2021-16310. Medicare Program; Inpatient Rehabilitation Facility Prospective Payment System for Federal Fiscal Year 2022 and Updates to the IRF Quality Reporting Program; Payment for Complex Rehabilitative Wheelchairs and Related Accessories (...
-
Start Preamble
Start Printed Page 42362
AGENCY:
Centers for Medicare & Medicaid Services (CMS), HHS.
ACTION:
Final rule.
SUMMARY:
This final rule updates the prospective payment rates for inpatient rehabilitation facilities (IRFs) for Federal fiscal year (FY) 2022. As required by statute, this final rule includes the classification and weighting factors for the IRF prospective payment system's case-mix groups and a description of the methodologies and data used in computing the prospective payment rates for FY 2022. This final rule also includes updates for the IRF Quality Reporting Program (QRP). In addition, we are finalizing a Medicare provision adopted in an interim final rule with comment period (IFC) issued on May 11, 2018 related to fee schedule adjustments for wheelchair accessories (including seating systems) and seat and back cushions furnished in connection with group 3 or higher complex rehabilitative power wheelchairs as well as changes to the regulations related to the Further Consolidated Appropriations Act, 2020 governing payment for these and other items.
DATES:
Effective date: These regulations are effective on October 1, 2021.
Applicability dates: The updated IRF prospective payment rates are applicable for IRF discharges occurring on or after October 1, 2021, and on or before September 30, 2022 (FY 2022).
Start Further InfoFOR FURTHER INFORMATION CONTACT:
Gwendolyn Johnson, (410) 786-6954, for general information.
Catie Cooksey, (410) 786-0179, for information about the IRF payment policies and payment rates.
Kadie Derby, (410) 786-0468, for information about the IRF coverage policies.
Ariel Adams, (410) 786-8571, for information about the IRF quality reporting program.
DMEPOS@cms.hhs.gov or Alexander Ullman, (410) 786-9671, for issues related to the DMEPOS payment policy.
End Further Info End Preamble Start Supplemental InformationSUPPLEMENTARY INFORMATION:
Availability of Certain Information Through the Internet on the CMS Website
The IRF prospective payment system (IRF PPS) Addenda along with other supporting documents and tables referenced in this final rule are available through the internet on the CMS website at https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/InpatientRehabFacPPS.
We note that prior to 2020, each rule or notice issued under the IRF PPS has included a detailed reiteration of the various regulatory provisions that have affected the IRF PPS over the years. That discussion, along with detailed background information for various other aspects of the IRF PPS, is now available on the CMS website at https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/InpatientRehabFacPPS.
I. Executive Summary
A. Purpose
This final rule updates the prospective payment rates for IRFs for FY 2022 (that is, for discharges occurring on or after October 1, 2021, and on or before September 30, 2022) as required under section 1886(j)(3)(C) of the Social Security Act (the Act). As required by section 1886(j)(5) of the Act, this final rule includes the classification and weighting factors for the IRF PPS's case-mix groups (CMGs) and a description of the methodologies and data used in computing the prospective payment rates for FY 2022. This final rule adds one new measure to the IRF QRP and modifies the denominator for another measure currently under the IRF QRP beginning with the FY 2023 IRF QRP. In addition, this final rule modifies the number of quarters used for publicly reporting certain IRF QRP measures due to the public health emergency (PHE). In this final rule, we summarize comments we sought on the use of Health Level Seven International (HL7®) Fast Healthcare Interoperability Resources® (FHIR)-based standards in post-acute care, specifically the IRF QRP, and on our continued efforts to close the health equity gap. This final rule also finalizes a Medicare provision adopted in an interim final rule with comment period (IFC) published in the May 11, 2018 Federal Register entitled “Medicare Program; Durable Medical Equipment Fee Schedule Adjustments to Resume the Transitional 50/50 Blended Rates to Provide Relief in Rural Areas and Non-Contiguous Areas” (83 FR 21912) that excludes the fee schedule amounts for wheelchair accessories (including seating systems) and seat and back cushions furnished in connection with group 3 or higher complex rehabilitative power wheelchairs from adjustments based on information from the Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) Competitive Bidding Program (CBP). In response to public comments on the IFC published in the May 11, 2018 Federal Register, we are also finalizing an extension of this policy to wheelchair accessories (including seating systems) and seat and back cushions furnished in connection with complex rehabilitative manual wheelchairs in this final rule. In addition, this rule finalizes a Medicare provision that was included in the proposed rule published in the November 4, 2020 Federal Register entitled “Medicare Program; Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) Policy Issues and Level II of the Healthcare Common Procedure Coding System (HCPCS)” (85 FR 70358). The provision implements section 106(a) of division N, title I of the Further Consolidated Appropriations Act, 2020 (FCAA) (Pub. L. 116-94, December 20, 2019) by modifying a regulatory definition in order to exclude complex rehabilitative manual wheelchairs and certain other manual wheelchairs and related accessories when furnished in connection with these wheelchairs from the DMEPOS CBP.
Start Printed Page 42363B. Summary of Major Provisions
In this final rule, we use the methods described in the FY 2021 IRF PPS final rule (85 FR 48424) to update the prospective payment rates for FY 2022 using updated FY 2020 IRF claims and the most recent available IRF cost report data, which is FY 2019 IRF cost report data. This final rule updates certain requirements for the IRF QRP. In addition, this final rule addresses fee schedule adjustments for wheelchair accessories (including seating systems) and seat and back cushions furnished in connection with Group 3 or higher complex rehabilitative power wheelchairs and complex rehabilitative manual wheelchairs. This final rule also revises the definition of “item” under the DMEPOS CBP at 42 CFR 414.402 to exclude complex rehabilitative manual wheelchairs and certain other manual wheelchairs and related accessories from the DMEPOS CBP, as required by section 106(a) of the FCAA.
C. Summary of Impact

II. Background
A. Statutory Basis and Scope for IRF PPS Provisions
Section 1886(j) of the Act provides for the implementation of a per-discharge PPS for inpatient rehabilitation hospitals and inpatient rehabilitation units of a hospital (collectively, hereinafter referred to as IRFs). Payments under the IRF PPS encompass inpatient operating and capital costs of furnishing covered rehabilitation services (that is, routine, ancillary, and capital costs), but not direct graduate medical education costs, costs of approved nursing and allied health education activities, bad debts, and other services or items outside the scope of the IRF PPS. A complete discussion of the IRF PPS provisions appears in the original FY 2002 IRF PPS final rule (66 FR 41316) and the FY 2006 IRF PPS final rule (70 FR 47880) and we provided a general description of the IRF PPS for FYs 2007 through 2019 in the FY 2020 IRF PPS final rule (84 FR 39055 through 39057).
Under the IRF PPS from FY 2002 through FY 2005, the prospective payment rates were computed across 100 distinct CMGs, as described in the FY 2002 IRF PPS final rule (66 FR 41316). We constructed 95 CMGs using rehabilitation impairment categories (RICs), functional status (both motor and cognitive), and age (in some cases, cognitive status and age may not be a factor in defining a CMG). In addition, we constructed five special CMGs to account for very short stays and for patients who expire in the IRF.
For each of the CMGs, we developed relative weighting factors to account for a patient's clinical characteristics and expected resource needs. Thus, the weighting factors accounted for the relative difference in resource use across all CMGs. Within each CMG, we created tiers based on the estimated effects that certain comorbidities would have on resource use.
We established the Federal PPS rates using a standardized payment conversion factor (formerly referred to as the budget-neutral conversion factor). For a detailed discussion of the budget-neutral conversion factor, please refer to our FY 2004 IRF PPS final rule (68 FR 45684 through 45685). In the FY 2006 IRF PPS final rule (70 FR 47880), we discussed in detail the methodology for determining the standard payment conversion factor.
We applied the relative weighting factors to the standard payment conversion factor to compute the unadjusted prospective payment rates under the IRF PPS from FYs 2002 through 2005. Within the structure of the payment system, we then made adjustments to account for interrupted stays, transfers, short stays, and deaths. Finally, we applied the applicable adjustments to account for geographic variations in wages (wage index), the percentage of low-income patients, location in a rural area (if applicable), and outlier payments (if applicable) to the IRFs' unadjusted prospective payment rates.
For cost reporting periods that began on or after January 1, 2002, and before October 1, 2002, we determined the final prospective payment amounts using the transition methodology prescribed in section 1886(j)(1) of the Act. Under this provision, IRFs transitioning into the PPS were paid a blend of the Federal IRF PPS rate and the payment that the IRFs would have received had the IRF PPS not been implemented. This provision also allowed IRFs to elect to bypass this blended payment and immediately be paid 100 percent of the Federal IRF PPS rate. The transition methodology expired as of cost reporting periods beginning on or after October 1, 2002 (FY 2003), and payments for all IRFs now consist of 100 percent of the Federal IRF PPS rate.
Section 1886(j) of the Act confers broad statutory authority upon the Secretary to propose refinements to the IRF PPS. In the FY 2006 IRF PPS final rule (70 FR 47880) and in correcting amendments to the FY 2006 IRF PPS final rule (70 FR 57166), we finalized a number of refinements to the IRF PPS case-mix classification system (the CMGs and the corresponding relative weights) and the case-level and facility-level adjustments. These refinements included the adoption of the Office of Management and Budget's (OMB's) Core-Based Statistical Area (CBSA) market definitions; modifications to the CMGs, tier comorbidities; and CMG relative weights, implementation of a new teaching status adjustment for IRFs; rebasing and revising the market basket Start Printed Page 42364index used to update IRF payments, and updates to the rural, low-income percentage (LIP), and high-cost outlier adjustments. Beginning with the FY 2006 IRF PPS final rule (70 FR 47908 through 47917), the market basket index used to update IRF payments was a market basket reflecting the operating and capital cost structures for freestanding IRFs, freestanding inpatient psychiatric facilities (IPFs), and long-term care hospitals (LTCHs) (hereinafter referred to as the rehabilitation, psychiatric, and long-term care (RPL) market basket). Any reference to the FY 2006 IRF PPS final rule in this final rule also includes the provisions effective in the correcting amendments. For a detailed discussion of the final key policy changes for FY 2006, please refer to the FY 2006 IRF PPS final rule.
The regulatory history previously included in each rule or notice issued under the IRF PPS, including a general description of the IRF PPS for FYs 2007 through 2020, is available on the CMS website at https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/InpatientRehabFacPPS.
In late 2019,[1] the United States began responding to an outbreak of a virus named “SARS-CoV-2” and the disease it causes, which is named “coronavirus disease 2019” (abbreviated “COVID-19”). Due to our prioritizing efforts in support of containing and combatting the PHE for COVID-19, and devoting significant resources to that end, we published two interim final rules with comment period affecting IRF payment and conditions for participation. The interim final rule with comment period (IFC) entitled, “Medicare and Medicaid Programs; Policy and Regulatory Revisions in Response to the COVID-19 Public Health Emergency”, published on April 6, 2020 (85 FR 19230) (hereinafter referred to as the April 6, 2020 IFC), included certain changes to the IRF PPS medical supervision requirements at 42 CFR 412.622(a)(3)(iv) and 412.29(e) during the PHE for COVID-19. In addition, in the April 6, 2020 IFC, we removed the post-admission physician evaluation requirement at § 412.622(a)(4)(ii) for all IRFs during the PHE for COVID-19. In the FY 2021 IRF PPS final rule, to ease documentation and administrative burden, we also removed the post-admission physician evaluation documentation requirement at 42 CFR 412.622(a)(4)(ii) permanently beginning in FY 2021.
A second IFC entitled, “Medicare and Medicaid Programs, Basic Health Program, and Exchanges; Additional Policy and Regulatory Revisions in Response to the COVID-19 Public Health Emergency and Delay of Certain Reporting Requirements for the Skilled Nursing Facility Quality Reporting Program” was published on May 8, 2020 (85 FR 27550) (hereinafter referred to as the May 8, 2020 IFC). Among other changes, the May 8, 2020 IFC included a waiver of the “3-hour rule” at § 412.622(a)(3)(ii) to reflect the waiver required by section 3711(a) of the Coronavirus Aid, Relief, and Economic Security Act (CARES Act) (Pub. L. 116-136, enacted on March 27, 2020). In the May 8, 2020 IFC, we also modified certain IRF coverage and classification requirements for freestanding IRF hospitals to relieve acute care hospital capacity concerns in states (or regions, as applicable) that are experiencing a surge during the PHE for COVID-19. In addition to the policies adopted in our IFCs, we responded to the PHE with numerous blanket waivers [2] and other flexibilities,[3] some of which are applicable to the IRF PPS.
B. Statutory Basis and Scope for DMEPOS Provisions
Section 1847(a) of the Act, as amended by section 302(b)(1) of the Medicare Prescription Drug, Improvement, and Modernization Act of 2003 (Pub. L. 108-173, December 8, 2003), requires CMS to implement the Medicare Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) Competitive Bidding Program (CBP) for contract award purposes in order to furnish certain competitively priced DMEPOS items and services subject to the CBP. Such items and services include:
- Off-the-shelf (OTS) orthotics, for which payment would otherwise be made under section 1834(h) of the Act;
- Enteral nutrients, equipment, and supplies described in section 1842(s)(2)(D) of the Act; and
- Certain DME and medical supplies, which are covered items (as defined in section 1834(a)(13) of the Act) for which payment would otherwise be made under section 1834(a) of the Act.
Section 1834(a)(1)(F)(ii) of the Act requires the Secretary to use information on the payment determined under the Medicare DMEPOS CBP to adjust the fee schedule amounts for DME items and services furnished in all non-CBAs on or after January 1, 2016. Section 1834(a)(1)(F)(iii) of the Act requires the Secretary to continue to make these adjustments as additional covered items are phased in under the CBP or information is updated as new CBP contracts are awarded.
Section 2 of the Patient Access and Medicare Protection Act of 2015 (Pub. L. 114-115, December 28, 2015) excluded the accessories furnished in connection with Group 3 complex rehabilitative power wheelchairs from the fee schedule adjustments under section 1834(a)(1)(F)(ii) of the Act from January 1 through December 31, 2016. Congress then extended this exclusion through June 2017 under section 16005 of the 21st Century Cures Act of 2016 (Pub. L. 114-255, December 13, 2016). In June 2017, we elected to continue this policy through program instructions, followed by interim final rule in 2018, entitled “Medicare Program; Durable Medical Equipment Fee Schedule Adjustments to Resume the Transitional 50/50 Blended Rates to Provide Relief in Rural Areas and Non-Contiguous Areas” (83 FR 21912). On April 26, 2021, we announced the continuation of effectiveness of the 2018 interim final rule and the extension of the timeline for publication of the final rule (86 FR 21949).
Section 106(a) of the FCAA excludes complex rehabilitative manual wheelchairs and certain other manual wheelchairs and wheelchair accessories and seat and back cushions when furnished in connection with these wheelchairs from the DMEPOS CBP. Section 106(b) of the FCAA excludes these items from fee schedule adjustments based on information from the DMEPOS CBP through June 30, 2021. We address section 1834(a)(1)(F)(ii) of the Act and payment for these items in this final rule.
We issued a proposed rule on November 4, 2020 (85 FR 70358) to make conforming changes to the regulations to reflect section 106(a) of the FCAA. This rule proposed to revise the definition of “item” under the CBP at 42 CFR 414.402 to exclude complex rehabilitative manual wheelchairs and certain other manual wheelchairs and related accessories when furnished in connection with such wheelchairs from the CBP as required by section 106(a) of the FCAA.Start Printed Page 42365
C. Provisions of the PPACA and the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) Affecting the IRF PPS in FY 2012 and Beyond
The Patient Protection and Affordable Care Act (PPACA) (Pub. L. 111-148) was enacted on March 23, 2010. The Health Care and Education Reconciliation Act of 2010 (Pub. L. 111-152), which amended and revised several provisions of the PPACA, was enacted on March 30, 2010. In this final rule, we refer to the two statutes collectively as the “Patient Protection and Affordable Care Act” or “PPACA”.
The PPACA included several provisions that affect the IRF PPS in FYs 2012 and beyond. In addition to what was previously discussed, section 3401(d) of the PPACA also added section 1886(j)(3)(C)(ii)(I) of the Act (providing for a “productivity adjustment” for FY 2012 and each subsequent FY). The productivity adjustment for FY 2022 is discussed in section VI.B. of this final rule. Section 1886(j)(3)(C)(ii)(II) of the Act provides that the application of the productivity adjustment to the market basket update may result in an update that is less than 0.0 for a FY and in payment rates for a FY being less than such payment rates for the preceding FY.
Sections 3004(b) of the PPACA and section 411(b) of the MACRA (Pub. L. 114-10, enacted on April 16, 2015) also addressed the IRF PPS. Section 3004(b) of PPACA reassigned the previously designated section 1886(j)(7) of the Act to section 1886(j)(8) of the Act and inserted a new section 1886(j)(7) of the Act, which contains requirements for the Secretary to establish a QRP for IRFs. Under that program, data must be submitted in a form and manner and at a time specified by the Secretary. Beginning in FY 2014, section 1886(j)(7)(A)(i) of the Act requires the application of a 2 percentage point reduction to the market basket increase factor otherwise applicable to an IRF (after application of paragraphs (C)(iii) and (D) of section 1886(j)(3) of the Act) for a FY if the IRF does not comply with the requirements of the IRF QRP for that FY. Application of the 2 percentage point reduction may result in an update that is less than 0.0 for a FY and in payment rates for a FY being less than such payment rates for the preceding FY. Reporting-based reductions to the market basket increase factor are not cumulative; they only apply for the FY involved. Section 411(b) of the MACRA amended section 1886(j)(3)(C) of the Act by adding paragraph (iii), which required us to apply for FY 2018, after the application of section 1886(j)(3)(C)(ii) of the Act, an increase factor of 1.0 percent to update the IRF prospective payment rates.
D. Operational Overview of the Current IRF PPS
As described in the FY 2002 IRF PPS final rule (66 FR 41316), upon the admission and discharge of a Medicare Part A fee-for-service (FFS) patient, the IRF is required to complete the appropriate sections of a Patient Assessment Instrument (PAI), designated as the IRF-PAI. In addition, beginning with IRF discharges occurring on or after October 1, 2009, the IRF is also required to complete the appropriate sections of the IRF-PAI upon the admission and discharge of each Medicare Advantage (MA) patient, as described in the FY 2010 IRF PPS final rule (74 FR 39762 and 74 FR 50712). All required data must be electronically encoded into the IRF-PAI software product. Generally, the software product includes patient classification programming called the Grouper software. The Grouper software uses specific IRF-PAI data elements to classify (or group) patients into distinct CMGs and account for the existence of any relevant comorbidities.
The Grouper software produces a five-character CMG number. The first character is an alphabetic character that indicates the comorbidity tier. The last four characters are numeric characters that represent the distinct CMG number. A free download of the Grouper software is available on the CMS website at http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/InpatientRehabFacPPS/Software.html. The Grouper software is also embedded in the internet Quality Improvement and Evaluation System (iQIES) User tool available in iQIES at https://www.cms.gov/medicare/quality-safety-oversight-general-information/iqies.
Once a Medicare Part A FFS patient is discharged, the IRF submits a Medicare claim as a Health Insurance Portability and Accountability Act of 1996 (HIPAA) (Pub. L. 104-191, enacted on August 21, 1996)-compliant electronic claim or, if the Administrative Simplification Compliance Act of 2002 (ASCA) (Pub. L. 107-105, enacted on December 27, 2002) permits, a paper claim (a UB-04 or a CMS-1450 as appropriate) using the five-character CMG number and sends it to the appropriate Medicare Administrative Contractor (MAC). In addition, once a MA patient is discharged, in accordance with the Medicare Claims Processing Manual, chapter 3, section 20.3 (Pub. L. 100-04), hospitals (including IRFs) must submit an informational-only bill (type of bill (TOB) 111), which includes Condition Code 04 to their MAC. This will ensure that the MA days are included in the hospital's Supplemental Security Income (SSI) ratio (used in calculating the IRF LIP adjustment) for FY 2007 and beyond. Claims submitted to Medicare must comply with both ASCA and HIPAA.
Section 3 of the ASCA amended section 1862(a) of the Act by adding paragraph (22), which requires the Medicare program, subject to section 1862(h) of the Act, to deny payment under Part A or Part B for any expenses for items or services for which a claim is submitted other than in an electronic form specified by the Secretary. Section 1862(h) of the Act, in turn, provides that the Secretary shall waive such denial in situations in which there is no method available for the submission of claims in an electronic form or the entity submitting the claim is a small provider. In addition, the Secretary also has the authority to waive such denial in such unusual cases as the Secretary finds appropriate. For more information, see the “Medicare Program; Electronic Submission of Medicare Claims” final rule (70 FR 71008). Our instructions for the limited number of Medicare claims submitted on paper are available at http://www.cms.gov/manuals/downloads/clm104c25.pdf.
Section 3 of the ASCA operates in the context of the administrative simplification provisions of HIPAA, which include, among others, the requirements for transaction standards and code sets codified in 45 CFR part 160 and part 162, subparts A and I through R (generally known as the Transactions Rule). The Transactions Rule requires covered entities, including covered healthcare providers, to conduct covered electronic transactions according to the applicable transaction standards. (See the CMS program claim memoranda at http://www.cms.gov/ElectronicBillingEDITrans/ and listed in the addenda to the Medicare Intermediary Manual, Part 3, section 3600).
The MAC processes the claim through its software system. This software system includes pricing programming called the “Pricer” software. The Pricer software uses the CMG number, along with other specific claim data elements and provider-specific data, to adjust the IRF's prospective payment for interrupted stays, transfers, short stays, and deaths, and then applies the applicable adjustments to account for the IRF's wage index, percentage of low-Start Printed Page 42366income patients, rural location, and outlier payments. For discharges occurring on or after October 1, 2005, the IRF PPS payment also reflects the teaching status adjustment that became effective as of FY 2006, as discussed in the FY 2006 IRF PPS final rule (70 FR 47880).
E. Advancing Health Information Exchange
The Department of Health and Human Services (HHS) has a number of initiatives designed to encourage and support the adoption of interoperable health information technology and to promote nationwide health information exchange to improve health care and patient access to their health information.
To further interoperability in post-acute care settings, CMS and Office of the National Coordinator for Health Information Technology (ONC) participate in the Post-Acute Care Interoperability Workgroup (PACIO) (https://pacioproject.org/) to facilitate collaboration with industry stakeholders to develop FHIR standards. These standards could support the exchange and reuse of patient assessment data derived from the minimum data set (MDS), inpatient rehabilitation facility patient assessment instrument (IRF-PAI), long term care hospital continuity assessment record and evaluation (LCDS), outcome and assessment information set (OASIS), and other sources. The PACIO Project has focused on FHIR implementation guides for functional status, cognitive status and new use cases on advance directives and speech, and language pathology. We encourage post-acute care (PAC) provider and health IT vendor participation as these efforts advance.
The CMS Data Element Library (DEL) continues to be updated and serves as the authoritative resource for PAC assessment data elements and their associated mappings to health IT standards such as Logical Observation Identifiers Names and Codes (LOINC) and Systematized Nomenclature of Medicine Clinical Terms (SNOMED). The DEL furthers CMS' goal of data standardization and interoperability. When combined with digital information systems that capture and maintain these coded elements, their standardized clinical content can reduce provider burden by supporting exchange of standardized healthcare data; supporting provider exchange of electronic health information for care coordination, person-centered care; and supporting real-time, data driven, clinical decision making. Standards in the Data Element Library (https://del.cms.gov/DELWeb/pubHome) can be referenced on the CMS website and in the ONC Interoperability Standards Advisory (ISA). The 2021 ISA is available at https://www.healthit.gov/isa.
The 21st Century Cures Act (Cures Act) (Pub. L. 114-255, enacted on December 13, 2016) requires HHS to take new steps to enable the electronic sharing of health information ensuring interoperability for providers and settings across the care continuum. The Cures Act includes a trusted exchange framework and common agreement (TEFCA) provision [4] that will enable the nationwide exchange of electronic health information across health information networks and provide an important way to enable bi-directional health information exchange in the future. For more information on current developments related to TEFCA, we refer readers to https://www.healthit.gov/topic/interoperability/trusted-exchange-framework-and-common-agreement and https://rce.sequoiaproject.org/.
The ONC final rule entitled, “21st Century Cures Act: Interoperability, Information Blocking, and the ONC Health IT Certification Program” final rule (85 FR 25642) published in the May 1, 2020 Federal Register (hereinafter “ONC Cures Act Final Rule”) implemented policies related to information blocking required under section 4003 of the 21st Century Cures Act. Information blocking is generally defined as a practice by a health IT developer of certified health IT, health information network, health information exchange, or health care provider that, except as required by law or specified by the Secretary of Health and Human Services (HHS) as a reasonable and necessary activity, is likely to interfere with access, exchange, or use of electronic health information. The definition of information blocking includes a knowledge standard, which is different for health care providers than for health IT developers of certified health IT and health information networks or health information exchanges. A healthcare provider must know that the practice is unreasonable as well as likely to interfere with access, exchange, or use of electronic health information. To deter information blocking, health IT developers of certified health IT, health information networks and health information exchanges whom the HHS Inspector General determines, following an investigation, have committed information blocking, are subject to civil monetary penalties of up to $1 million per violation. Appropriate disincentives for health care providers need to be established by the Secretary through rulemaking. Stakeholders can learn more about information blocking at https://www.healthit.gov/curesrule/final-rule-policy/information-blocking. ONC has posted information resources including fact sheets (https://www.healthit.gov/curesrule/resources/fact-sheets),, frequently asked questions (https://www.healthit.gov/curesrule/resources/information-blocking-faqs), and recorded webinars (https://www.healthit.gov/curesrule/resources/webinars).
We invited providers to learn more about these important developments and how they are likely to affect IRFs.
III. Summary of Provisions of the Proposed Rule
In the FY 2022 IRF PPS proposed rule, we proposed to update the IRF PPS for FY 2022 and the IRF QRP for FYs 2022 and 2023.
The proposed policy changes and updates to the IRF prospective payment rates for FY 2022 are as follows:
- Update the CMG relative weights and average length of stay values for FY 2022, in a budget neutral manner, as discussed in section IV. of the FY 2022 IRF PPS proposed rule (86 FR 19086, 19090 through 19095).
- Update the IRF PPS payment rates for FY 2022 by the market basket increase factor, based upon the most current data available, with a productivity adjustment required by section 1886(j)(3)(C)(ii)(I) of the Act, as described in section V. of the FY 2022 IRF PPS proposed rule (86 FR 19086, 19095 through 19096).
- Update the FY 2022 IRF PPS payment rates by the FY 2022 wage index and the labor-related share in a budget-neutral manner, as discussed in section V. of the FY 2022 IRF PPS proposed rule (86 FR 19086, 19096 through 19098).
- Describe the calculation of the IRF standard payment conversion factor for FY 2022, as discussed in section V. of the FY 2022 IRF PPS proposed rule (86 FR 19086, 19098 through 19099).
- Update the outlier threshold amount for FY 2022, as discussed in section VI. of the FY 2022 IRF PPS proposed rule (86 FR 19086, 19102 through 19103).
- Update the cost-to-charge ratio (CCR) ceiling and urban/rural average CCRs for FY 2022, as discussed in Start Printed Page 42367section VI. of the FY 2022 IRF PPS proposed rule (86 FR 19086, 19103).
We also proposed policy changes and updates to the IRF QRP for FYs 2022 and 2023 as follows:
- Updates to quality measures and reporting requirements under the IRF QRP, as well as requests for information discussed in section VII. of the FY 2022 IRF PPS proposed rule (86 FR 19086, 19103 through 19116).
In a separate 2018 interim final rule with comment period (IFC), entitled “Medicare Program; Durable Medical Equipment Fee Schedule Adjustments To Resume the Transitional 50/50 Blended Rates To Provide Relief in Rural Areas and Non-Contiguous Areas” (hereinafter 2018 interim final rule), we:
- Excluded accessories furnished in connection with group 3 or higher complex rehabilitative power wheelchairs from fee schedule adjustments based on payments determined under the DMEPOS CBP (83 FR 21912 through 21925). In a 2021 notice of continuation, we announced the continuation of effectiveness of the 2018 interim final rule and the extension of the timeline for publication of the final rule (86 FR 21949).
Finally, in a separate proposed rule published on November 4, 2020, entitled “Medicare Program; Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) Policy Issues and Level II of the Healthcare Common Procedure Coding System (HCPCS),” we:
- Proposed to make changes to the definition of “item” at 42 CFR 414.402 to reflect that complex rehabilitative manual wheelchairs, certain other manual wheelchairs, and accessories furnished in connection with these wheelchairs are excluded from the DMEPOS CBP by section 106(a) of the FCAA (85 FR 70405). This is a conforming change to the regulations to implement section 106(a) of the FCAA. We are finalizing this change to 42 CFR 414.402 as part of this final rule.
IV. Analysis of and Responses to Public Comments
A. FY 2022 IRF PPS Proposed Rule
In response to the FY 2022 IRF PPS proposed rule (86 FR 19086), we received 50 timely responses from the public. We received comments from various trade associations, inpatient rehabilitation facilities, individual physicians, therapists, clinicians, health care industry organizations, and health care consulting firms. The following sections, arranged by subject area, include a summary of the public comments that we received, and our responses.
B. 2018 Interim Final Rule
The 2018 interim final rule (83 FR 21912) included changes in fee schedule adjustments for accessories (including seating systems) and seat and back cushions furnished in connection with group 3 or higher complex rehabilitative power wheelchairs. We received 5 timely responses from wheelchair suppliers, manufacturers, and a patient advocacy organization related to fee schedule adjustments for accessories (including seating systems) and seat and back cushions furnished in connection with complex rehabilitative wheelchairs.
C. DMEPOS/HCPCS Proposed Rule
The November 2020 proposed rule (85 FR 70358) included a provision to revise the definition of “item” under the CBP at 42 CFR 414.402 to exclude complex rehabilitative manual wheelchairs, certain other manual wheelchairs and accessories furnished in connection with these wheelchairs from the DMEPOS CBP. We received 11 timely responses from wheelchair suppliers, manufacturers, and a national coalition of consumers and clinicians regarding excluding complex rehabilitative manual wheelchairs, certain other manual wheelchairs and related accessories furnished in connection with these wheelchairs from the CBP.
V. Update to the Case-Mix Group (CMG) Relative Weights and Average Length of Stay (ALOS) Values for FY 2022
As specified in § 412.620(b)(1), we calculate a relative weight for each CMG that is proportional to the resources needed by an average inpatient rehabilitation case in that CMG. For example, cases in a CMG with a relative weight of 2, on average, will cost twice as much as cases in a CMG with a relative weight of 1. Relative weights account for the variance in cost per discharge due to the variance in resource utilization among the payment groups, and their use helps to ensure that IRF PPS payments support beneficiary access to care, as well as provider efficiency.
We proposed to update the CMG relative weights and ALOS values for FY 2022. Typically, we use the most recent available data to update the CMG relative weights and average lengths of stay. As such, section 1886(j) of the Act confers broad statutory authority upon the Secretary to propose refinements to the IRF PPS. For FY 2022, we proposed to use the FY 2020 IRF claims and FY 2019 IRF cost report data. These data are the most current and complete data available at this time. Currently, only a small portion of the FY 2020 IRF cost report data are available for analysis, but the majority of the FY 2020 IRF claims data are available for analysis. We also proposed that if more recent data become available after the publication of the proposed rule and before the publication of the final rule, we would use such data to determine the FY 2022 CMG relative weights and ALOS values in the final rule.
We proposed to apply these data using the same methodologies that we have used to update the CMG relative weights and ALOS values each FY since we implemented an update to the methodology. The detailed CCR data from the cost reports of IRF provider units of primary acute care hospitals is used for this methodology, instead of CCR data from the associated primary care hospitals, to calculate IRFs' average costs per case, as discussed in the FY 2009 IRF PPS final rule (73 FR 46372). In calculating the CMG relative weights, we use a hospital-specific relative value method to estimate operating (routine and ancillary services) and capital costs of IRFs. The process to calculate the CMG relative weights for this final rule is as follows:
Step 1. We estimate the effects that comorbidities have on costs.
Step 2. We adjust the cost of each Medicare discharge (case) to reflect the effects found in the first step.
Step 3. We use the adjusted costs from the second step to calculate CMG relative weights, using the hospital-specific relative value method.
Step 4. We normalize the FY 2022 CMG relative weights to the same average CMG relative weight from the CMG relative weights implemented in the FY 2021 IRF PPS final rule (85 FR 48424).
Consistent with the methodology that we have used to update the IRF classification system in each instance in the past, we proposed to update the CMG relative weights for FY 2022 in such a way that total estimated aggregate payments to IRFs for FY 2022 are the same with or without the changes (that is, in a budget-neutral manner) by applying a budget neutrality factor to the standard payment amount. We note that, as we typically do, we updated our data between the FY 2022 IRF PPS proposed and final rules to ensure that we use the most recent available data in calculating IRF PPS payments. This updated data reflects a more complete set of claims for FY 2020 and additional cost report data for FY 2019. To calculate the appropriate Start Printed Page 42368budget neutrality factor for use in updating the FY 2022 CMG relative weights, we use the following steps:
Step 1. Calculate the estimated total amount of IRF PPS payments for FY 2022 (with no changes to the CMG relative weights).
Step 2. Calculate the estimated total amount of IRF PPS payments for FY 2022 by applying the changes to the CMG relative weights (as discussed in this final rule).
Step 3. Divide the amount calculated in step 1 by the amount calculated in step 2 to determine the budget neutrality factor of 1.0005 that would maintain the same total estimated aggregate payments in FY 2022 with and without the changes to the CMG relative weights.
Step 4. Apply the budget neutrality factor from step 3 to the FY 2022 IRF PPS standard payment amount after the application of the budget-neutral wage adjustment factor.
In section VI.E. of this final rule, we discuss the use of the existing methodology to calculate the standard payment conversion factor for FY 2022.
In Table 2, “Relative Weights and Average Length of Stay Values for Case-Mix Groups,” we present the CMGs, the comorbidity tiers, the corresponding relative weights, and the ALOS values for each CMG and tier for FY 2022. The ALOS for each CMG is used to determine when an IRF discharge meets the definition of a short-stay transfer, which results in a per diem case level adjustment.
Start Printed Page 42369
Start Printed Page 42370
Start Printed Page 42371
Start Printed Page 42372

Generally, updates to the CMG relative weights result in some increases and some decreases to the CMG relative weight values. Table 2 shows how we estimate that the application of the revisions for FY 2022 would affect particular CMG relative weight values, which would affect the overall distribution of payments within CMGs and tiers. We note that, because we implement the CMG relative weight revisions in a budget-neutral manner (as previously described), total estimated aggregate payments to IRFs for FY 2022 are not affected as a result of the CMG relative weight revisions. However, the revisions affect the distribution of payments within CMGs and tiers.

As shown in Table 3, 97.2 percent of all IRF cases are in CMGs and tiers that would experience less than a 5 percent change (either increase or decrease) in the CMG relative weight value as a result of the revisions for FY 2022. The changes in the ALOS values for FY 2022, compared with the FY 2021 ALOS values, are small and do not show any particular trends in IRF length of stay patterns.
The comments we received on our proposed updates to the CMG relative weights and ALOS values for FY 2022 and our responses are summarized below.
Comment: Several commenters supported the proposed updates to the CMG relative weights and ALOS values using the latest available data (the FY 2020 claims and FY 2019 cost report data). These commenters noted that applying Functional Independence MeasureTM (FIMTM)-based FY 2019 claims data in FY 2022 will not reflect effects of numerous changes that occurred during the COVID-19 PHE. These changes include enhanced use of personal protective equipment (PPE), increased staffing costs, COVID-19 testing for staff and patients, and other infection control protocols, to name just a few examples. However, the commenters requested more details of the analysis for determining how the COVID-19-related claims affect the relative weight and ALOS calculations.
Response: We appreciate the commenters' support for the proposed updates. The annual updates to the CMG relative weights, which include both increases and decreases to the CMG relative weights, are intended to ensure that IRF payments are aligned as closely as possible with the current costs of care. The relative weights for each of the CMGs and tiers represent the relative costliness of patients in those CMGs and tiers compared with patients in other CMGs and tiers. Using FY 2020 claims data does not result in significantly different CMG relative weight values than the relative weight values obtained using FY 2019 claims data. The relative weight budget neutrality factor would be 1.0005 using FY 2020 claims in comparison to 0.9998 using FY 2019 claims.
Additionally, with regard to providing additional analysis of the ALOS values, we found that the variation in the ALOS values between FY 2019 and FY 2020 was similar to the year-to-year fluctuations in these values that we typically see. In addition, we note that a decline in ALOS values, which the commenter expresses concern about, would actually have the effect of slightly increasing IRF PPS payments to providers, as more patients would qualify for full IRF PPS payments instead of reduced short-stay transfer payments, and the reduced short-stay transfer payments would be slightly higher (because we divide by the ALOS values in calculating the short-stay transfer per diem payment amounts). We note, also, that changes in ALOS values have no effect on IRF coverage, as these values are not used in determining coverage of IRF claims. In the IRF PPS, ALOS values are only used in determining which cases qualify for the short-stay transfer policy. Thus, we believe that the ALOS values that we are finalizing in this final rule are appropriate and will not result in any unintended consequences.
As stated in the FY 2022 IRF PPS proposed rule, the FY 2020 claims data is the most current and complete data available for updating payments. As most recently discussed in detail in the FY 2021 IRF PPS final rule (85 FR 48424), we believe that these data Start Printed Page 42373accurately reflect the severity of the IRF patient population and the associated costs of caring for these patients in the IRF setting. We believe using the FY 2020 claims-based calculation reflects as accurately as possible the current costs of care in IRFs. Therefore, we believe it is appropriate to use the FY 2020 claims data to update the CMG relative weights and ALOS values for FY 2022 to ensure the case mix system is as reflective as possible of recent changes in IRF utilization and case mix. With regard to the additional request for further analysis to be provided on the use of FY 2020 claims data, CMS examined the relative weight values calculated both including and excluding cases associated with a COVID-19 ICD-10 diagnosis code. This analysis indicated that for the majority of CMGs relative weight values would change by less than 1 percent when such COVID cases were removed. In addition, we do not believe removing COVID-19 related claims from the analysis provides the best prediction of FY 2022 data because as most commenters said, we will likely still be seeing evidence of the PHE in the data for FY 2022.
Comment: Some commenters requested that CMS provide analyses of how the COVID-19 PHE would affect the IRF PPS payment rates in FY 2022. Some commenters suggested that, despite the progress being made with vaccinations and other infection control efforts, IRFs are likely to continue to treat COVID-19 survivors as well as “Long COVID” patients for the foreseeable future.
Response: We appreciate the commenters' suggestions and will consider providing additional analyses in future rule updates. However, we agree with most commenters, that we will be seeing evidence of the PHE in the data for FY 2022 and beyond. We believe future evaluation and impact from the PHE will generate a more robust data set for analysis giving greater insight on IRF impacts as they relate to CMG relative weights.
Comment: A few commenters stated CMS should evaluate and incorporate adjustments to the FY 2020 data for any major reductions in volumes and surgical admissions due to the PHE, which they stated resulted in a significantly different case mix from a normal year. The commenters recommended that CMS should use a blended approach (that is, blending the relative weights obtained using the FY 2019 and FY 2020 data) in determining the relative weight updates, which may mean that a larger payment increase is warranted.
Response: We appreciate the commenters' suggestions regarding changes to the methodology used to establish the CMG relative weights for the IRF PPS payments. We will continue to monitor the CMG relative weight updates to ensure that they continue to compensate IRFs appropriately. However, we disagree that a blended approach would result in the most accurate CMG relative weights, as this blended approach would not fully reflect the most recent available data (the FY 2020 IRF claims data). We believe the utilization of the FY 2020 claims data accurately reflects the severity of the IRF patient population and the associated costs of caring for these patients in the IRF setting.
Comment: One commenter expressed concerns about the underlying construction of the CMGs, specifically the commenter stated that the proposed adjustments neither account for newer coding practices nor provide adequate coverage and payment for severe patients who benefit from IRF services, thus leading to CMS relative weights and ALOS values that do not reflect current clinical practice. The commenter expressed particular concern that CMS proposed to reduce the relative weight values for patients with a stroke, traumatic brain injury, and traumatic spinal cord injury. The commenter stated that the proposed updates would decrease the relative weights for 18 of the 24 stroke CMGs, 19 of the 20 traumatic brain injury CMGs, and 16 of the 28 traumatic spinal cord injury CMGs.
Response: CMG relative weights are updated in a budget neutral manner, thus leading to increases in some relative weights and corresponding decreases in other CMG relative weights. We have carefully examined all of the decreases and increases in the CMG relative weights for FY 2022, and we believe that these changes accurately reflect our best estimates of the relative costs of caring for different types of patients in the IRF in FY 2022. As the commenter notes, the relative weights in the stroke, traumatic brain injury, and traumatic spinal cord injury conditions included both increases and decreases, and the variation for FY 2022 is similar to the typical year-to-year variation that we observe. The increases and decreases also appear to be related to severity, with the increases concentrated in the CMGs for more severe patients and the decreases concentrated in the CMGs for less severe patients. We believe that this is appropriate and reflects the most current and complete information that we have for estimating the FY 2022 relative costs of care.
Therefore, we believe that these updates more closely align IRF PPS payments with the costs of caring for different types of patients, and more closely align the average lengths of stay with the actual lengths of stay for patients in the various CMGs. As indicated previously, the magnitude of the updates for FY 2022 is similar to the changes we see in a typical year.
Regarding the updates to “new coding practices”, we are not certain what the commenter means, but if, as we suspect, they may be referring to the changes in the CMGs and the data used to assign those CMGs, then our analysis indicates the FY 2020 IRF claims and the FY 2019 IRF cost report data provides the best available data for setting the CMS relative weights for FY 2022.
After consideration of the comments we received, we are finalizing our proposal to update the CMG relative weights and ALOS values for FY 2022, as shown in Table 2 of this final rule. These updates are effective for FY 2022, that is, for discharges occurring on or after October 1, 2021 and on or before September 30, 2022.
VI. FY 2022 IRF PPS Payment Update
A. Background
Section 1886(j)(3)(C) of the Act requires the Secretary to establish an increase factor that reflects changes over time in the prices of an appropriate mix of goods and services for which payment is made under the IRF PPS. According to section 1886(j)(3)(A)(i) of the Act, the increase factor shall be used to update the IRF prospective payment rates for each FY. Section 1886(j)(3)(C)(ii)(I) of the Act requires the application of the productivity adjustment described in section 1886(b)(3)(B)(xi)(II) of the Act. Thus, in the FY 2022 IRF PPS proposed rule, we proposed to update the IRF PPS payments for FY 2022 by a market basket increase factor as required by section 1886(j)(3)(C) of the Act based upon the most current data available, with a productivity adjustment as required by section 1886(j)(3)(C)(ii)(I) of the Act.
We have utilized various market baskets through the years in the IRF PPS. For a discussion of these market baskets, we refer readers to the FY 2016 IRF PPS final rule (80 FR 47046).
In FY 2016, we finalized the use of a 2012-based IRF market basket, using Medicare cost report (MCR) data for both freestanding and hospital-based IRFs (80 FR 47049 through 47068). Beginning with FY 2020, we finalized a rebased and revised IRF market basket to reflect a 2016 base year. The FY 2020 Start Printed Page 42374IRF PPS final rule (84 FR 39071 through 39086) contains a complete discussion of the development of the 2016-based IRF market basket.
B. FY 2022 Market Basket Update and Productivity Adjustment
For FY 2022 (that is, beginning October 1, 2021 and ending September 30, 2022), we proposed to update the IRF PPS payments by a market basket increase factor as required by section 1886(j)(3)(C) of the Act, with a productivity adjustment as required by section 1886(j)(3)(C)(ii)(I) of the Act. For FY 2022, we proposed to use the same methodology described in the FY 2021 IRF PPS final rule (85 FR 48432 through 48433), with one proposed modification to the 2016-based IRF market basket.
For the price proxy for the For-profit Interest cost category of the 2016-based IRF market basket, we proposed to use the iBoxx AAA Corporate Bond Yield index instead of the Moody's AAA Corporate Bond Yield index. Effective for December 2020, the Moody's AAA Corporate Bond series is no longer available for use under license to IHS Global Inc. (IGI), the nationally-recognized economic and financial forecasting firm with which we contract to forecast the components of the market baskets and multi-factor productivity (MFP). Since IGI is no longer licensed to use and publish the Moody's series, IGI was required to discontinue the publication of the associated historical data and forecasts of this series. Therefore, IGI constructed a bond yield index (iBoxx) that closely replicates the Moody's corporate bond yield indices currently used in the market baskets.
In the FY 2022 IRF PPS proposed rule, we stated that because the iBoxx AAA Corporate Bond Yield index captures the same technical concept as the current corporate bond proxy and tracks similarly to the current measure that is no longer available, we believed that the iBoxx AAA Corporate Bond Yield index is technically appropriate to use in the 2016-based IRF market basket.
Consistent with historical practice, we proposed to estimate the market basket update for the IRF PPS for FY 2022 based on IGI's forecast using more recent available data. Based on IGI's fourth quarter 2020 forecast with historical data through the third quarter of 2020, the proposed 2016-based IRF market basket increase factor for FY 2022 was projected to be 2.4 percent. We also proposed that if more recent data became available after the publication of the proposed rule and before the publication of this final rule (for example, a more recent estimate of the market basket update or MFP), we would use such data, if appropriate, to determine the FY 2022 market basket update in this final rule.
According to section 1886(j)(3)(C)(i) of the Act, the Secretary shall establish an increase factor based on an appropriate percentage increase in a market basket of goods and services. Section 1886(j)(3)(C)(ii) of the Act then requires that, after establishing the increase factor for a FY, the Secretary shall reduce such increase factor for FY 2012 and each subsequent FY, by the productivity adjustment described in section 1886(b)(3)(B)(xi)(II) of the Act. Section 1886(b)(3)(B)(xi)(II) of the Act sets forth the definition of this productivity adjustment. The statute defines the productivity adjustment to be equal to the 10-year moving average of changes in annual economy-wide, private nonfarm business MFP (as projected by the Secretary for the 10-year period ending with the applicable FY, year, cost reporting period, or other annual period) (the “productivity adjustment”). The U.S. Department of Labor's Bureau of Labor Statistics (BLS) publishes the official measure of private nonfarm business MFP. Please see http://www.bls.gov/mfp for the BLS historical published MFP data. A complete description of the MFP projection methodology is available on the CMS website at https://www.cms.gov/Research-Statistics-Dataand-Systems/Statistics-Trends-andReports/MedicareProgramRatesStats/MarketBasketResearch.html. We note that effective with FY 2022 and forward, CMS is changing the name of this adjustment to refer to it as the productivity adjustment rather than the MFP adjustment. We note that this is not a change in policy as the methodology for deriving the adjustment relies on the same underlying data and methodology. This change in terminology results in a title more consistent with the statutory language described in section 1886(j)(3)(C)(ii) of the Act.
Using IGI's fourth quarter 2020 forecast, the 10-year moving average growth of MFP for FY 2022 was projected to be 0.2 percent. Thus, in accordance with section 1886(j)(3)(C) of the Act, we proposed to base the FY 2022 market basket update, which is used to determine the applicable percentage increase for the IRF payments, on IGI's fourth quarter 2020 forecast of the 2016-based IRF market basket. We proposed to then reduce this percentage increase by the estimated productivity adjustment for FY 2022 of 0.2 percentage point (the 10-year moving average growth of MFP for the period ending FY 2022 based on IGI's fourth quarter 2020 forecast). Therefore, the proposed FY 2022 IRF update was equal to 2.2 percent (2.4 percent market basket update reduced by the 0.2 percentage point productivity adjustment).
Furthermore, we proposed that if more recent data became available after the publication of the proposed rule and before the publication of this final rule (for example, a more recent estimate of the market basket and/or MFP), we would use such data, if appropriate, to determine the FY 2022 market basket update and productivity adjustment in this final rule.
Based on the more recent data available for this FY 2022 IRF final rule (that is, IGI's second quarter 2021 forecast of the 2016-based IRF market basket with historical data through the first quarter of 2021), we estimate that the IRF FY 2022 market basket update is 2.6 percent. Based on the more recent data available from IGI's second quarter 2021 forecast, the current estimate of the productivity adjustment for FY 2022 is 0.7 percentage point. Therefore, the current estimate of the FY 2022 IRF increase factor is equal to 1.9 percent (2.6 percent market basket update reduced by 0.7 percentage point productivity adjustment).
For FY 2022, the Medicare Payment Advisory Commission (MedPAC) recommends that we reduce IRF PPS payment rates by 5 percent. As discussed, and in accordance with sections 1886(j)(3)(C) and 1886(j)(3)(D) of the Act, the Secretary proposed to update the IRF PPS payment rates for FY 2022 by a productivity-adjusted IRF market basket increase factor of 2.2 percent. Based on more recent data, the current estimate of the productivity-adjusted IRF market basket increase factor is 1.9 percent. Section 1886(j)(3)(C) of the Act does not provide the Secretary with the authority to apply a different update factor to IRF PPS payment rates for FY 2022.
We invited public comment on our proposals for the FY 2022 market basket update and productivity adjustment. The following is a summary of the public comments received on the proposed FY 2022 market basket update and productivity adjustment and our responses:
Comment: One commenter supported the change to the iBoxx AAA Corporate Bond Yield index for use in the IRF market basket price proxy for the For-profit interest cost category in lieu of the Moody's AAA Corporate Bond Yield Index that is no longer available.Start Printed Page 42375
Response: We appreciate the commenter's support of the use of the iBoxx AAA Corporate Bond Yield index as the replacement price proxy for the for-profit interest cost category in the 2016-based IRF market basket.
Comment: A few commenters noted their appreciation for the proposed increase in IRF payments as a result of the productivity-adjusted market basket update. Several commenters supported CMS continuing to update the market basket and productivity factor using the latest available data in the IRF PPS final rule.
Response: We appreciate the commenters' support for the use of the productivity-adjusted market basket to annually update IRF PPS payments. As proposed, we are using the latest available data to determine the FY 2022 IRF market basket update and productivity adjustment.
Comment: Several commenters expressed concern that the impact of the PHE due to COVID-19 is not factored into the payment rate update. One commenter stated that the PHE has required and continues to require IRFs to increase their labor costs through increased use of contract labor; incurrence of substantial additional paid time off for nurses and therapists who have contracted COVID-19 or been quarantined due to potential exposure to this disease; increased operating costs related to purchases of additional PPE; increases in purchases of other supply costs; and increased costs of cleaning supplies, among other cost increases. The commenters also stated that while many of these new or increased costs will likely extend into FY 2022, the current market basket update factors do not have these costs embedded into the underlying payment rate update. Commenters encouraged CMS to consider these factors and embed an additional update to account for this added cost to IRFs. Another commenter stated that while they appreciate the modest increase to the IRF payment rate, they believe it is insufficient to offset the negative financial impact of cost inflation and the COVID-19 pandemic and encouraged CMS to consider additional funding opportunities in the final rule. One commenter requested that CMS measure the impacts of COVID-19 and include them in the analysis for the final IRF rule.
Response: For this final rule, we have incorporated more recent historical data and forecasts provided by IGI to capture the price and wage pressures facing IRFs. By incorporating the more recent estimates available of the market basket update and productivity adjustment, we believe these data reflect the best available projection of input price inflation faced by IRFs for FY 2022, adjusted for economy-wide productivity, which is required by statute.
The current IRF market basket cost weights are based on Medicare cost report data from 2016. Typically, a market basket is rebased every 4 to 5 years. However, we continually monitor the cost weights in the market baskets to ensure they are reflecting the mix of inputs used in providing services. We do not yet have cost report data available to determine the impact of COVID-19 on IRF cost structures. When complete Medicare cost report data covering the full impact of the PHE become available, we plan to review this information for future rulemaking. Any future rebasing or revising of the IRF market basket will be proposed and subject to public comments in future rulemaking.
While the update factor for IRFs for FY 2022 use data that reflect the best available projection of input price inflation faced by IRFs, we acknowledge the commenters' concern that the rate update may not reflect certain additional costs incurred during the COVID-19 PHE. However, we note that Medicare providers, may be eligible for payments from the Provider Relief Fund (as authorized by Division B, Title VIII of the CARES Act, Division B, Title I of the Paycheck Protection Program and Health Care Enhancement Act (Pub. L. 116-139, enacted April 24, 2020), and Division M Title III of the Consolidated Appropriations Act, 2021 (Pub. L. 116-260, enacted December 27, 2020) or the American Rescue Plan Act (ARPA) Rural Distribution (as authorized by section 9911 of the American Rescue Plan Act of 2021) (Pub. L. 117-2, enacted March 11, 2021) to cover health-care related expenses and lost revenues attributed to COVID-19. The total appropriation for the Provider Relief Fund is $178 billion. These payments are intended to help healthcare providers respond to the productivity losses and extra expenses caused by the PHE.
IRFs are eligible to apply for reimbursement for providing COVID-19 testing, treatment, or vaccine administration to uninsured people. These payments are available from the COVID-19 Claims Reimbursement to Health Care Providers and Facilities for Testing, Treatment and Vaccine Administration for the Uninsured Program (additional information about the Uninsured Program can be found at https://www.hrsa.gov/coviduninsuredclaim). IRFs are also eligible to apply to the HRSA COVID-19 Coverage Assistance Fund (CAF) for reimbursement for administering COVID-19 vaccines to underinsured individuals, defined as those whose health plan either does not cover vaccines, or covers them with patient cost-sharing (additional information about the CAF can be found at https://www.hrsa.gov/covid19-coverage-assistance.)
In accordance with statutory requirements, the Provider Relief Fund and ARPA Rural payments may not be used to reimburse expenses or losses that have been reimbursed from other sources or that other sources are obligated to reimburse. Likewise, we do not believe that it is appropriate to account for PHE-related costs in our IRF rate setting to the extent that such costs were actually reimbursed by the Provider Relief Fund or may be reimbursed by the ARPA Rural Distribution program.
Comment: One commenter expressed concerns about the continued application of the productivity adjustment to IRFs. The commenter also stated that while it understands that CMS is bound by statute to reduce the market basket update by a productivity adjustment factor in accordance with the ACA, it remains concerned that IRFs will not have the ability to generate additional productivity gains at a pace matching the productivity of the economy at large on an ongoing, consistent basis as contemplated by the ACA. The commenter further stated that recent developments related to the PHE due to COVID-19 have resulted in further productivity challenges for IRFs and a loss of productivity efficiencies. The commenter stated that hospitals have been impacted by the additional costs and administrative processes associated with the PHE and various guidance and requirements issued by federal, state, and local health authorities arising as a result of it, such as—but by no means limited to—screening or testing of all employees, visitors, and vendors coming through the doors for COVID-19; revamping housekeeping processes and schedules; increased provision of in-room therapy; reorienting the patients and employees to new food/meal service processes, which includes in-room only meals for patients; the clinical inefficiencies of donning and doffing of PPE; the quarantining of employees with known or possible detection of COVID-19; purchasing of in-house COVID-19 testing devices; and the tracking and reporting of COVID-19 cases, tests, and vaccines administered, among other reporting requirements. The commenter Start Printed Page 42376stated that it is not clear when or whether these and other process changes will end. The commenter further stated that the PHE has caused disruption to staffing efficiencies, required staff to quarantine, and required them to alter their treatment patterns to care for COVID-19 positive patients. They noted that the PHE has underscored the concern that year-over-year productivity gains are unattainable and do not track with actual IRF operational experience. The commenter requested CMS monitor the impact that the productivity adjustments will have on the rehabilitation hospital sector and provide feedback to Congress as appropriate, and reduce the productivity adjustment.
Response: As the commenter acknowledged, section 1886(j)(3)(C)(ii)(I) of the Act requires the application of a productivity adjustment to the IRF PPS market basket increase factor. In response to the commenter's request to reduce the productivity adjustment, we note that we are required by statute to use an economy-wide productivity measure to derive this productivity adjustment. The current projection of the productivity adjustment for FY 2022 is provided by an independent contractor, IGI, and reflects their recent expectations regarding the 10-year moving average growth in private nonfarm business MFP for the period ending FY 2022. As requested by the commenter, we will continue to monitor the impact of the payment updates on IRF Medicare payment adequacy as well as beneficiary access to care.
We also note that the Provider Relief Fund and ARPA Rural Distribution payments discussed above are intended to help providers, including IRFs, respond to additional expenses and productivity losses caused by the PHE. We do not believe that the COVID-19 expenses that the commenter discusses in any way alter CMS' responsibility to estimate and apply a multifactor productivity adjustment to the IRF increase factor, as required by section 1886(j)(3)(C)(ii)(I) of the Act.
As stated in the FY 2020 IRF PPS final rule (84 FR 39087) and the FY 2021 IRF PPS final rule (85 FR 48443), we would be interested in better understanding IRF-specific productivity, including any insights into available data at the level required to estimate IRF-specific multi-factor productivity that would allow this analysis.
Comment: Several commenters recommended that CMS continue to examine productivity factors for health care providers and hospitals and provide findings to Congress in order to implement a more appropriate, healthcare specific productivity adjustment. One commenter recommended that CMS recommend to Congress a more specific productivity adjustment that would properly reflect the nature of healthcare services, and in particular, hospital services.
Response: We have estimated hospital-sector multi-factor productivity and regularly publish updated findings at https://www.cms.gov/Research-Statistics-Data-and-Systems/Statistics-Trends-and-Reports/ReportsTrustFunds/Downloads/ProductivityMemo2016.pdf. As more recent data become available regarding hospital-sector productivity, we plan to continue updating these estimates and reporting this information on our website. In addition, we note that MedPAC annually monitors various factors for Medicare providers in terms of profitability and beneficiary access to care and reports the findings to Congress on an annual basis. In chapter 9 of its March 2021 report to Congress, MedPAC has recommended that payments to IRF facilities be reduced because the Commission determined that Medicare's current payment rates for IRFs appear to be more than adequate. As noted previously, section 1886(j)(3)(C)(ii)(I) of the Act requires the application of a productivity adjustment based on the economy-wide productivity measure to the IRF PPS market basket increase factor.
Comment: MedPAC commented that while it understands that CMS is required to implement the statutory payment update; it noted that MedPAC determined that Medicare's current payment rates for IRFs appear to be more than adequate and recommended that the Congress reduce the IRF payment rate by 5 percent for FY 2022.
Response: We are required to update IRF PPS payments by the market basket update adjusted for productivity, as directed by section 1886(j)(3)(C) of the Act. Any change to the productivity adjusted-market basket update would need to be made through legislation.
Comment: One commenter noted that FY 2021 was the second year in a row where MedPAC has recommended a decrease in payments and CMS did not accept the recommendation. The commenter stated that MedPAC's recommendation was flawed for several reasons. The commenter disagreed that the metrics utilizing case-mix groups (CMG) payments are site neutral since one for-profit company alone controls one third of the U.S. Medicare IRF market, resulting in statistical bias. The commenter also stated that the proposed rule, with regards to the proposed increase for payments to IRF providers, should be withdrawn and reconsidered.
Response: We appreciate the commenter's concern regarding the payment increase for IRFs; however, we do not have the statutory authority to implement MedPAC's recommendation. As discussed, and in accordance with sections 1886(j)(3)(C), the Secretary is updating IRF PPS payment rates for FY 2022 by an adjusted market basket increase factor of 1.9 percent, as section 1886(j)(3)(C) of the Act does not provide the Secretary with the authority to apply a different update factor to IRF PPS payment rates for FY 2022. The CMGs utilized under the IRF PPS were implemented in accordance with statute and incorporate case-level and facility-level adjustments to best align IRF prospective payments with the expected costs of treating patients in the IRF setting.
After consideration of the comments we received, we are finalizing a FY 2022 IRF update equal to 1.9 percent based on the most recent data available.
C. Labor-Related Share for FY 2022
Section 1886(j)(6) of the Act specifies that the Secretary is to adjust the proportion (as estimated by the Secretary from time to time) of IRFs' costs that are attributable to wages and wage-related costs, of the prospective payment rates computed under section 1886(j)(3) of the Act, for area differences in wage levels by a factor (established by the Secretary) reflecting the relative hospital wage level in the geographic area of the rehabilitation facility compared to the national average wage level for such facilities. The labor-related share is determined by identifying the national average proportion of total costs that are related to, influenced by, or vary with the local labor market. We proposed to continue to classify a cost category as labor-related if the costs are labor-intensive and vary with the local labor market.
Based on our definition of the labor-related share and the cost categories in the 2016-based IRF market basket, we proposed to calculate the labor-related share for FY 2022 as the sum of the FY 2022 relative importance of Wages and Salaries, Employee Benefits, Professional Fees: Labor-related, Administrative and Facilities Support Services, Installation, Maintenance, and Repair Services, All Other: Labor-related Services, and a portion of the Capital-Related relative importance from the 2016-based IRF market basket. For more details regarding the methodology for determining specific cost categories for inclusion in the 2016-based IRF labor-Start Printed Page 42377related share, see the FY 2020 IRF PPS final rule (84 FR 39087 through 39089).
The relative importance reflects the different rates of price change for these cost categories between the base year (2016) and FY 2022. Based on IGI's fourth quarter 2020 forecast of the 2016-based IRF market basket, the sum of the FY 2022 relative importance for Wages and Salaries, Employee Benefits, Professional Fees: Labor-related, Administrative and Facilities Support Services, Installation Maintenance & Repair Services, and All Other: Labor-related Services was 69.0 percent. We proposed that the portion of Capital-Related costs that are influenced by the local labor market is 46 percent. Since the relative importance for Capital-Related costs was 8.4 percent of the 2016-based IRF market basket for FY 2022, we proposed to take 46 percent of 8.4 percent to determine the labor-related share of Capital-Related costs for FY 2022 of 3.9 percent. Therefore, we proposed a total labor-related share for FY 2022 of 72.9 percent (the sum of 69.0 percent for the labor-related share of operating costs and 3.9 percent for the labor-related share of Capital-Related costs). We proposed that if more recent data became available after publication of the proposed rule and before the publication of this final rule (for example, a more recent estimate of the labor-related share), we would use such data, if appropriate, to determine the FY 2022 IRF labor-related share in the final rule.
Based on IGI's second quarter 2021 forecast of the 2016-based IRF market basket, the sum of the FY 2022 relative importance for Wages and Salaries, Employee Benefits, Professional Fees: Labor-related, Administrative and Facilities Support Services, Installation Maintenance & Repair Services, and All Other: Labor-related Services is 69.0 percent. Since the relative importance for Capital-Related costs is 8.4 percent of the 2016-based IRF market basket for FY 2022, we take 46 percent of 8.4 percent to determine the labor-related share of Capital-Related costs for FY 2022 of 3.9 percent. Therefore, the current estimate of the total labor-related share for FY 2022 is equal to 72.9 percent (the sum of 69.0 percent for the labor-related share of operating costs and 3.9 percent for the labor-related share of Capital-Related costs).
Table 4 shows the current estimate of the FY 2022 labor-related share and the FY 2021 final labor-related share using the 2016-based IRF market basket relative importance.

We invited public comment on the proposed labor-related share for FY 2022.
We did not receive any comments on the proposed revisions to the labor related share for FY 2022 and, therefore, we are finalizing the use of the sum of the FY 2022 relative importance for the labor-related cost categories based on the most recent forecast (IGI's second quarter 2021 forecast) of the 2016-based IRF market basket labor-related share cost weights, as proposed.
D. Wage Adjustment for FY 2022
1. Background
Section 1886(j)(6) of the Act requires the Secretary to adjust the proportion of rehabilitation facilities' costs attributable to wages and wage-related costs (as estimated by the Secretary from time to time) by a factor (established by the Secretary) reflecting the relative hospital wage level in the geographic area of the rehabilitation facility compared to the national average wage level for those facilities. The Secretary is required to update the IRF PPS wage index on the basis of information available to the Secretary on the wages and wage-related costs to furnish rehabilitation services. Any adjustment or updates made under section 1886(j)(6) of the Act for a FY are made in a budget-neutral manner.
For FY 2022, we proposed to maintain the policies and methodologies described in the FY 2021 IRF PPS final rule (85 FR 48435) related to the labor market area definitions and the wage index methodology for areas with wage data. Thus, we proposed to use the core based statistical areas (CBSAs) labor market area definitions and the FY 2022 pre-reclassification and pre-floor hospital wage index data. In accordance with section 1886(d)(3)(E) of the Act, the FY 2022 pre-reclassification and pre-floor hospital wage index is based on data submitted for hospital cost reporting periods beginning on or after October 1, 2017, and before October 1, 2018 (that is, FY 2018 cost report data).
The labor market designations made by the OMB include some geographic areas where there are no hospitals and, thus, no hospital wage index data on which to base the calculation of the IRF PPS wage index. We proposed to continue to use the same methodology discussed in the FY 2008 IRF PPS final rule (72 FR 44299) to address those geographic areas where there are no hospitals and, thus, no hospital wage index data on which to base the Start Printed Page 42378calculation for the FY 2022 IRF PPS wage index.
We invited public comment on our proposals regarding the Wage Adjustment for FY 2022.
The following is a summary of the public comments received on the proposed revisions to Wage Adjustment for FY 2022 and our responses:
Comment: Some commenters who were supportive of using the concurrent year's IPPS wage data requested that CMS adopt other IPPS wage index methodologies for the IRF PPS, including geographic reclassification and the imposition of a rural floor.
Response: We appreciate the commenters' support for the continued use of the concurrent year's IPPS wage data. However, we note that the IRF PPS does not account for geographic reclassification under sections 1886(d)(8) and (d)(10) of the Act, and does not apply the “rural floor” under section 4410 of the Balanced Budget Act of 1997 (BBA) (Pub. L. 105-33, enacted August 5, 1997). Furthermore, as we do not have an IRF-specific wage index, we are unable to determine the degree, if any, to which a geographic reclassification adjustment or a rural floor policy under the IRF PPS would be appropriate. The rationale for our current wage index policies was most recently published in the FY 2021 IRF PPS final rule (85 FR 48435 through 48436) and fully described in the FY 2006 IRF PPS final rule (70 FR 47880, 47926 through 47928).
Comment: Several commenters requested that we apply a 5 percent wage index cap to ensure that wage index values do not change by more than 5 percent from year-to-year to protect IRFs from larger payment volatility.
Response: We note that certain changes to wage index policy may significantly affect Medicare payments. These changes may arise from revisions to the OMB delineations of statistical areas resulting from the decennial census data, periodic updates to the OMB delineations in the years between the decennial censuses, or other wage index policy changes. While we consider how best to address these potential scenarios in a consistent and thoughtful manner, we reiterate that our policy principles with regard to the wage index include generally using the most current data and information available and providing that data and information, as well as any approaches to addressing any significant effects on Medicare payments resulting from these potential scenarios, in notice and comment rulemaking. We also note that any hospital wage data used to derive the IRF PPS wage index would be available from the CMS IPPS wage index website for each respective FY, which can be accessed from https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/index.
Comment: Several commenters requested that we provide additional wage index data that relate to changes for low-wage index areas that were finalized in the FY 2021 IPPS final rule.
Response: Data pertaining to the FY 2021 IPPS final rule are available at https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/index. We do not have any additional data on this for the IRF PPS.
After considering the comments received, for the reasons discussed above and in the FY 2022 IRF PPS proposed rule (86 FR 19097), we are finalizing our proposal to continue to use the updated hospital inpatient wage data, exclusive of the occupational mix and floor adjustments, to develop the IRF PPS wage index.
2. Core-Based Statistical Areas (CBSAs) for the FY 2022 IRF Wage Index
a. Background
The wage index used for the IRF PPS is calculated using the pre-reclassification and pre-floor inpatient PPS (IPPS) wage index data and is assigned to the IRF on the basis of the labor market area in which the IRF is geographically located. IRF labor market areas are delineated based on the CBSAs established by the OMB. The CBSA delineations (which were implemented for the IRF PPS beginning with FY 2016) are based on revised OMB delineations issued on February 28, 2013, in OMB Bulletin No. 13-01. OMB Bulletin No. 13-01 established revised delineations for Metropolitan Statistical Areas, Micropolitan Statistical Areas, and Combined Statistical Areas in the United States and Puerto Rico based on the 2010 Census, and provided guidance on the use of the delineations of these statistical areas using standards published in the June 28, 2010 Federal Register (75 FR 37246 through 37252). We refer readers to the FY 2016 IRF PPS final rule (80 FR 47068 through 47076) for a full discussion of our implementation of the OMB labor market area delineations beginning with the FY 2016 wage index.
Generally, OMB issues major revisions to statistical areas every 10 years, based on the results of the decennial census. Additionally, OMB occasionally issues updates and revisions to the statistical areas in between decennial censuses to reflect the recognition of new areas or the addition of counties to existing areas. In some instances, these updates merge formerly separate areas, transfer components of an area from one area to another, or drop components from an area. On July 15, 2015, OMB issued OMB Bulletin No. 15-01, which provides minor updates to and supersedes OMB Bulletin No. 13-01 that was issued on February 28, 2013. The attachment to OMB Bulletin No. 15-01 provides detailed information on the update to statistical areas since February 28, 2013. The updates provided in OMB Bulletin No. 15-01 are based on the application of the 2010 Standards for Delineating Metropolitan and Micropolitan Statistical Areas to Census Bureau population estimates for July 1, 2012 and July 1, 2013.
In the FY 2018 IRF PPS final rule (82 FR 36250 through 36251), we adopted the updates set forth in OMB Bulletin No. 15-01 effective October 1, 2017, beginning with the FY 2018 IRF wage index. For a complete discussion of the adoption of the updates set forth in OMB Bulletin No. 15-01, we refer readers to the FY 2018 IRF PPS final rule. In the FY 2019 IRF PPS final rule (83 FR 38527), we continued to use the OMB delineations that were adopted beginning with FY 2016 to calculate the area wage indexes, with updates set forth in OMB Bulletin No. 15-01 that we adopted beginning with the FY 2018 wage index.
On August 15, 2017, OMB issued OMB Bulletin No. 17-01, which provided updates to and superseded OMB Bulletin No. 15-01 that was issued on July 15, 2015. The attachments to OMB Bulletin No. 17-01 provide detailed information on the update to statistical areas since July 15, 2015, and are based on the application of the 2010 Standards for Delineating Metropolitan and Micropolitan Statistical Areas to Census Bureau population estimates for July 1, 2014 and July 1, 2015. In the FY 2020 IRF PPS final rule (84 FR 39090 through 39091), we adopted the updates set forth in OMB Bulletin No. 17-01 effective October 1, 2019, beginning with the FY 2020 IRF wage index.
On April 10, 2018, OMB issued OMB Bulletin No. 18-03, which superseded the August 15, 2017 OMB Bulletin No. 17-01, and on September 14, 2018, OMB issued OMB Bulletin No. 18-04, which superseded the April 10, 2018 OMB Bulletin No. 18-03. These bulletins established revised delineations for Metropolitan Statistical Areas, Micropolitan Statistical Areas, and Combined Statistical Areas, and provided guidance on the use of the Start Printed Page 42379delineations of these statistical areas. A copy of this bulletin may be obtained at https://www.whitehouse.gov/wp-content/uploads/2018/09/Bulletin-18-04.pdf.
To this end, as discussed in the FY 2021 IRF PPS proposed (85 FR 22075 through 22079) and final (85 FR 48434 through 48440) rules, we adopted the revised OMB delineations identified in OMB Bulletin No. 18-04 (available at https://www.whitehouse.gov/wp-content/uploads/2018/09/Bulletin-18-04.pdf) beginning October 1, 2020, including a 1-year transition for FY 2021 under which we applied a 5 percent cap on any decrease in an IRF's wage index compared to its wage index for the prior fiscal year (FY 2020). The updated OMB delineations more accurately reflect the contemporary urban and rural nature of areas across the country, and the use of such delineations allows us to determine more accurately the appropriate wage index and rate tables to apply under the IRF PPS.
OMB issued further revised CBSA delineations in OMB Bulletin No. 20-01, on March 6, 2020 (available on the web at https://www.whitehouse.gov/wp-content/uploads/2020/03/Bulletin-20-01.pdf). However, we have determined that the changes in OMB Bulletin No. 20-01 do not impact the CBSA-based labor market area delineations adopted in FY 2021. Therefore, CMS did not propose to adopt the revised OMB delineations identified in OMB Bulletin No. 20-01 for FY 2022.
4. Wage Adjustment
To calculate the wage-adjusted facility payment for the payment rates set forth in this final rule, we multiply the unadjusted Federal payment rate for IRFs by the FY 2022 labor-related share based on the 2016-based IRF market basket relative importance (72.9 percent) to determine the labor-related portion of the standard payment amount. A full discussion of the calculation of the labor-related share is located in section VI.C. of this final rule. We then multiply the labor-related portion by the applicable IRF wage index. The wage index tables are available on the CMS website at https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/InpatientRehabFacPPS/IRF-Rules-and-Related-Files.html.
Adjustments or updates to the IRF wage index made under section 1886(j)(6) of the Act must be made in a budget-neutral manner. We proposed to calculate a budget-neutral wage adjustment factor as established in the FY 2004 IRF PPS final rule (68 FR 45689), codified at § 412.624(e)(1), as described in the steps below. We proposed to use the listed steps to ensure that the FY 2022 IRF standard payment conversion factor reflects the proposed update to the wage indexes (based on the FY 2018 hospital cost report data) and the proposed update to the labor-related share, in a budget-neutral manner:
Step 1. Calculate the total amount of estimated IRF PPS payments using the labor-related share and the wage indexes from FY 2021 (as published in the FY 2021 IRF PPS final rule (85 FR 48424)).
Step 2. Calculate the total amount of estimated IRF PPS payments using the FY 2022 wage index values (based on updated hospital wage data) and the FY 2022 labor-related share of 72.9 percent.
Step 3. Divide the amount calculated in step 1 by the amount calculated in step 2. The resulting quotient is the FY 2022 budget-neutral wage adjustment factor of 1.0032.
Step 4. Apply the budget neutrality factor from step 3 to the FY 2022 IRF PPS standard payment amount after the application of the increase factor to determine the FY 2022 standard payment conversion factor.
We discuss the calculation of the standard payment conversion factor for FY 2022 in section VI.E. of this final rule.
We did not receive any comments on the proposed revisions to the IRF wage adjustment for FY 2022, and therefore, we are finalizing the revisions as proposed.
E. Description of the IRF Standard Payment Conversion Factor and Payment Rates for FY 2022
To calculate the standard payment conversion factor for FY 2022, as illustrated in Table 5, we begin by applying the increase factor for FY 2022, as adjusted in accordance with sections 1886(j)(3)(C) of the Act, to the standard payment conversion factor for FY 2021 ($16,856). Applying the 1.9 percent increase factor for FY 2022 to the standard payment conversion factor for FY 2021 of $16,856 yields a standard payment amount of $17,176. Then, we apply the budget neutrality factor for the FY 2022 wage index, and labor-related share of 1.0032, which results in a standard payment amount of $17,231. We next apply the budget neutrality factor for the CMG relative weights of 1.0005, which results in the standard payment conversion factor of $17,240 for FY 2022.
We invited public comment on the proposed FY 2022 standard payment conversion factor.
We did not receive any comments on the proposed revisions to the FY 2022 standard payment conversion factor, and therefore, we are finalizing the revisions as proposed.

After the application of the CMG relative weights described in section V. of the proposed rule to the proposed FY 2022 standard payment conversion factor ($17,240), the resulting unadjusted IRF prospective payment rates for FY 2022 are shown in Table 6.
Start Printed Page 42380
Start Printed Page 42381

F. Example of the Methodology for Adjusting the Prospective Payment Rates
Table 7 illustrates the methodology for adjusting the prospective payments (as described in section VI. of this final rule). The following examples are based on two hypothetical Medicare beneficiaries, both classified into CMG 0104 (without comorbidities). The unadjusted prospective payment rate for CMG 0104 (without comorbidities) appears in Table 7.
Example: One beneficiary is in Facility A, an IRF located in rural Spencer County, Indiana, and another beneficiary is in Facility B, an IRF located in urban Harrison County, Indiana. Facility A, a rural non-teaching hospital has a Disproportionate Share Hospital (DSH) percentage of 5 percent (which would result in a LIP adjustment of 1.0156), a wage index of 0.8594, and a rural adjustment of 14.9 percent. Facility B, an urban teaching hospital, has a DSH percentage of 15 percent (which would result in a LIP adjustment of 1.0454 percent), a wage index of 0.8695, and a teaching status adjustment of 0.0784.
To calculate each IRF's labor and non-labor portion of the prospective payment, we begin by taking the unadjusted prospective payment rate for Start Printed Page 42382CMG 0104 (without comorbidities) from Table 7. Then, we multiply the labor-related share for FY 2022 (72.9 percent) described in section VI.C. of this final rule by the unadjusted prospective payment rate. To determine the non-labor portion of the prospective payment rate, we subtract the labor portion of the Federal payment from the unadjusted prospective payment.
To compute the wage-adjusted prospective payment, we multiply the labor portion of the federal payment by the appropriate wage index located in the applicable wage index table. This table is available on the CMS website at https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/InpatientRehabFacPPS/IRF-Rules-and-Related-Files.html.
The resulting figure is the wage-adjusted labor amount. Next, we compute the wage-adjusted Federal payment by adding the wage-adjusted labor amount to the non-labor portion of the Federal payment.
Adjusting the wage-adjusted Federal payment by the facility-level adjustments involves several steps. First, we take the wage-adjusted prospective payment and multiply it by the appropriate rural and LIP adjustments (if applicable). Second, to determine the appropriate amount of additional payment for the teaching status adjustment (if applicable), we multiply the teaching status adjustment (0.0784, in this example) by the wage-adjusted and rural-adjusted amount (if applicable). Finally, we add the additional teaching status payments (if applicable) to the wage, rural, and LIP-adjusted prospective payment rates. Table 7 illustrates the components of the adjusted payment calculation.

Thus, the adjusted payment for Facility A would be $28,876.57, and the adjusted payment for Facility B would be $28,037.56.
VII. Update to Payments for High-Cost Outliers Under the IRF PPS for FY 2022
A. Update to the Outlier Threshold Amount for FY 2022
Section 1886(j)(4) of the Act provides the Secretary with the authority to make payments in addition to the basic IRF prospective payments for cases incurring extraordinarily high costs. A case qualifies for an outlier payment if the estimated cost of the case exceeds the adjusted outlier threshold. We calculate the adjusted outlier threshold by adding the IRF PPS payment for the case (that is, the CMG payment adjusted by all of the relevant facility-level adjustments) and the adjusted threshold amount (also adjusted by all of the relevant facility-level adjustments). Then, we calculate the estimated cost of a case by multiplying the IRF's overall CCR by the Medicare allowable covered charge. If the estimated cost of the case is higher than the adjusted outlier threshold, we make an outlier payment for the case equal to 80 percent of the difference between the estimated cost of the case and the outlier threshold.
In the FY 2002 IRF PPS final rule (66 FR 41362 through 41363), we discussed our rationale for setting the outlier threshold amount for the IRF PPS so that estimated outlier payments would equal 3 percent of total estimated payments. For the FY 2002 IRF PPS final rule, we analyzed various outlier policies using 3, 4, and 5 percent of the total estimated payments, and we concluded that an outlier policy set at 3 percent of total estimated payments would optimize the extent to which we could reduce the financial risk to IRFs of caring for high-cost patients, while still providing for adequate payments for all other (non-high cost outlier) cases.
Subsequently, we updated the IRF outlier threshold amount in the FYs 2006 through 2021 IRF PPS final rules and the FY 2011 and FY 2013 notices (70 FR 47880, 71 FR 48354, 72 FR 44284, 73 FR 46370, 74 FR 39762, 75 FR 42836, 76 FR 47836, 76 FR 59256, 77 FR 44618, 78 FR 47860, 79 FR 45872, 80 FR 47036, 81 FR 52056, 82 FR 36238, 83 FR 38514, 84 FR 39054, and 85 FR 48444, respectively) to maintain estimated outlier payments at 3 percent of total estimated payments. We also stated in the FY 2009 final rule (73 FR 46370 at 46385) that we would continue to analyze the estimated outlier payments for subsequent years and adjust the outlier threshold amount as appropriate to maintain the 3 percent target.
To update the IRF outlier threshold amount for FY 2022, we proposed to use FY 2020 claims data and the same methodology that we used to set the initial outlier threshold amount in the FY 2002 IRF PPS final rule (66 FR 41316 and 41362 through 41363), which is also the same methodology that we used to update the outlier threshold amounts for FYs 2006 through 2021. The outlier Start Printed Page 42383threshold is calculated by simulating aggregate payments and using an iterative process to determine a threshold that results in outlier payments being equal to 3 percent of total payments under the simulation. To determine the outlier threshold for FY 2022, we estimated the amount of FY 2022 IRF PPS aggregate and outlier payments using the most recent claims available (FY 2020) and the proposed FY 2022 standard payment conversion factor, labor-related share, and wage indexes, incorporating any applicable budget-neutrality adjustment factors. The outlier threshold is adjusted either up or down in this simulation until the estimated outlier payments equal 3 percent of the estimated aggregate payments. Based on an analysis of the preliminary data used for the proposed rule, we estimated that IRF outlier payments as a percentage of total estimated payments would be approximately 3.3 percent in FY 2021. Therefore, we proposed to update the outlier threshold amount from $7,906 for FY 2021 to $9,192 for FY 2022 to maintain estimated outlier payments at approximately 3 percent of total estimated aggregate IRF payments for FY 2022.
We note that, as we typically do, we updated our data between the FY 2022 IRF PPS proposed and final rules to ensure that we use the most recent available data in calculating IRF PPS payments. This updated data includes a more complete set of claims for FY 2020. Based on our analysis using this updated data, we continue to estimate that IRF outlier payments as a percentage of total estimated payments are approximately 3.4 percent in FY 2021. Therefore, we will update the outlier threshold amount from $7,906 for FY 2021 to $9,491 for FY 2022 to account for the increases in IRF PPS payments and estimated costs and to maintain estimated outlier payments at approximately 3 percent of total estimated aggregate IRF payments for FY 2022.
The comments received on the proposed update to the FY 2022 outlier threshold amount to maintain estimated outlier payments at approximately 3 percent of total estimated IRF payments and our responses are summarized below.
Comment: Commenters were generally supportive of the update to the outlier threshold. However, one commenter suggested that CMS consider policies that would better target outlier payments, such as placing a 10 percent cap on the amount of outlier payments any IRF could receive or lowering the 3 percent outlier pool. Additionally, another commenter suggested that any outlier change should be limited to no more than plus or minus 5 percent in any given year.
Response: We thank the commenters for their support of the update to the outlier threshold. We continue to believe that maintaining the outlier pool at 3 percent of aggregate IRF payments optimizes the extent to which we can reduce financial risk to IRFs of caring for highest-cost patients, while still providing for adequate payments for all other nonoutlier cases. However, as we did not propose changes to this methodology, these comments are outside the scope of this final rule. We will continue to monitor our IRF outlier policies to ensure that they continue to compensate IRFs appropriately. We refer readers to the FY 2002 IRF PPS final rule (66 FR 41316, 41362 through 41363) for more information regarding the rationale for setting the outlier threshold amount for the IRF PPS so that estimated outlier payments would equal 3 percent of total estimated payments.
Comment: One commenter asked CMS to provide further analysis and expand upon the relationship between COVID-19 related claims in the outlier calculations so that stakeholders could better understand CMS's perspective on the continuing impact of public health emergency claims from both the prior and current fiscal years on FY 2022 payments and beyond.
Response: We thank the commenter and appreciate the suggestion regarding further analysis to be conducted on outlier payments and COVID-19 claim interactions. We examined the relative weight values calculated both including and excluding cases associated with a COVID-19 ICD-10 diagnosis code. This analysis indicated that the majority of the changes in relative weight value would be less than 1 percent when COVID cases were removed.
Comment: Several commenters expressed concerns that the use of 2020 data in establishing the fixed-loss threshold would result in an excessively high fixed loss threshold that may be disconnected from the expected characteristics of patients in FY 2022 as the pandemic continues to subside. These commenters noted that the net result would be a substantial underpayment of outliers. The commenters requested that CMS freeze the fixed-loss threshold amount at the FY 2021 level, which was based on FY 2019 claims.
Response: We do not believe that freezing the fixed-loss threshold at the FY 2021 level is appropriate because to do so would fail to address the fact that we estimate for FY 2021 that we are overpaying by 0.4 percent the established outlier pool of 3 percent for the IRF PPS. As discussed previously, providers have access to Provider Relief Funds to assist with COVID-19 related costs, and it is unclear why IRFs would have incurred higher costs during the pandemic that were not COVID-19 related. We issued several IRF waivers to assist with the COVID-19 pandemic that, if anything, would have significantly lowered the costs of caring for patients in the IRF setting. Thus, we do not find any justification for continuing to overpay the established outlier pool of 3 percent.
Further, in FY 2022, we believe that IRFs, as the leader in rehabilitation services, will be very involved in treating the sequela of the COVID-19 infection in patients. Also, we believe that many of the infection control measures, such as personal protective equipment, private room and isolation protocols, and provision of therapies in a patient's room rather than a group setting, will continue to be used throughout IRFs in FY 2022 as new variants of COVID-19 emerge.
Comparing the outlier threshold adjustments in prior years, we continue to believe that maintaining the outlier pool at 3 percent of aggregate IRF payments optimizes the extent to which we can reduce financial risk to IRFs of caring for highest-cost patients, while still providing for adequate payments for all other non-outlier cases.
We will continue to monitor our IRF outlier policies to ensure that they continue to compensate IRFs appropriately. If we find any overpayments or underpayments in IRF outliers, we will continue to adjust the IRF outlier threshold amount appropriately to maintain IRF outlier payments at 3 percent of total IRF payments in future rulemaking cycles.
After consideration of the comments received and taking into account the most recent available data, we are finalizing the outlier threshold amount of $9,491 to maintain estimated outlier payments at approximately 3 percent of total estimated aggregate IRF payments for FY 2022.
B. Update to the IRF Cost-to-Charge Ratio Ceiling and Urban/Rural Averages for FY 2022
CCRs are used to adjust charges from Medicare claims to costs and are computed annually from facility-specific data obtained from MCRs. IRF specific CCRs are used in the development of the CMG relative weights and the calculation of outlier payments under the IRF PPS. In Start Printed Page 42384accordance with the methodology stated in the FY 2004 IRF PPS final rule (68 FR 45674, 45692 through 45694), we proposed to apply a ceiling to IRFs' CCRs. Using the methodology described in that final rule, we proposed to update the national urban and rural CCRs for IRFs, as well as the national CCR ceiling for FY 2022, based on analysis of the most recent data available. We apply the national urban and rural CCRs in the following situations:
- New IRFs that have not yet submitted their first MCR.
- IRFs whose overall CCR is in excess of the national CCR ceiling for FY 2022, as discussed below in this section.
- Other IRFs for which accurate data to calculate an overall CCR are not available.
Specifically, for FY 2022, we proposed to estimate a national average CCR of 0.478 for rural IRFs, which we calculated by taking an average of the CCRs for all rural IRFs using their most recently submitted cost report data. Similarly, we proposed to estimate a national average CCR of 0.393 for urban IRFs, which we calculated by taking an average of the CCRs for all urban IRFs using their most recently submitted cost report data. We apply weights to both of these averages using the IRFs' estimated costs, meaning that the CCRs of IRFs with higher total costs factor more heavily into the averages than the CCRs of IRFs with lower total costs. For this final rule, we have used the most recent available cost report data (FY 2019). This includes all IRFs whose cost reporting periods begin on or after October 1, 2018, and before October 1, 2019. If, for any IRF, the FY 2019 cost report was missing or had an “as submitted” status, we used data from a previous FY's (that is, FY 2004 through FY 2018) settled cost report for that IRF. We do not use cost report data from before FY 2004 for any IRF because changes in IRF utilization since FY 2004 resulting from the 60 percent rule and IRF medical review activities suggest that these older data do not adequately reflect the current cost of care. We proposed that if more recent data become available after the publication of the proposed rule and before the publication of the final rule, we would use such data to determine the FY 2022 national average rural and urban CCRs and the national CCR ceiling in the final rule. Using updated FY 2019 cost report data for this final rule, we estimate a national average CCR of 0.478 for rural IRFs, and a national average CCR of 0.394 for urban IRFs.
In accordance with past practice, we proposed to set the national CCR ceiling at 3 standard deviations above the mean CCR. Using this method, we proposed a national CCR ceiling of 1.34 for FY 2022. This means that, if an individual IRF's CCR were to exceed this ceiling of 1.34 for FY 2022, we will replace the IRF's CCR with the appropriate proposed national average CCR (either rural or urban, depending on the geographic location of the IRF). We calculated the proposed national CCR ceiling by:
Step 1. Taking the national average CCR (weighted by each IRF's total costs, as previously discussed) of all IRFs for which we have sufficient cost report data (both rural and urban IRFs combined).
Step 2. Estimating the standard deviation of the national average CCR computed in step 1.
Step 3. Multiplying the standard deviation of the national average CCR computed in step 2 by a factor of 3 to compute a statistically significant reliable ceiling.
Step 4. Adding the result from step 3 to the national average CCR of all IRFs for which we have sufficient cost report data, from step 1.
Using the updated FY 2019 cost report data for this final rule, we estimate a national average CCR ceiling of 1.35, using the same methodology.
We invited public comment on the proposed update to the IRF CCR ceiling and the urban/rural averages for FY 2022.
However, we did not receive any comments on the proposed revisions to the IRF CCR ceiling and the urban/rural averages for FY 2022, and therefore, we are finalizing the national average urban CCR at 0.394, the national average rural CCR at 0.478, and the national average CCR ceiling at 1.35 for FY 2022.
VIII. Inpatient Rehabilitation Facility (IRF) Quality Reporting Program (QRP)
A. Background and Statutory Authority
The Inpatient Rehabilitation Facility Quality Reporting Program (IRF QRP) is authorized by section 1886(j)(7) of the Act, and it applies to freestanding IRFs, as well as inpatient rehabilitation units of hospitals or Critical Access Hospitals (CAHs) paid by Medicare under the IRF PPS. Under the IRF QRP, the Secretary must reduce by 2 percentage points the annual increase factor for discharges occurring during a fiscal year for any IRF that does not submit data in accordance with the IRF QRP requirements established by the Secretary. For more information on the background and statutory authority for the IRF QRP, we refer readers to the FY 2012 IRF PPS final rule (76 FR 47873 through 47874), the CY 2013 Hospital Outpatient Prospective Payment System/Ambulatory Surgical Center (OPPS/ASC) Payment Systems and Quality Reporting Programs final rule (77 FR 68500 through 68503), the FY 2014 IRF PPS final rule (78 FR 47902), the FY 2015 IRF PPS final rule (79 FR 45908), the FY 2016 IRF PPS final rule (80 FR 47080 through 47083), the FY 2017 IRF PPS final rule (81 FR 52080 through 52081), the FY 2018 IRF PPS final rule (82 FR 36269 through 36270), the FY 2019 IRF PPS final rule (83 FR 38555 through 38556), and the FY 2020 IRF PPS final rule (84 FR 39054 through 39165).
B. General Considerations Used for the Selection of Measures for the IRF QRP
For a detailed discussion of the considerations we use for the selection of IRF QRP quality, resource use, or other measures, we refer readers to the FY 2016 IRF PPS final rule (80 FR 47083 through 47084).
1. Quality Measures Currently Adopted for the FY 2022 IRF QRP
The IRF QRP currently has 17 measures for the FY 2022 program year, which are set out in Table 8.
Start Printed Page 42385
C. IRF QRP Quality Measures Beginning With the FY 2023 IRF QRP
Section 1899B(h)(1) of the Act permits the Secretary to remove, suspend, or add quality measures or resource use or other measures described in sections 1899B(c)(1) and section 1899B(d)(1) of the Act respectively, so long as the Secretary publishes in the Federal Register (with a notice and comment period) a justification for such removal, suspension, or addition. We proposed to adopt one new measure: The COVID-19 Vaccination Coverage among Healthcare Personnel (HCP) [5] measure as an “other” measure under the resource use or other measure domain under section 1899B(d)(1) of the Act beginning with the FY 2023 IRF QRP. In accordance with section 1899B(a)(1)(B) of the Act, the data used to calculate this measure is standardized and interoperable. The proposed measure supports the Meaningful Measures domain of Promote Effective Prevention and Treatment of Chronic Disease. CMS identified the measure's concept as a priority in response to the current public health crisis. This process measure was developed with the Centers for Disease Control and Prevention (CDC) to track COVID-19 vaccination Coverage among HCP in the IRF setting. This measure is described in more detail below.
In addition, we proposed to update the denominator for one measure, the Transfer of Health (TOH) Information to the Patient-Post-Acute Care (PAC) measure to exclude patients discharged home under the care of an organized home health service or hospice.
1. COVID-19 Vaccination Coverage Among Healthcare Personnel (HCP) Measure Beginning With the FY 2023 IRF QRP
a. Background
On January 31, 2020, the Secretary of the U.S. Department Health and Human Services declared a public health emergency (PHE) for the United States in response to the global outbreak of Start Printed Page 42386SARS-CoV-2, a novel (new) coronavirus that causes a disease named “coronavirus disease 2019” (COVID-19).[6] COVID-19 is a contagious respiratory infection [7] that can cause serious illness and death. Older individuals, racial and ethnic minorities, and those with underlying medical conditions are considered to be at higher risk for more serious complications from COVID-19.[8 9] As stated in the proposed rule, as of March 31, 2021, the U.S. reported over 30 million cases of COVID-19 and over 548,000 COVID-19 deaths.[10] Hospitals and health systems saw significant surges of COVID-19 patients as community infection levels increased.[11] In December 2020 and January 2021, media outlets reported that more than 100,000 Americans were in the hospital with COVID-19.[12] As of July 21, 2021, the U.S. has reported over 33 million cases of COVID-19 and over 600,000 COVID-19 deaths.[13]
Evidence indicates that COVID-19 primarily spreads when individuals are in close contact with one another.[14] The virus is typically transmitted through respiratory droplets or small particles created when someone who is infected with the virus coughs, sneezes, sings, talks or breathes.[15] Experts believe that COVID-19 spreads less commonly through contact with a contaminated surface.[16]
According to the CDC, those at greatest risk of infection are persons who have had prolonged, unprotected close contact (that is, within 6 feet for 15 minutes or longer) with an individual with confirmed SARS-CoV-2 infection, regardless of whether the individual has symptoms.[17] Subsequent to the publication of the proposed rule, the CDC has confirmed that the three main ways that COVID-19 is spread are: (1) Breathing in air when close to an infected person who is exhaling small droplets and particles that contain the virus; (2) Having these small droplets and particles that contain virus land on the eyes, nose, or mouth, especially through splashes and sprays like a cough or sneeze; and (3) Touching eyes, nose, or mouth with hands that have the virus on them.[18] Personal protective equipment (PPE) and other infection-control precautions can reduce the likelihood of transmission in health care settings, but COVID-19 can still spread between health care personnel (HCP) and patients given the close contact that may occur during the provision of care.[19] The CDC has emphasized that health care settings, including IRFs, can be high-risk places for COVID-19 exposure and transmission.[20] Vaccination is a critical part of the nation's strategy to effectively counter the spread of COVID-19 and ultimately help restore societal functioning.[21]
On December 11, 2020, the Food and Drug Administration (FDA) issued the first Emergency Use Authorization (EUA) for a COVID-19 vaccine in the United States.[22] Subsequently, the FDA issued EUAs for additional COVID-19 vaccines. In issuing these EUAs, the FDA determined that it was reasonable to conclude that the known and potential benefits of each vaccine, when used as authorized to prevent COVID-19, outweighed its known and potential risks.[23 24 25]
As part of its national strategy to address COVID-19, the Biden administration stated that it would work with states and the private sector to execute an aggressive vaccination strategy and has outlined a goal of administering 200 million shots in 100 days.[26] Although the goal of the U.S. government is to ensure that every American who wants to receive a COVID-19 vaccine can receive one, federal agencies recommended that early vaccination efforts focus on those critical to the PHE response, including healthcare personnel (HCP),[27] and individuals at highest risk for developing severe illness from COVID-19.[28] For example, the CDC's Advisory Start Printed Page 42387Committee on Immunization Practices (ACIP) recommended that HCP should be among those individuals prioritized to receive the initial, limited supply of the COVID-19 vaccination, given the potential for transmission in health care settings and the need to preserve health care system capacity.[29] Research suggests most states followed this recommendation,[30] and HCP began receiving the vaccine in mid-December of 2020.[31] Subsequent to the publication of the IRF PPS proposed rule, on June 3, 2021 the White House confirmed that there was sufficient vaccine supply for all Americans.[32]
HCP are at risk of carrying COVID-19 infection to patients, experiencing illness or death as a result of COVID-19 themselves, and transmitting it to their families, friends, and the general public. We believe it is important to require that IRFs report COVID-19 HCP vaccination in order to assess whether they are taking steps to limit the spread of COVID-19 among their HCP, reduce the risk of transmission of COVID-19 within their facilities, and to help sustain the ability of IRFs to continue serving their communities throughout the PHE and beyond.
We also believe that publishing facility level COVID-19 HCP vaccination rates on Care Compare would be helpful to many patients, including those who are at high-risk for developing serious complications from COVID-19, as they choose facilities from which to seek treatment. Under CMS' Meaningful Measures framework, the COVID-19 Vaccination Coverage among Healthcare Personnel measure addresses the quality priority of “Promote Effective Prevention & Treatment of Chronic Disease” through the Meaningful Measures Area of “Preventive Care.”
Therefore, we proposed a new measure, COVID-19 Vaccination Coverage among HCP to assess the proportion of an IRF's healthcare workforce that has been vaccinated against COVID-19.
b. Stakeholder Input
In the development and specification of the measure, a transparent process was employed to seek input from stakeholders and national experts and engage in a process that allows for pre-rulemaking input on each measure, under section 1890A of the Act.[33] To meet this requirement, the following opportunity was provided for stakeholder input.
The pre-rule making process includes making publicly available a list of quality and efficiency measures, called the Measures Under Consideration (MUC) List that the Secretary is considering adopting, through federal rulemaking process, for use in Medicare program(s). This allows multi-stakeholder groups to provide recommendations to the Secretary on the measures included on the list. The COVID-19 Vaccination Coverage among Healthcare Personnel measure was included on the publicly available “List of Measures under Consideration for December 21, 2020”.[34] Five comments were received from industry stakeholders during the pre-rulemaking process on the COVID-19 Vaccination Coverage among HCP measure, and support was mixed. Commenters generally supported the concept of the measure. However, there was concern about the availability of the vaccine and measure definition for HCP, and some commenters encouraged CMS to continue to update the measure as new evidence comes in.
c. Measure Applications Partnership (MAP) Review
When the Measure Applications Partnership (MAP) Post-Acute Care/Long-Term Care (PAC-LTC) Workgroup convened on January 11, 2021, it reviewed the MUC List and the COVID-19 Vaccination Coverage among HCP measure. The MAP recognized that the proposed measure represents a promising effort to advance measurement for an evolving national pandemic and that it would bring value to the IRF QRP measure set by providing transparency about an important COVID-19 intervention to help limit COVID-19 infections.[35] The MAP also stated that collecting information on COVID-19 vaccination Coverage among healthcare personnel and providing feedback to facilities would allow facilities to benchmark coverage rates and improve coverage in their facility, and that reducing rates of COVID-19 in healthcare personnel may reduce transmission among patients and reduce instances of staff shortages due to illness.[36]
In its preliminary recommendations, the MAP PAC-LTC Workgroup did not support this measure for rulemaking, subject to potential for mitigation.[37] To mitigate its concerns, the MAP believed that the measure needed well-documented evidence, finalized specifications, testing, and NQF endorsement prior to implementation.[38] Subsequently, the MAP Coordinating Committee met on January 25, 2021, and reviewed the COVID-19 Vaccination Coverage among Healthcare Personnel measure. In the 2020-2021 MAP Final Recommendations, the MAP offered conditional support for rulemaking contingent on CMS bringing the measures back to the MAP once the specifications are further clarified. The final MAP report is available at http://www.qualityforum.org/Publications/2021/03/MAP_2020-2021_Considerations_for_Implementing_Measures_Final_Report_-_Clinicians,_Hospitals,_and_PAC-LTC.aspx.
In response to the MAP request for CMS to bring the measure back once the specifications were further clarified, CMS met with the MAP Coordinating Committee on March 15, 2021. First, CMS and CDC clarified the alignment of the COVID-19 Vaccination Coverage among HCP with the Influenza Vaccination among HCP (NQF #0431), an NQF-endorsed measure since 2012. The COVID-19 Vaccination Coverage among HCP measure is calculated using the same approach as the Influenza Vaccination among HCP measure.[39] The Start Printed Page 42388approach to identifying HCPs eligible for the COVID-19 vaccination is analogous to those used in the NQF endorsed flu measure which underwent rigorous review from technical experts about the validity of that approach and for which ultimately received NQF endorsement. More recently, prospective cohorts of health care personnel, first responders, and other essential and frontline workers over 13 weeks in eight U.S. locations confirmed that authorized COVID-19 vaccines are highly effective in real-world conditions. Vaccine effectiveness of full immunization with two doses of vaccines was 90 percent.[40]
Additionally, to support the measure's data element validity, CDC conducted testing of the COVID-19 vaccination numerator using data collected through the NHSN and independently reported through the Federal Pharmacy Partnership for Long-term Care Program for delivering vaccines to long-term care facilities. These are two completely independent data collection systems. In initial analyses of the first month of vaccination, the number of HCP vaccinated in approximately 1,200 facilities, which had data from both systems, the number of HCP vaccinated was highly correlated between these two systems with a correlation coefficient of nearly 90 percent in the second 2 weeks of reporting. Of note, assessment of data element reliability may not be required by NQF if data element validity is demonstrated.[41] In addition, for assessing the validity of new performance measure score (in this case, percentage COVID-19 vaccination coverage), NQF allows assessment by face validity (subjective determination by experts that the measure appears to reflect quality of care, done through a systematic and transparent process) [42] and the MAP concurred with face validity of the measure of COVID-19 vaccination coverage. Materials from the March 15, 2021 MAP Coordinating Committee meeting are on the NQF website at https://www.qualityforum.org/ProjectMaterials.aspx?projectID=75367.
This measure is not NQF endorsed, but CMS, in collaboration with the CDC, plans to submit the measure for NQF endorsement in the future.
d. Competing and Related Measures
Section 1886(j)(7)(D)(i) of the Act requires that, absent an exception under section 1886(j)(7)(D)(ii) of the Act, measures specified by the Secretary under section 1886(j)(7)(D) of the Act be endorsed by the entity with a contract under section 1890(a) of the Act, currently the National Quality Forum (NQF). In the case of a specified area or medical topic determined appropriate by the Secretary for which a feasible and practical measure has not been endorsed, section 1886(j)(7)(D)(ii) of the Act permits the Secretary to specify a measure that is not so endorsed, as long as due consideration is given to the measures that have been endorsed or adopted by a consensus organization identified by the Secretary. Section 1899B(e)(2)(A) of the Act requires that, subject to section 1899B(e)(2)(B) of the Act, each measure specified by the Secretary under section 1899B of the Act be endorsed by the entity with a contract under section 1890(a) of the Act. However, in the case of a specified area or medical topic determined appropriate by the Secretary for which a feasible and practical measure has not been endorsed by the entity with a contract under section 1890(a) of the Act, the Secretary may specify a measure that is not so endorsed as long as due consideration is given to measures that have been endorsed or adopted by a consensus organization identified by the Secretary.
The proposed COVID-19 Vaccination Coverage among HCP measure is not currently NQF endorsed and has not been submitted to the NQF for consideration, so we considered whether there are other available measures that assess COVID-19 vaccinations among HCP. After review of the NQF's consensus-endorsed measures, we were unable to identify any NQF endorsed measures for IRFs focused on capturing COVID-19 vaccination coverage of HCP and we found no other feasible and practical measure on the topic of COVID-19 vaccination Coverage among HCP, and we found no other feasible and practical measure on the topic of COVID-19 vaccination Coverage among HCP. The only other vaccination coverage of HCP measure found was the Influenza Vaccination Coverage among Healthcare Personnel (NQF #0431) measure which is NQF endorsed and was adopted in the IRF QRP in the FY 2014 IRF PPS Final Rule (78 FR 47905 through 47906).
Given the novel nature of the SARS-CoV-2 virus, and the significant and immediate risk it poses in IRFs, we believed it was necessary to propose the measure as soon as possible. Therefore, after consideration of other available measures that assess COVID-19 vaccination rates among HCP, we believe the exception under section 1899B(e)(2)(B) of the Act applies. This proposed measure has the potential to generate actionable data on vaccination rates that can be used to target quality improvement among IRF providers.
e. Quality Measure Calculation
The COVID-19 Vaccination Coverage among Healthcare Personnel (HCP) measure is a process measure developed by the CDC to track COVID-19 vaccination Coverage among HCP in facilities such as IRFs. Since this proposed measure is a process measure, rather than an outcome measure, it does not require risk-adjustment.
The denominator would be the number of HCP eligible to work in the IRF for at least one day during the reporting period, excluding persons with contraindications to COVID-19 vaccination, that are described by the CDC.[43]
The numerator would be the cumulative number of HCP eligible to work in the IRF for at least one day during the reporting period and who received a complete vaccination course against SARS-CoV-2. A complete vaccination course may require one or more doses depending on the specific vaccine used. The finalized measure specifications are available on the CDC website at https://www.cdc.gov/nhsn/nqf/index.html.
We proposed that IRFs would submit data for the measure through the CDC/NHSN data collection and submission framework.[44] This framework is currently used for reporting the CAUTI (NQF #0138) and Influenza Vaccination Coverage among Healthcare Personnel (NQF #0431) measures. IRFs would use the COVID-19 vaccination data reporting module in the NHSN Healthcare Personnel Safety (HPS) Component to report the number of HCP eligible who have worked at the facility Start Printed Page 42389that week (denominator) and the number of those HCP who have received a completed COVID-19 vaccination course (numerator). IRFs would submit COVID-19 vaccination data for at least 1 week each month. If IRFs submit more than one week of data in a month, the most recent week's data would be used for measure calculation purposes. Each quarter, the CDC would calculate a summary measure of COVID-19 vaccination coverage from the three monthly modules reported for the quarter. This quarterly rate would be publicly reported on the Care Compare website. Subsequent to the first refresh, one additional quarter of data would be added to the measure calculation during each advancing refresh, until the point four full quarters of data is reached. Thereafter, the measure would be reported using four rolling quarters of data on Care Compare.
For purposes of submitting data to CMS for the FY 2023 IRF QRP, IRFs would be required to submit data for the period October 1, 2021 through December 31, 2021. Following the data submission quarter for the FY 2023 IRF QRP, subsequent compliance for the IRF QRP would be based on four quarters of such data submission. For more information on the measure's proposed public reporting period, we refer readers to section VII.G.2 of the proposed rule.
We invited public comment on our proposal to add a new measure, COVID-19 Vaccination Coverage among Healthcare Personnel (HCP) measure, to the IRF QRP beginning with the FY 2023 IRF QRP.
The following is a summary of the public comments received on the proposed revisions to add a new measure, COVID-19 Vaccination Coverage among HCP measure, to the IRF QRP beginning with the FY 2023 IRF QRP, and our responses:
Comment: A number of organizations, including provider associations and patient advocacy groups, supported the proposal to adopt the COVID-19 Vaccination Coverage among HCP measure for the IRF QRP. Commenters agreed that the measure is vitally important to protect the health and well-being of older adults in IRFs and reporting of this measure through the NHSN would help to ensure transparency and accountability in community infection prevention and control efforts. The commenters supported the idea that reporting of HCP vaccination rates helps inform patient and caregiver choices when considering IRFs from which to seek care, particularly for those at high risk for developing serious complications from COVID-19. Another commenter noted that reporting COVID-19 HCP vaccination rates would provide greater transparency to federal officials and other stakeholders seeking to effectively target vaccine hesitancy and resources related to the COVID-19 vaccines. One commenter noted that vaccinations are particularly important because the nature of care settings like IRFs makes other COVID-19 transmission mitigation strategies (for example, social distancing) much less effective.
Response: We thank the commenters for their support and agree that the COVID-19 Vaccination Coverage among HCP measure is critically important to the protection of health and well-being of older adults in IRFs, and that reporting this measure will help to ensure transparency and accountability in community infection prevention and control efforts. We also agree that the nature of care settings like IRFs makes other COVID-19 transmission mitigation strategies less effective, which makes COVID-19 vaccinations of HCP in this setting especially important. The CDC has also emphasized that healthcare settings, including IRFs, can be high-risk places for COVID-19 exposure and transmission and notes that COVID-19 can spread between HCP and patients given the close contact that may occur during the provision of care.[45]
Although we received a number of comments in support of the measure's concept as well as the need to encourage widespread vaccination among HCP, some commenters expressed concerns with the measure, including administrative burden, lack of access to the vaccine, concerns that staff may be intimidated into receiving the vaccine, the lack of certainty about whether a booster vaccination will be necessary, concern that the vaccinations have not received full FDA approval, and finally that the measure is not NQF endorsed. We will address each of these comments below.
Comment: Several commenters expressed concern over the potential for inequality among providers because vaccines are not equally available across the nation. They point out that the type of vaccine available to them is out of their control and since the availability of the single-dose vaccines may be different across the country, some providers would be at a disadvantage because of the 4-week waiting period between doses of the two-dose vaccines to reach complete vaccination status. Some providers were concerned about vaccine availability. These commenters pointed out that at times the COVID-19 vaccine supply chain has been disrupted and believe the measure should not be implemented until there is a more definitive understanding of the future supply of vaccines.
Response: As part of its national strategy to address COVID-19, the current administration stated that it would work with states and the private sector to execute an aggressive vaccination strategy. The goal of the U.S. government is to ensure that every American who wants to receive a COVID-19 vaccine can receive one. While we acknowledge that vaccine supply was initially limited, more than 20 states are no longer ordering all the vaccine doses allocated to them due to decline in demand,[46] and more than 1,000 counties are reporting a surplus of vaccine appointments.[47] We understand that vaccine availability may vary based on location, and vaccination and medical staff authorized to administer the vaccination may not be readily available in all areas. Supply distribution is the responsibility of each state, and IRFs should continue to consult state and local health departments to understand the range of options for how vaccines can be made available to patients and staff.
As discussed in section VIII.C.1.e of this final rule, we proposed that IRFs would submit data for the COVID-19 vaccination Coverage among HCP measure data for at least 1 week each month. If IRFs submit more than 1 week of data in a month, the most recent week's data would be used for measure calculation purposes. Each quarter, the CDC would calculate a summary measure of COVID-19 vaccination coverage from the three monthly modules reported for the quarter. This quarterly rate would be publicly reported on the Care Compare website. As a result, there will be time within the quarter for persons receiving the two-dose vaccine to reach complete vaccination status.
Comment: Several commenters were concerned about the effect potential booster shots could have on the definition of a “complete vaccination course,” and raised questions about Start Printed Page 42390whether a booster shot would be needed, the timing of such a shot, and at what intervals. They pointed out that it could complicate the tracking of the measure, while others questioned how booster shots would factor into reporting requirements. Commenters requested that CMS clarify how the potential need for “booster” vaccinations would be accounted for in IRFs going forward. A commenter noted that in the FY 2022 Inpatient Prospective Payment System (IPPS) proposed rule, CMS states that the numerator would be calculated based on HCP who received a completed vaccination course “since the vaccine was first available or on a repeated interval if revaccination is recommended.” Since this language is not included in the FY 2022 IRF PPS proposed rule, they requested clarification on how evolving vaccine recommendations will be accounted for in this proposed measure.
Response: The COVID-19 Vaccination Coverage among HCP measure is a measure of a completed COVID-19 vaccination course as defined in section VIII.C.1.e. of this final rule. A complete vaccination course may require one or more doses depending on the specific vaccine used. Currently, the need for COVID-19 booster doses has not been established, and no additional doses are currently recommended for HCP.[48] However, we believe that the numerator is sufficiently broad to include potential future boosters as part of a “complete vaccination course” and therefore the measure is sufficiently specified to address boosters.
Comment: We received several comments posing questions about the uncertainty the provider community believes about the future of the COVID-19 vaccination. Commenters voiced concern about the uncertainty of how long the vaccines confer immunity. They point to the amount of misinformation that has been and is still currently being spread about COVID-19 and the vaccinations.
Response: We acknowledge the science relating to the SARS-CoV-2 virus continues to evolve. It is another reason the COVID-19 Vaccination Coverage among HCP measure is so important. Population immunity means that enough people in a community are protected from getting a disease because they have already had the disease or because they have been vaccinated. Population immunity makes it hard for the disease to spread from person to person.[49]
We are still learning how effective the vaccines are against new variants of the virus that causes COVID-19. Current evidence suggests that the COVID-19 vaccines authorized for use in the United States offer protection against most variants currently spreading in the United States.[50] The CDC will continue to monitor how vaccines are working to see if variants have any impact on how well COVID-19 vaccines work in real-world conditions.
Comment: Because the vaccine is new, several commenters suggested that CMS not adopt the measure until more is known about SARS-CoV-2. Other commenters urged CMS to either make the measure voluntary for the FY 2023 program, or delay implementation by at least 1 year.
Response: We believe it is important that all IRFs report COVID-19 Vaccination Coverage among HCP as soon as possible in order to assess the potential spread of COVID-19 among their HCP and within their facilities to help sustain the ability of IRFs to continue serving their communities throughout the PHE and beyond. Allowing IRFs to voluntarily report may result in selective reporting among high-performing facilities, which would reduce the usefulness of the publicly reported data. Because of the ongoing PHE for COVID-19 and risk of infection transmissions in the IRF population, this measure will be informative to beneficiaries and consumers who receive inpatient rehabilitation services from IRFs.
Comment: Commenters pointed out that there is still a degree of vaccine hesitancy remaining among the general population as well as hospital staff. They believe the lack of certainty could create an unnecessary burden on IRFs until the vaccines receive FDA approval or there is some equivalent guidance from the federal government clarifying how IRFs should proceed with mandating vaccinations.
Response: We reiterate that the COVID-19 vaccines are authorized by FDA for use through Emergency Use Authorizations (EUAs). We refer readers to the FDA website for additional information related to FDA's process for evaluating an EUA request at https://www.fda.gov/vaccines-blood-biologics/vaccines/emergency-use-authorization-vaccines-explained. Additionally, two of the three vaccines authorized for emergency use are shown to be 90 to 95 percent effective in preventing COVID-19 in persons without prior infection, and are equally effective across a variety of characteristics, including age, gender, race, ethnicity, and body mass index or presence of other medical conditions.[51] In clinical trials, the Pfizer vaccine was 100 percent effective at preventing severe disease. The third vaccine authorized for emergency use demonstrates it is 93.1 percent effective at preventing COVID-19 hospitalization and 75 percent effective against all-cause death.[52] The FDA is closely monitoring the safety of the COVID-19 vaccines authorized for emergency use.
We believe it is critical to measure staff vaccination rates among IRFs even as vaccinations become more common, especially in light of the vaccine hesitancy the commenters have pointed out. As reported by Medscape Medical News on June 28, 2021,[53] federal data show that one in four hospital workers across the United states are still unvaccinated, and only one in every three hospital workers are vaccinated in the nation's 50 largest health systems. Moreover, the adoption of this measure does not mandate or require that HCP complete a COVID-19 vaccination course. Even if IRFs have limited control over the vaccination status of their employees, the information collected by this measure is vitally important and useful to stakeholders.
Comment: We received several comments stating that while the COVID-19 Vaccination Coverage among HCP measure does not directly compel IRFs to ensure that their employees are vaccinated, publicly reporting performance on this measure might Start Printed Page 42391incent IRFs to adopt mandatory vaccination policies for their personnel. As a result, commenters suggest the measure has the potential to jeopardize an already challenged workforce, exacerbating critical workforce issues, if IRFs attempt to produce a positive performance by either mandating vaccination and/or not hiring or letting go of staff who choose not to be vaccinated. One commenter noted that multiple states have introduced or passed legislation prohibiting discrimination based on COVID-19 vaccination status. Several state legislatures have considered legislation that would prohibit an employer from forcing employees to be vaccinated for COVID-19. Other state legislatures are considering legislation to specifically authorize employer-mandated vaccinations. Commenters cautioned that IRFs unable to mandate the vaccine could be at a systematic performance disadvantage on the measure.
Response: We believe that the unprecedented risks associated with the COVID-19 PHE warrant direct attention, especially because HCP are working directly with and in close proximity to patients, but are clarifying that the COVID-19 Vaccination Coverage among HCP measure does not require providers to adopt mandatory vaccination policies. To support a comprehensive vaccine administration strategy, we encourage IRFs to voluntarily engage in the provision of appropriate and accessible education and vaccine-offering activities. Many IRFs across the country are educating staff, patients, and patient representatives, participating in vaccine distribution programs, and voluntarily reporting vaccine administration. The CDC has a number of resources [54] available to providers to assist in building vaccine confidence. CMS also has a web page to help providers, including IRFs, find resources related to the COVID-19 vaccines.[55] There are a number of toolkits and videos providers can use to stay informed and to educate their employees, patients and communities about the COVID-19 vaccines.
Consistent vaccination reporting by IRFs via the NHSN will help patients and their caregivers identify IRFs that have potential issues with vaccine confidence or slow uptake among staff. Implementation of voluntary COVID-19 vaccine education and vaccination programs in IRFs will help protect patients and staff, allowing for an expedited return to more normal routines, including timely preventive healthcare; family, caregiver, and community visitation; and group and individual activities.[56]
Regarding concerns over discrimination based on COVID-19 vaccination status, the Equal Employment Opportunity Commission (EEOC) released updated and expanded technical assistance on May 28, 2021,[57] stating that federal equal employment opportunity (EEO) laws do not prevent an employer from requiring all employees physically entering the workplace to be vaccinated for COVID-19, so long as the employer complies with the reasonable accommodation provisions of the Americans with Disabilities Act (ADA) and Title VII of the Civil Rights Act of 1964 and other EEO considerations.
Comment: One commenter referenced new state laws restricting an employer's ability to obtain information regarding an employee's vaccination status unless it is for the purpose of determining whether the facility should implement reasonable accommodation measures to protect health and safety.
Response: We acknowledge the commenter's concern regarding state laws prohibiting providers from obtaining information regarding an employee's COVID-19 vaccination status except in certain circumstances related to health and safety. We believe, however, that obtaining COVID-19 vaccination status information is important for determining reasonable measures to protect the health and safety of not only the patients it serves, but other staff working within the facility. Within the NHSN reporting module, there is an option to select “unknown COVID-19 vaccination status” and providers should utilize this response for employees who choose not to disclose their status. Additionally, as mentioned in the previous comment response, the EEOC released updated and expanded technical assistance on May 28, 2021,[58] stating that federal EEO laws do not prevent an employer from requiring all employees physically entering the workplace to be vaccinated for COVID-19, so long as the employer complies with the reasonable accommodation provisions of the Americans with Disabilities Act (ADA) and Title VII of the Civil Rights Act of 1964 and other EEO considerations.
Comment: One commenter questioned whether the proposal was in conflict with guidance from the EEOC, which states employers must provide a reasonable accommodation if an employee's sincerely held religious belief, practice, or observance prevents them from receiving the vaccination.
Response: We believe the commenter is referring to the updated and expanded technical assistance the EEOC issued on May 28, 2021.[59] CMS disagrees that the proposal conflicts with the EEOC's guidance. Specifically, the EEOC stated the federal EEO laws do not prevent an employer from requiring all employees physically entering the workplace to be vaccinated for COVID-19, so long as the employer complies with the reasonable accommodation provisions of the Americans with Disabilities Act (ADA) and Title VII of the Civil Rights Act of 1964 and other EEO considerations. This measure is intended to report the number of HCP who have received a COVID-19 vaccination, but it does not mandate HCP to receive a COVID-19 vaccination.
Comment: One commenter questioned why this information would be used in a quality measure that impacts payments when providers cannot mandate their staff to become vaccinated. Another commenter pointed out that the potential for interstate regulatory differences raises concerns about a future employee vaccination metric in a pay-for-performance program.
Response: We proposed the COVID-19 Vaccination Coverage among HCP measure beginning with the FY 2023 IRF QRP. The IRF QRP is a pay-for-reporting program under which IRFs are not financially penalized based on measure performance, but rather on Start Printed Page 42392their adherence to the reporting requirements.
Comment: A few commenters raised the issue of the possibility of legal risk to their organization if HCP experience an adverse event related to a vaccine, given the vaccines are not FDA-approved. They point out that this creates ethical and legal challenges to the organization.
Response: It is unclear what legal and ethical challenges the commenters are referring to, as the COVID-19 Vaccination Coverage among HCP measure does not require HCP to be vaccinated. In addition, all of the COVID-19 vaccines have been authorized by the FDA for widespread use through an EUA. We refer readers to the FDA website for additional information related to the process of vaccination vetting and approval found here: https://www.fda.gov/vaccines-blood-biologics/vaccines/emergency-use-authorization-vaccines-explained.
Comment: A number of commenters stated that it is premature to begin tracking COVID-19 vaccinations because the COVID-19 vaccines are authorized through an EUA and do not have full FDA approval at this time. One provider acknowledged that they were confident in the safety and efficacy of the three current vaccine products but still find it to be incongruous to adopt a measure into federal quality reporting programs that assesses the use of a product that has not yet received full federal approval.
Response: We believe there is still risk of transmitting infections in the IRF population. COVID-19 vaccines are a crucial tool for slowing the spread of disease and death among residents, staff, and the general public. Based on the FDA's review, evaluation of the data, and its decision to authorize three vaccines for emergency use, these vaccines meet FDA's standards for an EUA for safety and effectiveness to prevent COVID-19 disease and related serious outcomes, including hospitalization and death. The combination of vaccination, universal source control (wearing masks), social distancing, and handwashing offers further protection from COVID-19.[60] Given the emergency use authorization by the FDA and the continued PHE for COVID-19, we disagree with the commenter, and believe our proposal to add the COVID-19 Vaccination Coverage among HCP measure to the IRF QRP is appropriate and necessary for patient safety.
Comment: We received numerous comments requesting that CMS delay the adoption of the COVID-19 Vaccination Coverage among HCP measure until it has received NQF endorsement. These commenters expressed concern that since the measure has not been fully specified, tested, or endorsed by the NQF, it may not be thoroughly tested and vetted. They urged CMS, in addition to seeking NQF endorsement, to fully develop and test the measure for reliability and validity before implementing it in the IRF QRP.
Response: Given the novel nature of the SARS-CoV-2 virus, and the significant and immediate health risk it poses in IRFs, we believe it is necessary to propose the measure as soon as possible. Additionally, given the results from CDC's preliminary validity testing of the data elements required for the measure numerator (described further in section VIII.C.1.c. of this final rule), the alignment between the denominator of this measure and the denominator of the Influenza Vaccination among HCP measure (which is NQF-endorsed), and the MAP's determination that the measure has face validity, CMS believes it is appropriate to propose the COVID-19 Vaccination Coverage among HCP measure for the FY 2023 QRP. The CDC, in collaboration with CMS, are planning to submit the measure for consideration in the NQF Fall 2021 measure cycle.
Comment: One commenter expressed concern that the measure was developed for public health tracking during a PHE, not for quality assessment or payment purposes.
Response: This measure was developed for quality assessment purposes. COVID-19 is a contagious respiratory infection [61] that can cause serious illness and death. As of June 25, 2021, the U.S. reported over 33 million cases of COVID-19 and over 600,000 COVID-19 deaths.[62] Immunization has a significant role in reducing the incidence and prevalence—as well as the morbidity and mortality—of vaccine-preventable diseases.[63] Over the past decade, there has been increased focus on improving adult immunization rates. In 2010, the Department of Health & Human Services (HHS) published a National Vaccination Plan which provided a strategic approach for preventing infectious diseases and improving the public's health through vaccination.[64] More recently, a 2014 NQF report emphasized addressing adult immunization measures outside of those addressing influenza and pneumococcal disease and offered recommendations to advance measurement, including a composite of all Advisory Committee on Immunization Practices (ACIP) of the CDC (ACIP/CDC) recommended vaccinations for HCP.[65] The measure was developed in collaboration with the CDC because we believe it is important to require that IRFs report COVID-19 HCP vaccination to assess the potential spread of COVID-19 among their HCP and the risk of transmission of COVID-19 within their facilities, and to help sustain the ability of IRFs to continue serving their communities throughout the PHE and beyond.
Comment: We received a comment asking CMS not to finalize the COVID-19 Vaccination Coverage among HCP measure due to the burden associated with it. The commenter pointed to the reasons previously cited in 2018 for removing the Influenza vaccination measures through NHSN as justification.
Response: We presume the commenter is referring to the removal of the Percent of Residents of Patients Who Were Assessed and Appropriately Given the Seasonal Influenza Vaccine (Short Stay) (NQF #0680), which was removed from the IRF QRP in the FY 2019 IRF PPS final rule (83 FR 38559 to 38560). The reason the measure was removed was not because of the burden associated with collecting it. We use measure removal factors (§ 412.634(b)(2)) to determine when measures should be removed from the IRF QRP. The Percent of Residents of Patients Who Were Assessed and Appropriately Given the Seasonal Influenza Vaccine (Short Stay) (NQF #0680) measure performance among Start Printed Page 42393IRFs was so high and unvarying that meaningful distinctions in improvements in performance could no longer be made. Therefore, it met the standard for measure removal Factor 1 (set forth at § 412.634(b)(2)(i)) of the IRF QRP regulations and was removed.
Comment: Several commenters who were concerned about the burden on IRFs stated that the measure would divert resources currently being used to combat the COVID-19 pandemic since their IT systems must be updated to accommodate changes to the IRF QRP. The commenters recommended that CMS delay this measure for at least one full calendar year following the conclusion of the COVID-19 PHE declaration. They believe a delay in adding this new measure to the IRF QRP is needed to avoid imposing an additional burden on IRFs.
Response: We believe it is important to require that IRFs report COVID-19 HCP vaccination as soon as possible to assess the potential spread of COVID-19 among their HCP and the risk of transmission of COVID-19 within their facilities, and to help sustain the ability of IRFs to continue serving their communities throughout the PHE and beyond. Additionally, consistent vaccination reporting by IRFs via the NHSN will help CMS to identify additional resources and tools IRFs may need to address the challenges of the PHE. Accordingly, we do not believe that a delayed reporting effective date is appropriate.
Comment: We received several comments related to the burden of tracking vaccination records. One commenter attributed the burden of reporting the measure to the fact that they keep employee health records outside of their electronic health record (EHR) due to health privacy concerns. Therefore, attempting to identify and collect data on employee vaccine adherence is inherently difficult and burdensome. Another commenter noted the challenges inherent in monitoring and tracking employees who receive multi-dose courses on varying schedules. Still other commenters pointed to the fact that many vaccination sites, including federally run mass vaccination sites, do not communicate with all registries, and that some states do not maintain a registry. We received several comments asking CMS to consider easing the reporting frequency for the COVID-19 Vaccination Coverage among HCP measure. Some commenters stated that reporting vaccinations one week per month rather than one time per quarter is burdensome, while others raise concern that it could cause fluctuations in vaccination rates.
Response: IRFs are currently required to submit data for the Influenza Vaccination among HCP (NQF #0431) measure to the CDC's NHSN Healthcare Personnel Safety Component (HPS) annually. While IRFs will not have the burden of registering and learning how to use the NHSN, we acknowledge there will be burden with collecting the required information. However, we believe it will be minimal because IRFs already have experience successfully reporting information using the NHSN reporting modules. We refer readers to section XIII.C.7. of this final rule for an estimate of burden related to the COVID-19 Vaccination Coverage among HCP measure. The data sources for the number of HCP who have received COVID-19 vaccines may include HCP health records and paper and/or electronic documentation of vaccination given at the healthcare facility, pharmacy, or elsewhere. Further, HCP receiving vaccination elsewhere may provide documentation of vaccination. Additionally, the CDC has provided a number of resources including a tool called the Data Tracking Worksheet for COVID-19 Vaccination among Healthcare Personnel to help IRFs log and track the number of healthcare personnel (HCP) who are vaccinated for COVID-19. IRFs would enter COVID vaccination data for each HCP in the tracking worksheet, and select a reporting week, the data to be entered into the NHSN will automatically be calculated on the Reporting Summary.[66]
Comment: One commenter pointed to the fact that for IRFs within acute care hospitals, separating out which HCP may have had contact with the IRF unit may present a substantial reporting burden while providing little useful information that could not be gleaned from the hospital-wide reports already submitted. Rather than creating an additional reporting requirement applying solely to IRFs, the agency should leverage existing COVID-19 vaccination rate reporting to achieve the agency's goals.
Response: The IRF QRP is a separate reporting program from the Hospital Inpatient Quality Reporting (IQR) Program. Section 1886(b)(3)(B)(viii) of the Act requires subsection (d) hospitals to submit quality measure data to the Secretary. Separately, section 1886(j)(7) of the Act requires the Secretary, among other things, to specify reporting requirements for IRFs. Each distinct Medicare provider reports separately to CMS to meet its reporting obligations for their respective quality programs, as applicable. Because the IRF QRP and the Hospital IQR are separate programs, any HCP who is eligible to work one day during the reporting period in the IRF would be counted for purposes of the IRF QRP COVID-19 Vaccination Coverage among HCP measure, regardless of whether those HCP work in another facility that is also reporting the same measure.
Comment: A few commenters commented on CMS' statement that the COVID-19 Vaccination Coverage among HCP measure was modeled after the Influenza Vaccination among HCP measure. They believe that there are key differences between the two measures, such as how the vaccines are administered and data are collected. They stated that it is common for influenza vaccinations to be administered by the facility itself, whereas COVID-19 vaccination administration has been varied depending on the state and locality the provider is located in. They also point to the fact that the influenza vaccine is administered one time for the entire flu season with a numerator and denominator that can be calculated with relative ease. Another commenter listed the different reporting requirements for the numerator for the COVID-19 vaccination as compared to the influenza vaccination.
Response: We agree that there are key differences between the Influenza Vaccination among HCP measure and the COVID-19 Vaccination Coverage among HCP measure. We acknowledge that even though the CDC modeled the COVID-19 Vaccination Coverage among HCP measure after the Influenza Vaccination among HCP measure, FDA-approved influenza vaccines and the authorized COVID-19 vaccines differ in multiple ways. The reporting requirements for the numerator of the COVID-19 Vaccination Coverage among HCP measure that one commenter listed are due to the fact that some COVID-19 vaccines require two doses to reach full vaccination status, while some COVID-19 vaccines require only one dose. The measures are aligned with respect to the reporting mechanism used to report data (the NHSN) and key components of the measure specifications (for example, the definition of the denominator), but the measures allow for important differences to reflect the reality that the circumstances around vaccine administration (that the commenter points out) are not identical.Start Printed Page 42394
Comment: One commenter disagreed with the proposal of adopting the COVID-19 Vaccination Coverage among HCP measure to the IRF QRP, citing the fact that any new measure added to the IRF QRP creates another basis for CMS to financially penalize IRFs for even the smallest infractions of the multitudinous guidance documents concerning not only the reporting of the quality data itself, but the many technical elements required by the CDC's NHSN system for quality data to be processed and transferred to CMS. The commenters stated providers should never be financially penalized if they report all their quality data by the reporting deadlines, but especially when the quality measure concerns an ongoing global pandemic. Other commenters stated that the COVID-19 measure should be outside of the IRF QRP and not be subject to the 2 percent payment penalty or used for payment decisions.
Response: Section 1886(j)(7)(A)(i) of the Act requires the Secretary to apply a 2 percent payment penalty under the IRF QRP to IRFs that fail to meet the IRF QRP reporting requirements during a fiscal year. IRFs that submit IRF QRP data according to the program's requirements during a fiscal year will not receive the 2 percent payment for the fiscal year.
We received comments about the measure in general, but also specific to the numerator and denominator. We address those comments here.
Comment: Several commenters pointed to the fact that providers have many questions about the specifics of the COVID-19 Vaccination Coverage among HCP measure such as what the long-term plans for using the measure in the IRF QRP are. Another commenter believes the measure seemed unnecessary based on the current vaccination push and the fact that due to the Federal Vaccination Schedule, healthcare workers would already have received the vaccination. This commenter did not believe that the measure addressed many of the unknowns still ahead regarding the virus.
Response: We interpret the commenter's reference to the “Federal Vaccination Schedule” to be referring to the eligibility criteria during the initial rollout of the COVID-19 vaccine. When the U.S. supply of COVID-19 vaccine was limited, CDC provided recommendations to federal, state, and local governments about who should be vaccinated first. While CDC made recommendations for who should be offered the COVID-19 vaccines first, each state had its own plan. CMS acknowledges that healthcare workers were given priority in receiving the vaccine, but as reported by Medscape Medical News on June 28, 2021,[67] federal data show that one in four hospital workers across the United states are still unvaccinated, and only one in every three hospital workers are vaccinated in the nation's 50 largest health systems. We believe it is critical to measure staff vaccination rates among IRFs even as vaccinations become more common, especially in light of the vaccine hesitancy other commenters have pointed out. As with all measures within the IRF QRP, this measure will be routinely monitored and evaluated, and if substantive changes are necessary, it will be re-specified through the rulemaking process.
In response to the comment questioning the long-term plans for using the measure, as described in sections VIII.C.1.e and VIII.H.2. of this final rule, we proposed to adopt the COVID-19 Vaccination Coverage among HCP measure into the IRF QRP and publicly report on IRF performance. Once a measure is adopted under the IRF QRP, the measure will remain in effect until CMS proposes that it be removed, suspended, or replaced. We refer readers to the CY 2013 Hospital Outpatient Prospective Payment System/Ambulatory Surgical Center (OPPS/ASC) Payment Systems and Quality Reporting Programs final rule (77 FR 68500 through 68507) for details on this policy.
Comment: One commenter had questions on what “fully vaccinated” meant.
Response: The term “fully vaccinated” is not used in the proposed COVID-19 Vaccine Coverage among HCP measure. We proposed the numerator for the COVID-19 Vaccination Coverage among HCP measure to include a complete vaccination course as defined in section VIII.C.1.e of this final rule. We refer the commenter to the CDC's website at https://www.cdc.gov/coronavirus/2019-ncov/vaccines/fully-vaccinated.html where the term “fully vaccinated” is defined.
Comment: One commenter requested that once the pandemic subsided, that CMS restructure the reporting of this measure to be more similar to the influenza measure.
Response: The Influenza Vaccination among HCP (NQF #0431) measure reports the percentage of HCP who receive the influenza vaccination during the time from October 1 (or when the vaccine is available) through March 31 of the following year,[68] and is reported annually. CMS will continually monitor and evaluate this measure to ensure it remains clinically valid. If substantive revisions are needed in the future, such revisions would be proposed through the notice and comment rulemaking process.
Comment: Commenters pointed out that the Influenza Vaccination among HCP (NQF #0431) measure utilizes providers working in the facility for the denominator, whereas the proposed COVID-19 metric utilizes providers eligible to work in the facility. Several commenters requested that CMS revise the denominator to include eligible providers who have worked at the facility during the period being measured, similar to the influenza measure. They believe this would be important due to differences across states as to whom would be considered “eligible” to work due to laws such as the Family Medical Leave Act (FMLA) and state-level laws associated with defining employee status.
Response: The COVID-19 Vaccination Coverage among HCP measure includes in its calculation HCP who work regularly in an IRF. At times HCP who work in a facility may be temporarily absent from the facility for any reason including illness, injury, vacation, or leave. The Influenza Vaccination among HCP measurement period is the entire 6-month influenza season so such temporary absences will not affect the influenza measure denominator. However, the COVID-19 vaccination Coverage among HCP measure has a measurement period of only 1 week, which is shorter than the timeframe covered by the influenza vaccination measure. This difference accounts for a HCP who works at an IRF who may be absent during this shortened period. Therefore, HCP who work in the IRF, but may be temporarily absent from the facility for up to 2 weeks, are still to be included in the measure denominator.[69]
Comment: Several providers and provider organizations sent in comments about the vaccine's contraindications. Several commenters Start Printed Page 42395stated that contraindications are poorly defined, continue to change, and vary depending on the vaccine administered. They point out that misinterpretation could lead to fluctuations in the denominator. They acknowledge that CDC has narrowed the list of contraindications, but “precautions” still exist, and they are uncertain how precautions should be taken into account for reporting purposes.
Response: Since authorized for emergency use by the FDA, over 300 million doses of the COVID-19 vaccine have been administered in the United States.[70] These vaccines have undergone the most intensive safety monitoring for a vaccine in U.S. history.[71] This monitoring includes using both established and new safety monitoring systems to make sure that COVID-19 vaccines are safe. Contraindications are listed in the FDA patient and provider Fact Sheets and in the Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Authorized in the United States at https://www.cdc.gov/vaccines/covid-19/clinical-considerations/covid-19-vaccines-us.html. Information may be updated based on data from safety monitoring systems at any time. Contraindications and other clinical considerations, while rare, are accounted for in the COVID-19 Vaccination Coverage among HCP measure. However, the precautions listed should not be reported as contraindications, as these are not measure exclusions.
Comment: One commenter questioned whether immunization sites are currently capturing all immunization activity, which could lead to lapses in and inaccurate reporting.
Response: We are unclear what issue the commenter is referring to and how it impacts the proposal to adopt the COVID-19 Vaccination Coverage among HCP measure into the IRF QRP. The data sources for the number of HCP who have received COVID-19 vaccines may include HCP health records and paper and/or electronic documentation of vaccination given at the healthcare facility, pharmacy, or elsewhere. HCP receiving vaccination elsewhere should provide documentation of vaccination.[72]
Comment: Several commenters shared their opinion that refining the measure and timeline would be appropriate before full implementation. They stated that adopting the measure into the QRP should hinge upon full approval by the FDA across all existing submitted vaccines under the EUA. They stated that feedback from the field is needed to ensure that the measure reflects the most current knowledge and evidence. They stated that there is still much unknown regarding the long-term effectiveness of the current COVID-19 vaccine under the EUA, and whether there will be the need for periodic re-inoculation to maintain immunity. They urged CMS to remain flexible on the proposed measure and adjust it accordingly based on the need to revaccinate.
Response: We appreciate that there are unanswered questions related to the SARS-CoV-2 virus and COVID-19 vaccinations. We will routinely monitor and evaluate this measure to ensure it remains valid, reliable, and useful to consumers, and if substantive revisions are needed in the future, such revisions would be proposed through the notice and comment rulemaking process. In the meantime, we believe that the measure specifications as proposed are appropriate, and should be implemented in a manner that provides stakeholders with timely information about staff vaccination rates.
Comment: We received several comments raising concerns that the vaccination rates collected for this measure could vary significantly from the time of data submission to the time they are publicly reported. They believe the time between data submission and reporting will not provide patients with accurate data on the vaccination status of HCP in a specific IRF. They question whether the definition of a fully vaccinated individual could change between the data submission and public reporting of the data, which would provide an even more incomplete window into HCP vaccination rates.
Response: We acknowledge the commenters' concern with regard to timely display of publicly reported data. CMS believes it is important to make the most up-to-date data available to beneficiaries, which will aid them in making essential decisions about health care. In the FY 2016 IRF PPS final rule (80 FR 47126 through 47127), we finalized our procedures for making available to the public information regarding the performance of individual IRFs with respect to the measures required under section 1899B of the Act. The IRF QRP's public display policy allows 4.5 months beyond the end of each calendar year quarter for a number of administrative tasks to occur in sequential order, including allowing sufficient time for IRFs to be able to submit data, review data, make corrections to the data, and view their performance prior to public reporting. Subsequently, a number of administrative tasks must then occur in sequential order between the time IRF QRP data are submitted and they are reported in Care Compare to ensure the validity of the data. We have streamlined the process as much as possible, but must take these steps to ensure we post IRF QRP data accurately. Additionally, the COVID-19 Vaccination Coverage among HCP measure will be one of several measures on Care Compare that patients and caregivers can use to make informed healthcare decisions.
Comment: Several commenters stated that because IRFs would be dependent upon the HCP's permission to allow reporting their vaccination status, it would result in an undercounting of vaccinated HCP for a facility since they could choose not to share this information.
Response: We understand that obtaining information about a person's vaccination status is dependent upon the HCP sharing that information, which is why we encourage providers to voluntarily engage in the provision of appropriate and accessible education and vaccine-offering activities. Many facilities, including IRFs, across the country are educating staff, patients, and patient representatives, and voluntarily reporting vaccine administration. The CDC has a number of resources [73] available to providers to assist in building vaccine confidence. The Department of Health and Human Services (HHS) has launched a national initiative, the “We Can Do This” Campaign, to increase public confidence in and uptake of COVID-19 vaccines while reinforcing basic prevention measures such as mask wearing and social distancing. There are a number of resources and toolkits available on the website at https://wecandothis.hhs.gov/resources,, and the COVID-19 Community Corps is available for communities to participate in to help build vaccine confidence in your Start Printed Page 42396community. Additionally, the EEOC has guidance [74] that states requesting documentation or other confirmation showing that an employee received a COVID-19 vaccination in the community is not a disability-related inquiry covered by the Americans with Disabilities Act (ADA) and that the federal EEO laws do not prevent an employer from requiring all employees physically entering the workplace to be vaccinated for COVID-19, subject to the reasonable accommodation provisions of Title VII and the ADA.
Comment: A few commenters stated there is no evidence that these measures are reliable, valid, or differentiate between providers. As a result, they have concern that the data informing the measure are not reliable for public consumption. They believe that because of the number of challenges associated with reporting, the data reported are unlikely to be reliable and could therefore unfairly skew a hospital's score on this safety and quality measure.
Response: There is evidence that this measure can identify clinically important differences between providers. As of June 14, 2021, based on reporting to NHSN, there are facilities which reported HCP COVID-19 vaccination coverage rates approaching 100 percent and other facilities which reported HCP COVID-19 vaccination coverage rates below 50 percent (COVID-19 Nursing Home Data | Data.CMS.gov). We expect the same level of differentiation to translate to IRFs. This measure was judged to have face validity by the MAP Coordinating Committee, which recognized the unique role that measurement plays in meeting the COVID-19 healthcare crisis through direct measurement of vaccination rates and noted that direct measurement of vaccination for patients and HCP is a key approach to addressing a national healthcare challenge.[75] Additionally, to support the measure's data element validity, CDC conducted testing of the COVID-19 vaccination numerator using data collected through the NHSN and independently reported through the Federal Pharmacy Partnership for Long-term Care Program for delivering vaccines to long-term care facilities. These are two completely independent data collection systems. In initial analyses of the first month of vaccination, the number of HCP vaccinated in approximately 1,200 facilities, which had data from both systems, was highly correlated between these two systems with a correlation coefficient of nearly 90 percent in the second 2 weeks of reporting.[76] We expect similar validity to translate to IRFs. Finally, we proposed the measure's denominator to use the same identification and categorization as the existing Influenza Vaccination among HCP measure,[77] an NQF-endorsed measure since 2012, which was adopted for the IRF QRP in the FY 2014 IRF PPS final rule (78 FR 47859).
Comment: Two commenters urged CMS to delay adopting the measure until at least a full calendar year following the COVID-19 PHE has ended. They believe the additional time would allow CMS and relevant stakeholders the opportunity to discuss and address the challenges, avoid negative unintended consequences, and ensure the data captured allow accurate reporting that can be trusted by patients and their families. Other commenters recommended that CMS either delay adoption of the measure for at least one year or adopt the measure for voluntary reporting for at least the first year, but any voluntarily reported data should not be publicly reported.
Response: We believe that the unprecedented risks associated with the COVID-19 PHE warrant direct attention. Data show that eight out of every 10 deaths related to COVID-19 have been in adults 65 years of age and older. When compared to 18- to 29-year-olds, adults over 65 have a five to eight times higher risk of being hospitalized from COVID-19 and those older than 75 have a 220 times higher risk of dying.[78] Moreover, many common chronic conditions raise the risks associated with contracting COVID-19, including hypertension, obesity, chronic obstructive pulmonary disease, heart disease, diabetes, and chronic kidney disease.[79]
We believe consistent vaccination reporting by IRFs via the NHSN and public reporting of this information on Care Compare will assist Medicare beneficiaries to make informed choices when selecting IRF care. Further, this measure would facilitate patient care and care coordination during the discharge planning process. A discharging hospital/facility, in collaboration with the patient and family, can use this measure to coordinate care and ensure patient preferences are considered in the discharge plan. Patients at high risk for negative outcomes due to COVID-19 (perhaps due to underlying conditions) can use healthcare provider vaccination rates when they are selecting an IRF for next-level care. While we have taken into consideration comments suggesting that we delay implementation of this measure, we do not believe we can delay monitoring and publicly reporting the COVID-19 Vaccination Coverage among HCP measure. Therefore, we believe it is important to begin publicly reporting this measure as proposed. CMS will routinely monitor and evaluate this measure to identify unintended consequences and to ensure it remains valid, reliable, and useful to consumers. The CDC, in collaboration with CMS are planning to submit the measure for consideration in the NQF Fall 2021 measure cycle.
After careful consideration of the public comments, we are finalizing our proposal to adopt the COVID-19 Vaccination Coverage among HCP measure to the IRF QRP beginning with the FY 2023 IRF QRP.
2. Update to the Transfer of Health (TOH) Information to the Patient—Post-Acute Care (PAC) Measure Beginning With the FY 2023 IRF QRP
We proposed to update the Transfer of Health (TOH) Information to the Patient—Post-Acute Care (PAC) measure (TOH-Patient) denominator to exclude patients discharged home under the care of an organized home health service or hospice. This measure assesses for and reports on the timely transfer of health information, specifically transfer of a medication list. We adopted this Start Printed Page 42397measure in the FY 2020 IRF PPS final rule (84 FR 39099 through 39107) beginning with the FY 2022 IRF QRP. It is a process-based measure that evaluates for the transfer of information when a patient is discharged from his or her current PAC setting to a private home/apartment, board and care home, assisted living, group home, transitional living, or home under the care of an organized home health service organization or hospice.
This measure, adopted under section 1899B(c)(1)(E) of the Act, was developed to be a standardized measure for the IRF QRP, LTCH QRP, SNF QRP, and Home Health (HH) QRP. The measure is calculated by one standardized data element that asks, “At the time of discharge, did the facility provide the patient's current reconciled medication list to the patient, family, and/or caregiver?” The discharge location is captured by items on the Inpatient Rehabilitation Facility-Patient Assessment Instrument (IRF-PAI).
Specifically, we proposed to update the measure denominator. Currently the measure denominators for both the TOH-Patient and the TOH-Provider measure assess the number of patients discharged home under the care of an organized home health service organization or hospice. In order to align the measure with the SNF QRP, LTCH QRP, and HH QRP and avoid counting the patient in both TOH measures in the IRF QRP, we proposed to remove this location from the definition of the denominator for the TOH-Patient measure. Therefore, we proposed to update the denominator for the TOH-Patient measure to only discharges to a private home/apartment, board and care home, assisted living, group home, or transitional living. For additional technical information regarding the TOH-Patient measure, we refer readers to the document titled “Final Specifications for IRF QRP Quality Measures and Standardized Patient Assessment Data Elements (SPADEs)” available at https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/IRF-Quality-Reporting/Downloads/Final-Specifications-for-IRF-QRP-Quality-Measures-and-SPADEs.pdf.
We invited public comment on our proposal to update the denominator of the Transfer of Health (TOH) Information to the Patient—Post-Acute Care (PAC) measure beginning with the FY 2023 IRF QRP.
The following is a summary of the public comments received on our proposal to update the denominator of the TOH-Patient measure beginning with the FY 2023 IRF QRP and our responses:
Comment: We received overwhelming support for our proposal to update the TOH-Patient measure's denominator to remove the inclusion of “home under care of an organized home health service organization or hospice.” Commenters agreed that the update will further improve the validity and usefulness of the measure, while reducing provider burden. Some commenters stated that while they recognize the burden the PHE has had on all healthcare facility types, an accurate medication list is important to continuity of care. One commenter urged CMS to seek endorsement from the NQF on this measure, since it is not currently endorsed for use in PAC settings, including IRFs.
Response: We appreciate the commenter's support. We plan to submit the measure for NQF endorsement.
Comment: One provider noted disappointment that the measure has been delayed for at “least two full fiscal years after the end of the PHE.”
Response: We refer the commenter to the CY 2022 HH PPS proposed rule (86 FR 35874) where we proposed to revise the compliance date for the collection of data on the Transfer of Health Information to Provider-PAC measure and Transfer of Health Information to Patient-PAC measure and certain Standardized Patient Assessment Data Elements under the IRF QRP beginning October 1, 2022 and invite public comment on the proposal.
After careful consideration of the public comments, we are finalizing our proposal to update the denominator of the Transfer of Health (TOH) Information to the Patient—Post Acute Care (PAC) measure beginning with the FY 2023 IRF QRP.
D. IRF QRP Quality Measures Under Consideration for Future Years: Request for Information
We solicited input on the importance, relevance, appropriateness, and applicability of each of the measures and concepts under consideration listed in Table 9 for future years in the IRF QRP.

We received several comments on this RFI, which are summarized below:
Comment: Several commenters supported the inclusion of all the proposed measures listed in Table 9. One commenter stated that all of the measures and measure concepts are important and relevant for assessing quality of care delivered to IRF patients. Another commenter stated that the concepts should generate valuable data points to consider.
Many commenters supported the concept of frailty, and one commenter stated they are encouraged to see frailty included since a frailty diagnosis can be linked to a risk for falls and subsequent adverse clinical events. Several commenters, however, did not recommend a measure of frailty be included in the IRF QRP. Another commenter thought that the term “frailty” is non-specific and is a concept that may not be well understood or applied.
Many commenters supported the measure concept of the shared decision-making process while others questioned how it could be captured in the IRF QRP. One commenter stated that while shared decision-making is a very important component of patient-Start Printed Page 42398centered care, IRFs are unique settings that are not well-suited for inclusion in certain shared decision-making performance measures since shared decision-making requires that multiple options of the same clinical value be presented to the patient. Other commenters stated that since informed decision making is already part of the CMS Conditions of Participation (CoP), this would likely not add any value to providers or patients, and they do not support adding what they believe would likely be another process measure.
Several commenters supported the concept of patient-reported outcomes (PROs). One commenter stressed the importance of PROs since they determine outcomes based on information obtained directly from patients, and therefore provide greater insight into patients' experience of the outcomes of care. Some commenters did not support the concept of PROs because they believe many patients treated in the IRF are unable to verbalize and/or lack the cognitive capacity to accurately express themselves.
Several commenters were supportive of the inclusion of pain management quality measures, while others were concerned about the reporting of opioid use and frequency as a quality measure due to the potential for over- or under-prescribing of opioids. One commenter stated that because pain is often an inherent part of intensive rehabilitation therapy, and is already frequently assessed, it is not an appropriate quality reporting measure for the IRF QRP. Several commenters stated that a more meaningful pain measure in the IRF setting would be designed to assess whether staff are responsive to and help manage patients' pain.
Commenters were generally supportive of the concept of health equity in quality measurement. They agree that closing the health equity gap is essential to ensure optimal health services and outcomes to all Americans regardless of individual characteristics.
A couple of commenters encouraged CMS to remove topped-out measures and low-occurrence measures to ensure the IRF QRP remains relevant to quality and performance, and another commenter suggested removal of two of the IRF QRP measures currently reported. Finally, one commenter did not support any additional measures or measure concepts due to the burden associated with adding measures to the IRF QRP.
Commenters also suggested other concepts for quality measurement in the IRF QRP such as quality of life, mental health, and nutritional status.
Response: We appreciate the input provided by commenters. While we will not be responding to specific comments submitted in response to this RFI in this final rule, we intend to use this input to inform our future measure development efforts.
E. Fast Healthcare Interoperability Resources (FHIR) in Support of Digital Quality Measurement in Quality Programs—Request for Information
1. Solicitation of Comments
We sought input on the following steps that would enable transformation of CMS' quality measurement enterprise to be fully digital:
- What EHR/IT systems do you use and do you participate in a health information exchange (HIE)?
- How do you currently share information with other providers?
- In what ways could we incentivize or reward innovative uses of health information technology (IT) that could reduce burden for post-acute care settings, including but not limited to IRFs?
- What additional resources or tools would post-acute care settings, including but not limited to IRFs, and health IT vendors find helpful to support the testing, implementation, collection, and reporting of all measures using FHIR standards via secure APIs to reinforce the sharing of patient health information between care settings?
- Would vendors, including those that service post-acute care settings, such as IRFs, be interested in or willing to participate in pilots or models of alternative approaches to quality measurement that would align standards for quality measure data collection across care settings to improve care coordination, such as sharing patient data via secure FHIR API as the basis for calculating and reporting digital measures?
We received a number of comments and appreciate the time commenters took to respond. We plan to continue working with other agencies and stakeholders to coordinate and to inform our transformation to dQMs leveraging health IT standards. We will actively consider all input as we develop future regulatory proposals or future subregulatory policy guidance. Any updates to specific program requirements related to quality measurement and reporting provisions would be addressed through separate and future notice-and-comment rulemaking, as necessary.
F. Closing the Health Equity Gap in Post-Acute Care Quality Reporting Programs—Request for Information
1. Solicitation of Public Comment
Under authority of the IMPACT Act and section 1886(j)(7) of the Act, we sought comment on the possibility of revising measure development, and the collection of other SPADEs that address gaps in health equity in the IRF QRP. Any potential health equity data collection or measure reporting within a CMS program that might result from public comments received in response to this solicitation would be addressed through a separate notice-and-comment rulemaking in the future.
Specifically, we invited public comment on the following:
- Recommendations for quality measures or measurement domains that address health equity, for use in the IRF QRP.
- As finalized in the FY 2020 IRF PPS Final Rule (84 FR 39149 through 39161), IRFs must report certain standardized patient assessment data (SPADEs) on SDOH, including race, ethnicity, preferred language, interpreter services, health literacy, transportation and social isolation.[80] CMS is seeking guidance on any additional items, including SPADEs that could be used to assess health equity in the care of IRF patients, for use in the IRF QRP.
- Recommendations for how CMS can promote health equity in outcomes among IRF patients. For example, we are interested in feedback regarding whether including facility-level quality measure results stratified by social risk factors and social determinants of health (for example, dual eligibility for Medicare and Medicaid, race) in confidential feedback reports could allow facilities to identify gaps in the quality of care they provide. (For example, methods similar or analogous to the CMS Disparity Methods [81] which provide hospital-level confidential results stratified by dual eligibility for condition-specific readmission measures which are currently included in the Hospital Readmission Reduction Program (see 84 FR 42496 through 42500)).
- Methods that commenters or their organizations use in employing data to reduce disparities and improve patient outcomes, including the source(s) of data used, as appropriate.Start Printed Page 42399
- Given the importance of structured data and health IT standards for the capture, use, and exchange of relevant health data for improving health equity, the existing challenges providers encounter for effective capture, use, and exchange of health information, such as data on race, ethnicity, and other social determinants of health, to support care delivery and decision making.
While we will not be responding to specific comments submitted in response to this Health Equity RFI in this final rule, we appreciate all of the comments and interest in this topic. We will continue to take all concerns, comments, and suggestions into account as we continue work to address and develop policies on this important topic. It is our hope to provide additional stratified information to providers related to race and ethnicity if feasible. The provision of stratified measure results will allow IRFs to understand how they are performing with respect to certain patient risk groups, to support these providers in their efforts to ensure equity for all of their patients and to identify opportunities for improvements in health outcomes.
G. Form, Manner, and Timing of Data Submission Under the IRF QRP
1. Background
We refer readers to the regulatory text at 42 CFR 412.634(b) for information regarding the current policies for reporting IRF QRP data.
2. Schedule for Data Submission of the COVID-19 Vaccination Coverage Among Healthcare Personnel Measure Beginning With the FY 2023 IRF QRP
As discussed in section VII.C.1 of the proposed rule, we proposed to adopt the COVID-19 Vaccination Coverage among HCP measure beginning with the FY 2023 IRF QRP. Given the time-sensitive nature of this measure in light of the PHE, we proposed an initial data submission period from October 1, 2021 through December 31, 2021. Starting in CY 2022, IRFs would be required to submit data for the entire calendar year beginning with the FY 2024 IRF QRP.
IRFs would submit data for the measure through the CDC/NHSN web-based surveillance system. IRFs currently utilize the NHSN for purposes of meeting other IRF QRP requirements.[82] IRFs would use the COVID-19 vaccination data reporting module in the NHSN Healthcare Personnel Safety (HPS) Component to report the cumulative number of HCP eligible to work in the healthcare facility for at least 1 day during the reporting period, excluding persons with contraindications to COVID-19 vaccination (denominator) and the cumulative number of HCP eligible to work in the IRF for at least 1 day during the reporting period and who received a complete vaccination course against COVID-19 (numerator). IRFs would submit COVID-19 vaccination data through the NHSN for at least 1 week each month and the CDC would report to CMS quarterly.
We invited public comment on this proposal.
The following is a summary of the public comments received on the proposed revisions to the Form, Manner, and Timing of Data Submission under the IRF QRP and our responses:
Comment: A number of commenters wrote to CMS about the administrative burden associated with reporting of the measure through NHSN. They pointed to other reporting systems being used around the country and stated that this would be duplicative reporting. Several commenters referenced the Department of Health and Human Services TeleTracking system, VaccineFinder, and various state agencies and databases. They stated that having to utilize these systems with different reporting periods in addition to the NHSN and its reporting period utilizes additional resources and will require multiple tracking strategies to keep up. They urged CMS to use data from these systems without requiring additional data collection in the NHSN. Several of these commenters requested that if the measure is finalized, that CMS utilize the data submitted through the TeleTracking system.
Response: The TeleTracking system was one system that was used to manage the critical first months of the COVID-19 PHE, as it was critical that the federal government received data to facilitate planning, monitoring, and resource allocation during the PHE for COVID-19. The TeleTracking system collects a number of data points, such as ventilators in the facility, ventilators in use, ICU beds available, and ICU beds occupied. However, the TeleTracking system was not used for the IRF QRP. We have proposed to use the NHSN COVID-19 Modules for tracking COVID-19 Vaccination Coverage among HCP across all sites of service, including IRFs, as most of the state Immunization Information Systems do not include the information needed to calculate the COVID-19 Vaccination Coverage among HCP.
For meeting the requirements of the IRF QRP, we do not prescribe which day of the week the data for the COVID-19 vaccinations must be submitted. We refer readers to section VIII.G.2 describing the proposal for data submission to the NHSN for more detail.
Comment: Another commenter encouraged CMS to evaluate both methods of how data are submitted (that is, the TeleTracking system and the NHSN) and select just one standardized data reporting system and process. This commenter was in favor of using the NHSN to report the COVID-19 Vaccination Coverage among HCP measure because all care settings are using it to report the Influenza Vaccination Coverage among HCP and discontinuing COVID-19 vaccination reporting to the HHS tracking system. Another commenter urged CMS to use the TeleTracking system since the data fields collected in it are less detailed than what is required in the NHSN.
Response: We proposed to use the NHSN COVID-19 Modules for tracking COVID-19 Vaccination Coverage among HCP across all sites of service, including IRFs. IRFs are familiar with NHSN since they use it to submit information for other CDC measures and this system facilitates calculation of the COVID-19 Vaccination Coverage among HCP measure so CMS can meet its public reporting obligations to provide information to beneficiaries seeking care from IRFs.
Comment: One commenter stated that the reporting burden would be high depending on how reporting for the COVID-19 Vaccination Coverage among HCP measure interacts with other COVID-19 data reporting requirements, and adding this measure would require adjustments in workflow for which CMS would need to provide significant technical support.
Response: IRFs are currently required to submit data for the Influenza Vaccination among HCP measure (NQF #0431) to the CDC's NHSN Healthcare Personnel Safety Component (HPS) annually. Therefore, we believe the burden for adding the COVID-19 Vaccination Coverage among HCP measure will be minimal for IRFs, since IRFs already have experience successfully reporting information using the NHSN reporting modules.
Comment: We received several comments requesting that CMS consider reducing the reporting frequency for the COVID-19 Vaccination Coverage among HCP measure. They stated that reporting COVID-19 vaccinations 1 week per month, rather than one time per quarter Start Printed Page 42400is burdensome. They recommended CMS use quarterly reporting periods to align with the influenza vaccination reporting schedule.
Response: The COVID-19 Vaccination Coverage among HCP measure measurement period is only 1 week, considerably shorter than the time period covered by the Influenza Vaccination among HCP measure (NQF #0431). Additionally, the reporting schedule of 1 week per month was chosen to provide vaccination coverage data on a more timely basis than the Influenza Vaccination among HCP measure (NQF #0431), while also reducing the burden on IRFs that weekly reporting of this information would have been.
Comment: A couple of commenters were concerned that allowing IRFs to select which week of the month they will report could lead to IRFs selecting the week in which the highest number of employees completed a vaccination course. They were also concerned about having only 1 week out of the month represent a full month because it might add a confounding variable to the data and potentially reduce the value to healthcare consumers.
Response: We proposed to allow IRFs to select which week of the month to report for additional flexibility. We note that counts reported during a given week should reflect the cumulative number of eligible HCP (as defined in the COVID-19 Vaccination Coverage among HCP measure specifications [83] ) during the reporting period. Thus, IRFs have the flexibility to select a week that they determine is sufficiently representative of the month. The amount of burden reduction by reporting 1 week a month vs. every week a month is expected to outweigh any confounding variable that the commenters may be referring to. While the reporting experience during the PHE may not reflect the experience after the PHE, it is not expected the week -to -week variation will significantly change vaccination coverage rates, particularly as the denominator of HCP consists of those who regularly work in the facility, including HCP who may be on temporary (less than 2-week) leave.
Comment: A few commenters were concerned about having a shortened reporting period of October 1, 2021 through December 31, 2021 to assess reporting requirements for the FY 2023 IRF QRP.
Response: In the FY 2016 IRF PPS Final Rule (80 FR 47122 to 47123), CMS revised the data collection time frame for the IRF QRP to a calendar year, unless there is a clinical reason for an alternative data collection time frame.[84] We believe this simplifies the data collection and submission time frame under the IRF QRP for IRFs, and also eliminates the situation in which data collection during a quarter in the same calendar year can affect two different years of annual payment update determination.[85] Therefore this proposed data collection and submission time frame is consistent with the IRF QRP, and we are confident in IRFs' ability to meet the reporting period since they have demonstrated their ability to do so since FY 2016.
Comment: A couple of commenters are also concerned about having different reporting timelines for the COVID-19 Vaccination Coverage among HCP measure and the Influenza Vaccination among HCP measure (NQF #0431). They raised the question of whether providers would only have 6 weeks after the end of the quarter to submit data for the COVID-19 Vaccination Coverage among HCP measure, since this is the deadline for the Influenza Vaccination among HCP measure (NQF #0431). Some commenters recommended that CMS use the reporting deadlines used for the influenza measures, while others recommended CMS set the deadline for reporting the proposed COVID-19 Vaccination Coverage among HCP measure data consistent with existing NHSN requirements.
Response: We thank the commenter for the question. While both measures assess vaccination rates among HCP, they are operationalized differently. The shortened deadline for the Influenza Vaccination among HCP measure (NQF #0431) is necessary to make the data available in the public reporting cycle more timely. Since the influenza vaccination season ends March 31, a 6-week reporting period is necessary in order to publish the measure in the next available public reporting refresh. Because the transmission of SARS-CoV-2 virus currently has no established seasonality, we proposed 4.5 months after the end of the quarter for IRFs to report the data. Additionally, since the measure will not be publicly reported until the Fall of 2022, we are able to allow the standard review and correct time periods.
Comment: One commenter stated that since the measure requires COVID-19 vaccination rates to be reported monthly, using 1 week of data, it would mean that reporting IRFs will need to recalculate the numerator and denominator every reporting period in order to submit an accurate report. They stated it would require outreach to all employees, and a weekly review of the employee roster to ensure ongoing accuracy, since the number could potentially change daily.
Response: IRFs do not need to recalculate the numerator and denominator every reporting period. IRFs complete the weekly COVID-19 cumulative vaccination counts among HCP using the NHSN module, and the CDC reports the data to CMS quarterly.
After careful consideration of the public comments, we are finalizing our proposal to require IRFs to submit COVID-19 Vaccination Coverage among HCP measure data through the NHSN for at least 1 week each month for the CDC to report to CMS quarterly.
H. Policies Regarding Public Display of Measure Data for the IRF QRP
1. Background
Section 1886(j)(7)(E) of the Act requires the Secretary to establish procedures for making the IRF QRP data available to the public after ensuring that IRFs have the opportunity to review their data prior to public display. IRF QRP measure data are currently displayed on the Inpatient Rehabilitation Facilities website within Care Compare and the Provider Data Catalog. Both Care Compare and the Provider Data Catalog replaced IRF Compare and Data.Medicare.gov, which were both retired in December 2020. For a more detailed discussion about our policies regarding public display of IRF QRP measure data and procedures for the opportunity to review and correct data and information, we refer readers to the FY 2017 IRF PPS final rule (81 FR 52125 through 52131).
2. Public Reporting of the COVID-19 Vaccination Coverage Among Healthcare Personnel (HCP) Measure Beginning With the FY 2023 IRF QRP
We proposed to publicly report the COVID-19 Vaccination Coverage among Healthcare Personnel (HCP) measure beginning with the September 2022 Care Compare refresh or as soon as technically feasible based on data Start Printed Page 42401collected for Q4 2021 (October 1, 2021 through December 31, 2021). If finalized as proposed, an IRF's HCP COVID-19 vaccination coverage rates would be displayed based on one quarter of data updated quarterly. Subsequent to this, one additional quarter of data would be added to the measure calculation during each advancing refresh, until the point four full quarters of data is reached. Thereafter, the measure would be reported using four rolling quarters of data.
We invited public comment on the proposal for the public display of the measure, COVID-19 Vaccination Coverage among HCP.
The following is a summary of the public comments received on our proposal for the public display of the measure, COVID-19 Vaccination Coverage among HCP and our responses:
Comment: One commenter voiced concern that it was premature to publicly report this measure at this time due the fact the measure would need to be reported for several years and the underlying evidence needed time to become more stable. Another commenter stated that the measure is not mature enough for use in a payment program at this time, and questions the value this outdated, and potentially incomplete information would bring in FY 2023.
Response: The global outbreak of SARS-CoV-2, which resulted in the declaration of a PHE, took a significant toll on institutionalized patients, including those in IRFs, who are often at higher risk for more serious complications from the virus. We acknowledge that the science relating to SARS-CoV-2 virus is continuing to evolve, and we are still learning how effective the vaccines are against new variants of the virus that causes COVID-19. However, current information suggests that COVID-19 vaccines authorized for use in the United States offer protection against most variants in the United States.[86]
Furthermore, we do not believe that the public reporting of this information should be delayed because patients should have access to vaccination information when selecting an IRF in which they will receive care. CMS will be actively monitoring this measure and the evolving circumstances around the PHE. If substantive revisions to this measure are needed in the future, such revisions would be proposed through the notice and comment rulemaking process at that time.
Comment: Several commenters stated that if CMS adopted the COVID-19 Vaccination Coverage among HCP measure, then the data will be publicly displayed on Care Compare without proper context. They are concerned the public will not understand the legal issues providers feel pressured and/or constrained by, nor the information concerning FDA approval.
Response: The comments concerning legal risks are vague and we are not clear about the legal risks that commenters are referring to. Commenters have raised these concerns related to the vaccine's FDA approval and the inability to require their HCP to receive a COVID-19 vaccination. The COVID-19 vaccinations received Emergency Use Authorization (EUA) by the FDA. We refer readers to the FDA website for additional information related to the process of vaccination vetting and approval at https://www.fda.gov/vaccines-blood-biologics/vaccines/emergency-use-authorization-vaccines-explained. The EEOC released updated and expanded technical assistance on May 28, 2021.[87] Specifically the EEOC stated the federal equal employment opportunity (EEO) laws do not prevent an employer from requiring all employees physically entering the workplace to be vaccinated for COVID-19, so long as the employer complies with the reasonable accommodation provisions of the Americans with Disabilities Act (ADA) and Title VII of the Civil Rights Act of 1964 and other EEO considerations.
Comment: Several commenters questioned whether the COVID-19 Vaccination Coverage among HCP measure data will be of value in 2023 and beyond given the time associated with data collection, submission, and validation. While they support the rights of consumers to access real-time meaningful data to help inform healthcare decision-making, they believe that the use of a single, dated measure is not a true reflection of the safety or quality of care delivered at the IRF.
Response: We proposed the COVID-19 Vaccination Coverage among HCP measure be reported beginning with the September 2022 Care Compare refresh or as soon as technically feasible, rather than 2023. However, we acknowledge the commenters' concern with regard to timely display of publicly reported data. We believe it is important to make the most up-to-date data available to beneficiaries, which will support them in making essential decisions about health care. Based on these concerns, we believe it is appropriate to revise the measure's public reporting policy to use quarterly reporting, as opposed to averaging over four rolling quarters, which would allow the most recent quarter data to be displayed without combining it with older quarters of data. This revision would not affect the data collection schedule we proposed for submitting data to NHSN for the COVID-19 vaccination Coverage among HCP measure. This revision would simply update the way the measure's data are displayed for public reporting purposes. As always, IRFs will be given the chance to preview their COVID-19 Vaccination Coverage among HCP measure score, prior to the public posting of these data.
CMS will closely monitor this measure over the next year, and consider any adjustments that are needed with respect to the status of and the circumstances surrounding the PHE at that time. If substantive revisions are needed in the future, such revisions would be proposed through the notice and comment rulemaking process. Additionally, reporting of a new or revised measure would be addressed at the time of the notice and comment rulemaking process.
Comment: Commenters had different opinions on whether the information obtained from the COVID-19 Vaccination Coverage among HCP measure would be helpful to consumers. Some stated that it does little to guide patients and their caregivers in the discharge planning process or to distinguish IRFs from one another. Another commenter acknowledged the value of this information for public health and educational purposes, but still believes it would not be appropriate at this time to report publicly on the COVID-19 Vaccination Coverage among HCP measure for the purposes of assessing IRF quality performance.
Response: We believe remaining COVID-19- free while receiving IRF care is critically important for Medicare beneficiaries, and therefore would be helpful to consumers. We regularly perform consumer testing on measures that are available on Care Compare to ensure that Care Compare supports patients and caregivers in making Start Printed Page 42402informed choices about critical dimensions of quality. Public reporting of this measure will inform patients and caregivers on IRFs' response to the PHE.
We also disagree that the measure does little to guide the discharge planning process, but rather this measure would facilitate patient care and care coordination during the discharge planning process. A discharging hospital/facility, in collaboration with the patient and family, can use this measure to coordinate care and ensure patient preferences are considered in the discharge plan. Patients at high risk for negative outcomes due to COVID-19 (perhaps due to underlying conditions) can use healthcare provider vaccination rates when they are selecting an IRF for next-level care.
After careful consideration of the public comments, we are finalizing our proposal to publicly report the COVID-19 Vaccination Coverage among Healthcare Personnel (HCP) measure beginning with the September 2022 Care Compare refresh or as soon as technically feasible based on data collected for Q4 2021 (October 1, 2021 through December 31, 2021) with the modification that we will not finalize our plan to add one additional quarter of data during each advancing refresh, until the point that four full quarters of data is reached and then report the measure using four rolling quarters of data. We will instead only report the most recent quarter of data.
3. Public Reporting of Quality Measures in the IRF QRP With Fewer Quarters Due to COVID-19 Public Health Emergency (PHE) Exemptions
a. COVID-19 Public Health Emergency Temporary Exemptions
Under the authority of section 319 of the Public Health Service Act, the Secretary of Health and Human Services declared a public health emergency (PHE) effective as of January 27, 2020. On March 13, 2020, subsequent to a presidential declaration of national emergency under the Stafford Act, the Secretary invoked section 1135(b) of the Act (42 U.S.C. 1320b-5) to waive or modify the requirements of titles XVIII, XIX, and XXI of the Act and regulations related to the PHE for COVID-19, effective as of March 1, 2020.[88] On March 27, 2020, we sent a guidance memorandum under the subject title, “Exceptions and Extensions for Quality Reporting Requirements for Acute Care Hospitals, PPS-Exempt Cancer Hospitals, Inpatient Psychiatric Facilities, Skilled Nursing Facilities, Home Health Agencies, Hospices, Inpatient Rehabilitation Facilities, Long-Term Care Hospitals, Ambulatory Surgical Centers, Renal Dialysis Facilities, and MIPS Eligible Clinicians Affected by COVID-19” to the Medicare Learning Network (MLN) Connects Newsletter and Other Program-Specific Listserv Recipients,[89] hereafter referred to as the March 27, 2020 CMS Guidance Memo. In that memo we granted an exception to the IRF QRP reporting requirements from Q4 2019 (October 1, 2019-December 31, 2019), Q1 2020 (January 1, 2020-March 31, 2020), and Q2 2020 (April 1, 2020-June 30, 2020). We also stated that we would not publicly report any IRF QRP data that might be greatly impacted by the exceptions from Q1 and Q2 of 2020. This exception impacted the schedule for public reporting that would have included those two quarters of data.
IRF quality measures are publicly reported on Care Compare. Care Compare uses four quarters of data for IRF-PAI assessment-based measures and eight quarters for claims-based measures. Table 10 displays the original schedule for public reporting of IRF QRP measures.[90]
Start Printed Page 42403
During 2020, we conducted testing to inform decisions about publicly reporting data for those refreshes, which include partially and/or fully exempt data (discussed below). The testing helped us develop a plan for posting data that are as up-to-date as possible and that also meet acceptable standards for public reporting. We believe that the plan allows us to provide consumers with helpful information on the quality of IRF care, while also making the necessary adjustments to accommodate the exemption provided IRFs. The following sections provide the results of our testing, and explains how we used the results to develop plans for accommodating exempt and partially-exempt data in public reporting.
b. Exempted Quarters
In the March 27, 2020, Medicare Learning Network (MLN) Newsletter on Exceptions and Extensions for Quality Reporting Program (QRP) Requirements, we stated that we would not report any PAC quality data that might be greatly impacted by the exemptions granted for Quarter 1 and Quarter 2 of 2020. Given the timing of the PHE onset, we determined that we would not use IRF-PAI assessments or IRF claims from Quarter 1 and Quarter 2 of 2020 for public reporting, but that we would assess the COVID-19 PHE impact on data from Quarter 4 2019. Before proceeding with the December 2020 refresh, we conducted testing to ensure that, despite the voluntary nature of reporting for that quarter, public reporting would still meet our public reporting standards. We found the level of reporting, measured in the number of eligible stays and providers, and the reported outcomes, to be in line with levels and trends observed in FY 2018 and FY 2019. We note that Quarter 4 2019 ended before the onset of the COVID-19 pandemic in the United States. Thus, we proceeded with including these data in IRF QRP measure calculations for the December 2020 refresh.
c. Update on Data Freeze and Proposal for December 2021 Public Reporting Methodology for IRF Claims-Based and IRF-PAI Assessment-Based Measures
In addition to the March 2021 refresh, there are several other forthcoming refreshes for which the original public reporting schedules included exempted quarters of IRF QRP data. The impacted refreshes for IRF-PAI assessment and claims based measures are outlined above (Table 10). We determined that freezing the data displayed on the website with the December 2020 refresh values—that is, hold data constant after the December 2020 refresh data on the website without subsequent update—would be the most straightforward, efficient, and equitable approach for IRFs. Thus, we decided that, for as many refreshes as necessary, we would hold data constant on the website with the December 2020 data, and communicate this decision to the public.
Because December 2020 refresh data will become increasingly out-of-date and thus less useful for consumers, we Start Printed Page 42404analyzed whether it would be possible to use fewer quarters of data for one or more refreshes and thus reduce the number of refreshes that continue to display December 2020 data. Using fewer quarters of more up-to-date data requires that: (1) A sufficient percentage of IRFs would still likely have enough assessment data to report quality measures (reportability); and (2) fewer quarters would likely produce similar measure scores for providers, with similar reliability, and thus not unfairly represent the quality of care IRFs provide during the period reported in a given refresh (reliability).
To assess these criteria, we conducted reportability and reliability analysis using 3 quarters of data in a refresh, instead of the standard 4 quarters of data for reporting assessment-based measures and using 6 quarters instead of 8 for claims-based measures. Specifically, we used historical data to calculate IRF-PAI assessment-based and IRF claims-based measures under two scenarios:
(1) Standard Public Reporting (SPR) Base Scenario: We used four quarters of CY 2019 data as a proxy alternative for the exempted quarters in CY 2020 in order to compare results. For assessment-based measures, the quarters used in this scenario are Q1 through Q4 2019. For claims-based measures, the quarters used in this scenario are Q1 2018 through Q4 2019.
(2) COVID-19 Affected Reporting (CAR) Scenario: We calculated IRF QRP measures using 3 quarters (Q2 2019 through Q4 2019) of IRF QRP data for assessment-based measures, and 6 quarters (Q1 2018 through Q4 2018 and Q3 2019 through Q4 2019) for claims-based measures. The CAR scenario uses the most recently available data to simulate the public health emergency reality where quarters 1 and 2 of a calendar year must be excluded from calculation. Quarterly trends in IRF-PAI assessment-based and IRF claims-based measures indicate that these measures do not exhibit substantial seasonal variation.
To assess performance in these scenarios, we calculated the reportability as the percent of IRFs meeting the case minimum for public reporting (the public reporting threshold). To test the reliability of restricting the IRFs included in the SPR Base Scenario to those included in the CAR Scenario, we performed three tests on the set of IRFs included in both scenarios. First, we evaluated measure correlation using the Pearson and Spearman correlation coefficients, which assess the alignment of IRFs' provider scores. Second, for each scenario, we conducted a split-half reliability analysis and estimated intraclass correlation (ICC) scores, where higher scores imply better internal reliability. Modest differences in ICC scores between both scenarios would suggest that using fewer quarters of data does not impact the internal reliability of the results. Third, we estimated reliability scores where a higher value indicates that measure scores are relatively consistent for patients admitted to the same IRF and variation in the measure reflects true differences across providers. To calculate the reliability results, we restricted the IRFs included in the SPR scenario included in the CAR scenario.
Our testing indicated that the expected impact of using fewer quarters of data on reportability and reliability of IRF-PAI assessment-based measures and IRF claims-based measures is acceptable.
We proposed to use the CAR scenario as the approach for the following affected refreshes: For IRF-PAI assessment-based measures, the affected refresh is the December 2021 refresh; for claims-based measures, the affected refreshes occur from December 2021 through June 2023. For the earlier three affected refreshes (March, June, and September 2021), we decided to hold constant the Care Compare website with December 2020 data. We communicated this decision in a Public Reporting Tip Sheet, which is located at https://www.cms.gov/files/document/irfqrp-covid19prtipsheet-october-2020.pdf.
Our proposal of the CAR approach for the affected refreshes would allow us to begin displaying more recent data in December 2021, rather than continue displaying December 2020 data (Q1 2019 through Q4 2019 for assessment-based measures, Q4 2017 through Q3 2019 for claims-based measures). We believe that resuming public reporting refreshes starting in December 2021 with fewer quarters of data can assist consumers by providing more recent quality data as well as more actionable data for IRF providers. Our testing results indicate we can achieve these positive impacts with acceptable changes in reportability and reliability. Table 11 summarizes the revised schedule (that is, frozen data) and the proposed schedule (that is, using fewer quarters in the affected refreshes) for assessment-based measures. Table 12 summarizes the revised schedule (that is, frozen data) and the proposed schedule (that is, using fewer quarters in the affected refreshes) for claims-based measures.
We invited public comments on the proposal to use the CAR scenario to publicly report IRF measures for the December 2021-June 2023 refreshes.
Start Printed Page 42405

The following is a summary of the public comments received on the proposed revisions to use the CAR scenario to publicly report IRF measures for the December 2021-June 2023 refreshes and our responses:
Comment: We received a few comments on the COVID-19 Affected Reporting (CAR) scenario methodology proposed. Two commenters stated that the CAR scenario appeared to adequately ensure data reportability and reliability and also requested that CMS continue to monitor the modified Care Compare refreshes until normal reporting resumes to ensure the CAR scenario produces valid and reliable results. One commenter recommended that CMS continue using the Standard Public Reporting (SPR) base scenario, stating that it is more consistent and logical to use a continuous time-period rather than a mixture of time periods. Three commenters who disagreed with the CAR methodology did not provide specific alternative methods. However, they encouraged CMS to engage with stakeholders to determine alternative methods for updating Care Compare.
Response: We thank the commenters for their support. Regarding the use of the SPR scenario, the use of only continuous time periods would have the effect of excluding one or more quarters of data (beyond the already excluded Q1 and Q2 2020 quarters) from measure calculations, resulting in a longer freeze of the measures on Care Compare. Thus, we believe the CAR scenario to be a more appropriate choice moving forward. We agree that it will be critical to monitor measures to identify any concerning trends, and we will continue to do so as part of its routine monitoring activities to regularly assess measure performance, reliability, and reportability for all data submitted for the IRF QRP.
Comment: Most commenters expressed their appreciation for the flexibility that CMS offered to IRFs during the early months of the COVID-19 PHE in granting an exception to the IRF QRP reporting requirements from Start Printed Page 42406Q1 2020 (January 1, 2020 through March 31, 2020) and Q2 2020 (April 1, 2020 through June 30, 2020). However, a number of commenters raised concerns with CMS' proposal to utilize fewer than the standard number of quarters for public reporting of quality measures on Care Compare, since it will still include Q3 2020 (July 1, 2020 through September 30, 2020) and Q4 2020 (October 1, 2020 through December 31, 2020). Several commenters are concerned that the proposed public reporting schedule would utilize data submitted while the country was still under a PHE, particularly during the proposed Q3 2020 and Q4 2020 timeframes. A few commenters pointed out that the pandemic community infection rate surged repeatedly across different regions of the country. One commenter noted in some parts of the country the highest infection rates occurred after IRFs resumed collecting QRP data in Q3 2020. Another commenter raised concern that with fewer quarters being reported, more weight would be assigned to data reported for Q3 and Q4 2020. Several commenters urged CMS to exclude the entire calendar year 2020 data.
Response: While we understand that there are concerns related to the use of Q3 and Q4 2020 data, we do not believe that further exempting providers from QRP reporting requirements, nor the continued suspension of public reporting, are actionable solutions. We granted a 6-month exception to IRF QRP reporting requirements related to the PHE for COVID-19 under 42 CFR 412.634(c)(4)(i) of our regulations, a sufficient timeframe for IRFs to adjust to the change in care patterns associated with the PHE for COVID-19. We further believe that the public display of quality data is extremely important, and the continued need for access to IRF quality data on Care Compare by CMS beneficiaries outweighs any potential provider impacts.
We conducted testing to inform our decisions about publicly reporting data for refreshes using Q3 and Q4 2020 As discussed in section VII.H.3.c of the FY 2021 IRF PPS proposed rule (86 FR 19114 through 19115), the testing helped us develop a plan that we believe meets acceptable standards for public reporting. IRFs that believe they were disproportionately affected by the PHE may apply for an individual exception or extension to the IRF QRP reporting requirement for Q3 and/or Q4 2020. We direct readers to our regulations at 42 CFR 412.634(c). Instructions for requesting an extraordinary circumstances exemption (ECE) may be found on the IRF QRP Reconsideration and Exception and Extension web page at https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/IRF-Quality-Reporting/IRF-Quality-Reporting-Reconsideration-and-Exception-and-Extension.
Comment: One commenter stated that public reporting should be frozen until the first quarter after the end of the PHE.
Response: We disagree with the commenter about freezing the data until after the first quarter of the end of the PHE. Care Compare provides a single user-friendly interface that patients and caregivers can use to make informed decisions about healthcare based on cost, quality of care, volume of services, and other data. COVID-19 has caused CMS to take a number of actions to further protect IRF patients. Resuming public reporting will inform patients and families of more recent information on quality of care provided in IRFs. As we progress, CMS will analyze the quality measures for any significant changes, and take any actions needed to continue the improvement and protection of patient health and safety.
Comment: One commenter requested that CMS include a notation on Care Compare to explain the temporary adjustments made for the PHE. Another commenter expressed concern that the public would not have the necessary context required to interpret the data that were collected during the pandemic.
Response: We will notify consumers of the use of fewer quarters of data reported on Care Compare when the website is refreshed. However, we do not believe that posting additional explanation on how IRF measure scores may or may not be affected by the ongoing PHE would be helpful. Such messages would give the impression the data posted on Care Compare are inaccurate or cannot be used when making informed healthcare decisions, which is not the case given the extensive testing CMS conducts.
Comment: One commenter suggested that CMS conduct a complete review and update the entire Care Compare platform and its reporting metrics while the website is in a data freeze, including removing measures that are outdated.
Response: On September 3, 2020, we announced the launch of Care Compare, a streamlined redesign of eight legacy CMS healthcare compare tools that were available on Medicare.gov, including Inpatient Rehabilitation Facility Compare. We will continue to enhance the information available to patients, families, and consumers, so they can more easily learn about the quality of care nursing homes provide.
After careful consideration of the public comments, we are finalizing our proposal to use the CAR scenario to publicly report IRF measures for the December 2021-June 2023 refreshes as proposed without modification.
d. Update on Data Freeze and December 2021 Public Reporting Methodology for NHSN-Based Measures
CDC recommends using the four most recent non-contiguous non-exempted quarters of data for NHSN reporting in the IRF QRP. This non-contiguous compilation of quarterly reporting would continue until the time when four contiguous quarters of reporting resumes (based on CDC's review, this would occur in July 2022). Tables 13 and 14 display the original schedules for public reporting of IRF CDI NHSN and CAUTI NHSN measures and the HCP Influenza NHSN measure, respectively. Tables 15 and 16 summarize the revised schedule and the proposed schedules for IRF CDI and CAUTI NHSN measures and the HCP Influenza measure, respectively.
Start Printed Page 42407

Start Printed Page 42408

The following is a summary of the public comments received on the proposed schedules for IRF CDI and CAUTI NHSN measures and the HCP Influenza measure and our responses:
Comment: We received one comment regarding the appropriateness of reporting Q3 and Q4 2020 data, where the commenter believes that using Q3 and Q4 2020 data is problematic and an alternative methodology is required.
Response: As described above in our response to comments regarding the general use of Q3 and Q4 2020 data, we do not believe that further exempting providers from QRP reporting requirements, nor the continued suspension of public reporting, are actionable solutions. We further believe that the public display of quality data is extremely important, and the continued need for access to provider quality data on Care Compare by CMS beneficiaries outweighs any potential provider impacts.
After careful consideration of the public comment received, we are finalizing our proposal to publicly report the IRF CDI and CAUTI NHSN measures and the HCP Influenza measure using the four most recent non-contiguous non-exempted quarters of data until the time when four contiguous quarters of reporting resumes.
IX. Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) Policy Issues
A. Fee Schedule Adjustments for Accessories (Including Seating Systems) and Seat and Back Cushions Furnished in Connection With Group 3 or Higher Complex Rehabilitative Power Wheelchairs and Complex Rehabilitative Manual Wheelchairs
1. Background
For additional details on Medicare fee schedule payments for DMEPOS and specifically for wheelchairs and wheelchair accessories, see the interim final rule with comment period entitled “Medicare Program; Durable Medical Equipment Fee Schedule Adjustments to Resume the Transitional 50/50 Blended Rates to Provide Relief in Rural Areas and Non-Contiguous Areas” (83 FR 21912 through 21925).
a. Medicare Coding and Payment for Wheelchairs
In 1989, Medicare began making payment for durable medical equipment (DME) using fee schedule amounts calculated from supplier charges for furnishing the equipment during the 1980s, increased by annual update factors specified under the statute. In 1994, CMS in collaboration with the wheelchair manufacturing industry and national associations representing wheelchair suppliers and manufacturers replaced all Healthcare Common Procedure Coding System (HCPCS) codes and statutorily-mandated fee schedule amounts for wheelchairs with new codes and fee schedule amounts for wheelchair “bases” and separate codes for “options” or accessories furnished in connection with the various wheelchair bases. For example, a separate HCPCS code K0040 and payment was created for an adjustable angle footplate used on the various wheelchair bases. The fee schedule amounts for the separately paid and covered wheelchair options/accessories did not vary based on the type of wheelchair base furnished with the option/accessory.
Complex rehabilitative wheelchairs are generally used by patients with severe impairments. Such wheelchairs may have features such as specialty seating systems that can tilt the patient into various positions and special controls such as sip and puff versus a standard joystick. In general, the first codes for complex rehabilitative manual wheelchairs, which include adult and pediatric size wheelchairs with special seating systems, were added to the HCPCS in January 2003, although code K0005 for ultralight-weight manual wheelchairs was added to the HCPCS in 1994 and was later classified as a complex rehabilitative wheelchair in 2012. The first codes for complex rehabilitative power wheelchairs were added to the HCPCS in November 2006. These wheelchairs are further separated into “Group 2” and “Group 3” wheelchair bases based on performance capabilities such as speed, distance, and obstacle clearance. The fee schedule amounts initially established for the separately coded features such as power seating systems and sip and puff controls did not vary depending on whether they were furnished in connection with a Group 2 complex rehabilitative power wheelchair or a Group 3 complex rehabilitative power wheelchair.Start Printed Page 42409
b. DMEPOS Competitive Bidding Program (CBP)
Section 1847(a) of the Act mandates the implementation of the Medicare DMEPOS CBP in competitive bidding areas (CBAs) throughout the United States for contract award purposes for the furnishing of competitively priced items and services falling under three main categories specified in paragraph (2) of such section of the Act:
- Off-the-shelf (OTS) orthotics, for which payment would otherwise be made under section 1834(h) of the Act;
- Enteral nutrients, equipment, and supplies described in section 1842(s)(2)(D) of the Act; and
- Certain DME and medical supplies, which are covered items (as defined in section 1834(a)(13) of the Act) for which payment would otherwise be made under section 1834(a) of the Act.
Certain DME items are excluded from the DMEPOS CBP in section 1847(a)(2)(A), including certain complex rehabilitative power wheelchairs recognized by the Secretary as classified within group 3 or higher (and related accessories when furnished in connection with such wheelchairs). More recently, section 106(a) of the FCAA excluded complex rehabilitative manual wheelchairs (as determined by the Secretary), and certain manual wheelchairs (identified, as of October 1, 2018, by HCPCS codes E1235, E1236, E1237, E1238, and K0008 or any successor to such codes) and related accessories when furnished in connection with such wheelchairs from the DMEPOS CBP.
Wheelchair accessories frequently furnished in connection with manual wheelchairs include adjustable armrests, headrests, anti-tipping devices, safety belts and harnesses, adjustable angle footplates, and seat and back cushions. These accessories were included under the CBP when furnished in connection with standard manual wheelchairs from July 2013 through December 2018. Wheelchair accessories frequently furnished in connection with power wheelchairs include batteries, adjustable armrests, headrests, elevating leg rests, safety belts and harnesses, and seat and back cushions. These accessories were included under the CBP when furnished in connection with standard power wheelchairs from January 2011 through December 2018 and when furnished in connection with Group 2 complex rehabilitative power wheelchairs from January 2011 through December 2013. Wheelchair accessories frequently furnished uniquely in connection with complex rehabilitative power wheelchairs include power seating systems, special interface controls (for example, sip and puff versus joystick), and expandable controllers and other special electronics. These accessories were included under the CBP when furnished in connection with Group 2 complex rehabilitative power wheelchairs from January 2011 through December 2013. Complex rehabilitative manual wheelchairs have never been included in the CBP.
c. Group 3 or Higher Complex Rehabilitative Power Wheelchairs and Related Accessories Excluded From the CBP
Complex rehabilitative power wheelchairs classified as groups 2 and 3 were included in Round 1 of the DMEPOS CBP. Section 154(a)(1)(A) of Medicare Improvements for Patients and Providers Act (MIPPA) of 2008 (Pub. L. 110-275) amended section 1847(a)(1) of the Act to add paragraph (D) which terminated Round 1 of the DMEPOS CBP and required rebidding Round 1 for the same items and services and the same areas with some changes. Section 154(a)(1)(B) of MIPPA amended section 1847(a)(2)(A) of the Act to exclude group 3 or higher complex rehabilitative power wheelchairs and related accessories when furnished in connection with such wheelchairs from the DMEPOS CBP. Since we included group 2 complex rehabilitative power wheelchairs and related accessories (including seating systems) and seat and back cushions in Round 1 of the DMEPOS CBP, we were required to include those wheelchairs and accessories in the Round 1 Rebid of the DMEPOS CBP. The accessories (including seating systems) and seat and back cushions furnished in connection with group 2 complex rehabilitative power wheelchairs (HCPCS codes K0835 through K0843) are the same items furnished in connection with group 3 complex rehabilitative power wheelchairs (HCPCS codes K0848 through K0864). Standard power wheelchairs and related accessories were also included in the Round 1 Rebid and included accessories such as batteries that are used in both complex rehabilitative and standard power wheelchairs but did not include accessories that are only used with complex rehabilitative power wheelchairs such as power seating systems and specialty interface controls (for example, sip and puff).
The contract performance period and single payment amounts under the Round 1 Rebid of the DMEPOS CBP became effective on January 1, 2011, in the nine Round 1 Rebid areas. Therefore, contract suppliers received the single payment amounts established under the CBP for furnishing group 1 and 2 standard power wheelchair bases, group 2 complex rehabilitative power wheelchair bases, and the interchangeable accessories used with the different bases (for example, batteries used with all power wheelchairs and power seating systems used with both group 2 and 3 complex rehabilitative power wheelchairs) in the Round 1 Rebid areas. As noted above, we did not competitively bid group 3 complex rehabilitative power wheelchairs or accessories used with a group 3 complex rehabilitative power wheelchair in the Round 1 Rebid of the DMEPOS CBP, as such items were excluded from the CBP under section 1847(a)(2)(A) of the Act. Although group 2 complex rehabilitative power wheelchair bases and accessories furnished in connection with these wheelchairs were included in the Round 1 Rebid of the DMEPOS CBP, these items were not included in subsequent rounds of the DMEPOS CBP due to the low number of claims and expenditures associated with these items and our determination that including these items under the DMEPOS CBP would not result in significant savings. However, these items could be included in future rounds of the DMEPOS CBP if the number of claims and expenditures associated with these items increases.
d. Fee Schedule Adjustments
Section 1834(a)(1)(F)(ii) of the Act mandates that in the case of “covered items” furnished on or after January 1, 2016, information on the payment determined under the CBP shall be used to adjust the fee schedule amounts for an area that is not a competitive bidding area. Section 1834(a)(13) of the Act defines covered items as durable medical equipment and medical supplies. The “Medicare Program; End-Stage Renal Disease Prospective Payment System, Quality Incentive Program, and Durable Medical Equipment, Prosthetics, Orthotics, and Supplies” final rule establishing the methodology for using CBP payments to adjust fee schedule amounts was issued on November 6, 2014 (79 FR 66120). We issued a specific rule under § 414.210(g)(5) for accessories used with different types of wheelchair base equipment, such as batteries furnished in connection with standard power wheelchairs, as well as Group 2 complex rehabilitative power wheelchairs (79 FR 66223 through 66233). Our intent was that this standard fee schedule adjustment methodology would apply to both Start Printed Page 42410wheelchair accessories furnished in connection with wheelchairs that were not included under the CBP, such as batteries or power seating systems furnished in connection with Group 3 complex rehabilitative power wheelchairs, as well as wheelchair accessories furnished in connection with wheelchairs that were included in the CBP. In that rulemaking, we stated the Agency's belief that it would be unnecessarily burdensome to have different fee schedule amounts for the same item (HCPCS code) when it is used with similar, but different types of base equipment, and that the costs of furnishing the accessory should not vary significantly based on the type of base equipment it is used with (79 FR 66230). We began adjusting the fee schedule amounts for these common wheelchair accessories based on the rules in 42 CFR 414.210(g) effective on January 1, 2016.
Section 2 of the Patient Access and Medicare Protection Act of 2015 (Pub. L. 114-115) delayed the fee schedule adjustments for accessories (including seating systems) and seat and back cushions when furnished in connection with group 3 complex rehabilitative power wheelchairs until January 1, 2017. Subsequently, section 16005 of the Cures Act extended this delay in the fee schedule adjustments based on competitive bidding information from January 1, 2017 until July 1, 2017. Since Congress has acted twice to address the issue, we stated in the “Medicare Program; Durable Medical Equipment Fee Schedule Adjustments to Resume the Transitional 50/50 Blended Rates to Provide Relief in Rural Areas and Non-Contiguous Areas” interim final rule with comment period (83 FR 21912 through 21925) (hereinafter referred to as the “May 2018 IFC”) that these legislative actions highlighted a general concern regarding access to this specialized equipment by the vulnerable patient population that depends on this equipment and technology (83 FR 21919).
We discussed in the May 2018 IFC that complex rehabilitative power wheelchairs are used by patients needing functionality, such as head or sip and puff controls, power tilt or recline seating, or ventilators mounted to the wheelchair, which are not available on standard power wheelchairs. The ability and performance of the wheelchair in meeting the patients' specialized needs is critical, and most patients use wheelchair bases with group 3 level performance to meet these needs. Far fewer use group 2 wheelchair bases, which are the bases that the accessories were included with under Round 1 of the DMEPOS CBP.
Section 1847(a)(2)(A) of the Act provides the categories of items that are subject to the CBP and excludes certain complex rehabilitative power wheelchairs recognized by the Secretary as classified within group 3 or higher (and related accessories when furnished in connection with such wheelchairs). We stated in the May 2018 IFC that this statutory exclusion should inform our implementation of section 1834(a)(1)(F) of the Act such that the fee schedule amounts for wheelchair accessories and back and seat cushions used in conjunction with group 3 complex rehabilitative power wheelchairs should not be adjusted based on the methodologies set forth in § 414.210(g)(5). Therefore, as we announced in guidance available on the CMS website in June 2017 (located at https://www.cms.gov/Center/Provider-Type/Durable-Medical-Equipment-DME-Center.html), we stated in the May 2018 IFC that the fee schedule amounts for wheelchair accessories and back and seat cushions used in conjunction with group 3 power wheelchairs would continue to be based on the unadjusted fee schedule amounts updated by the covered item update specified in section 1834(a)(14) of the Act. In the May 2018 IFC (83 FR 21919) and continuation notice in 2021 (86 FR 21949), we stated that the fee schedule amounts for all other accessories and cushions used with other wheelchairs would continue to be adjusted based on information from the CBP. We are changing our position in this final rule; this payment policy for wheelchair accessories and back and seat cushion used in conjunction with group 3 power wheelchairs would also apply for accessories used in conjunction with complex rehabilitative manual wheelchairs for the reasons articulated below.
We note that recently section 106(a) of the FCAA excluded complex rehabilitative manual wheelchairs and (as determined by the Secretary), and certain manual wheelchairs (identified, as of October 1, 2018, by HCPCS codes E1235, E1236, E1237, E1238, and K0008 or any successor to such codes) and related accessories from the DMEPOS CBP. In addition, section 106(b) of this Act excluded accessories (including seating systems) and seat and back cushions when furnished in connection with these manual wheelchairs from fee schedule adjustments based on information from the DMEPOS CBP from January 1, 2020, through June 30, 2021. On June 23, 2021, we announced in guidance that we would continue the unadjusted fee schedule rates for these manual wheelchair accessories through the quarter beginning July 1, 2021. We stated in the guidance that we would continue these payment rates based on several factors. Beneficiaries with disabilities such as amyotrophic lateral sclerosis, cerebral palsy, multiple sclerosis, muscular dystrophy, spinal cord injury, and traumatic brain injury often rely on complex rehabilitative wheelchairs and accessories to maximize their function and independence. It is important to avoid any potential operational difficulties for suppliers, our partners in the Medicaid program, or private payers that have elected to rely on the DMEPOS fee schedule that could result from frequent updates to the Medicare fee schedules. Finally, this action is consistent with prior Medicare program policy actions related to similar accessories for complex power rehabilitative wheelchairs as described in section 2 of the Patient Access and Medicare Protection Act of 2015.
We received 5 timely pieces of correspondence containing comments on the May 2018 IFC regarding fee schedule adjustments for accessories (including seating systems) and seat and back cushions for Group 3 or higher complex rehabilitative power wheelchairs. The comments were from wheelchair suppliers and manufacturers as well as a patient advocacy organization.
The following is a summary of the public comments received on the Fee Schedule Amounts for Accessories Used with Group 3 Complex Rehabilitative Power Wheelchairs policy included in the May 2018 IFC and our responses:
Comment: All of the commenters supported the policy to continue paying unadjusted fee schedule amounts for accessories (including seating systems) and seat and back cushions furnished in connection with group 3 or higher complex rehabilitative power wheelchairs and recommended that the same policy be applied to wheelchair accessories (including seating systems) and seat and back cushions furnished in connection with complex rehabilitative manual wheelchairs. Commenters stated that this would ensure access to complex rehabilitative wheelchair technology Medicare beneficiaries with significant disabilities depend on for functionality and that these needs are just as important for manual wheelchair users as they are for power wheelchair users. One commenter stated that the functionality that complex rehabilitative technology provides enhances lives and prevents painful, costly and wholly preventable hospital visits and is as Start Printed Page 42411needed by a person using a manual wheelchair as it is by a person using a power wheelchair. One commenter noted that Congress has acted several times to protect complex rehabilitative wheelchair technology from payment reductions and that CMS should use its authority to do the same. One commenter stated that applying competitive bidding pricing to accessories used in connection with complex rehabilitative manual wheelchairs and not to accessories used in connection with complex rehabilitative power wheelchairs creates a disparity in that people with disabilities who use complex rehabilitative manual wheelchairs have less access to needed accessories than those using complex rehabilitative power wheelchairs and that there should be equal access for all beneficiaries who use complex rehabilitative wheelchairs.
One commenter indicated that complex rehabilitative wheelchair accessories are designed to meet a unique clinical need and are costlier to provide than standard wheelchair accessories. They also indicated that since these special accessories are not used on standard wheelchair bases, they are not items that have been included in the CBP because only standard wheelchair bases and related accessories have been included in the CBP. They stated that CMS is using information obtained through the competitive bidding of accessories used on standard wheelchairs and inappropriately applying that pricing to complex rehabilitative accessories that were not part of the CBP. This commenter indicated that the June 2017 policy clarification posted on the CMS website regarding application of competitive bidding pricing on accessories for complex rehabilitative power wheelchairs should have also applied to accessories for complex rehabilitative manual wheelchairs as well.
Response: We agree with the commenters that the issues faced by wheelchair users with significant disabilities who depend on complex rehabilitative wheelchair technology for functionality and to avoid adverse health outcomes is vitally important for this special population of wheelchair users and that this issue is no different for users of complex rehabilitative manual wheelchairs than it is for users of complex rehabilitative power wheelchairs. As noted above by a commenter, Congress has acted several times with regards to both manual and power complex rehabilitative wheelchair technology to exempt such technology from pricing reductions stemming from the CBP, specifically fee schedule adjustments based on competitive bidding pricing for accessories (including seating systems) and seat and back cushions when furnished with either Group 3 or higher complex rehabilitative power wheelchairs or complex rehabilitative manual wheelchairs. We believe that we should be consistent in applying our policies regarding pricing of accessories (including seating systems) and seat and back cushions when furnished with either Group 3 or higher complex rehabilitative power wheelchairs and complex rehabilitative manual wheelchairs to safeguard beneficiaries with significant disabilities who rely on this technology to function independently on a daily basis.
After consideration of the public comments received, we are finalizing our policy to exempt accessories (including seating systems) and seat and back cushions furnished in connection with Group 3 or higher complex rehabilitative power wheelchairs from the fee schedule adjustments using prices for these items when furnished with standard power wheelchairs or Group 2 complex rehabilitative power wheelchairs under the CBP.
Further, in light of the comments that we believe correctly point out that this issue is the same for complex rehabilitative manual wheelchairs as it is for Group 3 or higher complex rehabilitative power wheelchairs, we are extending this policy to also exempt accessories (including seating systems) and seat and back cushions furnished in connection with complex rehabilitative manual wheelchairs and other complex manual wheelchairs described by HCPCS codes E1235, E1236, E1237, E1238, and K0008 from the fee schedule adjustments based on information from the CBP. We agree with commenters that these accessories (including seating systems) and seat and back cushions are different items when furnished in connection with Group 3 or higher complex rehabilitative power wheelchairs or complex rehabilitative manual wheelchair bases, and that if these wheelchairs are excluded from the CBP by statute, then the wheelchairs and related accessories should also be excluded from the fee schedule adjustments. We believe that the combination of the more complex wheelchair bases and accessories and seat and back cushions furnished with those bases make up a completely different covered DME item than the combination of the less complex wheelchair bases and accessories and seat and back cushions. In addition, the statute excludes both related accessories furnished in connection with Group 3 or higher complex rehabilitative power wheelchair bases and more recently complex rehabilitative manual wheelchair bases from the CBP. Complex rehabilitative manual wheelchairs and manual wheelchairs described by HCPCS codes E1235, E1236, E1237, E1238, and K0008 and related accessories were not included in previous rounds of the DMEPOS CBP, and therefore, single payment amounts from the DMEPOS CBP are not available for these items. In light of comments received on this general issue, we now believe it would not be accurate or appropriate to rely on single payment amounts established under the DMEPOS CBP based on bids submitted by suppliers who are not required to use assistive technology providers to adjust the fee schedule amounts for more complex wheelchairs for patients with significant disabilities who depend on these important items to function every hour of the day.
Therefore, we are finalizing an exemption for accessories (including seating systems) and seat and back cushions furnished in connection with Group 3 or higher complex rehabilitative power wheelchairs from the fee schedule adjustments under section 1834(a)(1)(F) of the Act. In light of comments received in response to the May 2018 IFC, and out of an abundance of caution, we are also extending this exemption to accessories (including seating systems) and seat and back cushions furnished in connection with complex rehabilitative manual wheelchairs. We agree with commenters that we should treat these accessories (including seating systems) and seat and back cushions the same whether they are furnished in connection with Group 3 or higher complex rehabilitative power wheelchair or complex rehabilitative manual wheelchair bases. We note that these items are excluded from the CBP and therefore the fee schedule amounts should not be adjusted based on information from the CBP. We also note again that Congress has acted several times to delay or prohibit fee schedule adjustments for these items, and this final rule will continue to protect these items from fee schedule adjustments based on information from the DMEPOS CBP. Notably, such information from the CBP (single payment amounts) was calculated based on bids from suppliers who furnished these cushions and accessories in connection with different wheelchair bases, so we now believe this information is inapplicable in the context of payment for complex Start Printed Page 42412rehabilitative manual wheelchairs and their cushions and accessories.
B. Exclusion of Complex Rehabilitative Manual Wheelchairs and Certain Other Manual Wheelchairs From the DMEPOS Competitive Bidding Program (CBP)
Section 106(a) of the FCAA amended section 1847(a)(2)(A) of the Act to exclude complex rehabilitative manual wheelchairs, (as determined by the Secretary), certain manual wheelchairs described by HCPCS codes E1235, E1236, E1237, E1238, and K0008 or any successor codes, and related accessories from the DMEPOS CBP. Therefore, as part of the “Medicare Program; Durable Medical Equipment, Prosthetics, Orthotics, and Supplies (DMEPOS) Policy Issues and Level II of the Healthcare Common Procedure Coding System (HCPCS)” proposed rule (85 FR 70358 through 70414) (hereinafter referred to as the “November 2020 proposed rule”), we proposed to make conforming changes to the definition of “item” under § 414.402 to reflect that these wheelchairs and related accessories are excluded from the DMEPOS CBP. We proposed to edit the definition of item in § 414.402 to exclude “power wheelchairs, complex rehabilitative manual wheelchairs, manual wheelchairs described by HCPCS codes E1235, E1236, E1237, E1238, and K0008, and related accessories when furnished in connection with such wheelchairs.”
In addition, section 106(b) of the FCAA mandated that, during the period beginning on January 1, 2020 and ending June 30, 2021, CMS not adjust the Medicare fee schedule amounts for wheelchair accessories (including seating systems) and seat and back cushions furnished in connection with complex rehabilitative manual wheelchairs (determined by the Secretary as HCPCS codes E1161, E1231, E1232, E1233, E1234 and K0005) and certain manual wheelchairs currently described by HCPCS codes E1235, E1236, E1237, E1238, and K0008 based on information from the CBP. We implemented the changes to the fee schedule amounts for these items through program instructions based on the discretion provided by the FCAA.
We received 11 timely comments on the November 2020 proposed rule regarding excluding complex rehabilitative manual wheelchairs, certain other manual wheelchairs, and related accessories furnished in connection with these wheelchairs from the CBP. The comments were from wheelchair suppliers and manufacturers, as well as a national coalition of consumers and clinicians advocating for access to and coverage of assistive devices and technologies for persons with injuries, illnesses, disabilities, and chronic conditions of all ages.
The following is a summary of the public comments received on our proposal to revise the definition of “item” under § 414.402 to reflect that complex rehabilitative manual wheelchairs and related accessories are excluded from the DMEPOS CBP and our responses:
Comment: All commenters supported the exclusion of the complex rehabilitative manual wheelchairs, other manual wheelchairs and related accessories furnished in connection with these wheelchairs from the DMEPOS CBP.
Response: We thank the commenters for supporting the provisions of the proposed rule.
Comment: Several commenters stated that the accessories for these wheelchairs should also be permanently excluded from fee schedule adjustments based on pricing for the accessories when furnished in connection with other wheelchairs included under the CBP. Commenters stated that section 1834(a)(1)(F) of the Act requires CMS to adjust the fee schedule rates for “covered items,” defined as DMEPOS included in the CBP, when the same items are furnished outside of CBAs. The commenters noted that Congress excluded complex rehabilitative manual wheelchairs and related accessories from the CBP, and therefore, they cannot be “covered items” as defined by section 1834(a)(1)(F) of the Act that can be subject to CBP-based adjustments. They stated that complex rehabilitative manual wheelchairs and related accessories are not CBP items, and therefore, CMS has no data from the CBP for these covered items that they can use to adjust the fee schedule amounts for such items when furnished outside of competitive bidding areas. Commenters also stated that in 2017, CMS recognized the same implication in the context of complex rehabilitative power wheelchairs and related accessories, which Congress excluded from the CBP and, by extension, prohibited any CBP-based adjustments to their fee schedule amounts. Commenters noted that CMS, via subregulatory guidance posted on its website, stated that the statutory exclusion of complex rehabilitative power wheelchairs and related accessories under section 1847(a)(2)(A) of the Act should “inform [the agency's] implementation of section 1834(a)(1)(F) . . . such that fee schedule amounts for wheelchair accessories and seat cushions used in conjunction with group 3 complex rehabilitative power wheelchairs would not be adjusted based on the methodologies in § 414.210(g)(5).” The commenters noted that this same rationale supports a permanent exemption for complex rehabilitative manual wheelchairs and related accessories because of the enactment of section 106(a) of the FCAA and the corresponding exclusion of complex rehabilitative manual wheelchairs and related accessories from the CBP.
Response: We agree with the commenters that complex rehabilitative manual wheelchairs and certain other complex manual wheelchairs described by HCPCS codes E1235, E1236, E1237, E1238, and K0008 and related accessories should be exempt from the fee schedule adjustments under section 1834(a)(1)(F) of the Act and address this issue in detail under section III of this final rule.
After consideration of the public comments we received, we are finalizing the proposal to revise the definition of “item” under § 414.402 to conform with section 106(a) of the FCAA. The new definition of item appears in the regulation text of this final rule. In addition, as discussed in section III. of this final rule, based on public comments we received in response to the May 2018 IFC, we are finalizing a fee schedule adjustment exemption for accessories (including seating systems) and cushions used with complex manual wheelchairs and other complex manual wheelchairs described by HCPCS codes E1235, E1236, E1237, E1238, and K0008. We agree with commenters that we should treat these accessories (including seating systems) and seat and back cushions the same whether they are furnished in connection with a Group 3 or higher complex rehabilitative power wheelchair or complex rehabilitative manual wheelchair bases. We note that these items are excluded from the CBP and therefore the fee schedule amounts should not be adjusted based on information from the CBP.
X. Miscellaneous Comments
Comment: We received several additional comments that were outside the scope of the FY 2022 IRF PPS proposed rule. Specifically, we received comments regarding the facility-level adjustment factors, the inclusion of recreational therapy, and rehabilitation physician training and experience.
Response: We thank the commenters for bringing these issues to our attention, and will take these comments Start Printed Page 42413into consideration for potential policy refinements.
Comment: We received a comment in response to the proposed adoption of the COVID-19 Vaccination Coverage among HCP measure for the IRF QRP recommending CMS assess Immunization Information Systems (IIS).
Response: This comment falls outside the scope of the FY 2022 IRF PPS proposed rule.
Comment: One commenter provided a document that included a series of proposed Care Compare reforms. Another commenter provided comments relative to documentation requirements, therapy requirements, prior authorization of managed care organizations, burden in the appeals process, regulatory flexibility for participation in alternative payment models, improving PAC navigability, and changes for specialty hospitals.
Response: We thank the commenter for these suggestions, and will take these comments into consideration for potential Care Compare refinements.
XI. Provisions of the Final Regulations
In this final rule, we are adopting the provisions set forth in the FY 2022 IRF PPS proposed rule (86 FR 19086), specifically:
- We will update the CMG relative weights and average length of stay values for FY 2022, in a budget neutral manner, as discussed in section V. of this final rule.
- We will update the IRF PPS payment rates for FY 2022 by the market basket increase factor, based upon the most current data available, with a productivity adjustment required by section 1886(j)(3)(C)(ii)(I) of the Act, as described in section VI. of this final rule.
- We will update the FY 2022 IRF PPS payment rates by the FY 2022 wage index and the labor-related share in a budget-neutral manner, as discussed in section VI. of this final rule.
- We will calculate the final IRF standard payment conversion factor for FY 2022, as discussed in section VI. of this final rule.
- We will update the outlier threshold amount for FY 2022, as discussed in section VII. of this final rule.
- We will update the cost-to-charge ratio (CCR) ceiling and urban/rural average CCRs for FY 2022, as discussed in section VII. of this final rule.
The policy changes and updates to the IRF QRP for FYs 2022 and 2023 are as follows:
- Updates to quality measures and reporting requirements under the IRF QRP.
In this final rule, we are also adopting certain policy changes and provisions set forth in the interim final rule with comment period entitled “Medicare Program; Durable Medical Equipment Fee Schedule Adjustments to Resume the Transitional 50/50 Blended Rates to Provide Relief in Rural Areas and Non-Contiguous Areas” (83 FR 21912 through 21925) and the proposed rule entitled “Medicare Program; Durable Medical Equipment, Prosthetics, Orthotics, and Supplies DMEPOS) Policy Issues and Level II of the Healthcare Common Procedure Coding System (HCPCS)” (85 FR 70358 through 70414) as follows:
- Changes to exclude complex rehabilitative manual wheelchairs, certain other manual wheelchairs, and accessories furnished in connection with these wheelchairs from the DMEPOS CBP.
- Changes to exclude Group 3 or higher CRT power wheelchairs and accessories furnished in connection with these wheelchairs from the fee schedule adjustments under section 1834(a)(1)(F) of the Act.
In this final rule, we are also extending the fee schedule adjustment exclusion for Group 3 or higher CRT power wheelchairs and accessories furnished in connection with these wheelchairs to complex rehabilitative manual wheelchairs, certain other manual wheelchairs, and accessories furnished in connection with these wheelchairs as well.
XII. Collection of Information Requirements
Under the Paperwork Reduction Act of 1995 (PRA), we are required to provide 60-day notice in the Federal Register and solicit public comment before a collection of information requirement is submitted to the OMB for review and approval. To fairly evaluate whether an information collection should be approved by OMB, section 3506(c)(2)(A) of the PRA requires that we solicit comment on the following issues:
- The need for the information collection and its usefulness in carrying out the proper functions of our agency;
- The accuracy of our estimate of the information collection burden;
- The quality, utility, and clarity of the information to be collected; and
- Recommendations to minimize the information collection burden on the affected public, including automated collection techniques.
This final rule does not impose any new information collection requirements as outlined in the regulation. However, this final rule does make reference to an associated information collection that is not discussed in the regulation text contained in this document. The following is a discussion of this information collection, which has already received OMB approval.
As stated in section VII.C. of the FY 2022 IRF PPS proposed rule, for purposes of calculating the IRF Annual Increase Factor (AIF), we proposed that IRFs submit data on one new quality measure: COVID-19 Vaccination Coverage among Healthcare Personnel (HCP) beginning with the FY 2023 IRF QRP. The aforementioned measure will be collected via the following means.
A. COVID-19 Vaccination Coverage Among Healthcare Personnel (HCP) Measure
IRFs will submit data for this quality measure using the Centers for Disease Control and Prevention (CDC)/National Healthcare Safety Network (NHSN). Data submission by the NHSN occurs via a web-based tool hosted by the CDC. This reporting service is provided free of charge to healthcare facilities, including IRFs. IRFs currently utilize the NHSN for purposes of meeting other IRF QRP requirements.
We note that the CDC would account for the burden associated with the COVID-19 Vaccination Coverage among HCP measure collection under OMB control number 0920-1317 (expiration 1/31/2024). Currently, the CDC does not estimate burden for COVID-19 vaccination reporting under the CDC PRA package currently approved under OMB control number 0920-1317 because the agency has been granted a waiver under section 321 of the National Childhood Vaccine Injury Act of 1986 (Pub. L. 99-660, enacted on November 14, 1986 (NCVIA)).[91] However, we refer readers to section X.C.7. of the FY 2022 IRF PPS proposed rule, where we provided an estimate of the burden and cost to IRFs, and the CDC will include it in a revised information collection request for 0920-1317.
In section VII.C.2. of the proposed rule, we proposed to update the Transfer of Health (TOH) Information to the Patient—Post-Acute Care (PAC) measure to exclude residents discharged Start Printed Page 42414home under the care of an organized home health service or hospice. This measure was adopted in the FY 2020 IRF PPS final rule (84 FR 39099 through 39107) and burden accounted for in OMB control number 0938-0842 (expiration December 31, 2022). The finalized update to the measure's denominator does not affect the information collection burden already established.
XIII. Regulatory Impact Analysis
A. Statement of Need
This final rule updates the IRF prospective payment rates for FY 2022 as required under section 1886(j)(3)(C) of the Act and in accordance with section 1886(j)(5) of the Act, which requires the Secretary to publish in the Federal Register on or before August 1 before each FY, the classification and weighting factors for CMGs used under the IRF PPS for such FY and a description of the methodology and data used in computing the prospective payment rates under the IRF PPS for that FY. This final rule also implements section 1886(j)(3)(C) of the Act, which requires the Secretary to apply a productivity adjustment to the market basket increase factor for FY 2012 and subsequent years.
Furthermore, this final rule adopts policy changes under the statutory discretion afforded to the Secretary under section 1886(j) of the Act. We are also finalizing updates to quality measures and reporting requirements under the IRF QRP. In addition, this final rule finalizes a Medicare provision adopted in an interim final rule with comment period (IFC) issued on May 11, 2018 related to fee schedule adjustments for wheelchair accessories (including seating systems) and seat and back cushions furnished in connection with group 3 or higher complex rehabilitative power wheelchairs as well as changes to the regulations related to implementation of section 106(a) of the FCAA.
B. Overall Impact
We have examined the impacts of this rule as required by Executive Order 12866 on Regulatory Planning and Review (September 30, 1993), Executive Order 13563 on Improving Regulation and Regulatory Review (January 18, 2011), the Regulatory Flexibility Act (RFA) (September 19, 1980, Pub. L. 96-354), section 1102(b) of the Social Security Act, section 202 of the Unfunded Mandates Reform Act of 1995 (March 22, 1995; Pub. L. 104-4), Executive Order 13132 on Federalism (August 4, 1999), and the Congressional Review Act (5 U.S.C. 804(2)).
Executive Orders 12866 and 13563 direct agencies to assess all costs and benefits of available regulatory alternatives and, if regulation is necessary, to select regulatory approaches that maximize net benefits (including potential economic, environmental, public health and safety effects, distributive impacts, and equity). Section 3(f) of Executive Order 12866 defines a “significant regulatory action” as an action that is likely to result in a rule: (1) Having an annual effect on the economy of $100 million or more in any 1 year, or adversely and materially affecting a sector of the economy, productivity, competition, jobs, the environment, public health or safety, or state, local or tribal governments or communities (also referred to as “economically significant”); (2) creating a serious inconsistency or otherwise interfering with an action taken or planned by another agency; (3) materially altering the budgetary impacts of entitlement grants, user fees, or loan programs or the rights and obligations of recipients thereof; or (4) raising novel legal or policy issues arising out of legal mandates, the President's priorities, or the principles set forth in Executive Order 12866.
Section (6)(a) of Executive Order 12866 provides that a regulatory impact analysis (RIA) must be prepared for major rules with economically significant effects ($100 million or more in any 1 year). We estimate the total impact of the policy updates described in this final rule by comparing the estimated payments in FY 2022 with those in FY 2021. This analysis results in an estimated $130 million increase for FY 2022 IRF PPS payments. Additionally, we estimate that costs associated with the proposal to update the reporting requirements under the IRF QRP result in an estimated $489,536.16 addition to costs in FY 2022 for IRFs. We also estimate a $170 million dollar increase in Medicare payments for the provisions related to paying higher rates for wheelchair accessories used with complex power and manual wheelchairs for the period from FY 2022 to FY 2026. Based on our estimates OMB's Office of Information and Regulatory Affairs has determined that this rulemaking is “economically significant” as measured by the $100 million threshold, and hence also a major rule under Subtitle E of the Small Business Regulatory Enforcement Fairness Act of 1996 (also known as the Congressional Review Act).
Note that the Medicare DMEPOS provisions related to wheelchair accessories are assumed to add a total of $170 million dollars in increased Medicare payments to the overall impact of the rule from FY 2022 to FY 2026.
Also, the rule has been reviewed by OMB. Accordingly, we have prepared an RIA that, to the best of our ability, presents the costs and benefits of the rulemaking.
C. Anticipated Effects
1. Effects on IRFs and DME Suppliers
a. Effects on IRFs
The RFA requires agencies to analyze options for regulatory relief of small entities, if a rule has a significant impact on a substantial number of small entities. For purposes of the RFA, small entities include small businesses, nonprofit organizations, and small governmental jurisdictions. Most IRFs and most other providers and suppliers are small entities, either by having revenues of $8.0 million to $41.5 million or less in any 1 year depending on industry classification, or by being nonprofit organizations that are not dominant in their markets. (For details, see the Small Business Administration's final rule that set forth size standards for health care industries, at 65 FR 69432 at https://www.sba.gov/sites/default/files/2019-08/SBA%20Table%20of%20Size%20Standards_Effective%20Aug%2019%2C%202019_Rev.pdf,, effective January 1, 2017 and updated on August 19, 2019.) Because we lack data on individual hospital receipts, we cannot determine the number of small proprietary IRFs or the proportion of IRFs' revenue that is derived from Medicare payments. Therefore, we assume that all IRFs (an approximate total of 1,114 IRFs, of which approximately 54 percent are nonprofit facilities) are considered small entities and that Medicare payment constitutes the majority of their revenues. HHS generally uses a revenue impact of 3 to 5 percent as a significance threshold under the RFA. As shown in Table 17, we estimate that the net revenue impact of this final rule on all IRFs is to increase estimated payments by approximately 1.5 percent. The rates and policies set forth in this final rule will not have a significant impact (not greater than 3 percent) on a substantial number of small entities. The estimated impact on small entities is shown in Table 17. MACs are not considered to be small entities. Individuals and states are not included in the definition of a small entity.Start Printed Page 42415
In addition, section 1102(b) of the Act requires us to prepare an RIA if a rule may have a significant impact on the operations of a substantial number of small rural hospitals. This analysis must conform to the provisions of section 604 of the RFA. For purposes of section 1102(b) of the Act, we define a small rural hospital as a hospital that is located outside of a Metropolitan Statistical Area and has fewer than 100 beds. As shown in Table 17, we estimate that the net revenue impact of this final rule on rural IRFs is to increase estimated payments by approximately 1.6 percent based on the data of the 133 rural units and 12 rural hospitals in our database of 1,114 IRFs for which data were available. We estimate an overall impact for rural IRFs in all areas between -0.1 percent and 3.0 percent. The Secretary hereby certifies that this final rule will not have a significant impact on a substantial number of small entities.
Section 202 of the Unfunded Mandates Reform Act of 1995 (Pub. L. 104-04, enacted on March 22, 1995) (UMRA) also requires that agencies assess anticipated costs and benefits before issuing any rule whose mandates require spending in any 1 year of $100 million in 1995 dollars, updated annually for inflation. In 2021, that threshold is approximately $158 million. This final rule does not mandate any requirements for State, local, or tribal governments, or for the private sector.
Executive Order 13132 establishes certain requirements that an agency must meet when it issues a proposed rule (and subsequent final rule) that imposes substantial direct requirement costs on state and local governments, preempts state law, or otherwise has federalism implications. As stated, this final rule will not have a substantial effect on state and local governments, preempt state law, or otherwise have a federalism implication.
b. Effects on DME Suppliers
The RFA requires agencies to analyze options for regulatory relief of small entities, if a rule has a significant impact on a substantial number of small entities. The DMEPOS provisions of this rule are not considered to have a significant impact on a substantial number of small entities as payments continue at their current levels.
In addition, section 1102(b) of the Act requires us to prepare an RIA if a rule may have a significant impact on the operations of a substantial number of small rural hospitals. The DMEPOS provisions of this rule are not considered to have a significant impact on the operations of a substantial number of small rural hospitals.
Section 202 of the UMRA also requires that agencies assess anticipated costs and benefits before issuing any rule whose mandates require spending in any 1 year of $100 million in 1995 dollars, updated annually for inflation. In 2021, that threshold is approximately $158 million. The DMEPOS provisions of this rule do not mandate any requirements for State, local, or tribal governments, or for the private sector.
Executive Order 13132 establishes certain requirements that an agency must meet when it issues a proposed rule (and subsequent final rule) that imposes substantial direct requirement costs on state and local governments, preempts state law, or otherwise has federalism implications. As stated, the DMEPOS provisions of this final rule will not have a substantial effect on state and local governments, preempt state law, or otherwise have a federalism implication.
2. Detailed Economic Analysis
This final rule will update the IRF PPS rates contained in the FY 2021 IRF PPS final rule (85 FR 48424). Specifically, this final rule will update the CMG relative weights and ALOS values, the wage index, and the outlier threshold for high-cost cases. This final rule will apply a productivity adjustment to the FY 2022 IRF market basket increase factor in accordance with section 1886(j)(3)(C)(ii)(I) of the Act.
We estimate that the impact of the changes and updates described in this final rule would be a net estimated increase of $130 million in payments to IRF providers. The impact analysis in Table 17 of this final rule represents the projected effects of the updates to IRF PPS payments for FY 2022 compared with the estimated IRF PPS payments in FY 2021. We determine the effects by estimating payments while holding all other payment variables constant. We use the best data available, but we do not attempt to predict behavioral responses to these changes, and we do not make adjustments for future changes in such variables as number of discharges or case-mix.
We note that certain events may combine to limit the scope or accuracy of our impact analysis, because such an analysis is future-oriented and, thus, susceptible to forecasting errors because of other changes in the forecasted impact time period. Some examples could be legislative changes made by the Congress to the Medicare program that would impact program funding, or changes specifically related to IRFs. Although some of these changes may not necessarily be specific to the IRF PPS, the nature of the Medicare program is such that the changes may interact, and the complexity of the interaction of these changes could make it difficult to predict accurately the full scope of the impact upon IRFs.
In updating the rates for FY 2022, we are implementing the standard annual revisions described in this final rule (for example, the update to the wage index and market basket increase factor used to adjust the Federal rates). We are also reducing the FY 2022 IRF market basket increase factor by a productivity adjustment in accordance with section 1886(j)(3)(C)(ii)(I) of the Act. We estimate the total increase in payments to IRFs in FY 2022, relative to FY 2021, would be approximately $130 million.
This estimate is derived from the application of the FY 2022 IRF market basket increase factor, as reduced by a productivity adjustment in accordance with section 1886(j)(3)(C)(ii)(I) of the Act, which yields an estimated increase in aggregate payments to IRFs of $160 million. However, there is an estimated $30 million decrease in aggregate payments to IRFs due to the update to the outlier threshold amount. Therefore, we estimate that these updates would result in a net increase in estimated payments of $130 million from FY 2021 to FY 2022.
The effects of the updates that impact IRF PPS payment rates are shown in Table 17. The following updates that affect the IRF PPS payment rates are discussed separately below:
- The effects of the update to the outlier threshold amount, from approximately 3.4 percent to 3.0 percent of total estimated payments for FY 2022, consistent with section 1886(j)(4) of the Act.
- The effects of the annual market basket update (using the IRF market basket) to IRF PPS payment rates, as required by sections 1886(j)(3)(A)(i) and (j)(3)(C) of the Act, including a productivity adjustment in accordance with section 1886(j)(3)(C)(i)(I) of the Act.
- The effects of applying the budget-neutral labor-related share and wage index adjustment, as required under section 1886(j)(6) of the Act.
- The effects of the budget-neutral changes to the CMG relative weights and ALOS values under the authority of section 1886(j)(2)(C)(i) of the Act.
- The total change in estimated payments based on the FY 2022 payment changes relative to the estimated FY 2021 payments.Start Printed Page 42416
3. Description of Table 17
Table 17 shows the overall impact on the 1,114 IRFs included in the analysis.
The next 12 rows of Table 17 contain IRFs categorized according to their geographic location, designation as either a freestanding hospital or a unit of a hospital, and by type of ownership; all urban, which is further divided into urban units of a hospital, urban freestanding hospitals, and by type of ownership; and all rural, which is further divided into rural units of a hospital, rural freestanding hospitals, and by type of ownership. There are 969 IRFs located in urban areas included in our analysis. Among these, there are 665 IRF units of hospitals located in urban areas and 304 freestanding IRF hospitals located in urban areas. There are 145 IRFs located in rural areas included in our analysis. Among these, there are 133 IRF units of hospitals located in rural areas and 12 freestanding IRF hospitals located in rural areas. There are 407 for-profit IRFs. Among these, there are 373 IRFs in urban areas and 34 IRFs in rural areas. There are 599 non-profit IRFs. Among these, there are 509 urban IRFs and 90 rural IRFs. There are 108 government-owned IRFs. Among these, there are 87 urban IRFs and 21 rural IRFs.
The remaining four parts of Table 17 show IRFs grouped by their geographic location within a region, by teaching status, and by DSH patient percentage (PP). First, IRFs located in urban areas are categorized for their location within a particular one of the nine Census geographic regions. Second, IRFs located in rural areas are categorized for their location within a particular one of the nine Census geographic regions. In some cases, especially for rural IRFs located in the New England, Mountain, and Pacific regions, the number of IRFs represented is small. IRFs are then grouped by teaching status, including non-teaching IRFs, IRFs with an intern and resident to average daily census (ADC) ratio less than 10 percent, IRFs with an intern and resident to ADC ratio greater than or equal to 10 percent and less than or equal to 19 percent, and IRFs with an intern and resident to ADC ratio greater than 19 percent. Finally, IRFs are grouped by DSH PP, including IRFs with zero DSH PP, IRFs with a DSH PP less than 5 percent, IRFs with a DSH PP between 5 and less than 10 percent, IRFs with a DSH PP between 10 and 20 percent, and IRFs with a DSH PP greater than 20 percent.
The estimated impacts of each policy described in this rule to the facility categories listed are shown in the columns of Table 17. The description of each column is as follows:
- Column (1) shows the facility classification categories.
- Column (2) shows the number of IRFs in each category in our FY 2022 analysis file.
- Column (3) shows the number of cases in each category in our FY 2022 analysis file.
- Column (4) shows the estimated effect of the adjustment to the outlier threshold amount.
- Column (5) shows the estimated effect of the update to the IRF labor-related share and wage index, in a budget-neutral manner.
- Column (6) shows the estimated effect of the update to the CMG relative weights and ALOS values, in a budget-neutral manner.
- Column (7) compares our estimates of the payments per discharge, incorporating all of the policies reflected in this final rule for FY 2022 to our estimates of payments per discharge in FY 2021.
The average estimated increase for all IRFs is approximately 1.5 percent. This estimated net increase includes the effects of the IRF market basket increase factor for FY 2022 of 1.9 percent update based on an IRF market basket update of 2.6 percent, less a 0.7 percentage point productivity adjustment, as required by section 1886(j)(3)(C)(ii)(I) of the Act. It also includes the approximate 0.4 percent overall decrease in estimated IRF outlier payments from the update to the outlier threshold amount. Since we are making the updates to the IRF wage index, labor-related share and the CMG relative weights in a budget-neutral manner, they will not be expected to affect total estimated IRF payments in the aggregate. However, as described in more detail in each section, they will be expected to affect the estimated distribution of payments among providers.
Start Printed Page 42417
Start Printed Page 42418

4. Impact of the Update to the Outlier Threshold Amount
The estimated effects of the update to the outlier threshold adjustment are presented in column 4 of Table 17.
For the FY 2022 proposed rule, we used preliminary FY 2020 IRF claims data, and, based on that preliminary analysis, we estimated that IRF outlier payments as a percentage of total estimated IRF payments would be 3.3 percent in FY 2022. As we typically do between the proposed and final rules each year, we updated our FY 2020 IRF claims data to ensure that we are using the most recent available data in setting IRF payments. Therefore, based on updated analysis of the most recent IRF claims data for this final rule, we estimate that IRF outlier payments as a percentage of total estimated IRF payments are 3.4 percent in FY 2022. Thus, we are adjusting the outlier threshold amount in this final rule to maintain total estimated outlier payments equal to 3 percent of total estimated payments in FY 2022. The estimated change in total IRF payments for FY 2022, therefore, includes an approximate 0.4 percentage point decrease in payments because the estimated outlier portion of total payments is estimated to decrease from approximately 3.4 percent to 3 percent.
The impact of this outlier adjustment update (as shown in column 4 of Table 17) is to decrease estimated overall payments to IRFs by 0.4 percentage point.
5. Impact of the Wage Index and Labor-Related Share
In column 5 of Table 17, we present the effects of the budget-neutral update of the wage index and labor-related share. The changes to the wage index and the labor-related share are discussed together because the wage index is applied to the labor-related share portion of payments, so the changes in the two have a combined effect on payments to providers. As discussed in section VI.C. of this final rule, we are updating the labor-related share from 73.0 percent in FY 2021 to 72.9 percent in FY 2022.
6. Impact of the Update to the CMG Relative Weights and ALOS Values.
In column 7 of Table 17, we present the effects of the budget-neutral update of the CMG relative weights and ALOS values. In the aggregate, we do not estimate that these updates will affect overall estimated payments of IRFs. However, we do expect these updates to have small distributional effects.
7. Effects of Requirements for the IRF QRP for FY 2022
In accordance with section 1886(j)(7)(A) of the Act, the Secretary must reduce by 2 percentage points the annual market basket increase factor otherwise applicable to an IRF for a fiscal year if the IRF does not comply with the requirements of the IRF QRP for that fiscal year. In section VII.A of this final rule, we discussed the method for applying the 2 percentage point reduction to IRFs that fail to meet the IRF QRP requirements. As discussed in section VIII C. of this final rule, we are finalizing the adoption of one measure to the IRF QRP beginning with the FY 2023 IRF QRP, the COVID-19 Vaccination Coverage among Healthcare Personnel (HCP) measure, and finalizing our proposal to update the denominator of the Transfer of Health (TOH) Information to the Patient—Post-Acute Care (PAC) measure beginning with the FY 2023 IRF QRP. As discussed in section VIII.G. of this final rule, we are finalizing the CDC/NHSN web-based surveillance system for data submission for the COVID-19 Vaccination Coverage among HCP measure. As discussed in section VIII.H., we are finalizing two public reporting policies. The first is to publicly report the COVID-19 Vaccination Coverage among Healthcare Personnel (HCP) measure beginning with the September 2022 Care Compare refresh or as soon as technically feasible based on data collected for Q4 2021 (October 1, 2021 through December 31, 2021) using the most recent quarter of data. Second, we are finalizing use of the CAR scenario to publicly report IRF QRP measures for the December 2021-June 2023 refreshes and to publicly report the NHSN Facility-wide Inpatient Hospital-onset Clostridium difficile Infection (CDI) Outcome Measure (NQF #1717), the NHSN Catheter Associated Urinary Tract Infection (CAUTI) Outcome Measure (NQF #0138), and the NHSN Influenza Vaccination among HCP (NQF #0431) measure using the four most recent non-contiguous non-exempted quarters of data until the time when four contiguous quarters of reporting resumes.
We believe that the burden associated with the IRF QRP is the time and effort associated with complying with the requirements of the IRF QRP. The finalized IRF QRP requirements add no additional burden to the active collection under OMB control number 0938-0842 (expiration 12/31/2022). Currently, the CDC does not estimate burden for COVID-19 vaccination reporting under the CDC PRA package currently approved under OMB control number 0920-1317 because the agency has been granted a waiver under section 321 of the NCVIA. However, CMS has provided an estimate of burden and cost for IRFs here, and the CDC will include it in a revised information collection request for 0920-1317. Consistent with the CDC's experience of collecting data Start Printed Page 42419using the NHSN, we estimate that it would take each IRF an average of 1 hour per month to collect data for the COVID-19 Vaccination Coverage among HCP measure and enter it into NHSN. We have estimated the time to complete this entire activity, since it could vary based on provider systems and staff availability. We believe it would take an administrative assistant from 45 minutes up to 1 hour and 15 minutes to enter this data into NHSN. For the purposes of calculating the costs associated with the collection of information requirements, we obtained mean hourly wages from the U.S. Bureau of Labor Statistics' (BLS) May 2019 National Occupational Employment and Wage Estimates.[92] To account for overhead and fringe benefits, we have doubled the hourly wage. These amounts are detailed in Table 18.

Based on the time range, it would cost each IRF between $27.47 and $45.78 each month or an average cost of $36.62 each month, and between $329.64 and $549.36 each year. We believe the data submission for the COVID-19 Vaccination Coverage among HCP measure would cause IRFs to incur additional average burden of 12 hours per year for each IRF and a total annual burden of 13,368 hours across all IRFs. The estimated annual cost across all 1,114 IRFs in the U.S. for the submission of the COVID-19 Vaccination Coverage among HCP measure would range from $367,218.96 and $611,987.04 with an average of $489,536.16.
We recognize that many IRFs may also be reporting other COVID-19 data to HHS. However, we believe the benefits of reporting data on the COVID-19 Vaccination Coverage among HCP measure to assess whether the potential spread of COVID-19 among their HCP, and the risk of transmission of COVID-19 within IRFs, and to help sustain the ability of IRFs to continue serving their communities throughout the PHE and beyond outweigh the costs of reporting. We received no comments on the estimated time to collect data and enter it into NHSN.
8. Effects of Requirements for the DMEPOS Provisions
a. Fee Schedule Adjustments for Accessories (Including Seating Systems) and Seat and Back Cushions Furnished in Connection With Group 3 or Higher Complex Rehabilitative Power Wheelchairs and Complex Rehabilitative Manual Wheelchairs
In this final rule, we are finalizing a policy exempting wheelchair accessories furnished in connection with Group 3 complex rehabilitative power wheelchairs from fee schedule adjustments based on information from the DMEPOS CBP. The cost of this provision is estimated to be $130 million dollars in increased Medicare payments with $30 million dollars in increased beneficiary copayments from FY 2022 to FY 2026. This cost can be considered in the FY 2022 President's budget baseline. We are also finalizing a policy exempting wheelchair accessories furnished in connection with complex rehabilitative manual wheelchairs from fee schedule adjustments based on information from the DMEPOS CBP. This policy was not reflected in the FY 2022 President's budget baseline and has an estimated cost of $40 million dollars in increased Medicare payments with $10 million dollars in increased beneficiary copayments from FY 2022 to FY 2026.
b. Exclusion of Complex Rehabilitative Manual Wheelchairs and Certain Other Manual Wheelchairs From the DMEPOS CBP
This rule finalizes conforming changes to the regulations at 42 CFR 414.402 to revise the definition of “item” at 42 CFR 414.402 under the CBP to exclude complex rehabilitative manual wheelchairs and certain other wheelchairs from the CBP and is estimated to have no fiscal impact and is considered in the baseline of the FY 2022 President's Budget.
D. Alternatives Considered
The following is a discussion of the alternatives considered for the IRF PPS updates contained in this final rule.
Section 1886(j)(3)(C) of the Act requires the Secretary to update the IRF PPS payment rates by an increase factor that reflects changes over time in the prices of an appropriate mix of goods and services included in the covered IRF services.
As noted previously in this final rule, section 1886(j)(3)(C)(ii)(I) of the Act requires the Secretary to apply a productivity adjustment to the market basket increase factor for FY 2022. Thus, in accordance with section 1886(j)(3)(C) of the Act, we update the IRF prospective payments in this final rule by 1.9 percent (which equals the 2.6 percent estimated IRF market basket increase factor for FY 2022 reduced by a 0.7 percentage point productivity adjustment as determined under section 1886(b)(3)(B)(xi)(II) of the Act (as required by section 1886(j)(3)(C)(ii)(I) of the Act)).
We considered utilizing FY 2019 claims data to update the prospective payment rates for FY 2022 due to the potential effects of the PHE on the FY 2020 IRF claims data. However, it has been our long-standing practice to utilize the most recent full fiscal year of data to update the prospective payment rates, as this data is generally considered to be the best overall predictor of experience in the upcoming fiscal year. Additionally, the FY 2019 data does not reflect any of the changes to the CMG definitions or the data used to classify IRF patients into CMGs that became effective in FY 2020 and will continue to be used in FY 2022. As such, we believe it would be appropriate to utilize FY 2020 data to update the prospective payment rates for FY 2022 at this time. While we believe maintaining our existing methodology of utilizing the most recent available IRF data to update the prospective payment rates for FY 2022 is appropriate, we solicited comment in the FY 2020 proposed rule on the use of FY 2019 data to update the prospective payment rates for FY 2022. Start Printed Page 42420For more information on the proposed FY 2022 estimated impacts utilizing FY 2019 claims data, we refer readers to the FY 2022 IRF PPS proposed rule (86 FR 19086). As the comments received in response to this solicitation are pertinent to the updates in this final rule, we are providing a summary of the feedback we received from stakeholders regarding this solicitation in this final rule.
The following is a summary of the comments received on the use of FY 2019 data to update the prospective rates for FY 2022 and our responses:
Comment: In general, the majority of commenters supported the use of FY 2020 data to update the prospective payment rates for FY 2022. Several commenters suggested that FY 2020 data should be used to update the payment rates for FY 2022 as these data reflect changes in IRF care related to the pandemic and will therefore be more likely to reflect IRF utilization in FY 2022, as COVID-19 will continue to impact IRFs in the future. Additionally, these commenters supported the use of FY 2020 data noting that it reflects changes to the CMG definitions that were implemented in FY 2020 and that will continue to be used in FY 2022. In contrast, a few commenters expressed concern with the proposed use of FY 2020 data to update the prospective payment rates for FY 2020 and recommended that CMS use FY 2019 data for this purpose. These commenters stated that they believe the FY 2020 data was heavily impacted by the pandemic and would result in skewed relative weights and an inflated outlier threshold and suggested that FY 2019 data would be more likely to reflect IRF utilization in FY 2022 as the pandemic continues to subside. A few of these commenters requested that CMS use FY 2019 claims data to update the relative weights and the outlier threshold while other commenters requested that CMS maintain the relative weights and outlier threshold at the current FY 2021 levels for FY 2022.
Response: We appreciate the commenters' support of using FY 2020 data to update the prospective payment rates for FY 2022. It has been our longstanding practice to use the most recent full fiscal year of claims data available to update the prospective payment rates as we believe this data is reflective of the current Medicare IRF population and is generally the best overall predictor of experience in the upcoming fiscal year. We also agree with the commenters' recommendation to use FY 2020 data for rate setting purposes as this data reflects the changes to the CMG definitions that were implemented in FY 2020 and that will continue to be used in FY 2022.
We appreciate the commenters' feedback regarding how the PHE has impacted individual facilities and acknowledge that the PHE impacted many aspects of IRF operations. However, we disagree with the commenters' assertions that the FY 2020 claims data were impacted by the PHE to the extent that they would be unsuitable to use for payment updates under the IRF PPS. An analysis of FY 2020 IRF claims data indicates that admissions under the IRF PPS dropped by approximately 7 percent overall compared to FY 2019. Decreased admissions were observed across almost all conditions in the IRF setting, with the largest declines occurring among patients treated for lower-extremity joint replacements and pain syndrome. However, there were only slight changes observed in the share of IRF admissions across all RICs in FY 2020 compared to FY 2019. For example, the share of IRF admissions for lower-extremity joint replacements dropped from 3.7 percent in FY 2019 to 3.0 percent in FY 2020, while the share of IRF admissions for pain syndrome dropped from 0.3 percent in FY 2019 to 0.2 percent in FY 2020.
Additionally, we attempted to approximate changes in IRF utilization in the FY 2020 IRF claims data that could be attributable to the PHE. When the PHE for COVID-19 was declared, we announced a number of waivers to provide regulatory flexibilities to IRF providers. When submitting claims under these waivers, IRFs billed Medicare using a “DR” condition code on the claim. To approximate the number of IRF stays for admissions that would not have been expected in the absence of the PHE, we identified claims that included a COVID-19 ICD-10 diagnosis code and claims that could be considered waiver admissions, as identified by the presence of a “DR” condition code on the claim. While we are not able to definitively identify claims that are solely attributable to the PHE based on the presence of a COVID-19 diagnosis code or waiver code on the claim, this methodology allows us to understand the overall utilization of the waivers and the overall frequency of COVID-19 diagnoses among the IRF population. This analysis indicated that approximately 1.0 percent of IRF stays included a COVID-19 ICD-10 diagnosis code, while 4.2 percent of IRF stays could be considered waiver admissions. This would suggest that the FY 2020 IRF claims data were not disproportionally impacted by the PHE, as the overwhelming majority of IRF beneficiaries entered into IRF stays in FY 2020 as they would have in any other year. Therefore, we believe this data is representative of typical IRF utilization of the current Medicare population and would therefore be appropriate to use when updating the prospective payment rates for FY 2022, as well as updates to the outlier threshold and the relative weights.
We do not believe it would be appropriate to freeze the outlier threshold and the relative weights at their current FY 2021 levels for FY 2022. The annual updates to the outlier threshold and the relative weights are intended to better align IRF payments with the costs of caring for IRF patients and to ensure that IRFs will be appropriately compensated for treating unusually high-cost patients while taking into account changes in IRF utilization as well as changes in estimated costs and payments from year to year. Therefore, we believe it is appropriate to update these values for FY 2022 using FY 2020 claims data, as proposed in the FY 2022 proposed rule.
Comment: One commenter suggested that CMS try to isolate the effects of the PHE in the IRF setting and recommended that CMS exclude claims with a COVID-19 diagnosis and claims considered to be wavier admissions from the 2020 data when setting the outlier threshold as these claims may be atypical.
Response: As discussed above, we are not able to definitively identify claims that are directly attributable to the PHE, such as IRF stays that would not qualify for IRF level services in the absence of the PHE, solely based on the presence of a COVID-19 diagnosis code or waiver code on the claim. Additional information beyond the presence of these codes would be necessary to determine if the stay would qualify for IRF level services through review of IRF medical records. However, given the significant amount of resources that would be required to complete a comprehensive review of the medical records for these cases by both IRFs and CMS contractors we do not believe this undertaking is feasible at this time. As such, we do not believe it would be appropriate to exclude claims from, or otherwise apply adjustments to, the underlying pool of claims data that is used to determine adjustments to the IRF prospective payment rates. We also agree with the commenters' assertion that IRFs will continue to be impacted by the PHE in the near future and therefore it would be appropriate to maintain claims with a COVID-19 ICD-10 diagnosis code in the methodology used to determine adjustments under Start Printed Page 42421the IRF PPS as IRFs will continue to treat patients with a COVID-19 diagnosis in the near future.
Comment: A few commenters noted analysis presented in other proposed payment rules related to other Medicare settings and indicated that the proposal to use FY 2020 data to update the IRF prospective payment rates for FY 2022 was inconsistent with CMS' proposed policies in other Medicare settings. Some commenters requested that additional data and analysis be shared with stakeholders to allow them to more fully assess the effects of the pandemic in the IRF setting and encouraged us to continue evaluating the effects of the PHE and to provide additional analysis in future years.
Response: The proposed use of FY 2020 claims data to update the prospective payment rates for FY 2022 was based on analysis of both FY 2019 and FY 2020 IRF claims data. As discussed above, we did not observe increases and decreases in IRF utilization in the FY 2020 claims data of the same magnitude observed in other Medicare settings and described in other Medicare proposed rules. As such, we believe it would be appropriate to use the FY 2020 IRF claims data to update the prospective payment rates for FY 2022. We appreciate the commenters' feedback regarding the types of information that would be most useful to them in assessing the effects of the PHE in the IRF setting. We also appreciate the commenters' concerns regarding the impacts of the PHE in the IRF setting and will continue to monitor the IRF data to ensure that IRF payments are appropriately aligned with costs of care.
After careful consideration of the comments we received in response to this solicitation, we are finalizing the use of FY 2020 claims data, as described in the FY 2022 proposed rule, to update the prospective rates for FY 2022.
We considered maintaining the existing CMG relative weights and ALOS values for FY 2022. However, in light of recently available data and our desire to ensure that the CMG relative weights and ALOS values are as reflective as possible of recent changes in IRF utilization and case mix, at this time we believe that it is appropriate to update the CMG relative weights and ALOS values using FY 2020 claims data to ensure that IRF PPS payments continue to reflect as accurately as possible the current costs of care in IRFs.
We also considered maintaining the existing outlier threshold amount for FY 2022. As outlier payments are a redistribution of payment, it is important to adjust the outlier threshold amount to maintain the targeted 3 percent outlier pool as closely as possible. Maintaining an outlier threshold that would yield estimated outlier payments greater than 3 percent would leave less payment available to cover the costs of non-outlier cases. Therefore, analysis of updated FY 2020 data indicates that estimated outlier payments would be greater than 3 percent of total estimated payments for FY 2022, by approximately 0.4 percent. Consequently, we are adjusting the outlier threshold amount in this final rule to reflect a 0.4 percentage point decrease thereby setting the total outlier payments equal to 3 percent, instead of 3.4 percent, of aggregate estimated payments in FY 2022.
E. Regulatory Review Costs
If regulations impose administrative costs on private entities, such as the time needed to read and interpret this final rule, we should estimate the cost associated with regulatory review. Due to the uncertainty involved with accurately quantifying the number of entities that will review the rule, we assume that the total number of unique commenters on the FY 2022 IRF PPS proposed rule will be the number of reviewers of this final rule. We acknowledge that this assumption may understate or overstate the costs of reviewing this final rule. It is possible that not all commenters reviewed the FY 2022 IRF PPS proposed rule in detail, and it is also possible that some reviewers chose not to comment on the FY 2022 proposed rule. For these reasons, we thought that the number of commenters would be a fair estimate of the number of reviewers of this final rule.
We also recognize that different types of entities are in many cases affected by mutually exclusive sections of this final rule, and therefore, for the purposes of our estimate we assume that each reviewer reads approximately 50 percent of the rule. We sought comments on this assumption.
Using the national mean hourly wage data from the May 2020 BLS for Occupational Employment Statistics (OES) for medical and health service managers (SOC 11-9111), we estimate that the cost of reviewing this rule is $114.24 per hour, including overhead and fringe benefits (https://www.bls.gov/oes/current/oes_nat.htm). Assuming an average reading speed, we estimate that it would take approximately 3 hours for the staff to review half of this final rule. For each reviewer of the rule, the estimated cost is $342.72 (3 hours × $114.24). Therefore, we estimate that the total cost of reviewing this regulation is $1,137,144.96 ($342.72 × (2,668 IRF reviewers and 650 DME reviewers).
F. Accounting Statement and Table
As required by OMB Circular A-4 (available at https://www.whitehouse.gov/sites/whitehouse.gov/files/omb/circulars/A4/a-4.pdf), in Tables 19, 20, and 21, we have prepared accounting statements showing the classification of the expenditures associated with the provisions of this final rule. Table 19 provides our best estimate of the increase in Medicare payments under the IRF PPS as a result of the updates presented in this final rule based on the data for 1,114 IRFs in our database. Tables 20 and 21 provides our best estimate of the impacts associated with the DME provisions in this final rule.
Start Printed Page 42422


G. Conclusion
Overall, the estimated payments per discharge for IRFs in FY 2022 are projected to increase by 1.5 percent, compared with the estimated payments in FY 2021, as reflected in column 7 of Table 17.
IRF payments per discharge are estimated to increase by 1.5 percent in urban areas and 1.6 percent in rural areas, compared with estimated FY 2021 payments. Payments per discharge to rehabilitation units are estimated to increase 1.2 percent in urban areas and 1.4 percent in rural areas. Payments per discharge to freestanding rehabilitation hospitals are estimated to increase 1.8 percent in urban areas and increase 2.3 percent in rural areas.
Overall, IRFs are estimated to experience a net increase in payments as a result of the policies in this final rule. The largest payment increase is estimated to be a 3.0 percent increase for rural IRFs located in the rural South Atlantic region. The analysis above, together with the remainder of this preamble, provides an RIA.
The Medicare DMEPOS provisions will continue payments for affected items at the current levels.
In accordance with the provisions of Executive Order 12866, this regulation was reviewed by OMB.
Chiquita Brooks-LaSure,
Administrator of the Centers for Medicare & Medicaid Services, approved this document on July 21, 2021.
Start List of SubjectsList of Subjects in 42 CFR Part 414
- Administrative practice and procedure
- Biologics
- Diseases
- Drugs
- Health facilities
- Health professions
- Medicare
- Reporting and recordkeeping requirements
For the reasons set forth in the preamble, the Centers for Medicare & Medicaid Services amends 42 CFR Chapter IV as follows:
Start PartPART 414—PAYMENT FOR PART B MEDICAL AND OTHER SERVICES
End Part Start Amendment Part1. The authority citation for part 414 continues to read as follows:
End Amendment Part Start Amendment Part2. In § 414.402 amend the definition of “Item” by revising paragraph (1) introductory text to read as follows:
End Amendment PartStart SignatureDefinitions.* * * * *Item * * *
(1) Durable medical equipment (DME) other than class III devices under the Federal Food, Drug and Cosmetic Act, as defined in § 414.202, group 3 complex rehabilitative power wheelchairs, complex rehabilitative manual wheelchairs, manual wheelchairs described by HCPCS codes E1235, E1236, E1237, E1238, and K0008, and related accessories when furnished in connection with such wheelchairs, and further classified into the following categories:
* * * * *End Signature End Supplemental InformationDated: July 27, 2021.
Xavier Becerra,
Secretary, Department of Health and Human Services.
Footnotes
1. Patel A, Jernigan DB. Initial Public Health Response and Interim Clinical Guidance for the 2019 Novel Coronavirus Outbreak—United States, December 31, 2019—February 4, 2020. MMWR Morb Mortal Wkly Rep 2020;69:140-146. DOI http://dx.doi.org/10.15585/mmwr.mm6905e1.
Back to Citation2. CMS, “COVID-19 Emergency Declaration Blanket Waivers for Health Care Providers,” (updated Feb. 19 2021) (available at https://www.cms.gov/files/document/summary-covid-19-emergency-declaration-waivers.pdf).
Back to Citation3. CMS, “COVID-19 Frequently Asked Questions (FAQs) on Medicare Fee-for-Service (FFS) Billing,” (updated March 5, 2021) (available at https://www.cms.gov/files/document/03092020-covid-19-faqs-508.pdf).
Back to Citation4. ONC, Draft 2 Trusted Exchange Framework and Common Agreement, https://www.healthit.gov/sites/default/files/page/2019-04/FINALTEFCAQTF41719508version.pdf.
Back to Citation5. The measure steward changed the name of the measure from SARS-CoV-2 Vaccination Coverage among Healthcare Personnel to COVID-19 Vaccination Coverage among Healthcare Personnel. There were no changes to the measure itself, other than the name change.
Back to Citation6. U.S. Dept. of Health and Human Services, Office of the Assistant Secretary for Preparedness and Response. (2020). Determination that a Public Health Emergency Exists. Available at https://www.phe.gov/emergency/news/healthactions/phe/Pages/2019-nCoV.aspx.
Back to Citation7. Centers for Disease Control and Prevention. (2020). Your Health: Symptoms of Coronavirus. Available at https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html.
Back to Citation8. Centers for Disease Control and Prevention. (2020). Your Health: Symptoms of Coronavirus. Available at https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html.
9. Centers for Disease Control and Prevention (2021). Health Equity Considerations and Racial and Ethnic Minority Groups. Available at https://www.cdc.gov/coronavirus/2019-ncov/community/health-equity/race-ethnicity.html.
Back to Citation10. Centers for Disease Control and Prevention. (2020). CDC COVID Data Tracker. Available at https://covid.cdc.gov/covid-data-tracker/#cases_casesper100klast7days.
Back to Citation11. Associated Press. Tired to the Bone. Hospitals Overwhelmed with Virus Cases. November 18, 2020. Accessed on December 16, 2020, at https://apnews.com/article/hospitals-overwhelmed-coronavirus-cases-74a1f0dc3634917a5dc13408455cd895. Also see: New York Times. Just how full are U.S. intensive care units? New data paints an alarming picture. November 18, 2020. Accessed on December 16, 2020, at https://www.nytimes.com/2020/12/09/world/just-how-full-are-us-intensive-care-units-new-data-paints-an-alarming-picture.html.
Back to Citation12. NPR. U.S. Hits 100,000 COVID-19 Hospitalizations, Breaks Daily Death Record. Dec. 2, 2020. Accessed on December 17, 2020 at https://www.npr.org/sections/coronavirus-live-updates/2020/12/02/941902471/u-s-hits-100-000-covid-19-hospitalizations-breaks-daily-death-record;; The Wall Street Journal. Coronavirus Live Updates: U.S. Hospitalizations, Newly Reported Cases, Deaths Edge Downward. Accessed on January 11 at https://www.wsj.com/livecoverage/covid-2021-01-11.
Back to Citation13. Centers for Disease Control and Prevention. (2020). CDC COVID Data Tracker. Available at https://covid.cdc.gov/covid-data-tracker/#cases_casesper100klast7days.
Back to Citation14. Centers for Disease Control and Prevention. (2021). COVID-19. Your Health. Frequently Asked Questions. Accessed on January 11, 2021 at https://www.cdc.gov/coronavirus/2019-ncov/faq.html.
Back to Citation15. Centers for Disease Control and Prevention (2021). COVID-19. Your Health. Frequently Asked Questions. Accessed on January 11, 2021 at https://www.cdc.gov/coronavirus/2019-ncov/faq.html.
Back to Citation16. Centers for Disease Control and Prevention (2021). COVID-19. Your Health. Frequently Asked Questions. Accessed on January 11, 2021 at https://www.cdc.gov/coronavirus/2019-ncov/faq.html.
Back to Citation17. Centers for Disease Control and Prevention. (2020). Clinical Questions about COVID-19: Questions and Answers. Accessed on December 2, 2020 at https://www.cdc.gov/coronavirus/2019-ncov/hcp/faq.html.
Back to Citation18. Centers for Disease Control and Prevention. (2021). How COVID-19 Spreads. Accessed on July 15, 2021 at https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/how-covid-spreads.html.
Back to Citation19. Centers for Disease Control and Prevention. (2020). Interim U.S. Guidance for Risk Assessment and Work Restrictions for Healthcare Personnel with Potential Exposure to COVID-19. Accessed on December 2 at https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-risk-assesment-hcp.html.
Back to Citation20. Dooling, K, McClung, M, et al. “The Advisory Committee on Immunization Practices' Interim Recommendations for Allocating Initial Supplies of COVID-19 Vaccine—United States, 2020.” Morb Mortal Wkly Rep. 2020; 69(49): 1857-1859.
Back to Citation21. Centers for Disease Control and Prevention. (2020). COVID-19 Vaccination Program Interim Playbook for Jurisdiction Operations. Accessed on December 18 at https://www.cdc.gov/vaccines/imz-managers/downloads/COVID-19-Vaccination-Program-Interim_Playbook.pdf.
Back to Citation22. U.S. Food and Drug Administration. (2021). Pfizer-BioNTech COVID-19 Vaccine. Available at https://www.fda.gov/emergency-preparedness-and-response/coronavirus-disease-2019-covid-19/pfizer-biontech-covid-19-vaccine.
Back to Citation23. Ibid.
24. U.S. Food and Drug Administration. (2021). ModernaTX, Inc. COVID-19 Vaccine EUA Letter of Authorization. Available at https://www.fda.gov/media/144636/download.
25. U.S. Food and Drug Administration (2021). Janssen Biotech, Inc. COVID-19 Vaccine EUA Letter of Authorization. Available at https://www.fda.gov/media/146303/download.
Back to Citation26. The White House. Remarks by President Biden on the COVID-19 Response and the State of Vaccinations. March 29, 2021. Accessed at https://www.whitehouse.gov/briefing-room/speeches-remarks/2021/03/29/remarks-by-president-biden-on-the-covid-19-response-and-the-state-of-vaccinations/.
Back to Citation27. Centers for Disease Control and Prevention. Glossary of Terms. https://cdc.gov/infectioncontrol/guidelines/healthcare-personnel/appendix/terminology.html.
Back to Citation28. Health and Human Services, Department of Defense. (2020) From the Factory to the Frontlines: The Operation Warp Speed Strategy for Distributing a COVID-19 Vaccine. Accessed December 18 at https://www.hhs.gov/sites/default/files/strategy-for-distributing-covid-19-vaccine.pdf;; Centers for Disease Control (2020). COVID-19 Vaccination Program Interim Playbook for Jurisdiction Operations. Accessed December 18 at https://www.cdc.gov/vaccines/imz-managers/downloads/COVID-19-Vaccination-Program-Interim_Playbook.pdf.
Back to Citation29. Dooling, K, McClung, M, et al. “The Advisory Committee on Immunization Practices' Interim Recommendations for Allocating Initial Supplies of COVID-19 Vaccine—United States, 2020.” Morb. Mortal Wkly Rep. 2020; 69(49): 1857-1859. ACIP also recommended that long-term care residents be prioritized to receive the vaccine, given their age, high levels of underlying medical conditions, and congregate living situations make them high risk for severe illness from COVID-19.
Back to Citation30. Kates, J, Michaud, J, Tolbert, J. “How Are States Prioritizing Who Will Get the COVID-19 Vaccine First?” Kaiser Family Foundation. December 14, 2020. Accessed on December 16 at https://www.kff.org/policy-watch/how-are-states-prioritizing-who-will-get-the-covid-19-vaccine-first/.
Back to Citation31. Associated Press. `Healing is Coming:' US Health Workers Start Getting Vaccine. December 15, 2020. Accessed on December 16 at https://apnews.com/article/us-health-workers-coronavirus-vaccine-56df745388a9fc12ae93c6f9a0d0e81f.
Back to Citation32. Press Briefing by White House COVID-19 Response Team and Public Health Officials | The White House. Accessed on July 21, 2021 at https://www.whitehouse.gov/briefing-room/press-briefings/2021/06/03/press-briefing-by-white-house-covid-19-response-team-and-public-health-officials-40/.
Back to Citation33. Centers for Medicare & Medicaid Services. Pre-rulemaking. Accessed at https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/QualityMeasures/Pre-Rulemaking.
Back to Citation34. National Quality Forum. List of Measures Under Consideration for December 21, 2020. Accessed at https://www.cms.gov/files/document/measures-under-consideration-list-2020-report.pdf on January 12, 2021.
Back to Citation35. Measure Applications Partnership. MAP Preliminary Recommendations 2020-2021. Accessed on February 3, 2021 at https://www.qualityforum.org/WorkArea/linkit.aspx?LinkIdentifier=id&ItemID=94650.
Back to Citation36. Ibid.
Back to Citation37. Ibid.
Back to Citation38. Ibid.
Back to Citation39. The Influenza Vaccination Coverage among Healthcare Personnel (NQF #0431) measure which is NQF endorsed and was adopted in the IRF QRP in the FY 2014 IRF PPS Final Rule (78 FR 47905 through 47906), and in the LTCH QRP in the FY 2013 IPPS/LTCH PPS Final Rule (77 FR 53630 through 53631).
Back to Citation40. Centers for Disease Control and Preventions. Morbidity and Mortality Weekly Report. March 29, 2021. Available at https://www.cdc.gov/mmwr/volumes/70/wr/mm7013e3.htm?s_cid=mm7013e3_w.
Back to Citation41. National Quality Form. Key Points for Evaluating Scientific Acceptability. Revised January 3, 2020. https://www.qualityforum.org/Measuring_Performance/Scientific_Methods_Panel/Docs/Evaluation_Guidance.aspx#:~:text.
Back to Citation42. Ibid.
Back to Citation43. Centers for Disease Control and Prevention. Interim Clinical Considerations for Use of COVID-19 Vaccines Currently Authorized in the United Sates, Appendix B. Accessed at https://www.cdc.gov/vaccines/covid-19/info-by-product/clinical-considerations.html#Appendix-B.
Back to Citation44. Centers for Disease Control and Prevention. Surveillance for Weekly HCP COVID-19 Vaccination. Accessed at https://www.cdc.gov/nhsn/hps/weekly-covid-vac/index.html on February 10, 2021.
Back to Citation45. Dooling, K, McClung, M, et al. “The Advisory Committee on Immunization Practices' Interim Recommendations for Allocating Initial Supplies of COVID-19 Vaccine—United States, 2020.” Morb Mortal Wkly Rep. 2020; 69(49): 1857-1859.
Back to Citation46. CBS News. More than 20 States Not Ordering All Available Doses as COVID-19 Vaccinations Slow. May 3, 2021. Available at https://www.cbsnews.com/news/covid-19-vaccine-doses-states/. Accessed June 24, 2021.
Back to Citation47. GoodRx. From Shortage to Surplus: A Growing Number of U.S. Counties Have Vacant COVID-19 Vaccine Appointments. April 20, 2021. Available at https://www.goodrx.com/;blog/covid-19-vaccine-surplus-vacant-appointments/. Accessed June 24, 2021.
Back to Citation48. Centers for Disease Control and Prevention. Vaccine Administration. Available at https://www.cdc.gov/vaccines/covid-19/clinical-considerations/covid-19-vaccines-us.html. Accessed June 25, 2021.
Back to Citation49. Centers for Disease Control and Prevention. Population Immunity. Available at https://www.cdc.gov/coronavirus/2019-ncov/vaccines/keythingstoknow.html. Accessed June 25, 2021.
Back to Citation50. Centers for Disease Control and Prevention. Covid-19 vaccines and new variants. Available at https://www.cdc.gov/coronavirus/2019-ncov/vaccines/effectiveness/work.html#:~:text=COVID%2D19%20vaccines%20and%20new%20variants%20of%20the%20virus&text=Current%20data%20suggest%20that%20COVID,after%20they%20are%20fully%20vaccinated. Accessed June 25, 2021.
Back to Citation51. Effectiveness of Pfizer-BioNTech and Moderna Vaccines Against COVID-19 Among Hospitalized Adults Aged ≥65 Years—United States, January-March 2021. Morbidity and Mortality Weekly Report (MMWR). May 7, 2021. Available at https://www.cdc.gov/mmwr/volumes/70/wr/mm7018e1.htm?s_cid=mm7018e1_w. Accessed July 19, 2021.
Back to Citation52. The Advisory Committee on Immunization Practices' Interim Recommendation for Use of Janssen COVID-19 Vaccine—United States, February 2021. Morbidity and Mortality Weekly Report (MMWR). March 5, 2021. Available at https://www.cdc.gov/mmwr/volumes/70/wr/mm7009e4.htm. Accessed July 19, 2021.
Back to Citation53. Medscape. Disturbing Number of Hospital Workers Still Unvaccinated. Available at https://www.medscape.com/viewarticle/953871. Accessed July 13, 2021.
Back to Citation54. Centers for Disease Control and Prevention. Building Confidence in COVID-19 Vaccines. Available at https://www.cdc.gov/vaccines/covid-19/vaccinate-with-confidence.html.
Back to Citation55. Centers for Medicare and Medicaid Services. Coronovirus (COVID-19) Partner Resources. Available at https://www.cms.gov/outreach-education/partner-resources/coronavirus-covid-19-partner-resources.
Back to Citation56. Centers for Disease Control and Prevention. Updated Healthcare Infection Prevention and Control Recommendations in Response to COVID-19 Vaccination. Available at https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-after-vaccination.html. Accessed June 26, 2021.
Back to Citation57. U.S. Equal Employment Opportunity Commission. What You Should Know About COVID-19 and the ADA, the Rehabilitation Act, and Other EEO Laws. Available at https://www.eeoc.gov/wysk/what-you-should-know-about-covid-19-and-ada-rehabilitation-act-and-other-eeo-laws. Accessed June 25, 2021.
Back to Citation58. U.S. Equal Employment Opportunity Commission. What You Should Know About COVID-19 and the ADA, the Rehabilitation Act, and Other EEO Laws. Available at https://www.eeoc.gov/wysk/what-you-should-know-about-covid-19-and-ada-rehabilitation-act-and-other-eeo-laws. Accessed June 25, 2021.
Back to Citation59. U.S. Equal Employment Opportunity Commission. What You Should Know About COVID-19 and the ADA, the Rehabilitation Act, and Other EEO Laws. Available at https://www.eeoc.gov/wysk/what-you-should-know-about-covid-19-and-ada-rehabilitation-act-and-other-eeo-laws. Accessed June 25, 2021.
Back to Citation60. Centers for Disease Control and Prevention. Guidance for Unvaccinated People: How to Protect Yourself & Others. June 11, 2021. Available at https://www.cdc.gov/coronavirus/2019-ncov/prevent-getting-sick/prevention.html. Accessed June 24, 2021.
Back to Citation61. Centers for Disease Control and Prevention. (2021). Symptoms of COVID-19. Available at https://www.cdc.gov/coronavirus/2019-ncov/symptoms-testing/symptoms.html. Accessed June 24, 2021.
Back to Citation62. Centers for Disease Control and Prevention. (2020). CDC COVID Data Tracker. Available at https://covid.cdc.gov/covid-data-tracker/#cases_casesper100klast7days. Accessed June 24, 2021.
Back to Citation63. Vaccinate Your Family website. Vaccines are cost saving. Available at https://vaccinateyourfamily.org/why-vaccinate/vaccine-benefits/costs-of-disease-outbreaks/. Accessed June 25, 2021.
Back to Citation64. U.S. Department of Health & Human Services. 2010 National Vaccine Plan. Available at https://www.hhs.gov/sites/default/files/nvpo/vacc_plan/2010-Plan/nationalvaccineplan.pdf. Accessed June 25, 2021.
Back to Citation65. National Quality Forum. Priority Setting for Healthcare Performance Measurement: Addressing Performance Measure Gaps for Adult Immunizations. Available at https://www.qualityforum.org/Publications/2014/08/Priority_Setting_for_Healthcare_Performance_Measurement_Addressing_Performance_Measure_Gaps_for_Adult_Immunizations.aspx. Accessed June 25, 2021.
Back to Citation66. Data Tracking Worksheet for COVID-19 Vaccination among Healthcare Personnel at https://www.cdc.gov/nhsn/hps/weekly-covid-vac/index.html.
Back to Citation67. Medscape. Disturbing Number of Hospital Workers Still Unvaccinated. Available at https://www.medscape.com/viewarticle/953871. Accessed July 13, 2021.
Back to Citation68. National Quality Forum. Influenza Vaccination Coverage among Healthcare Personnel. Available at https://qualityforum.org/QPS/QPSTool.aspx?Exact=fase&Keyword=0431#. Accessed June 26, 2021.
Back to Citation69. National Healthcare Safety Network. Instructions for Completion of the Weekly Healthcare Personnel COVID-19 Cumulative Vaccination Summary Form for Non-Long-Term Care Facilities (57.220, Rev 3). Available at https://www.cdc.gov/nhsn/forms/instr/57.220-toi-508.pdf. Accessed June 26, 2021.
Back to Citation70. Centers for Disease Control and Prevention. COVID Data Tracker. Available at https://covid.cdc.gov/covid-data-tracker/#vaccinations. Accessed June 26, 2021.
Back to Citation71. Centers for Disease Control and Prevention. Safety of COVID-19 Vaccines. Available at https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/safety-of-vaccines.html. Accessed June 26, 2021.
Back to Citation72. National Healthcare Safety Network. Instructions for Completion of the Weekly Healthcare Personnel COVID-19 Cumulative Vaccination Summary Form for Non-Long-Term Care Facilities (57.220, Rev 3). Available at https://www.cdc.gov/nhsn/forms/instr/57.220-toi-508.pdf. Accessed June 26, 2021.
Back to Citation73. Centers for Disease Control and Prevention. Building Confidence in COVID-19 Vaccines. Available at https://www.cdc.gov/vaccines/covid-19/vaccinate-with-confidence.html. Accessed June 24, 2021.
Back to Citation74. U.S. Equal Employment Opportunity Commission. What You Should Know About COVID-19 and the ADA, the Rehabilitation Act, and Other EEO Laws. Available at https://www.eeoc.gov/wysk/what-you-should-know-about-covid-19-and-ada-rehabilitation-act-and-other-eeo-laws. Accessed June 25, 2021.
Back to Citation75. National Quality Forum. Measure Applications Partnership 2020-2021 Considerations for Implementing Measures in Federal Programs: Clinician, Hospital & PAC/LTC. Final Report. March 11, 2021. Available at http://www.qualityforum.org/Projects/i-m/MAP/MAP_2020-2021_Considerations_for_Implementing_Measures_Final_Report.aspx. Accessed June 26, 2021.
Back to Citation76. Geller, et al. Surveillance of COVID-19 vaccination in US nursing homes, December 2020-April 2021. Medrxiv.org. Available at https://www.medrxiv.org/content/10.1101/2021.05.14.21257224v1.full.pdf. Accessed June 26, 2021.
Back to Citation77. National Quality Forum. Influenza Vaccination Coverage among Healthcare Personnel. Available at https://qualityforum.org/QPS/QPSTool.aspx?Exact=fase&Keyword=0431#. Accessed June 26, 2021.
Back to Citation78. National Institute for Health Care Management (NIHCM). Aging & COVID-19: Vaccination, Mental and Physical Health, and Isolation. Updated February 17, 2021. Available at https://nihcm.org/publications/aging-covid-19-vaccination-mental-and-physical-health-and-isolation. Accessed June 26, 2021.
Back to Citation79. Centers for Disease Control and Prevention. Science Brief: Evidence used to update the list of underlying medical conditions that increase a person's risk of severe illness from COVID-19. Available at https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/underlying-evidence-table.html. Accessed June 26, 2021.
Back to Citation80. In response to the COVID-19 PHE, CMS released an Interim Final Rule (85 FR 27595 through 27597) which delayed the compliance date for the collection and reporting of the SDOH for at least one full fiscal year after the end of the PHE.
Back to Citation81. https://qualitynet.cms.gov/inpatient/measures/disparity-methods/methodology.
Back to Citation82. Centers for Disease Control and Prevention. Surveillance for Weekly HCP COVID-19 Vaccination. Accessed at https://www.cdc.gov/nhsn/hps/weekly-covid-vac/index.html on February 10, 2021.
Back to Citation83. Centers for Disease Control and Prevention. Measure Specification: NHSN COVID-19 Vaccination Coverage Updated March 2021. Available at https://www.cdc.gov/nhsn/pdfs/nqf/covid-vax-hcpcoverage-508.pdf. Accessed June 27, 2021.
Back to Citation84. The NHSN Influenza Vaccination among HCP measure's (NQF #0431) data collection period is tied to the influenza vaccination season.
Back to Citation85. We refer readers to Section IX.H.3. of the FY 2016 IRF PPS Final Rule (80 FR 47122 to 47123). Available at https://www.federalregister.gov/documents/2015/08/06/2015-18973/medicare-program-inpatient-rehabilitation-facility-prospective-payment-system-for-federal-fiscal. Accessed June 26, 2021.
Back to Citation86. Centers for Disease Control and Prevention. Covid-19 vaccines and new variants. Available at https://www.cdc.gov/coronavirus/2019-ncov/vaccines/effectiveness/work.html#:~:text=COVID%2D19%20vaccines%20and%20new%20variants%20of%20the%20virus&text=Current%20data%20suggest%20that%20COVID,after%20they%20are%20fully%20vaccinated. Accessed June 25, 2021.
Back to Citation87. U.S. Equal Employment Opportunity Commission. What You Should Know About COVID-19 and the ADA, the Rehabilitation Act, and Other EEO Laws. Available at https://www.eeoc.gov/wysk/what-you-should-know-about-covid-19-and-ada-rehabilitation-act-and-other-eeo-laws. Accessed June 25, 2021.
Back to Citation88. https://www.phe.gov/emergency/news/healthactions/section1135/Pages/covid19-13March20.aspx.
Back to Citation90. More information about the IRF QRP Public Reporting schedule can be found on the IRF QRP Public Reporting website at https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/IRF-Quality-Reporting/IRF-Quality-Public-Reporting.
Back to Citation91. Section 321 of the NCVIA provides the PRA waiver for activities that come under the NCVIA, including those in the NCVIA at section 2102 of the Public Health Service Act (42 U.S.C. 300aa-2). Section 321 is not codified in the U.S. Code, but can be found in a note at 42 U.S.C. 300aa-1.
Back to Citation92. https://www.bls.gov/oes/current/oes_nat.htm. Accessed on March 30, 2021.
Back to CitationBILLING CODE 4120-01-P
BILLING CODE 4120-01-C
BILLING CODE 4120-01-P
BILLING CODE 4120-01-C
BILLING CODE 4120-01-P
BILLING CODE 4120-01-C
BILLING CODE 4120-01-P
BILLING CODE 4120-01-C
BILLING CODE 4120-01-P
BILLING CODE 4120-01-C
[FR Doc. 2021-16310 Filed 7-29-21; 4:15 pm]
BILLING CODE 4120-01-P
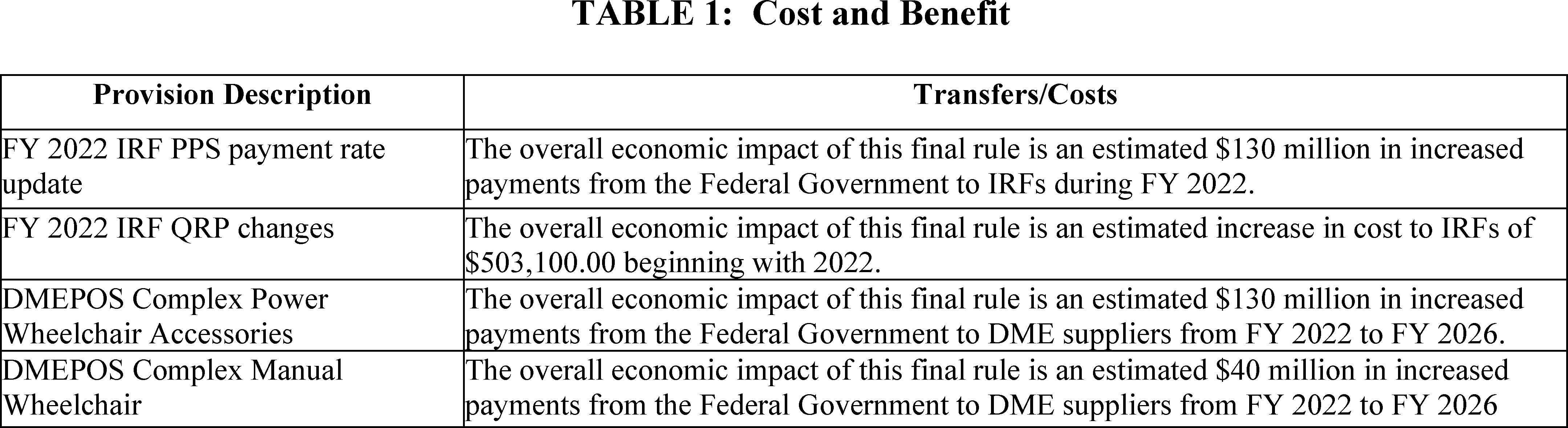
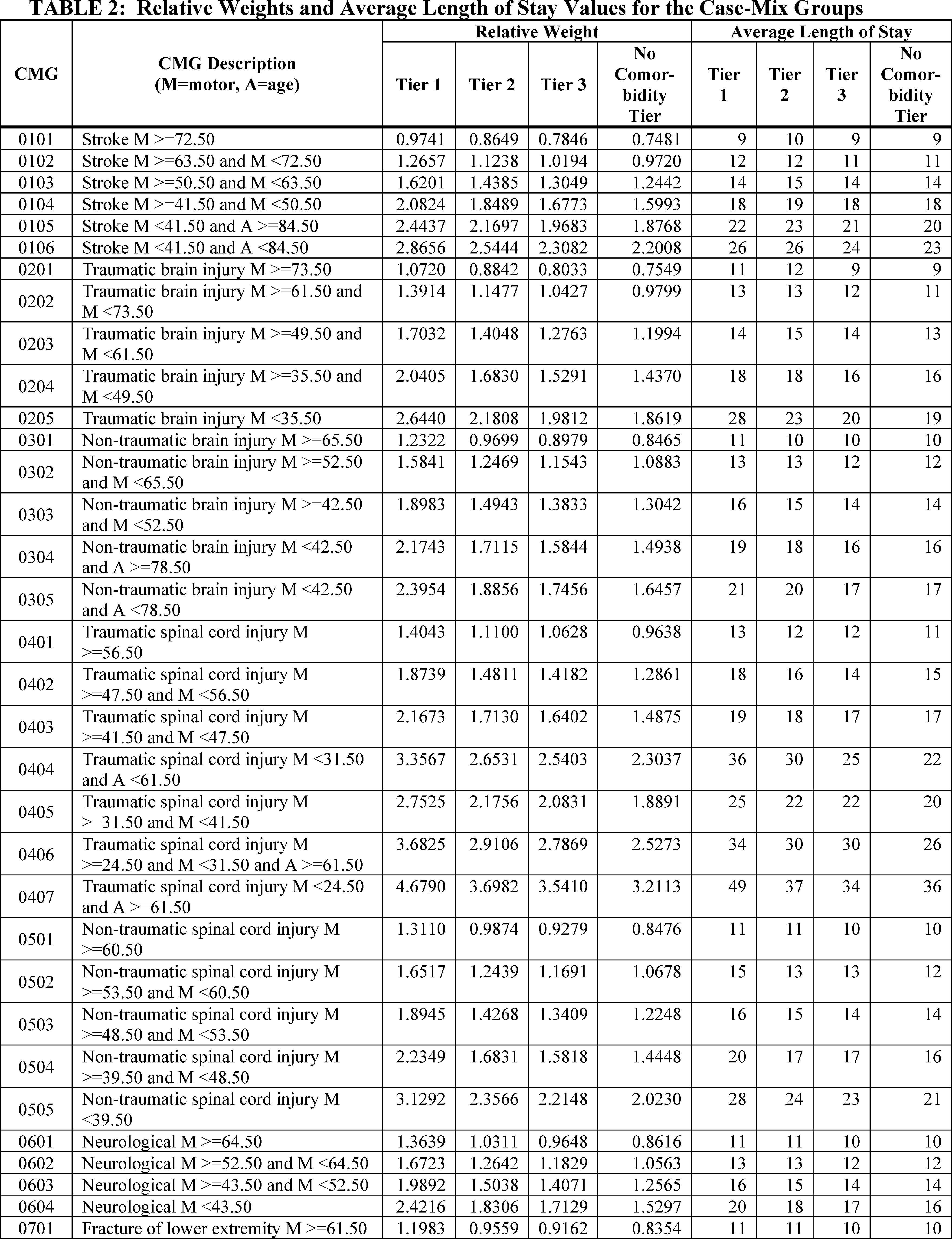






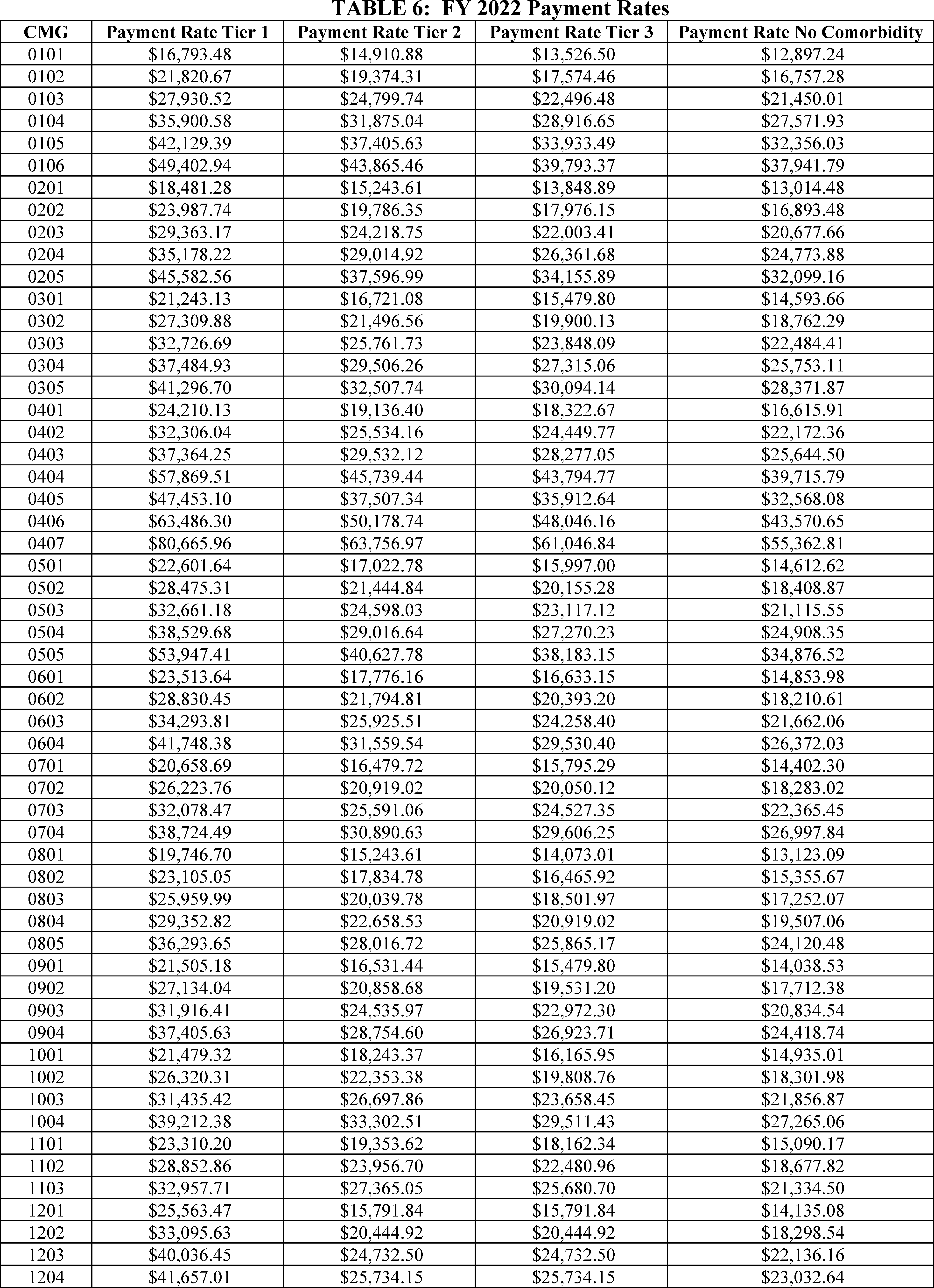









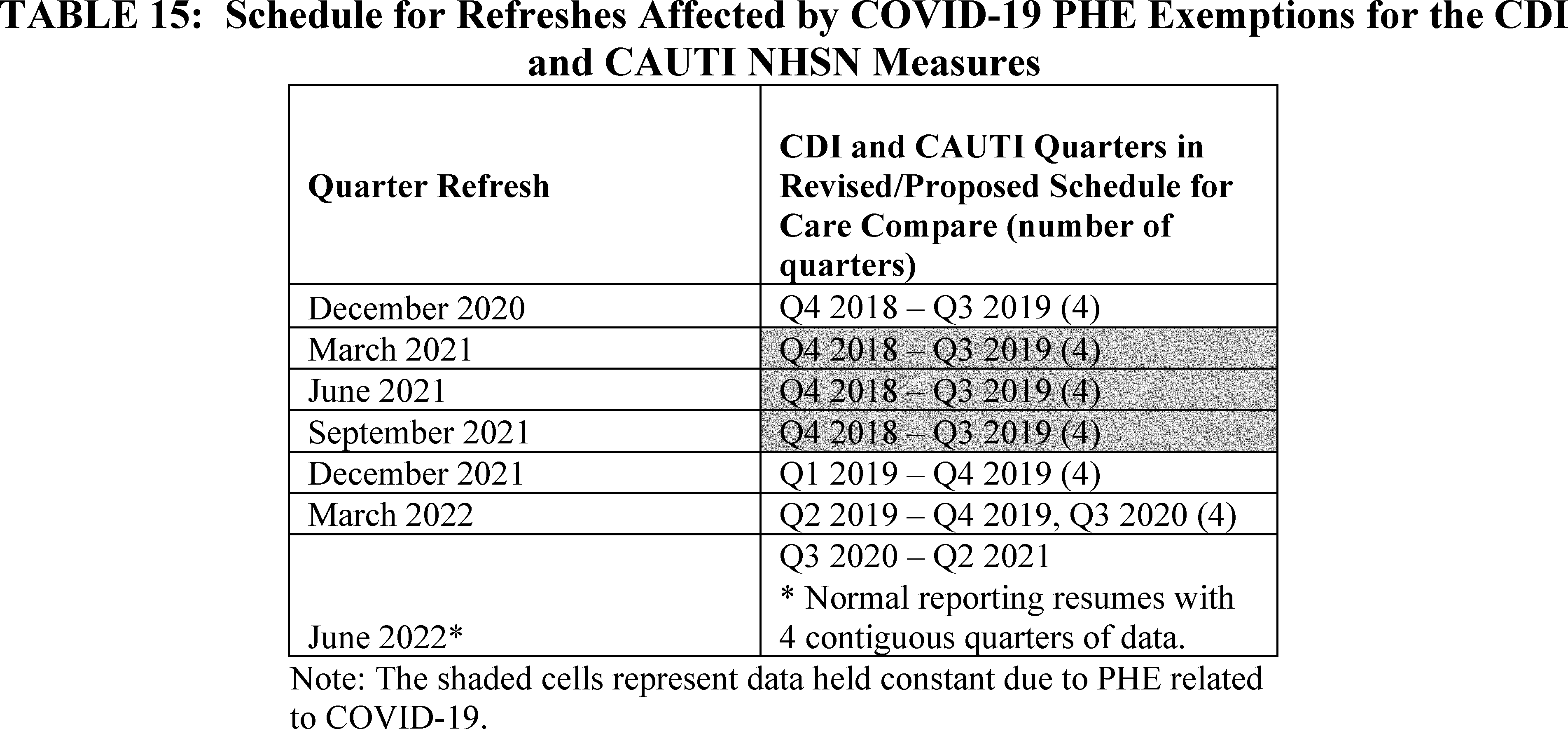






Document Information
- Effective Date:
- 10/1/2021
- Published:
- 08/04/2021
- Department:
- Centers for Medicare & Medicaid Services
- Entry Type:
- Rule
- Action:
- Final rule.
- Document Number:
- 2021-16310
- Dates:
- Effective date: These regulations are effective on October 1, 2021.
- Pages:
- 42362-42422 (61 pages)
- Docket Numbers:
- CMS-1748-F, CMS-1687-IFC, and CMS-1738-F
- RINs:
- 0938-AT21: Durable Medical Equipment Fee Schedule, Adjustments to Resume the Transitional 50/50 Blended Rates to Provide Relief in Non-Competitive Bidding Areas (CMS-1687), 0938-AU17: Durable Medical Equipment, Prosthetics, Orthotics and Supplies (DMEPOS) Policy Issues and Level II of the Healthcare Common Procedure Coding System (HCPCS) (CMS-1738), 0938-AU38: FY 2022 Inpatient Rehabilitation Facility (IRF) Prospective Payment System Rate Update and Quality Reporting Requirements (CMS-1748)
- RIN Links:
- https://www.federalregister.gov/regulations/0938-AT21/durable-medical-equipment-fee-schedule-adjustments-to-resume-the-transitional-50-50-blended-rates-to, https://www.federalregister.gov/regulations/0938-AU17/durable-medical-equipment-prosthetics-orthotics-and-supplies-dmepos-policy-issues-and-level-ii-of-th, https://www.federalregister.gov/regulations/0938-AU38/fy-2022-inpatient-rehabilitation-facility-irf-prospective-payment-system-rate-update-and-quality-rep
- Topics:
- Administrative practice and procedure, Biologics, Diseases, Drugs, Health facilities, Health professions, Medicare, Reporting and recordkeeping requirements
- PDF File:
- 2021-16310.pdf
- Supporting Documents:
- » Medicare Program: Inpatient Rehabilitation Facility Prospective Payment System for Federal Fiscal Year 2022 and Updates to the IRF Quality Reporting Program; Payment for Complex Rehabilitative Wheelchairs and Related Accessories (Including Seating Systems) and Seat and Back Cushions Furnished in Connection with Such Wheelchairs
- » Medicare Program: Inpatient Rehabilitation Facility Prospective Payment System for Federal Fiscal Year 2022 and Updates to the IRF Quality Reporting Program (CMS-1748-P)
- » Display - Inpatient Rehabilitation Facility Prospective Payment System for Federal Fiscal Year 2022 and Updates to the IRF Quality Reporting Program (CMS-1748-P)
- CFR: (1)
- 42 CFR 414.402