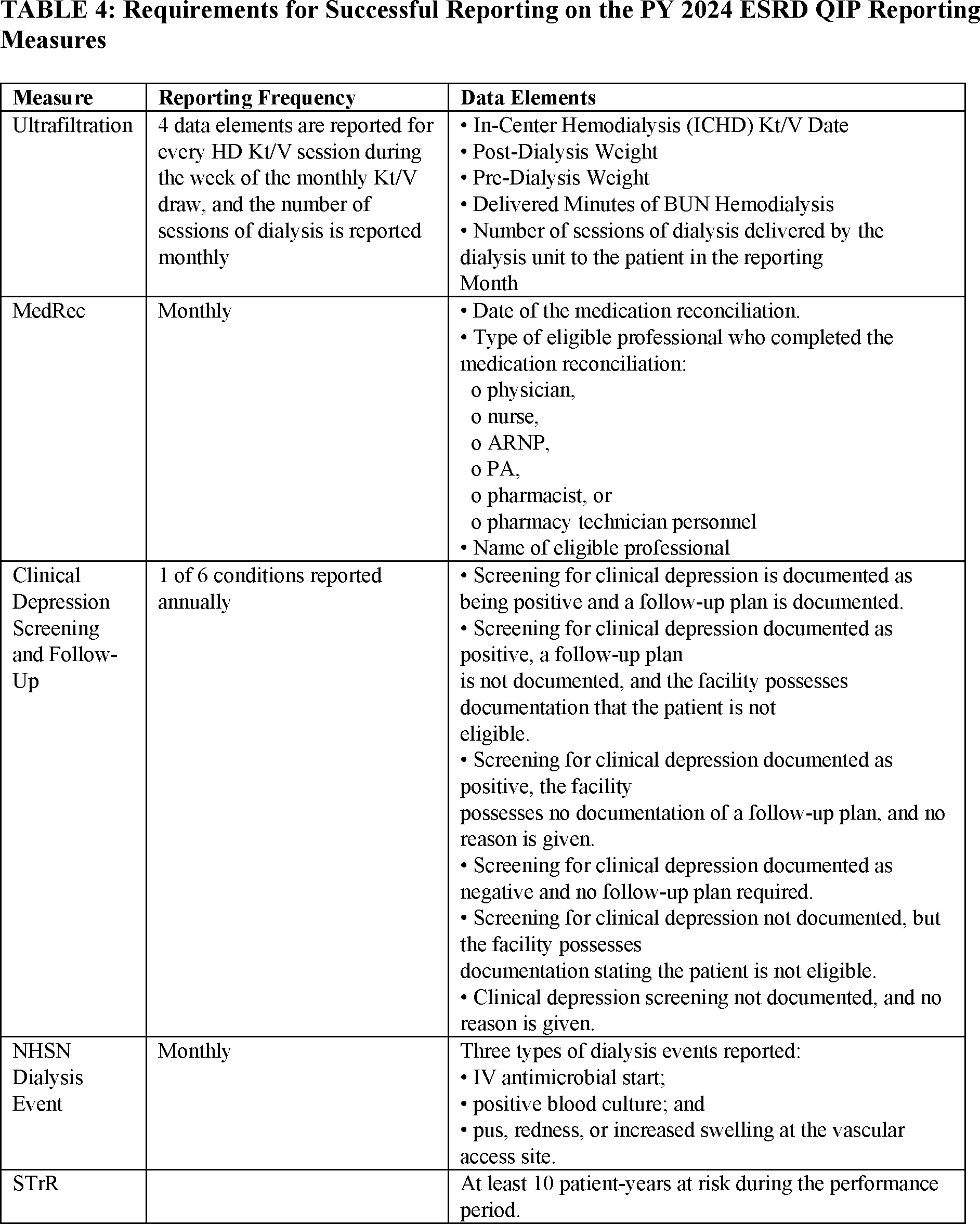
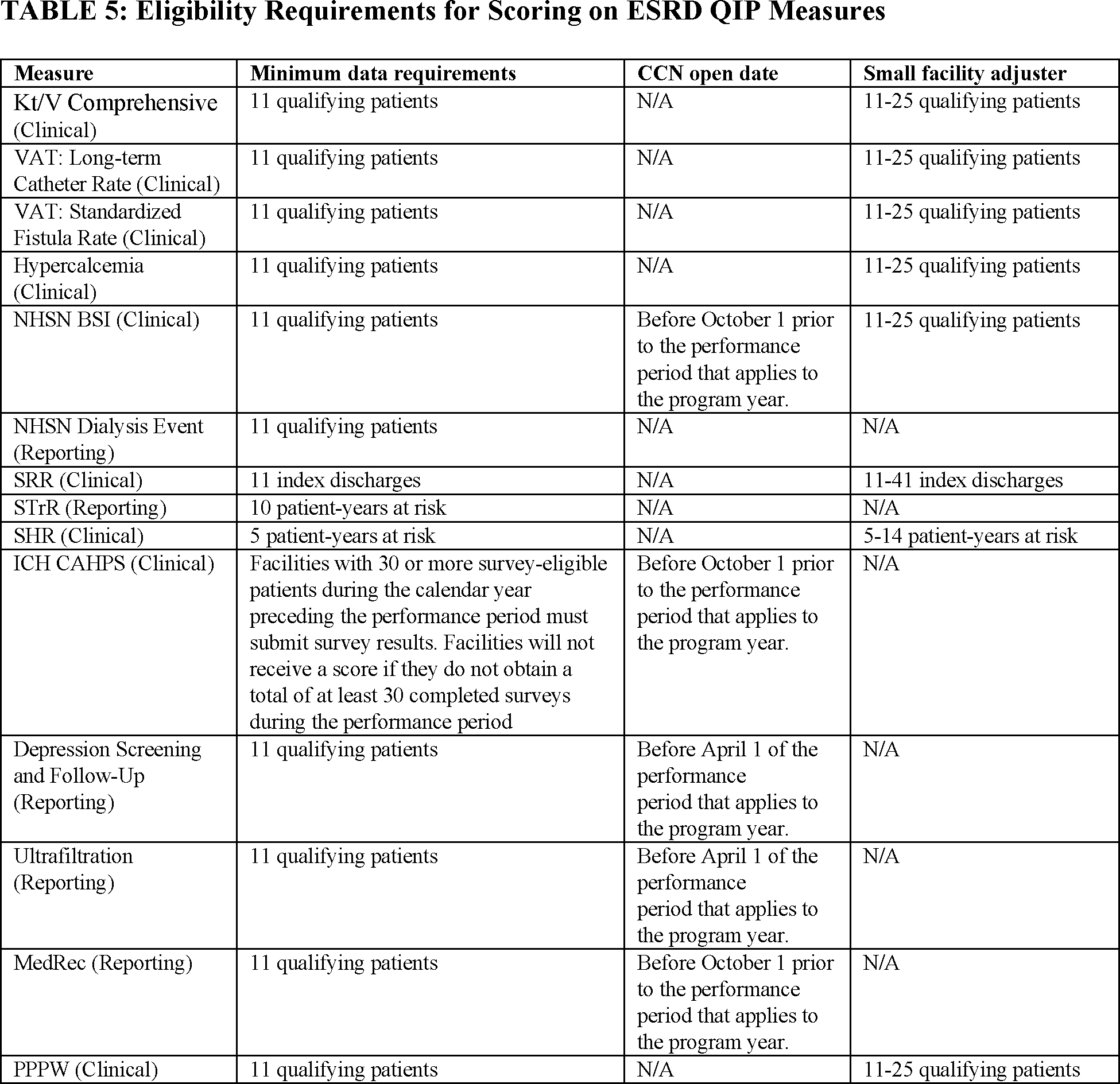
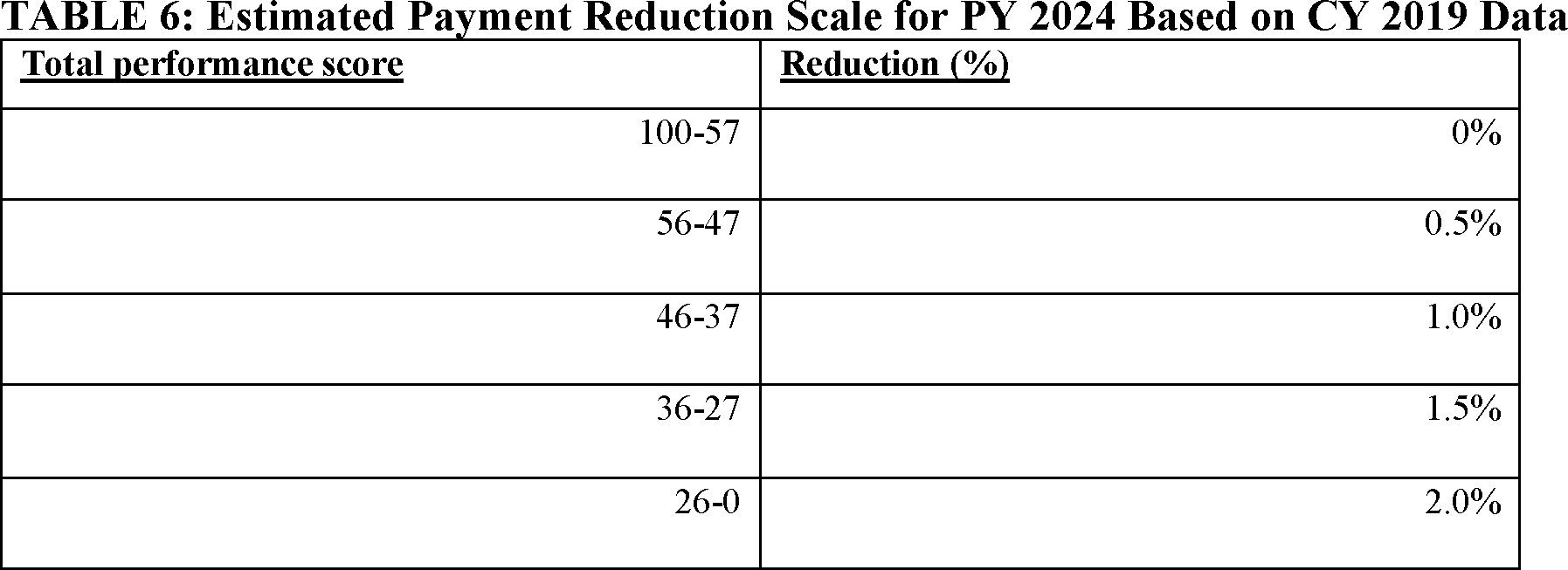













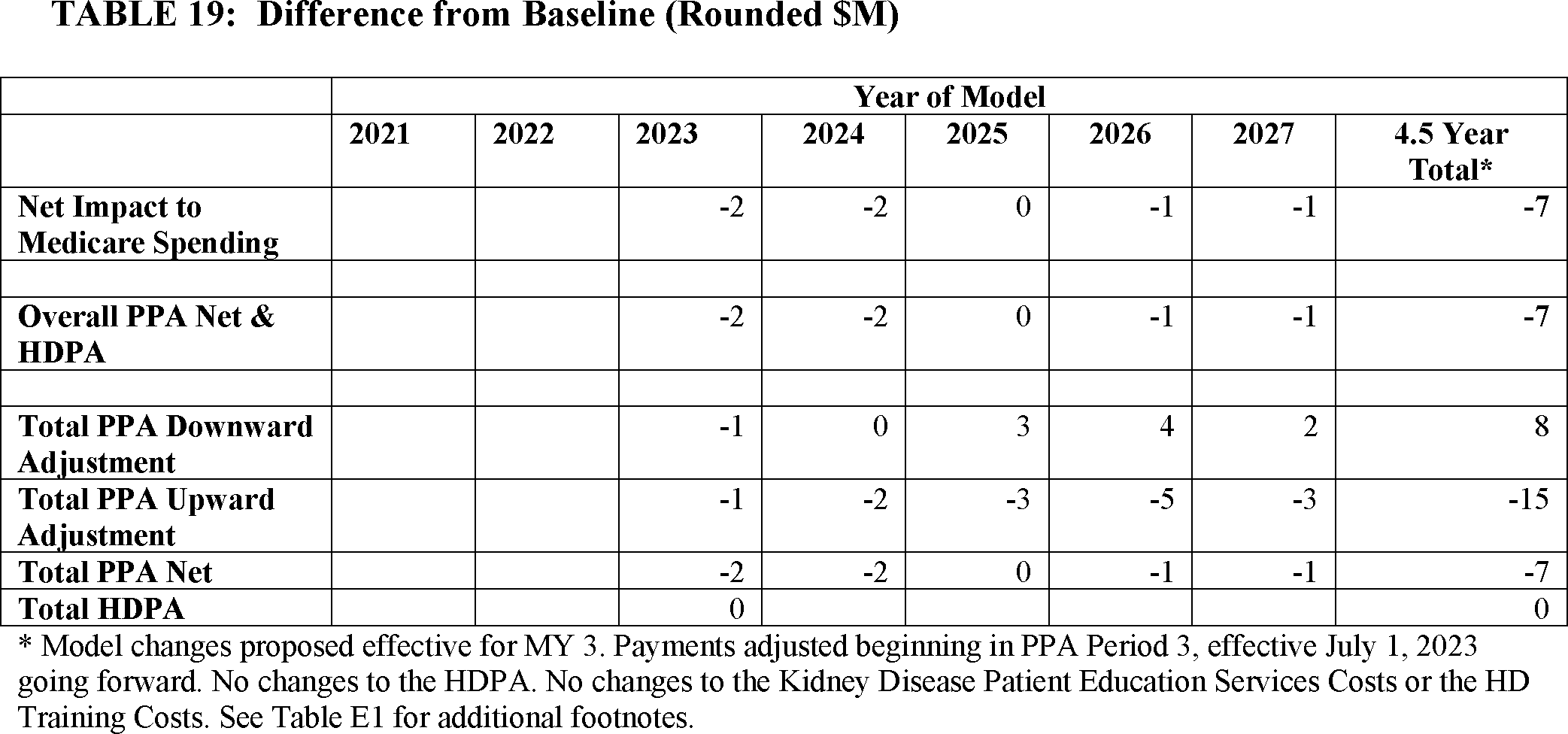



Document Information
- Published:
- 07/09/2021
- Department:
- Centers for Medicare & Medicaid Services
- Entry Type:
- Proposed Rule
- Action:
- Proposed rule.
- Document Number:
- 2021-14250
- Dates:
- To be assured consideration, comments must be submitted at one
- Pages:
- 36322-36437 (116 pages)
- Docket Numbers:
- CMS-1749-P
- RINs:
- 0938-AU39: CY 2022 Changes to the End-Stage Renal Disease (ESRD) Prospective Payment System and Quality Incentive Program (CMS-1749)
- RIN Links:
- https://www.federalregister.gov/regulations/0938-AU39/cy-2022-changes-to-the-end-stage-renal-disease-esrd-prospective-payment-system-and-quality-incentive
- Topics:
- Administrative practice and procedure, Diseases, Health facilities, Medicare, Puerto Rico, Reporting and recordkeeping requirements
- PDF File:
- 2021-14250.pdf
- Supporting Documents:
- » Medicare Program: End-Stage Renal Disease Prospective Payment System, Payment for Renal Dialysis Services Furnished to Individuals With Acute Kidney Injury, End-Stage Renal Disease Quality Incentive Program, andEnd-Stage Renal Disease Treatment Choices Model; Correction
- » Medicare Program: End-Stage Renal Disease Prospective Payment System, Payment for Renal Dialysis Services Furnished to Individuals with Acute Kidney Injury, End-Stage Renal Disease Quality Incentive Program, and End-Stage Renal Disease Treatment Choices Model
- » Medicare Program: End-Stage Renal Disease Prospective Payment System, Payment for Renal Dialysis Services Furnished to Individuals with Acute Kidney Injury, End-Stage Renal Disease Quality Incentive Program, and End-Stage Renal Disease Treatment Choices Model
- » CMS-1749-P Display
- CFR: (9)
- 42 CFR 413.177
- 42 CFR 413.178
- 42 CFR 512.160
- 42 CFR 512.310
- 42 CFR 512.360
- More ...